life threatening asthma - some pearls and pitfalls
TRANSCRIPT

Life Threatening Asthma
– Pearls and Pitfalls
Dr. Chew Keng Sheng, MD, MMED Universiti Sains Malaysia

Contents
1. Pathophysiology: “Baby lung” concept 2. Two different phenotypes of severe asthma 3. 3Mg Trial: Does The Use of MgSO4 Really
Translate Into Clinical Benefits? 4. Management of severe exacerbations 5. Role of NIV and mechanical ventilation -
indications and strategies

Pathophysiology
• Inhomogenous obstruction • A = normal • B = mucus plugging – total
obstruction • C = severe partial
obstruction ! incomplete expiration ! auto-PEEP
• D = lesser partial obstruction throughout breathing cycle
Oddo et al, 2006

Pathophysiology
• Most tidal volume will be preferentially delivered to the healthy compartment, mainly A thus risking over-distending segment A
Oddo et al, 2006
“BABY LUNG CONCEPT”
Crucial objective of management of severe asthma is
TO PREVENT FURTHER LUNG HYPERINFLATION
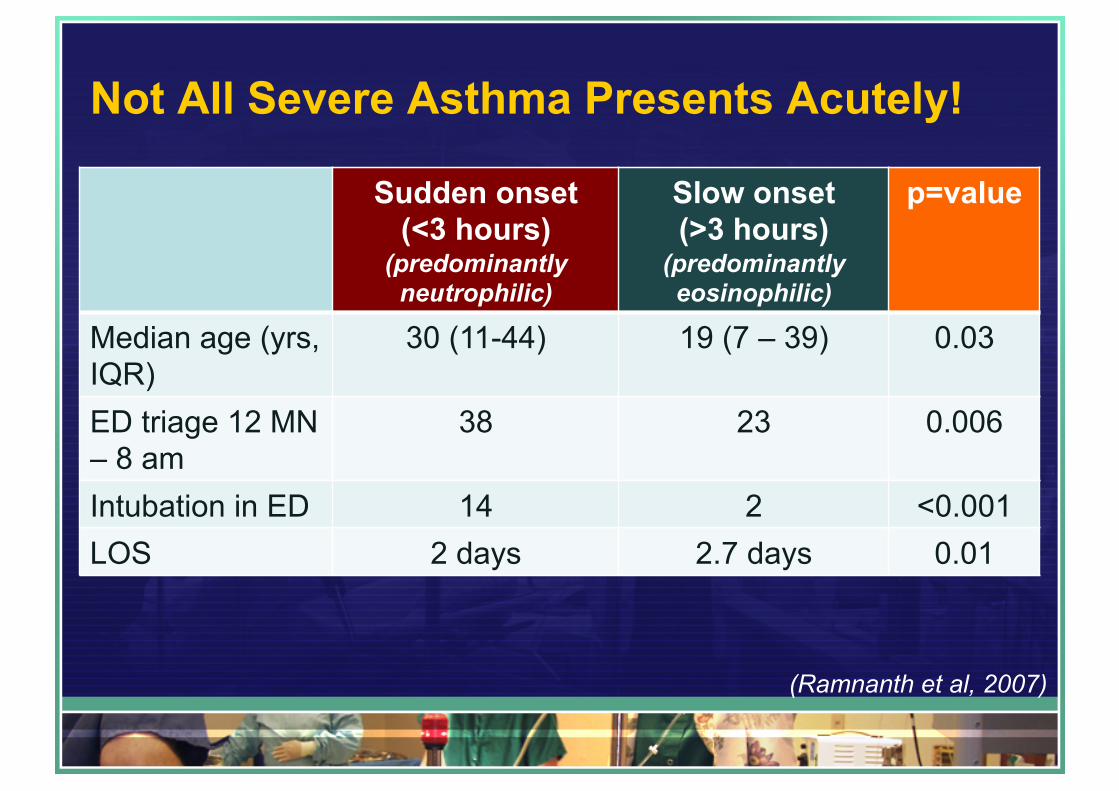
Not All Severe Asthma Presents Acutely!
Sudden onset (<3 hours)
(predominantly neutrophilic)
Slow onset (>3 hours)
(predominantly eosinophilic)
p=value
Median age (yrs, IQR)
30 (11-44) 19 (7 – 39) 0.03
ED triage 12 MN – 8 am
38 23 0.006
Intubation in ED 14 2 <0.001 LOS 2 days 2.7 days 0.01
(Ramnanth et al, 2007)

Risk Factors Associated With Life Threatening Asthma
OR (95% CI) P=value History of mechanical ventilation
6.69 (2.80 – 15.97) 0.0001
Increased use of nebulizers 2.45 (1.52 – 3.93) 0.0002 History of ICU admission 5.14 (1.91 – 13.86) 0.001 Increased use of steroids 2.71 (1.34 – 5.51) 0.006 History of hospital admission 2.62 (1.04 – 6.58) 0.04 Increased use of short acting B2-agonists
1.67 (0.99 – 2.84) 0.057
Prior ED visit 1.13 (0.43 – 2.92) 0.810 (Alvarez et al 2005)

Management of Severe Exacerbations
• SABA – continuous neb vs intermittent neb; – MDI 4 – 8 puffs q10 as alternative – No evidence to support IV salbutamol
• Steroids – give early; 4 – 6 hours onset • Anti-cholinergics – synergistic effects; slower onset,
longer effect • IV Ketamine – dissociative anesthesia,
bronchodilatory effects
(Murata et al 2012; Restrepo & Peters, 2008)

3Mg Trial: Does The Use of MgSO4 really translate into Clinical Benefits? • A randomized controlled
trial of IV MgSO4 vs Neb MgSO4 vs placebo in adults with acute severe asthma
• 190 pages report! • Full text available at:
http://tinyurl.com/q9cx9va
Background
• Magnesium sulphate in asthma : 1. Smooth muscle relaxation 2. Blocks calcium channel 3. Anti-inflammatory action
Is MgSO4 a magic bullet?

What’s the evidence so far prior to 3Mg Trial? IV MgSO4 • 5 meta-analyses: 1. Rowe et al (2000) – 5 adults; 2 pediatrics trials; no
improvement; only effective in severe asthma 2. Alter et al (2000) – 7 adults; 2 pediatrics;
spirometric improvement 3. Rodrigo et al (2000) – 5 adults; no improvement 4. Cheuk et al (2005) – 5 pediatrics; improvement in
lung function, hosp adm & clinical symptoms

What’s the evidence so far prior to 3Mg Trial? 5 Mohammed & Goodacre (2007) (24 trials) " IV MgSO4: 10 adults, 5 pediatric trials " Neb MgSO4: 7 adults, 2 pediatric trials " IV MgSO4: significant improvement in pulmonary
function but no improvement in hosp adm " Neb MgSO4: maybe some weak benefit in hospital
adm rate (RR 0.68, 95% CI 0.46 to 1.02; p = 0.06), otherwise no significant effect

What’s the evidence so far prior to 3Mg Trial? Neb MgSO4 • 3 meta-analyses: 1. Mohammed & Goodacre (2007) (9 trials on neb): as
mentioned 2. Blitz et al (2005): (3 adults, 2 pediatrics, 1 mixed);
significant improvement in pulmonary function, but not hosp adm
3. Villeneuve & Zed (2005): 6 trials, no improvement in lung function

3Mg Trial
• Research Questions: • Does the changes in pulmonary function translate
into changes in patient management and a clinically meaningful symptoms improvement
Arm IV Neb 1 IV MgSO4 2 g in 100 ml over
20 min Neb saline q20 min * 3
2 IV saline 100 ml over 20 min Neb MgSO4 q20 min *3 3 IV saline 100 ml over 20 min Neb saline q20 min * 3

3Mg Trial
• P = Adults (> 16 years) in ED with acute severe asthma (defined as PEFR < 50% of best or predicted, respiratory rate > 25 breaths per minute, heart rate > 110 beats per minute or inability to complete sentences in one breath)
• I = IV MgSO4, Neb MgSO4 • C = Placebo • O = 1) Hospital adm after ED Rx to next 1/52 • = 2) subjective changes in VAS for SOB

3Mg Trial
• N = 1084 patients, 34 hospitals in UK • Hospital admission after ED Rx or next 1/52
– 285/394 (72%) in IV – 261/332 (79%) in Neb – 281/358 (78%) in placebo – Active Rx vs placebo OR 0.84, 95% CI: 0.61 – 1.15, p =
0.276 – IV vs neb OR 0.76, 95% CI: 0.53 – 1.10, p = 0.146 – IV vs placebo OR 0.73, 95% CI: 0.51-1.04, p = 0.083 – Neb vs placebo OR 0.96, 95% CI: 0.65 – 1.40, p = 0.819

3Mg Trial
• Mean (SD) change from baseline to 2 hours – 34.3 mm (SD +/- 27.7 mm) in IV – 28.2 mm (SD +/- 27.4 mm) in neb – 31.3 mm (SD +/- 29.4 mm) in placebo
• Mean differences in improvement in VAS: – Active Rx vs placebo = 0 (95% CI –3.7 to 3.7; p = 0.999) – IV vs neb = 5.1 mm (95% CI 0.8 to 9.4 mm; p = 0.019) – IV vs placebo = 2.6 mm (95% CI –1.6 to 6.8 mm; p =
0.231) – Neb vs placebo = – 2.6mm (95% CI –7.0 to 1.8, p =
0.253)*

Conclusion
• 3Mg Trial was unable to demonstrate a clinically worthwhile benefit from magnesium sulphate in acute severe asthma although there was some weak evidence of an effect of IV MgSO4 on hospital admission.

Caveats In Interpreting 3Mg Trial Results
• 3Mg Trial included adult patients with severe asthma defined as: – PEFR<50% of best/predicted – Inability to complete sentences in one breath
• However, 3Mg Trial excluded patients with: – patients with life-threatening features, defined as one or
more of: SaO2< 92% despite O2 Rx; silent chest; cyanosis; poor respiratory effort; bradycardia; arrhythmia; hypotension; exhaustion; coma; or confusion
– patients who had received IV or neb MgSO4 in the last 24 hours prior to ED visit

Non-Invasive Ventilation
• Reduce the patient’s respiratory effort • Start low: IPAP: EPA 7/3, increase pressure
support 2 cmH2O q15 min • Make sure patient cooperative, good ventilatory
effort • Strong evidence for NIV? Not really • Cochrane review by Lim et al (2012):
– Primary outcome intubation rate: 2/45 participants on NIV and 0/41 control patients (RR 4.48; 95% CI 0.23 to 89.13). No deaths in either of these studies.

Warning Signs Patients Need Mechanical Ventilation • No evidence to support a specific pH or PCO2 for
intubation – Decision should be made on clinical grounds
• Exhaustion • Decreasing level of consciousness • Inability to maintain oxygenation using mask
Best strategy: Avoid mechanical ventilation if possible but not unnecessary delay.
(Hodder et al, 2010)

Ventilation Strategy (Weingatt S. 2010): “Let pt have adequate time to breathe out”
Vt (Lung
protection)
IFR (Patient’s comfort)
RR* (Ventilation)
FiO2/ PEEP
(Oxygenation)
6 – 8 ml/kg IBW Keep Pplat <30 cm H20
80 – 100 lpm IBW
FiO2 1.0 ! 0.4 (SaO2 ~ 95%)
PEEP = 0
8 - 10 bpm; keep I:E = 1:4 Allow permissive hypercapnia
Vol AC
(http://emcrit.org/podcasts/vent-part-2/)

References
• Wills CP, Young M, White DW. Pitfalls in the evaluation of shortness of breath. Emerg Med Clin North Am 2010;28(1):163-81
• Ramnath VR, Clark S, Camargo CA, Jr. Multicenter study of clinical features of sudden-onset versus slower-onset asthma exacerbations requiring hospitalization. Respir Care 2007;52(8):1013-20.
• Restrepo RD, Peters J. Near-fatal asthma: recognition and management. Curr Opin Pulm Med 2008;14(1):13-23.

References
• Goodacre S, Cohen J, Bradburn M, et al. The 3Mg trial: a randomised controlled trial of intravenous or nebulised magnesium sulphate versus placebo in adults with acute severe asthma. Health Technol Assess 2014;18(22):1-168.
• Murata A, Ling PM. Asthma diagnosis and management. Emerg Med Clin North Am 2012;30(2):203-22, vii.

References
• Mohammed S, Goodacre S. Intravenous and nebulised magnesium sulphate for acute asthma: systematic review and meta-analysis. Emerg Med J 2007;24(12):823-30.
• Alvarez GG, Schulzer M, Jung D, et al. A systematic review of risk factors associated with near-fatal and fatal asthma. Can Respir J 2005;12(5):265-70.

References
• Oddo M, Feihl F, Schaller MD, et al. Management of mechanical ventilation in acute severe asthma: practical aspects. Intensive Care Med 2006;32(4):501-10.
• Lim WJ, Mohammed Akram R, Carson KV, et al. Non-invasive positive pressure ventilation for treatment of respiratory failure due to severe acute exacerbations of asthma. Cochrane Database Syst Rev 2012;12:CD004360.

References
• Hodder R, Lougheed MD, FitzGerald JM, et al. Management of acute asthma in adults in the emergency department: assisted ventilation. CMAJ 2010;182(3):265-72.
www.PresentationPro.com