levels of 5-hydroxyindoleacetic acid, gamma-aminobutyric acid...
TRANSCRIPT
Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
695
LEVELS OF 5-HYDROXYINDOLEACETIC ACID, GAMMA-AMINOBUTYRIC ACID AND
NITRIC OXIDE METABOLITES IN CEREBROSPINAL FLUID OF EGYPTIAN
WOMEN SUFFERING OF FIBROMYALGIA SAHAR AHMAD SAAD, MANAL A. M. MANDOUR * AND HASSAN KOTB **
Rheumatology & Rehabilitation, Biochemistry* Departments and Pain Unit** Assiut University Faculty of Medicine and Assiut
University Hospitals** KEY WORDS: CEREBROSPINAL FLUID IN FIBROMYALGIA, 5-HYDROXYINDOL-ACETIC ACID, GAMMA AMINOBUTYRIC ACID, NITRIC OXIDE METABOLISM.
ABSTRACT Hypothesis: Fibromyalgia (FM) is a complex chronic
disorder predominately affects women. The lack of objective analytical image for diagnosis and prognosis of FM attract many investigators to evaluate the neuroendocrine changes in body fluids that may be related to the pathophysiology of FM.
Objectives & Methodology: To compare the levels of 5-hydroxyindoleacetic acid (5-HIAA, serotonin metabolite), gamma-aminobutyric acid (GABA) and nitric oxide (NO) metabolites in cerebrospinal fluid (CSF) of normoglycemic women suffering of FM with those of control group. In addition, levels of insulin, insulin like growth factor-1 (IGF-1), cortisol, 5-hydroxytryptamine (5-HT, serotonin), GABA, and NO metabolites were determined in serum of FM patients compared to control group. Moreover, the correlations between all the studied parameters were performed.
Results: The present study showed altered serum levels of insulin and cortisol in normoglycemic women suffering of FM (n=15) compared to those of control group (n=15). However, the data did not find significant differences between serum levels of IGF-1 in women suffering of FM and those in healthy women. Cortisol levels in FM sera were inversely correlated with the number of tender points (r=-0.76, p<0.001). Also, negative

CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
696
correlation was observed between serum IGF-1 levels and age of FM patients (r=-0.63, p< 0.05). Low levels of serum 5-HT and CSF 5-HIAA were also noticed among women suffering of FM. A decrement of both serum and CSF levels of GABA in those patients compared to controls was detected. Furthermore, there was a positive correlation between serum GABA levels and serum cortisol levels (r=0.61, p< 0.05), and between CSF GABA and 5-HT (r=0.56, p< 0.05). However, CSF GABA levels were negatively correlated with age of women suffering of FM. These findings may clarify the significant role of GABA in the pathogenesis of FM. A higher serum and CSF levels of NO metabolites were detected in FM patients than in control group. In addition, serum levels of NO metabolites were correlated with those levels in CSF (r=0.63, p< 0.05). The involvement of NO in pain process was revealed by a strong correlation between serum and CSF levels of NO metabolites with the number of tender points (r=0.91, p< 0.001; r=0.73, p< 0.01 respectively). Also, by a negative correlation between serum levels of NO metabolites and serum cortisol levels (r=0.70, p< 0.01) in FM patients.
Conclusions: The changes in the levels of studied hormones and neurotransmitters in women suffering of FM support the hypothesis of neuroendocrine involvement in FM pathogenesis. The current study suggested that GABA and NO may play a role in modulating FM. Alterations of their levels in serum and CSF of women suffering of FM and their correlations with age, number of tender points and/ or cortisol may confirm this suggestion. Accordingly, this investigation recommended the examination of GABAergic agents, NO synthase (NOS) inhibitors, or antioxidants for therapy of various symptoms in women suffering of FM. Furthermore, our study may find utility of these neurotransmitters as possible markers of FM, but this study warrant more investigations to confirm these findings.
INTRODUCTION Fibromyalgia (FM) is a complex chronic disorder characterized by
symptoms of diffuse pain, unrefreshing sleep, fatigue, emotional distress, and irritable bowel syndrome (Wolfe et al., 1990). The disorder
Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
697
predominately affects middle-aged women. FM is now recognized and diagnosed frequently among females with somatic pain (Wolfe et al., 1995).
The etiology of FM is unknown, although several lines of evidence support the involvement of disturbed serotonin (5-HT) metabolism along with disturbances in several other chemical pain modulators (Russell et al., 1992 and Alnigenis & Barland, 2001). Moreover, there is alteration of neuroendocrine functioning include altered hypothalamic-pituitary-adrenal axis (HPA) activity with hypocortisolism (Riedel et al., 1998, Torpy et al., 2000 and Fries et al., 2005). Other neuroendocrine axes, such as the growth and thyroid axes are perturbed in FM, as evidenced by low levels of insulin-like growth factor 1 (IGF-1) (Bennett et al., 1997). Neeck (2000) revealed that neuroendocrine and hormonal perturbations may be related to the serotonergic system in FM.
Determination of gamma-aminobutyric acid (GABA) concentration in human cerebrospinal fluid (CSF) can be used to assess GABAergic activity in the central nervous system (CNS) (Schechter & Sjoerdsma, 1990). Most of the data from direct and indirect studies are consistent with GABA involvement in mood disorders and depressive illness and showed low CSF GABA levels in these states (Petty 1995, Tunnicliff & Malatynska, 2003 and Kalia, 2005). Recently, GABA analogue and GABA agonist were examined for treatment of CNS disorders including FM, and has been found to be effective in raising the pain threshold and improving other related symptoms (Dixit & Bhargava 2002 and Grofford et al., 2005).
Nitric oxide (NO) metabolites in CSF could be useful prognostic markers in neurological diseases and may facilitate understanding the involvement of NO in these diseases (Bratasz et al., 2004 and Wang et al., 2005). NO may be pro- or antinociceptive molecule depending on its concentration and sites of action (Durate et al., 1992, Meller et al., 1992 and Christopherson & Bredt, 1997). The involvement of NO in pain process in FM was previously documented (Larson et al., 2000, Pall 2001and Sackner et al., 2004). FM patients show abnormalities in allodynia (heightened pain sensitivity) that could result from aberrant CNS perception of normal stimuli (Central sensitization) (Woolf, 1983, Coderre et al., 1993 and Bradely et al., 2000). Central sensitization appears to depend on activation of N-methyl D-aspartate (NMDA) receptors (Woolf & Thompson, 1991). Activation of excitatory receptors as NMDA receptors (Coderre & Melzack, 1992) and substance P (Radhakrishnan et al., 1995) increases intracellular calcium and activates NO synthase (NOS) (Garthwaite et al., 1988 and Garthwaite & Boulton, 1995).
CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
698
The diagnosis of FM is based exclusively on subject data because of the lack of objective analytical image or pathological data (Andreu & Sanz, 2005). On the other hand, understanding specific etiological factors and mechanisms involved in individual patients will allow clinicians to determine treatments that are most effective for a given patients. Therefore, the current study aimed to estimate the levels of insulin, IGF-1, cortisol, 5-HT, GABA and NO metabolites in serum of women suffering of FM. In addition, levels of 5-hydroxyindoleacetic acid (5-HIAA; metabolite of 5-HT), GABA, and NO metabolites were determined in CSF of those patients in a trial to elucidate their roles and relations with clinical signs of FM.
SUBJECTS AND METHODS Subjects:
Fifteen normoglycemic patients all of them females their ages range between 23 and 55 years old (mean ± SD, 37.4 ± 8.5) diagnosed as primary fibromyalgia according to the American College of Rheumatology (ACR) criteria (Wolfe et al., 1990). Laboratory investigations were done in form of level of blood sugar, ESR, CRP, complete blood picture. Rheumatoid factor and antinuclear antibodies to exclude any other diseases interfere with the study. Fifteen control subjects all of them females without fibromyalgia they were matched in age with the patients’ group. All subjects agreed to donate CSF obtained by lumbar puncture and blood sample. None of the patients or healthy control subjects was on psychotropic drugs. After giving informed consent using a document approved by the local ethics committee, all subjects agreed to donate CSF obtained by lumbar puncture. Primary fibromyalgia patients who were on analgesics were discontinued 48 hours prior to lumbar puncture.
Serum and CSF collection: The samples were collected between 09:00 and 11:00 h after overnight fast. None of the CSF samples were blood stained. The serum and CSF samples were divided into aliquots, frozen at – 70 °C until thawed for analysis. Determination of 5-HT and 5 –HIAA:
Because of the low levels of 5-HT in normal CSF samples, determination of its metabolite 5-HIAA levels were performed. 5-HT and 5-HIAA levels were determined fluorimetrically according to Curzon & Green (1970) with minor modification (Jonsson & Lewander, 1970). Briefly, 2ml of sample were treated with 3ml acidified butanol. After centrifugation for 5 min. at 3,000 rev/min., 2.5ml of the supernatant were

Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
699
pipette into 25 mL glass stoppered tube and shaken for 5 min. with 5 ml n-heptane and 0.4 ml 0.1N HCL containing 0.1% cysteine. The aqueous phase was used for determination of 5-HT and the organic phase retained for the 5-HIAA determination. For 5-HT determination 0.004% O-phthalaldehyde (in 10N HCL) was used. For 5-HIAA determination, organic phase was added to 0.5M phosphate buffer (pH 7), centrifuged for 3 min. at 3.000 rev/min. and divided into two portions (one for test and other for blank). 1% cysteine, 0.1% O- phthalaldehyde (in methanol), conc. HCL, and 0.02% sodium periodate was used. Activation and fluorescent wavelengths were 360 nm and 470 nm respectively.
Determination of GABA levels: GABA levels were estimated in serum and CSF samples by
fluorimetric method with minor modification (Uchida & Brien, 1964). An equal volume of 10% trichloracetic acid was added to sample, centrifuged, and the supernatant was pipette in 10 ml test tube, 0.05M glutamic acid in 0.2M phosphate buffer (pH 6.4) and ninhydrin solution were added. The tubes were kept at 60° for 30 min and then cooled and copper tart rate reagent was added. Activation and fluorescent wavelengths were 380 nm and 450 nm respectively. Determination of NO metabolites:
This assessed by using Griess reagent (1% sulfanilamide, 0.1% naphthylethylene diamine diHCL, and 2.3% orthophosphoric acid) according to method of Ding et al. (1988). Determination of insulin, IGF-1, and cortisol:
Insulin levels were estimated in FM sera using a solid phase enzyme amplified sensitivity immunoassay (MEDGENIX-INS-EASI) kit (Frier et al., 1981). IGF-1 levels were determined using enzyme linked immunosorbent assay (ELISA) kit (Blum et al., 1993). Also, cortisol levels were estimated using ELISA kit (Tijssen, 1985). Statistical analysis:
Prism software program, graph Pad version 3.0 was used for all analyses. Clinical data was expressed as mean ±SE or numbers (percentages). Data of hormones and neurotransmitters was expressed as mean + SE and quartiles [median (25th, 75th percentile)] because of the wide range of their levels. Hormone and neurotransmitter concentrations for women suffering of FM were compared with those in the control group by unpaired 2-tailed t-test. For nonparametric comparisons, Mann-Whitney test

CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
700
was performed because of non-normal distribution of hormones and neurotransmitters. Spearman’s rank correlation coefficient was used for evaluating the correlation between age, number of tender points, hormones, and neurotransmitters. P< 0.05 was considered a significant difference.
RESULTS Clinical characteristics of women suffering of FM were
demonstrated in table 1. The present data showed altered serum levels of some hormones in normoglycemic women suffering of FM (table 2). This is revealed by reduced levels of cortisol (p<0.05) and elevated levels of insulin (p<0.01) in FM sera. The data did not find significant differences between serum levels of IGF-1 in women suffering of FM and those in healthy women. Table (1): Clinical characteristics of women suffering of FM. Variables
Age (years) 37.4 + 2.19
Number of tender points 13.27 + 0.35 Pain 15 (100%) Morning stiffness 11 (73.3%) Fatigue 14 (93.3%) Sleep disturbance 5 (33.3%) Paresthesias 3 (20%) Headache 6 (40%) Psychiatric syndrome& depression 6 (40%) Irritable bowel 4 (26.7%) Data are expressed as mean ±SE or number (percentage).
In addition, cortisol levels in FM sera were inversely correlated with number of tender points (r= -0.76, p<0.001). Negative correlation (r= -0.63, p<0.05) was also observed between IGF-1 levels and age of FM (table 4).
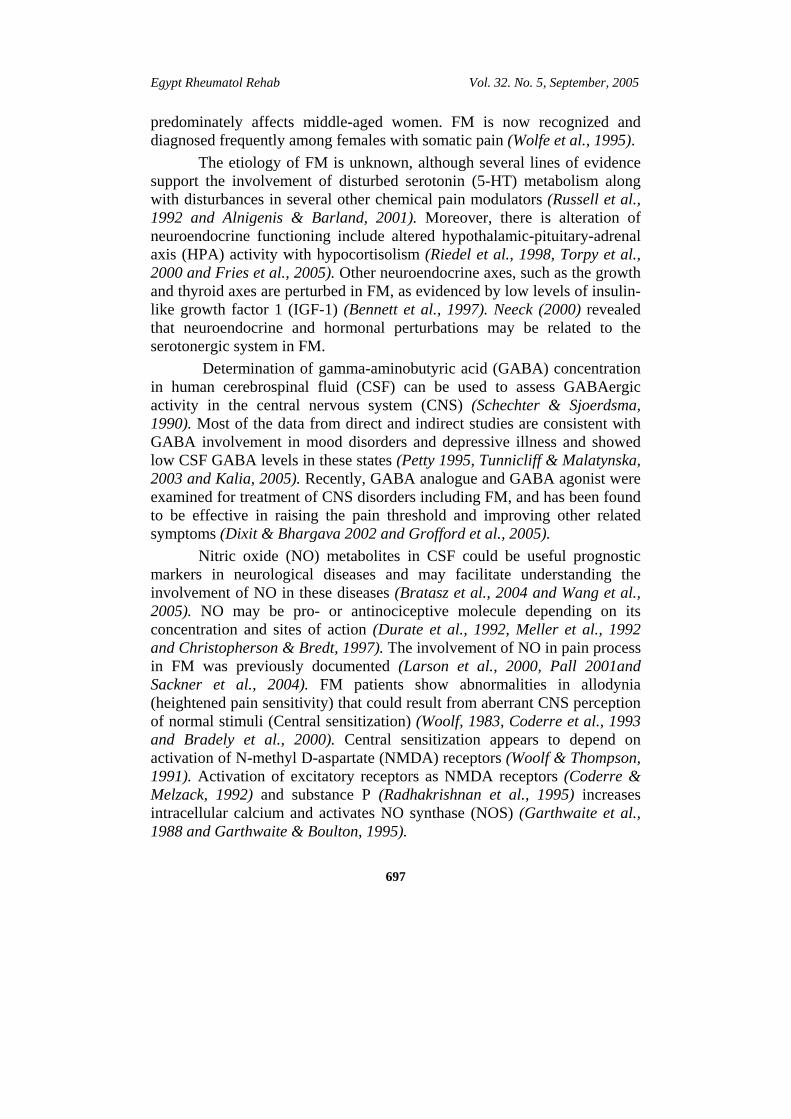
Quartiles [median (25th, 75th percentile)] of serum and CSF levels of neurotransmitters were presented in table 2 and 3. Low levels of serum 5-HT (p< 0.01) and CSF 5-HIAA (p<0.001) in women suffering of FM compared to control group was demonstrated in figure 1. In this study (table 4) serum levels of 5-HT were correlated positively with the levels of CSF GABA (r= 0.56, p< 0.05).

Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
701
Table (2): Serum levels of hormones and neurotransmitters in studied groups. Parameters Control (n= 15) FM (n= 15) U p
Insulin (μIU/mL) Mean + SE Median (25, 75th percentile)
19.37 + 1.83
20.6 (13.25, 26.3)
27.72 + 1.61
30.3 (23.9, 33.1)
38
** 0.002
IGF-1 (ng/ ml) Mean + SE Median (25, 75th percentile)
216.2 + 14.12 202 (175, 275)
246.3 + 22.45
238 (178.5, 329.5)
93.3
0.443
Cortisol (μg/ dl) Mean + SE Median (25, 75th percentile)
10.29 + 0.85 10 (7.5, 17.3)
7.86 + 0.93 7 (5, 10.25)
63
* 0.040
5-HT (ng/ ml) Mean + SE Median (25, 75th percentile)
128 + 12.57
135 (83.75,177.5)
73.9 + 10.32
82.5 (36.25, 100)
48.5
** 0.005
GABA (ng/ ml) Mean + SE Median (25, 75th percentile)
85.35 + 6.39
75.5 (62.75, 110)
55.99 + 5.91
55 (40.25, 72.5)
40
** 0.003
NO (nmol/ ml) Mean + SE Median (25, 75th percentile)
33.69 + 2.78
29 (25, 42.25)
63.07 + 5.36
69 (59.1, 79.5)
35.5
** 0.002
**p< 0.01,*p< 0.05, comparing controls vs. FM groups using Mann-Whitney test. Table (3): CSF levels of neurotransmitters in studied groups. Parameters Control (n= 15) FM (n= 15) U p
CSF 5-HIAA (ng/ ml) Mean + SE Median (25, 75th percentile)
29.07 + 1.35
27.5 (26.65, 34)
19.75 + 0.89 19 (17.5, 24)
15
*** <
0.001 CSF GABA (ng/ ml) Mean + SE Median (25, 75th percentile)
41.58 + 2.06 43 (37, 55.3)
29.95 + 2.36
25 (22.75, 38.5)
38
** 0.002
CSF NO (nmol/ ml) Mean + SE Median (25, 75th percentile)
21.18 + 1.02 21 (18, 23.3)
28.78 + 2.48 27.6 (19.79,
40.25)
61
* 0.034
***p< 0.001, **p < 0.01, *p< 0.05 comparing controls vs FM groups using Mann-Whitney test.

CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
702
Fig. (1): Mean serum levels of 5-HT and mean CSF levels of 5-HIAA in FM and control group.
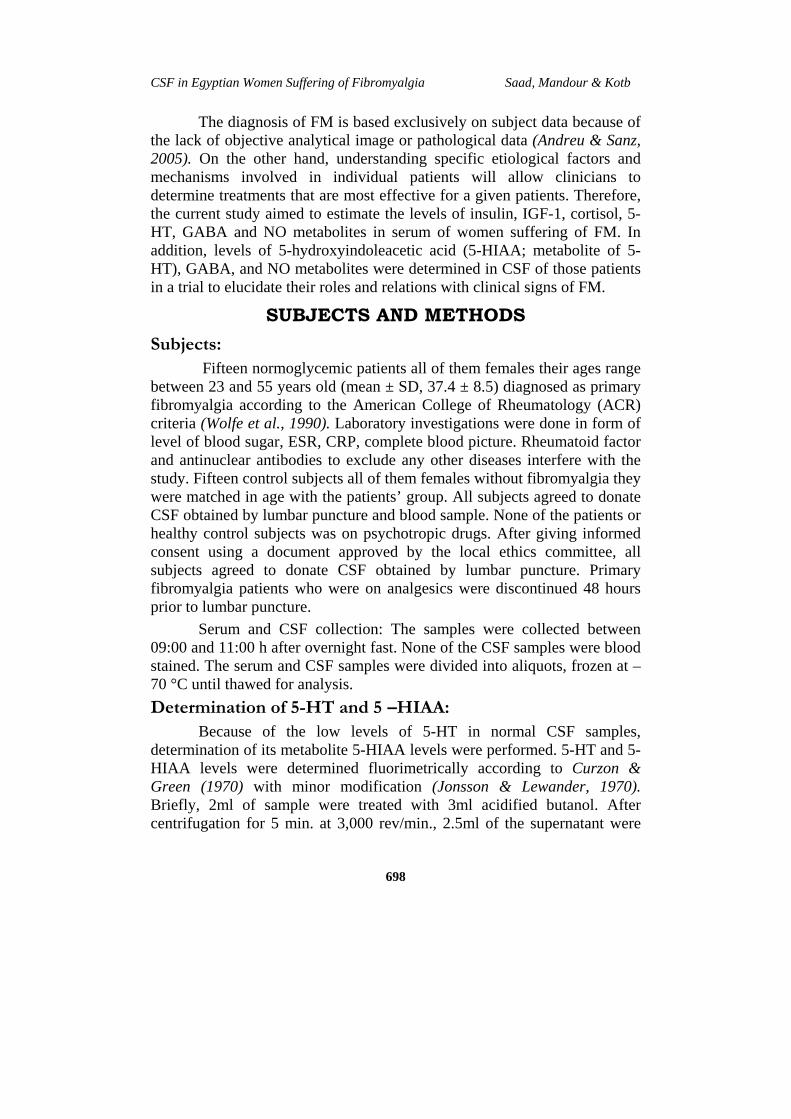
Fig. (2): Mean serum and CSF levels of GABA in FM and control group.
Con FM CSF Con CSF FM0
50
100
150 < 0.01
< 0.01
GAB
A ng
/ ml
Con FM CSF Con CSF FM0
100
200
< 0.01
< 0.001
5-HT 5-HIAA
ng/ m
l

Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
703
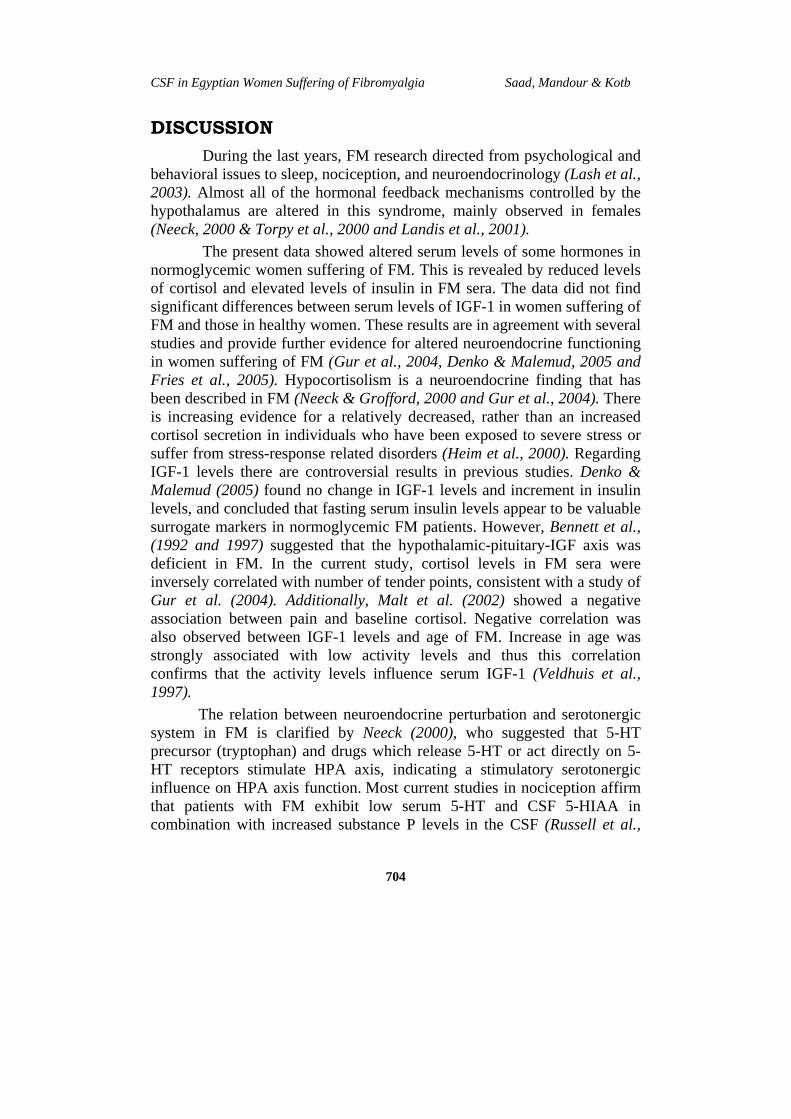
Fig. (3): Mean serum and CSF levels of NO in FM and control group.
The decrement of both serum and CSF levels of GABA (p<0.01) were detected in women suffering of FM compared with control group (figure 2). Moreover, CSF GABA levels were positively correlated (r= 0.67, p<0.01) with serum levels of GABA in those patients. In contrast, negative correlation was showed between age and CSF GABA levels (r= -0.74, p<0.01) among women suffering of FM. Our statistical analysis demonstrated a positive correlation (r= 0.61, p<0.05) between serum cortisol and serum GABA levels in women suffering of FM (table 4).
The higher serum and CSF levels of NO metabolites were detected (figure 3) in women suffering of FM than control group (p<0.01, p<0.05 respectively). Table 4 mentioned that levels of serum NO metabolites were correlated with levels of CSF NO metabolites in those patients (r=0.63, p<0.05). Our study also noticed strong correlation between levels of NO metabolites (either in serum or CSF) and number of tender points (r= 0.91, p<0.001; r=0.73, p<0.01 respectively). In contrast, there was inverse correlation between those levels in sera of women suffering of FM and serum levels of cortisol (r= -0.70, p< 0.01).
Con FM CSF-Con CSF-FM0
25
50
75
100
NO
(nm
ol/ m
l)
< 0.01
< 0.05
CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
704
DISCUSSION During the last years, FM research directed from psychological and
behavioral issues to sleep, nociception, and neuroendocrinology (Lash et al., 2003). Almost all of the hormonal feedback mechanisms controlled by the hypothalamus are altered in this syndrome, mainly observed in females (Neeck, 2000 & Torpy et al., 2000 and Landis et al., 2001).
The present data showed altered serum levels of some hormones in normoglycemic women suffering of FM. This is revealed by reduced levels of cortisol and elevated levels of insulin in FM sera. The data did not find significant differences between serum levels of IGF-1 in women suffering of FM and those in healthy women. These results are in agreement with several studies and provide further evidence for altered neuroendocrine functioning in women suffering of FM (Gur et al., 2004, Denko & Malemud, 2005 and Fries et al., 2005). Hypocortisolism is a neuroendocrine finding that has been described in FM (Neeck & Grofford, 2000 and Gur et al., 2004). There is increasing evidence for a relatively decreased, rather than an increased cortisol secretion in individuals who have been exposed to severe stress or suffer from stress-response related disorders (Heim et al., 2000). Regarding IGF-1 levels there are controversial results in previous studies. Denko & Malemud (2005) found no change in IGF-1 levels and increment in insulin levels, and concluded that fasting serum insulin levels appear to be valuable surrogate markers in normoglycemic FM patients. However, Bennett et al., (1992 and 1997) suggested that the hypothalamic-pituitary-IGF axis was deficient in FM. In the current study, cortisol levels in FM sera were inversely correlated with number of tender points, consistent with a study of Gur et al. (2004). Additionally, Malt et al. (2002) showed a negative association between pain and baseline cortisol. Negative correlation was also observed between IGF-1 levels and age of FM. Increase in age was strongly associated with low activity levels and thus this correlation confirms that the activity levels influence serum IGF-1 (Veldhuis et al., 1997).
The relation between neuroendocrine perturbation and serotonergic system in FM is clarified by Neeck (2000), who suggested that 5-HT precursor (tryptophan) and drugs which release 5-HT or act directly on 5-HT receptors stimulate HPA axis, indicating a stimulatory serotonergic influence on HPA axis function. Most current studies in nociception affirm that patients with FM exhibit low serum 5-HT and CSF 5-HIAA in combination with increased substance P levels in the CSF (Russell et al.,

Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
705
1992, 1994 and Legangneux et al., 2001). Substance P levels are normally high in the axons of primary unmyelinated C-fiber sensory neurons (McNeill et al., 1989) and its physiologic functions are mediated by 5-HT (Murphy & Zemla, 1987). On the other hand, Jonsson et al. (2004) stated that concentrations of monoamine metabolites in human CSF have been used extensively as indirect estimates of monoamine turnover in the brain. This study concerning serum 5-HT and CSF 5-HIAA confirm those of the aforementioned researches. Low levels of serum 5-HT and CSF 5-HIAA showed in this study probably result from disturbed 5-HT metabolism. 5-HT is recognized chemical mediator of sleep and of pain perception by both the thalamus and the peripheral nervous system (Harvey et al., 1975). The role of 5-HT is supported by an observation of Juhl (1998) who examined 5-HT substrates as supplements in FM. The author reported that L-tryptophan or 5-hydroxytryptophan has been shown to improve symptoms of depression, anxiety, insomnia and somatic pain in a variety of FM patient cohorts. The effects of 5-HT2 and 5-HT3 receptor antagonists were performed for treatment of FM (Farber et al., 1998 and Stratz & Muller, 2000). The investigators sought a possible reduction in pain based on the premise that binding of 5-HT to its receptor can trigger pain, probably due to the release of potent pain mediators such as substance P and other neurokines. Some medical literature demonstrated the relationship between age and CSF levels of 5-HIAA (Larsson et al., 1988 and Russell et al., 1992). However, the present data showed no correlation between age and CSF 5-HIAA levels in FM. This finding is compatible with other investigations (Kruesi et al., 1988 and Faustman et al., 1990).
The balance between excitatory signaling mediated by glutamate and inhibitory signaling mediated by GABA plays a pivotal role in mechanisms underlying the modulation and maintenance of a variety of neural functions. Therefore, abnormalities in GABAergic signaling molecule would lead to a crisis of severe symptoms relevant to number of neuropsychiatric disorders including depression (Fujimori & Yoneda, 2004, Kaluev & Nutt, 2004 and Kalia 2005). The decrement of both serum and CSF levels of GABA were detected in women suffering of FM compared with control group. Moreover, CSF GABA levels were correlated with serum levels of GABA in those patients. Petty (1995) reported that low GABA levels are found in brain, CSF and plasma of patients with depression. This could be attributed to decreased levels of glutamate decarboxylase (Fatemi et al., 2005). Other study showed no differences in CSF GABA between depressed patients and normal controls (Roy et al., 1991). The current investigations showed

CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
706
negative correlation between age and CSF GABA levels among women suffering of FM. Later, the CSF GABA concentrations were found to be varied with age, sex, CSF fraction collection and storage (Schechter & Sgoerdsma, 1990 and Takayama et al., 1992). GABA, the principal neurotransmitter in the cerebral cortex is formed within GABAergic axon terminals and released into synapse, where it acts at one of the two types of receptor. GABAA, which control chloride entry into the cell, and GABAB which increases potassium conductance, decreases calcium entry and inhibits the presynaptic release of other neurotransmitters (Treiman, 2001). GABA analogue and GABA agonist have been found to be effective for treatment of CNS disorders (Dixit & Bhargava, 2002 and Grofford et al., 2005). GABA analogue is effective in raising the pain threshold, reducing allodynia increasing slow-wave non rapid eye movement sleep, relieving anxiety, modulating acute pain symptoms, and reducing colon-related pain in FM (Grofford et al., 2005). Our statistical analysis demonstrated a positive correlation between serum cortisol and serum GABA levels in women suffering of FM. There is no explanation for this correlation. However, a recent study revealed a role of GABA in mediating the effects of corticotrophin-releasing factor on the rat dorsal raphe 5-HT system (Waselus et al., 2005). In this study serum levels of 5-HT were correlated positively with the levels of CSF GABA. 5-HT might elicit the inhibitory effect through a Ca (2+)-sensitive release of GABA from intercalated GABAergic local neurons that are excised first by 5-HT (Kang et al., 2002). On the other hand, the pineal hormone, melatonin (5-HT product) seems to be the natural hormone to facilitate sleep in insomnia patients acts via GABA receptor (Rohr & Herold, 2002).
Recent literatures demonstrated that the inhibition of NOS especially inducible NOS (iNOS) produces antinociception in different models of pain suggest that the iNOS-NO system plays in pain processing (Eriksen 2004, Goadsby 2005 and Labuda et al., 2005). NO exhibits a peripheral analgesic effect, whereas it mediates hyperalgesia at spinal or supraspinal level (Durate et al., 1992 & Kawabata et al., 1992 & Meller et al., 1992). Herein the higher serum and CSF levels of NO metabolites were detected in women suffering of FM than control group. Furthermore, levels of serum NO metabolites were correlated with levels of CSF NO metabolites in those patients. Our study also noticed strong correlation between levels of NO metabolites (either in serum or CSF) and number of tender points. In contrast, there was inverse correlation between those levels in sera of women suffering of FM and serum levels of cortisol. These data clarified
Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
707
the implication of NO in pain processing in FM (Larson et al., 2000, Pall, 2001 and Sackner et al., 2004). The elevated levels of NO metabolites may be due to increase NOS activity with increased pain (Larson et al., 2000). NOS activity was associated with NMDA receptor-mediated events as well as substance P activity during thermal and mechanical nociceptive transmission in the cat dorsal horn (Radhakrishnans & Henry, 1993 and Mens, 2001) reported that in contrast to excitability, the resting activity of dorsal neurons which is likely to induce spontaneous pain does not appear to depend on the release of substance P and glutamate but on the concentration of NO in the spinal cord.
The ability of NOS inhibitors to prevent the development and expression of many types of hyperalgesia including FM may be by blocking the downstream mediators of NMDA activation (Meller et al., 1992, Rao, 2002,Llabuda et al., 2005 and Pall 2001) suggested that variation in symptoms might be explained by a variation in NO /peroxynitrite tissue distribution. Peroxynitrite is formed from reaction of NO with superoxide radical (Henry et al., 1991). Peroxynitrite concentration may affect dopamine concentration inversely and may act to facilitate glutamate and GABA release (Trabace & Kendrik, 2000).
Because arginine is the first amino acid at the amino terminus of substance P, one might speculate that the source of arginine in patients with FM may reflect, in part, degradation of substance P in CSF (Russell et al., 1993).
Apart from the known role of 5-HT in the pathogenesis of FM. GABA and NO are involved in either mood, depression, anxiety, or pain and fatigue. Therefore, the current study suggests that they may play a role in modulating FM. This is clarified by the alterations of these neurotransmitters either in serum or CSF of women suffering of FM. In addition, levels of the studied neurotransmitters appear to be partly correlated to age, number of tender points and/or cortisol. Accordingly, this study recommended the possibility of using innovative therapy as GABAergic agents, NOS inhibitors, or antioxidants for therapy of various symptoms in women suffering of FM. Moreover, our study may find utility of these neurotransmitters as possible markers of FM, but this warrant more studies to confirm these findings.

CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
708
REFERENCES Alnigenis MN and Barland P (2001): Fibromyalgia syndrome and serotonin. Clin. Exp.
Rheumatol 19(2): 205-10. Andreu JL and Sanz J (2005): Fibromyalgia and its diagnosis. Rev. Clin. Esp. 205 (7):
333- 6. Bennett RM, Clark SR, Campbell SM and Burckhardt CS (1992): Low levels of
somatomedin-C in patients with the fibromyalgia syndrome. Arthritis Rheum 35: 1113- 16.
Bennett RM, Clark SR, Burckhardt CS, Campbell SM and Cook DM (1997): Hypothalamic-pituitary-insulin-like growth factor-1 axis dysfunction in patients with fibromyalgia. J. Rheumatol 24: 1384- 89.
Blum WF, Albertsson- Wikland K, Rosberg S and Ranke MB (1993): Serum levels of insulin-like growth factor-1 (IGF) and IGF binding protein 3 reflect spontaneous growth hormone secretion J. Clin End and Metab 76: 1610- 16.
Bradley LA, Mckendree-Smith NL and Alarcon GS (2000): Pain complaints in patients with fibromyalgia versus chronic fatigue syndrome. Cur. Rev. Pain 4 (2): 148- 72.
Bratasz A, Kuter I, Konior R, Goscinski I and Lukiewicz S (2004): Nitric oxide as a prognostic marker for neurological diseases. Antioxid. Redox. Signal 6 (3):613- 7.
Christopherson KS and Bredt DS (1997): Perspective series: nitric oxide and nitric oxide synthase. Nitric oxide in excitable tissues: physiologic roles and disease. J. Clin. Invest 100: 2424- 9.
Coderre TJ and Melzack R (1992): The role of NMDA receptor operated calcium channels in persistent nociception after formalin-induced tissue injury. J. Neurosci 12: 3671- 75.
Corderre TJ, Katz J, Vaccarino AL and Melzack R (1993): Contribution of central neuroplasticity to pathological Pain: review of clinical and experimental evidence. Pain 52:259-85.
Curzon G and Green AR (1970): Rapid method for determination of 5-hydroxytryptamine and 5-hydroxyindoleacetic acid in small regions of rat brain. Br. J. Pharmacol 39: 653- 55.
Denko CW and Malemud CJ (2005): Serum growth hormone and insulin but not insulin-like growth factor-1 levels are elevated in patients with fibromyalgia syndrome. Rheumatol Int. 25 (2): 146-51.
Ding AH, Nathan CF and Stuchr DJ (1988): Release of reactive nitrogen intermediate from mouse peritoneal macrophage comparison of activating cytokines and evidence for independent production. J. Immunol 141: 240712.
Dixit RK and Bhargava VK (2002): Neurotransmitter mechanisms in gabapentin antinociception. Pharmacology 65(4): 198- 203.

Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
709
Durate IDG, Pols-Satos IR, Lorenzetti BB and Eerreira (1992): Analgesia by direct antagonism of nociceptor sensitization involves the arginine-nitric oxide cyclic GMP pathway. Eur. J. Pharmacol 215: 225-7.
Eriksen W (2004): Linking work factors to neck myalgia: the nitric oxide/oxygen ratio hypothesis. Med. Hypotheses 62 (5): 721-6.
Farber L, Stratz Th and Muller W (1998): New aspects for the medical treatment of results of a double-blind, randomized, placebo-controlled multi-centre trial evaluating the efficacy and tolerability of the 5-HT3-antagonist tropisetron in primary fibromyalgia. Zschr Rheumatol.57 Supplemet 1: 30.
Fatemi SH, Stary JM, Earle JA, Araghi-Niknam M and Eagan E (2005): GABAergic dysfunction in schizophrenia and mood disorders as reflected by decreased levels of glutamic acid decarboxylase 65 and 67 kDa and Reelin proteins in cerebellum. Schizophr Res. 1; 72 (2-3): 109-22.
Faustman WO, Faull KF, Whiteford HA, Borchert C and Csernansky JG (1990): CSF 5-HIAA, serum cortisol and age differentially predict vegetative and cognitive symptoms in depression Biol. Psychiatry 27: 311- 18.
Frier BM, Ashby JP, Nairan IM and Bairs JD (1981): Plasma insulin, C peptide and glucagon concentrations in patients with insulin-independent diabetes treated with chlorpropamide Diab Metab 7, 1, 45-9.
Fries E, Hesse J, Hellhammer J and Hellhammer DH (2005): A new view on hypocortisolism. Psychoneuroendocrinology 30 (10): 1010-6
Fujimori S and Yoneda Y (2004): Neuropsychiatric disorders and GABA. Nihon Shinkei Seishin Yakurigaku Zasshi. 24 (5): 265-71.
Garthwaite J, Charles SL and Chess-Williams R (1988): Endothelium-derived relaxing factor release on activation of NMDA receptors suggests role as intracellular messengers in the brain Nature 336: 385- 88.
Garthwaite J and Boulton CL (1995): Nitric oxide signaling in the central nervous system Annu Rev Physiol 57:683- 706.
Goodsby PJ (2005): New targets in the acute treatment of headache. Curr. Opin. Neurol. 18 (3): 283-8.
Grofford LJ, Rowbotham MC, Mease PJ, Russell IJ, Dworkin RH, Corbin AE, Young JP Jr, LaMoreaux LK, Martin SA and Sharma U (2005): Pregabalin for treatment of fibromyalgia syndrome: results of randomized, double-blind, placebo-controlled trial. Arthritis Rheum 52 (4): 1264-73.
Gur A, Cevik R, Sarac AJ, Colpan L and Em S (2004): Hypothalamic-pituitary-gonadal axis and cortisol in young women with primary fibromyalgia: the potential roles of depression, fatigue, and sleep disturbance in the occurrence of hypocortisolism. Ann. Rheum. Dis. 63 (11): 1504- 6.
Harvey JA, Schlosberg AJ and Yunger LM (1975): Behavioral correlates of serotonin depletion Fed Proc 34:1796- 801.
CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
710
Heim C, Ehlert U, Dirk H and Helhammer H (2000): The potential role of hypocortisolism in the pathophysiology of stress-related bodily disorders. Psychoendocrinology 25:1-35.
Henry Y, Ducrocq C, Drapier C, Servent D, Pellat C and Guissani A (1991): Nitric oxide, a biological effector electron paramagnetic resonance detection of nitrosyl-iron-protein complexes in whole cells. Eur. Biophys. J. 20: 1- 15.
Jonsson J and Lewander T (1970): A method for the simultaneous determination of 5-hydroxy-3-indole-acetic acid (5-HIAA) and 5-hydroxytryptamine (5-HT) in brain tissue and cerebrospinal fluid Acta physiol Scand 78: 43- 51.
Jonsson EG, Bah J, Melke J, Abou Jamra R, Schumacher J, Westberg L, Ivo R, Cichon S, Propping P, Nothen MM, Eriksson E and Sedvall GC (2004): Monoamine related functional gene variants and relationships to monoamine metabolite concentrations in CSF of healthy volunteers. BMC Psychiatry 4; 4 (1): 4.
Juhl JH (1998): Fibromyalgia and the serotonin pathway. Altern Med. Rev. 3 (5): 367-75.
Kalia M (2005): Neurobiological basis of depression: an update. Metabolism 54 (5 Suppl 1): 24-7.
Kaluev AV and Nutt DJ (2004): On the role of GABA in anxiety and depression. Eksp. Klin. Farmakol 67 (4): 71- 6.
Kang YM, Chen JY, Ouyang W and Qiao JT (2002): Serotonin excites arcuate neurons directly but inhibits them through intercalated GAB. Aergic neurons. Sheng Li Xue Bao 25, 54 (3): 189-95.
Kawabata A, Nishimura Y, Takagi H (1992): L-leucyl-L-arginine, naltrindole and D-arginine block antinociception elicited by L-arginine in mice with carrageenin induced hyperalgesia. Br. J. Pharmacol 107: 1096-101.
Kruesi MJP, Swedo SE, Hamburger SD, Potter WZ and Rapoport JL (1988): Concentration gradient of CSF monoamine metabolites in children and adolescents. Biol. Psychiatry 24:507-14.
Labuda CJ, Koblish M, Tuthill P, Dolle RE and Little PJ (2005): Antinociceptive activity of the selective iNOS inhibitor AR-C102222 in rodent models of inflammatory, neuropathic and post-operative pain. Eur. J. Pain 23.
Landis CA, Lentz MJ, Rothermel J, Riffle SC, Chapman D, Buchwald D and Shaver JLF (2001): Decreased nocturnal levels of prolactin and growth hormone in women suffering of fibromyalgia J. Clin Endocrinol Metab 86: 1672- 78.
Lash AA, Ehrlich-Jones L and McCoy D (2003): Fibromyalgia: evolving concepts and management in primary care settings. Medsurg. Nurs 12 (3): 145-59, 190; quiz 160.
Larson AA, Giovengo SL, Russell IJ and Michalek JE (2000): Changes in the concentrations of amino acids in the cerebrospinal fluid that correlate with pain
Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
711
in patients with fibromyalgia: implications for nitric oxide pathways. Pain 87:201-11.
Larsson M, Forsman A and Hallgren J (1988): HPLC assays of 5-HIAA and tryptophan in blood: a methodological study with clinical applications. Methods Find Exp Clin Pharmacol 10: 453- 60.
Legangneux E, Mora JJ, Spreux-Varoquaux O, Thorin I, Herrou M Alvado G and Gomeni C (2001): Cerebrospinal fluid biogenic amine metabolites, plasma-rich platelet serotonin and [3H] imipramine reuptake in the primary fibromyalgia syndrome. Rheumatology 40:290-6.
Malt EA, Olafsson S, Lund A and Ursin H (2002): Factors explaining variance in perceived pain in women suffering of fibromyalgia BMC Musculoskelet Disord 25; 3: 12.
McNeill DL, Westlund KN and Coggeshall RE (1989): Peptide immunoreactivity of unmyelinated primary afferent axons in rat lumbar dorsal roots. J. Histochem. Cytochem 37 (7): 1047-52.
Meller ST, Pechman PS, Gebhart GF and Maves TJ (1992): Nitric oxide mediates the thermal hyperalgesia produced in a model of neuropathic pain in the rat. J. Neurosci 50: 7-10.
Mens S (2001): Pathophysiology of low back pain and the transition of the chronic state-experimental data and new concepts. Schmerz 15 (6): 413- 17.
Murphy RM and Zemlan FP (1987): Differential effects of P on serotonin-modulated spinal nociceptive reflexes Psychopharmacology (Berl) 93: 118- 21.
Neeck G and Grofford LJ (2000): Neuroendocrine perturbations in fibromyalgia and chronic fatigue syndrome Rheum. Dis. Clin. North Am. 26:989-1002.
Neeck G (2000): Neuroendocrine and hormonal perturbations and relations to the serotonergic system in fibromyalgia patients Scand J. Rheumatol Suppl 113: 8- 12.
Pall ML (2001): Common etiology of post-traumatic stress disorder, fibromyalgia, chronic fatigue syndrome, and multiple chemical sensitivity via elevated nitric oxide/peroxynitrite. Med. Hypotheses 57 (2): 139-45.
Petty F (1995): GABA and mood disorders: a brief review and hypothesis. J. Affect. Disord. 18; 34 (4): 275- 81.
Radhakrishnan V and Henry JL (1993): L-NAME blocks responses to NMDA, substance P and noxious cutaneous stimuli in cat dorsal horn Neuro Report 4: 323- 26.
Radhakrishnan V, Yashpal K, Hui-Chan CW and Henry JL (1995): Implication of a nitric oxide synthase mechanism in the action of substance P: L-NAME blocks thermal hyperalgesia induced by endogenous and exogenous substance P in the rat Eur. J. Neurosci 7: 1920- 25.
Roa SG (2002): The neuropharmacology of centrally-acting analgesic medications in fibromyalgia Rheum Dis. Clin. North Am 28 (2): 235-59.

CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
712
Riedel W, Layka H and Neeck G (1998): Secretory pattern of GH, TSH, thyroid hormones, ACTH, cortisol, FSH and LH in patients with fibromyalgia syndrome following systemic injection of the relevant hypothalamic-releasing factors. Z. Rheumatol. 57 (Suppl 2): 81-7.
Rohr UD and Herold J (2002): Melatonin deficiencies in women. Maturitas 15; 41 Suppl 1: S 85- 104.
Roy A, Dejong J and Ferraro T (1991): CSF GABA in depressed patients and normal controls. Psychol Med. 21(3): 613-8.
Russell IJ, Michalek JE, Vipraio GA, Fletcher EM, Javors MA and Bowden CL (1992): Serum serotonin and platelet 3H-imipramine binding receptor density in patients with fibromyalgia /fibrositis syndrome. J. Rheumatol 19: 104- 9.
Russell IJ, Orr MD, Michalek JE, Nyberg F and Ericksson U (1993): Substance P (SP), SP endopeptidase activity, and SP N-terminal peptide fragment (SP1-7) in fibromyalgia syndrome cerebrospinal fluid. J. Musculoskel. Pain 3 (suppl 1): 51995.
Russell IJ, Orr MD, Littman B, Vipraio GA, Alboukrek D, Michalek JE and Lopez y, Mackillip F (1994): Elevated cerebrospinal fluid levels of substance P in patients with the fibromyalgia syndrome Arthritis Rheum 37: 1593- 601.
Sackner MA, Gummels EM and Adams JA (2004): Say NO to fibromyalgia and chronic fatigue syndrome: an alternative and complementary therapy to aerobic exercise. Med. Hypotheses 63 (1): 118-23.
Schechter PJ and Sjoerdsma A (1990): Clinical relevance of measuring GABA concentrations in cerebrospinal fluid. Neurochem. Res 15 (4): 419- 23.
Stratz Th and Muller W (2000): The use of 5-HT3 receptor antagonists in various rheumatic diseases – a clue to the mechanism of action of these agents in fibromyalgia? Scand J. Rheumatol 29 Suppl 113: 66- 71.
Takayama H, Ogawa N, Yamamoto M, Asanuma M, Hirata H and Ota Z (1992): Age-related change in cerebrospinal fluid gamma-aminobutyric acid concentration. Eur. J. Clin. Chem. Clin. Biochem 30 (5): 271-4.
Tijssen P (1985): Laboratory techniques in biochemistry and molecular biology, practice and theory of EIA, p. 174, Elsevier, Amsterdam.
Torpy DJ, Papanicolaou DA, Lotsikas AJ, Wilder RL, Chrousos GP and Pillemer SR (2000): Response of the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis to interleukin-6. A pilot study in fibromyalgia Arthritis Rheum 43: 872- 80.
Trabace L and Kendrick KM (2000): Nitric oxide can differentially modulate striatal neurotransmitter concentrations via soluble guanylate cyclase and peroxynitrite formation. J. Neurochem 75 (4): 1664-74.
Treiman DM (2001): GABAergic mechanisms in epilepsy. Epilepsia 42 Suppl. 3: 8-12. Tunnicliff G and Malatynska E (2003): Central GABAergic systems and depressive
illness. Neurochem. Res. 28 (6): 967-76.
Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
713
Uchida T and Brien RDO (1964): The effects of hydrazine on rat brain 5- hydroxytryptamine, norepinephrine, and gamma-aminobutyric acid. Biochem. Pharmacol 13: 752-60.
Veldhuis JD, Iranmanesh A and Weltman A (1997): Elements in the pathophysiology of diminished growth hormone (GH) secretion in aging humans. Endocrine 7: 41-48.
Wang X, Kimura S, Yazawa T and Endo N (2005): Cerebrospinal fluid sampling by lumbar puncture in rat-repeated measurements of nitric oxide metabolites. J. Neurosci. Methods 30; 145 (1-2): 89-95.
Waselus M, Valentino RJ and Van Bockstaele EJ (2005): Ultrastructural evidence for a role of gamma-aminobutyric acid in mediating the effects of corticotropin-releasing factor on the rat dorsal raphe serotonin system. J. Comp. Neurol.7, 482 (2): 152-65.
Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombadier C, Goldenberg DL, Tugwell P, Campbell SM, Abeles M, Clark P, Fam AG, Farber SJ, Fiechtner JJ, Franklin CM, Gatter RA, Hamaty D, Lessard J, Lichtbroun AS, Masi AT, McGain GA, Reynolds WJ, Romano TJ, Russell IJ and Sheon RP (1990): The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: report of the multicenter criteria committee Arthritis Rheum 33: 160-72.
Wolfe F, Ross K, Anderson J, Russell IJ and Hebert L (1995): The prevalence and characteristics of fibromyalgia in the general population Arthritis Rheum 38: 19- 28.
Woolf CJ (1983): Evidence for a central component of post-injury pain hypersensitivity Nature 308: 686- 88.
Woolf CJ and Thompson SWN (1991): The induction and maintenance of central sensitization is dependent on N-methyl-D-aspartic acid receptor activation: implications for treatment of post-injury pain hypersensitivity states. Pain 44: 293- 99.
CSF in Egyptian Women Suffering of Fibromyalgia Saad, Mandour & Kotb
714
اندول اسيتيك وحمض الجاما يهيدروآس-5مستويات حمض ال للسيدات ي سائل النخاع الفقريأمينوبيوتيريك ونواتج أآسيد النيتريك ف
ي العضلي األلم الليفاتالمصريات ذو *قطب حسن و *مندور محمد أحمد ومنال سعد محمد أحمد سحر
**ووحدة األلم الطبية *أقسام الروماتيزم والتأهيل و الكيمياء الحيوية ي أسيوط الجامعفي جامعة أسيوط ومستش-آلية الطب
دة الت من اإل ي العضل ي ُيعد األلم الليف :مقدمة ا تصيب يضطرابات المزمنة المعق ًا م غالب
دم المرض جذبت واإل. السيدات ة تق شخيص أو متابع ل من أجل ت فتقار إلى صورة واضحة للتحليد تكون فيالموصالت العصبية والهرمونات العديد من الباحثين لقياس تغيرات سوائل الجسم التى ق
.بفسيولوجية المرض لها عالقة ستويات حمض ال إ لذا فإن هذه الدراسة :الهدف ة م دول ي هيدروآس 5ستهدفت مقارن إن
ك ف سيد النيتري واتج أآ ك ون ا أمينوبيوتيري يتيك و حمض جام سيدات يأس شوآي ل سائل المخي ال الضابطة ا الليفي العضلي وذوات مستوى سكر طبيعي في الدم بتلك مصابات باأللم ،لتي للمجموعة ال
ك ف ى ذل افة إل سيولين إباإلض بيه اإلن ل ش سيولين وعام ستويات اإلن ورتيزول و 1-ن م والكسيد ي هيدروآس 5السيروتينين وحمض ال واتج أآ ا أمينوبيوتيريك ون يتيك و حمض جام دول أس إنديرها م تق د ت ك ق يالنيتري ضابطة ف ة ال ة بالمجموع ضلي بالمقارن ي الع م الليف . مصل مرضى األل
.رتباط بين آل القياسات المدروسةإوأيضًا فقد أجريت عالقات ورتيزول ف ي ف اشاهدت الدراسة الحالية تغيير : النتائج سيولين والك مصل ي مستويات اإلن
يدة 15(ي يعالسيدات المصابات باأللم الليفي العضلي ذوات مستوى السكر الطب ة في ) س دم مقارن البيه يولكن النتائج لم تجد أى فروق جوهرية ف). سيدة15(بالمجموعة الضابطة ستويات عامل ش م
نهم في 1-اإلنسيولين األلم الليفي العضلي ع سيدات المصابات ب سليمات في أمصال ال سيدات ال . الورتيزول وعد إوآانت هناك عالقة ستويات الك ين م اط عكسي ب م رتب اط األل ضًا لوحظت . د نق وأي
م الليفي ي ف 1-رتباط سالبة بين مستويات عامل شبيه اإلنسيولين إعالقة المصل وعمر مرضى األلسيروتونين ف . العضلي يتيك 5 المصل و حمض ال يوقد نقصت مستويات ال دول أس هيدروآسى إن
ين نقصان . السائل النخاعي الشوآي بين مرضى األلم الليفي العضلي في ستويات حمض في وتب مك ا أمينوبيوتيري يجام ة ف ؤالء المرضى مقارن ي ه شوآي ف اعي ال سائل النخ صل وال ن الم ل م آستويات حمض إباإلضافة إلى ذلك فقد آان هناك عالقة . بالمجموعة الضابطة ين م ة ب اط إيجابي رتب
ستويات حمض جاما أمينو ين م ضًا ب بيوتيريك في المصل و مستويات الكورتيزول في المصل و أيك ف . جاما أمينوبيوتيريك في السائل النخاعي الشوآي و السيروتونين في المصل ستويات إمع ذل ن م
رتبط سالبًا مع عمر السيدات المصابات إحمض جاما أمينوبيوتيريك في السائل النخاعي الشوآي قد سبب . ليفي العضلي باأللم ال ا أمينوبيوتيريك في ال ام لحمض جام دور اله د توضح ال ائج ق ذه النت ه
ضلي ي الع م الليف ضح . المرضى لألل صل إأت ي الم ك ف سيد النيتري واتج أآ ستويات ن ي م اع ف رتفك . والسائل النخاعي الشوآي لمرضى األلم الليفي العضلي عن المجموعة الضابطة باإلضافة إلى ذل
ستويإف ك ن م سيد النيتري واتج أآ يات ن د ف سائل إ المصل ق ي ال ستويات ف ذه الم ا به رتبطت إيجابية اإل . النخاعي الشوآي د اتضح بعالق م ق ين إن اشتراك أآسيد النيتريك في عملية األل ة ب اط القوي رتب
Egypt Rheumatol Rehab Vol. 32. No. 5, September, 2005
715
شوآي (مستويات نواتج أآسيد النيتريك سائل النخاعي ال م ) في المصل و ال اط األل ذلك . وعدد نق آورتيزول في القة اإل بع ستويات الك رتباط السالبة بين مستويات نواتج أآسيد النيتريك في المصل وم
.المصل مرضى األلم الليفي العضليي درست في :االستنتاج إن التغيرات في مستويات الهرمونات و الموصالت العصبية الت
ة ت نظري ضلي دعم ي الع األلم الليف صابات ب سيدات الم ث لل ذا البح ات و شإه تراك الهرموني العضلي م الليف سبب المرضى لألل ي ال د . الموصالت العصبية ف ة أن إوق قترحت الدراسة الحالي
ب دورا ا تلع ك ربم سيد النيتري ك و أآ ا أمينوبيوتيري يحمض جام ل ف ضلي تقللي ي الع م الليف . األلم الليفي شوآي لمرضى األل سائل النخاعي ال ستوياتهم في المصل وال ذلك وتغيرات م العضلي و آ
ا . قتراحأو الكورتيزول ربما تؤآد هذا اإل /رتباط بينهم وبين العمر وعدد نقاط األلم و عالقات اإل طبقا أمينوبيوتيريك أو مثبطات إلذلك فينصح هذا البحث ب وم بعمل حمض جام ى تق ختبار العوامل الت
المختلفة لأللم الليفي العضلي اإلنزيم المخلق ألآسيد النيتريك أو مضادات األآسدة لعالج األعراض ك ف . في السيدات ا تجد إباإلضافة إلى ذل تنا ربم ه من المحتمل أن دراس ذه الموصالت إن ستخدام ه
ذه ،العصبية آدالالت لأللم الليفي العضلي ولكن هذه الدراسة تحتاج المزيد من األبحاث للتأآد من ه .النتائج