leucocytes benign disorders nada mohamed ahmed, md, mt (ascp)i
TRANSCRIPT
leucocytes Benign Disorders
Nada Mohamed Ahmed ,MD, MT (ASCP)i

Contents. Definitions Classification Benign WBCs disorders
QuantitativeChange in number
QualitativeChange in (function & structure)
LEUCOCYTES BENIGN DISORDERS
Terminology Cytosis / philia
Increase in number Cytopenia
Decrease in number

Relative vs Absolute values Total white blood cell count Differential count Absolute count
Differential gives the relative percentage of each WBCAbsolute value gives the actual number of each WBC/mm3 of blood Calculation: absolute count= Total WBC x
percent
How to diffrentiate between LEUCOCYTOSIS and LEUCOPENIA

Quantitative changes (LEUCOCYTOSIS)
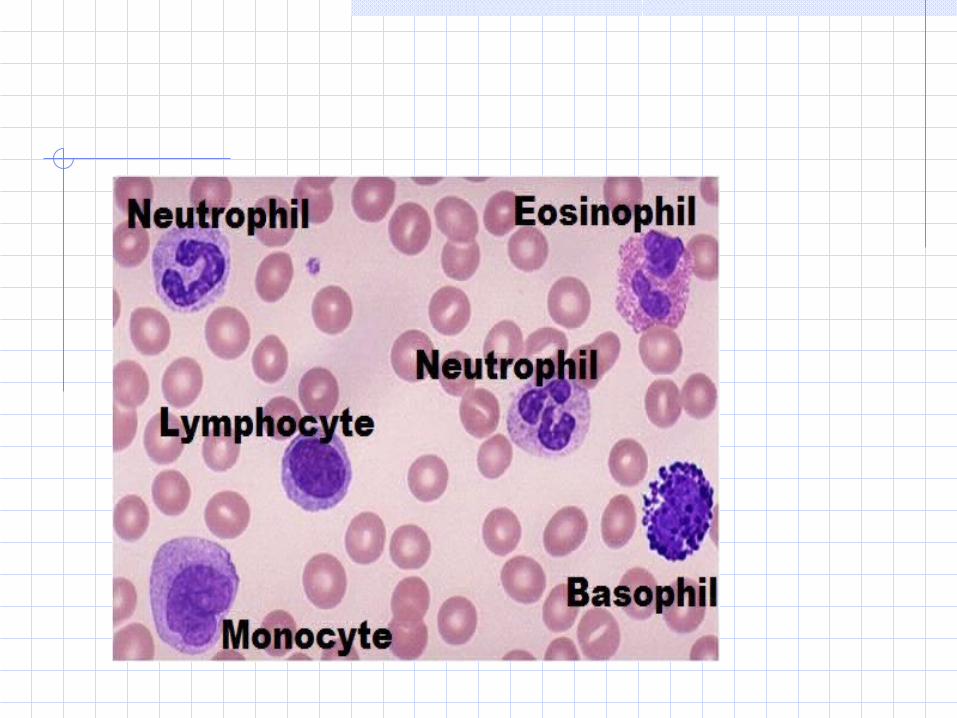
Leucocytes Phagocytes
Granulocytes Neutrophils Eosinophils BasophilsAgranulocytes
Mononuclear phagocytic cells Monocytes
Lymphocytes B-cells T-cells

LEUCOCYTES BENIGN DISORDERS Quantitative changes
(LEUCOCYTOSIS) increase WBCs count more than normal range
decrease TWBC lower than the normal range for the ,the body more susceptible to infection
(LEUCOPENIA)Normal range (adult)
4.5 -- 11.0 x 109/L
Definition:

LEUCOCYTES BENIGN DISORDERS Quantitative changes (contd.)
GranulocytosisIncrease in the count of all or one of the granulocytic component
Neutrophils Basophils Eosinophils
AgranulocytosisDecrease in the count of all or one granulocytic component

LEUCOCYTES BENIGN DISORDERS Quantitative changes (NEUTROPHILIA)
Definition Increase in the number of neutrophils and / or its precursors In adults count >7.5 x 109/L
Causes of NeutrophiliaInfection
BacterialInflammatory conditions
Autoimmune disorders
Marrow infiltration/fibrosisMyeloproliferative disorders
Quantitative changes (NEUTROPENIA)
Neutropenia is a decrease in Neutrophils absolute count.
Causes of NeutropeniaDrugs(chemotherapy of cancer patients)Irradiation exposureHyperslplenism

LEUCOCYTES BENIGN DISORDERS Quantitative changes (NEUTROPENIA) contd.
Causes of Neutropenia Drugs Irradiation exposure Immune disorders
HIV Neonatal i and autoimmune neutropenia
Hyperslplenism

Quantitative changes (EOSINOPHILIA)
Increase in the eosinophil count mustThe causes of eosinophilia
Allergy Atopic, drug sensitivity and pulmonary eosinophilia
Infection Parasites,
Malignancy Hodgkin’s disease, myeloproliferative disorders
Drugs

LEUCOCYTES BENIGN DISORDERS Quantitative changes (MONOCYTOSIS)
Increase in Absolute monocytes count
Causes of monocytosis Infections
Chronic infection (TB, typhoid fever) Malignant disease Connective tissue disorders
Ulcerative colitis, Sarcoidosis, Crohn’s disease

Quantitative changes (LYMPHOCYTOSIS)
Causes of LYMPHOCYTOSIS Infections
Viral infections
Increase in Absolute lymphocyte count
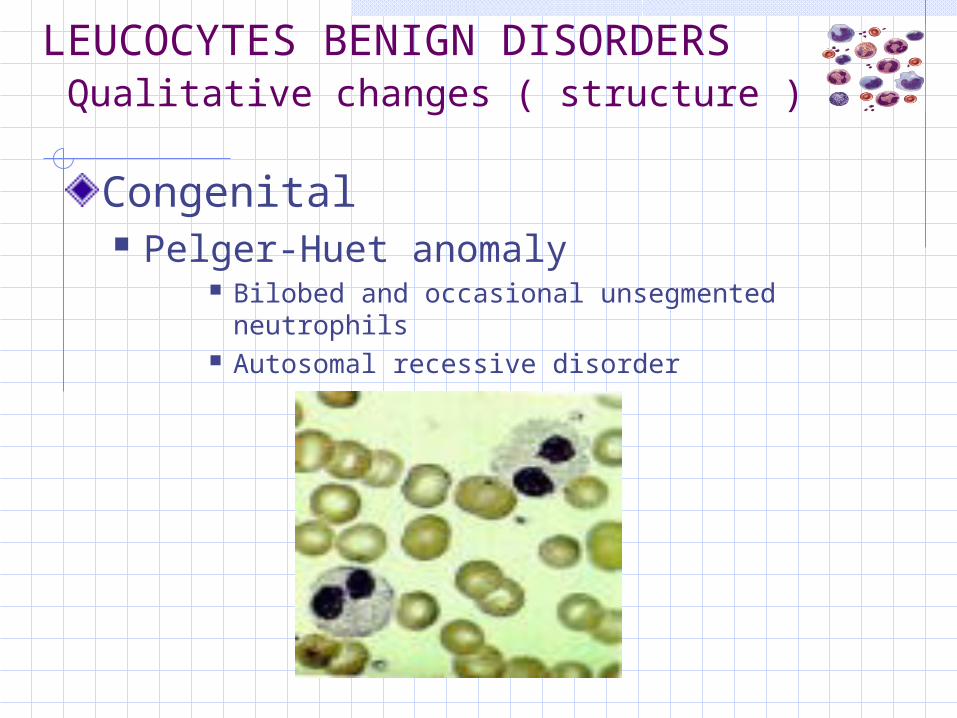
LEUCOCYTES BENIGN DISORDERS Qualitative changes ( structure )
Congenital Pelger-Huet anomaly
Bilobed and occasional unsegmented neutrophils Autosomal recessive disorder
LEUCOCYTES BENIGN DISORDERS Qualitative changes (MORPHOLOGY) contd.
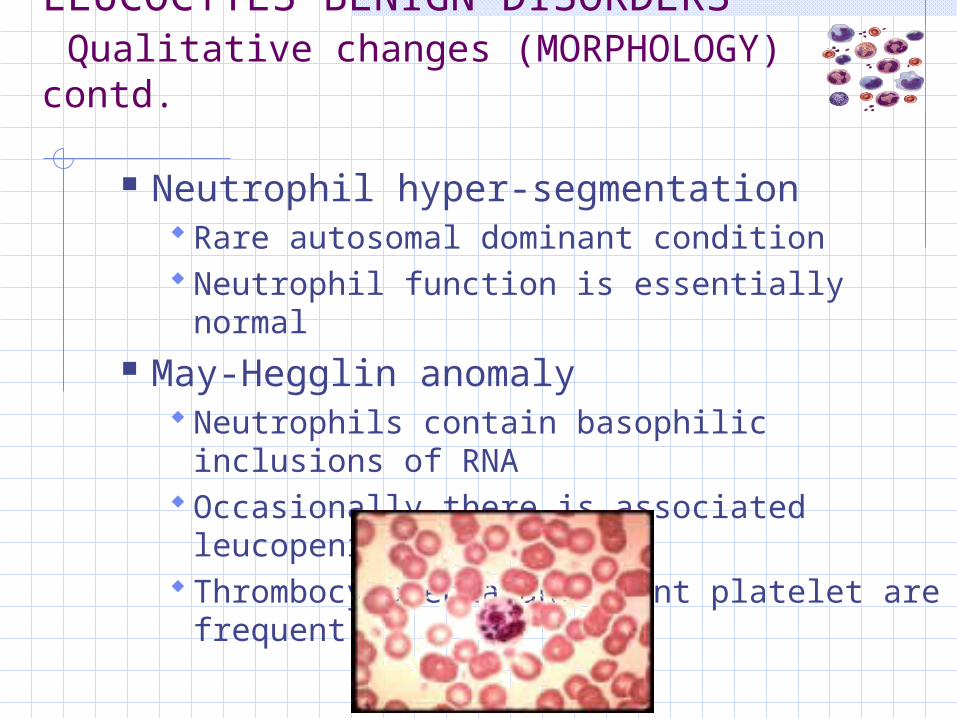
Neutrophil hyper-segmentation Rare autosomal dominant condition Neutrophil function is essentially normal
May-Hegglin anomaly Neutrophils contain basophilic inclusions of
RNA Occasionally there is associated leucopenia Thrombocytopenia and giant platelet are
frequent

LEUCOCYTES BENIGN DISORDERS Qualitative changes (MORPHOLOGY) contd.
Alder’s anomaly Granulocytes, monocytes and lymphocytes
contain granules which stain purple with Romanowsky stain
Granules contain mucopolysaccharides
LEUCOCYTES BENIGN DISORDERS Qualitative changes (MORPHOLOGY) contd.
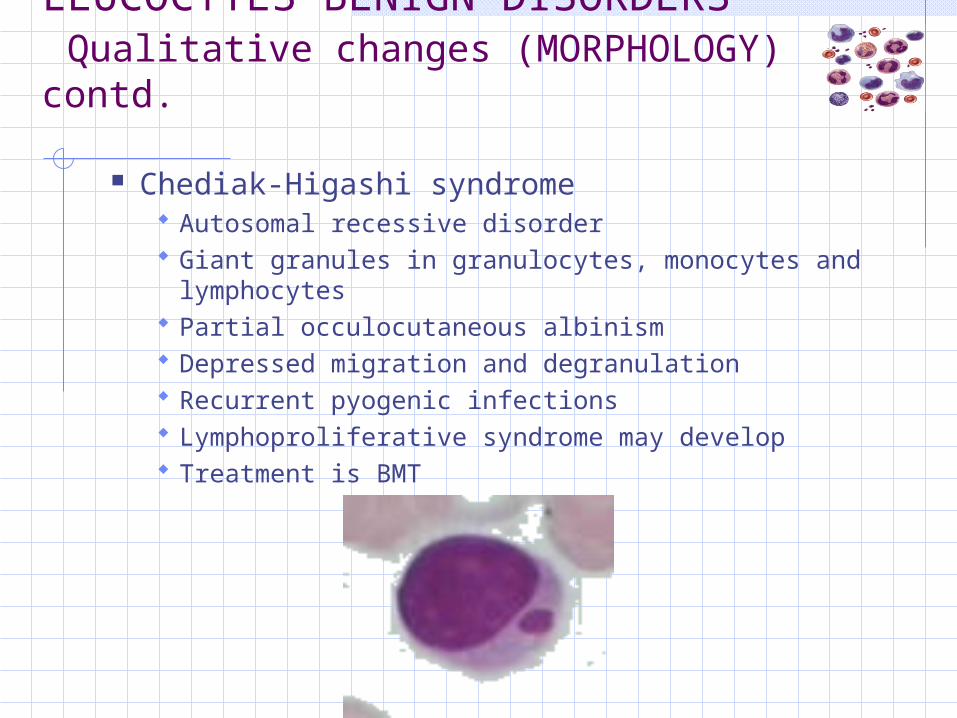
Chediak-Higashi syndrome Autosomal recessive disorder Giant granules in granulocytes, monocytes and
lymphocytes Partial occulocutaneous albinism Depressed migration and degranulation Recurrent pyogenic infections Lymphoproliferative syndrome may develop Treatment is BMT

LEUCOCYTES BENIGN DISORDERS Qualitative changes (MORPHOLOGY) contd.
Acquired Toxic granulation Dohle bodies Pelger cells Hypersegmented neutrophils

LEUCOCYTES BENIGN DISORDERS Qualitative changes (FUNCTIONAL)
Leucocyte adhesion deficiencyChronic granulomatous diseaseChediak-Higashi syndromePrimary immunodeficiency
Severe combined immunodeficiency Common variable immunodeficiency Isolated IgA deficiency T-cell immunodeficiency Thymic aplasia (Di George syndrome)
