lessons from three mile island: lessons from big industrial accidents and their relevance for the...
TRANSCRIPT
Lessons from TMI Lessons from big industrial accidents and
their relevance for the Pharma industry
ARETE-ZOE, LLC
Registered address: 1334 E Chandler Blvd 5A-19, Phoenix 85048 AZ, USA
Solutions to complex problems in the high stakes and high consequence environment
of Global Pharmaceuticals, including clinical research, healthcare informatics, and
public health. We blend established, Pharma sector methodologies, innovation, and
adaptations/transfers from other sectors to identify and resolve consequential
practices that pose risk and often result in avoidable patient casualty.
Three Mile Island, PA, USA
(1979)

Reactor
Cadmium
rods
Steam
generator
Cooling
circuit

Turbines
Steam pipes

03:58 AM, March 28, 1979
Routine repair of clogged filter
Trace of water left inside air circuit
Alarms went off
…causing confusion in the operating room

Computers interpreted “water in air
system” as “dangerous invader” and
shut down the pumps in cooling circuit

Steam generator Nuclear reactor
Pumps in cooling circuit shut down Why: Misinterpreted information from the air circuit
Consequence: Cooling system disabled, reactor heating up
Operators faced situation they
were not trained for and was
not covered by their procedures
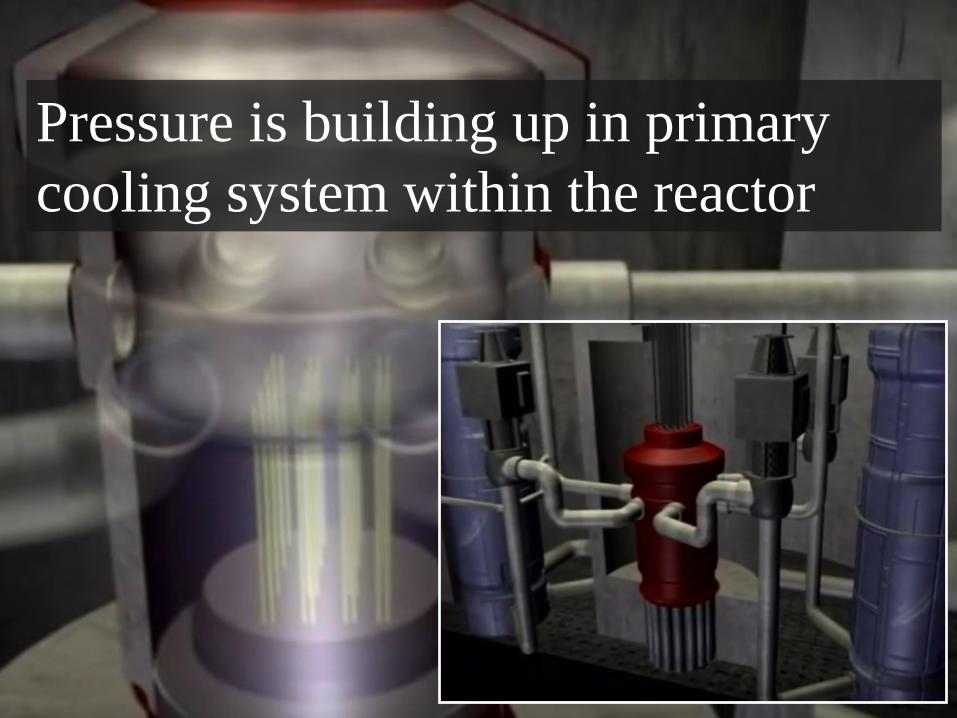
Pressure is building up in primary
cooling system within the reactor
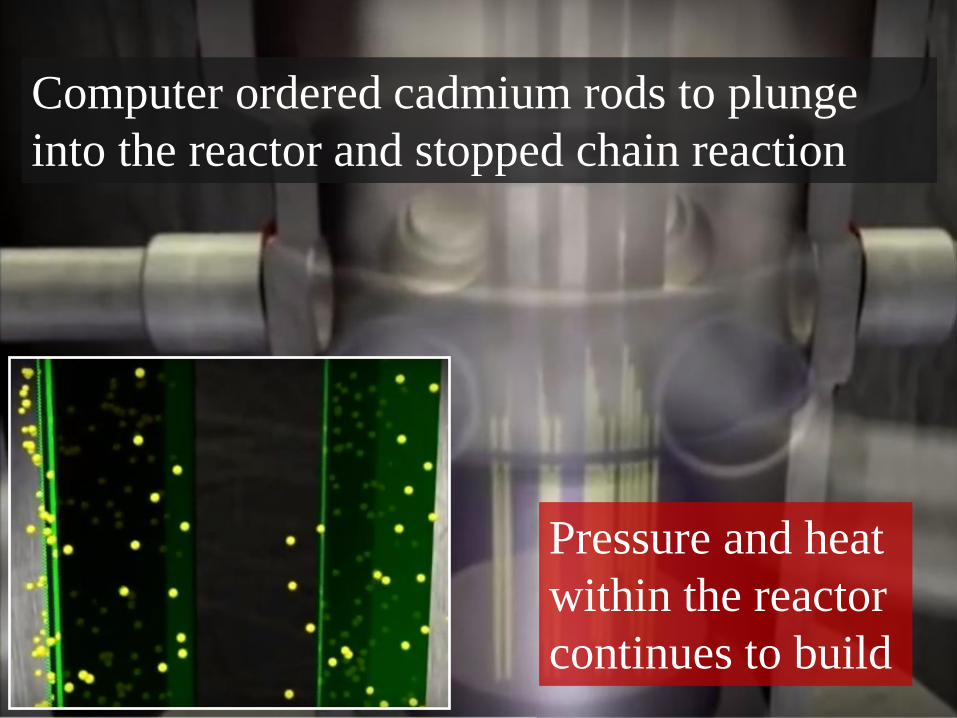
Computer ordered cadmium rods to plunge
into the reactor and stopped chain reaction
Pressure and heat
within the reactor
continues to build
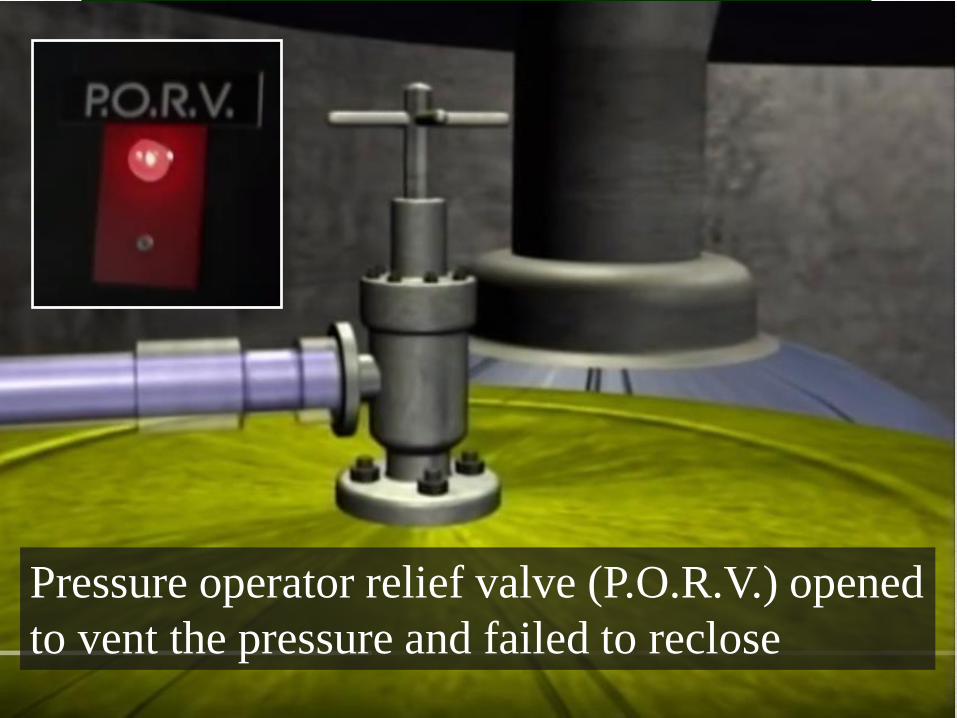
Pressure operator relief valve (P.O.R.V.) opened
to vent the pressure and failed to reclose
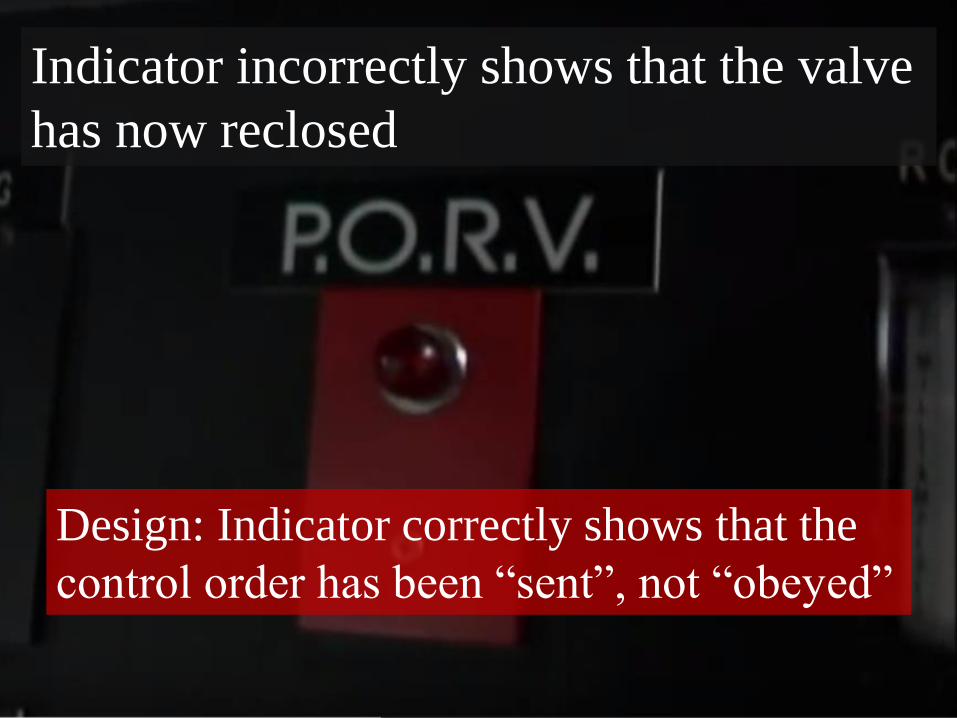
Indicator incorrectly shows that the valve
has now reclosed
Design: Indicator correctly shows that the
control order has been “sent”, not “obeyed”

Surrogate endpoint
In clinical trials, a surrogate endpoint (or marker) is a
measure of effect of a specific treatment that may correlate
with a real clinical endpoint but does not necessarily have
a guaranteed relationship.
Disease Surrogate
endpoint
True clinical
endpoint
Intervention
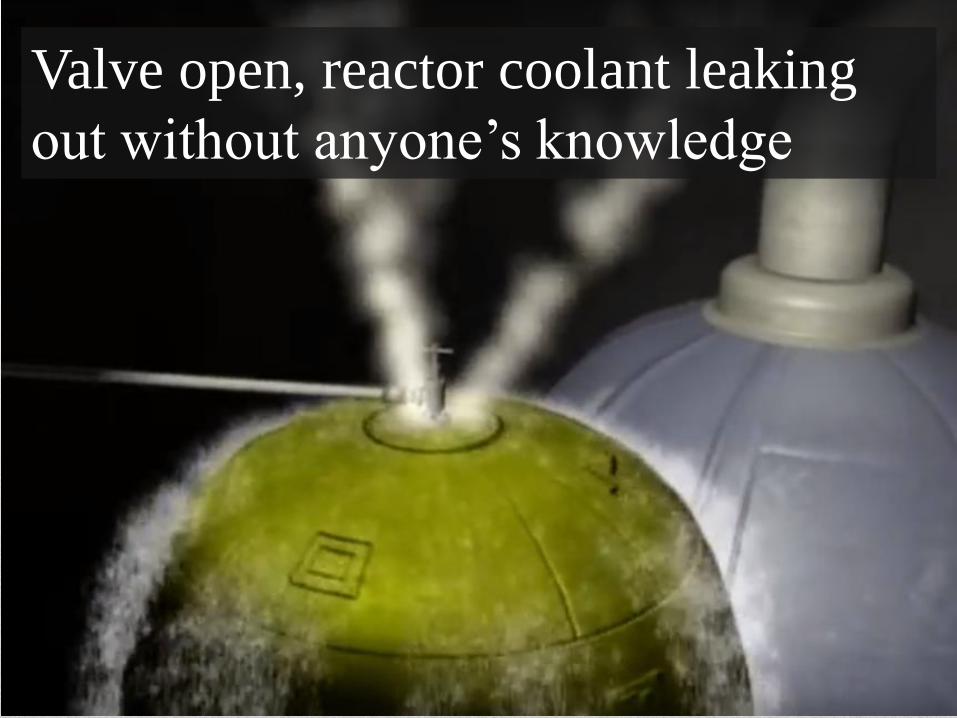
Valve open, reactor coolant leaking
out without anyone’s knowledge

Stuck valve undetected Why: Misinterpreted information from indicators
Consequence: cooling system disabled, reactor heating up

Communication failure Single phone line in the operating room
Key people unable to get through
1

Overheated reactor Incorrect readings from instruments
Volume of coolant measured indirectly
Decision: to turn off reactor pumps
Incorrect conclusions
Loss of trust in the instruments
System did not behave as expected
OB
SE
RV
E
OR
IEN
T
DE
CID
E
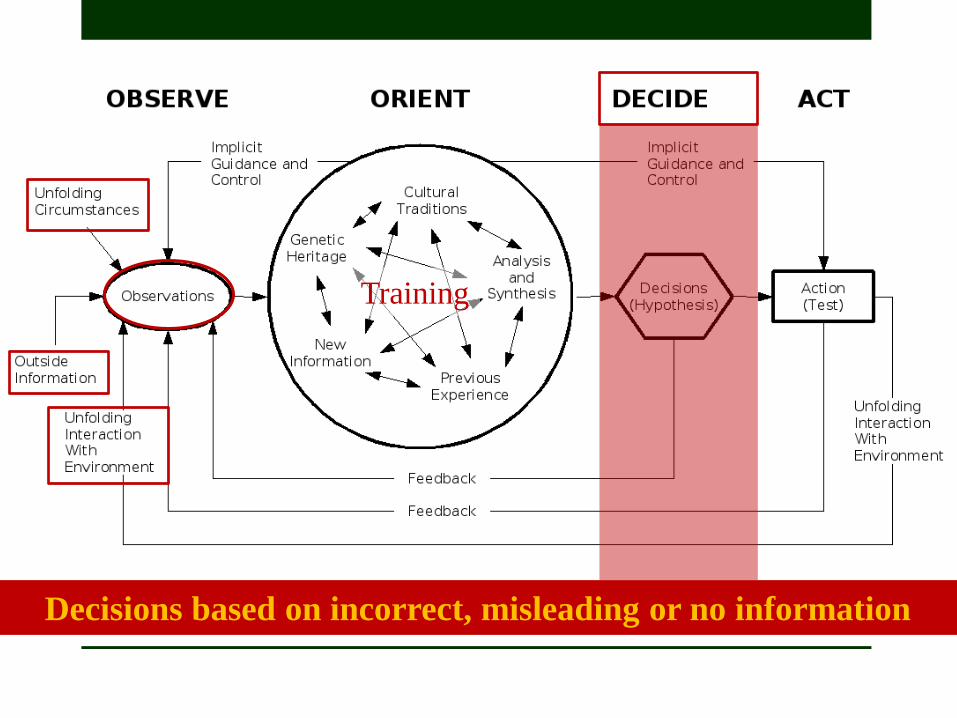
Training
Decisions based on incorrect, misleading or no information
7:15 AM stuck valve finally discovered Pumps were finally restarted Reactor still overheating
Misleading temperature readings
Why: Instruments not designed for temperatures this high
Radiation in operating room
Mounting pressure
8:33 AM – General emergency Misleading and deceptive information provided to
the public by the company
Minimum information provided to state
administration and regulators
Partial evacuation within 5 mile radius
Freedom of speech, anyone?
U.S. v. Caronia
Amarin v. FDA
Not an issue during TMI
Real concern now in off-label
promotion (Must be “truthful”)
Reactor cracked
Sample of contaminated coolant
Basement full of contaminated water Radioactive gas was eventually released into the atmosphere
Oh, BTW, it can
blow up because
of accumulated
hydrogen
Fierce dispute within the NRC whether this can happen or not
This risk did not materialize. Partial reactor meltdown did not
result in any additional release of radiation.

Complex combination of minor equipment failures
and major inappropriate human actions
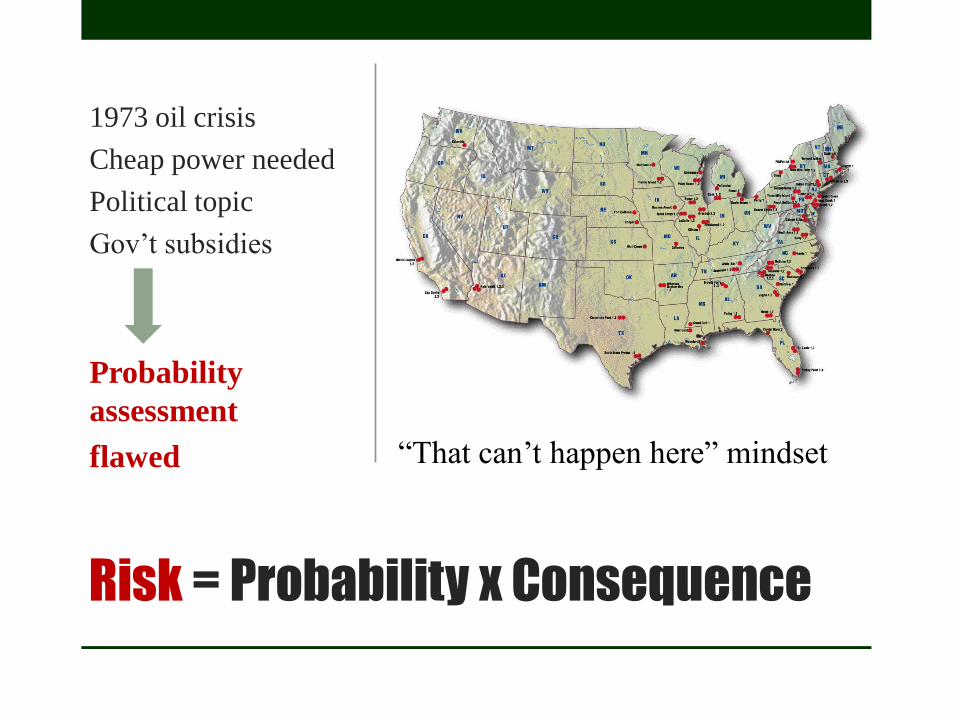
Risk = Probability x Consequence
1973 oil crisis
Cheap power needed
Political topic
Gov’t subsidies
Probability
assessment
flawed “That can’t happen here” mindset
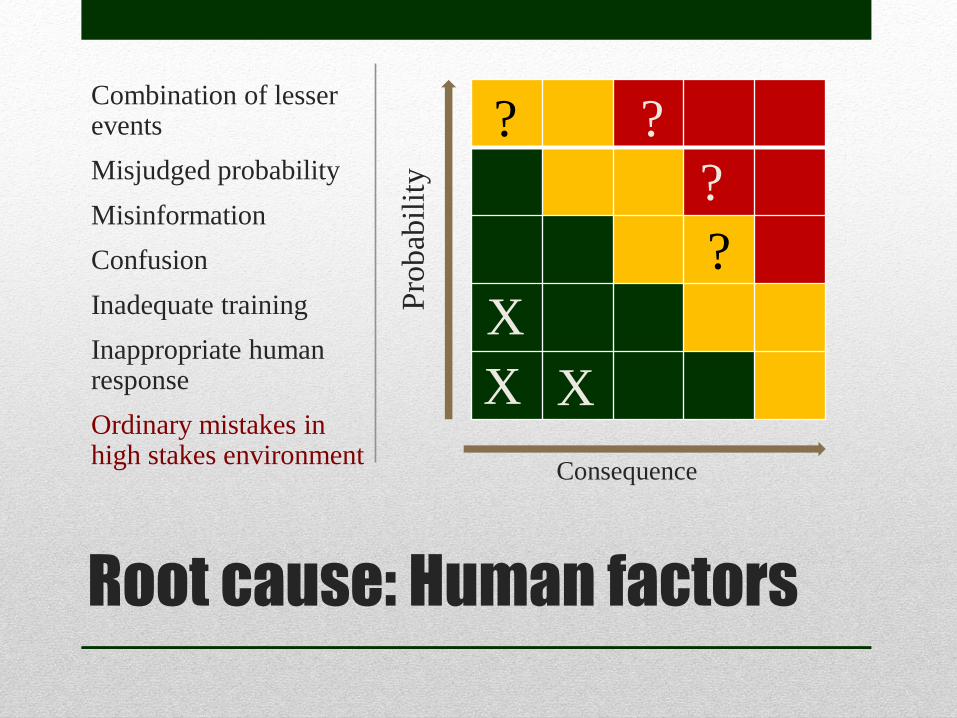
Root cause: Human factors
Combination of lesser events
Misjudged probability
Misinformation
Confusion
Inadequate training
Inappropriate human response
Ordinary mistakes in high stakes environment
Pro
bab
ilit
y
Consequence
X
X X
?
?
?
?
The need for change
RECOMMENDATIONS
Fundamental changes in
• Organizational procedures and
practices
• The attitude of regulators
• Operator training, updates
• Emergency response and planning
Organization failed to learn
from previous failures
The need for change
RECOMMENDATIONS
• More attention to human factors
• Combination of lesser events
(slower to develop, more likely)
• Training, fitness for duty
• Organizational structure
• Communication
Focus on equipment safety
and large break accidents
Compliance v. Safety culture
“It is the responsibility of the NRC to issue regulations to
assure the safety of nuclear power plants. However,
regulations alone cannot assure safety. Once regulations
become as voluminous and complex as those now in place,
they can serve as a negative factor in nuclear safety. The
complexity requires immense efforts to assure compliance.
Requirement v. Consequence
The satisfaction of regulatory requirements is
equated with safety.
• Focus on compliance with regulations
instead of intrinsic system safety
• Inspection manual voluminous and
complex – unclear to many inspectors
• Enforcement actions limited/unused
• Reliance on industry own data
• No systematic evaluation of patterns
• Unclear Roles & Responsibilities
The role of regulators
NRC has erred on the side of
the industry's convenience
rather than its primary
mission of assuring safety
The role of regulators
HUMAN FACTORS Fiduciary responsibilities of
public servants

Worst problem:
Loss of public trust
• Misinformation
• Deception
• Misunderstanding
• Fear & Confusion

Outcome
Transformation of
the industry
Major regulatory
reform
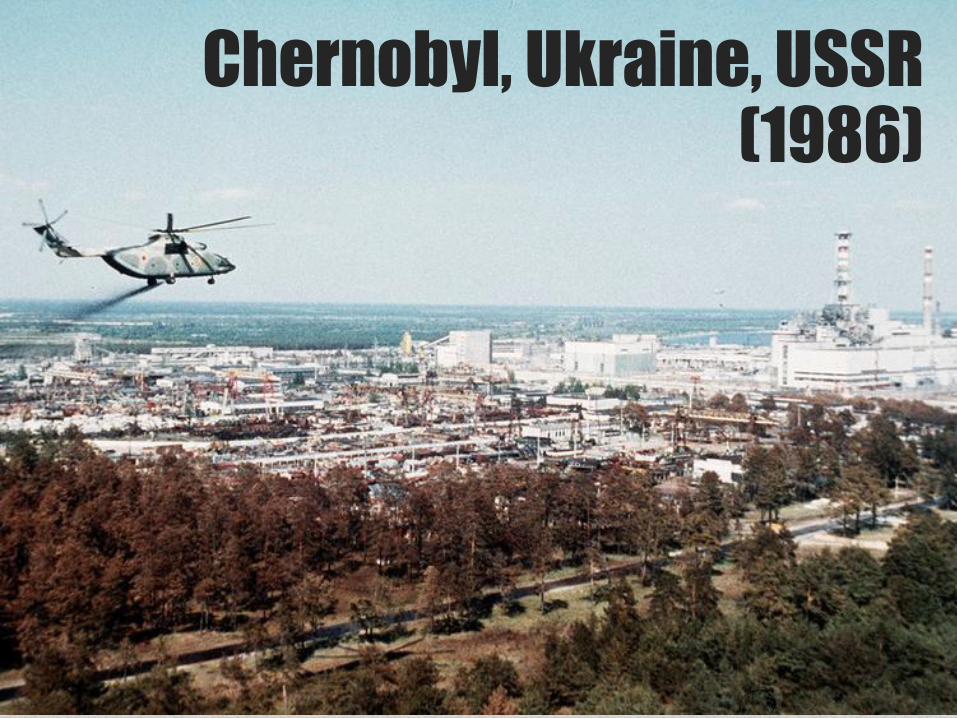
Chernobyl, Ukraine, USSR (1986)
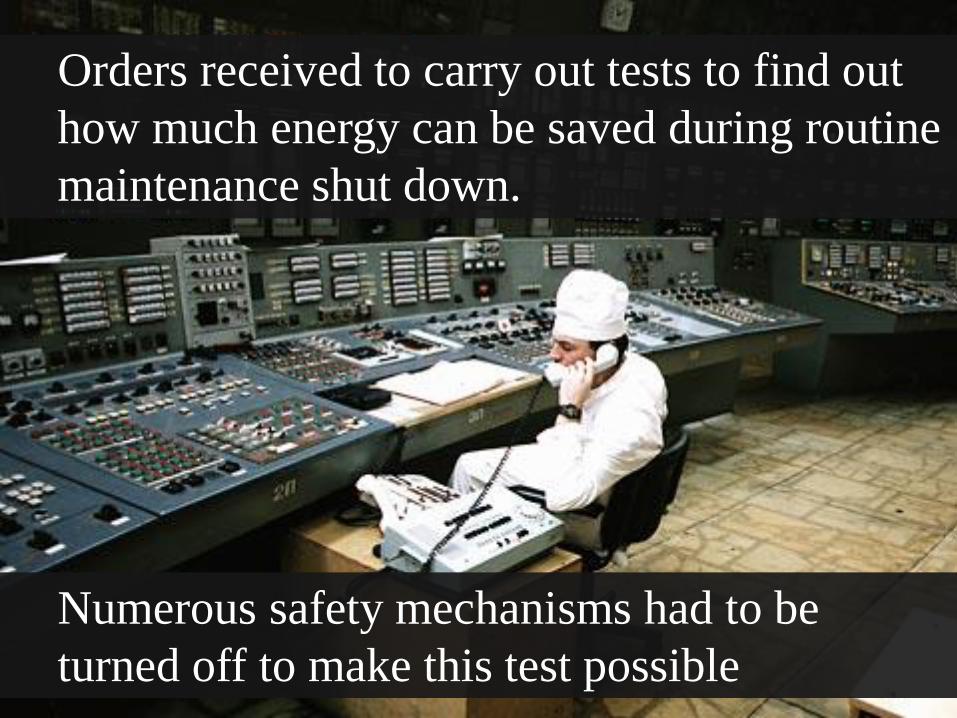
Orders received to carry out tests to find out
how much energy can be saved during routine
maintenance shut down.
Numerous safety mechanisms had to be
turned off to make this test possible

Power levels lowered
to perform tests
Emergency core
cooling system shut off
Operator failed to program computer
to prevent power from dropping
below minimum safe level
Automatic scram
devices an alarms
switched off
Control
rods
withdrawn
too far to
reinsert
quickly
= Bad idea = Very bad idea
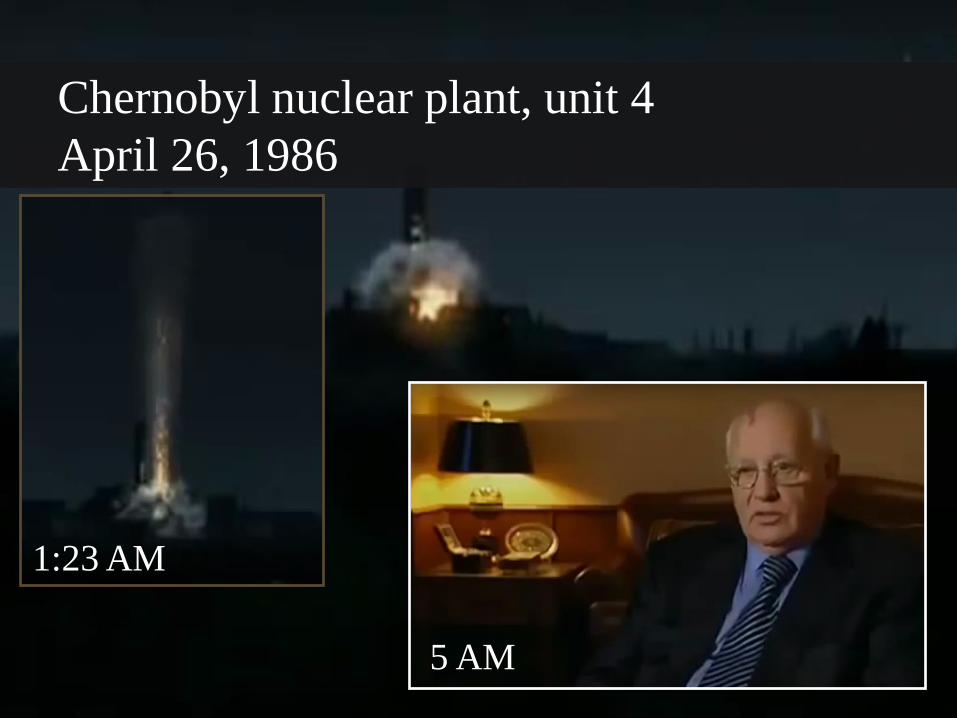
Chernobyl nuclear plant, unit 4
April 26, 1986
5 AM
1:23 AM
Systemic factors
Long record of sometimes fatal accidents
ACCIDENT WAITING TO HAPPEN
National 5-year production goals oblivious to reality
Training often suspect and shoddy
Lax observance of rules and regulations
Causes of
disaster
Irresponsibility
Negligence
Indiscipline Flawed performance metrics
HUMAN FACTORS
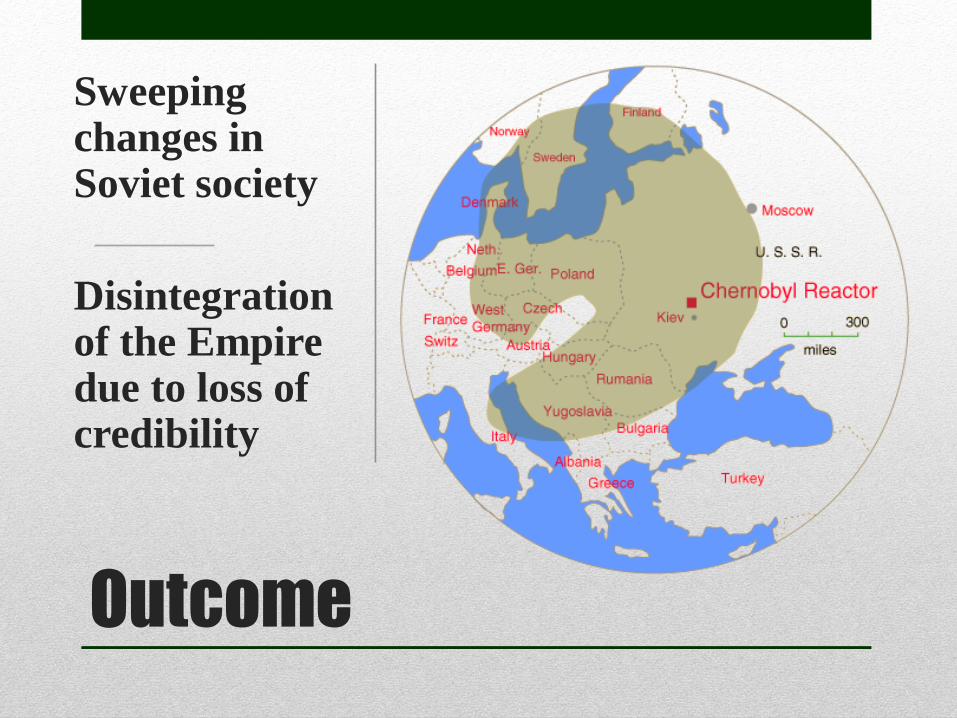
Outcome
Sweeping changes in Soviet society
Disintegration of the Empire due to loss of credibility
Volkswagen, Germany
(2015)
Martin Winterkorn, CEO of Volkswagen, AG acknowledged that 11 million vehicles were equipped with
diesel engines with defeat devices to cheat pollution tests


…And spreading
Criminal probe
underway

Root cause
Cause entirely
internal
Flawed
performance
metrics VW very sensitive to its own image
Internal pressures to improve metrics
caused someone to manipulate the system –
in a manner that amounted to conspiracy
Lessons learned?
Behavior of organizations follows the same
principles regardless industry
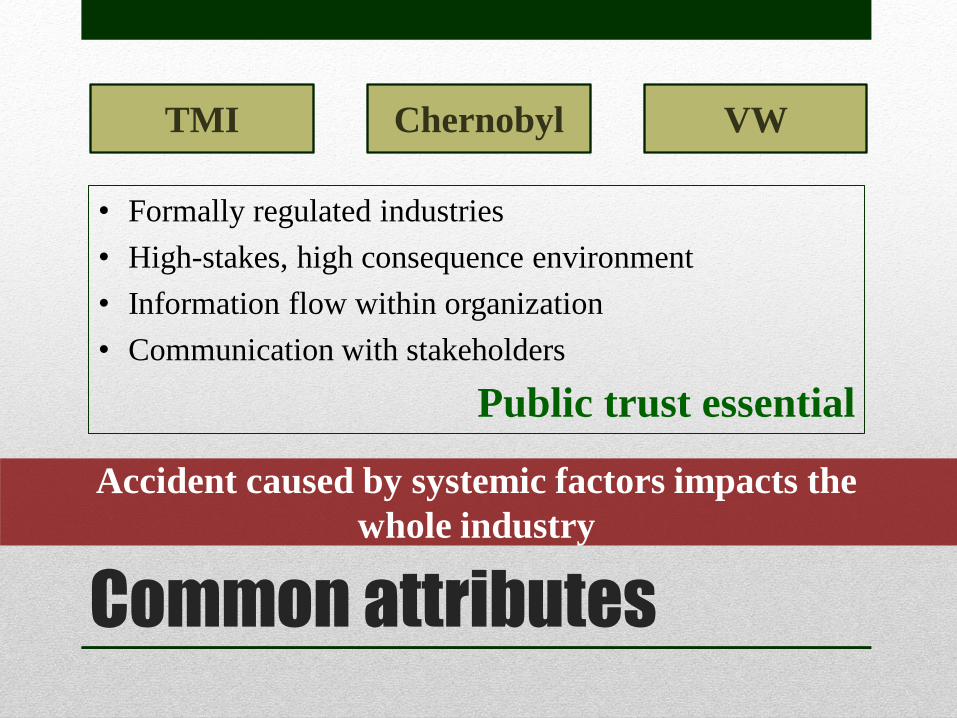
Common attributes
• Formally regulated industries
• High-stakes, high consequence environment
• Information flow within organization
• Communication with stakeholders
Public trust essential
TMI VW Chernobyl
Accident caused by systemic factors impacts the
whole industry
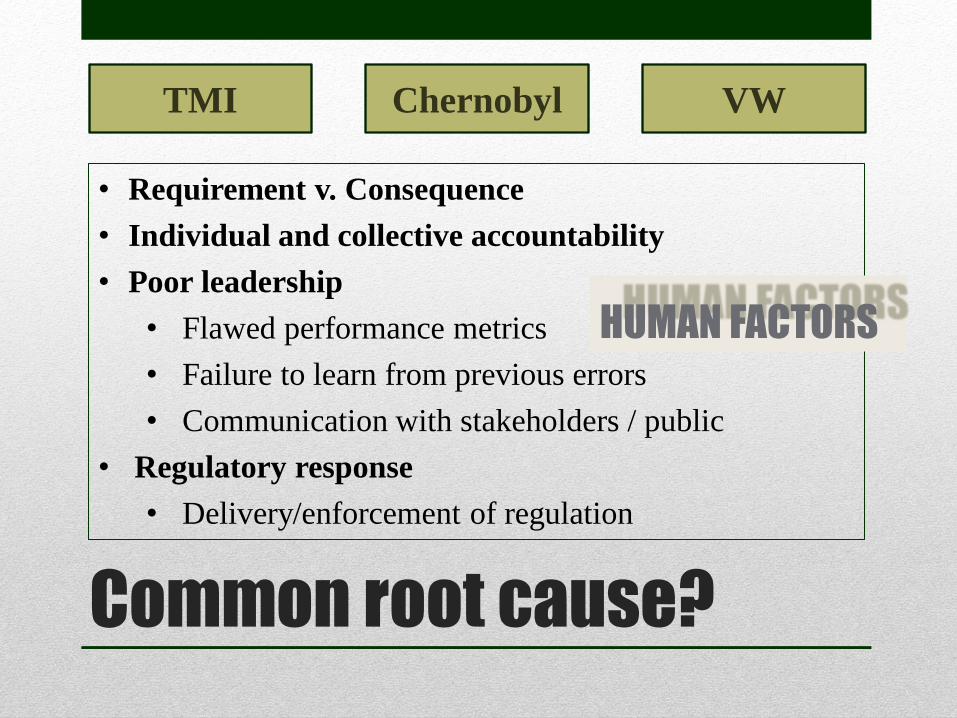
Common root cause?
• Requirement v. Consequence
• Individual and collective accountability
• Poor leadership
• Flawed performance metrics
• Failure to learn from previous errors
• Communication with stakeholders / public
• Regulatory response
• Delivery/enforcement of regulation
TMI VW Chernobyl
HUMAN FACTORS
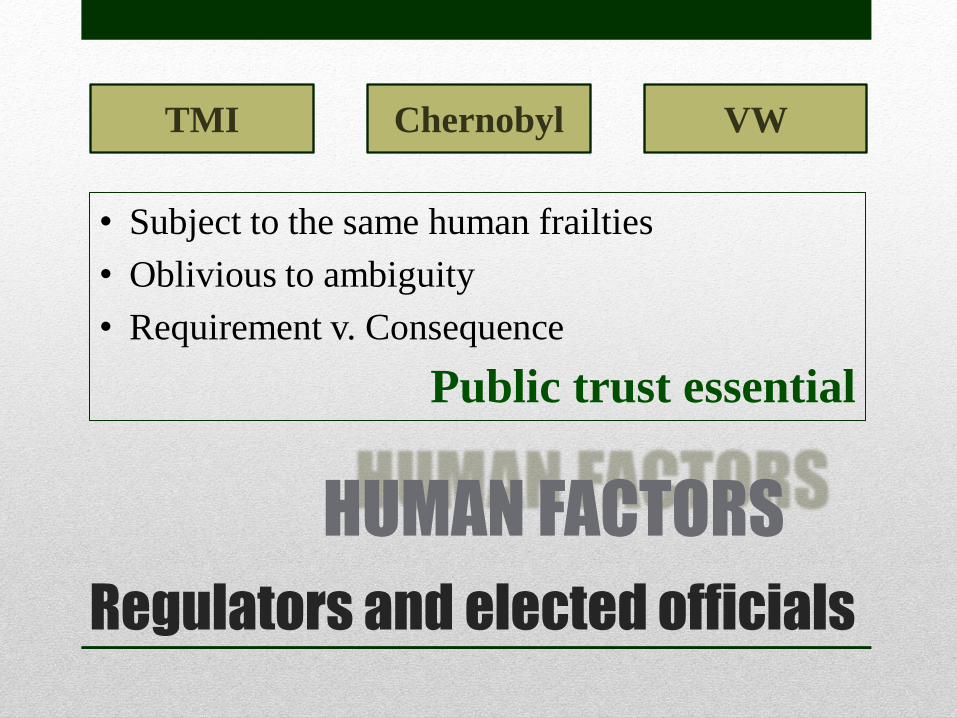
Regulators and elected officials
• Subject to the same human frailties
• Oblivious to ambiguity
• Requirement v. Consequence
Public trust essential
TMI VW Chernobyl
HUMAN FACTORS

HUMAN FACTORS
Experience, training, education
Capabilities Demographics Frailties Values
Organizational culture
Reporting structure
Leadership
EN
VI
RO
NM
EN
T
Ethical
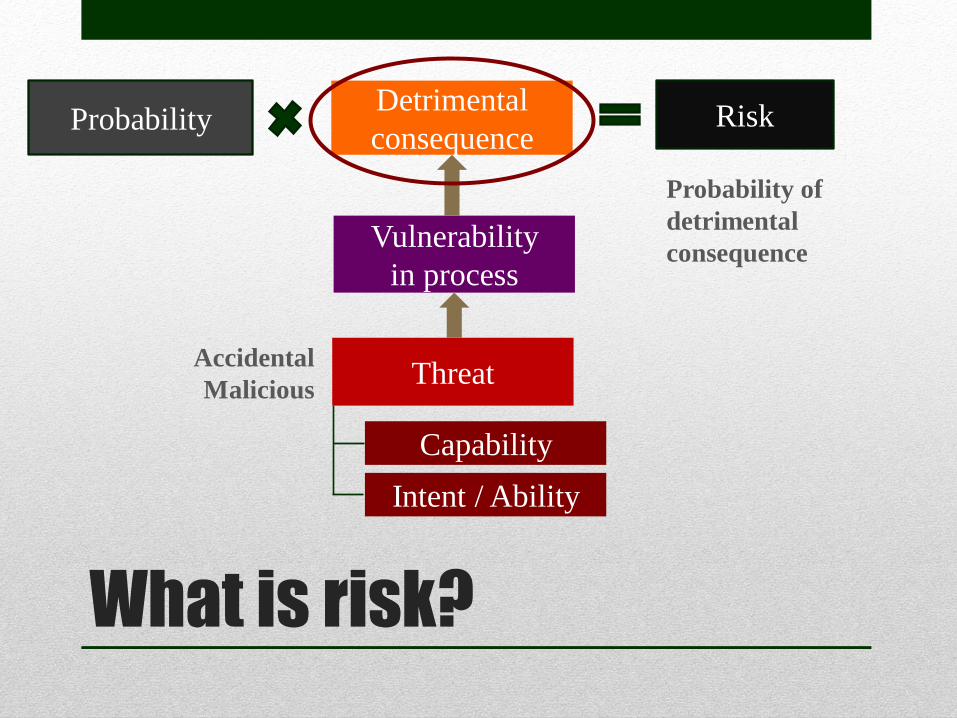
What is risk?
Probability of
detrimental
consequence
Risk
Vulnerability
in process
Probability
Threat
Capability
Intent / Ability
Detrimental
consequence
Accidental
Malicious
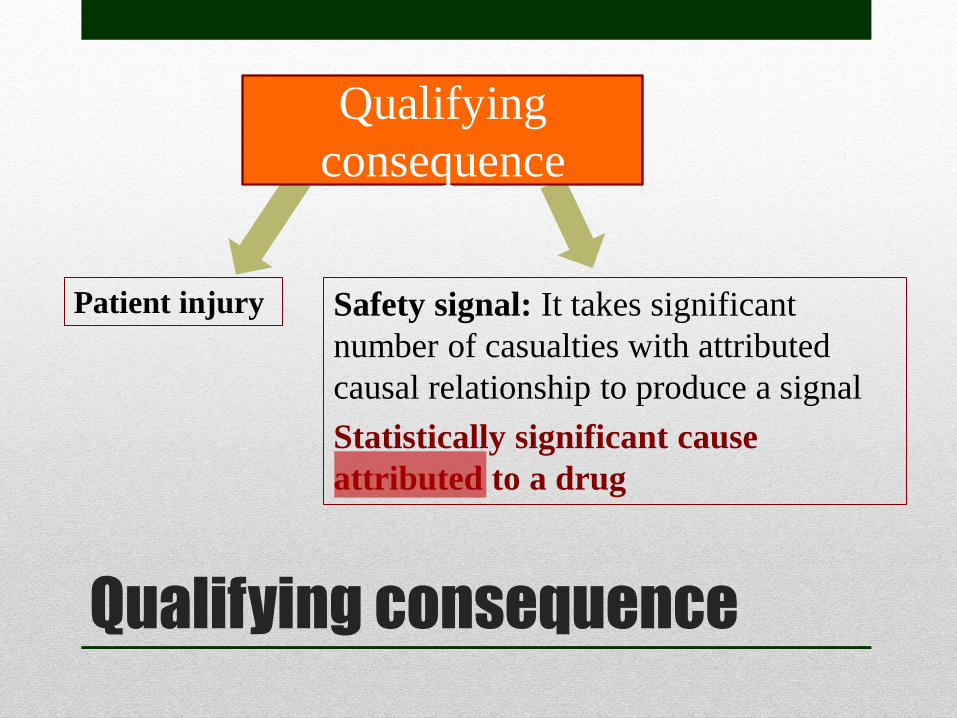
Qualifying consequence
Safety signal: It takes significant
number of casualties with attributed
causal relationship to produce a signal
Statistically significant cause
attributed to a drug
Patient injury
Qualifying
consequence

Attribution
Dispensing error / incorrect substitution)
Non-compliance with treatment
Self-medication (OTC, Rx, illicit)
Atypical manifestation of disease
Misdiagnosis
Prescribing error
Wrong dose (predictable, unpredictable)
Individual variability in response
Misleading information on drug
Drug interactions (known, unknown)
Off-label use (appropriate, inappropriate)
Counterfeit medications
Limitation of science
Honest mistake
Omission
Commission
Deception
False Claim
PATIENT INJURY
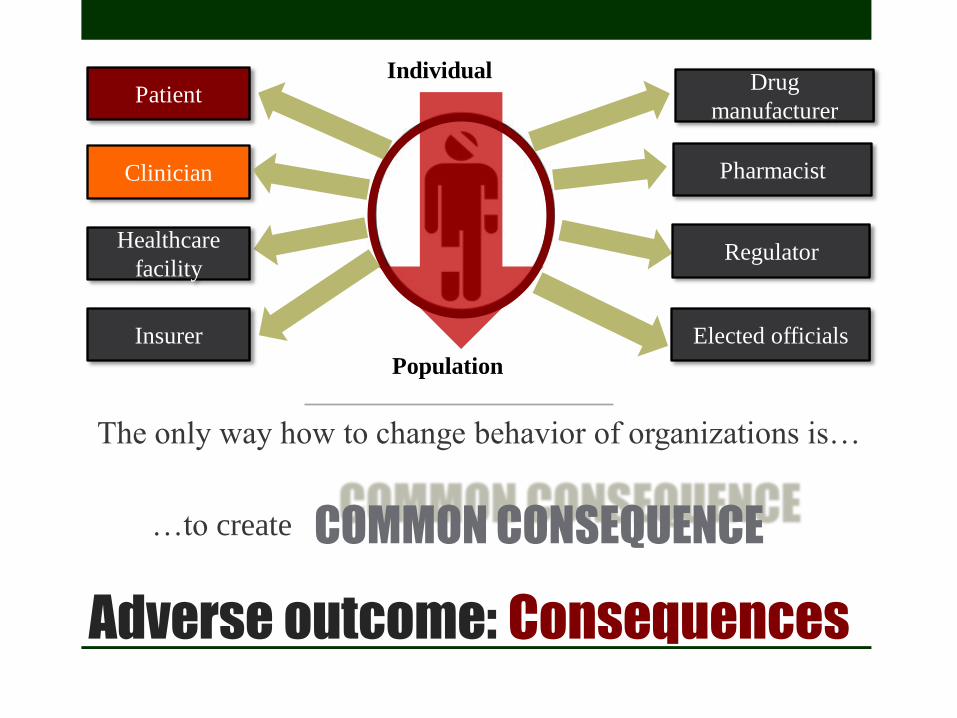
Adverse outcome: Consequences
Patient
Clinician Pharmacist
Regulator
Drug
manufacturer
Healthcare
facility
Insurer Elected officials
Individual
Population
COMMON CONSEQUENCE
The only way how to change behavior of organizations is…
…to create
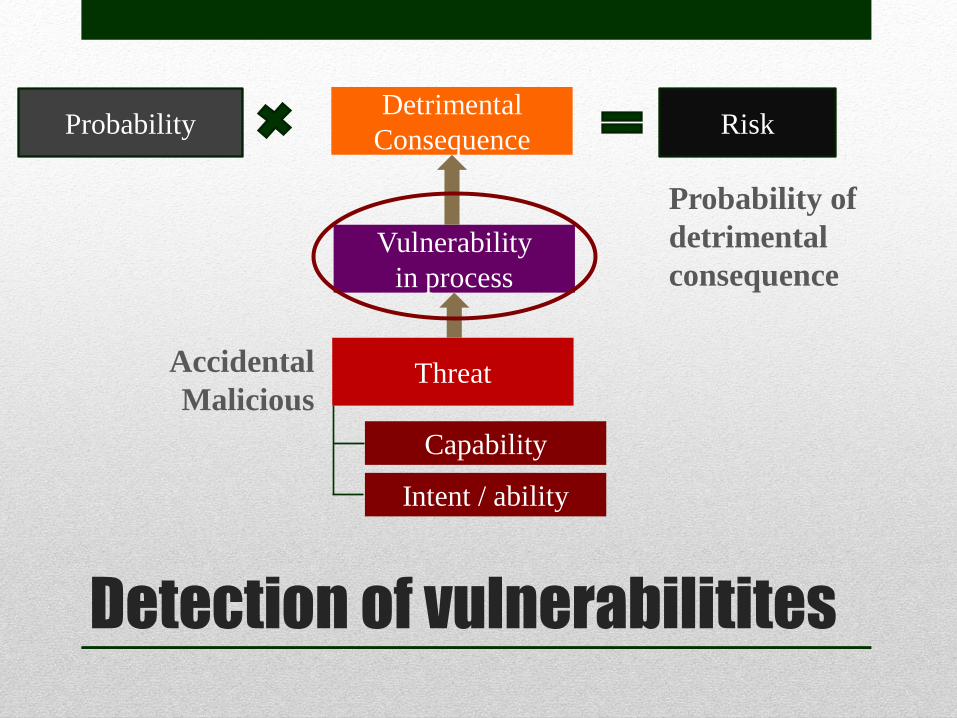
Detection of vulnerabilitites
Probability of
detrimental
consequence
Risk
Vulnerability
in process
Probability
Threat
Capability
Intent / ability
Detrimental
Consequence
Accidental
Malicious
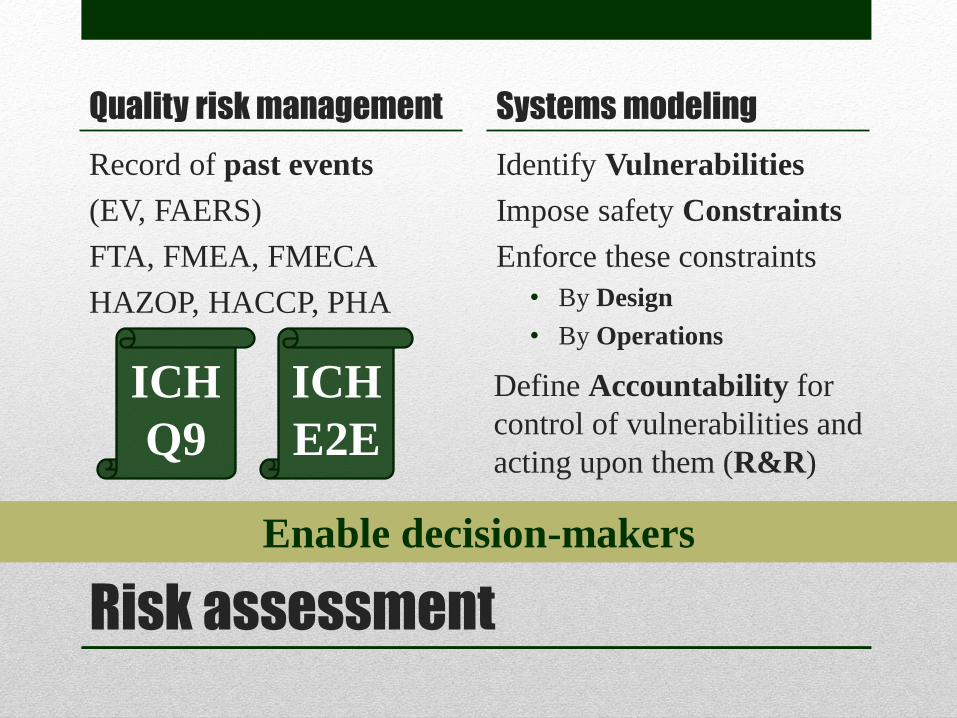
Quality risk management
Record of past events
(EV, FAERS)
FTA, FMEA, FMECA
HAZOP, HACCP, PHA
Systems modeling
Identify Vulnerabilities
Impose safety Constraints
Enforce these constraints
• By Design
• By Operations
Risk assessment
ICH
Q9
ICH
E2E
Define Accountability for
control of vulnerabilities and
acting upon them (R&R)
Enable decision-makers

Systems theoretic accident
process and modeling (STAMP)
Imposing constraints on a system whilst ensuring
enforceability of these constraints by design and operations
Human supervisor
(Controller)
Model of
process
Model of
automation
Automated Controller
Model of
process
Model of
interfaces
Controlled
process
Sensor
Displays
Controls
Process inputs
Disturbances
Process outputs Actuators Controlled
variables
Measurable
variables
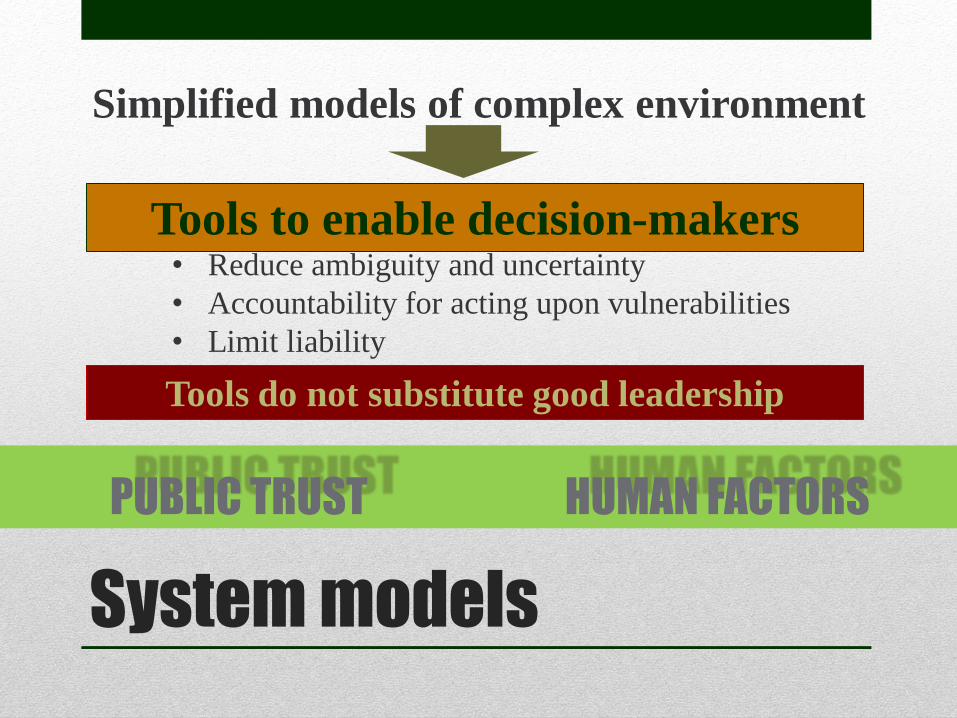
System models
Simplified models of complex environment
Tools to enable decision-makers • Reduce ambiguity and uncertainty
• Accountability for acting upon vulnerabilities
• Limit liability
HUMAN FACTORS
Tools do not substitute good leadership
PUBLIC TRUST

Training
Correct input – accurate and timely orientation

Download presentation
Thank you