lifestyle and cvd risk reduction - amazon s3 and cvd risk ... the two mediterranean-diet groups had...
TRANSCRIPT

Lifestyle and CVD risk

Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be
reproduced, copied, stored, or transmitted in any form or by any
means – graphic, electronic, or mechanical, including
photocopying, recording, or information storage and retrieval
systems without prior written permission of Sea Courses Inc.
except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s
statements, materials, acts or omissions.
2017-09-08
1

Acknowledgments/Disclosures
Speaking:
HT Canada , Sea Courses, Université Laval et McGill
Consulting Insurance :
La Capitale , SSQ-Ass, SSQ-Vie et l’Union -Vie
Guidelines :
Diagnosis et CV risk stratification, Canadian Hypertension
Guidelines
Continuous Professional Development :
AAIM ,CCS
2

• The information presented is based on recent information that
is explicitly ‘‘evidence-based’’ and
is based on CCS and HT Canada Guidelines,2016- 2017
Mitigating Potential Bias
3

Lifestyle and CVD Risk
• recognise lifestyle as « primordial » CVD risk factors.
• distinguish « alleged and proven » links between lifestyle
and CVD
• support lifestyle modification in clinical practice as the Rx for
classical ( primary ) CVD risk factors.
After participating to this session,
the attendees will…
No potential conflicts of interest
G.T. – D.D. 2017 4

Are other risk factors equally or
more effective at predicting CVD
Olsen, et al. Current Vascular Pharmacology, 2010, 8, 134-139
Genetics
Age
Gender
Lifestyle
Social status
Physical
activity
Alcohol
Smoking
Waist/
hip-ratio
BMI
Metabolic
factors
Lipids
Glucose
Haemodynamic
factors
Blood pressure
Heart rate
Preclinical desease
Atherosclerosis
Endothelial
dysfunction
Vascular stiffness
LV hypertrophy
LV dysfunction
CV disease
MI
Stroke
CV death
X
G.T. – D.D. 2017 5

Overview
Risk FactorsSuccess story
Smoking
Stress management
Physical Exercise
Nutrition
G.T. – D.D. 2017 6

CHD Mortality Rates in Men < 65 Years Old
Finland
France
Hungary
Japan
United Kingdom
USA
Mortality from ischaemic heart disease, men 0-64 years. Source: WHO HFA database.G.T. – D.D. 2017 7

Contribution of Risk Factors to Burden of
Disease Mortality*
*Based on The World Health Report 2003. Yach et al. JAMA. 2004;291:2616-2622.
Percentage of Mortality Attributable to Risk Factors
G.T. – D.D. 2017 8

Lifestyles & Characteristics Associated
with Increased Risk of Future CHD events
• Age
• Sex
• Family history of
premature CHD or other
atherosclerotic disease
at early age
• (man <55 years)
• (woman <65 years)
• Personal history of CHD
or other atherosclerotic
disease
• Elevated blood pressure
• Elevated LDL-cholesterol
• Low HDL-cholesterol
• Elevated triglycerides
• Hyperglycaemia/Diabetes
• Obesity
• Thrombogenic factors
• Diet high in saturated fat,
cholesterol and calories
• Tobacco smoking
• Excess alcohol
consumption
• Low physical activity
• Physical inactivity
Lifestyles « Treatable/Disease » Non modifiable
G.T. – D.D. 2017 9

The Finnish experience
• Some facts: 1960
• High initial population CVD and hypertension rates
• Some of the key actions
• Some monitoring and surveillance
• Part of a pilot (North Karelia) and then national program to
reduce CVD
• Multi sector collaboration
• Regulation (warning labels)
• Strong armed voluntary reduction in salt
• Salt substitute (Pan salt)
• Major newspaper engagement
• Strong key opinion leaders
G.T. – D.D. 2017 10
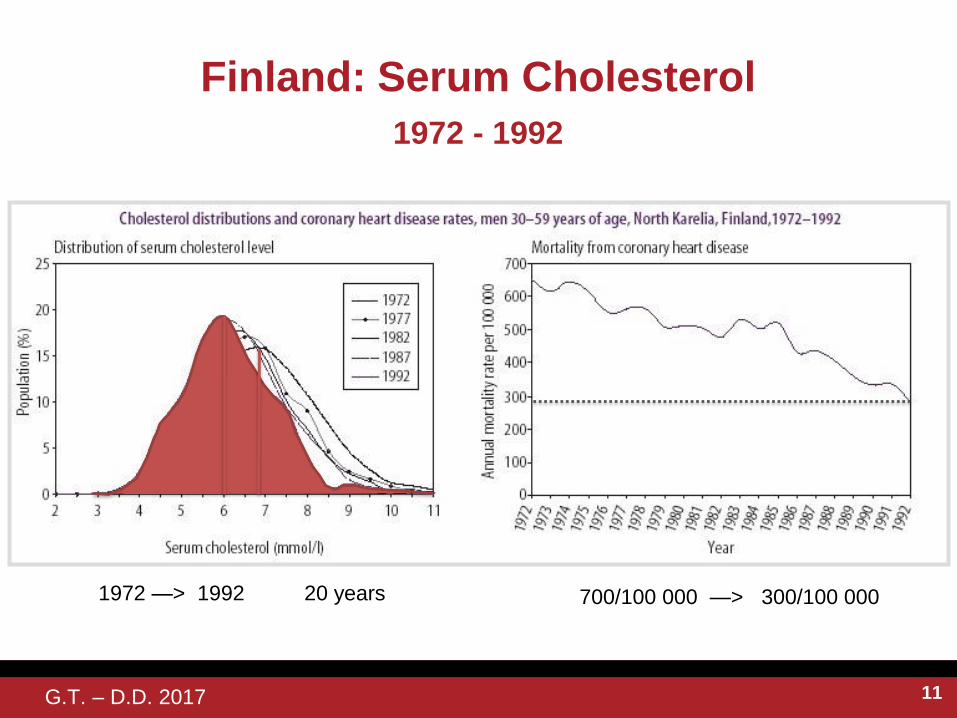
Finland: Serum Cholesterol
700/100 000 —> 300/100 000
1972 - 1992
1972 —> 1992 20 years
G.T. – D.D. 2017 11

Observed and predicted decline in mortality
from ischaemic heart disease in men aged 35-
64 in Finland
Vartiainen J et al. BMJ Vol 309 July 2, 1994
G.T. – D.D. 2017 12

Smoking
Quitting at any age is most beneficial
G.T. – D.D. 2017 13

Quitting at Any Age Increases Life Expectancy
Doll R et al. BMJ. 2004;328:1519–1527.
Quitting at a younger age is most beneficial
% Survival
From Age
40
Stopped Age
35-44
Non-smokers Cigarette Smokers
Years
72%
42%
- 30%
- 10 years(60y)
1
2
3
G.T. – D.D. 2017 14

Physicians and Smoking cessation counselling
Bupropion
Varenicline
Nicotine replacement Rx.
Express empathy, Offer Help
G.T. – D.D. 2017 15

Average number of cigarettes smoked per
day by household and workplace
Data source: 2003 Canadian Community Health Survey * Significantly higher than estimate for previous category(-
ies) (p < 0.05)
Men: - 39%
Women: - 37%
1916
1210
Average number of cigarettes smoked per
day by household and workplace smoking
restrictions and sex, employed daily
smokers aged 18 to 54, Canada excluding
territories, 2003.
G.T. – D.D. 2017 16

Year
Admissions, Acute MIHelena, Minnesota, (Scott County), USA
Sargent RP Shepard, Robert M, Glantz SA. Reduced incidence of admissions for myocardial
infarction associated with public smoking ban: before and after study. BMJ 2004;328:977-980
Admissions for acute myocardial infarction during 6 month periods, June-November 2002
before, during, and after the smoke-free ordinance. (Ordinance did not apply outside
Helena). The ordinance was implemented on June 5th, 2002 and then revoqued.
Helena
Outside Helena
1998 1999 2000 2001 2002 2003
60
50
40
20
10
0
30
G.T. – D.D. 2017 17

Risk Factor
Stress / Physical Exercise
G.T. – D.D. 2017 18

G.T. – D.D. 2017 19

Longevity and # heart beats
Adapted. Levine H.j » JACC 1997 ; 30 : 1104-6 GT, jan 2008
(10,000,000,000) 86 000 / day
G.T. – D.D. 2017 20
Longevity and # heart beats
G.T. – D.D. 2017 21

Physical Exercise
Meta-analysis: dose-response relation between physical activity and risk of coronary heart disease. The thick blue line
represents a fitted curve and the thin blue lines the confidence intervals. (From Sattelmair J, Pertman J, Ding EL, et al:
Doseresponsebetweenphysicalactivityandriskofcoronaryheartdisease:Ameta-analysis.Circulation124:789,2011.)
G.T. – D.D. 2017 22

Risk Factor
Nutrition
G.T. – D.D. 2017 23

Risk Factor
CHOLESTEROL
G.T. – D.D. 2017 24

« Normal » cholesterol
3.9
2.6
1.3
Physiologic LDL-C
from receptor studies
: .66
Humans, NA
Average Adults
New borns
LDL.
C
Rat
Guinea Pig
Sheep
Cow
CamelRabbit
Pig
25

Change of Diet Pattern
Traditional Low fat
G.T. – D.D. 2017 26

Osmo Turpeinen, et al. Journal of Epidemiology Vol 8. No 2; 1979.
Dietary Prevention of CHDFinnish mental hospital (1959-1971)
Serum Cholesterol over a period of 10 years
Practically total replacement of dairy fats by vegetable oils
in the diets of these two hospitals
G.T. – D.D. 2017 27
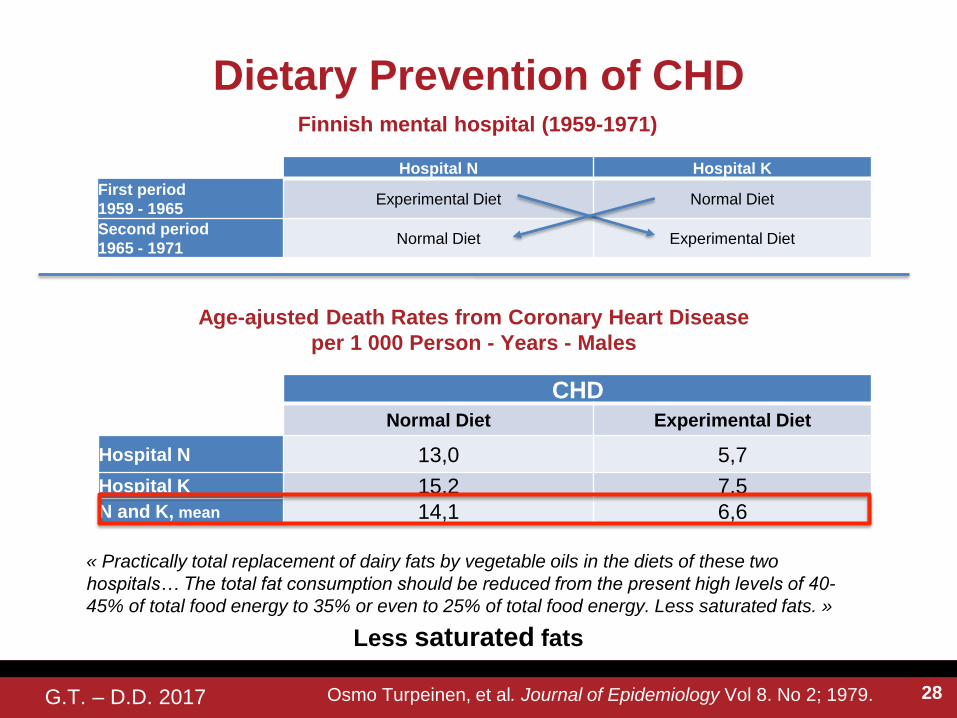
Osmo Turpeinen, et al. Journal of Epidemiology Vol 8. No 2; 1979.
Dietary Prevention of CHDFinnish mental hospital (1959-1971)
« Practically total replacement of dairy fats by vegetable oils in the diets of these two
hospitals… The total fat consumption should be reduced from the present high levels of 40-
45% of total food energy to 35% or even to 25% of total food energy. Less saturated fats. »
Hospital N Hospital K
First period
1959 - 1965Experimental Diet Normal Diet
Second period
1965 - 1971Normal Diet Experimental Diet
CHD
Normal Diet Experimental Diet
Hospital N 13,0 5,7
Hospital K 15,2 7,5N and K, mean 14,1 6,6
Age-ajusted Death Rates from Coronary Heart Disease
per 1 000 Person - Years - Males
Less saturated fats
G.T. – D.D. 2017 28

Mediterranean Diet Dietary Patten
http://www.mdpi.com/1422-0067/15/7/11678/htm
G.T. – D.D. 2017 29

Mediterrean Diet (Post MI)
de Lorgeril et al. (Circulation. 1999;99:779-785
Cumulative survival without nonfatal infarction, without major secondary
end points, and without minor secondary end points.
Lyon Heart Study
G.T. – D.D. 2017 30

Lyon Heart Study
15
10
5
0
Event
Rate
(%)
Death Cardiac
Mortality
Non Fatal
MI
Cancer
de Lorgeril et al. (Circulation. 1998;158 :1161; Circulation 1999;99 .
-56%
p=.03
-65%
p=.01
-70%
p=.01-61%
p=.05
Control diet
Mediterranean diet
24
19
25
17
6
14
8 7
G.T. – D.D. 2017 31
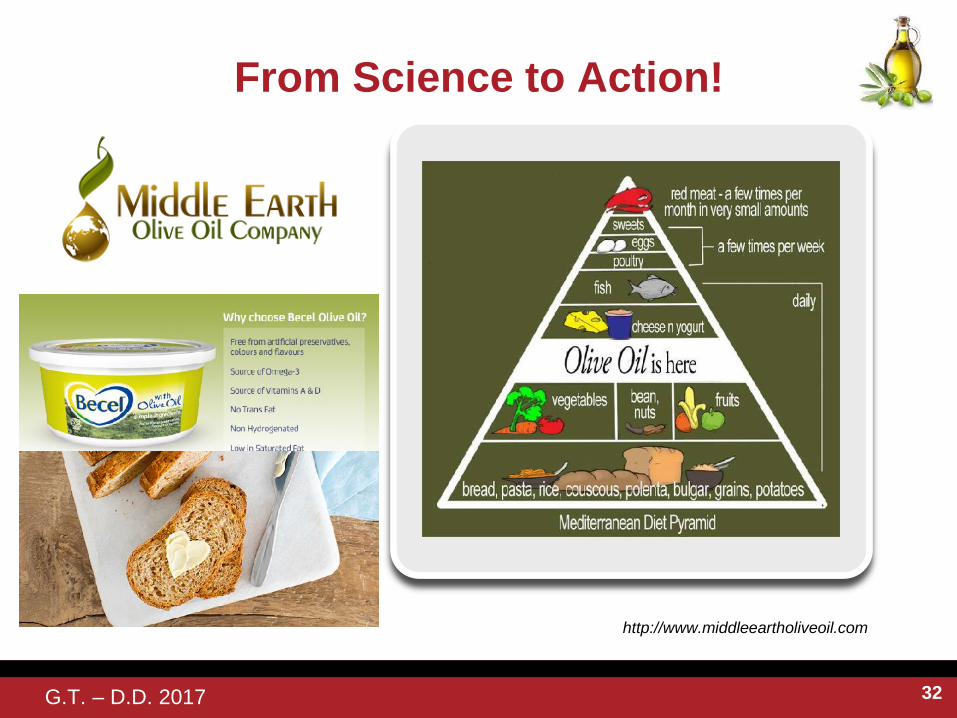
From Science to Action!
http://www.middleeartholiveoil.com
G.T. – D.D. 2017 32

Primary Prevention of CV Disease with a
Mediterranean Diet
Estruch et al. N ENGL J MED 368;14 NEJM.ORG APRIL 4, 2013
PREMIMED Study
A total of 7447 persons were enrolled (age range, 55 to 80 years); 57% were women.
The two Mediterranean-diet groups had good adherence to the intervention, according to self-
reported intake and biomarker analyses.
… free provision of extra-virgin olive
oil, mixed nuts, or small nonfood gifts.
G.T. – D.D. 2017 33

Mediterranean dietRecommended Goal
Olive oil * ≥4 tbsp/day
Tree nuts and peanuts ≥3 servings/wk
Fresh fruits ≥3 servings/day
Vegetables ≥2 servings/day
Fish (especially fatty fish), seafood ≥3 servings/wk
Legumes ≥3 servings/wk
Sofrito‡ ≥2 servings/wk
White meat Instead of red meat
Wine with meals (optionally, only for habitual drinkers) ≥7 glasses/wk
Discouraged Goal
Soda drinks <1 drink/day
Commercial bakery goods, sweets, and pastries <3 servings/wk
Spread fats <1 serving/day
Red and processed meats <1 serving/day
Low-fat diet (control)Recommended Goal
Low-fat dairy products ≥3 servings/day
Bread, potatoes, pasta, rice ≥3 servings/day
Fresh fruits ≥3 servings/day
Vegetables ≥2 servings/day
Lean fish and seafood ≥3 servings/wk
DiscouragedVegetable oils (including olive oil) ≤2 tbsp/day
Commercial bakery goods, sweets, and pastries ≤1 serving/wk
Nuts and fried snacks ≤1 serving /wk
Red and processed fatty meats ≤1 serving/wk
Visible fat in meats and soups. Always remove
Fatty fish, seafood canned in oil ≤1 serving/wk
Spread fats ≤1 serving/wk
Sofrito ≤2 servings/wk * Extra Virgin Olive Oil: EVOO
Estruch et al. N ENGL J MED 368;14 NEJM.ORG APRIL 4, 2013G.T. – D.D. 2017 34

Primary Prevention of CV Disease with a
Mediterranean Diet
N ENGL J MED 368;14 NEJM.ORG APRIL 4, 2013
EVOO: Extra Virgin Olive Oil
G.T. – D.D. 2017 35

Primary Prevention of Metabolic syndrome
with a Mediterranean Diet
Arch Intern Med. 2008;168(22):2449-2458
MetS: Metabolic Syndrome
MetS Reversion
MetS Incidence
G.T. – D.D. 2017 36

Cumulative diabetes free-survival
Salas-Salvadó J. et al. Reduction in the Incidence of Type 2 Diabetes With the Mediterranean Diet. Diab Care, volume 34, 14-19 2011
MedDiet
+
MedDiet
+
Traditional
G.T. – D.D. 2017 37

Incidence of diabetes or cardiovascular
end point, %
Salas-Salvadó J. et al. Reduction in the Incidence of Type 2 Diabetes With the Mediterranean Diet. Diab Care, volume 34, 14-19 2011
Traditional
G.T. – D.D. 2017 38

Primary Prevention of CV Disease
with a Mediterranean Diet
Pharmacological Research 65 (2012) 577-583
LFD: Low Fat Diet; Med-Diet : with Olive oil; Med Diet with Nuts
G.T. – D.D. 2017 39

Primary Care
Applicability
G.T. – D.D. 2017 40
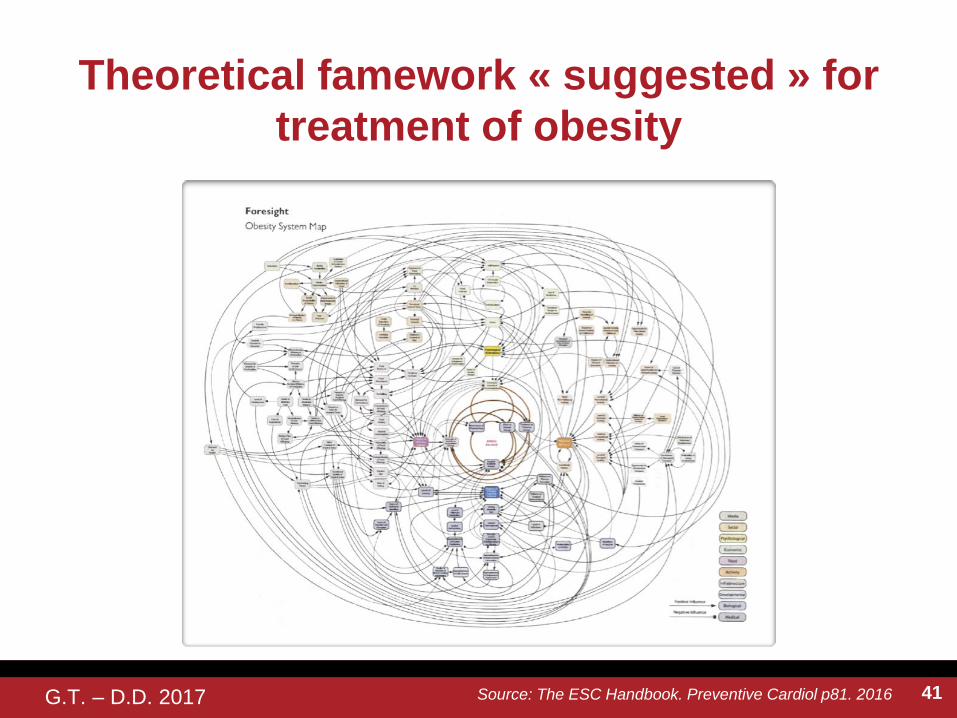
Theoretical famework « suggested » for
treatment of obesity
Source: The ESC Handbook. Preventive Cardiol p81. 2016G.T. – D.D. 2017 41

G.T. – D.D. 2017
From Yarnall and Coll 2009. Cited in Profession Santé, Janvier 2015, Volume 1, No. 1
Time required for the practitioner to fully
implement practice guidelines developed by
learned societies
Acute
care
Chronic
care
Preventive
care
3,7 h 3 h 1,3 h
On average, a family physician spends
3,7 h 10,6 h 7,4 h
21,7 hours / day
If he had to follow all clinical practice guidelines, he would spend
8 hours
21,7 hours
Acute
care
Chronic
care
Preventive
care
42

Change4LIFE Initiative in the United Kingdom
G.T. – D.D. 2017 43

• A prospective single centered randomized controlled trial.
• New guidelines for secondary prevention in coronary artery
disease were distributed by mail and presented at a common
lecture for all general practitioners and specialists in 1995
• Two primary health care clusters were matched and
randomised to Intervention (I) or Control (C)
Pr Gunilla Hedlin ,Center for Allergy Research
Study desing
44

Trial profile
45

Secondary preventive local guidelines for
patients with CHD in 1995 ,Target goals :
• Total cholesterol < 5.0 mmol
• LDL-cholesterol < 3.5 mmol/l
• HDL-cholesterol > 1.0 mmol/l
• F-Triglycerids <2.3 mmol/l
• Stop smoking
• Diastolic blood pressure <95 mmHg)
• Blood sugar control
• Improved Quality of life by healthy food intake, weight reduction,
increased physical activity and stress reduction
24 % smokers
Tot chol 6,4 + 1,1
LDL-chol 4,2 + 1,0
46

• 44 % of the included patient in the control group had deceased
after ten years as compared to 22 % in the intervention group
(p= 0.0173; log rank test).
• Patients treated by a specialist deceased at a rate comparable
to the intervention group (23%).
Result after ten years
47

The CHAMP Initiative
The UCLA Medical
Center’s Cardiac
Hospitalization
Atherosclerosis
Management Program
(CHAMP) increases
guideline intervention and
reduced recurrent and
myocardial infarction.
Fonarow GC et al. Am J Cardiol 2001;87:819-822.
Guideline Intervention Use%
Post-CHAMP(1 year)
Beta-blocker
ACE Inhibitor
Aspirin
Statin
100
80
60
40
20
0Pre-CHAMP
92%
86%
61%
56%
78%
12%
6%
4%
64%
58%
CCB
G.T. – D.D. 2017 48

CHAMP study: Death or recurrent MI
Fonarow GC et al. Am J Cardiol 2001;87:819-822.
The UCLA Medical
Center’s Cardiac
Hospitalization
Atherosclerosis
Management Program
(CHAMP) increases
guideline intervention
and reduced recurrent
and myocardial
infarction.
14.8%
6.4%
0
5
10
15
20
Pre-CHAMP Post-CHAMP
%
G.T. – D.D. 2017 49

Lifestyle and CVD Risk
• recognise lifestyle as « primordial » CVD risk factors.
• distinguish « alleged and proven « links between lifestyle and
CVD
• support lifestyle modification in clinical practice as the Rx for
classical CVD risk factors ..
After participating to this session, the attendees will…
G.T. – D.D. 2017 50

Lifestyle and CVD risk
51