liver abscess
TRANSCRIPT
LIVER ABSCESS
By :Hamad Emad Hamad
Dhuhayr

OBJECTIVES
Anatomy of liver Classification Etiology and patho-physiology Management

ANATOMY OF LIVER

CLASSIFICATIONPYOGENIC
Gram Positive Gram-negative Anaerobic
Staph aureus,Strepto pyogenes,Strepto milleri,strepto faecalis
E coli,Klebsiella,Proteus Bacteroids,Clostridium,Actinomyces
AMOEBIC
CANDIDA
TB (rare)

PATHO PHYSIOLOGY
Liver largest portion of reticuloendothelial system so continuous exposure to bacteria from enteric tract
Due to high level of reticuloendothelial tissue, non-viral infections are uncommon

RISK FACTORS
PYOGENIC DM Cancer Liver Transplant
ENTAMOEBA Pregnancy Steroids Cancer Endemic area travel (short or long term)

PYOGENIC LIVER ABSCESS

EPIDEMIOLOGY
MALE > FEMALE3 : 1
MORE IN RIGHT LOBE, SUPERIOR ASPECT INCREASED INCIDENCE IN DIABETES
MELLITIS

PATHO PHYSIOLOGY OF PYOGENIC ABCESS PYOGENIC:
Peritonitis To liver via portal circulation
Direct Spread Biliary infections(ascending cholingitis
Hematogenous Seeding Bacteremia, septecemia(unusual)
Adjacent infections Sub phrenic abscess, Cholecystitis
Sites: R lobe most common Blood supply

…PATHO PHYSIOLOGY
Mostly multiple abscesses/sometimes single 40 % monomicrobial 40 % polymicrobial 20 % negative culture

SIGN AND SYMPTOMS
Rigors high swinging temp(90 %) Tender palpable liver(50 %) Jaundice 1/3 Charcot’s triad Or non-specific malaise over month

INVESTIGATIONS
NON SPECIFIC total lymphocyte count: increase leukocytosis Increase ESR Increase alk phosphate(mild)(67-90%)
SPECIFIC USG DIAGNOSTIC ASPIRATION & CULTURE SENSITIVITY CT scan

ULTRASOUND OF PYOGENIC ABSCESS
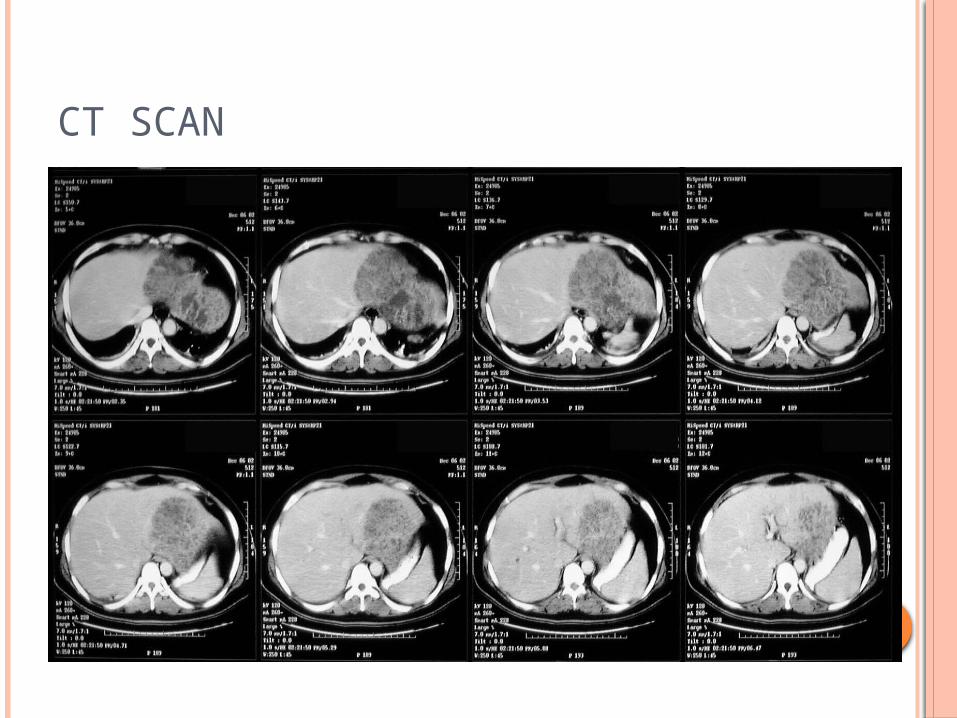
CT SCAN

TREATMENT
MEDICAL BROAD SPECTRUM ANTIBIOTICS
triple regime(penicillin , amino glycoside and Metronidazole)
cephalosporin and Metronidazole SPECIFIC
ACCORDING TO CULTURE SENSITIVITY i/v fluids to prevent hepatorenal syndrome ANALGESICS & ANTIPYRATICS Urgent drainage

CONTINUED
INVASIVE TO DRAIN OR NOT TO DRAIN:
<5cm, single abscess- needle aspiration or catheter
>5cm- catheter Also: Surgery, ERCP
URGENT DRAINAGE USG GUIDED, AND PIG TAIL CATHETER OPEN
ERCP IN CASE OF OBSTRUCTION

AMOEBIC LIVER ABSCESS
AMOEBIC ABSCESS
Epidemiology M > F 7:1 10 % world population 40-50 million amoeba infections/year worldwide Age Extremes Endemic Areas most susceptible Country of origin or Travel

GEOGRAPHIC DISTRIBUTION

ETIOLOGY AND PATHOPHYSIOLOGY
Entemoeba histolytica


MODE OF TRANSMISSION Large intestine (history of dysentery) Travel to liver most common superior aspect near
diaphragm through portal vein Where proliferates to produce cytolytic enzymes Destroy liver tissues Abscess which is sterile(anchovy paste or
chocolate sauce Amoeba may be found in abscess wall

SIGN AND SYMPTOMS
Fever Pain RHC Dysentery Tenderness
INVESTIGATIONS
NON SPECIPIC Increase TLC Increase LFT’s Most common biochemical abnormality(alk phosphate)
SPECIFIC USG CT SCAN IMAGE GUIDED ASPIRATION ANCHOVY SAUCE
LIKE CULTURE AND SENSTIVITY Fluorescent antibody test for Entamoeba(can be
positive even after clinical cure) If serology is negative , amoebiasis is uncertain
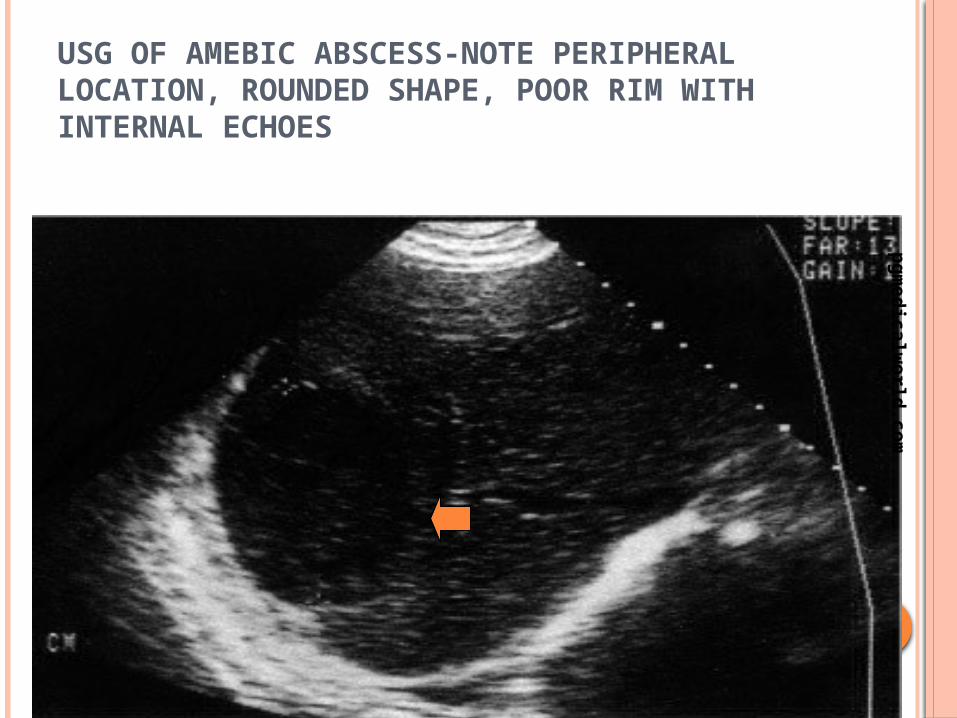
USG OF AMEBIC ABSCESS-NOTE PERIPHERAL LOCATION, ROUNDED SHAPE, POOR RIM WITH INTERNAL ECHOES
pgmedicalw
orld.com

CT SHOWING SUPERFICIAL ABSCESS
pgmedicalw
orld.com

CT SCAN OF AMEBIC ABSCESS (A). THE LESION IS PERIPHERALLY LOCATED AND ROUND. RIM IS NONENHANCING BUT SHOWS PERIPHERAL EDEMA (BLACK ARROWS). NOTE THE EXTENSION INTO THE INTERCOSTAL SPACE (WHITE ARROWS).
pgmedicalw
orld.com

TREATMENT
NON INVASIVE Metronidazole 400-800 mg TDS …….7 to 10 days
INVASIVE Ultrasound guided aspiration Surgery
Amoeba: drainage not usually required Exceptions:
Verge of rupture Abx not working Imminent need to exclude other dx Large abscess

COMPARISON

PROGNOSIS & NATURAL HISTORY
• Mortality 2-12%• Often due to co morbidities, not
necessarily abscess itself
SUMMARY
If untreated LA is potentially fatal. Must be diagnosed & treated promptly Investigations-LFT,USG and CT SEROLOGY-corner stone to differentiate Pyogenic liver abscess-Antibiotics plus
drainage Causative pathology should also be treated

ALA-most cases treated with amebicidal agents alone with drainage procedures reserved for resistant or complicated cases
Luminal amebicides should also be given When there is high index of suspicion for LA
Rx should not be withheld until diagnosis is confirmed

REFERRENCES
Baily and love

Thank you