lipid. molecules made up of long hydrocarbon chains fatty acids - single chain hydrocarbons with 4...
TRANSCRIPT

Lipid

Lipid Molecules made up of long hydrocarbon chains
Fatty Acids - single chain hydrocarbons with 4 – 22 carbons
Triglycerides - 3-carbon glycerol backbone with three fatty acids attached to the 3 carbons
Diglycerides - above with 2 fatty acids
Monoglycerides - above with 1 fatty acid
Phospholipids - glycerol with fatty acids attached to carbons 1 & 2 with a phosphorous attached to the 3rd.
Cholesterol - 3 6-carbon & 1 5-hydrocarbon rings (modified to produce the various steroids)

EFA’sStructure of some lipids
Glycerol
Fatty Acids

Omega 3
One of those “evil” trans-fats*
Omega 3
Omega 3
Omega 6
*The only reason “trans-fats” are considered bad is because high consumption of these tends to increase serum TGs and LDLs; neither of which are the actual cause of CAD; and no experiments in humans has ever demonstrated an actual increase in mechanisms of disease by doing so!

Dietary Fat is a source of the Essential Fatty Acids: Linoleic and α-linolenic acid.
Arachidonic acid (AA) is synthesized from linoleic acid;
Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are synthesized from α-linolenic acid
Arachidonic acid is made into various proinflammatory prostaglandins, leukotrienes, and thromboxanes; - predominantly PGE2, PGI2, TXA2, LTB4, and LTC4; the START signals for inflammation
- as inflammatory responses progress toward resolution, increased synthesis of COX-2 and 12- & 15-lipoxygenase enzymes shifts production of proinflammatory eicosanoids to the production of anti-inflammatory lipoxins from AA; essentially STOP signals for inflammation
DHA and EPA are made into anti-inflammatory signaling compounds called resolvins, protectins, and maresins; essentially the STOP signals for inflammation
EPA can be made into the less proinflammatory PGE3, PGA3, PGD3, and TXA3/TXB3, and LTB5; and reduces production of PGE2 and LTB4

Α-Linolenic
EPA
DHA
~ 0.2%
~ 37%
~ 63%
Pawloski et al. 2001

Proinflammatory prostaglandins, leukotrienes, and thromboxanes are synthesized from arachidonic acid.

Proresolution lipoxins are synthesized from arachidonic acid and proresolution resolvins, and maresins are synthesized from DHA and EPA to shut down an inflammatory response.

Other Physiologic/Metabolic Uses of Lipids:
Synthesize steroid hormones from cholesterol
Synthesize bile from cholesterol & FFA
Membrane phospholipids
Essential component of PDH & α-kGDH
Primary storage form of NRG & major substrate for energy (especially at rest)
Absorption of Fat soluble vitamins (A, D, E, &K)
Common Food Sources (oils)
linoleic: corn, safflower, soybeans, peanuts, sunflower seeds…
α-linolenic: soybeans, linseed, flax, most other seed oils…

Steroid hormonesare made fromcholesterol

Bile acids are also synthesized from cholesterol . . .

AI 12 & 17 g/day linoleic acid (C18:2; n6, 9 - all cis): F / M; based on on median intake1.1 & 1.6 g/day α-linolenic acid (C18:3; n9, 12, 15 - all cis) F / M; based on median intakeOr: 10 - 35% of total calories (9kcal/g)… so… lets see what you have to eat to…
Some older texts suggested a minimum total intake of 20g/day to insure a sufficient uptake of fat soluble vitamins which greatly underestimates the actual dietary lipid requirement (RDAs are based on fatty acid intake, not TG intake and eating exactly 12g linoleic acid or 1.1 g α-linolenic acid would obviously necessitate eating more than 13g total fat since the EFA are a small minority of total FFAs)
EFA Content of various foods in % of total FA
Linoleic α-Linolenic % Fat by WtCanola Oil ~ 26 - 100Corn Oil ~ 35 - 65 - 100Olive Oil ~ 3 - 20% ~ 1% 100Palm Oil ~ 6 - 12 ~ 0.5 100Peanut Oil ~ 14 - 43 ~ 0.4 100Flax Oil ~ 14 ~ 50 - 60 100Beef (grain-fed-trimmed) ~ 3.4 ~ 0.4 ~ 5Beef (grass-fed-trimmed) ~ 4.4 ~ 1.2 ~ 2.5Chicken (skinless-breast) ~ 21 ~ 0.9 ~ 4.5Salmon (Norway-wild) ~ 1 ~ 1 (2%EPA/20% DHA) ~ 3 - 4
Human Milk ~7 - 18 ~ 1 ~ 2 - 4Cow Milk Fat ~ 2.6 ~ 1.6 ~ 0, 1, 2, or ~3.5
Based on the EFA content of common foods (as a percent of total fatty acids) you clearly have to eat a lot more grams of fat than the RDA (as expressed in grams for the EFA’s) ) – 60 g/day would not be an outlandish estimate if you consume the usual (North American) array of fats (see next slide…)

so let’s figure it out… average calories/day for adults 19 – 50 yrs: ~ 2400 F ~ 3000 M at 10% - 35% calories from fat… (240 – 840 kcal) (300 – 1050 kcal)
EFA Content of various foods in % of total FA
Linoleic α-Linolenic % Fat *Fat intake / kCal Fat intake / kCal Total “Food” Intake mean (range) by Wt (g) (g) to meet RDA
Linoleic α-Linolenic (min g/kcal)
Canola Oil ~ 26 - 100 48/432 - -Corn Oil ~ 50 (35 – 65) - 100 18-34 /162-306 - -Olive Oil ~ 10 (3 – 20) ~ 1 100 60-400/54-3600 110/990 110/990Palm Oil ~ 9 (6 – 12) ~ 0.5 100 100-200/900-1800 220/1980 220/1980Peanut Oil ~ 30 (14 – 43) ~ 0.4 100 30-85/270-765 275/2475 275/2475Flax Oil ~ 14 ~ 50 (50 – 60) 100 86/774 2-3/18-24 86/774Beef (grain-trimmed) ~ 3.4 ~ 0.4 ~ 5 353/3177 275/2475 7060/30,005Beef (grass-trimmed) ~ 4.4 ~ 1.2 ~ 2.5 272/2448 916/819 10,880/44,880Chicken (skinless-breast) ~ 21 ~ 0.9 ~ 4.5 57/513 122/1098 2711/11,454Salmon - Norway - wild ~ 1 ~ 1 ~ 3-4 1200/10,800 110/990 30,000/125,000 Human Milk ~ 10 (7 – 18) ~ 1 ~ 2-4 67-171/603-1539 110/990 4275/ why botherCow Milk (butter fat) ~ 2.6 ~ 1.6 ~ 2 461/4149 69/621 23,050/ “
Based on the EFA content of common foods (as a percent of total fatty acids) you clearly have to eat a lot more grams of fat than the AI (as expressed in grams for the EFA’s)
*Fat Intake calculated for an (“average”) adult female (for males, the intake would be approximately 25% higher). Calculations of total food intake are based on that single food item being the sole source of EFAs.
From these values it is clear that eating less than 30% of calories from common sources of fat is a near guarantee of EFA (borderline?) deficiency. It also is clear that the fat in meats & milk is not very relevant in terms of significant contributions to total EFA intake. Fats in “spreads”, cooking oils, and cheeses seem to make the most difference… and of the added fats, cold-press, virgin olive oil (tends to be at the lower end in linoleic content) and butter/cheese from cows, along with cooked fish 2x/week and maybe a small amount of added flax oil would be the most logical frequent choices to ensure adequate intake of the EFAs and of DHA & EPA .
Using the average EFA content of oils... ~4g Flax oil ensures adequate α-Linolenic for both men and women. Add to that 46g and 65g Canola for linoleic requirements (♀ & ♂, respectively) to get minimum fat intakes of 50 and 69g! Or add 24 g and 34g of corn oil for a minimum total of 28g and 38g (♀ & ♂, respectively).... Or add 120 g and 170 g olive oil for a minimum of 124 and 174 g (♀ & ♂, respectively)... Or add 40 g and 57 g peanut oil for a minimum of 44 and 61 g (♀ & ♂, respectively)... And so on and so on and so on... With the exception of a flax/corn oil mix it looks like lots of fat calories are necessary...
With canola, palm, and corn oils being the major oils used in cooking oils and spreads in the US (and among the lowest in α-Linolenic content); and with constant admonition against animal fats, it is no wonder that 30% of Americans now eat insufficient amounts of α-Linolenic acid.



Two major dietary/nutritional problems with “fat” are: 1) consuming too few EFAs; insufficient consumption of α-Linolenic acid (30% of Americans) leads to poor control of inflammation and high risk for all chronic diseases... 2) over consumption of calories leads to increases in the amount of adipose tissue and fat cells.
With caloric excess, endoplasmic reticulum dysfunction occurs in adipocytes. This condition reduces the ability of adipocytes to synthesize TGs so they release FFAs into the blood. In addition, production of MCP-1, TNFα and other pro-inflammatory cytokines by adipose cells leads to the recruitment and activation of monocytes into the tissue to become new macrophages as well as the activation of resident macrophages to greatly enhance the production of proinflammatory cytokines , growth factors, and PGs, TXs, and LTs. The enhanced levels of prostaglandins activate cell division of the resident mesenchymal stem cells while the resulting daughter cells are stimulated to differentiate into new functional adipocytes through binding of the (excess) FFA to PPARα; the numerous cytokines and growth factors released by the adipocytes and inflammatory cells also initiate and sustain angiogenesis to supply the expanding adipose tissue.
These proinflammatory molecules also enter the circulation to enhance inflammatory functions throughout the entire body with detrimental results: chronic release of TNFα and FFA leads to both mitochondrial dysfunction and insulin resistance in both adipocytes and skeletal muscle.
Calorie overload → TG synthesis → adipocyte hypertrophy → ER dysfunction → inflammatory signaling → adipocyte hyperplasia → adipose angiogenesis & ↑TNFα and FFA → IR
inflammatory signaling → high risk for all chronic diseases
Abdominal fat is more “pro-inflammatory” than subcutaneous fat with a preferential infiltration by macrophages and it is known that adipogenesis in abdominal fat pads is a more substantial risk associated with CHD, cancer, and other chronic diseaseas than subcutaneous fat.

Calorie overload → TG synthesis → Adipocyte Hypertrophy → ER Dysfunction → Inflammatory Signaling → Adipocyte Hyperplasia → Adipose Angiogenesis & ↑TNFα and FFA → IR
With continuing caloric overload the expanding size of the adipose tissue accumulates much greater numbers of inflammatory cells, producing a tissue that is even more sensitive to proinflammatory stresses of caloric overload: a vicious cycle of accelerating risk with constant gain in adiposity.

Digestion/Absorption & Distribution Issues
For Lipids
- Mastication in mouth Bolus w/ saliva/mucus
- Lipids break up to tiny droplets in chyme from stomach/acid action
- Bile from liver bile salts & acids made from cholesterol, fatty acids, sodium, potassium & chloride
-Lipases from Pancreas
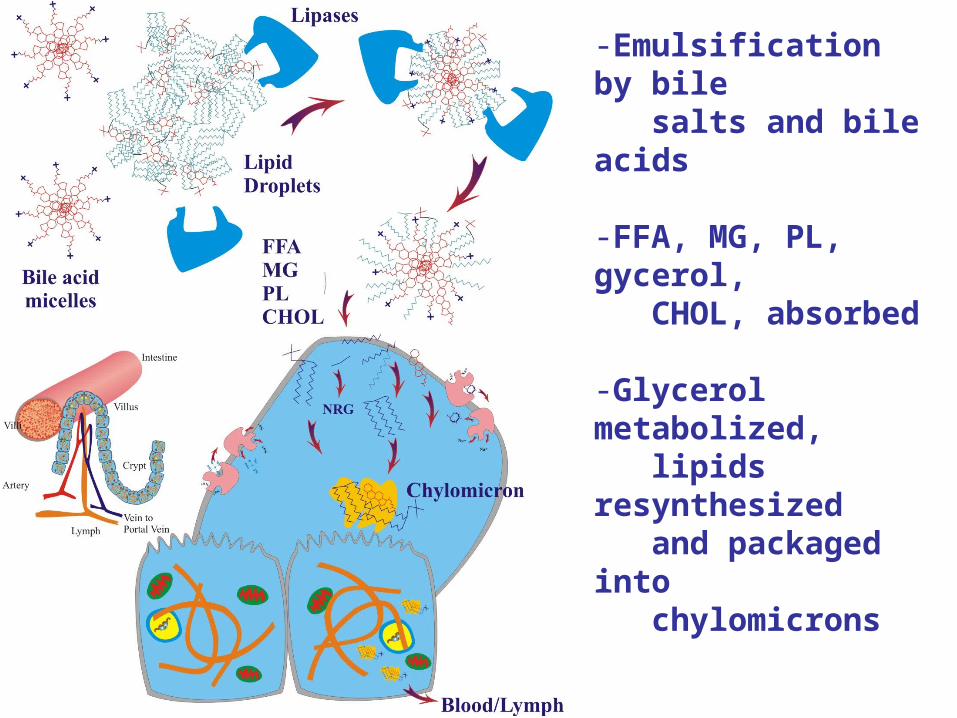
-Emulsification by bile salts and bile acids
-FFA, MG, PL, gycerol, CHOL, absorbed
-Glycerol metabolized, lipids resynthesized and packaged into chylomicrons
(apoB-48, *apoC-II, apoC-III, apoE)

Chylomicrons - Lipoprotein + lipids TG PL Chol ~85% ~9% ~4%
released into lymph/blood ~ 50 : 50
ApoC-II activates lipoprotein lipase in capillaries
Tissues remove FFA, PL
Liver picks up chylomicron remnants

Lipoprotein content of the chylomicron changes as it circulates throughout the body - acquiring the apo E & C2 from HDL
apoE & apoB-48 are ligands for liver uptake of remnants . . . apoCII is ligand to activate lipoprotein lipase for removal of fatty acids in tissues . . .
Deliver dietary TG and PL to cells dietary CHOL to liver . . .

apoE is ligand for liver uptake & apoB-100 is ligand for tissue uptake . . . apoCII is ligand to activate Lipoprotein lipase for removal of fatty acids
Delivers endogenous TG and PL to cells . . .
Delivers CHOL to cells . . .

HDL really serves as a circulating resevoir for apoE and apoC’s for efficient removal of LDL’s and lipids from the blood
Note that HDL also picks up CHOL from tissues and returns it to the liver for bile synthesis (CHOL excretion pathway)
Function of these apoprotein ligands and the cellular receptors that recognize them have important implications for atherosclerosis

Please see the PowerPoint:
Dietary Prevention of Coronary Artery Disease & Cancer
for details on the etiology of Atherosclerosis