leiomyomas of the lower respiratory tract - thorax.bmj.com · leiomyomasofthe lowerrespiratory...
TRANSCRIPT

Thorax 1985;40:306-31 1
Leiomyomas of the lower respiratory tract
SH WHITE, NBN IBRAHIM, CP FORRESTER-WOOD, K JEYASINGHAM
From the Departments of Thoracic Surgery and Pathology, Frenchay Hospital, Bristol
ABSTRACr Leiomyomas account for about 2% of benign tumours of the lower respiratory tract.
From the relatively few cases reported in the literature, it appears that these tumours most
commonly occur in the fourth decade, although one third of patients are under the age of 20years. The distribution of leiomyomas favours the distal part of the tracheobronchial tree and themost common site for tracheal lesions is the membranous portion of the lower third. Over 90% ofpulmonary parenchymal leiomyomas, which themselves are more common in women, are inci-dental findings on chest radiographs whereas bronchial lesions are important causes of irrevers-ible lung damage. Tracheal lesions may present as bronchial asthma. Accurate early diagnosisrests on a high index of clinical suspicion and histological examination of bronchoscopic biopsyspecimens or frozen section material obtained at exploratory thoracotomy. Treatment could beconservative surgery, but 65% of reported cases have been managed by lobectomy or
pneumonectomy as a result of advanced irreversible lung disease or unawareness of the benignnature of the lesion.
Several individual and collected case reports ofleiomyoma of the lung,' 2 bronchus,34 and trachea56have been published. Such tumours are rare, and sofar only 65 cases have been reported.'1'3 In thisarticle we report three cases of leiomyoma of thelower respiratory tract, which illustrate the three dis-tinct anatomical varieties-namely parenchymal,bronchial, and tracheal leiomyomas.
Case reports
CASE 1A 54 year old man was admitted for investigation inNovember 1983. One year previously he had had anepisode of bilateral pneumonia and left ventricularfailure, for which he was treated at another hospital.He made a complete recovery but follow up chestradiographs showed a persistent right hilar shadow.There was no other important past medical historyand his only medication was digoxin. On admissionhe was mildly obese but there were no abnormalcardiovascular or respiratory symptoms or signs.Lung function studies showed a vital capacity of3.43 litres and an FEV, of 2.73 1. Conventional
Address for reprint requests: Dr Nassif BN Ibrahim, Departmentof Histopathology, Frenchay Hospital, Bristol BS16 ILE.
Accepted 1984
anteroposterior tomograms showed a peribronchialopacity in the upper part of the right hilum, bestdefined at 14 cm from the plate.
Bronchoscopy showed diffuse inflammation justdistal to the bifurcation of the right main bronchusand narrowing at the origin of the right upper lobebronchus. The intersegmental carinae in the upperlobe bronchus were widened, suggesting an extra-bronchial lesion. Bronchial brushing smears showedno malignant cells and bronchial biopsy showed noevidence of tumour.
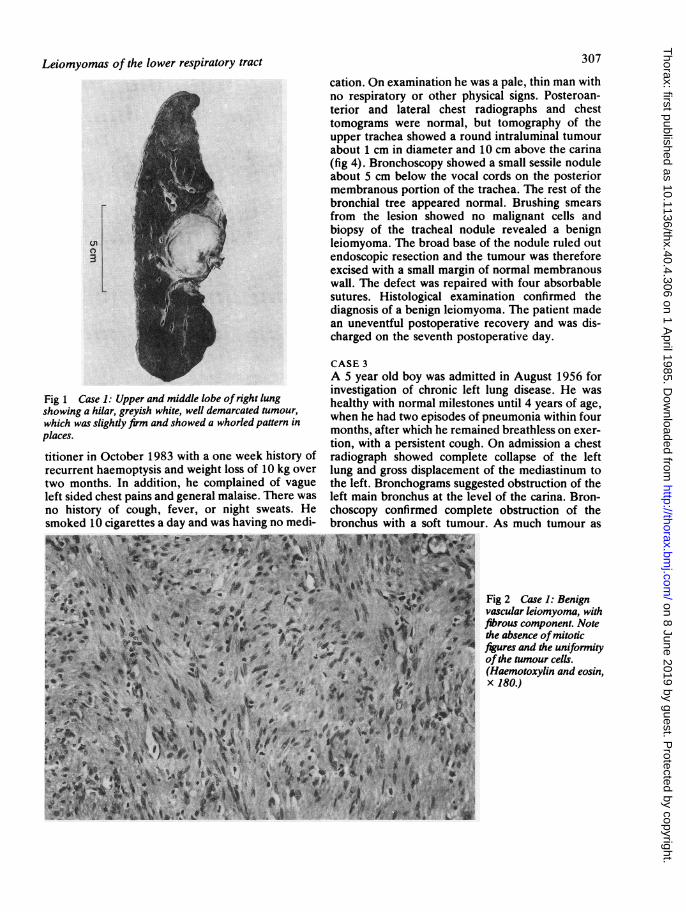
With a presumptive diagnosis of bronchogeniccarcinoma the patient underwent a right exploratorythoracotomy. The lung was found to contain a largerounded mass arising in the parenchyma of theupper lobe at its junction with the hilum (fig 1),which was well defined but adherent to the sur-rounding structures, including the phrenic nerve,superior vena cava, and azygos vein. When thelesion had been separated from these structures bydissection, a biopsy was obtained and histologicalexamination of a frozen section showed a vascularleiomyoma, the diagnosis being later confirmed byexamination of a paraffin section (fig 2) and by elec-tron microscopy of the resected lesion (fig 3). Thepostoperative course was uneventful and he was dis-charged on the 1 th postoperative day.
CASE 2A 46 year old man was referred by his medical prac-
306
on 8 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.40.4.306 on 1 April 1985. D
ownloaded from
307Leiomyomas of the lower respiratory tract
Fig 1 Case 1: Upper and middle lobe ofright lungshowing a hilar, greyish white, well demarcated tumour,which was slightly finn and showed a whorled pattern inplaces.
titioner in October 1983 with a one week history ofrecurrent haemoptysis and weight loss of 10 kg overtwo months. In addition, he complained of vagueleft sided chest pains and general malaise. There wasno history of cough, fever, or night sweats. Hesmoked 10 cigarettes a day and was having no medi-
cation. On examination he was a pale, thin man withno respiratory or other physical signs. Posteroan-terior and lateral chest radiographs and chesttomograms were normal, but tomography of theupper trachea showed a round intraluminal tumourabout 1 cm in diameter and 10 cm above the carina(fig 4). Bronchoscopy showed a small sessile noduleabout 5 cm below the vocal cords on the posteriormembranous portion of the trachea. The rest of thebronchial tree appeared normal. Brushing smearsfrom the lesion showed no malignant cells andbiopsy of the tracheal nodule revealed a benignleiomyoma. The broad base of the nodule ruled outendoscopic resection and the tumour was thereforeexcised with a small margin of normal membranouswall. The defect was repaired with four absorbablesutures. Histological examination confirmed thediagnosis of a benign leiomyoma. The patient madean uneventful postoperative recovery and was dis-charged on the seventh postoperative day.
CASE 3A 5 year old boy was admitted in August 1956 forinvestigation of chronic left lung disease. He washealthy with normal milestones until 4 years of age,when he had two episodes of pneumonia within fourmonths, after which he remained breathless on exer-tion, with a persistent cough. On admission a chestradiograph showed complete collapse of the leftlung and gross displacement of the mediastinum tothe left. Bronchograms suggested obstruction of theleft main bronchus at the level of the carina. Bron-choscopy confirmed complete obstruction of thebronchus with a soft tumour. As much tumour as
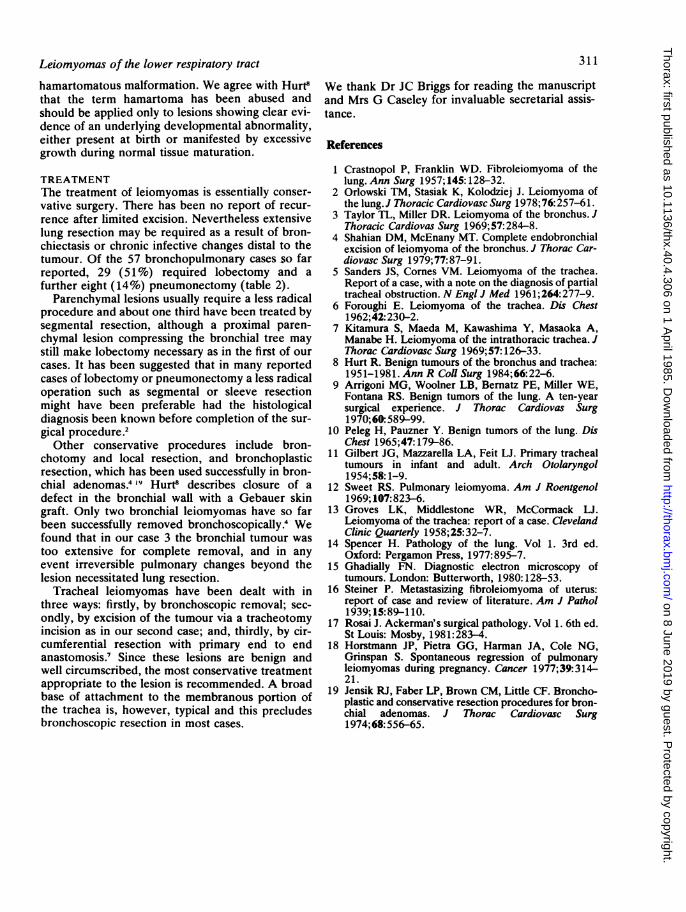
Fig 2 Case]1: Benigni ki, I vascular leiomyoma, with
2 'fibrous component. Notethe absence of mitotic
*,X,,figures and the uniformityof the tumour cells.(Haemotoxylin and eosin,
>}t:i :x=}jR x 180.)
on 8 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.40.4.306 on 1 April 1985. D
ownloaded from

White, Ibrahim, Forrester- Wood, Jeuyasingham
Fig 3 Case 1: Electron micrograph showing parts oftwo smooth muscle cells in apposition.Many myofdaments (M) with focal densities (oudined arrows), pinocytotic vesicles (longarrows), and dense plaques (arrow heads) are present. (Formalin fixed material, uranyl acetateand lead citrate, x 17 500.)
Fig 4 Case 2: Anteroposterior tomogram of tracheal inlet
showing a well circumscribed lesion. best seen in the 14 cm
cut.
Fig 5 Case 3: Collapsed left lung with considerablebronchiectasis due to the presence ofa whitish grey polypoidtumour arising in and completely obstructing the mainbronchus. Tongues oftumour tissue are extending into thelumina ofthe adjacentsegmental bronchi ofthe upper lobe.
308
,z6.il'.!:--..:!. -iia
on 8 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.40.4.306 on 1 April 1985. D
ownloaded from

Leiomyomas of the lower respiratory tract
possible was removed with biopsy forceps until thebronchial lumen was almost cleared. Histologicalexamination of the biopsy material showed featuresof a benign leiomyoma.
After bronchoscopy the patient began to expecto-rate pus. He continued to be febrile and his left lungfailed to re-expand. Repeat bronchoscopy threeweeks later showed further tumour, which appearedto be arising from the posterior wall of the left mainbronchus close to the upper lobe orifice. Histologicalexamination again showed fragments of aleiomyoma. Resection of the collapsed lung wasdecided on since the bronchus could not be clearedowing to the extent of the tumour.At thoracotomy in September 1956 the left lung
was completely atelectatic and adherent to the chestwall. A large mass was palpable at the hilum of theleft upper lobe. There was inflammatory enlarge-ment of the hilar lymph nodes. A left pneumonec-tomy was carried out (fig 5). Histological examina-tion showed a benign leiomyoma.The patient made an uneventful recovery, has
remained entirely symptom free, and is now a 33year old lecturer whose hobbies include cross coun-try running and football.
Discussion
INCIDENCEBenign tumours of the tracheobronchial tree com-prise 4% of all surgically excised tumours.Leiomyomas are extremely rare and only 65 caseshave so far been reported.'' 3 In a review of 128benign tumours excised at the North MiddlesexHospital during 30 years Hurt8 found only twoleiomyomas (one was of bronchial origin and theother was in the lung parenchyma); this parallels theexperience of Arrigoni et a19 at the Mayo Clinic,where only two leiomyomas (one bronchial and theother parenchymal) were encountered among 130benign tumours seen over a period of 10 years.
Peleg and Pauzner'° in Israel reviewed 34 benigntumours and added one to the existing publishedcases. These reviews indicate that leiomyomaaccounts for less than 2% of benign tumours of thelower respiratory tract. The trachea itself is the leastcommon site, for only 10 such cases have beenreported Gilbert et al" found only two leiomyomasin their review of 256 benign tumours of the trachea.
AGE AND SEXLeiomyomas are predominantly tumours of theyoung and the middle aged, with a mean age of 35years for bronchial and lung parenchymal lesions2and 40.6 years for tracheal lesions.5-7 The youngest
patient with a bronchial leiomyoma was the 5 year
309
old child reported here, and the youngest patientreported so far with a tracheal leiomyoma was a 3month old infant.6 One third of patients presentbefore the age of 20 years.2 The oldest patientreported was 67.5Leiomyomas of lung parenchyma occur twice as
often in females as males,2 whereas leiomyomas ofthe trachea have been reported more often inmales.6 Endobronchial lesions show no sex predilec-tion.4
SITE AND PRESENTATIONThese tumours are more often encountered in thedistal part of the tracheobronchial tree than proxi-mally (table 1). Only three of the 51 cases reviewedby Orlowski et a12 arose from the main stem bronchi.The commonest segment of the trachea to beaffected is the lower third and the usual site of originis the posterior membranous portion.56Over a third of leiomyomas are asymptomatic and
are incidental findings on routine chest radiographs.3This reflects the prevalence of peripheral and paren-chymal lesions for these are asymptomatic in over90% of cases.2 The presentation depends on thelocation of the tumour, its size, and changes in thelung distal to the lesion.
Patients with bronchial lesions all have symptomsdue to partial or complete obstruction of theaffected bronchus. These include wheeze, cough,chest pain, and fever, as a result of atelectasis, con-solidation, collapse, or bronchiectasis. Haemoptysisis common and may reflect lung damage or ulcera-tion of the surface of the lesion. With the risk ofrecurrent pneumonia and irreversible collapse of thelung, together with bronchiectasis and ultimate lungdestruction, as in case 3, there is a high premium oncorrect early diagnosis. Shahian and McEnany4reported a case of pneumothorax secondary to airtrapping beyond an endobronchial leiomyoma.
Intermittent or constant dyspnoea and wheezingare the most common symptoms of trachealleiomyoma and have been erroneously ascribed tobronchial asthma. The duration of asthma likesymptoms before correct diagnosis has been as longas nine years.7 Wheezing due to an obstructingtracheal tumour must be distinguished from bron-
Table 1 Reported cases ofleiomyoma ofthe lowerrespiratory tract*'-'3
Site No of %cases
Trachea 12 16Bronchus 22 33Parenchyma 34 51Total 68
*Including the three cases reported in this paper.
on 8 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.40.4.306 on 1 April 1985. D
ownloaded from

310
chial asthma in any patient irrespective of age.Leiomyomas may produce paroxysmal attacks ofwheezing, which are precipitated or relieved by a
change in position, and there is no response to bron-chodilator treatment. Other features includehaemoptysis, which is associated with asthmaticwheezing, and orthopnoea or paroxysmal nocturaldyspnoea in the absence of significant cardiovasculardisease. The characteristic appearances of the flowvolume loop of a patient with an obstructive lesionin the proximal bronchial tree distinguish an organicobstructive lesion from bronchial asthma.
INVESTIGATIONMost leiomyomas can be detected on plain chestradiographs but there are no pathognomonic fea-tures. Parenchymal tumours usually appear asrounded shadows but they cannot be distinguishedclearly from other benign, malignant, or metastaticlesions. Most authors stress that the presence ofcalcification within rounded shadows on a chestradiograph argues against malignancy, although thisis not a very reliable feature. In the two patients withleiomyomas reported by Crastnopol and Franklin'and Sweet'2 calcification was described. Nocalcification was seen in any of our cases.
Radiological features include the sequelae ofbronchial obstruction. The tumour may be obscuredby the features of atelectasis or pneumonitis. Hyper-lucency due to air trapping and even pneumothoraxhave been reported. Tracheal leiomyomas may beseen on plain radiographs of the thoracic inlet, espe-cially in the lateral view.'3Tomography is an excellent method of showing
tracheal lesions and is useful for delineatingleiomyomas in the rest of the bronchial tree. Theplace of computed tomography for evaluating thesetumours has yet to be explored. The absolute diag-nosis of leiomyomas of the lower respiratory tract is
by bronchoscopy, which gives direct visualisation,and biopsy material is sent for histological examina-tion. Frozen section is required, in the absence of a
preoperative tissue diagnosis, when an atypicaltumour is found at thoractomy. This obviatesunnecessary lung resection.
PATHOLOGYLeiomyomas of the trachea and bronchi arise fromthe smooth muscles of the tracheal and bronchialwall and grow as polypoid tumours, usually withbroad bases. Typically bronchial leiomyomas extendalong the bronchial lumen for a considerable dis-tance, as tongues of soft tissue.'4 While tracheal andbronchial leiomyomas are very cellular neoplasms,with minimal vascular or stromal fibrous compo-nent, parenchymal lung tumours tend to be of a
White, Ibrahim, Forrester- Wood, Jeuyasingham
Table 2 Surgically excised leiomyomas ofthe lowerrespiratory tract*' -13
Extent of No of Sresection cases
Pneumonectomy 8 14%Lobectomy 29 51%Segmentectomy 12 21%Open local excision 2 4%Bronchoscopic local
excision 3 5%Unspecified 3 5%
*Including the three cases reported in this paper.
more fibrous consistency and macroscopically have awhorled appearance. Histological examination ofparenchymal pulmonary leiomyomas show them toconsist largely of smooth muscle fibres, although anappreciable fibrous and vascular component is usu-ally present. These lesions may be difficult to dif-ferentiate from fibromas, neurofibromas, orneurilemomas with ordinary haematoxylin and eosinstains. Special stains or electron microscopic exami-nation may be required to establish their smoothmuscle origin.4 '5 Pulmonary leiomyomas arethought to arise from the smooth muscle of thebronchi, bronchioles, or blood vessels.4Of particular interest is the fact that the histologi-
cal appearances of parenchymal leiomyoma closelymimic those of the uterine fibroid. On rare occasionspulmonary tumours with features of benignfibroleiomyomas were shown to be metastaticdeposits from uterine "fibroids" of an apparentlybenign and well differentiated nature.'4 In describ-ing these cases, Steiner'6 coined the term "metas-tasising fibroleiomyoma of the uterus." There isconsiderable controversy about whether the pulmo-nary nodules represent metastases from anextremely well differentiated leiomyosarcoma ormulticentric benign leiomyomatous growth.'7 It maybe unjustifiable'4 to diagnose an intrapulmonaryfibroleiomyoma in the absence of a complete exami-nation of the uterus to exclude a malignant fibroid,even if the pulmonary lesion is solitary and appar-ently well encapsulated, and has minimal cytologicalatypia. Such a possibility, however, was excluded inour case of parenchymal pulmonary leiomyoma, asthe patient (case 1) was a man.
Recently Horstmann et al'8 reviewed 14 cases ofmultiple leiomyomatous hamartomas consisting ofbundles of smooth muscle, collagen fibres, and glan-dular epithelial cells. In one case the pulmonarynodules regressed spontaneously during pregnancyand the postpartum period, an observation that sug-gested hormonal dependence.'8The absence of epithelial or other mesenchymal
components in the three cases documented here is infavour of a true neoplastic lesion rather than a
on 8 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.40.4.306 on 1 April 1985. D
ownloaded from
Leiomyomas of the lower respiratory tract
hamartomatous malformation. We agree with Hurt8that the term hamartoma has been abused andshould be applied only to lesions showing clear evi-dence of an underlying developmental abnormality,either present at birth or manifested by excessivegrowth during normal tissue maturation.
TREATMENTThe treatment of leiomyomas is essentially conser-vative surgery. There has been no report of recur-rence after limited excision. Nevertheless extensivelung resection may be required as a result of bron-chiectasis or chronic infective changes distal to thetumour. Of the 57 bronchopulmonary cases so farreported, 29 (51%) required lobectomy and afurther eight (14%) pneumonectomy (table 2).
Parenchymal lesions usually require a less radicalprocedure and about one third have been treated bysegmental resection, although a proximal paren-chymal lesion compressing the bronchial tree maystill make lobectomy necessary as in the first of ourcases. It has been suggested that in many reportedcases of lobectomy or pneumonectomy a less radicaloperation such as segmental or sleeve resectionmight have been preferable had the histologicaldiagnosis been known before completion of the sur-gical procedure.2
Other conservative procedures include bron-chotomy and local resection, and bronchoplasticresection, which has been used successfully in bron-chial adenomas.4 19 Hurt8 describes closure of adefect in the bronchial wall with a Gebauer skingraft. Only two bronchial leiomyomas have so farbeen successfully removed bronchoscopically.4 Wefound that in our case 3 the bronchial tumour wastoo extensive for complete removal, and in anyevent irreversible pulmonary changes beyond thelesion necessitated lung resection.
Tracheal leiomyomas have been dealt with inthree ways: firstly, by bronchoscopic removal; sec-ondly, by excision of the tumour via a tracheotomyincision as in our second case; and, thirdly, by cir-cumferential resection with primary end to endanastomosis.7 Since these lesions are benign andwell circumscribed, the most conservative treatmentappropriate to the lesion is recommended. A broadbase of attachment to the membranous portion ofthe trachea is, however, typical and this precludesbronchoscopic resection in most cases.
311
We thank Dr JC Briggs for reading the manuscriptand Mrs G Caseley for invaluable secretarial assis-tance.
References
1 Crastnopol P, Franklin WD. Fibroleiomyoma of thelung. Ann Surg 1957; 145:128-32.
2 Orlowski TM, Stasiak K, Kolodziej J. Leiomyoma ofthe lung.J Thoracic Cardiovasc Surg 1978;76:257-61.
3 Taylor TL, Miller DR. Leiomyoma of the bronchus. JThoracic Cardiovas Surg 1969;57: 284-8.
4 Shahian DM, McEnany MT. Complete endobronchialexcision of leiomyoma of the bronchus. J Thorac Car-diovasc Surg 1979;77:87-91.
5 Sanders JS, Cornes VM. Leiomyoma of the trachea.Report of a case, with a note on the diagnosis of partialtracheal obstruction. N Engl J Med 1961;264:277-9.
6 Foroughi E. Leiomyoma of the trachea. Dis Chest1962;42:230-2.
7 Kitamura S, Maeda M, Kawashima Y, Masaoka A,Manabe H. Leiomyoma of the intrathoracic trachea. JThorac Cardiovasc Surg 1969;57: 126-33.
8 Hurt R. Benign tumours of the bronchus and trachea:1951-1981. Ann R Coll Surg 1984; 66:22-6.
9 Arrigoni MG, Woolner LB, Bernatz PE, Miller WE,Fontana RS. Benign tumors of the lung. A ten-yearsurgical experience. J Thorac Cardiovas Surg1970;60:589-99.
10 Peleg H, Pauzner Y. Benign tumors of the lung. DisChest 1965;47:179-86.
11 Gilbert JG, Mazzarella LA, Feit LJ. Primary trachealtumours in infant and adult. Arch Otolaryngol1954;58: 1-9.
12 Sweet RS. Pulmonary leiomyoma. Am J Roentgenol1969; 107:823-6.
13 Groves LK, Middlestone WR, McCormack LJ.Leiomyoma of the trachea: report of a case. ClevelandClinic Quarterly 1958;25:32-7.
14 Spencer H. Pathology of the lung. Vol 1. 3rd ed.Oxford: Pergamon Press, 1977:895-7.
15 Ghadially FN. Diagnostic electron microscopy oftumours. London: Butterworth, 1980:128-53.
16 Steiner P. Metastasizing fibroleiomyoma of uterus:report of case and review of literature. Am J Pathol1939; 15:89-110.
17 Rosai J. Ackerman's surgical pathology. Vol 1. 6th ed.St Louis: Mosby, 1981:283-4.
18 Horstmann JP, Pietra GG, Harman JA, Cole NG,Grinspan S. Spontaneous regression of pulmonaryleiomyomas during pregnancy. Cancer 1977;39:314-21.
19 Jensik RJ, Faber LP, Brown CM, Little CF. Broncho-plastic and conservative resection procedures for bron-chial adenomas. J Thorac Cardiovasc Surg1974;68:556-65.
on 8 June 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.40.4.306 on 1 April 1985. D
ownloaded from