leeds and york partnership nhs …...jt 14.1 minutes of the audit committee for the meeting held 13...
TRANSCRIPT

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
PUBLIC MEETING OF THE BOARD OF DIRECTORSwill be held at 13.30 on Thursday 29 January 2015
in Meeting Room 1&2 at Trust Headquarters, 2150 Century Way, Thorpe Park, LeedsLS15 8ZB
______________________________________________________________________________
A G E N D A
Members of the public will be given the opportunity to ask questions at both the beginning and theend of the meeting.
It is preferable if questions could be written down and handed to either the Chair or the Head ofCorporate Governance at the meeting, before these points in the meeting are reached or if they
could be submitted in advance of the meeting (contact details provided below *). However, theabsence of a written comment/question will not preclude members of the public from being allowed
to put these to the Board.
LEAD
1 Apologies for Absence FG
2 Declaration of a Change in Directors’ Interests and any Conflicts of Interest in respectof Agenda Items
FG
3 Opportunity to receive comments/questions from members of the public in order to
inform the discussion on any agenda item *FG
4 Minutes of the Previous Meeting
4.1 Minutes of the Meeting held on 2 December 2014 (enclosure) FG
5 Matters Arising
5.1 Update on the Staff Communication Regarding Worsley Court (enclosure) AD
5.2 Opening of Mill Lodge (verbal) JC
6 Chief Executive’s Report (enclosure) CB
7 Actions Outstanding from the Public Meetings of the Board of Directors (enclosure) CH
PART A - STRATEGIC ITEMS
8 Refreshed Workforce Strategy (enclosure) ST
9 Operational Plan Implementation Quarter 3 Report (enclosure) JC
10 Implementing NICE guidance (PH48) – smoking cessation in MH Services (enclosure) AD
PART B – GOVERNANCE ITEMS
11 Care Quality Commission – Action Plan (enclosure) AD
12 Verbal Report from the Chair of the Quality Committee for the meeting held 11December 2014 (verbal)
CT

12.1 Minutes of the meeting of the Quality Committee held 11 December 2014(enclosure)
CT
13 Verbal Report from the Chair of the Mental Health Act Committee for the meeting held15 December 2014 (verbal)
KW
13.1 Minutes of the Mental Health Legislation Committee for the meeting held 15December 2014 (enclosure)
KW
14 Verbal Report from the Chair of the Audit Committee for the meeting held 23 January2015 (verbal)
JT
14.1 Minutes of the Audit Committee for the meeting held 13 November 2014(enclosure)
JT
15 Verbal Report from the Chair of the Finance and Business Committee for the meetingheld 23 January 2015 (verbal)
GT
15.1 Minutes from the Finance and Business Committee for the meeting held 27October 2014 (enclosure)
GT
16 Integrated Quality and Performance Report and 2014/15 Quarter 3 MonitoringReturns/Self-certification (enclosure)
AD
17 Safe Staffing October and November 2014 (enclosure) AD
18 Complaints Summary Report (enclosure) AD
19 Signing up to Safety (enclosure) JI
20 National Confidential Inquiry into Suicide and Homicide by People with Mental Illness(enclosure)
JI
21 Serious Untoward Incidents Update and Lessons Learnt following the Trust IncidentReview Group meetings held: 12/11/2014, 10/12/2014, 14/01/2015(enclosure)
JI
22 Duty of Candour regulatory requirements (enclosure) AD
23 Regulation 5: Fit and Proper Persons: Directors (FPPR) (enclosure) ST
PART C – FOR INFORMATION ITEMS
24 Chair’s Report (verbal) FG
25 Draft Minutes from the Council of Governors’ meeting 4 November 2014 (enclosure) FG
26 Use of Trust Seal (verbal) FG
27 Any Other Business FG
28 Opportunity for any further comments/questions from members of the public FG
The next PUBLIC meeting of the Board of Directors’ meeting will be heldon Thursday 26 March 2015 in the Crown Room, Royal York Hotel, Station Road, York YO24 1AA
(time to be advised)
* Questions for the Board can be submitted to Cath Hill (Head of Corporate Governance / Trust
Board Secretary) using the following contact details:


1
AGENDA ITEM 4.1
LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
Minutes of the Public Meeting of the Board of Directorsheld on held on Tuesday 2 December 2014 at 2.45 pm
in Meeting Room 1&2, Trust Headquarters, 2150 Century Way, Thorpe Park, LeedsLS15 8ZB
Board Members Apologies VotingMembers
Mr C Butler Chief Executive
Ms J Copeland Chief Operating Officer
Mr A Deery Interim Director of Nursing
Mr F Griffiths Chair of the Trust
Mrs D Hanwell Chief Financial Officer
Dr J Isherwood Medical Director
Mrs M Sentamu Non-executive Director
Mrs J Tankard Non-executive Director
Dr G Taylor Non-executive Director (Senior Independent Director)
Prof C Thompson Non-executive Director
Mrs S Tyler Director of Workforce Development
Mr K Woodhouse Non-executive Director (Deputy Chair of the Trust)
Mr S Wrigley-Howe Non-executive Director
In attendanceMrs C Hill Head of Corporate Governance/Trust Board Secretary (secretariat and minutes)4 Members of the public, 1 of which was a member of the Council of Governors
Action
The Chair opened the meeting at 14.45 and welcomed members of the Board ofDirectors and members of the public.
14/190 Apologies for Absence (agenda item 1)
There were no apologies.
14/191 Declaration of Change in Directors’ Interests and any Conflict of Interestsin respect of Agenda Items (agenda item 2)
It was noted that as a new director Mr Deery had completed a Declaration ofInterest form and that no interests had been declared. Mr Griffiths noted thatthis form was filed in the Chief Executive’s office and would be available forinspection should it be required.
With regard to conflicts of interests in respect of any of the agenda items DrIsherwood declared an interest in item 7 regarding the tender for the YorkServices, noting that as well as being a director he was also employed as aconsultant psychiatrist within the York services. This was noted by the Board.No other director present at the meeting declared a conflict of interest in respectof the agenda items to be discussed.

2
14/192 Opportunity to Receive Comments / Questions from Members of the Public(agenda item 3)
Mrs Roper noted that the Trust would be working with Social Services in Leedsto improve the health of service users and asked if the Trust was successful withthe bid for York services whether this work would be replicated there. MrGriffiths asked for the question to be addressed later in the meeting.
14/193 Minutes of the Meeting held on 30 October 2014 (agenda item 4.1)
The minutes of the meeting held on 30 October 2014 were received and agreedas a true record.
14/194 Matters Arising (agenda item 5)
There were no matters arising.
14/195 Bootham Park Hospital and Lime Trees Update Report (agenda item 6)
Ms Copeland presented a high level update report noting that Mill Lodge wasstill on track for completion and that it was expected services would move intothe premises on 15 December 2014. She noted that there had been delays withthe move to Cherry Tree House and that completion was now scheduled for May2015, but noted the NHS Property Service Ltd (NHSPS) was looking at thepossibility of bringing this dae forward.
With regard to the refurbishments at Bootham Park Hospital Ms Copeland notedthat there was now an outline timetable for this work and that the expectedcompletion date was September 2015, although she noted there was still noProject Initiation Document or Business Case for the work. Ms Copelandadvised the Board that there was a meeting of the Bootham ProgrammeManagement Board on the 3 December 2014 and that Mrs Hanwell would beattending and would press for further information and details in respect of thetimetable for the work.
With regard to risks, Ms Copeland noted that these were now in the process ofbeing reviewed in the light of the information received about the tender processfor York services.
Mr Wrigley-Howe noted that whilst the timetable had been received from NHSPSit was clear there had been some slippage and expressed concern that the Trusthad very little influence over controlling this and asked what more could be doneto bring pressure to bear to ensure work is completed within the timescalesoriginally agreed. Mr Wrigley-Howe noted that at the October meeting the Boardhad suggested further legal advice be taken in respect of the potential course ofaction open to it. Mrs Hanwell informed the Board that the solicitors had advisedher that NHSPS are taking remedial action and as such that there is littlerecourse through the Business Transfer Agreement (BTA) due to them being inthe process of taking that action; however, she noted that she was waitingfurther clarification on this matter.

3
Mr Wrigley-Howe noted that he had found there to be no evidence via agendasthat either the Vale of York CCG or NHSPS had discussed this matter at theirBoard meetings during the course of the year and suggested that Mrs Hanwellascertains why this was. In response, Mrs Hanwell assured the Board that thismatter was top of the agenda for the Vale of York CCG and for NHSPS and thatthey were both taking the matter very seriously. Mr Butler supported MrsHanwell’s comments.
Mr Woodhouse asked what the process is for escalating the matter formally andasked how the executive directors were taking this forward. Mrs Hanwellassured the Board that she had escalated the matter with NHSPS and hadclearly outlined the risks to safety. Mr Butler noted that raising the matter withthe organisations had resulted in them taking action thus far, but indicated thathe would raise the matter again.
Mr Griffiths asked if it would be possible to accelerate matters using theimpending CQC reports as a lever. Mr Butler indicated that this might bepossible. Ms Copeland also noted that the comments made by the CQC inrespect of mixed sex accommodation would have implications for various sites.Prof Thompson noted that regardless of the findings set out in the impendingCQC reports the Trust was still carrying the risk. Mrs Hanwell advised the Boardthat whilst the Trust is carrying the risk this is being managed and there is aremedial action plan in place.
Prof Thompson also asked what more the Trust could do to expedite the matter,noting that notwithstanding the action being taken by the CCG and NHSPS workwas not progressing at the pace expected by the Trust. The Board discussedsome of the potential options open to the Trust.
In summary Mr Griffiths noted that there was a high level of frustration within theBoard in respect of the timeline. It was agreed that Mrs Hanwell would takelegal advice about the options open to the Trust and would be advised as towhether it is prudent to write to the organisations before the Board meets inJanuary to set out any potential course of action.
It was also agreed that Mr Griffiths would write to the chair of NHSPS to set outthe view of the Board and seek assurance that the timeline will be adhered to.
DH
FG
The Board received and noted the update report and also provided a view asto what more could be done by the Trust to progress the matter.
14/196 NHS Vale of York CCG – Tender Opportunity (agenda item 7)
Mrs Hanwell presented a paper which set out the formal timeline and process forthe prospective tender for mental health and learning disability services in theVale of York noting that it presented to the Board a recommendation as to how itmight wish to proceed.
Mrs Hanwell advised the Board that separate to the main tender opportunity

4
there was to be a separate process for county-wide autism services and that theTrust would also be looking to participate in this tender process. This proposalwas supported by the Board.
Ms Copeland noted that there was a lot of work already being undertaken inpreparation for the start of the process in order to put the Trust in a betterposition to complete the tender documentation within the tight deadline.
At the invitation of the Chair, Dr Taylor outlined some of the discussion that hadtaken place in the private meeting as to how the Trust would proceed in respectof the process, noting that the Board had taken an ‘in-principle’ decision topursue the tender opportunity unless following the release of the documentation,due diligence identified any significant reason as to why it should not moveforward with the bid on the grounds of safety, quality or finances.
Dr Taylor also noted the short timescale to complete the tender documentationand noted the need for the executive team to look at the governance andoversight arrangements for this. Mr Griffiths also noted the need to ensure thatthe Council of Governors was linked into this process.
Mrs Sentamu noted the agreement that had been made to expand partnershipwork to include collaborative partners including those in the businesscommunities. Mr Butler welcomed working with partners in terms of the deliveryand development of services.
Mr Butler also noted the need for there to be an appropriate communicationmade to staff in order to keep them informed and re-assured of the process as itunfolds.
DH
The Board received and noted the timeline and process for the forthcomingtender process for services in the Vale of York.
14/197 ‘Achieving Better Access to Mental Health Services by 2020’ – theproposed new standards – implications for the Trust (agenda item 8)
Mr Deery presented a paper which informed the Board of the plans set out bythe Department of Health and NHS England in their recent publication AchievingBetter Access to Mental Health Services by 2020 and the issues for Trust. MrDeery noted that whilst there were a number of matters addressed in thepublication this paper focused in particular on the new waiting time standards forImproving Access to Psychological Therapies (IAPT) and Early Intervention inPsychosis services (EIS).
Mr Deery explained to the Board the new national waiting time standards inrespect of IAPT and EIS and noted that whilst there were already standards inplace the new targets represented a significant change to these.
Mr Deery noted that there was much work ongoing in the Trust to look at currentactivity and what needs to be done to meet these new standards; that furtherguidance was awaited which would inform that work; and that a report would be AD

5
brought back to a future Board on the outcome of this work.
Ms Copeland highlighted a risk around the IAPT targets, noting that the nationaltarget for those with a mild to moderate mental health problem accessingpsychological therapies is 15% and that by introducing waiting time targets andincreasing the profile of the service this could lead to an increase in demand.Ms Copeland supported there being more people treated within the IAPT servicebut noted that current funding would not meet any extra demand and that thiscould impact negatively on the length of waiting lists.
Mrs Sentamu asked for a view on how well the Trust is likely to meet the newrequirements and what the gap might be. Ms Copeland noted that the workneeds to be completed first before any view can be formed.
The Board received the paper. It noted the new standards and receivedassurance that work was ongoing to look at the impact of this and noted that areport would be brought back to the Board.
14/198 Mental Capacity Act – Supreme Court Ruling (agenda item 9)
Mr Deery presented a paper which outlined the changes to the definition ofdeprivation of liberty which followed the Supreme Court Judgement 19.3.14 in Pversus Cheshire West and Others. Mr Deery outlined to the Board whatchanges the ruling made; the actions required to meet the ruling; and broadlywhat the implications are for the Trust.
Mr Deery noted that during their recent announced inspection the CQC hadfound good practice in respect of the Mental Capacity Act, but that they hadraised concerns about the provision of training in respect of this. Mr Deeryoutlined to the Board the proposal for a group to assess the impact of this ruling;whether it is being applied consistently for those service users that fall within thisrisk group; and whether all the necessary training is in place. Dr Isherwoodnoted that whilst the CCGs are offering training in this area this should notpreclude the Trust from also carrying this out in-house.
Prof Thompson suggested that this assessment could be something that theClinical Audit Team could undertake. Dr Isherwood indicated that it wasprobably not appropriate for the Clinical Audit Team to undertake an audit as itwould need significant clinical involvement in determining if liberty is to bedeprived.
Mr Woodhouse noted that the ruling had been discussed at the Mental HealthAct Committee and that he had outlined to the Board some of the issues. Healso noted that Ms Murphy had initiated some work in respect of this and thatthis might be used to inform the further work proposed. Mr Woodhouse notedthe need for the MHA Committee to look at this again at its next meeting.
AD

6
The Board received a formal report on the Supreme Court Ruling and notedthat work is still ongoing to look at the implications of this for the Trust and itsservice users and that a report would be brought back to the Board in March2015 in respect of the outcome of this work.
AD
14/199 LYPFT and Leeds City Council Adult Social Care Integrated DeliveryModel (agenda item 10)
Ms Copeland presented a paper for information to inform it of the work ongoingto pursue greater integration and partnership working with Adult Social Care inLeeds, noting that this was fully in line with the Trust’s strategic intention todevelop more partnership working arrangements. Ms Copeland advised theBoard that at this point there was an intention expressed to work together todevelop a project and that further information would be brought back to theBoard as work gets underway and progresses.
With regard to the question asked by Mrs Roper, Ms Copeland advised theBoard that there would be an intention to pursue similar approaches in York asthere was in Leeds and that there was the possibility of some earlyconversations in respect of this.
Dr Taylor welcomed this model. She noted that supporting this work would bethe need to carry out modelling not only of care, but also of the finances whichwould need to take account of which organisation carries the risk. Dr Taylorsuggested that this could come to the Finance and Business Committee so itcan be looked at in greater detail than is possible at Board. Ms Copelandwelcomed this approach.
JC
The Board received information about the work progressing to implement aproject to explore options of there being a closer working relationship andintegration with Adult Social Care, noting that further information would comeback to the Board as the project progresses.
14/200 Assurance on the Additional Findings by the Care Quality Commission(CQC) following their announced visit in September 2014 (agenda item 11)
Mr Deery presented a paper which set out the Trust’s responsive action plan tothe initial findings by the CQC. Mr Deery noted that the action plan set out thefinding not only in respect of the visits made during September and October, butalso the findings from follow-up visits in early November to the older people’sservices in York.
Mr Deery outlined these additional findings including the apparent lack ofmedical staffing cover in the service during core hours; the length of time takento administer medication in the service; and issues around delayed transfers ofcare.
With regard to delayed transfers of care Mr Deery noted that he had requested

7
further information from the CQC in respect of this and had carried out a detailedanalysis of the data for a 12 month period and assured the Board that the Trustwas not an outlier in terms of performance; that the delays had not been causedby the Trust; and that the low number of nursing home placements in the Yorkarea had adversely impacted on the Trust’s ability to transfer service users toappropriate accommodation. Mr Deery noted that this matter had not beenadded to the action plan and that the CQC would be advised of the Trust’sstance on this matter.
Mr Woodhouse suggested that delayed transfers of care should be added to theaction plan noting that Mental Health Act Managers have experienced difficultiesin discharging patients from section due to an inability to appropriately placeservice users. The Board discussed the factors that impact on the ability totransfer service users; the work that had been undertaken in the past to reducethe number of delays; and the national picture in terms of social care placesavailable.
Mrs Tankard asked what the governance process would be for monitoringprogress in respect of the action plan. It was noted that this would be monitoredby a small group and would also be taken through the Quality Committee forassurance on progress.
Mr Butler noted that the CQC had released its Intelligent Monitoring report formental health trusts and that this Trust was rated ‘green’ overall.
Ms Copeland noted that the reference in the report to Millfield should readMeadowfields. This was noted for the purpose of clarity.
The Board received an update in respect of the additional findings made by theCQC and noted that the action plan would be monitored through the QualityCommittee.
14/201 Safe Staffing October 2014 (agenda item 12)
Mr Deery presented the Safe Staffing Report for October 2014 noting that thiswas an exception report that highlighted any wards where there had been a lessthan 80% fill rate against planned staffing levels. Mr Deery also noted that thereport included the variables which may have affected the staffing levels. Withregard to those wards that have exceptionally high fill rates Mr Deery suggestedthat this data be included in future reports as it may highlight where the plannedlevels have been set too low.
Mr Deery advised the Board that the report did not include figures for: Fieldveiw,due to it only recently being classified as an inpatient unit, noting that this will beincluded in future reports; and for Worsley Court due to this being temporarilyclosed.
In presenting the information Mr Deery reported that eight wards had variationsto the planned staffing levels and assured the Board that the reasons as to whythis had occurred had been looked at and drew attention to the information

8
included in the report in respect of these variables. Mr Deery assured the Boardthat this information would be shared with ward managers in detail to look at thereasons and better understand how staff can be deployed more effectively. MrDeery noted that the Workforce Development Team would be assisting with thiswork. Mrs Tyler noted that e-Rostering has been implemented in all areas withinthe Trust and that this provides an effective tool for managers to use to look athow the right staff are placed across the Trust.
Prof Thompson noted that another way of measuring safe staffing was throughthe number of incidents and suggested that this information should be a crossreferenced.
Mr Woodhouse again raised the point about whether there was the rightmanagement structure in place to support those on the ward in using a tool suchas e-Rostering to best effect and to effectively manage staff day-to-day in termsof the scheduling of, for example, annual leave on an individual basis. It wasconfirmed that there was.
The Board of Directors received the report and received assurance thatstaffing levels on the wards were safe. The Board also noted the work to beundertaken to work with managers to look at how staff can be effectivelydeployed across the services.
14/202 Complaints Summary Report (agenda item 13)
Mr Deery presented the Complaints Summary Report for October andhighlighted the key issues including that of not meeting the Trust’s agreedstandard of responding to complaints within a 30 day period. Mr Deery outlinedsome of the reasons for this and also noted that work is being done to look atmaking the process of responding more efficient.
Mr Griffiths noted that the Care Quality Commission had identified complaints asbeing an issue for the Trust in their initial feedback from the recent inspection.
Dr Taylor expressed disappointment with the narrative in the report noting that itcame across as being rather defensive. Dr Taylor also suggested that by havingindividually agreed timescales for responding to complaints it will make it harderto track progress.
Dr Isherwood drew attention to the ‘Sign Up to Safety’ initiative noting that thisencourages organisation to bring together all the strands of work from whichlessons can be learnt in order to improve safety. Dr Isherwood also noted theneed to ensure that the Trust has in place the right resource in terms ofnumbers, skills and training to carry forward this work. Prof Thompsonsupported such information being pulled together.
Prof Thompson expressed surprise that the number of complaints had remainedconstant for a long period of time despite the actions taken to increaseawareness of how to make a complaint.

9
Mr Woodhouse asked who was ensuring that the function was effectivelymanaged and that staff were held to account for performance in terms ofmeeting the target time for responding to complaints. Mr Butler outlined wheresome of the delays can occur in the system. Ms Copeland explained thecapacity issues within Care Services and how this has impacted to some degreeon the investigation of complaints within the services.
Dr Taylor noted that the Board had discussed this on a number of occasions andexpressed some frustration that things do not appear to have improved.
The Board received the Complaints Summary Report and noted the pointsdiscussed in relation to the delays in responses.
14/203 Statement of Compliance with NHS England’s Emergency Preparedness,Resilience and Response Standard 2014 (agenda item 14.1)
Mrs Hanwell noted that this was a new requirement for this financial year and assuch was presented to the Board for the first time.
Mrs Hanwell drew attention to the declaration made and advised the Board thata declaration of ‘partial compliance’ had been made noting that this is largely asa result of non-compliance with new hazardous materials and chemical,biological, radiological and nuclear (HAZMAT/CBRN) standards. Mrs Hanwellassured the Board that whilst non-compliance in this area had been declaredthis posed a low risk to the Trust in terms of a potential emergency, but that workwas on going to address the requirements of this new standard.
The Board received and approved the compliance declaration made and notedthe actions to address all areas of non-compliance.
14/204 Emergency Preparedness, Resilience and Response Annual Report 2014
(agenda item 14.2)
Mrs Hanwell presented the Emergency Preparedness, Resilience and ResponseAnnual Report, noting that during the coming year the Finance and BusinessCommittee will receive updates in respect of the work ongoing.
The Board of Directors received the report and noted the content.
14/205 Chair’s Report (agenda item 15)
Mr Griffiths noted that he had received a very favourable report from a memberof the public in respect of the care that had been received by a member of theirfamily at the Lime Trees unit in York. Mr Griffiths advised the Board that theservice had been described to him as ‘outstanding’ and observed that this viewhad been formed by the family member despite the poor environment at the unit

10
itself. Mr Griffiths asked for the praise given by the individual to be conveyed tothe staff at the unit.
14/206 Use of the Trust seal (agenda item 16)
It was noted that since the last meeting the seal had not been used.
The Board noted that the seal had not been applied.
14/207 Any Other Business (agenda item 17)
There were no items of other business.
14/208 Further Questions or Comments from the Public (agenda item 25)
There were no other questions from members of the public and Mrs Roperindicated that she was happy with the response that she had received in respectof her question although she did make an observation about the amount of studyleave and training that staff had undertaken and how this impacted on incidents.Mr Griffiths thanked her for this observation.
At the conclusion of business the Chair closed the public meeting of the Board of Directors of Leeds andYork Partnership NHS Foundation Trust at 16:30 and thanked members of the Board and members of
the public for attending.

11
BOARD OF DIRECTORS’ ACTION SUMMARY(PUBLIC MEETING)
Meeting held 2 December 2014
MINUTE ACTION SUMMARY (PUBLIC MEETING – PART A)LEAD
DIRECTOR
14/195 Bootham Park Hospital and Lime Trees Update Report (agenda item 6)
In summary Mr Griffiths noted that there was a high level of frustration withinthe Board in respect of the timeline. It was agreed that Mrs Hanwell would takelegal advice about the options open to the Trust and would be advised as towhether it is prudent to write to the organisations before the Board meets inJanuary to set out any potential course of action.
It was also agreed that Mr Griffiths would write to the chair of NHSPS to set outthe view of the Board and seek assurance that the timeline will be adhered to.
DH
FG
14/196 NHS Vale of York CCG – Tender Opportunity (agenda item 7)
Dr Taylor also noted the short timescale to complete the tender documentationand noted the need for the executive team to look at the governance andoversight arrangements for this. Mr Griffiths also noted the need to ensure thatthe Council of Governors was linked into this process. DH
14/197 ‘Achieving Better Access to Mental Health Services by 2020’ – theproposed new standards – implications for the Trust (agenda item 8)
Mr Deery noted that there was much work ongoing in the Trust to look atcurrent activity and what needs to be done to meet these new standards; thatfurther guidance was awaited which would inform that work; and that a reportwould be brought back to a future Board on the outcome of this work.
AD
14/198 Mental Capacity Act – Supreme Court Ruling (agenda item 9)
Mr Woodhouse noted that the ruling had been discussed at the Mental HealthAct Committee and that he had outlined to the Board some of the issues. Healso noted that Ms Murphy had initiated some work in respect of this and thatthis might be used to inform the further work proposed. Mr Woodhouse notedthe need for the MHA Committee to look at this again at its next meeting.
The Board received a formal report on the Supreme Court Ruling and notedthat work is still ongoing to look at the implications of this for the Trust and itsservice users and that a report would be brought back to the Board in March2015 in respect of the outcome of this work.
AD
AD

12
MINUTE ACTION SUMMARY (PUBLIC MEETING – PART A)LEAD
DIRECTOR
14/199 LYPFT and Leeds City Council Adult Social Care Integrated DeliveryModel (agenda item 10)
Dr Taylor welcomed this initiative. She noted that supporting this work wouldbe the need to carry out modelling not only of care, but also of the financeswhich would need to take account of which organisation carries the risk. DrTaylor suggested that this could come to the Finance and Business Committeeso it can be looked at in greater detail than is possible at Board. Ms Copelandwelcomed this approach.
JC

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Chief Executive’s Report
DATE OF MEETING: 29th January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Chris ButlerSTRATEGIC:
PAPER AUTHOR: Chris ButlerGOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)SO1 We provide excellent quality, evidence-based, safe care that involves people and promotes
recovery and wellbeing
SO2 We work with partners and local communities to improve health and lives SO3 We value and develop our workforce and those supporting us SO4 We provide efficient and sustainable services SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individualsOther – not yet a public documentMatters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
6

SUMMARY:
This paper summarises topics of interest to the Board of Directors.
Its intention is that of setting the scene for the meeting of the Board of Directors in thecontext of national issues, also matters impacting on the business of the Trust.
RECOMMENDATIONS:
The Board of Directors is asked if the report is helpful as a high level summary of currenttopics in mental health and learning disability services, also if it provides sufficientassurance concerning our Trust’s response to those matters highlighted.

Page 1 of 8
Chief Executive’s Report to the Board of Directors
January 2015Today’s Agenda
Today we consider our action plan in response to the publication of the reports of theinspection of the Care Quality Commission (CQC) www.cqc.org.uk following the“Quality Summit” held on the 7th of January.
Members of the Board have had sight of the information we made available to staff,partners and the media www.leedsandyorkpft.nhs.uk/about_us/CQCInspection
In summary, the Trust’s overall rating is “requires improvement”. The majority of theconcerns raised by the CQC relate to services in York and North Yorkshire,particularly older people’s inpatient care which was rated “inadequate”.
During time with the media I described the report as a “tale of two cities”. Services inLeeds have mostly been rated as good whilst there are a number of concerns raisedabout services in York. The CQC acknowledges the historical underdevelopmentand underinvestment in mental health and learning disability services in York. TheBoard is aware that with the Vale of York Clinical Commissioning Group over thepast three years we have been steadily improving services. The next major phase ofdevelopment is a £2.7 million scheme to refurbish the three inpatient wards atBootham Park Hospital which will be completed later this year. However this will dono more than bring inpatient services up to an acceptable standard and a long termsolution is still needed for inpatient mental health care in York.
Though the action plan is ours to develop and deliver, it requires close collaborationbetween ourselves and our partners to ensure its full implementation.
Working with the media at the time of the publication of the CQC’s reports, ajournalist commented on how transparent we were being about the reportsthemselves and our views. In the spirit of this, it is good that we are considering“Sign up to Safety” today, at the heart of which is being open about mistakes;understanding what went wrong; committing to making improvements; and gettingthe right balance between professional accountability allied to a view thatprofessionals want to do the right thing for service users and cares.
What’s happening in the Trust?
2015 Membership CampaignMan Up? Let’s Talk about MENtal Health
As well as providing services we also work to improve the health and lives of thepeople who use our services every day. We are committed to campaigning to raise

Page 2 of 8
awareness of mental health and learning disabilities, working in partnership with ourmembers, staff, and local organisations over time in order to eliminate stigma.
The Men’s Health theme was chosen as our membership campaign during amember and governor vote which took place during Annual Members Day 2014. Thisis a campaign chosen by the members, for the members.
“Man Up?” Is a campaign focusing on men’s mental health, targeting men of allages and their friends and families. This is an important issue as, for example, 72%of people treated for depression are female yet 75% of people who take their ownlives are male.
Men’s mental health can be a taboo subject. Masculinity, pride, peer pressure andsocial norms can all lend themselves culturally to an environment in which men,more so than women, can feel isolated, alone and unable to express concerns overtheir mental wellbeing. Phrases such as “man up”, “real men don’t cry” and “big girlsblouse” have become societal norms which should be challenged. Using “Man Up?”as a questioning title for this campaign creates an instant and engaging point ofdiscussion.
Though primarily a membership campaign, our intention is that it will utilise socialmarketing principles to bring together a wealth of local resources, information, facts,learning experiences and activities to empower individuals, families, friends,organisations and local communities across Leeds and York.
Our Membership Team will focus their efforts on signposting to existing Trustservices and activities and to organising events which encourage active discussion,whilst providing links to our NHS colleagues and partner organisations whospecialise in the wide variety of men’s mental health associated services and issues.
The Campaign Structure
To provide structure within such a large subject area the campaign will focus on adifferent area of men’s health each month. Here are some examples:
Home Truths: men in crisis Uppers & Downers: addiction and how men cope Hidden Lives: little-talked-about issues for men Tough Turf: unhealthy aspects of health Employment Special Men in focus: Spotting the warning signs Meaning of Masculinity: What does it mean to be a man in 2015? Kick into Touch: linking between physical health and mental wellbeing Find your Tribe: signposting to local services and support networks
The membership team will work in partnership with the Council of Governors todevelop activities, create contacts, showcase Trust work, advertise partner eventsand organise bespoke events within each Governors responsible constituency.
This is an exciting initiative and I know that members of the Board will give it their fullsupport and participate in campaign activities. The Campaign launched yesterday inYork and today in Leeds.

Page 3 of 8
The University of Leeds - Associated Teaching Trust
The Board is aware of our major role in training health and social care professionals.
In recognition of this The University of Leeds has formally designated our Trust as anAssociated Teaching Trust.
Becklin Centre Café
FoodWorks, a charitable organisation, has been chosen to run our cafés at theBecklin Centre and The Mount. Meetings have been held with service user and staffrepresentatives to agree the design of the café at the Becklin Centre; and a detailedimplementation plan is in place. The opening of the Becklin Centre café wasplanned for January 2015, but unfortunately this has been delayed until 6 April dueto delays in progressing building works and the contractual agreement with our PFIpartners. The building works are necessary to ensure that the kitchen at the BecklinCentre is fit for purpose and meets current food safety requirements. The provisionof a café by a third party requires a change to our existing contractualarrangements. The building works have now been agreed and work on the servicelevel agreement with our PFI partners is progressing. We are therefore confidentthat the Becklin Centre café will open in April.
Carers’ entitlements under the new Care Act
At a previous meeting the Board asked that we ensure that our staff are aware ofcarers’ entitlements under the new Care Act. The Care Act gives local authorities aresponsibility to assess carer’s needs for support where a carer appears to havesuch needs; and, if the carer meets the eligibility criteria, to agree a support plan. ADepartment of Health fact sheet entitled “The Care Act – the law for carers” has nowbeen circulated to all staff via Trust wide email and will be cascaded through CareServices.
The Outside World
Director of Adult Social Services in Leeds
Cath Roff has been appointed as the Director of Adult Social Services in Leeds.Cath is currently the Strategic Director: Adults, Health and Housing at Derby CityCouncil. Prior to working in Derby, Cath was the Director of Adult’s Services atSheffield City council.
Improving complaint handling across the NHS and social care
The Parliamentary and Health Service Ombudsman www.ombudsman.org.uk hasworked with patients and service users to define what would make complainingabout the NHS or social care a positive experience for people. The outcome of thiswork is My expectations for raising concerns and complaints produced inpartnership with the Local Government Ombudsman and Healthwatch England, andin consultation with over 100 patients and service users and over 40 organisations, itdescribes people's expectations for good complaint handling. This includes, knowing

Page 4 of 8
they have a right to complain and where to complain, being kept informed andfeeling their complaint made a difference so the same thing does not happen toanyone else, and feeling confident to complain again.
The CQC has adopted “My expectations” as a measurement tool for its inspections.
We will take “My expectations” into account in increasing our focus on responding tocomplaints in a full and timely way.
“Children and adolescents' mental health and CAMHS” – Report of the Houseof Commons Health Committee
The House of Commons Health Committee’s (the Committee) published an inquiryinto CAMHS on the 5th of November 2014.www.publications.parliament.uk/pa/cm201415/cmselect/cmhealth/342/34202.htm
It found “serious and deeply ingrained problems” with the commissioning andprovision of children and adolescents' mental health services from prevention andearly intervention, through to CAMHS inpatient services. The Committee maderecommendations for action across eight areas. These are:
1. Information2. Early intervention3. Outpatient specialist CAMHS services (Tier 3)4. Tier 4 inpatient services5. Bridging the gap between inpatient and community services6. Education and digital culture7. GPs8. National priority and scrutiny
The report and its findings will be taken into account by the national Department ofHealth/NHS England Children and Young People’s Mental Health and WellbeingTaskforce www.gov.uk/government/groups/children-and-young-peoples-mental-health-and-well-being-taskforce which is due to report in February.
With regard to our services, the Board will recall that the CQC found that ourinpatient services were rated as “requires improvement”. The issues alighted on bythe CQC largely centred on environmental issues which have been resolved. OurCAMHS community services were rated as “good”.
Young people encouraged to go online to treat mental health issues
Reports in the media suggest that young people will be encouraged to use apps totreat themselves for depression under government plans to improve mental health.Ministers want children and adults to be able to get treatment for mental healthproblems online as part of a transformation of how illnesses such as depression aredealt with by the NHS. Care minister Norman Lamb wants to use online tools,including computerised cognitive behavioural therapy, online counselling and peersupport networks.
Page 5 of 8
Across Leeds we are doing a lot of interesting work on the role of digital solutions inhealthcare through the development of the mHealthhabitathttp://mhealthhabitat.co.uk led by Victoria Betton.
Cross-government mental health taskforce
The Deputy Prime Minister, Nick Clegg, has set up a Ministerial cross-governmenttaskforce (the taskforce). The taskforce will be chaired by the Deputy Prime MinisterClegg and includes senior ministers such as Theresa May, Jeremy Hunt and VinceCable. One of its early activities is to examine how to improve mental healthservices for young people and to improve crisis care.
Independent Report into the future care of people with learning disabilities
On the 26th of November 2014 NHS England published a report about the future careof people with learning disabilities http://www.england.nhs.uk/wp-content/uploads/2014/11/transforming-commissioning-services.pdf
Recommendations in the report include:
The introduction of a Charter of Rights for people with learning disabilitiesand/or autism and their families
Giving people with learning disabilities and their families a ‘right tochallenge’ decisions and the right to request a personal budget
A requirement for local decision-makers to follow a mandatory frameworkthat sets out who is responsible, for which services and how they will beheld to account, including improved data collection and publication
A planned closure programme of inappropriate institutional in-patientfacilities supporting patient choice
Improved training and education for NHS, local government and providerstaff
The founding of a social investment fund to build capacity in community-based services
The report gives fresh impetus to people with learning disabilities and theirfamilies increasingly taking control of how the services they want and how theirneeds are met, including increasing the use of personal budgets and “integratedpersonal commissioning”, as well as broader action on employment rights andopportunities.”
Autumn Statement
The Chancellor of the Exchequer gave his Autumn Statement on the 3 Decemberwww.gov.uk/government/topical-events/autumn-statement-2014 there wereannouncements specific to mental health:
£20m in 2015-16 and in 2016-17 to fund courses to help adults experiencing mildto moderate depression, anxiety and sleep disorders in England

Page 6 of 8
£3m to expand existing psychological work and wellbeing pilots starting in 2015-16
£150m to help children with eating disorders £15m partnership fund to find new dementia treatments
The Dalton Review
The Dalton review concerning the options for the provision of NHS care waspublished on the 5 December www.gov.uk/government/publications/dalton-review-options-for-providers-of-nhs-care
It identifies 5 key themes:
One size of provider does not fit all Quicker transformational and transactional change is required of the NHS Ambitious organisations with a proven track record should be encouraged to
expand their reach and have greater impact The overall sustainability for the provider sector is a priority as NHS finances
tighten A dedicated implementation programme is needed to make change happen
This review needs to be read in the context of the 5 Year Forward View published byNHS England.
We will factor into the refresh of strategic and operational plans both the DaltonReview and the 5 Year Forward View. We are also fully participating in discussionsacross the Leeds and York Health and Social Care economies.
Care Quality Commission Report – “The State of health care and adult socialcare in England 2013/2014”On the 19th of December 2014 the CQC published the “The State of health care andadult social care in England 2013/2014”http://www.cqc.org.uk/sites/default/files/state-of-care-201314-full-report-1.1.pdf
The CQC found many examples of good and outstanding care, also wide variation inquality. At the end of the reporting period, the end of August 2014, 9 trusts achievedan overall rating of “good”, 24 trusts were rated “requires improvement”, and 5 trustswere rated “inadequate”.
A key issue in the report is variation in the quality of the care inspected. Variation isan issue for us to address in our CQC action plan.
Friends and Family Test (FFT) across community and mental healthcare
The Board will recall that we have been inviting people who work for the Trust to saywhether they would be happy to use our services or for a family member to do so.
The FFT is now more widely available. It went live in 8000 GP practices acrossEngland from 1 December and in all NHS-funded mental health and communityhealth services from 1 January this year www.england.nhs.uk/ourwork/pe/fft/

Page 7 of 8
NHS England accepts that the results will not be statistically comparable againstother organisations because of the various data collection methods; however theintention is that the FFT will provide a broad measure of patient experience that canbe used alongside other data to inform service improvement and patient choice.
I will bring an update to the Board on this at a future date.
The Deputy Prime Minister spoke about removing mental health stigma andthe need to adopt a 'zero suicide' ambition across the NHS
On the 19th of January 2015 the Deputy Prime Minister set out an ambition for zerosuicides in the NHS. In his speech he cited a mental health programme in Detroit,USA, which signed up to a ‘zero suicide’ commitment and has reported that nobodyin the care of their depression services has taken their own life in over two years.
Methods to make this possible include:
Keeping in touch with service users after an inpatient stay Having a personal safety plan in place so that patients, family and friends know
what to do and where to go for help if they need it and have regular contact withsomeone they know and trust
Bringing safety systems in line with treatment for physical health – for example,designing a process for any member of staff to follow if a patient is at high risk ofsuicide. This would tell staff what to do, who to call, where to send the patient, andhow to follow it up
Joining all services up so that patients who are at risk will not fall through thecracks – linking GP, carers and mental health services
There are mental health service services in England working in this.
Mersey Care in Liverpool has created a programme to eliminate suicide by 2017/2018 which includes:
Improved training for staff, focusing on the clinical skills needed to work withpatients and their families to develop a ‘safety plan’ – a personalised care planwith clear ways to get help 24/7
Working with other providers and stakeholders to share best practice –including CALM, Samaritans and the Cheshire and Merseyside ReductionPartnership
A dedicated “Safe from Suicide” team will provide advice, support, assessmentand monitoring
The NHS in the South West of England “Project Zero” is looking to:
Work closely with A&E to better identify and support people who present withsuicidal thoughts or attempts
Explore ways of providing better mental health support for people once they’vebeen discharged, regardless of which NHS service they’ve been in contact with
Explore how to target high risk groups, such as middle aged men, with tailoredsupport

Page 8 of 8
Work with other agencies, such as the police and transport services, to identify‘hot-zones’ – areas where higher than average numbers of suicides occur – andunderstand the reasons behind these figures
In the NHS in the East of England, the whole region has come together to pledge tosuicide prevention, with four pilot areas helping to improve care by:
Providing training to give police, paramedics, midwives and GPs greaterconfidence in talking to people who are in distress and help provide the careneeded to keep them safe
Working to remove the means of suicide in local communities, for exampleerecting barriers at a ‘hot-spot’ at a shopping centre
Setting up a website (led by the local MIND) to help educate communities inCambridge and Peterborough and raise awareness about suicide. This is nowbeing rolled out in other locations across the region
Developing ‘safety plans’ – a personalised care plan developed with every personwith risk factors, involving families and carers, with clear ways to get help aroundthe clock
In England 4,700 people commit suicide the majority of whom are men.
Conclusion
I hope that this report informs the meeting of the Board of both national issues andmatters impacting on the business of the Trust.
Chris ButlerChief ExecutiveJanuary 2015

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Actions Outstanding from Public Meetings of the Board ofDirectors
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Cath Hill, Head of CorporateGovernance (Trust Board Secretary)
STRATEGIC:
PAPER AUTHOR: Cath Hill, Head of CorporateGovernance (Trust Board Secretary)
GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)
G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)
SO1 We provide excellent quality, evidence-based, safe care that involves people and promotesrecovery and wellbeing
SO2 We work with partners and local communities to improve health and lives
SO3 We value and develop our workforce and those supporting us
SO4 We provide efficient and sustainable services
SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individuals
Matters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
7

SUMMARY:
It is considered good practice to formally monitor progress against actions agreed by theBoard of Directors, so that undue delay or failure to complete actions is formally challengedand items are reported back to the Board in a timely manner. Accordingly, the cumulativeBoard action list is detailed in the attached report and will be updated following eachmeeting.
The Board is asked to note the attached report which shows the recently completedactions. These will be removed for the next iteration of report to Board. The Board is alsoasked to note those actions that are still outstanding and to be assured of their progresswhere detail is provided.
The Board is also asked to note the governance pathway and be assured that actions areconsidered and addressed outside of the Board meeting. The action log is not onlyreceived by the Board of Directors at each of its meetings but is also reported to executivedirectors so they can review their actions ahead of the Board meeting, with the ChiefExecutive maintaining an overview of the completion and progress of actions.
The action log was up to date at the point of being circulated and those named as lead forthe actions are invited to provide any recent significant update which has occurred after thereport was sent out.
RECOMMENDATIONS:
The Board of Directors is asked to:
Note the actions outstanding from previous Board meetings and the timescale forcompletion, seeking clarification on progress where it considers this necessary.

1BOARD OF DIRECTORS – Cumulative Action Log (public board)
Cumulative Action Report for the Public Board of Directors’ Meeting
Key to status =Still outstanding/awaiting completionCompleted
LO
GN
UM
BE
R MINUTENUMBER
ANDORIGINATING
MEETINGDATE
ACTION(INCLUDING THE TITLE OF THE PAPER THAT GENERATEDTHE ACTION)
PERSONLEADING
BOARDMEETING TO
BEBROUGHTBACK TO /
DATE TO BECOMPLETED
BY
COMMENTS
ST
AT
US
140 14/110 (July2014)
The Chief Executive’s Report (agenda item 6)
In respect of the national confidential enquiry into Suicide andHomicide by People with Mental Illness the Board agreed that apaper would come to a future meeting linked to the work on clinicalrisk management due to the linkages between these two matters.
JimIsherwood
January /March 2015
(see commentacross)
COMPLETED
This has been included on theJanuary Board agenda
143 14/142(September2014)
Bootham Park Hospital and Lime Trees Update Report (agendaitem 8)
Mr Woodhouse noted the importance of ensuring that momentum ismaintained and suggested that Mr Butler writes to NHS England andother parties involved reminding them of their responsibility to drivethrough the changes. This was supported by the Board.
Chris Butler Managementaction – to beadvised when
completed
THE BOARD IS REQUESTED TOCONSIDER THIS ITEM CLOSED
The Board is asked to note that thisspecific action has been closed asper the discussion at the October
Board, but that out of thatdiscussion there is a related action
at Log 151

2BOARD OF DIRECTORS – Cumulative Action Log (public board)
LO
GN
UM
BE
R MINUTENUMBER
ANDORIGINATING
MEETINGDATE
ACTION(INCLUDING THE TITLE OF THE PAPER THAT GENERATEDTHE ACTION)
PERSONLEADING
BOARDMEETING TO
BEBROUGHTBACK TO /
DATE TO BECOMPLETED
BY
COMMENTS
ST
AT
US
144 14/144(September2014)
Implementing NICE guidance (PH48) – Smoking Cessation inMental Health Services (agenda item 10)
It was agreed that the matter should be referred to the Council ofGovernors for consideration, with sufficient time to allow consultationwith members, and that it will be brought back to the Board for furtherconsideration.
BeverleyMurphyAnthony
Deery
This is to beadded to theforward plan
for the Councilof Governors
and back toBoard in
January 2015
CLOSED AS A BOARD ACTION
This has been added to the Councilof Governors forward schedule and
is on the January Board ofDirectors’ agenda
146 14/151(September2014)
Complaint Summary Report (agenda item 14)
Dr Taylor welcomed the report but asked if it needs to come to eachBoard and whether receiving the report less often would allow theBoard to understand the trends more easily. Ms Murphy remindedthe Board that the report ‘Review of the NHS Hospital ComplaintsSystem – Putting patients back in the picture’ made therecommendation that the Board receives a report on complaints ateach of its meetings. However, Ms Murphy suggested that theremay be a different way in which the information can be presented. Itwas agreed that Mr Griffiths, Mr Butler and Ms Murphy would look atthe frequency and reports.
FrankGriffiths /
Chris Butler /Anthony
Deery
Managementaction – to beadvised when
completed
THE BOARD IS ASKED TOCONFIRM THAT IT IS ASSUREDTHAT THIS IS NOW COMPLETED
There is a summary report sent toeach Board meeting with a fullerreport to the Board each quarter.
148 14/168(October2014)
The Chief Executive’s Report (agenda item 6)
Mr Butler presented his Chief Executive’s report and drew attentionto two key documents for the NHS these being the Five YearForward View published by NHS England, and also the Governments“Achieving better Access to Mental Health by 2020”. Mr Butler notedthat the key elements of these two reports would be folded into theTrust’s business plans, and also suggested that a paper be broughtto the Board which set out the short-term tactical considerations.
Chris Butler December2015
THE BOARD IS REQUESTED TOCONSIDER THIS ITEM CLOSED
A paper was provided to theDecember Board meeting followingwhich the nature of the action waschanged and is now listed at Log
163

3BOARD OF DIRECTORS – Cumulative Action Log (public board)
LO
GN
UM
BE
R MINUTENUMBER
ANDORIGINATING
MEETINGDATE
ACTION(INCLUDING THE TITLE OF THE PAPER THAT GENERATEDTHE ACTION)
PERSONLEADING
BOARDMEETING TO
BEBROUGHTBACK TO /
DATE TO BECOMPLETED
BY
COMMENTS
ST
AT
US
149 14/168(October2014)
The Chief Executive’s Report (agenda item 6)
With regard to the Care Act Dr Taylor asked how the new carers’entitlements would be publicised and communicated through theTrust. Mr Butler noted that in Leeds there had been a lot of workdone with Carers’ Leeds, but that in York he noted the need for thisto be looked at in greater detail. Mr Butler agreed to bring somethingback to a future meeting.
Chris Butler ManagementAction– to beadvised when
completed
COMPLETED
This has been communicated as aTrustwide email to staff so they can
appropriately advise carers andbring this to their attention
150 14/169(October2014)
Bootham Park Hospital and Lime Trees Update Report (agendaitem 8)
Mr Wrigley-Howe noted again his concern that there is no cleartimeline for the completion of the business plan and then the work inrespect of Bootham Park Hospital (BPH). Mr Wrigley-Howe notedthe contractual obligations of NHS Property Services Ltd (NHS PS)and suggested the need for further legal advice to be taken as towhat course of action may be open to the Trust to ensure thatpartners carry out their obligations. This view was supported byother non-executive directors.
Dawn Hanwell ManagementAction – to beadvised when
completed
THE BOARD IS REQUESTED TOCONSIDER THIS ITEM CLOSED
A similar action has been listed atLog 160
151 14/169(October2014)
Bootham Park Hospital and Lime Trees Update Report (agendaitem 8)
Mr Woodhouse suggested that the matter should be escalated to themost senior authority with responsibility for NHS PS to highlight thedifficulties encountered by the Trust in expediting a matter for whichit has legal responsibility but little ability to influence the overallprocess. This matter was discussed in some detail by the Board andit was suggested that any letter should be couched in terms of beingan exemplar/case study of the difficulties encountered in workingwithin the matrix of partnership arrangements. The Board supportedthis approach.
Dawn Hanwell ManagementAction – to beadvised when
completed

4BOARD OF DIRECTORS – Cumulative Action Log (public board)
LO
GN
UM
BE
R MINUTENUMBER
ANDORIGINATING
MEETINGDATE
ACTION(INCLUDING THE TITLE OF THE PAPER THAT GENERATEDTHE ACTION)
PERSONLEADING
BOARDMEETING TO
BEBROUGHTBACK TO /
DATE TO BECOMPLETED
BY
COMMENTS
ST
AT
US
152 14/169(October2014)
Bootham Park Hospital and Lime Trees Update Report (agendaitem 8)
Mr Woodhouse also asked the executive team to provide a paper atthe January Board which sets out the timescales and actions toensure that the risk will be mitigated and the outcomes expected aredelivered.
Jill Copeland January 2015 THE BOARD IS ASKED TOCONFIRM THAT THIS SHOULD BE
CLOSED AS A STANDALONEACTION
The Board is asked to support thisnot coming back as a standalone
paper as the timescales and actionswill be folded into the CQC action
plan
153 -155
14/170(October2014)
Operational Plan Implementation Quarter 2 Report (agenda item9)
The Board asked for the following amendments to be made to thereport:
The consequence of not delivering the cost improvementplans and suggested that a narrative in respect of this shouldbe included in future reports
For the RAG rating it would be helpful to show thepercentage achievement within the rating to provideclarification as to the progress
There should be a financial report for each project orprogramme which is shown separately to the overall financialposition of the Trust in order to assess if these are deliveringthe expected outcomes and savings
Jill Copeland January 2015 THE BOARD IS ASKED TO NOTETHAT THESE POINTS HAVE BEENADDRESSED IN THE QUARTERLY
REPORT AND IS ASKED TOCONFIRM THAT THIS ACTION
SHOULD BE CLOSED

5BOARD OF DIRECTORS – Cumulative Action Log (public board)
LO
GN
UM
BE
R MINUTENUMBER
ANDORIGINATING
MEETINGDATE
ACTION(INCLUDING THE TITLE OF THE PAPER THAT GENERATEDTHE ACTION)
PERSONLEADING
BOARDMEETING TO
BEBROUGHTBACK TO /
DATE TO BECOMPLETED
BY
COMMENTS
ST
AT
US
156 14/171(October2014)
Verbal Report from the Chair of the Quality Committee for themeeting held 9 October 2014 (agenda item 10)
Mr Woodhouse recommended that one of the Board away days wasused to discuss the matters of compulsory training, appraisals andCare Programme Approach in order to agree an action plan for eachof these.
FrankGriffiths /
Susan Tyler
This actionneeds to betransferred
into the BoardTimeoutschedule
157 14/177(October2014)
Safer Staffing Report August and September 2014 (agenda item14)
Ms Murphy noted that some of the issues in August were around thelevel of leave agreed for staff and that work is ongoing to look atwhat could be done differently to ensure levels are not compromisedand manage any risks. The Board discussed this matter in somedetail. Concern was expressed at the level of staffing on some of thewards and asked what the consequence was of managers notensuring adequate levels. It was concluded that the executive teamshould look at the issues raised by the Safer Staffing Report and theareas of concern to agree what more should be done and what mightneed to be done differently to address these.
AnthonyDeery
Action for ET TO BE CLOSED AS A BOARDACTION
This has been passed to ET so itcan look at the issues in further
detail
158 14/178(October2014)
Complaint Summary Report (agenda item 15)
Mr Woodhouse asked for the next substantive report to have a briefsummary of the new complaints system and how this will be morebeneficial for service users.
AnthonyDeery
January 2015 THE BOARD IS ASKED TOCONSIDER THIS ACTION CLOSED
A report on this has been includedin the report to the January Board

6BOARD OF DIRECTORS – Cumulative Action Log (public board)
LO
GN
UM
BE
R MINUTENUMBER
ANDORIGINATING
MEETINGDATE
ACTION(INCLUDING THE TITLE OF THE PAPER THAT GENERATEDTHE ACTION)
PERSONLEADING
BOARDMEETING TO
BEBROUGHTBACK TO /
DATE TO BECOMPLETED
BY
COMMENTS
ST
AT
US
159 14/181(October2014)
Employer Based Awards / Clinical Excellence Awards (agendaitem 18)
Prof Thompson questioned the impact of the awards on therecruitment of consultants. Dr Isherwood outlined some of the othertypes of reward schemes being offered by other Trust’s and notedthat these did have a direct impact on recruitment and retention.Prof Thompson also suggested that such a scheme should beopened up to other members of staff. There was support for theExecutive Team to look at other schemes that may be available toother groups of staff and also to look at those hard to recruit topositions and what else can be done to encourage applicants. Itwas suggested that this be returned to the Board in 6 months time.
Susan Tyler June 2015
160 14/195(December2014)
Bootham Park Hospital and Lime Trees Update Report (agendaitem 6)
In summary Mr Griffiths noted that there was a high level offrustration within the Board in respect of the timeline. It was agreedthat Mrs Hanwell would take legal advice about the options open tothe Trust and would be advised as to whether it is prudent to write tothe organisations before the Board meets in January to set out anypotential course of action.
Dawn Hanwell Managementaction – to beadvised when
completed
COMPLETED
Legal advice has been taken
161 14/195(December2014)
Bootham Park Hospital and Lime Trees Update Report (agendaitem 6)
It was also agreed that Mr Griffiths would write to the chair of NHSPSto set out the view of the Board and seek assurance that the timelinewill be adhered to.
FrankGriffiths
ManagementAction – to beadvised when
completed

7BOARD OF DIRECTORS – Cumulative Action Log (public board)
LO
GN
UM
BE
R MINUTENUMBER
ANDORIGINATING
MEETINGDATE
ACTION(INCLUDING THE TITLE OF THE PAPER THAT GENERATEDTHE ACTION)
PERSONLEADING
BOARDMEETING TO
BEBROUGHTBACK TO /
DATE TO BECOMPLETED
BY
COMMENTS
ST
AT
US
162 14/196(December2014)
NHS Vale of York CCG – Tender Opportunity (agenda item 7)
Dr Taylor also noted the short timescale to complete the tenderdocumentation and noted the need for the executive team to look atthe governance and oversight arrangements for this. Mr Griffithsalso noted the need to ensure that the Council of Governors waslinked into this process.
Dawn Hanwell ManagementAction – to beadvised when
completed
COMPLETED
The governance process for theVale of York tender has been
defined
163 14/197(December2014)
‘Achieving Better Access to Mental Health Services by 2020’ –the proposed new standards – implications for the Trust(agenda item 8)
Mr Deery noted that there was much work ongoing in the Trust tolook at current activity and what needs to be done to meet these newstandards; that further guidance was awaited which would informthat work; and that a report would be brought back to a future Boardon the outcome of this work.
AnthonyDeery
The date backto Board is tobe determined
164 14/198(December2014)
Mental Capacity Act – Supreme Court Ruling (agenda item 9)
Mr Woodhouse noted that the ruling had been discussed at theMental Health Act Committee and that he had outlined to the Boardsome of the issues. He also noted that Ms Murphy had initiatedsome work in respect of this and that this might be used to inform thefurther work proposed. Mr Woodhouse noted the need for the MHACommittee to look at this again at its next meeting.
AnthonyDeery
For the MentalHealth ActCommittee
CLOSED AS A BOARD ACTION
This has been passed to the adminsupport for the committee to be
added to its forward agendaplanning

8BOARD OF DIRECTORS – Cumulative Action Log (public board)
LO
GN
UM
BE
R MINUTENUMBER
ANDORIGINATING
MEETINGDATE
ACTION(INCLUDING THE TITLE OF THE PAPER THAT GENERATEDTHE ACTION)
PERSONLEADING
BOARDMEETING TO
BEBROUGHTBACK TO /
DATE TO BECOMPLETED
BY
COMMENTS
ST
AT
US
165 14/198(December2014)
Mental Capacity Act – Supreme Court Ruling (agenda item 9)
The Board received a formal report on the Supreme Court Rulingand noted that work is still ongoing to look at the implications of thisfor the Trust and its service users and that a report would be broughtback to the Board in March 2015 in respect of the outcome of thiswork.
AnthonyDeery
March 2015
166 14/199(December2014)
LYPFT and Leeds City Council Adult Social Care IntegratedDelivery Model (agenda item 10)
Dr Taylor welcomed this initiative. She noted that supporting thiswork would be the need to carry out modelling not only of care, butalso of the finances which would need to take account of whichorganisation carries the risk. Dr Taylor suggested that this couldcome to the Finance and Business Committee so it can be looked atin greater detail than is possible at Board. Ms Copeland welcomedthis approach.
Jill Copeland For theFinance and
BusinessCommittee
CLOSED AS A BOARD ACTION
This has been passed to the adminsupport for the committee to be
added to its forward agendaplanning

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Refreshed Workforce Development Strategy
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Susan Tyler, Director of WorkforceDevelopment
STRATEGIC:
PAPER AUTHOR: Susan Tyler, Director of WorkforceDevelopment
GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)G1 People achieve their agreed goals for improving health and improving lives
G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)SO1 We provide excellent quality, evidence-based, safe care that involves people and promotes
recovery and wellbeingSO2 We work with partners and local communities to improve health and lives
SO3 We value and develop our workforce and those supporting us SO4 We provide efficient and sustainable services
SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individualsOther – not yet a public documentMatters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
8

SUMMARY:
The Workforce Development Strategy 2014-2106 was approved by the Board of Directorsin May 2013. The strategy has been refreshed and updated to take account of progressmade to date and to reflect the strategic aims of the Trust and The Workforce Directoratefor the next two years.
A copy of the refreshed Workforce Development Strategy is attached showing trackedchanges. The refreshed Workforce Development Strategy was agreed by the QualityCommittee at its last meeting on 11 December 2014.
RECOMMENDATIONS:
The Board of Directors is asked to receive and note the changes to the WorkforceDevelopment Strategy.

1
WORKFORCE
DEVELOPMENT STRATEGY
20143 – 2016
Version 13
Refreshedvised 16 September 2014

2
INDEXPage
Glossary of Terms 3Executive Summary 4
1. Introduction 62. Trust Ambition 63. Context 6
3.1 63.2 73.3 73.4 8
4. Purpose 85. NHS Constitution - Staff Pledges 8
5.1 95.2 Our Culture 10
6. Key Workforce Aims 116.1 Strategic Workforce Change 116.2 Employee Engagement and Communication 136.3 Improving Health, Well-being and Attendance 1546.4 Maintain effective workforce planning and IT 176.5 Workforce Policy, Practice and Reward 1876.6 Learning and Development 20196.7 Supporting Plans and Strategies 231
APPENDICES
Appendix 1 Trust Values 243
Appendix 2 Actions Summary (14/15) 254
Appendix 3 Career Framework (Clinical) 2730
Appendix 4 Career Framework (Non-clinical) 2932
Appendix 5 Progress Measurement 31 Formatted: Left, Space After: 10 pt,Line spacing: Multiple 1.15 li

3
GLOSSARY OF TERMS
AFC Agenda For ChangeASC Andrew Simms CentreCIP Cost Improvement PlanCIPD Chartered Institute of Personnel DevelopmentEAP Employee Assistance ProgrammeEQi Emotional IntelligenceESR Electronic Staff RecordET Executive TeamFFTF Fit For The FutureHESS Health Education Support ServiceHSE Health and Safety ExecutiveILM Institute for Leadership and ManagementJLNC Joint Local Negotiating CommitteeJNCC Joint Negotiating Consultation CommitteeLETB Local Education and Training BoardMARS Mutually Agreed Resignation SchemeMBTI Myers Briggs Type IndicatorOD Organisational DevelopmentOEP Organisational Effectiveness ProgrammeOH Occupational HealthPDP Personal Development PlanPMVA Profession and Management of Violence and AggressionPRF Personal Responsibility FrameworkQC Quality CommitteeRAPID Recovery Aimed Personalised Interventions DriveSG Strategic GoalSHRM Senior Human Resources ManagerSO Strategic ObjectiveSPA Single Point of AccessSTAR Staff Achievement and Recognition SchemeTNA Training Needs AnalysisWFD Workforce DevelopmentWSG Workforce Steering Group

4
WORKFORCE DEVELOPMENT STRATEGY 2013 TO 2016
Executive Summary
The purpose of this strategy is to support and underpin the Trust’s Strategic Plan. A
summary of the Strategic Framework for 2013-2016 is shown below:-
Our Trust Strategy
Purpose
Improving health, improving lives
NHS Values
Respect and
dignity
Commitment
to quality of
care
Working
together
Improving
lives
Compassion Everyone
counts
Ambition
Working in partnerships, we aspire to provide excellent mental health and learning
disability care that supports people to achieve their goals for improving health and
improving lives.
Goals
1 People achieve their
agreed goals for
improving health and
improving lives
2 People experience safe
care
3 People have a positive
experience of their care
and support
Strategic Objectives
1 Quality and outcomes We provide excellent quality, evidence-based, safe
care that involves people and promotes recovery and
wellbeing.
2 Partnerships We work with partners and local communities to
improve health and lives
3 Workforce We value and develop our workforce and those
supporting us
4 Efficiency and sustainability We provide efficient and sustainable services
5 Governance and
compliance
We govern our Trust effectively and meet our
regulatory requirements.
The actions outlined in this document support Strategic Goal 3, Workforce. We Value andDevelop our Workforce and Those Supporting Us, however the Workforce aimshighlighted within the Strategy link to all strategic goals.
When all strategic aims included in this strategy have been achieved we will
Have a ‘healthy’ organisational culture where everyone feels confident to speak up,be listened to and play an active part in ‘developing services to meet the needs ofservice users.’

5
Have a workforce which is productive and cost-efficient, with an appropriate level ofskill and competence to deliver safe and high quality services and which is responsiveto ensure the sustainability of our service delivery model and meet the needs of thechanging NHS landscape.
Support the health and well-being of the workforce, by developing new and innovativeapproaches to managing attendance and well-being especially in relation to mentalhealth related conditions.
Have developed an inclusive leadership style which reflects the Trust’s values fromthe “Board to Frontline” and empowers all staff to be jointly accountable for theservices we provide.
We acknowledge that the Trust will need to adopt a developmental approach to achieve thestrategic aims highlighted within this strategy. The strategy will be updated and reviewedannually to respond to organisational needs.The Strategy covers a number of key workforce aims that will enable us to deliver theStrategy. These are
Strategic Workforce Change Employee Engagement and Communication Improving Health, Well-being and Attendance Workforce Planning, Information and Supporting Technology Workforce Policy, Practice and Reward Learning and Development
How will we measure our progress against the workforce aims
These will be measured using the workforce targets outlined in the strategy. See Appendix5 for a summary.
Acknowledgement
We would like to thank all members of the Trust’s staff who contributed to and commentedon the strategy during its development and review.

6
Workforce Development Strategy 2013 - 2016
1. Introduction
This strategy describes how the Trust will improve performance through its workforce overthe next 3 years. The Trust recognises that its workforce and volunteers are its greatestasset and successful implementation of the strategy will demonstrate this commitment bycreating an organisation that values and develops its workforce and those who support theTrust.
2. Trust Ambition
Our Trust ambition is that by:-
Working in partnerships we aspire to provide excellent mental health and learningdisability care that supports people to achieve their goals for improving health andimproving lives.
The Workforce and Organisational Development Strategy will support this vision by:
Developing a ‘healthy’ organisational culture where everyone feels confident to speakup, be listened to and play an active part in ‘developing services to meet the needs ofservice users.’
Developing a workforce that is motivated, productive and cost-efficient, withappropriate levels of skill and competence to deliver safe and high quality servicesand which is responsive to ensure the sustainability of our service delivery model andmeet the needs of the changing NHS landscape.
Supporting the health and well-being of the workforce, by developing new andinnovative approaches to managing attendance and well being especially in relation tomental health related conditions.
Having an organisational leadership style which reflects the Trust’s values from the“Board to Frontline” and empowers all staff to be jointly accountable and responsiblefor the services we provide.
Promoting, supporting and recognising innovation and good practice throughrecognition and talent management
3. Context
3.1 Outlined within the Trust’s Strategic Plan are a number of challenges which willimpact on the Trust’s workforce. These are:-
Ensuring the Trust remains a viable concern to enable a viable financial risk rating infuture
Delivering a substantial cost improvement plan
Increasing workforce productivity and improving quality

7
Implementing service development plans; integrating clinical services and patientchoice
Increasing competition and market testing
Estates reconfiguration and rationalisation.
Increasing flexibility and developing new and different job roles to meet futuredemands and partnership working across sectors
This will inevitably lead to challenges for the staff we employ and changes to pay, conditionsand ways of working. We will do our utmost to support staff through these changes and dealwith staff in a fair and consistent way.
This strategy applies to all Trust services, all locations and all staff groups includingvolunteers.
3.2 The pace of change has and will continue to be fast-paced and challenging, theapproach outlined in this strategy, being consistent with our Trust values (see Appendix 1)will assist in ensuring that we maintain a positive employment relations climate in the future.
3.3 The Trust currently employs 3,315293 staff. The Trust’s annual turnover is £171 millionand serves a population covering Leeds, York, Selby, Tadcaster and Easingwold.Approximately 80% (£129m) of the Trusts’ annual budget is spent on workforce costs.
Our Trust is the main provider of specialist mental health and learning disability services in
Leeds, York and parts of North Yorkshire (Selby, Tadcaster and Easingwold). We also
provide some specialist services across the whole of North Yorkshire, across the Yorkshire
and Humber region and nationwide.
We offer services to people aged 18 and over who need support and treatment to:
Live with a wide range of mental health problems, from depression, anxiety and OCD(obsessive compulsive disorder), to dementia, bipolar disorder, schizophrenia andpersonality disorder
Live with mental health problems whilst in contact with the criminal justice system
Live with other issues such as addictions, eating disorders, or physical problems withpsychological causes; or need the support of our gender identify service
Have a learning disability, often with challenging behaviour or complex physicalhealth
Deaf service
We offer services in York and North Yorkshire to children and young people under the age of18 who have emotional or behavioural problems or other mental health difficulties. Ourservices for deaf children cover the North of England.
We provide services to a diverse and changing population. There are marked variations inethnic diversity within the areas we serve; for example Leeds is now home to over 140
Formatted: Font: (Default) Arial

8
ethnic groups with an increasing black and minority ethnic (BME) population of 19% whereasthe city of York BME population is 9.8% and within Selby is 5.6%.
We also offer services to children and young people under the age of 18 who have
emotional or behavioural problems or other mental health difficulties.
3.4 In addition, the Trust currently has over 250 volunteers who we recognise as animportant element of our workforce and who deliver an essential service to enhance theexperience of people using our services. There is a dedicated Voluntary Services teamwhose role is to recruit and support the development of volunteers in positions throughoutthe Trust that they would like to work or develop in. Over 40% of our volunteers have directexperience of using our services and from their feedback volunteering is therapeutic tosupport their recovery and to support them to achieve their goals.
People are motivated to volunteer for our Trust for many reasons which include:
Wanting to give something back after they or their family have benefited fromservices
Exploring a career or to enhance their experience in health care
Wanting to develop or maintain skills and experience
Wanting to help and improve and develop specific services
4. Purpose
The document sets out the broad Workforce and Organisational Development Strategy forthe next 3 years. This will provide a framework to support the Trust’s Strategic Plan.
The document identifies further actions necessary to implement the Workforce andOrganisational Development Strategy. These are captured as ‘FURTHER ACTIONS’ underthe respective subject heading. They are summarised in Appendix 2.
5. NHS Constitution – Staff Pledges
In addition the NHS Constitution includes the following pledges to staff:-
Staff Pledge 1: To provide all staff with clear roles and responsibilities and rewarding jobsfor teams and individuals that make a difference to patients, their familiesand carers and communities.
Staff Pledge 2: To provide all staff with personal development, access to appropriatetraining for their jobs and line management support to succeed.
Staff Pledge 3: To provide support and opportunities for staff to maintain their health,well-being and safety.

9
Staff Pledge 4: To provide support and opportunities for staff to maintain their health,wellbeing and safety
Staff Pledge 5: The NHS commits to engage staff in decisions that affect them and theservices they provide, individually, through representative organisationsand through local partnership working arrangements. All staff will beempowered to put forward ways to deliver better and safer services forpatients and their families.
Staff Pledge 6: The NHS commits to have a process for staff to raise an internalgrievance.
Staff Pledge 7: The NHS commits to encourage and support all staff in raising concernsat the earliest reasonable opportunity about safety, malpractice orwrongdoing at work, responding to and, where necessary, investigatingthe concerns raised and acting consistently with the Public InterestDisclosure Act 1998.
The constitution also includes a set of responsibilities for staff. These are not legally bindingbut enable staff to have a clear understanding of what is required of them:-
Staff should aim to maintain the highest standards of care and service, takingresponsibility not only for the care you personally provide, but also for your widercontribution to the aims of your team and the NHS as a whole.
Staff should aim to take up training and developmental opportunities provided overand above those legally required of your post
Staff should aim to be open with patients, their families, carers or representatives,including if anything goes wrong, welcoming and listening to feedback andaddressing concerns promptly and in a spirit of co-operation. You should contributeto a climate where the truth can be heard and the reporting of and learning fromerrors is encouraged.
The strategic aims outlined will support the staff pledges in the NHS Constitution.
5.1 Although this strategy is predominantly concerned with activities relating to ServiceObjective 3, Workforce, it also impacts upon the achievement of other strategic goals andobjectives, as all Trust services are delivered through our employees and voluntary staff.Progress on the Strategy will be measured against the key performance indicators.
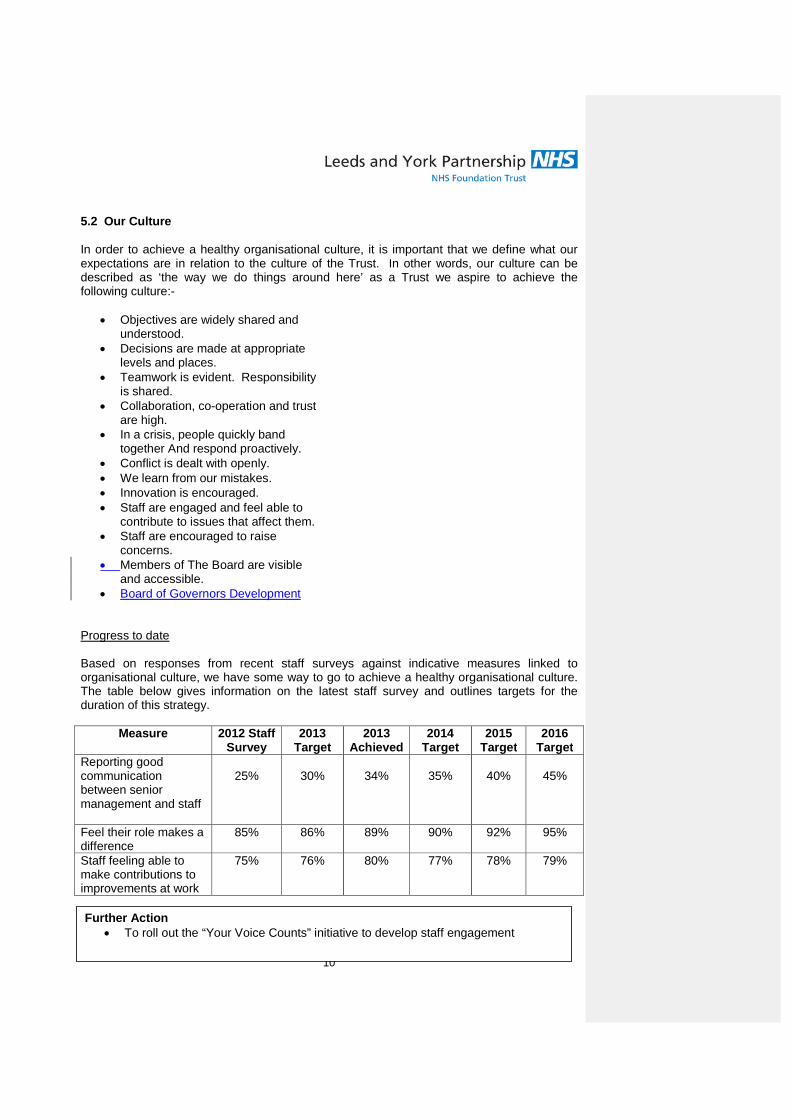
10
5.2 Our Culture
In order to achieve a healthy organisational culture, it is important that we define what ourexpectations are in relation to the culture of the Trust. In other words, our culture can bedescribed as ‘the way we do things around here’ as a Trust we aspire to achieve thefollowing culture:-
Objectives are widely shared andunderstood.
Decisions are made at appropriatelevels and places.
Teamwork is evident. Responsibilityis shared.
Collaboration, co-operation and trustare high.
In a crisis, people quickly bandtogether And respond proactively.
Conflict is dealt with openly. We learn from our mistakes. Innovation is encouraged. Staff are engaged and feel able to
contribute to issues that affect them. Staff are encouraged to raise
concerns. Members of The Board are visible
and accessible. Board of Governors Development
Progress to date
Based on responses from recent staff surveys against indicative measures linked toorganisational culture, we have some way to go to achieve a healthy organisational culture.The table below gives information on the latest staff survey and outlines targets for theduration of this strategy.
Measure 2012 StaffSurvey
2013Target
2013Achieved
2014Target
2015Target
2016Target
Reporting goodcommunicationbetween seniormanagement and staff
25% 30% 34% 35% 40% 45%
Feel their role makes adifference
85% 86% 89% 90% 92% 95%
Staff feeling able tomake contributions toimprovements at work
75% 76% 80% 77% 78% 79%
Further Action To roll out the “Your Voice Counts” initiative to develop staff engagement

11
6. Key Workforce Aims
Strategic Objective 3: We value and develop our workforce and those supporting usdemonstrates a commitment that our workforce is integral to the success of our organisation.
There are clear links between good employment practices and business outcomes. Ourgoal is to create an environment where employees are valued and rewarded, areappropriately trained and developed, regularly appraised and effectively managed which willhave a positive impact of on our service users. The strategy outlines key workforce aimsthat will support us in our overall goal, and these are outlined under the following headings:
Strategic workforce change
Employee engagement
Improving Health, well-being and attendance
Workforce planning, information and supporting technology
Workforce Policy and Reward
Learning and People Development
6.1 Strategic Workforce Change
In order to maintain our position as a high performing organisation in a competitiveenvironment we must strike a balance between reducing workforce costs whilst sustainingand improving the quality of the services we deliver.
To support this Strategic Workforce Change we will implement the Career Framework inAppendix 3 and Appendix 4 as the opportunity arises through service redesign and otherstructure changes. Workforce reduction will be managed wherever possible via naturalwastage and turnover. The Trust will do its utmost to redeploy staff affected byorganisational change and only in exceptional circumstances, when all other avenues havebeen explored, will the Trust resort to compulsory redundancy. The Trust may utilise eitherMARS (Mutually Agreed Resignation Schemes) and/or voluntary redundancy/earlyretirement schemes as appropriate.
We take steps to effectively engage staff at the start of the management of changeprocess and continually evaluate the change processes to take account of feedbackfrom staff who have undergone change and where necessary to make changes topolicies and processes to minimise the levels of uncertainty experienced by affectedstaff. We will use Staff Survey outcomes and barometer surveys to measureprogress on this aim.
We will support and develop people who volunteer within our services to access paidemployment within our Trust.
We recognise that Service Improvement and New Ways of Working will be crucial toquality of care and outcomes delivered to our service users. The Trust has adopted

12
a Lean6Sigma model for service improvement and will continue to use this model tosupport organisational change and care pathway development.
In conjunction with the Informatics Department and Estates Department, we willdevelop workforce policies that support mobile and remote working practices wherejob roles and design support such ways of working.
The need to reduce workforce costs applies to all elements of the Trust workforceincluding medical staff and the Trust will review existing workforce costs of medicalstaff and compare these to peer employers. Consideration will be given to numbersof additional programmed activities paid to consultant medical staff and to reviewlocal CEA procedures;
To support management of workforce costs, the Trust will, on occasions, use theoption of either ‘spot salaries’ or reduced incremental scales for posts at Bands 8aand above for either external or internal appointments.
The Trust’s turnover rate will be monitored to ensure that this remains at anacceptable range of between 10% and 15%. Where problems are identified we willwork with Teams and Departments to manage retention.
To enable the Trust to respond in a competitive market we will develop a rewardframework that will enable us to attract and retain talent. The frameowork will utilisethe flexibilities available to the Trust as a Foundation Trust by Dec. ’15.
Develop an effective Workforce Planning system to support service areas.
Ensure service areas have access to key management information related toworkforce to enable effective management and delivery of high quality services.
Continue to implement and develop e-rostering to support effective deployment ofstaff and effective vacancy management.
To support and promote flexibility and the development of new roles to supportcollaborative working across the health and social care sectors.
For Action Develop a reward framework using FT Flexibilities to attract, retain and reward
talented and high performing employees. and retain talent.
Formatted: Normal, Justified, Tabstops: 0.75 cm, Left
Formatted: Font: (Default) Arial
Formatted: Font: (Default) Arial
Formatted: Font: (Default) Arial
Formatted: Font: (Default) Arial
Formatted: Font: (Default) Arial
Formatted: Font: (Default) Arial

13
Where we are Now and how we will Measure Progress
Target 2014 Achieved2014
Target 2015 Target2016
In 2013 Average earnings LYPFT is£33,200
£33,000 £30.2k £29,000 £27,000
Trust Turnover Rate 10-15% 12% 10-15% 10-15%
6.2 Organisational Development, Engagement and Communication
The Chartered Institute of Personal Development defines Organisational Development (OD)as ‘planned and systematic approach to enabling sustained organisation performancethrough the involvement of its people’.
We will strive to improve the way we engage our staff in decisions that affect them and willbuild on the work already undertaken to support employee engagement and will undertakethe following actions over the duration of the strategy to support the engagement andinvolvement agenda:-
The Your Voice Counts – Moving Forward Together Programme launched in July2014 will commence in September 2014 with two Ideas Implementation Groupsfocusing on key issues arising from the 2013 Staff Survey. The programme willlaunch an organisational development model aimed at increasing staff engagementacross the Trust by listening to staff, putting them at the centre of the change,focusing on action and developing sustainable solutions with staff. Feedback tomeasure levels of staff engagement will be utilised to identify areas where levels ofengagement can be improved. The data received will check progress and alsoinform future development of the programme.
We will continue to develop the capacity and capability of the Trust’s OD Cohort toenable them to support change and service development.
Board members will, continue to take every opportunity to directly engage with theservices and staff of the Trust.
We will continue to ensure that equality and diversity is at the heart of ourorganisational culture. We will continue to develop our equality analysis andmonitoring processes to support us to address inequalities where identified.
The Trust expects all staff to take responsibility for their actions and to work withcolleagues to resolve any issues that may have a negative effect on service users,carers, visitors and colleagues. We acknowledge that feedback suggests that thereis a culture of “blame and fear” in certain parts of the organisation. The PersonalResponsibility Framework will be further developed to support the concept of “jointaccountability”. In a large, complex, people centred organisation it is inevitable thatmistakes and failures will occur. The concept of joint accountability will ensure that
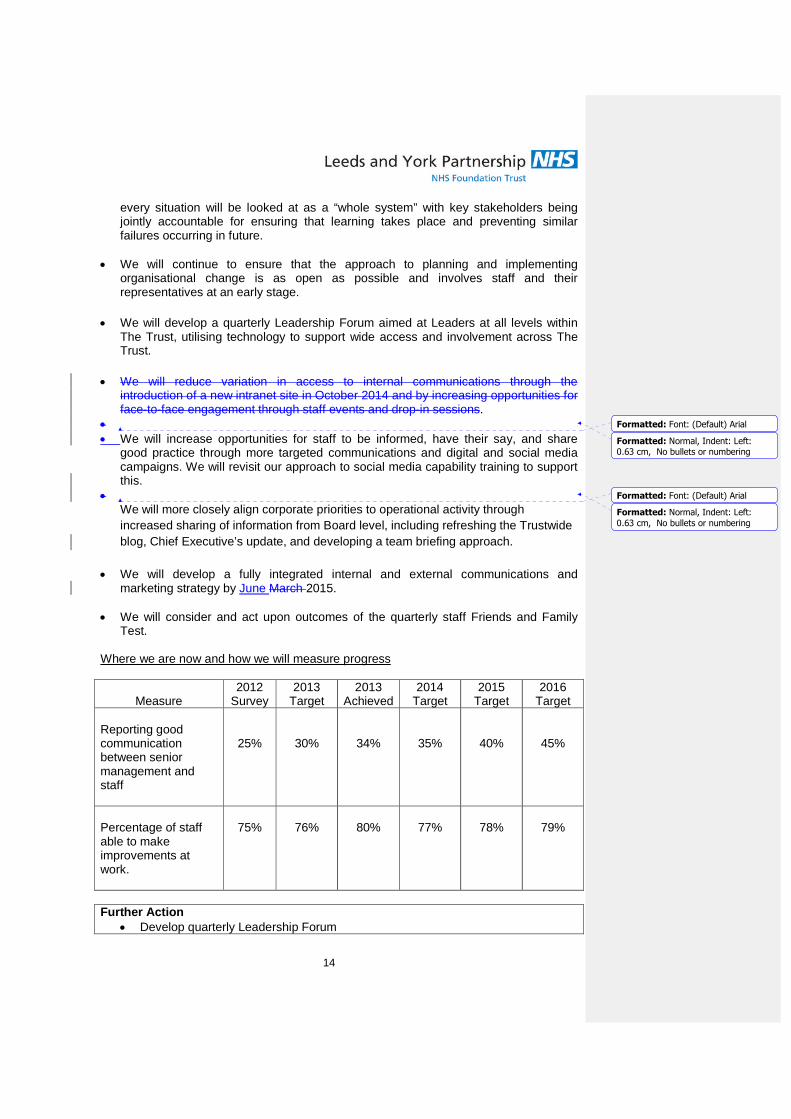
14
every situation will be looked at as a “whole system” with key stakeholders beingjointly accountable for ensuring that learning takes place and preventing similarfailures occurring in future.
We will continue to ensure that the approach to planning and implementingorganisational change is as open as possible and involves staff and theirrepresentatives at an early stage.
We will develop a quarterly Leadership Forum aimed at Leaders at all levels withinThe Trust, utilising technology to support wide access and involvement across TheTrust.
We will reduce variation in access to internal communications through theintroduction of a new intranet site in October 2014 and by increasing opportunities forface-to-face engagement through staff events and drop-in sessions.
We will increase opportunities for staff to be informed, have their say, and share
good practice through more targeted communications and digital and social mediacampaigns. We will revisit our approach to social media capability training to supportthis.
We will more closely align corporate priorities to operational activity through
increased sharing of information from Board level, including refreshing the Trustwide
blog, Chief Executive’s update, and developing a team briefing approach.
We will develop a fully integrated internal and external communications andmarketing strategy by June March 2015.
We will consider and act upon outcomes of the quarterly staff Friends and FamilyTest.
Where we are now and how we will measure progress
Measure2012
Survey2013
Target2013
Achieved2014
Target2015
Target2016
Target
Reporting goodcommunicationbetween seniormanagement andstaff
25% 30% 34% 35% 40% 45%
Percentage of staffable to makeimprovements atwork.
75% 76% 80% 77% 78% 79%
Further Action Develop quarterly Leadership Forum
Formatted: Font: (Default) Arial
Formatted: Normal, Indent: Left:0.63 cm, No bullets or numbering
Formatted: Font: (Default) Arial
Formatted: Normal, Indent: Left:0.63 cm, No bullets or numbering

15
Introduce new intranet by Oct. ‘14 Introduce Communications and Marketing Strategy by JuneMar ’15.
6.3 Improving Health, Well-being and Attendance
Providing a healthy work environment is conducive to creating high performing teams andindividuals that will support the delivery of the Trust vision. Our commitment to establishingan environment where staff feel good and function well both physically and mentally is setout in our Health and Well Being Action Plan. The level of health and well-being of theworkforce is a key indicator or organisational performance and service user outcomes.
The National Health and Wellbeing priorities are as follows and these are reflected in theTrust’s Health and Wellbeing Action Plan:-
Managing obesity
Smoking cessation
Supporting physical activity
Improving mental health.
The Trust has revised its Employee Wellbeing and Managing Attendance procedure which
aims to support staff who are unable to attend work through ill health and it also encourages
personal responsibility from staff in relation to their health and well-being. The procedure will
support the Trust in its aim to secure a 0.5% reduction in absence rates year on year and to
achieve and sustain an absence rate of 3.7% by April 2016.
We will undertake HSE stress assessments in areas on high levels of stress andwork with managers to take appropriate action to address the findings. We willencourage staff to assess their own personal resilience and develop personalsupporting strategies to cope with change
We will evaluate the impact of the stress management pathway introduced in July’14.
We will continue to work within the aims of Mindful Employer Charter and theJobcentre Plus ‘Two Ticks’ disability kite mark. The Mindful Employer Charterdemonstrates the Trust’s commitment to the employment of and support for staff withmental health conditions. The “Two Ticks” kite mark ensures that people with a longterm health condition or a disability are guaranteed an interview, if they meet theminimum criteria for any advertised role.
We will work with staff and Occupational Health professionals to develop innovativeapproaches to supporting staff with mental health conditions..

16
We will evaluate and continue to monitor and promote the effectiveness of the 24hour Employee Assistance Programme aimed at supporting staff in coping withpersonal change, bereavement and debt counselling.
We will continue to work towards delivery of The Trust’s health and well-being actionplan, developed via staff consultation.
We will undertake analysis to establish links between health and well-being issuesand role design.
We will fully implement First Care Absence Management Support by December2014.
We will participate in the Mentally Healthy Workplace pilot with the intention of rollingout training to our managers
We will develop our Staff Lived Experience Network and undertake a further nationalconference by Nov. ’15.
We will ensure that staff and managers have access to information via our intranetsite to support their health and wellbeing.
We will provide targeted support in relation to MSK absence utilising the Trust’sPhysiotherapist in both treatment and preventative measures.
We will continue to support staff to raise concerns through a targeted awarenesscampaign at both trust and team level
Where we are and how we will monitor progress
Target Q4 2014 2013Achieved
TargetQ4 2015
Target Q42016
Trust absence rate at March 20135.2% 4.7% 4.6% 4.2% 3.7%
Of the 5.2% absence, % due tostress related conditions at March2013:-
28%
25% 24.8% 20% 15%
Of the 5.2% absence, % due toMusco-skeletal related conditionsat March 2013:-
13.8%
11.8% 11.8% 10.8% 9.8%
Staff Survey Measure StaffSurvey2012
Target2013
2013Achieved
Target2014
Target2015
Target2016
% suffering work-relatedstress in the last twelve 48% 46% 58% 44% 43% 41%

17
months
Staff who reportexperience of physicalviolence from patientsrelatives or the public inlast twelve months
25% 20% 28% 18% 18% 15%
For Action Participate in the Mentally Healthy Workplace Pilot. Fully implement First Care Absence Management Programme by Dec. ’14.
6.4 Improve Maintain effective workforce planning and information systems, usingsupporting technology.
Phase 3 e-rostering commenced in February 2014 in York with a projectedcompletion date of June/July 2015. When all phases of e-rostering have beencompleted a review of the effectiveness and benefits realisation will be conducted.
Undertake a review of healthroster and increase benefits realisation.
As part of the Informatics Strategy, further work will be undertaken to utilisetechnology to reduce the need for excess travel, support remote working and ways ofimproving workforce productivity.
We will develop a local management dash board in conjunction with informatics tosupport performance management at local level by Dec. ’14.
We will develop a workforce plan for completion by June 2015 which will identifyworkforce requirements to meet The Trust’s Strategic Plan, with particular emphasison the impact of the ageing workforce.
We will develop and implement an effective workforce planning process to supportthe implementation of service delivery plans.
We will implement version 10 of Healthroster by January 2015
For Action
Develop Trust Workforce Plan by Jun. ’15.
Implement Local Workforce Management Dashboard by Dec. ’14.
Complete Phase 3 E-Rostering in York by Jul. ’15.
Undertake a review of Healthroster in increase benefits realisation.
Implement Version 10 of Healthroster by Jan 2015.
Formatted: Font: (Default) Arial
Formatted: Normal, Indent: Left:0.63 cm, Space After: 0 pt, Linespacing: single
Formatted: Font: (Default) Arial
Formatted: Normal, Indent: Left:0.63 cm, No bullets or numbering
Formatted: Font: (Default) Arial
Formatted: Left, Indent: Left: 1.27cm, Space After: 10 pt, Line spacing:Multiple 1.15 li, No bullets ornumbering, Tab stops: Not at 0.75 cm

18
6.5 Workforce Policy, Practice and Reward
We will undertake a cost/benefit analysis of whether it is cost-effective to maintain anin-house bank or whether consideration should be given to outsourcing thisarrangement or collaborating more closely with neighbouring Trusts/Local Authority.
We aim to recruit and retain high quality staff. Our approach to future recruitment willinvolve ‘values based’ pre-employment screening for all grades of staff.Strengthening this process will ensure that there is a congruence between individualsappointed and the values and behaviours of the Trust. The Trust will continue toparticipate in the national VBR project.
All staff should expect to have clear goals in relation to what is expected of them andreceive clear feedback about their performance. The appraisal process will bereviewed to ensure it meets individual and organisational needs. We will alsodevelop a 360 review process linked to Trust values to supplement the appraisalprocess.
Our workforce profile suggests that 29% of our staff are aged over 50 and there areonly 0.1% employees under the age of 20. It is important that the Trust develops anage diverse workforce. To support this aim well we will further expand the Trust’sApprenticeship Programme into Care Services and Admin Support roles. Theseschemes by their nature will attract a younger workforce, but they are open to allages. This will enable the Trust to grow and develop its own talent.
We will endeavour to ensure that the Trust workforce profile reflects the communitiesthat we serve and we will take steps to further understand the local labour marketand take positive action initiatives to improve representation in the workforce.
In conjunction with the Informatics Department and Estates Department, we willdevelop workforce policies that support mobile and remote working practices wherejob roles and design support such ways of working.
We will continue to utilise the monthly STAR scheme (Staff Achievement andRecognition Scheme) to recognise the outstanding contribution and efforts ofindividual members of staff.
We will take steps to develop leaders and managers in management skills in orderfor them to take more ownership of their team issues.
We will implement the NHS Equality Delivery System 2 linked to key organisationalpriorities.
We will work with Trade Union colleagues to review and strengthen partnershipworking arrangements and improve communication and engagement.
19
We will implement a clear and transparent Trust career framework which clearlyarticulates the grading structure and roles for each post within the Agenda forChange pay structure. Generic job descriptions and job titles will be developed tomatch each band within the Framework. The proposed Career Framework for bothclinical and non-clinical grades is shown at Appendix 3 and Appendix 4. The Trustwill adopt an incremental approach to implementing the career framework linked toreview of organisational structures; cost improvement plans.
. We will continue to engage and reward our volunteers through our quarterly
Volunteer Forum, bi-annual volunteer newsletter and annual volunteer celebrationevent.
We will continue to undertake an annual satisfaction survey with all our volunteersand implement annual service development plans based on their feedback.
We will develop a framework for developing managing talent within LYPFT by June2015.
We will ensure that we have effective employment procedures in place which arecompliant with employment legislation, adhere with good employment practice andprovide best value for money.
We will review our levels of vacancies to ensure these remain between 4-5%annually.
Formatted: Font: (Default) Arial
Formatted: Left, Indent: Left: 1.27cm, Space After: 10 pt, Line spacing:Multiple 1.15 li, No bullets ornumbering, Tab stops: Not at 0.75 cm
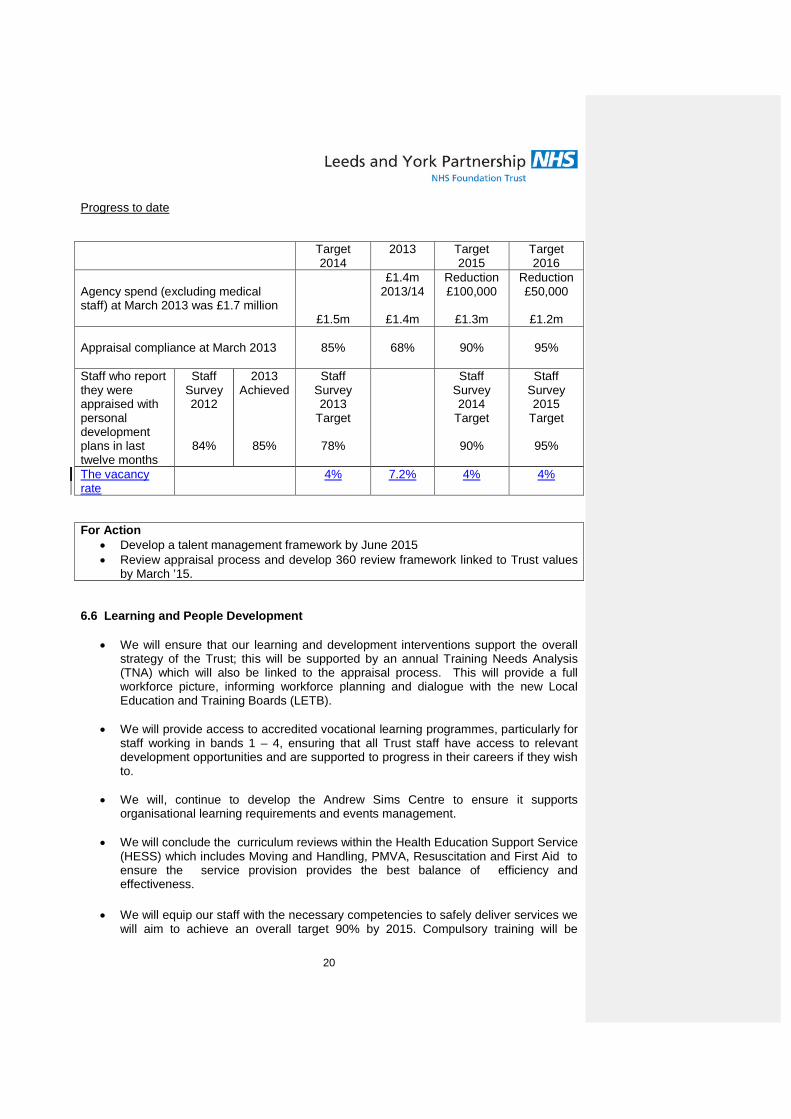
20
Progress to date
Target2014
2013 Target2015
Target2016
Agency spend (excluding medicalstaff) at March 2013 was £1.7 million
£1.5m
£1.4m2013/14
£1.4m
Reduction£100,000
£1.3m
Reduction£50,000
£1.2m
Appraisal compliance at March 2013 85% 68% 90% 95%
Staff who reportthey wereappraised withpersonaldevelopmentplans in lasttwelve months
StaffSurvey2012
84%
2013Achieved
85%
StaffSurvey2013
Target
78%
StaffSurvey2014
Target
90%
StaffSurvey2015
Target
95%
The vacancyrate
4% 7.2% 4% 4%
For Action Develop a talent management framework by June 2015 Review appraisal process and develop 360 review framework linked to Trust values
by March ’15.
6.6 Learning and People Development
We will ensure that our learning and development interventions support the overallstrategy of the Trust; this will be supported by an annual Training Needs Analysis(TNA) which will also be linked to the appraisal process. This will provide a fullworkforce picture, informing workforce planning and dialogue with the new LocalEducation and Training Boards (LETB).
We will provide access to accredited vocational learning programmes, particularly forstaff working in bands 1 – 4, ensuring that all Trust staff have access to relevantdevelopment opportunities and are supported to progress in their careers if they wishto.
We will, continue to develop the Andrew Sims Centre to ensure it supportsorganisational learning requirements and events management.
We will conclude the curriculum reviews within the Health Education Support Service(HESS) which includes Moving and Handling, PMVA, Resuscitation and First Aid toensure the service provision provides the best balance of efficiency andeffectiveness.
We will equip our staff with the necessary competencies to safely deliver services wewill aim to achieve an overall target 90% by 2015. Compulsory training will be

21
delivered through a number of blended learning arrangements including E-learningand where appropriate face to face training.
We will continually promote a culture of learning through providing a bespoke clinicaladvisory service though the Health Education Support Service, responding toemerging organisational needs and cascading the learning from incidents
We will develop team and individual coaching to support transformation and culturalintegration and engagement.
We will develop and maintain a Trust wide Education, Training and DevelopmentCurriculum by December 2014.
We will develop in-house expertise in Technology Enhanced Learning (TEL),providing a responsive and cost efficient service and enabling the development ofbespoke TEL solutions to identified Trust training needs.
As a Teaching Trust we will continue to work with medical schools, universities andcolleges to provide education programmes for aspiring doctors, nurses and otherhealth professionals. We remain deeply committed to medical training anddeveloping clinical knowledge and skills.
The Trust will continue with its aspiration to become a learning organisation. Thissupports the development of a healthy culture within the Trust. We will continue toutilise a blended approach to Learning and Development through the following:-
E-learning and other learning technologies
Distance learning
Blended learning solutions
Coaching (team and individual)
Mentoring
Shadowing
Stretch assignments
Secondment opportunities.
Bespoke learning solutions after learning from incidents.
Mediation.
We will continue to monitor staff access to learning and developmentopportunities to ensure that there is equitable access for staff throughout theorganisation.
We will further develop learning opportunities for people who volunteer within ourservices based on responses from our annual volunteer survey.
We will streamline our Induction Procedures to ensure all new starters have theprerequisite IT access, compulsory training and knowledge to be proficient intheir role from joining their department by June ’15.

22
We will develop leadership and management capability through engagingmanagers in bespoke accredited development programmes approved by internalstakeholders, delivered through the Trust Leadership Centre in partnership withsenior leaders within the organisation, whilst also maximising the benefits of theNHS Leadership Academy programmes where appropriate
We will support teams and individuals through the management of changeprocess using tailored interventions as appropriate
We will support the recruitment process by providing a bespoke assessmentcentre service for all senior recruitment
We will develop bespoke team interventions to support service improvement
We will develop a framework to attract, retain and develop talent within the Trustby June 2015
For Action
Support delivery of 90% Compulsory Training Compliance by March ’15.
Develop and maintain Trust wide Education and Development curriculum by Dec.
’14.
Implement streamlined induction process by June ’15.
Progress to date
Target2014
Achieved2014
Target2015
Target 2016
Trust compliance with compulsorytraining at March 2013
85% 78% 90% 90%
For Action Embed the new Compulsory Training Procedure pan-Trust to achieve minimum
90% compliance by March 2015 Develop Education Development and Training Plan by December 2014. Introduce streamlined induction processes by June ’15. Develop a framework to attract, retain and develop talent within the Trust by June
2015.
Formatted: No underline
Formatted: Font: (Default) Arial
Formatted: Left, Indent: Left: 1.27cm, Line spacing: Multiple 1.15 li, Nobullets or numbering
Formatted: No underline

23
6.7 Supporting Plans and Strategies
The key to achieving the Trust’s strategic goals and realising some of the aims within theWorkforce OD strategies are a number of underpinning strategies. These are:-
Annual Plan
Trust Strategy
Pan-Leeds Safeguarding children and education strategy
Pan City of York children and young people’s mental health Strategy 2011 – 14
Estates Strategy
Information Strategy
Procurement Strategy

24
Appendix 1 – Values and Behaviours
.

25
Appendix 2 – Workforce Development Strategy – further actions 2014/15.
ACTION BY WHEN LEADTo roll out Your Voice CountsEngagement Initiative
March ’15 for pilotlinked to staff survey
Head of OD
Develop a reward framework usingFT Flexibilities to attract, andretain and reward talented andhigh performing employees.talent
December 2015 (linkedto PMO workstreams15/16)
To be agreed
Develop quarterly LeadershipForum for leaders at all levels inthe Trust
June ‘15 Head of OD/Head ofComms.
Implement new intranet October ‘14 Head of CommunicationsAgree and implementCommunications and MarketingStrategy.
June March ‘15 Head of Communications
Participate in the national MentallyHealthy Workplace Pilot
March ‘15 Head of Diversity andInclusion
Full roll-out of First Care AbsenceManagement programme
December ‘14 Director of WorkforceDevelopment
Develop First Workforce Planlinked to Trust Strategy
June ‘15 HR Managers
Implement local WorkforceManagement Dashboard
December ‘14 Head of Workforce andInformation
Complete Phase 3 E-Rosteringroll-out in York
July ‘15 E-Rostering Project Lead
Implement Version 10 ofHealthroster
Jan ‘15 Head of Workforce Info
Development of TalentManagement Framework
June ‘15 Head of Learning and peopleDevelopment
Develop 360 review process linkedto Trust values to supportappraisal process
March ‘15 Head of learning and PeopleDevelopment
Support delivery of 90%Compulsory Training Compliance
March ‘15 Head of Learning andDevelopment
Develop and maintain Trust wideEducation and Developmentcurriculum
December ‘14 Head of Learning and PeopleDevelopment
Implement streamlined inductionprocess
June ‘15 Head of Learning and PeopleDevelopment
Develop a framework to attract,retain and develop talent
June 15 Head of Learning and PeopleDevelopment

26

27
Appendix 3
TRUST CAREER FRAMEWORK - CLINICAL
8d
8c
8b
8a
7
Charge Nurse/Team ManagerClinical supervision/leadership responsibilitiesAuthorised signatory/may hold a delegated budgetContributes to service planning and provisionDegree of post graduate qualification plus?????
Service Manager/Principal TherapistManagerial responsibilities for clinical practice and or planning andservices for more than one area.Authorised signatory/delegated budgetsMasters Level qualification or equivalent experience
Modern Matron/Prof.LeadAccountable for the professional leadership for high quality services,resolving professional issues, expert/advanced professional advice andsupportMasters Level qualification or equivalent experience
Lead Nurse/Advanced Therapist……….Advanced/expert clinical practitionerPost Graduate Qualification plus significant equivalent experience inrelevant clinical field(s)
General Manager/ Consultant Nurse/TherapistAccountable for development and delivery of high standard clinical services/providing expert level of clinical expertise. Implements new ways of working.Deputises for Assistant Director of Operations/Director of Nursing & Service Delivery as required/appropriateMasters qualification plus formal management/leadership qualification or equivalent experience.
Consultant Nurse/TherapistStaff working at a very high level of clinical expertiseResponsible for service development, clinical research (formal research, 20% of time. Min & publication, devising and delivery of training.Masters qualification, leadership and research skills, teaching qualification or equivalent experience.
Assistant Director/Deputy DirectorAccountable for the strategic leadership, of a Business UnitMember of the Trust Management Team, deputising for the Executive Directoras required/appropriateCreate/identify new & Changing business opportunitiesMasters qualification plus management/leadership qualification or equivalentexperience.
Assistant Director: Nursing/Policy & PracticeOperations/Assistant Lead/AHPStrategic leadership of PolicyPractice and DevelopmentMasters/Leadership qualification or equivalent experience

28
4
5
4
3
2
1
6
Apprentices undertaking duties as part of recognised Apprenticeship scheme.Apprenticeship
Band 1 Support WorkerUndertakes routine supervised support in a number of ancillary roles.
Band 2 Clinical(Healthcare Assistant/Support Worker)Undertakes personal care and related procedures, supervised by qualified Nurse/Senior Healthcare Assistant. May escort single patient off-site.
Healthcare Assistant/STR Worker/Activities Co-ordinator/Housekeeper/Therapy Support WorkerImplements clinical care and care packages under the supervision of a qualified Nurse. Developed physical skills to administer basic physiological tests, takeblood, lead on control restraint. May escort groups of patients off-site.
Associate Practitioner/Technical Instructor/Senior STR WorkerTheoretical knowledge of a range of procedures and practice gained through……..
Specialist Nurse/Therapist/Deputy Charge NurseAutonomous practitioner guided by broad occupational policies. Develops specialism and acts as a lead within the team, supporting the Lead Nurse/ChargeNurse and deputising as appropriate. Assesses patient needs and implements specialist programmes of care.Supervision of staff, supporting senior managers in the PDR and recruitment process……………
Registered Nurse/Practitioner/TherapistAutonomous practitioner working within professional codes of conduct. Assesses patients, develops programmes of care/care packagesDevelops an interest and knowledge or link role in a specific topic. Manager available for guidance. Clinical supervision of support staff and students

29
Appendix 4
TRUST CAREER FRAMEWORK – NON CLINICAL
8c/d
Assistant/Associate Director/Deputy Director (Corporate Governance, Corporate Assurance, Finance, Business & Planning, HR, Audit)Accountable for the strategic leadership, of a corporate service and associated functionsSignificant management, budget, policy and performance responsibilitiesStrategic planning of service/sAccountable for the efficient leadership, direction/advice and development of services within strategic and operational frameworks – deputise for the ExecutiveDirector as requiredMasters/Doctorate qualification plus management/leadership/teaching qualification or equivalent
Head of Service (Facilities, Training, Organisational Development, Management Accounts)Accountable for the leadership of corporate serviceSignificant management, budget, policy and performance responsibilitiesService specific professional leadership, direction/advice and development of the serviceAccountable for the interpretation of NHS policy and strategy in relation to the specific functional areaMasters qualification, leadership skills/teaching qualification/demonstrable service specific experience or equivalent experience.
8b/cc
8a
Senior Manager/Advisor/Lead (Medical Business Manager, Programme Manager, HR Advisor)Accountable for the effective leadership, development and delivery of a specialist corporate functionSpecific specialist function responsibilities e.g. HR, Training, Business, Finance, ITGuided by general health, organisational or broad occupational policies/interprets external policyMasters qualification or equivalent – formal management/leadership qualification or project qualification/experience or equivalent experience
Service/Department Manager (Hotel Services Manager, Pals/Complaints Manager)Provides advanced professional knowledge/management/leadership, ensuring proficient delivery of a service.Staff management and financial/budgetary responsibilitiesLocal and regional networking. Responsible for key service performance indicatorsGuided by principles and broad occupational policies, interprets/applies relevant external policiesPost-graduate or equivalent – demonstrable experience/knowledge/managerial leadership
7

30
Specialist Administrative Office/Manager (Project Manager, Training and Development Officer)Provides leadership, specialist knowledge and experience within a specialist service/functional areaSupervision or management of staff/devise, develop and delivery of training/management of projectWorks autonomously as a lead specialist within agreed objectives, organisational policy/guidancePost-graduate or equivalent – specialist knowledge across a range of work procedures and practices underpinned by theoretical knowledge/practical experience
6
Senior Administrative Officer (Project Lead, Administrative Manager)Provides professional leadership, knowledge and experience within specific service/functional areaInitiates the planning and development of the service/project, Provides supervision/management/training in own disciplineWorks autonomously in accordance with agreed objectives and develops substantial support systemsDegree or equivalent - understanding of a range of work procedures and practices, requiring expertise within a specialism underpinned by theoretical knowledge
5
Administrative Officer (Project Support/Team Leader/Administration)Provides an administrative support service to corporate or clinical areasInitiates development of the support service. Inducts/supervises/manages less experienced staffWorks autonomously within well established procedures, managed rather than supervisedNVQ4 or equivalent – Intermediate level of theoretical knowledge of a range of procedures and practices gained through short courses and experiential learning
4
Senior Administrative Assistant/Secretary/Administrative Officer/Analyst/Project AssistantProvides administrative/secretarial/project support to corporate or clinical areasWorks within well established procedures, managed rather than supervisedInducts or supervises less experienced staff, NVQ3 or equivalent – standard/advanced keyboard skillsDemonstrable experience of practice and procedures relevant to the area of work
3
Administrative Assistant/Receptionist/HelpdeskProvides administrative/clerical/reception/helpdesk assistance to corporate or clinical areasWorks within well established procedures under supervisionNVQ2 or equivalent experience – basic/standard keyboard skills
2
Administration SupportUndertakes supervised support in certain clerical roles. –1
Apprentices as part of recognised apprenticeship schemeApprenticeship

31
Appendix 5 – Progress Measurement
We will measure our progress against the actions in this strategy by using the metricsidentified as follows:Our culture
Measure 2012Staff
Survey
2013Target
2013Achieved
2014Target
2015Target
2016 Target
Reporting goodcommunicationbetween seniormanagement andstaff
25% 30% 27% 35% 40% 45%
Feel their rolemakes a difference
85% 86% 89% 87% 88% 89%
Staff feeling able tomake contributionsto improvements atwork
75% 76% 76% 77% 78% 79%
Strategic Workforce ChangeTarget 2014 Achieved
2014Target 2015 Target
2016
In 2013 Average earnings LYPFT is£33,200
£33,000 £30.2k £29,000 £27,000
Trust Turnover Rate ? 10-15% 10-15% 10-15%
Employee Engagement and Communication
Measure2012
Survey2013
Target2013
Achieved2014
Target2015
Target2016
Target
Reporting goodcommunicationbetween seniormanagement and staff
25% 30% 27% 35% 40% 45%
Percentage of staffable to makeimprovements at work.
75% 76% 76% 77% 78% 79%

32
Improving Health, Well-being and Attendance
Target Q42014
AchievedQ4 2014
Target Q42015
Target Q42016
Trust absence rate at March 20135.2% 4.7% 4.6% 4.2% 3.7%
Trust absence rates due to stressrelated conditions at March 2013
28%25% 24.9 26% 25%
Trust absence rates due to Musculo-skeletal related conditions at March2013
13.8%
11.8% ? 10.8% 9.8%
Staff Survey Measure StaffSurvey2012
Target2013
Achieved2013
Target2014
Target2015
Target2016
% suffering work-related stress in the lasttwelve months
48% 46% 42% 40% 38% 36%
Staff who reportexperience of physicalviolence from patientsrelatives or the public inlast twelve months
25% 20% 26% 18% 18% 15%
Workforce Policy, Practice and RewardTarget 2014 Achieved
2014Target 2015 Target 2016
Agency spend (excludingmedical staff) at March 2013was £1.3 million
£204,000 AwaitingAW
figures?
£100,000 £50,000
Appraisal compliance at March2013
85% 68% 90% 95%
Staff who report they wereappraised with personaldevelopment plans in lasttwelve months (staff survey)
85% 80% 90%(staff survey)
95%(staff survey)
Trust Vacancy Rate 4% 8.2% 4% 4%
Learning and DevelopmentTarget 2014 Achieved
2014Target 2015 Target 2016
Trust compliance with compulsorytraining at March 2013 85% 78% 90% 90%
Formatted Table

33

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Operational Plan Implementation Quarter 3 Report
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Jill Copeland, chief operating officerSTRATEGIC:
PAPER AUTHOR: Amanda Burgess, programmemanagement office manager
GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)
G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)
SO1 We provide excellent quality, evidence-based, safe care that involves people and promotesrecovery and wellbeing
SO2 We work with partners and local communities to improve health and lives
SO3 We value and develop our workforce and those supporting us
SO4 We provide efficient and sustainable services
SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individuals
Matters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
9

SUMMARY:
The attached summary report, read alongside our five-year Trust Strategy and two-yearOperational Plan, sets out those main areas of focus at the end of the third quarter of thisyear.
This is our third report of 2014/15 and is set out to provide an overall summary of ourposition at this stage of the financial year against each of the schemes in the 2014/15Operational Plan and also with our strategy milestones. Further narrative has beenprovided to summarise our areas of concern and the plans in place to address them.
Appendix one sets our overall progress against our cost improvement plan schemes.Appendix two provides a two page dashboard which provides a snapshot of our RAG (red,amber, green) rated progress against each element of the Trust’s work programme.
A number of the schemes monitored by the PMO are still in development. Those strategymeasures which are under development or projects which are currently being scoped arehighlighted as ‘grey’.
RECOMMENDATIONS:
Members of the Board of Directors are asked to:
Note the progress made against our Operational Plan priorities and strategy measures
at the end of quarter three 2014/15.

1
OPERATIONAL PLAN IMPLEMENTATION QUARTER 3 REPORT
1. Purpose
This report provides a summary of the Trust’s progress with the measures in our five-yearstrategy, schemes in our 2014/15 Operational Plan and the strategically significant projectsmonitored via the Programme Management Office. A two page dashboard provides a snapshot ofour RAG (red, amber, green) rated progress against each element of the Trust’s work programme(see appendix 2).
This is our third report of 2014/15 and is set out to provide an overall summary of our progressagainst each of the schemes in the 2014/15 two year Operational Plan and also with our strategymilestones. This report also includes how we are progressing against our top five costimprovement plans.
2. 2014/15 Operational Plan status summary
We are now part way through a significant programme of work to improve our services, which isbeing closely supported, monitored and reported upon via our Programme Management Office.We are part way through delivering on the vast majority of our schemes which have now formedour two-year Operational Plan 2014/15 which was submitted to Monitor on 4 April 2014.
This quarter three report starts to give an indication of our performance as we draw closer to theend of the financial year. For some of our schemes we may not achieve the milestones articulatedas part of our 2014/15 Operational Plan and we have projected this position by applying a ‘red’rating. For some of our schemes the milestones were stretched across a two year workprogramme and therefore an ‘amber’ rating has been applied. This in particular is noted for bothestates and workforce where we are delivering against the work programmes set out in theirrespective functional strategies.
Quarter three has also seen the establishment of a new project. This project sets out our plans tobecome a smoke-free organisation by April 2016. Scoping of this new project is well underwaywith the project initiation document, project plan and risk/issue logs to go through our governanceprocesses during quarter four.
2.1.Risks to the delivery of our 2014/15 Operational Plan
At the end of quarter three we have one risk recorded on the electronic risk register. No risks arerecorded as extreme. All risks are monitored routinely via the Strategy Implementation Board andrecorded on the operational/local risk register.

2
2.2.Delivery of our 2014/15 Cost Improvement Plans
Major cost improvement plans (CIPs) identified as part of our two-yearOperational Plan are managed as formal programmes or projects andadhere to MSP/PRINCE2 methodology. All our CIPs have been quality anddelivery impact assessed, with the CIP proforma being completed for eachindividual scheme. Each scheme has been scored and electronically signedoff by both the Medical Director and the (former) Chief Nurse and Director ofQuality Assurance. A report setting out any impact a scheme may behaving upon the quality and delivery of our services is routinely presented tothe Quality Committee. The Finance and Business Committee on aquarterly basis receive the financial progress against each individualscheme.
Our 2014/15 cost improvement plans have been challenging with £1.4mslippage at the end of quarter three against an overall plan of £3.46m. Thisequates to a shortfall of 40% against our overall plans at the end of quarter3, with a 30% shortfall forecast for the year end. Our gaps largely relatedto a delay to the redesign of the acute care pathway for the Leeds CareGroup (see section 2.2 of this report), linked to delays in getting approval forrevenue investment from the Leeds CCGs to support the establishment ofthe Crisis Assessment Unit. This is managed as a formal project and a keyissue for the Leeds Care Group. In addition, reducing shift handoverperiods and enacting the on-call arrangements have equally been delayed,contributing to the overall cost improvement plan slippage. This work is notformally project managed. Achievement of these CIPs has been delayed,but CIPs remain priorities for delivery.
A summary of our progress against the top five plans including ourperformance against the overall 2014/15 cost improvement plan can befound at appendix 1. The cost improvement plan thermometer shows ourend of quarter four forecasted position against our overall target.
The tables below set out the priorities for clinical services which have an ‘amber’ or ‘red’ rating.For the schemes with a cost improvement plan attached, details of our progress have beenincluded.
CIP Thermometer
0
10
20
30
40
50
60
70
80
90
100
1

3
Strategic objective 1: we provide excellent quality, evidence-based, safe care thatinvolves people and promotes recovery and wellbeing:
AMBER: Develop and implement recovery, integrated care pathways and outcomes:extensive work has been undertaken over the last 12 months to implement outcome measures.A clinician reported outcome measure (CROM) is now completed for people who use ourservices and the patient reported experience measure (PREM), which includes the friends andfamily test, went live on 1 January 2015. Further work is required to ensure all service users areroutinely offered a patient reported outcome measure (PROM) and an identified lead is now inpost to deliver this work. In addition, outcomes are a core quality improvement objective foreach care group.
We have however slipped behind with some of these scheme milestones, as articulated in our2014/15 Operational Plan. This is due to some our original recovery plans being a littlechallenging in the timeframes stipulated and results of the integrated care pathways model officetesting requiring the team to seek alternative options. Consequently, we have already initiatedour plans to bring together our outcomes, recovery and integrated care pathway developmentpriorities and manage this work as a programme. This will enable the synergies between theschemes to be realised and set a clear roadmap for success.
No cost improvement plan is linked with this scheme.
AMBER: Build our reputation for high quality research: during quarter three delays havebeen encountered to some of our research campaign timescales. This includes a delay to thesubmission of the bid for the peer support worker project following collaboration with mentalhealth services in Melbourne, Australia. The bid submission date is now potentially delayed untilSeptember 2015 and is dependent upon University of York colleagues’ availability. In addition,during quarter three we were notified that our bid for continued research into computerisedcognitive behaviour therapy for adolescents with depression and randomised control trial (RCT)had been unsuccessful. Alternative bids are currently being worked up.
No cost improvement plan is linked with this scheme.
AMBER: Increasing dementia/memory services to meet the needs of the growing numberof older people in Leeds: detailed service improvement has been underway to develop a newmodel for community alternative services for people with dementia. This work has now beenpulled together in the form of a business case for our commissioners and feedback should beknown during quarter four. The original milestones we set ourselves have therefore not all beachieved and will transfer into our 2015/16 plans, hence an amber rating has been applied.
It is envisaged that the £44k cost improvement plan target associated with this scheme will beachieved by the end of the financial year.

4
RED: Develop the pathway for people needing acute mental health services in Leeds: thisproject has been delayed due to delays in achieving confirmation from the Leeds CCGs ofrevenue funding to support the Crisis Assessment Unit (CAU); and there has also been a delayto the commencement of the environmental works at the Becklin Centre to enable the opening ofthe new CAU. A revised detailed quotation and specification is required from the contractors toinclude anti-ligature sink basins, a full refurbishment of toilets and replacement curtain rails. It isanticipated that this work will commence before the end of the financial year however it will notbe completed until early 2015/16, hence a red rating has been applied. Meanwhile, the CAU hasopened from January 2015 with two beds, with further beds to be opened once therefurbishment work has been completed.
It is envisaged that the £649k cost improvement plan target associated with this scheme willnot be achieved in 2014/15. A shortfall of £580k is anticipated by the end of the financial year.This CIP will be carried forward into 2015/16.
AMBER: York and North Yorkshire schemes: all the schemes are delayed due to theforthcoming tender process. This rating may change following release of the tender specificationwhich is due in late January 2015.
No cost improvement plan is linked to these schemes.
AMBER: Improve pathways for service users and deliver commissioner priorities acrossforensic services: extensive work had been underway to develop a new forensic servicestrategy which would in turn inform discussions with commissioners. This has regrettably beendelayed due to the need to divert attentions to developing the immediate quality improvementplan. The original milestones we set ourselves have therefore not all be achieved and willtransfer into our 2015/16 plans, hence an amber rating has been applied.
It is envisaged that the £55k cost improvement plan target associated with this scheme will beachieved by the end of the financial year.
Strategic objective 2: we work with partners and local communities to improve health andlives
AMBER: Develop equitable locality and Trust-wide processes for involving people whoaccess services: our plans to establish locality based service user network (SUN) groups usinga café/network model in each of the localities has been delayed. The implementation phaserequires a coordinated approach with operational services and a working group will take thisforward during quarter four. Outcomes from this group will report through the recoveryprogramme.
No cost improvement plan is linked with this scheme.

5
Strategic objective 3: we value and develop our workforce and those supporting us
RED: Implement the Workforce Development Strategy, promoting a healthy culture thatmeets the recommendations of the Francis Report: the Trust has a key performanceindicator to achieve a 90% compliance rate for appraisals by the end of 2014/15. At the end ofthe third quarter we are currently at 71% compliance. This continues to be a challenging areafor the organisation and it is anticipated that the target will not be achieved by the end of thefinancial year. Progress during quarter three includes the introduction of a dedicated inbox toassist staff with the recording of completed appraisals and further training workshops have beenheld across Leeds and York sites. Work is underway during quarter four to review the automaticgateway linked to the completion of appraisals and also objectivising line managers.
During quarter three the new ‘mysite’ intranet was launched, however there has been a delay tothe implementation of the new upgraded intranet system. A Communications Strategy is to bedeveloped which will include delivery of a new intranet, a business case outlining requirementswill be completed and considered during quarter four.
No cost improvement plan is linked with this scheme.
RED: Support new ways of working following service redesign through training, skillsdevelopment, clear roles and responsibilities and performance objectives: the Trust has akey performance indicator to achieve by the end of 2014/15 of 90% compliance for allcompulsory training, as specified in the Workforce Strategy. At the end of the third quarter weare currently at 78% compliance, therefore it is anticipated that the target will not be achieved bythe end of the financial year.
Agreement has been reached to procure a new learning management system which it isanticipated will have an impact on compliance. A full procurement process has alreadycommenced and it anticipated that this will be completed during quarter four, with full rollouttimetable known.
No cost improvement plan is linked with this scheme.
AMBER: Develop our Occupational Health Service and improve health and wellbeing ofour staff: musculoskeletal (MSK) absence has decreased slightly during quarter three, howeverit still continues to be above the target of 10.8% of total absences. The Trust physiotherapist isworking closely with HR to identify hotspots, delivering sessions to work areas on prevention andinterventions to support staff, working with the moving and handling team regarding training andbest practice.
Communication and promotion of the MSK service to staff through leaflets and a short film isavailable on our intranet site. Over quarter four we will continue to work with the new First Caresystem using the improved management information to better analyse absence and identifyinterventions and support to reduce absence.
Furthermore, sickness absence during quarter three is currently at 4.9% against a target of4.7%. With the introduction of the new First Care system which enables the timely production ofsickness action plans, it is envisaged that the target will be achieved by the end of the financialyear.
No cost improvement plan is linked with this scheme.

6
Strategic objective 4: we provide efficient and sustainable services
AMBER: Develop our IT infrastructure to put us in control of health and care informationacross Leeds, York and North Yorkshire: the Paris Development Programme is nearingcompletion of its third project, with the Vision Upgrade Project restarting in February, followingthe completion of the initial roll out of Paris to York services. Over the past 18 months a numberof events have, and continue to, influence the direction and fulfilment of the initial businessrequirements through the final Vision Development Project hence a delay to the overalltimescales. This includes the introduction of the Paris Design Authority, the decision followingmodel office to develop ICPs clinically and outside of Paris, the EDRM procurement of a systemto centrally store current paper based clinical information and the decision to procure an E-Prescribing solution outside of Paris. Continuing Paris developments will be fulfilled through theParis Design Authority, steered by care services. This will allow the flexibility to respond toemerging needs and changing priorities.
Our two-year Operational Plan set out our plans to integrate our systems with Leeds TeachingHospitals NHS Trust middleware to support electronic exchange of clinical documents iereferrals and e-letters. Since establishing this citywide collaborative scheme it has beenacknowledged that this work will not be achievable by the end of March 2015, hence an amberrating has been applied. This initiative will however be set out in the Health Informatics Strategyas a long term development scheme.
No cost improvement plan is linked with this scheme.
AMBER: Ensure our Leeds estate is fit-for-purpose, meets the needs of people using ourservices and is cost effective: the Yorkshire Centre for Psychological Medicine (YCPM) iscurrently situated at Ward 40, Brotherton Wing, at Leeds General Infirmary. Our two-yearOperational Plan sets out our plans to expand the bed base from 8 to 14. Whilst LeedsTeaching Hospitals Trust have committed to including YCPM in future plans, timescales remainunclear. The need to find new premises for the YCPM was also highlighted by the CQC in theirrecent inspection and we are working up alternative options to relocation on an LTHT site.
Our plans to develop St Mary’s House site in Leeds into a community hub are now on schedule,however, given the age of the building, the issues it can present, the complexity of movingvarious services whilst maintaining operations and the tight timescales, the project remainsamber.
It is envisaged that the £422k cost improvement plan target associated with this scheme willbe achieved by the end of the financial year.

7
RED: Work with our landlord (NHS Property Services Ltd) to ensure our York estate is fit-for-purpose, meets the needs of people using our services and is cost effective: due toNHS Property Services delays, the start of contractors on site at Cherry Tree House has beendelayed to February 2015 (previously November 2014). This will result in the older people’sservice estimated timescales to be relocated from Ward 6 Bootham Park Hospital to Cherry TreeHouse in June 2015 (previously March 2015).
Detailed refurbishment plans for Bootham Park Hospital have now been provided by NHSProperty Services. Ward 6 will be refurbished for male service users and Ward 1 for femaleservice users by the end of July 2015.
In light of these estates issues, amber status has been applied to the York and North Yorkshireplans (schemes 1.7.1, 1.7.2, 1.7.3, 1.7.4) and ensure we meet our statutory and regulatoryrequirements (scheme 5.1) schemes.
No cost improvement plan is linked with this scheme.
AMBER: Establish robust working practices for implementation of Mental HealthPayments: we have not met the mental health payment system trajectory at the end of quarterthree for the percentage of people receiving care and treatment who are allocated a ‘carecluster’ and also for the percentage of people receiving care and treatment whose ‘care cluster’is in date. A milestone of 95% has been used as a guide by the Regional Care Pathways andPackages Project and is based upon the fact that approximately 5% of people will be in somestage of assessment.
Leeds services have 66.4% of in-date clusters. York and North Yorkshire services have 40.4%of in-date clusters. Actions continue to address clinical engagement with the mental healthpayments project. This includes the on-going training programme across Leeds and Yorkservices with clustering clinics continuing in Leeds and York community hubs. Clusteringperformance reports are being issued to individual clinicians and managers, and qualityindicators and outcomes reports by cluster are in development.
No cost improvement plan is linked with this scheme.

8
3. Progress against the measures in our five-year strategy
Our three goals set out in our five-year strategy are the quality goals described in the QualityReport. The report at appendix two sets out our performance against each of the strategymeasures and details any action plans in place to improve performance.
When refreshing our five-year strategy we set ourselves some very aspirational standards that wewant to achieve by 2017/18. This report provides a summary of our progress against the 2014/15stretch milestones for achievement and therefore indicates the progress we have made againstthese milestones at the end of quarter three. We have also captured trend position to indicatewhether there has been an improvement in our performance year-on-year, a deterioration inperformance or no change. Across all our strategy measures the majority have improved year-on-year or stayed the same.
As with the Integrated Quality Performance Report we have adopted the red/green rating system;however, for the strategy measures, we have applied a 5% threshold to enable a ‘green’ rating tobe applied.
During quarter three the results of the 2014 community and inpatient mental health surveys havebeen made public. NHS Surveys have made a number of changes to this year’s communitymental health survey in terms of design, question layout and to the questions themselves. Someof the measures in our five-year strategy were set based upon the questions in the communitymental health survey and are affected by the survey changes.
All the measures in our strategy have been built into our Patient Reported Experience Measure(PREM). Our in-house survey called ‘Your Views’ was launched on 1 January 2015 and theFriends and Family Test is incorporated. Our ‘Your Views’ survey will enable more accuratequality performance measurement, however the figures will not be available for January 2015 untilFebruary 2015. It is proposed that the Trust wait for at least six months before a baseline can beestablished from this PREM.
During quarter three the results from our two national service user surveys have been reportedthroughout our governance structure. Key areas of focus for the 2014 community mental healthsurvey are: a coordinated trust wide approach to physical healthcare for community and CMHTs;and outcomes and arrangements for service users in crisis. For the 2014 inpatient survey anumber of key areas of focus have been agreed which will feed into the ‘sign up for safety’ workplan.
Actions from the two surveys will be coordinated and will then translate into an improvement planwhich the Patient Experience Team will oversee during quarter four. Consequently, these resultswill be triangulated with our local ‘Your Views’ survey (PREM) and other mechanisms for patientfeedback, including themes and trends from complaints and PALS contacts.
In terms of the partnership survey, during quarter three we commenced reviewing the content ofthe partnerships survey to provide a better measure of relationships. We will have an agreedmethod of collecting this data by the end of quarter four.
The other red areas show our performance at the end of the third quarter; the ‘trigger to board’measure is due to two inpatient suicides which were reported: one within our Leeds services andone within York and North Yorkshire services. The research and development measure isreflective of our actual recruitment figures up to the end of quarter three. Our year-to-dateperformance does not include figures for all current recruitment in external Portfolio studies asthere is a six week time lag in receiving up to date information. The annual audit which collectsrecruitment for all studies is underway but not all reports have been returned. New studies are inthe process of being opened which will help towards achieving the 2014/15 target.

9
The timely provision of information to support ‘real time’ measurement of outcomes andperformance trajectory is continually discussed within the Care Services Performance andInformation Group, with a view to attaining the target of 97% within 7 days by the end of quarterfour.
The mental health payments measure is linked to the scheme described in section 2 of this report.
4. Development of strategy measures
Within our refreshed strategy, the development of outcome measures is our first priority understrategic objective one. A project has been established to develop local outcome measures, whichis being monitored via the Programme Management Office.
5. Recommendation
Members of the Board of Directors are asked to note the progress made against our OperationalPlan priorities and strategy measures at the end of quarter three 2014/15.

10
APPENDIX 1 – COST IMPROVEMENT PLAN PERFORMANCE
CIP Themes 2014/15Plan£’000
Year to date ForecastPlan£’000
Actual£’000
Variance£’000
Variance%
Plan£’000
Actual£’000
Variance£’000
Variance%
Leeds Mental Health Care Group 1,688 1,266 221 (1,045) -82.5% 1,688 490 (1,199) -71.0%York & North Yorkshire CareGroup
34 26 26 0 0.0% 34 34 0 0.0%
Specialist & Learning DisabilityCare Group
595 446 348 (98) -22.0% 595 502 (93) -15.7%
Providing services from fit-for-purpose, cost effective buildings
422 317 387 70 22.1% 422 515 93 22.1%
Delivering cost effectivecorporate services
727 545 577 32 5.9% 727 883 156 21.5%
TOTAL CIP 3,467 2,600 1,559 (1,041) -40.0% 3,467 2,424 (1,042) -30.1%
Performance against CIP plan -40.0% -30.1%

11
APPENDIX 2 – 2014/15 OPERATIONAL PLAN & STRATEGY MEASURE PROGRESS
Strategy measures dashboard [areas marked in black denotes survey question removed]Target Actual Trend
Go
al1
People report that the services they receive definitely help them to achieve their goals:
People using mental health services 55% 41% ↑
People using learning disability services 82% 88% ↑
Clinical outcomes have been improved for people who use our servicesCarers report that their own health needs are recognised and they are supported tomaintain their physical, mental and emotional health and wellbeing
Go
al2
People who use our services report that they experience safe care:
People using mental health services 90% 85% ↑
People using learning disability services 93% 78% ↓
People using our children and young people’s services 85% 72% N/A
Number of ‘no harm’ or ‘low harm’ incidents increases as % of total:
Total % ‘no harm’ and ‘low harm’ 97% 95% ↓
Number of ‘Trigger to Board’ events 0 2 ↓
Go
al3
People who use our services report overall rating of care in last 12 months verygood/excellent:
People using mental health services 68% 70% ↑
People using learning disability services 92% 96% ↑
People who use our services report definitely treated with respect and dignity by staffproviding care:
People using mental health services 92% 72% ↑
People using learning disability services 92% 96% ↑
Carers report that they are recognised, identified and valued for their caring role andtreated with dignity and respect
SO
1
Access to crisis care:
People who use our services have the number of someone from the Trust that theycan phone out of office hours 55% 61% ↑
People who called the number definitely got the help they wanted 78% 44% ↓
Support towards recovery and inclusion: % of service users who would have liked helpfrom our mental health services who received such help:
With finding or keeping work 60% 47% ↓
In finding and/or keeping their accommodation 65% 47% ↓
In getting financial advice or benefits 65% 57% ↔
Involvement in care planning: people who use our mental health services report that:
Their views were definitely taken into account when deciding what was in their careplan
They were definitely given (or offered) a written or printed copy of their care planPeople using our learning disability services report that:
They had accessible information to support their care 87% 94% ↓
Their views were definitely taken into account when deciding what was in their careplan
80% 86.5% ↓
People using our children and young people’s services report that:
Their care plans met their needs 90% 72% ↑
They had received a copy of their care plan 100% 87% ↓
Commitment to improving outcomes through research and development: total number ofpeople (service users/staff/carers) participating in research studies 1000 636 ↓
SO
2
Partners report that the Trust demonstrates successful partnership working and theability to influence partners’ prioritiesEvidence that we are working with partners to reduce mental health and learningdisability stigma
Evidence inplace
↔
Evidence of effective engagement and involvement of service users and carers,governors and members
Evidence inplace
↔
SO
3
Quality of care: staff who report they feel satisfied with the quality of work and patientcare they are able to deliver 75% 89%
↑
Job satisfaction: staff who report job satisfaction 72% 3.67out of 5
↔
Personal development: staff who report they were appraised with personal developmentplans in last 12 months 90% 78%
↓

12
Strategy measures dashboard [areas marked in black denotes survey question removed]Target Actual Trend
Health & wellbeing: staff who report experiencing physical violence from patients,relatives of the public in last 12 months 20% 28%
↑
Staff engagement: to engage staff who report good communication between seniormanagement and staff 30% 34%
↑
SO
4
Maintain a financial position which meets the obligations measured under Monitor’scontinuity of services risk assessment
Monitor RiskAssessmentFramework
4↔
Timely provision of information to support ‘real time’ measurement of outcomes andperformance
97% in 7days
88.4% ↓
Payment by Results: ensuring people who use our services are appropriately andaccurately allocated a care cluster:
% of people receiving care and treatment who are allocated a ‘care cluster’ 95% 75.1% ↓
% of people receiving care and treatment whose ‘care cluster’ review is in date 75% 56.6% ↑
SO
5
Maintain a position of no outstanding compliance actions on our Care QualityCommission registration Compliant
↔
Maintain a governance position which meets the obligations measured under Monitor’sgovernance risk assessment
Monitor RiskAssessmentFramework
↔

13
Operational Plan scheme dashboardScheme 1.1 Develop validated outcome measures across all services
Scheme 1.2 Implement a Recovery & Person-centred Care Programme
Scheme 1.3 Develop and implement Integrated Care Pathways (ICPs)
Scheme 1.4 Improve young people’s experiences of our services
Scheme 1.5 Build our reputation for high quality research
Scheme 1.6 Leeds: increasing dementia/memory services to meet needs of growing number of older peopleLeeds: develop the pathway for people needing acute mental health services
Leeds: improve outcomes for service users with severe and enduring mental illness by improvingrehabilitation and recovery pathways and alternatives to admission for this group of service users
Scheme 1.7 YNY: improve IAPT (Improving Access to Psychological Therapies) and primary care mental healthservices in York & North Yorkshire
YNY: redesign community services and alternatives to hospital admission to support integrated carepathways across York & North YorkshireYNY: manage the inpatient resource effectively and reduce the number of service users requiring out ofarea placementsYNY: review mental health services for older people in Vale of York, aiming to enhance communityprovision and ensure inpatient services meet commissioner requirementsYNY: develop hospital liaison services in York
Scheme 1.8 Learning disability services: work together with commissioners and partners in social care to providepeople with learning disabilities with the most appropriate care in the most appropriate placeForensic services: improve pathways for service users and deliver commissioner priorities
Offender health services: maximise opportunities open to the Trust from re-tendering of offender healthservices across the regionRegional offender personality disorder services: support probation trust staff to better deal withpersonality disorder clients within criminal justice settingsEating disorder services: maximise clinical outcomes for service users in inpatient and communityservices and improve transition from adolescent to adult eating disorder services
Child and adolescent mental health services: improve services in response to commissionerspecifications
Carer support service (Leeds): provide a single service for all carers support in partnership with 3rd
sector carer support providersYorkshire Centre for Psychological Medicine: secure suitable accommodation for YCPM and expansionof bed base from 8 to 14Leeds Addiction Unit: develop partnership bid to retain current contract
Scheme 2.1 Develop and implement new service models in collaboration with the voluntary sector
Scheme 2.2 Develop and implement new service models in collaboration with health and social care partners inLeeds (integration pioneer) and York and North Yorkshire
Scheme 2.3 Work with our partners to campaign against the stigma and discrimination experienced by people withmental health and learning disabilities
Scheme 2.4 Develop equitable locality and Trust wide processes for involving people who access services
Scheme 3.1 Implement the Workforce Development Strategy, promoting a healthy culture that meets therecommendations of the Francis Report
Scheme 3.2 Support new ways of working following service redesign through training, skills development, clearroles and responsibilities and performance objectives
Scheme 3.3 Develop our occupational health service and improve health and wellbeing of our staff
Scheme 4.1 Review and explore opportunities to grow our organisation and work in partnership
Scheme 4.2 Deliver management, corporate and back office efficiency savings
Scheme 4.3 Develop our IT infrastructure to put us in control of health and care information across Leeds, York andNorth Yorkshire
Scheme 4.4 Ensure our Leeds estate is fit-for-purpose, meet the needs of people using our services and is costeffective
Scheme 4.5 Work with our landlord (NHS Property Services Ltd) to ensure our York estate is fit-for-purpose, meetsthe needs of people using our services and is cost effective
Scheme 4.6 Establish robust working practices for implementation of Mental Health PaymentsScheme 5.1 Ensure we meet our statutory and regulatory requirementsScheme 5.2 Develop the effectiveness of our Board of Directors and Council of Governors

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Implementing NICE guidance (PH48) – smoking cessation in MHServices
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Anthony Deery - Interim Director of Nursing& Quality
STRATEGIC:
PAPER AUTHOR: Helen Wiseman – Strategic Lead for AlliedHealth Professionals
GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)SO1 We provide excellent quality, evidence-based, safe care that involves people and promotes
recovery and wellbeing
SO2 We work with partners and local communities to improve health and lives SO3 We value and develop our workforce and those supporting us SO4 We provide efficient and sustainable services SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individualsOther – not yet a public documentMatters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
10

SUMMARY:
In September 2014, the Board was asked to endorse and support the implementation ofNICE guidance (PH48) following a decision by the Executive Team to commit resources toprepare and enable the organisation to do so by April 2016.
A number of comments were made at that Board meeting, which the Project Lead hascarefully considered and responded to in Section 4 of the attached paper.
The health benefits to both service users and staff, by the introduction of smoke freeenvironments, is well researched and documented.
In achieving a successful smoke free setting it is recognised that it is necessary to adopt awhole organisation approach, with Director sponsorship and full Board support.
This paper sets out why and how Leeds and York Partnership NHS Foundation Trust canimplement NICE guidance (PH48), the issues, risks and benefits.
RECOMMENDATIONS:
It is recommended that:
The Board is asked to support and endorse the implementation of NICE guidance (PH48) toensure the organisation has a supported ‘smoke free’ environment by April 2016.

1
Board Paper
Implementing NICE Guidance (PH48) Smoking Cessation in all Leeds and York
Partnership NHS Foundation Trust services.
1. Purpose
This paper seeks Board endorsement to support the implementation of NICE
guidance (PH48) ‘Smoking Cessation in secondary care, acute, maternity and
mental health services’ published in November 2013. The guidance contains clear
recommendations to ensure that all people who use or work in mental health
services are encouraged to stop smoking and have access to stop smoking support,
including nicotine replacement therapy.
The guidance sets out a framework requiring mental health services to become
completely smoke-free across all sites, including grounds, gardens, car parks,
entrances to building and exits. Service users are to be provided with specialist
support to manage withdrawal from tobacco and abstain from smoking during
inpatient admissions.
Whilst mental health services are not mandated to deliver smoke-free services, the
NICE Guidance puts an onus on commissioners to commission smoke-free services
and recommends that secondary care providers have a duty of care to protect the
health of, and promote, healthy behaviour among people who use, or work in their
services.
2. Executive Summary
People with a serious mental illnesses like schizophrenia, die on average, 15-20
years earlier than the rest of the population (ref.1).
Tobacco use contributes significantly to the main causes of ill-health and mortality in
people with mental health disorders: half of all long-term smokers will die of a
smoking related illness (ref. 2). The rates of cancer, heart disease and respiratory
diseases among individuals with schizophrenia (who have the highest rates of
smoking of any group) are up to double those of age-matched controls (ref. 3).
It was recognised in the Confidential Enquiry into the Premature Deaths of People
with Learning Disabilities (CIPOLD) 2013, that illness related deaths that were
directly impacted upon by smoking had the same prevalence as in the general
population (ref. 4).

2
With the increasing plethora of evidence of the effects of smoking on people with a
mental health condition, and the significant reduction in life expectancy, it is
becoming an increasingly untenable position for Leeds and York Partnership NHS
Foundation Trust (LYPFT), as a health provider, to maintain current practice which
allows the use of tobacco products by service users in its premises. In so doing it
exposes staff, visitors and other service users to second hand smoke.
In September 2014, the Board was asked to endorse and support the
implementation of NICE guidance (PH48), following a decision by the Executive
Team to commit resources to prepare and enable the organisation to do so by April
2016.
A number of comments were made at that Board meeting, which the Project Lead
has carefully considered and responded to in Section 4 of this paper.
3. Background
People with mental health problems smoke at a much higher rate and are more
dependent smokers than the general population (ref. 5). Studies of patients on
mental health units show that up to 70% smoke and around 50% of those are heavy
smokers (ref. 6). The majority of mental health service users start smoking on
average 5 years before the onset of their illness i.e. not because of their illness (ref.
7).
On one day in the Leeds Adult inpatient services, 169 service users were recorded
as smoking. If all were long-term smokers and maintained their smoking habit, then
a projected 84 service users would die from a smoking related disease (ref.1). On
the same day in our Leeds community services 2,985 service users were recorded
as smoking. If they were all long-term smokers and maintained their smoking habit,
then a possible 1,492 individuals would be at risk of premature death from a smoking
related disease (ref.1).
The risk factors associated with smoking, social deprivation, stress, alcohol use and
poverty, amongst others, are also associated with poorer mental health and
therefore it is not surprising that people with mental health problems also smoke
more.
The proposal to implement NICE Guidance (PH48) is based on discussion and
learning from other Mental Health and Learning Disability provider organisations,
who have successfully gone smoke free. These organisations include Cheshire and
Wirral Partnership NHS Foundation Trust, Nottinghamshire Healthcare NHS Trust
and South London and Maudsley NHS Foundation Trust.

3
4. Comments made at the September 2014 Board meeting
Can we learn other organisations who have successfully gone
Smoke Free?
The Project Lead is in contact with a number of mental health and
learning disability secondary care providers who have successfully
achieved a smoke free environment. They have achieved this by
thorough preparation, active engagement, timely communication and
smoking cessation training for their staff.
A workshop was organised for the Council of Govenors in November
2014, where a service user and his carer were invited from Cheshire and
Wirral Partnership NHS Foundation Trust to share their experiences.
This was well received and Governors were asked to consult with their
constituents and feed back to the Project Lead.
A number of comments were returned to the Project Lead as below:
- The questions and concerns raised by the Governors, related to
ensuring there was adequate support for service users. Would they
have timely access to nicotine replacement therapy, offered by a
suitably qualified member of staff?
- The smoking cessation training for staff will enable them to
dispense nicotine replacement therapy and be equipped to address
the behaviours associated with smoking. All inpatient wards will
receive additional funding to facilitate improved opportunities for
social activities.
- Community staff will have access to smoking cessation training and
be aware of how to assist and facilitate service users to access their
local smoking cessation services.
- Other concerns related to the ‘right to smoke’. Was this proposal a
deprivation of liberty?
Deprivation of Liberty – do people have a right to smoke?
This has been formally challenged by service users and the courts found
in favour of the secondary care provider, Nottinghamshire Health Care
NHS Trust.

4
In July 2009 (ref. 11), the Court of Appeal agreed with the High Court that
the patients of Rampton Hospital (part of Nottinghamshire Healthcare
NHS Trust) had no ‘legal right to smoke’ under Article 8 of the European
Convention.
The Court of Appeal also decided that, for some patients smoking is a
form of self-harm and it is reasonable for Trusts to take action to preserve
the health of their patients by preventing smoking in such circumstances.
The Court noted that the Trust owed a duty of care to staff and that when
it identified a risk to its staff from second hand smoke, it followed that it
had a duty to take ‘all reasonable precautions’ to protect staff from that
risk.
It also means that Trusts can introduce measures that may be unpopular
and have some disadvantages in the short term, if there is evidence that
the long term benefits will be substantial, as long as those measures are
introduced in a carefully managed way.
As an organisation, LYPFT should emphasise its wish to promote an
individual’s right to health, as opposed to what it prevents an individual
doing, that is ‘improving health, improving lives’.
Does smoking fulfil a therapeutic function?
It is sometimes thought that smoking is used as ‘self-medication’, helping
people to cope with stress, anxiety and low mood, and is therefore the
effect of mental health problems. In fact, people with a mental illness start
smoking for the same reasons as mentally healthy people do, usually
because of social factors, because family and friends do, because it
makes them feel part of a group, for an image, and they get addicted to
the nicotine in the same way as mentally healthy people do (ref.7). As
nicotine is removed from the body quite quickly, withdrawal symptoms
(feeling irritable, restless and not able to concentrate) can occur within a
couple of hours following the last cigarette, and people feel the urge for
more nicotine in the form of another cigarette. So having another
cigarette, smoking, alleviates nicotine withdrawal symptoms, not stress.
Secondary reinforcers are the behaviours which are paired with smoking,
such as socialising and relieving boredom, so both the psychological
(behaviours) and biological (nicotine) impetuses to smoke need to be
addressed if someone is to stop smoking.

5
The smoking cessation training for staff will enable them to dispense
nicotine replacement therapy and be equipped to address the behaviours
associated with smoking.
Is there a robust Project Plan?
A comprehensive Project Initiation Document (PID) has been developed
which includes objectives, benefits, outcomes, constraints and risks,
together with identified work streams covering Estates, Human
Resources, Staff Training, Communication and Engagement and has
been presented and received at the Care Services Strategic Management
Group (CSSMG) chaired by the Chief Operating Officer and Deputy Chief
Executive. This group will oversee the operational delivery of the project.
The project will further report to the Workforce Steering Group chaired by
the Director of Workforce Development and to the Effective Care
Committee, chaired by the Medical Director.
What are staff attitudes?
A primary concern voiced by staff is a perceived increase in violence and
aggression. However, evidence from psychiatric in-patient services in
Australia Dingman et al (1988) and from Smith et al (1999) in the USA
where a smoking ban was successfully introduced reported no significant
increase in patient aggression. More importantly, the smoking ban in
Broadmoor Hospital and throughout the forensic services of
Northamptonshire Healthcare NHS Trust since 2007 have proved highly
successful with enormous health benefits for staff and patients alike.
Whether staff are wholly supportive of, or have reservations about this
project, a comprehensive smoking cessation training package will be
available to staff. Staff need to feel confident and be competent to
support service users to abstain and go on to quit smoking.
A senior clinician has been appointed as the Clinical Lead for the project,
and this individual is tasked with delivering a comprehensive smoking
cessation training programme for staff across the organisation.
A staff survey will be offered in January 2015 to provide information that
will support this project in planning for and implementing a totally smoke
free Mental Health and Learning Disability service. It will also provide a
baseline for benefit realisation purposes.
6
What are service user attitudes?
Cessation rates among smokers with mental health problems are two to
three times lower than in the general population (ref.7) though according
to the 2010 Health Survey for England, 66% of smokers with mental
illness would like to quit. This suggests that mainstream smoking
cessation programmes are not adequately addressing the needs of
people with mental health issues.
Current practice dictates that all service users are asked if they smoke
and if they would like to reduce or stop. Although presently a limited
smoking cessation service is available to LYPFT’s service users, only
10% of the smoking inpatient population currently access it.
A review of smoking cessation treatments for people with mental illness
(ref.8) concluded that pharmacological aids given to the general
population can be as effective in helping people with mental illness to stop
smoking as those in the general population.
Research has shown that the successful implementation of a smoke free
environment is dependent on the provision of smoking cessation services
at the point of contact and available 24 hours a day.
Is there a Communication and Engagement plan?
The Project’s success will depend on a meaningful communication and
engagement plan, evidenced by timely and ongoing communication with
all the key stakeholders both internal and external to the organisation.
The Senior Clinician, who has been appointed as the project’s Clinical
Lead, will ensure that information, answers and solutions are sought,
received and acted upon, with a visible two-way stakeholder dialogue.
This will involve focus groups, attending Service User Network (SUN)
meetings, briefings, widespread use of Staffnet and letters/presentations
to partner organisations.
5. What are the risks?
The key risk is not progressing the actions to be smoke free. With the increasing
plethora of evidence of the effects of smoking on people with a mental health
condition, and the significant reduction in life expectancy, it is becoming an
increasingly untenable position for LYPFT, as a health provider, to maintain current
practice which allows the use of tobacco products by service users on its premises.
In so doing it also exposes staff, visitors and service users to second hand smoke.
7
6. What are the benefits?
An increase in the number of service users on a quit plan and the associated
physical health benefits;
The reduction in staff escort time to facilitate service users smoking, which will
result in staff releasing more time to care on the wards;
Smoking can affect the efficacy of anti-psychotic medication. Therefore,
smoking cessation will allow the dosage levels of prescribed anti-psychotic
medication to be reduced, along with any associated side effects;
Positive change in staff and service users’ attitudes towards no smoking
7. Next steps
The delivery of an 18 month programme, to enable the Trust to become ‘Smoke
Free’ by 2016. The programme will address several key areas:
An identified Executive lead (Director of Nursing and Quality);
The appointment of a senior Clinical Lead for the project (appointed 9/1/15);
A comprehensive project plan which will be monitored and managed through
a robust reporting, operational and governance structure (completed 9th
December 2014);
The establishment of a ‘Smoke-Free’ Task and Finish group (already
commenced);
The appointment of additional smoking cessation trainers x 3;
A communication and engagement work stream for service users, which will
establish the best way of implementing this goal by identifying shared
solutions ;
A communication and engagement work stream for staff which will address
their concerns, and identify shared solutions;
A communication and engagement work stream for our partner organisations
and relevant stakeholders. To ensure we have access to clearly identified
smoking cessation pathways to support our service users throughout their
journey;

8
As part of the communication and engagement work stream, hold a
conference and launch event for all key stakeholders;
A training programme for staff, to provide different levels of expertise, to
ensure we have sufficient smoking cessation advisors and nicotine
replacement prescribers available 24/7 on all our inpatient units;
Additional resources for the inpatient units, to ensure the availability of extra
recreational and social activities, to replace any reliance on smoking as a
social activity.
8. Recommendation:
The Board is asked to support and endorse the implementation of NICE
guidance (PH48) to ensure we have a supported Smoke-Free environment by
April 2016.

9
References
1. Parks, J., Svendsen, D., Singer, P., Foti M. E., (2006) Morbidity and Mortality in
People with Serious Mental Illness. (A Technical Report) from the National
Association of State Mental health Program Directors.
2. Health and Social Care Information Centre (2010). Statistics on NHS Stop Smoking
Services: England, April 2009-March 2010.
3. McNeil, A. (2004) Smoking and patients with mental health problems. NICE: pp1-16.
4. Confidential Enquiry into the Premature Deaths of People with Learning Disabilities
(CIPOLD) 2013 the University of Bristol, sponsored by the Department of Health.
5. McManus, S., Meltzer, H., Campion, J., (2010) Cigarette smoking and mental health
in England: Data from the Adult Psychiatric Morbidity Survey 2007 National
Centre for Social Research.
6. Health and Social Care Information Centre (2010). Statistics on NHS Stop Smoking
Services: England, April 2009-March 2010.
7. Mental Health Foundation, Taking a deep breath: The mental health implication of
anti-smoking legislation http://www.mentalhealth.org.uk/content/assets/PDF/publications/taking a
deep breath.pdf?view=standard 2007. Accessed April 2014.
8. Action on Smoking and Health (ASH) fact sheet: Smoking and mental health
http://ash.org.uk/files/documents/ASH120.pdg 2013. Accessed April 2014.
9. Morris C, Waxmonsky JA, May MG, Giese A (2009) What do persons with mental
illness need to quit smoking? Psychiatric Rehabilitation Journal, 32 (4) p.276-284
10. Ratschen E et al. Tobacco dependence, treatment and smoke-free policies: a survey
of mental health professionals’ knowledge and attitudes. Gen Hosp Psych 2009; 31
(6) 576-582
11.Mills & Reeve LLP – Second challenge to smoke free policy at Rampton Hospital fails -
July 2009
Helen Wiseman
Strategic Lead for Allied Health Professionals
January 2015

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Care Quality Commission – Action Plan
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Anthony Deery, Interim Director of Nursingand Quality
STRATEGIC:
PAPER AUTHOR: Anthony Deery, Interim Director of Nursingand Quality
GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)SO1 We provide excellent quality, evidence-based, safe care that involves people and promotes
recovery and wellbeing
SO2 We work with partners and local communities to improve health and lives SO3 We value and develop our workforce and those supporting us SO4 We provide efficient and sustainable services SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individualsOther – not yet a public documentMatters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
11

SUMMARY:
The attached paper gives details of the development of the Trust’s action plan followingpublication of the Care Quality Commission’s Inspection report.
The Care Quality Commission published their final report on the 31 December 2014. Theyheld a Quality Summit on the 7 January 2015 which was attended by key stakeholdersacross Leeds and York.
The Trust Action Plan needs to be submitted by 13 February 2015.
RECOMMENDATIONS:
The Board is asked to note the system in place to manage action plans.

1
LEEDS AND YORK PARTNERSHIPS NHS FOUNDATION TRUST
Board of Director 29 January 2015
CQC Action Plan - Governance arrangements
1. Introduction
Following the Care Quality Commission’s announced inspection on 29th September 2014 the
Trust received the Final Inspection Reports on the 31st December 2014.
In line with the CQC publication process, a Quality Summit was held on the 7 January 2015.
The Summit was divided into two parts. Part one included a presentation by CQC of their
findings. Chris Butler, CE LYPFT, responded to these on behalf of the Trust. Anthony Deery,
Director of Nursing (Interim) then summarised the actions taken to date and outlined the
Trust’s plan for taking forward a detailed action plan.
Part two was chaired by Monitor. They informed the Summit of their decision that, in the
wake of the findings, no regulatory action would be required on their behalf. They proceeded
to invite stakeholders to comment on the findings and identify those areas where they could
support the Trust to achieve the actions required. This led to a helpful discussion, particularly
in respect of those areas where the Trust is dependent on third party decisions, for example
Bootham Park Hospital. Where third party agreement is essential, it is anticipated that this
will be negotiated and agreed through the Action Plan process. However some decisions
may require escalation to the Board and the CQC Fundamental Standards Group (see
below) will be responsible for ensuring this happens.
The Trust is required to submit an Action Plan to CQC by 13th February 2015. This must
include timescales for completion which will be open to challenge by CQC where they
believe the risk to safe care is too great.
2. Action plan development
The Board are aware, that following the inspection a Responsive Action Plan was created by
the Chief Nurse and Director of Quality Assurance that captured all findings reported by the
Care Quality Commission during their inspection. This action plan has been discussed at
Executive Team meetings and progress was reported to the Board in December 2014.
Progress in respect of the action plan was also presented at the CQC Quality Summit.
2
In response to the CQC full report, the Responsive Action Plan will be incorporated into a
comprehensive Trustwide Action Plan. This will set out how the CQC compliance actions will
be met, who is responsible for the action and within what timeframe.
3. CQC Fundamental Standards Group.
To take forward the Action Plan the Trust has established the following governance.
CQC Fundamental Standards GroupPurpose:
1. To ensure a comprehensive action plan is developed to address the CQC inspectionfindings published December 2014.
2. To integrate any outstanding CQC requirements into the action plan.
3. To review progress of the action plan and report to Quality Committee, ET, Board ofDirectors and Council of Governors.
4. To identify prospective actions that may be required to ensure ongoing complianceacross all of the Fundamental Standards.
5. To keep under review, at regular intervals (TBC), compliance with CQC registrationrequirements
Time and Frequency: 8:30 – 9:30am Fortnightly
Membership: Chair – Director of Nursing and Quality
Care Services – Chief Operating Officer and senior managers and clinicians Finance/Estates – Chief Financial Officer and senior managers HR – Director of Workforce Head of Clinical Governance Corporate Governance Medical Directorate – Medical Director/Chief Pharmacist Other members co-opted as required
Progress to date – See Attached Appendix 1
Anthony Deery
Director of Nursing and Quality (Interim)
29.1.15

Appendix 1CQC Action plan – progress update – 15.1.15
Action Date Comments RAG
1. CQC Fundamental StandardsGroup
13.1.15 LYPFT Action Plan template discussed and agreed
2. Care Services ManagementGroup meeting
14.1.15 Provider level Must Do’s – Actions agreed. Need to set timeframe.Provider level Should Do’s still to complete and all Core Service Must and Should Do’s.AJ to sort by Care Group and circulate. Care Services to populate action plan by 23.1.15
3. Care Service AssociateDirectors’ meeting
23.1.15 Need to ensure all Must and Should Do’s have been addressed with proposed timelines.Cross reference actions between Core Services and provider level to ensure consistency andwhere necessary avoid duplication.Further refinement of Draft Action Plan following this meeting.
4. Finance and Estates meeting 26.1.15 Review Must and Should Do actions regarding Estates and Maintenance issues to establish atimescale for delivery of required improvements.This will establish if any actions sit jointly with Care Services and the Chief Financial Officer’s
staff.
5.CQC Fundamental StandardsGroup
27.1.15 Consider Draft Action Plan to ensure all Corporate and Care Service actions have beenaddressed.Consider proposed timelines and advise accordingly. Further review by designated ActionLeads
6. Submit Draft Action Plan toAndrew Jackson
6.2.15
7. DoN&Q and AJ 9.2.15 Quality assure the Action Plan
8. CQC Fundamental StandardsGroup and ET
10.2.15 Final Draft Action Plan for consideration and approval.Submit to Quality Committee
9. Final Action Plan to QualityCommittee
12.2.15 For approval

Appendix 1CQC Action plan – progress update – 15.1.15
Action Date Comments RAG
10. Submission to CQC 13.2.15 Follow up monitoring of the Action Plan via fortnightly CQC FS Group

Page 1 of 11
DRAFT Quality CommitteeThursday 11 December 2014 at 09.30
Meeting rooms 1 and 2, Trust HQ
Present: Carl Thompson (Non-Executive Director) - ChairAmanda Spencer (Leeds Community LD Consultant)Howard Dews (Informatics Manager)Lynn Parkinson (Deputy Chief Operating Officer)Melanie Hird (Head of Clinical Governance)Donna Kemp (Care Programme Approach Development Manager)Bev Thornton (Recovery and Social Inclusion Worker)Helen Wiseman (Strategic Lead for Allied Health Professionals)Guy Brookes (Clinical Director to the Leeds Care Group)Jim Isherwood (Medical Director)Chris Butler (Chief Executive)Susan Tyler (Director of Workforce Development)Anthony Deery,( Interim Director of Nursing)Jill Copeland (Chief Operating Officer and Deputy Chief Executive)Barry Wright (Clinical Director)Cath Hill (Head of Corporate Governance and Trust Board Secretary)Jayne Hawkins (Head of OP Psychology and Therapy Services)
In attendance: Keisha Allen (Governance Support Assistant) (secretariat support andminutes)Elizabeth Day (Head of Clinical Audit) ( item 7)Andria Hanbury, Associate for Evidence-Based ImprovementAndrew Bottomley (Governor Observer)Julia Raven (Governor Observer)
ItemNo.
Description Action
1. Apologies
Apologies were received from Dr Steve Wright, Ms Linda Rose and Mr StevenWrigley-Howe.
Prof Thompson noted that members would be removed from the committee ifthey had been absent for three times or more in one year and that apologiesshould be sent to Miss Allen to be noted.
2. Declarations of Interest
No member of the committee declared a conflict of interest in any item on theagenda.
3. Minutes of the meeting held on 9 October 2014
The minutes were accepted as an accurate record subject to:An amendment to the paragraph of minute 8 (on page 3 of the minutes) toreflect, ‘CT suggested taking the quality of CPA to the Board for a high levelstrategic discussion’.

Page 2 of 11
ItemNo.
Description Action
4. Cumulative Action Log
Miss Allen presented the log of those actions agreed at previous meetings whichwere either still outstanding or recently completed. The committee received thecumulative action log and noted the progress with the actions.
Prof Thompson indicated that the Quality Accounts and Reports should beadded as a future agenda item and Mrs Hill explained that this item would beadded to the committee’s cycle of business and circulated to the committee.
KA
5. Matters arising
Mrs Kemp gave an update on the CPA Recovery Work Plan noting that adifferent approach had been taken around training following a discussion at thelast committee meeting and that work had been done around performance. MrsKemp reported that the work plan is still ongoing and would not be completed forat least 12 months.
Prof Thompson asked how the committee would be assured that there would beno changes within the next 12 months and Mrs Kemp responded that thecommittee will be assured through the CPA audit and the service users’feedback form.
With regard to the number of CPA reviews completed, Mr Deery stated that thecommittee could be assured that the Trust had met their target but that it is thequality of the process that needs to be improved. In respect of the CPA process,Mr Deery indicated that the outcome would be measured on whether serviceusers felt they were meaningfully involved in their care plans.
Ms Copeland noted that service users’ experience may not be clearly reflectedwhen recording audit outcomes due to the time when the audit is completed. Inresponse, Ms Thornton indicated that there is a need to have a Triangle of Careapproach as a method for ensuring service users are feeling valued. MsThornton suggested that positive stories about the quality of care provided toservices users could be promoted through the press as a means to demonstratethat service users are appreciated by the Trust. She agreed to liaise with MrsKemp on this. Mrs Tyler also mentioned that a new Head of Communicationshad recently joined the Trust and will be able to support this initiative.
The committee received the update and was broadly assured with regard to theupdate on CPA/recovery Work Plan.
DK/BT/ST
6. Minutes from the sub-committees
The committee received the minutes of the sub-committees. These were:
6.1 Health and Safety Committee
6.2Infection Control and Medical DevicesCommittee
6.3 The Effective Care Committee
6.4 Trust Incident Review Group
6.5 Safeguarding Committee

Page 3 of 11
ItemNo.
Description Action
Members agreed to review the minutes of the sub-committees outside of themeeting and in future to avoid duplicating work of the sub-committees at themeeting; Prof Thompson encouraged the chairs of the sub-committees toescalate any significant matter from their respective sub-committees to theQuality Committee which they believe merits Board attention.
In this respect Mr Deery pointed out a matter from the Health and SafetyCommittee minutes relating to concerns at the Becklin centre. Mr Deery reportedthat he had met with Mrs Parkinson to discuss his findings following a seriousincident that happened at the Becklin centre noting that this would be fed into theHealth and Safety minutes action plan. It was agreed that the Board will beadvised of this matter and agreed to incorporate the following wording into thecommittee minutes:
‘The findings of the Health and Safety Committee in regards to loneworkers are being followed-up in the light of a serious incident at theBecklin Centre and that the actions arising following the Health andSafety meeting were noted.’
The committee considered the implication of the serious incident in respect ofthe Trust’s Statutory Duty of Candour. Prof Thompson advised the committeethat the Statutory Duty of Candour agenda item has been deferred to February’scommittee meeting; noting that at present the committee could not be assuredthat the Trust is satisfying all elements of the Statutory Duty of Candour but thatat its February meeting, the committee will expect to receive a detailed report (asa discussion item) on how the Trust is satisfying its statutory obligations.
The committee received and noted the minutes of the sub-committees.
AD/JI
7. Progress on Clinical Audit Plan 2014/2015
Ms Day presented the Clinical Audit Plan for 2014/2015 noting that the auditplan presented is a priority plan which provides a synopsis of the audit workcarried out. Ms Day reported that the Trust’s database had been modified tofocus on specific themes of the audit such as record keeping, physical health,safe guarding, the Mental Health Act and CPA to make it easier to provide areport on audit activities on these themes. Ms Day reported that there arechanges with regard to audit work by the clinical care groups for example theLeeds Care Group now has a specific audit group.
The committee discussed the report and it was noted that it appreciated thesignificance of conducting audits but requested a report on how clinical audit isbetter disseminated and examined. The committee received assurance thatimplementation of the Trust priority plan is managed efficiently. ED
Effectiveness
8. Worsley Court – Action Plan
Mr Deery introduced the Worsley Court action plan and report and updated thecommittee on a serious incident that happened at Worsley Court. Mr Deeryreported that following the death of an inpatient whose death was recorded as aresult of natural causes, concerns were raised with regard to her quality of careprior to her death. Mr Deery advised the committee that this had led to a widerinvestigation in respect of the care practices at Worsley Court and following the

Page 4 of 11
ItemNo.
Description Action
findings a decision was made to temporarily close the unit and to introduce atraining and development programme for staff at Worsley Court. Mr Deeryreported that the training had been undertaken throughout October and earlyNovember and staff were assessed in respect of the Trust’s values and the 6Cs(care, compassion, competence, communication, courage and commitment). MrDeery noted that following this assessment there were training needs required.In order to complete the necessary training and because of ongoing safetyconcerns Mr Deery said the unit could not be opened; but that furtherdevelopment plans would be introduced and that the unit is expected to bepartially reopen on 11 January 2015 and moving towards full reopening on 15February 2015.
Prof Thompson opened the discussion and asked about the views of thecommissioners and the professional implications of Worsley Court on staff. MrDeery responded that the commissioners are aware of the incident and aresatisfied with the action plan; and that the main professional implication whicharose was to ensure staff members are fully trained.
Mr Butler asked with regard to the reopening of Worsley Court where the serviceusers are to be drawn from and noted that there are questions in relation tohaving an older people’s mental health service in York. These issues ProfThompson suggested discussing at a later meeting. In respect of the questionaround mixed sex wards, Mr Deery reported that the CQC considered thatWorsley Court did not meet the mixed sex mental health wards standards andhave issued the Trust with a compliance order. Mr Deery explained thatfollowing a discussion with the commissioners, they have asked for an optionspaper which may include an option around environmental work or an option tomove to a single sex unit. However, Mr Butler replied that the Trust reserves itsright to deliver on the compliance order as it sees fit.
Ms Wiseman raised concerns about working in isolation and Ms Thorntonsuggested that Mr John Thorpe (Recovery Social Inclusion Worker) had donesome work at Bootham Park Hospital around this and could offer some advice.Ms Copeland agreed to liaise with Ms Thornton and indicated that Mr Thorpe’swork could be fed into the Business Improvement Plan. Ms Thornton suggestedthat in terms of supporting staff that peer support could be considered and MsCopeland agreed to take this forward.
Dr Isherwood stated that with regard to communication with staff, informationshould be disseminated in a reader-friendly, targeted manner which would easilyhighlight issues of concerns. Further, Dr Isherwood agreed that there was aneed to prevent staff working in isolation; suggested that staff should rotatearound wards and suggested an examination of the circumstances.
The committee requested a lessons learnt/reflective report to be brought to thenext committee meeting with messages that could be disseminated widely.
Mr Deery agreed to amend the report to ensure it did not contain any person’sidentifiable information.
Dr Isherwood was concerned that from the Worsley Court report it was notedthat in order to partially reopen Worsley Court it may be necessary to moveexisting staff from Peppermill Court and Meadowfields and questioned theimpact this would have on those two units. Mrs Parkinson assured the
JC
AD
AD
Page 5 of 11
ItemNo.
Description Action
committee that the process would be conducted in a careful way to avoid anyadverse impact.
The committee considered the report and noted the contents of the paper.
9. Research Report
Dr Isherwood gave a brief update on developments with regard to currentperformance by the Research and Development Team in meeting nationalresearch targets.
The committee received and noted the Research Report from information.10. Quality Indicators Implementation Plan
Mr Dews introduced the Quality Indicators Implementation Plan noting thatquality indicators for inpatient units are now being provided to clinical managersroutinely on a monthly basis and that a workshop with clinical managers will beheld in the new year to discuss how the indicators can be used by clinical teams.Members of the committee found the indicators to be useful.
A discussion followed with regard to accessing information from PARIS and theCognos system. With regard to the Cognos system, Mr Deery enquired aboutthe process for retrieving data and Mr Dews replied that currently staff receivean email to alert them that the information is available before they could accessthe information but that staff had some reservations with regard to using thesystem. Mr Dews stated that further development to the Cognos system will beundertaken to make it more user-friendly to staff and to improve speed. ProfThompson felt that staff having direct access to the Cognos system would bemore efficient and agreed to take this up with Mrs Hanwell outside of themeeting.
The committee considered the report and noted the implementation plan.
CT
11. Refreshed Workforce Development Strategy
Mrs Tyler presented the revised Workforce Strategy document and asked the
committee to agree the amendments in the document. A brief discussion
followed in respect of the Trust’s ‘Career Framework’ and staff pay and Mrs
Tyler explained that currently some staff were receiving higher earnings
compared with the NHS average earnings. She added that in respect of
measuring quality that the framework will ensure that there is a skilled workforce
whilst at the same time ensuring that staff are being paid appropriately for the
work they do.
The committee noted the report and agreed the revised Workforce Strategydocument.
12. Improving the quality and uptake of key CPA recommendations: planoverview
Dr Hanbury gave a presentation on evidence-based improvement in clinicalareas where the Trust is experiencing difficulty in stimulating change andidentified what the barriers to change are. The committee was pleased with thepresentation and noted the recommendations.
12.1 Professionals meetings good practice guidance

Page 6 of 11
ItemNo.
Description Action
The committee ratified the good practice guidance as an appendix to the CPAPolicy.
13. Board Assurance Framework (BAF)
Mrs Hill presented the Board Assurance Framework which sets out those key
controls in place to ensure that the risks to achieving the strategic objectives are
being well managed. The committee considered the BAF and Prof Thompson
asked for the framework to include a statement in respect of what should
happen when a committee is not assured on a matter. Mrs Hill agreed to
complete this action.
The committee noted where the Quality Committee is named as an assurance
receiver in the BAF and confirmed that within the context of the committee and
the cycle of business it has had sufficient assurance on the effectiveness of the
controls.
CH
Safety
14. Lessons Learned Report
Mrs Hird presented the Lessons Learnt Report which brings together informationabout incidents and complaints and considers trends, themes and lessonslearnt. The committee noted the contents of the report.
15. Bootham Park Hospital Quality Improvement Plan
The committee received and considered in some detail the Bootham ParkHospital Quality Improvement Plan and an update from Mrs Parkinson andnoted that this was version 10 of the plan. The committee noted the progress ofthe plan.
16. Compulsory Training Update
Mrs Tyler presented the Compulsory Training Update report noting that theExecutive Team has approved the Learning Management System, the e-Learning Platform; and that it is expected to be a more efficient e-learningprogramme and it is anticipated to increase compulsory training compliance.
The committee was assured of the procurement of a new Learning ManagementSystem; assured that the reporting areas are correctly captured and wasassured that the curriculum reviews have occurred or is close to completion.
16.1 The Prevention and Management of Violence and Aggression (PMVA)review
Mrs Tyler presented a report on the PMVA review noting that the report outlinesthe progress that had been made towards reducing the use of physicalrestraints. The committee was assured of the improvement actions that aretaking place within the Trust, in particular that the Trust has the right clinical skill-set to deal with PMVA issues.
The committee noted the contents of the paper.17. Procedure for the administration to adults of oil-based depot and other

Page 7 of 11
ItemNo.
Description Action
long-acting intramuscular injections
The committee received the procedure for ratification following approval at theEffective Care Committee on the 11th September 2014. The committee ratifiedthe procedure.
18. CQC revised responsive action plan
The CQC revised responsive action plan was deferred to the February meeting.Prof Thompson advised the committee that after the Quality Summit on the 7January 2015 that it is anticipated that a full responsive action plan will beproduced and be discussed in detail at the committee meeting in February.
19. Sign up to Safety
Dr Isherwood presented the final draft of the Sign up to Safety report noting that
at the previous Quality Committee meeting the report was discussed in detail.
The committee was asked to recommend that the Board signs up to safety and
Dr Isherwood advised that once the Board agree to this it would be committing
to the 5 pledges outlined in the report.
Dr Isherwood reported that since the last committee meeting he had inserted the
below paragraph into the report in respect to the Duty of Candour:
The Trust will expect all staff to contribute to its determination toprovide safe care and, in doing so, to uphold a common Duty ofCandour and to meet the responsibilities articulated in theirprofessional standards.
The committee considered this insertion and Dr Isherwood was asked to includethe word ‘Statutory’ where it referred to Duty of Candour in the report. Thecommittee approved the final version of the action plan and recommended theplan to the Board that it signs up to this safety initiative.
JI
Experience
20. National Service User Inpatient Survey
This agenda item has been deferred to the next committee meeting. AJH
21. Meeting the requirements of the Statutory Duty of Candour
This agenda item has been deferred to the next committee meeting AD
Committee Governance
22. Quality Committee Refreshed Terms of Reference
Mrs Hill introduced the Quality Committee refreshed Terms of Reference notingthat there were some structural changes that needed to be reflected in theTerms of Reference. With regard to the membership, Ms Wiseman noted that ata previous committee meeting that she was recorded as a member of thecommittee but that this had not been reflected in the Terms of Reference. MrsHill agreed to update the membership of the committee and to include MsWiseman’s role in the Terms of Reference. It was agreed that the membershipof the committee would be discussed outside of the meeting.
CH

Page 8 of 11
ItemNo.
Description Action
In addition Mrs Tyler indicated that the Workforce Steering Group requiredstronger accountability through the governance structure and suggested theQuality Committee as a useful channel. Although there was minor dissent giventhat there will be a governance review in the new year, the committee agreed torecommend to the Board to have the Workforce Steering Group temporarilyreport to the Quality Committee until further consideration with regard to where itshould sit within the governance structure is made.
Mr Deery added that the committee receives a number of policies andprocedures for ratification and wondered why. Mrs Hill agreed to circulate apaper to Mr Deery that had been agreed by the Executive Team on whereprocedures are approved and ratified.
The committee noted the Terms of Reference have been refreshed to a point,but that there is still more work to do and approved the changes alreadyhighlighted in red. Mrs Hill agreed to liaise further with some individuals in orderto finalise the Terms of Reference and noted that she would present the nextversion of the Terms of Reference to the committee meeting in February beforeit is submitted to the Board of Directors for ratification.
CH
CH
CH
23. Effectiveness of the Medical Revalidation & Appraisal Group Terms ofReference
Dr Isherwood presented the Medical Revalidation & Appraisal Group Terms ofReference and appendices.
The committee ratified the Medical Revalidation and Appraisal Group’s Terms ofReference; noted the results and comments from the questionnaire (AppendixA); and approved the method of reporting the summary of the meetings of theMedical Revalidation and Appraisal Group (Appendix B).
24. Meeting Dates for 2015 (enclosure)
The committee received and noted the dates and venues for Quality Committeemeetings in 2015.
25. Committee Effectiveness
The committee received the committee effectiveness questionnaire, inaccordance with its Terms of Reference and with best practice. The Committeewas asked to complete the questionnaire and to return it to Mrs Hill.
ALL
26. Any other business notified to the Chair before the start of the meeting
Ms Thornton gave a brief update on the situation at Inkwell and Mr Butlerconfirmed he and Mrs Hanwell were aware of it and were considering puttingforward an objection to planning permission.
27.Date and time of next meeting
The next meeting will be held on Thursday 12 February 2014 at 13.30 - MR1&2,Trust HQ.

Page 9 of 11
QUALITY COMMITTEE - ACTION SUMMARY
Thursday 11 December 2014
MINUTE ACTION SUMMARY LEAD
4
Cumulative Action Log
Prof Thompson indicated that the Quality Accounts and Reports should beadded as a future agenda item and Mrs Hill explained that this item would beadded to the committee’s cycle of business and circulated to the committee.
AK
5
Matters arising
Ms Thornton suggested that positive stories about the quality of care providedto services users could be promoted through the press as a means todemonstrate that service users are appreciated by the Trust. She agreed toliaise with Mrs Kemp on this. Mrs Tyler also mentioned that a new Head ofCommunications had recently joined the Trust and will be able to support thisinitiative.
DK/BT/ST
6
Minutes from the sub-committees
Members agreed to review the minutes of the sub-committees outside of themeeting and in future to avoid duplicating work of the sub-committees at themeeting, Prof Thompson encouraged the chairs of the sub-committees toescalate any significant matter from their respective sub-committees to theQuality Committee which they believe merits Board’s attention.
CHAIRS OFTHE SUB-
COMMITTEES
7
Progress on Clinical Audit Plan 2014/2015
The committee discussed the report and it was noted that it appreciated thesignificance of conducting audits but requested a report on how clinical audit isbetter disseminated and examined. The committee received assurance thatimplementation of the Trust priority plan is managed efficiently.
ED
8
Worsley Court – Action Plan
Ms Wiseman raised concerns about working in isolation and Ms Thorntonsuggested that Mr John Thorpe (Recovery Social Inclusion Worker) had donesome work at Bootham Park Hospital around this and could offer some advice.Ms Copeland agreed to liaise with Ms Thornton and indicated that Mr Thorpe’swork could be fed into the Business Improvement Plan. Ms Thorntonsuggested that in terms of supporting staff that peer support could beconsidered and Ms Copeland agreed to take this forward.
JC
8
Worsley Court – Action Plan
The committee requested a lessons learnt/reflective report to be brought to thenext committee meeting with messages that could be disseminated widely. MrDeery agreed to amend the report to ensure it did not contain any person’sidentifiable information.
AD

Page 10 of 11
MINUTE ACTION SUMMARY LEAD
10
Quality Indicators Implementation Plan
Mr Dews stated that further development to the Cognos system will beundertaken to make it more user-friendly to staff and to improve speed. ProfThompson felt that staff having direct access to the Cognos system would bemore efficient and agreed to take this up with Mrs Hanwell outside of themeeting.
CT
13
Board Assurance Framework (BAF)
Mrs Hill presented the Board Assurance Framework which sets out those key
controls in place to ensure that the risks to achieving the strategic objectives
are being well managed. The committee considered the BAF and Prof
Thompson asked for the framework to include a statement in respect of what
should happen when a committee is not assured on a matter. Mrs Hill agreed
to complete this action.
CH
19
Sign up to Safety
Dr Isherwood reported that since the last committee meeting he had inserted
the below paragraph into the report in respect to the Duty of Candour:
The Trust will expect all staff to contribute to its determination toprovide safe care and, in doing so, to uphold a common Duty ofCandour and to meet the responsibilities articulated in theirprofessional standards.
The committee considered this insertion and Dr Isherwood was asked toinclude the word ‘Statutory’ where it referred to Duty of Candour in the report.
JI
20
National Service User Inpatient Survey
This agenda item has been deferred to the next committee meetingAJH
21
Meeting the requirements of the Statutory Duty of Candour
This agenda item has been deferred to the next committee meetingAD

Page 11 of 11
MINUTE ACTION SUMMARY LEAD
22
Quality Committee Refreshed Terms of Reference
With regard to the membership, Mrs Hill agreed to update the membership ofthe committee and to include Ms Wiseman’s role in the Terms of Reference.
In addition Mrs Tyler indicated that the Workforce Steering Group requiredstronger accountability through the governance structure and suggested theQuality Committee as a useful channel. Although there was minor dissentgiven that there will be a governance review in the new year, the committeeagreed to recommend to the Board to have the Workforce Steering Grouptemporarily report to the Quality Committee until further consideration withregard to where it should sit within the governance structure is made.
Mrs Hill agreed to circulate a paper to Mr Deery that had been agreed by theExecutive Team on where procedures are approved and ratified.
The committee noted the Terms of Reference have been refreshed to a point,but that there is still more work to do; and approved the changes alreadyhighlighted in red. Mrs Hill agreed to liaise further with some individuals inorder to finalise the Terms of Reference and noted that she would present thenext version of the Terms of Reference to the committee meeting in Februarybefore it is submitted to the Board of Directors for ratification.
CH
25
Committee Effectiveness
The committee received the committee effectiveness questionnaire, inaccordance with its Terms of Reference and with best practice. The Committeewas asked to complete the questionnaire and to return it to Mrs Hill.
ALL

1MHA Committee Meeting Minutes 15
thDecember 2014
LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
Minutes of the Mental Health Act Committee Meeting
Held on; Monday 15th December 2014 1.30pm – 4.00pm, Trust Head Quarters
LIST OF PEOPLE AT THE MEETING;
Members of the group
Mr Keith Woodhouse Non-Executive Director - Chair of the meeting
Mr Anthony Deery Director of Nursing and Quality (interim)
Mr Stephen Wrigley-Howe Non-Executive Director
In attendance
Mrs Gill Walton Mental Health Legislation Manager
Ms Melanie Hird Associate Director
Dr Chris Hosker Associate Medical Director
Mrs Cath Hill Head of Corporate Governance
Ms Alison Kenyon Associate Director
Dr David Leung Responsible Clinician
Mrs Elizabeth Day Head of Clinical Audit & NICE Guidelines
Ms Sue Ledwith Clinical Psychologist
Miss Carly Thimm Administrator
Observer
Ms Kumari Priyanka Trainee
Actions1 Welcome and Introductions
2 Apologies for Absence
Mr Kwai Mo, Ms Lindsay Britton, Mr Cameron Brookes, Ms Lynn Parkinson, MsClaire Woodam, Mr Andy Weir
3 Minutes and Actions of the Meeting held on; Thursday 16th October 2014
Minutes:
Mrs Hill advised that Mr Marran’s apologies should not be noted as he is not asubstantive member of the group, and that Ms Parkinson attended the last meetingso needs to be added on to the list in attendance.
Miss Thimm assured Mr Woodhouse that a cumulative list of all actions since thecommencement of the committee is kept, but only outstanding actions brought tothe meeting.
CT

2MHA Committee Meeting Minutes 15
thDecember 2014
Actions:
14/004 Mr Woodhouse requested an update and a copy of the priorities that wereagreed. Ms Hird confirms that this action also takes in to account action 14/007(trends and themes). Ms Hird stated that Ms Jill Copeland (Deputy ChiefExecutive) has been asked to obtain an update from Ms Parkinson regarding thepriorities and that a paper detailing these will be brought to the next meeting.
Mr Woodhouse does not wish work to be duplicated, as there are two committeeswith similar interests. Mr Deery is happy to make a link between the Mental HealthAct Committee and the Quality Committee in taking actions forward, primarily thosesurrounding CPA. Mrs Day advised that the clinical audit team are available to aidthe group in any audit’s moving forward.
14/008 Ms Hird and Mrs Walton confirmed that all copies of original detentionpaperwork are stored on PARIS for all to access.
14/010 Ms Hird confirmed that the Mental Health Legislation Report was on theagenda for discussion, but reiterated that no feedback had been received from thegroup as to what the members wished to see within the report.
14/012 Mrs Walton confirmed that the centralisation of Mental Health Actadministration will commence on 19 January 2015 starting with the Becklin Centre.
14/014 Mrs Walton and Dr Hosker have received comments about the s17 leaveform, both old and new, and further work was to be done in moving this forward forall to use.
MH
4 Updated Terms of Reference and Work Plan
Mrs Hill was asked to look at the quoracy of the committee at the meeting inOctober; this was a direct result of the Chief Nurse not attending. Mrs Hill hasreworded the Terms of Reference to allow another executive director to attend butthis person is required to have the specialist knowledge of the Mental Health Act.The committee were in agreement with the new wording; however Mr Woodhouserequested that Mrs Hill be the person to source a replacement should the chiefnurse not be able to attend.
Mrs Hill also advised that the name of the committee be changed to the MentalHealth Legislation Committee; this will then cover both the Mental Health Act andthe Mental Capacity Act.
The work plan has also been amended following consultation with Ms Hird andMiss Thimm, and the cycle of business has also been amended to reflect the abovechanges.
The committee accepted and authorised the changes.
5 Service User Feedback
Ms Hird confirmed that this paper was compiled by Mr Andrew Howarth, the aimbeing that the committee confirm what is to be considered in terms of patientfeedback.

3MHA Committee Meeting Minutes 15
thDecember 2014
A discussion was held surrounding the points raised within the report, primarilyconcerning the giving of patient rights. Ms Hird confirmed that this is one of the toppriorities been dealt with and a paper will be submitted at the next meeting todiscuss further.
Ms Hird advised the committee that service user feedback was the only work planitem for quarter 3, and asked if this should stay as such. Mr Woodhouse stated thatthe report should come to the committee for information, but was assured that workwas been undertaken in other committees and meetings to address the issuesraised.
6 MCA Supreme court ruling
Mr Deery stated that the paper had been to the last Trust Board meeting and setsout the implications of the ruling regarding Deprivation of Liberty Safeguards(DoLS). Mr Deery confirmed that the purpose of this paper was to establish if thetrust had captured the implications regarding resources, policy and procedures inline with the court decision. It was suggested that a piece of work be completed toidentify the resources needed to fully comply with the ruling, and this to be takenback to the board.
Mr Deery is to lead on this paper and take the findings back to the board; howeverMr Woodhouse is happy for this piece of work to come back to the committee fortesting.
AD
7 Publication to consider
7.1 First Tier Tribunal Practice Direction
Mrs Walton highlighted the implications of the practice direction that was issued onthe 17th November. The Tribunal Service is becoming much more stringent on theirtimescales which if not adhered to could resort in a final sanction of a summons.
It was confirmed that since the 17th November, a further 21 Order to AnswerQuestions had been received from the Tribunal Service.
Mrs Walton advised the group that an all user email had been sent, however MsKenyon advised that this should go through clinical governance councils as well asgoing to Clinical Directors and Associate Directors. Mrs Walton is to circulate thisinformation to all mentioned.
Ms Kenyon would like to see a detailed breakdown of who is submitting late reportsto enable support to be given to those areas to ensure the submission dates areadhered to. Ms Hird requested that a process be put together for reporting onbreaches of reports.
GW
GW &CT
8 Trust Reports
8.1 Use of Community Treatment Order (CTOs) across Leeds and York Services
Dr Hosker advised the group that obtaining all data from York was problematic dueto the use of CPD systems. Dr Hosker discussed the report and its findings withthe committee.

4MHA Committee Meeting Minutes 15
thDecember 2014
Mr Woodhouse thanked Dr Hosker for the time spent on compiling the report andnarrative as it was found to be of great use. Mr Woodhouse was of the view thatthere was no requirement to take this forward, however Mr Wrigley-Howe still hasreservations as to why there are twice as many CTOs in Leeds than York and feelsthis needs further investigation.
Dr Hosker is of the opinion that this may need to go to Ms Alison Thompson as apossible research project. Dr Hosker is to speak with Dr Hughes for views on this.
Mr Deery questioned why data on ethnicity was not captured across the trust inrelation to detained patients. Mrs Walton confirmed again the difficultiesencountered by the Informatics Department when attempting to obtain data fromthe CPD system used in York. Mr Deery stated that Mental Health Act minimumdata set should be capturing this information.
List of actions:
- Report to be sent to Quality Committee for a view / information- To speak with Alison Thompson / Dr Hughes for a possible research project
to consider whether our use of CTOs I s effective and to consider if anyfurther work around variance is worthy of further research
- A copy of the report to be sent to the Chair of the Trust- The report is to be circulated to the Mental Health Act Managers
Mr Woodhouse again thanked Dr Hosker for his work on the report as it hadanswered the fundamental questions as to why there was a difference betweenboth areas.
CH
GW &CH
CT
8.2 Mental Health Legislation Report
Ms Hird confirmed that Mrs Walton, herself, Dr Hosker and Miss Thimm had met ona number of occasions to discuss the progress of a new Mental Health Legislationreport, but that the report was still not as well formed as was hoped.
Dr Hosker talked the committee through the report, however it was agreed that allcomments be sent to Dr Hosker following the meeting.
A discussion was held surrounding the use of control and restraint at learningdisability sites as the figures seemed much higher than those of other units, thiswas confirmed to a result of the nature of the wards as challenging behaviour andlearning disabilities.
Mr Woodhouse stated that the report was much improved but further work was tobe done.
ALL
8.3 Mental Health Act CQC Inspections Quarter 2 2014
Mrs Walton confirmed that the report format had changed, but this was to make thereport and information simpler to access and understand. The report itself goesthrough the lists of recommendations for each unit, the actions agreed to be takenby the staff and then whether or not those actions have been implemented. It wasconfirmed that each feedback summary contains a lot more detail should staff needto access this.
5MHA Committee Meeting Minutes 15
thDecember 2014
The committee discussed the confusion surrounding having single ad hocinspections at the same time as having the large inspection in September.
Mr Woodhouse confirmed that all actions seemed to be in order and adequatelymanaged. However, Ms Hird stated that the actions from the previous report werenot detailed in this quarter, so for quality and assurance those actions that were notmet would be brought back to the next meeting with updates.
Ms Hird discussed the process of feedback summaries and provider actionstatement and confirmed that the trust needs to improve its view on looking acrossall reports and detailing themes and actions. Ms Hird is to raise this at her next 1:1with Mr Deery.
It was confirmed by Mrs Walton that all provider action statements are / have beensigned off by the chief nurse before submission to the CQC.
GW &MH
MH
8.4 Mental Health Act Managers Forum Feedback
Mr Woodhouse confirmed these minutes are for information purposes only.
Mrs Walton raised a concern regarding the loss of experienced Mental Health ActManagers in September 2015, it has been agreed to continue to review the risk.Mrs Walton has spoken to those who are due to end their contracts on 30September 2015 and 11 are interested in extending their contract for a further 12months. Mr Woodhouse is happy for this to happen if there is justification to do so,therefore Mrs Walton is to prepare a proposal for the next meeting.
Mrs Walton informed the meeting that a request had been made to amend theremuneration arrangements for Mental Health Act Manager to enable them to claiman addition 5p per mile when passengers were carried on trust business. MrsWalton agreed to review the current remuneration.
GW
9 Procedural Documents for Ratification
9.1 Mental Capacity Act
Mrs Walton confirmed that the Mental Capacity Act protocol had been through thenecessary consultation process, however the feedback was minimal. Therefore thecommittee were asked to ratify the protocol but a short review period was to beadded.
The protocol was ratified by the committee.
9. Section 58
Mrs Walton confirmed that the Section 58 protocol had been through the approvalprocess with full consultation, however certain aspects of the operation cannot takeeffect until the centralisation of Health Records and the Mental Health LegislationDepartment.
Mr Woodhouse was concerned that he was not sufficiently qualified to sign off onsuch a complex document, Dr Hosker reassured Mr Woodhouse that a robustratification process was followed.

6MHA Committee Meeting Minutes 15
thDecember 2014
The protocol was ratified by the committee.
10 Clinical Audit – Completion of care plans in preparation of Tribunals
Mrs Day explained to the committee why the audit was undertaken, and highlightedthe cover sheet as this outlines the main findings and recommendations that weremade.
A discussion was held regarding the findings.
Mr Woodhouse raised concerns around the findings as they were not in line withthe findings of the CQC visit in September, and also personal experience fromattending hearings.
Mrs Day stated that information for the audit was gathered in an effective andconsistent way, which was very focused on the one aspect of discharge careplanning and nothing more. The Tribunal judiciary advice was used inbenchmarking the areas that had to be covered.
The committee were satisfied with the findings of the audit.
11 Risk Register
Ms Hird confirmed that the risks shown only pertain to this committee.
Mrs Hill asked if Mental Health Act and Mental Capacity Act training should be onthe risk register as the Mental Health Legislation Report showed a very smallpercentage of staff trained. Mr Woodhouse requested that training go on the riskregister.
GW
12 Board Assurance Framework
Mrs Hill stated that the committee had seen this report before, however were notlisted as a reassurance receiver and asked the committee if they wished this to bechanged.
Mr Woodhouse is happy for the committee to remain as a receiver only.
13 Committee Effectiveness Questionnaire
Mrs Hill is to send out the questionnaire with feedback to be sent back before thenext committee meeting.
CH
14 Any other business
14.1 Changed to AMD for MHL
Dr Hosker advised the committee that he is leaving the post of Associate MedicalDirector for Mental Health Legislation at the end of the December. Dr Hosker willnot be able to assist the committee past this point.
Ms Hird confirmed that an internal process to replace Dr Hosker will commence inthe new year.

7MHA Committee Meeting Minutes 15
thDecember 2014
Mr Woodhouse thanked Dr Hosker for being diligent and patient in his role asAssociate Medical Director and wished Dr Hosker the very best in his new role.
14.2 Article of Nearest Relative Barring Order Hearings
Dr Leung attended to talk to his report on barring order hearings. The committeediscussed the findings of the report.
It was agreed by the committee that further education and training was required forResponsible Clinicians, Mental Health Act Managers and other trainedprofessionals in the additional criteria of dangerousness.
Dr Leung wishes to publish the paper, but would like feedback from the MentalHealth Act Managers and Steven Evans of Hempsons Solicitors. Mr Woodhouseinvited Dr Leung to attend the next MHAMs Forum meeting in January. MissThimm to send out the date and time.
GW
CT
Mr Woodhouse thanked the members for their attendance and closed the meetingat 4.30pm
The next meeting will be held on Monday 16th March 2015, 1.30pm – 4.00pm –Trust Head Quarters
Actions Log
AgendaItem
Action Lead
3 To add Ms Parkinson as attendee at committee meeting inOctober
CT
3 Paper detailing top priorities agreed with Ms Parkinson to cometo next meeting
MH
6 Mr Deery to identify resource needs in regards to the ruling ofDeprivation of Liberty Safeguards and feedback to thecommittee.
AD
7.1 Mrs Walton to send practice direction to all clinical and associatedirectors for action.
GW
7.1 A process is to be completed on how we raise and recordbreaches of the report standards for Tribunals.
GW & CT
8.1 Dr Hosker to liaise with Dr Hughes and Alison Thompson to gainviews on CTO research project.
CH
8.1 CTO report to be sent to the Quality Committee CT8.1 CTO report to be sent to the chair of the trust. CT8.1 CTO report to be circulated to the Mental Health Act Manager CT8.2 All comments regarding the MHL Report to be sent to Dr Hosker ALL8.3 Outstanding actions from previous quarter of CQC visits to be
added to the next paperGW & MH
8.3 Mrs Hird to raise themes and actions with Mr Deery at the next1:1
MH
8.4 Mrs Walton to prepare a proposal confirming the number ofMental Health Act Managers required to enable the trust to carryout its responsibilities in relation to review of detention
GW
11 Training to go on the Risk Register GW13 Mrs Hill to send out effectiveness questionnaire CH
14.2 Dr Leung to be invited to the next MHAMs Forum Meeting CT14.2 Further education to be given to RCs and MHAMs surrounding GW

8MHA Committee Meeting Minutes 15
thDecember 2014
Barring Order Hearings

1
AGENDA ITEM 14.1
LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
Minutes of the Audit Committee Meetingheld on 13 November 2014 in Meeting Room 1 at Trust Headquarters
Present:
Mrs J Tankard, Non-executive Director (Chair of the Audit Committee)Dr G Taylor, Non-executive DirectorMrs M Sentamu, Non-executive Director
In Attendance:
Mr F Griffiths, Chair of the TrustMr C Butler, Chief ExecutiveMrs D Hanwell, Chief Financial OfficerMr I Looker, Partner, PricewaterhouseCoopers LLPMr J Fenton, Audit Manager, PricewaterhouseCoopers LLPMr N Bell, Head of Internal Audit, West Yorkshire Audit ConsortiumMrs S Blackburn, Deputy Head of Internal Audit, North Yorkshire Audit ServicesMrs L O'Reilly, Local Counter Fraud Specialist, West Yorkshire Audit Consortium.Ms E Day, Head of Clinical Audit (for minute number 14/095)Mr A Deery, Interim Director of Nursing (for minute numbers 14/097 and 14/098)Ms J Copeland, Chief Operating Officer (for minute number 14/102)Mrs C Hill, Head of Corporate Governance (secretariat)Miss K Allen, Governance Support Assistant (minutes)
Full details and supporting agenda papers are filed in the Chief Executive’s Office. However, some of thedetails of the issues discussed are of a confidential nature and the papers are not for circulation.
ActionMrs Tankard opened the meeting and welcomed everyone.
14/086 Apologies (agenda item 1)
There were no apologies received.
14/087 Declaration of any conflicts of interest in respect of agenda Items (agenda item 2)
No member of the committee declared a conflict of interest in respect of any item on theagenda.
14/088 Minutes of the meeting held on 12 September 2014 (agenda item 3)
The minutes of the meeting held on 12 September 2014 were agreed as a true record.
14/089 Matters arising (agenda item 4)
Mrs Hanwell gave an update to the committee about the fraud case noting that thedefendants had been charged and will appear at the crown court where it is expectedpleas will be entered. Mrs Hanwell advised the committee as to the advice received fromNHS Protect as to how it should proceed at the current time. It was noted that at somepoint details of the case would need to be communicated to staff and the public, but that

2
no action must be taken which could prejudice the case.
Mr Griffiths raised concerns about the reputational damage that could ensue from thecase and sought assurance as to the action that will be taken to mitigate any potentialrisk. It was noted that that there are other partners involved namely NHS England andLeeds Community Health but that the Trust was the majority partner in the case. It wasalso noted that the committee had discussed the implications of the case before and wasaware that it was imperative to not do anything that will prejudice the proceedings.
The committee discussed the matter and was of the view that a press release would notbe sufficient in dealing with the matter therefore Mr Butler agreed to liaise further with MrsTyler and colleagues in the communications team to agree the lead partner. However, MrButler suggested putting himself forward in the first instance to ensure that the Trustremains in control of the messages that will emerge about the case.
The committee agreed that refreshed legal advice should be sought as to what the Trustis allowed to disclose. Mrs Hanwell agreed to contact the Trust’s solicitor.
DH
14/090 Reports from PricewaterhouseCoopers LLP – Audit and Sector Updates (agendaitem 6.1)
Mr Fenton presented the update progress report for the external audit for 2014/15financial year which contains a general audit update and sector developments. Mr Fentonreported that the audit update section of the paper contains the audit timetable for nextyear noting that the auditors will be meeting with Trust officers and staff over the comingweeks to produce an audit plan, which will be presented to the committee at its nextmeeting in January.
Mr Fenton reported that the auditors will also meet with staff to discuss updates inrespect of updates to the accounting standards and the refreshed Annual ReportingManual from Monitor. Mr Fenton reminded the committee of the proposed changes tothe Annual Reporting Manual, which were discussed at its last meeting in September,noting that the consultation on this was still ongoing but that once finalised he will providean update to the committee.
With regard to the sector developments, Mr Fenton noted that this sets out a comparisonof the Trusts’ performance for the first quarter of the financial noting that the Trust wasmeeting the sector average for mental health. Mr Fenton reported that the costimprovement plans were performing better than expected overall and that the Trust isabove the 5% threshold although other Trusts have fallen below their targets for the year.
The committee received the internal auditor’s progress report and noted the contents.
14/091 Reports from the External Auditors (PricewaterhouseCoopers LLP) – A Safer NHS:the evolving focus on governance in the NHS (agenda item 6.2)
Mr Fenton presented the second report from PricewaterhouseCoopers which discussed‘A Safer NHS: the evolving focus on governance in the NHS;’ noting that this had beendeveloped from their work across the sector noting that it highlights consistent themeswithin failing organisations which include; focussing on financial results rather that aquality of care; a disconnect between the Board and the rest of the organisation; a weakculture that discourages staff from raising concerns; and not listening to patients and notusing data to identify risks and make improvements.
The committee considered the paper to be a very useful document but that in respect of

3
one of the themes which implied that it was wrong to focus on financial result rather thanquality of care; the committee was of the view that financial results and providing qualityof care were intrinsically linked.
The committee went on to discuss a paper on a safer NHS and evolving governance andhow the good practice in the document could be linked to the effectiveness of thecommittee as well as the effectiveness of the Board as a whole. Mrs Hanwell raised an apoint about workforce planning and how this is linked into the governance processes inthe organisation. The committee felt this was a very useful document and that it provideda useful framework against which the organisation could benchmark and be challengedon effectiveness. It was agreed that the document would be circulated to all Boardmembers.
The committee recommended that as part of Board development the paper is circulatedto the Board in order to consider these key themes particularly in regard to howeffectively the executives and non-executives collectively spend their time, resources andskills. Mr Griffiths supported this suggestion. It was agreed that a report would bebrought back to the Board and that this might look initially at the time spent by Boardmembers, particularly NEDs, on various aspects.
Mr Butler considered these comments and indicated that he would give some thought asto how the work can be taken forward. Committee members were asked to email theirsuggestions to Mr Butler who will progress the discussion further with the internalauditors as to whether this is put into the audit plan, and Susan Tyler as to whether this isan organisational development study. Mr Bell noted that this could be linked in with theaudit of the governance structure which is already within the audit plan. The committeesupported this suggestion. Mr Bell also agreed to support the work to develop aframework.
CH
CB
CB/ST/NB
The committee received the report and noted the contents.
14/092 Internal Audit Progress Report (agenda item 7.1 )
Mrs Blackburn presented the Internal Audit Progress Report which set out the progress todate in delivering the Internal Audit Annual Plan for 2014/15 noting that there were a fewaudits that were still due to start. Mrs Blackburn noted that the Safer Staffing report hadrecently been finalised and that all recommendations from the report have been agreedwith some already having been implemented. Mrs Blackburn noted that the report will bediscussed in detail at the next committee meeting. The committee noted that this workrelates directly to the report which ultimately comes to Board.
With regard to key performance indicators Mrs Blackburn stated that at the last meetingthe auditors were asked to track the number of recommendations made in the draftreport, the number of recommendations accepted by management and the number ofrecommendations completed on time and that this information was presented on pagetwo of the report.
With regard to the 2014/15 work plan particularly in respect of appraisals noted inAppendix A of the report Mrs Hanwell suggested deferring the audit of appraisals fromthis year’s plan until Dr Hanbury from University of York produced her findings on thebarriers for staff in respect of the up-take of both appraisals and compulsory training. MrsHanwell noted that she had already discussed this possibility and also indicated to thecommittee that the days saved from this audit could be used in other key areas of audit.The committee discussed this suggestion, but asked for more information about the remitand timescale of the remit before agreeing to internal audit not carrying out the work in2014/15. Mrs Hanwell agreed to confirm these details.
DH

4
The committee discussed whether the audit of compulsory training and appraisals shouldbe de-coupled, noting they are currently to be audit together. Mrs Hanwell indicated thatthere is still a lot of work to do on compulsory training and what is applicable to staff andbenchmark to other organisations, which internal audit will support. The committeediscussed training in some detail. The committee supported in principle de-couplingthese, but wanted to understand in more detail on what the emphasis of the audit workwill be and how this would fit with the other work being undertaken. It was agreed thatMrs Hanwell would report back to Mrs Tankard prior to the next meeting in order toprogress this decision.
DH
The committee received and noted the Internal Audit Progress Report.
14/093 Counter-Fraud Protocols Report (agenda item 7.2)
Mrs O’Reilly presented the Counter Fraud Progress Report to the committee which setout the work undertaken since the last Audit Committee meeting and summarised theanti-fraud work that supports the 2014/15 Counter Fraud Work Plan. Mrs O’Reilly statedthat the main focus of the report was on engagement; and highlighted in particular anotice that will be attached to staff’s payslips reminding them to be aware of potentialscams during the Christmas season.
Mrs O’Reilly reported that there had been some work undertaken on the National FraudInitiative noting that this is a sophisticated data matching exercise which matcheselectronic data with and between participating bodies to prevent and detect fraud. MrsO’Reilly stated that the data will be collected by the Finance Team and matches would bereleased in January 2015. Mrs O’Reilly noted that the findings from the matches will bereported to the committee at its next meeting.
Mrs O’Reilly explained the significance of the Fraud and Payroll Protocol, at appendix 2of the report noting that the protocol has been agreed with Leeds Teaching Hospital, ourpayroll service provider, and that the purpose of the protocol was that she would be ableto ascertain staff payroll data and/or witness statements (where applicable) if there was asuspicion of an employee fraud.
The committee received the Counter-Fraud Protocols Report and noted the contents.
14/094 Bribery Act Report (agenda item 7.3)
Mrs O’Reilly presented a report on the Bribery Act; noting in particular section 7 of the Actwhich stipulates that the Trust has a responsibility to take ‘adequate measures’ to preventand deter bribery. The report reviewed the processes and procedures the Trust has inplace to protect itself from bribery such as whether there was a commitment to preventbribery; whether due diligence was undertaken within the Trust and information aboutanti-bribery disseminated throughout the Trust. Mrs O’Reilly said these elements weresignificant defences against section 7 of the Act.
Mrs O’Reilly assured the committee that the Trust’s processes and procedures werealready in place namely the Anti-Fraud and Anti-Bribery Policy; the declarations ofinterest procedures and the Gifts and Hospitality Policy. Mrs O’Reilly made a number ofrecommendations in respect of dealing with suppliers noting in particular arecommendation from the Ministry of Justice that when dealing with suppliers, measuresshould be taken to ensure awareness of all parties involved such as knowing about thedirectors.

5
A discussion ensued with respect to whether the Trust should be looking beyond the leadsupplier within the supply chain especially where the supplier has sub-contractors orsubsidiary suppliers. During the course of the discussion it was noted that there was anincreasing expectation in respect of the NHS prime contract/sub-contractor model whichwill deliver services including clinical services in partnership and that as such the supplychain was potentially becoming more complex. The committee concluded that forthoroughness and assurance it was important to have knowledge about the full supplychain, but recognised the difficulties in achieving this. Mrs O’Reilly noted the suggestionthat a spot check is carried out on some suppliers.
The committee received the Bribery Act Report and noted its content.
14/095 Audit of the completion of care plans / aftercare plans in preparation for First TierTribunals and Mental Health Act Managers’ Hearings (Action log No. 44) (agendaitem 8)
Ms Elizabeth Day introduced a report to the committee on the audit of the completion ofcare plans, noting that concerns had been raised via the committee that there wereissues in connection with timely and robust discharge planning for people who weredetained and sectioned under the Mental Health Act; that there was an absence of careplanning which had resulted in discharge being delayed because the First Tier Tribunalsand Mental Health Act Managers’ Hearings were not being provided with assurance thatafter-care arrangements were adequate.
Ms Day explained the audit. She reported that the results from the audit were that thereappears to be sufficient evidence that planning had been undertaken in preparation fordischarging service users even in those cases where it was clear that discharge wouldnot be an option due to service users being too unwell.
Ms Day reported that it had been noted that the greatest gap had been a lack of localauthority representatives at the hearings and that there had been attempts by staff toinvolve them. Ms Day informed the committee that from the audit it was difficult todetermine how many attempts had been made to involve local authority representativesbut stated that every local authority representative did submit a report for consideration atthe hearings/tribunals and that other reports had also been available at the time whichwere the nursing report and the responsible officer report.
Ms Day advised the committee that the audit was a robust piece of work which looked indetail at the process for discharged planning and asked the committee to be assured ofits findings and also to be reassured that clinical practice in this area was safe andsupports the decision-making process at the time of hearings or tribunals. Ms Dayreported that no re-audit would be carried out in this specific area.
Ms Day also reported that as a result of the audit there were a number ofrecommendations were made in respect some aspects of the audit; particularly thatMental Health Act Managers felt able to report any areas of concern or delay and feedthese into the Mental Health Act Mangers Forum.
The committee raised a concern that only 69% of local authority representativescontributed to service users’ care plans and that there had not been an audit trail of theprocess staff undertook to ensure local authority representatives attendtribunals/hearings. In response to this, Mr Butler agreed to send a copy of the report tocolleagues in Adult Social Care in both Leeds and York.
Further, the committee expressed concern at the recommendation to not re-audit,
CB

6
particularly given the lack of local authority representation. The committee agreed that aclinical audit review of the case notes would be conducted within six months to look atthis matter specifically after which the outcome of the review would be brought back tothe committee.
It was noted that the report will be presented to the Mental Health Act Committee and theMental Health Act Forum.
ED
The committee was assured that there are no concerns with regard to clinical practicerelating to aftercare planning to enable timely discharge, if appropriate, following FirstTier Tribunals or Mental Health Act Managers Hearings, but requested a further report bebrought back to the committee in respect of local authority representation.
14/096 Access to information on SystemOne (Action log No. 29) (enclosure) (agenda item9)
Mrs Hanwell presented a report on accessing information from SystemOne noting thatshe was unable to provide the required assurance to the committee at this time becausethe internal audit is yet to be completed and that the report presented was a statement ofprogress.
The committee received and noted the information on SystemOne but had limitedassurance that appropriate processes are in place but was assured that the issuesemerging due to the changes to the service provision / contract arrangements are beingdealt with. The committee did not accept the report’s recommendations.
14/097 CQC full response action plan – progress update(December 2013 visit) (agenda item10)
Mr Deery presented the report on the CQC full response action plan providing thecommittee with an opportunity to review and comment on the plan. Noting there were twomain items outstanding: improvements to Bootham and record keeping.
With regard to an update on developments at Bootham Park Hospital, Mr Deery reportedthat discussions between the Trust, Commissioners and NHS Property Services Ltd hadprogressed to the stage where the Clinical Commissioning Group will be responsible forthe next stage of the re-provision of the wards. Mr Deery reported that despite someslippage in dates for relocating the wards that the action had progressed to a satisfactorystage.
In addition, Mrs Hanwell commented that she will be attending the Bootham ProgrammeBoard meeting with Mr Deery to discuss the slippage around the contract work andadvised the committee that she was uncertain that work due to start on 17 November atCherry Trees House would start on that date. Mrs Hanwell also assured the Board that inrespect of those things in the control of the Trust the CQC are satisfied with progress.
With regard to the action in respect of record keeping at Bootham Park Hospital, MrDeery reported that Bootham Park Hospital had been subjected to ongoing audits duringthe course of last year and that the CQC was now assured of the arrangements put inplace and suggested that this action could now be closed.
Mr Butler suggested that the action plan felt rather historic in nature given that things hadmoved on significantly. He suggested that any residual actions be consolidated into theresponsive plan from the announced CQC inspection that took place in

7
September/October 2014. The committee agreed with Mr Butler’s suggestion.
The committee received and considered the evidence of progress in the action plan andconfirmed there is sufficient evidence to be assured of progress.
14/098 Duty of Candour Action Plan (agenda item 11)
Mr Deery noted that the action plan before the committee had been devised by hispredecessor. He indicated that this was a detailed action plan on how the Trust wouldmeet the statutory requirements for the Duty of Candour noting that the Trust had alreadybeen bound by a Duty of Candour through the standard contract and that the action planexplained how any additional rigour brought in through the statutory requirements wouldbe met, including any additional training for staff.
Mr Deery reported that the CQC had closed their consultation on the Duty of Candourand that the Trust was waiting for more information on what their requirements will beand that anything additional will be factored into the action plan.
A discussion followed with regard to target dates on the action plan. It was noted inparticular that staff training was due to be completed by end of December 2014. DrTaylor asked if this was an accurate date by which all staff will be trained. Mr Deerynoted that the date referred to there being a plan in place to train all staff throughinduction. Dr Taylor asked what the arrangements were for existing staff, which MrDeery outlined, noting that work was currently being undertaken to address. However,.Mr Deery agreed that there needed to be further clarity around the actions and deadlinesand noted that this would be picked up under his portfolio.
The committee considered how the actions would be monitored and agreed that theycould be brought back to the committee in six months’ time. It was agreed that this wouldbe added to the committee’s work plan.
AD
The committee was assured that necessary steps have been taken to ensure the Trust isconsistently meeting the Duty of Candour, that further work was to be undertaken to firmup all the actions, and that a progress report on the actions would come back to thecommittee.
14/099 Board Assurance Framework (agenda item 12)
Mrs Hill presented the Board Assurance Framework noting that the version was nowcomplete in terms of format and content. Mrs Hill asked that he committee be assured ofthe information contained within it and informed the committee that it is a live documentand will be refreshed from time to time.
Mrs Hill advised the committee that it had been taken to the Mental Health Act Committeeand the Finance and Business Committee and was being used a tool for assurance bythe sub-committees. The committee received the document.
The committee received the current version of the Board Assurance Framework; wasassured of the completeness of the information presented in the Board AssuranceFramework and was assured that this is being used by the Board’s sub-committees as afurther tool to gain / seek assurance on the controls in place to manage the risks tostrategic objectives.

8
14/100 Follow up of outstanding audit actions (agenda item 13)
Mrs Hanwell presented the report on those audit actions that were still outstanding. Thecommittee noted that the responses from management were made on a self-declarationbasis, but that there would be a check as to the accuracy of those declarations during thenext audit of that particular area.
The committee was assured that a robust process now exists to track all auditactions as they become due for implementation.
14/101 Tender and Quotation Exception Report (agenda item 15)
The committee was asked to receive the Tender and Contract Exception Report forSeptember and October 2014 and two supporting Single Tender Waiver reports.
The committee noted the Tender and Quotation Exception Report and supported thewaivers as reported.
14/102 Assurance on the strategic planning cycle (agenda item 14)
Ms Copeland gave a brief presentation with regard to providing assurance on thestrategic planning cycle and drew attention to the two all-day workshops in January andApril to facilitate Board discussion about the Strategic Plan. Mrs Hill confirmed that thesedates are already in Board members’ diaries.
The committee received and noted the attached delivery cycle; confirmed it hadsufficient assurance of the processes and timescales in place for the sign off of the 2015-2016 Operational Plan and 2015 – 2020 Strategic Plan and confirmed it has sufficientassurance of the Trust’s strategic planning processes embedded in the organisation.
14/103 Losses and Special Payments (agenda item 16)
Mrs Hanwell introduced the Losses and Special Payments paper and noted in particularthat salary overpayments are not a loss, but is included for information. With regard toseverance payments Mrs Hanwell drew these to the attention of the committee notingthat these would be disclosed in the annual accounts.
The committee discussed the severance payments. Dr Taylor asked about payments inlieu of notice and Mrs Hanwell explained the basis on which these would be made.
The committee received the report and noted its contents.
14/104 Sponsorship Register (agenda item 17.1)
Mrs Hanwell presented a report which summarised the entries added to the SponsorshipRegister since last reported to the Committee on 4 November 2013. The committeebriefly discussed the basis on which a staff member would want to declare where theyhad declined sponsorship and it was agreed that it was good practice to ensure staffcontinue to do this.

9
The committee received the paper and noted the contents.
14/105 Hospitality Register (agenda item 17.2)
Mrs Hanwell presented a report which summarised entries added to the HospitalityRegister since last reported to the Committee on 4 November 2013.
The committee received the report and noted the contents.
14/106 Management Consultancy Register (agenda item 17.3)
Mrs Hanwell presented a report which summarised entries added to the ManagementConsultancy Register since last reported to the Committee on 4 November 2013. Withregard to Log 2 Mrs Hanwell noted that Mr Rowley had been asked to look at a moreformal arrangement for covering the services required and that he was looking at thepossibility of advertising for a substantive appointment.
The committee received the report and noted the contents.
14/107 Meeting Dates for 2015 (agenda item18)
Mrs Hill asked the committee to note and receive the dates and venues for AuditCommittee meetings in 2015.
The committee noted the meeting dates and venues for 2015.
14/108 Cumulative action log (agenda item 5)
Mrs Hill presented a log of those actions agreed at previous meetings which were eitherstill outstanding or recently completed, noting that the actions had been circulated toexecutive directors for comment and were presented to the committee for assurance onprogress.
Mrs Hill asked the committee to note that Log 45 is now closed, this was agreed by thecommittee; that Log 51 is ongoing and with regard to Log 48 that she noted that she willbe meeting with Mrs O’Reilly to discuss the matter further.
The committee received the cumulative action log and noted the progress with theactions.
14/109 New and Future Risks Identified (agenda item 19)
The committee did not identify any new and future risks.
14/110 Committee effectiveness questionnaire (agenda item 20)

10
The committee received the effectiveness questionnaire and noted that thequestionnaire will be circulated to members ahead of the January meeting and that MrsHill will bring a report back to the committee at that meeting.
14/111 Any other business (agenda item 21)
There were no items of any other business.
The next Audit Committee meeting will be held on 23 January 2015in Meeting Room 1&2 at Trust Headquarters between 1:00 and 4:30 pm.

11
AUDIT COMMITTEE - ACTION SUMMARY
13 November 2014
MINUTE ACTION SUMMARY LEAD
14/089 Matters arising (agenda item 4)
14/098.1 – Update on the Fraud Case - The committee agreed that refreshedlegal advice should be sought as to what the Trust is allowed to disclose. MrsHanwell agreed to contact the Trust’s solicitor.
DH
14/091 Reports from the External Auditors (PricewaterhouseCoopers LLP) – ASafer NHS: the evolving focus on governance in the NHS (agenda item 6.2)
The committee went on to discuss a paper on a safer NHS and evolvinggovernance and how the good practice in the document could be linked to theeffectiveness of the committee as well as the effectiveness of the Board as awhole. Mrs Hanwell raised an a point about workforce planning and how this islinked into the governance processes in the organisation. The committee felt thiswas a very useful document and that it provided a useful framework againstwhich the organisation could benchmark and be challenged on effectiveness. Itwas agreed that the document would be circulated to all Board members.
The committee recommended that as part of Board development the paper iscirculated to the Board in order to consider these key themes particularly inregard to how effectively the executives and non-executives collectively spendtheir time, resources and skills. Mr Griffiths supported this suggestion. It wasagreed that a report would be brought back to the Board and that this might lookinitially at the time spent by Board members, particularly NEDs, on variousaspects.
Mr Butler considered these comments and indicated that he would give somethought as to how the work can be taken forward. Committee members wereasked to email their suggestions to Mr Butler who will progress the discussionfurther with the internal auditors as to whether this is put into the audit plan, andSusan Tyler as to whether this is an organisational development study. Mr Bellnoted that this could be linked in with the audit of the governance structure whichis already within the audit plan. The committee supported this suggestion. MrBell also agreed to support the work to develop a framework.
CH
CB
CB/ST/NB

12
MINUTE ACTION SUMMARY LEAD
14/092 Internal Audit Progress Report (agenda item 7.1 )
With regard to the 2014/15 work plan particularly in respect of appraisals noted inAppendix A of the report Mrs Hanwell suggested deferring the audit of appraisalsfrom this year’s plan until Dr Hanbury from University of York produced herfindings on the barriers for staff in respect of the up-take of both appraisals andcompulsory training. Mrs Hanwell noted that she had already discussed thispossibility and also indicated to the committee that the days saved from this auditcould be used in other key areas of audit. The committee discussed thissuggestion, but asked for more information about the remit and timescale of theremit before agreeing to internal audit not carrying out the work in 2014/15. MrsHanwell agreed to confirm these details.
The committee discussed whether the audit of compulsory training and appraisalsshould be de-coupled, noting they are currently to be audit together. Mrs Hanwellindicated that there is still a lot of work to do on compulsory training and what isapplicable to staff and benchmark to other organisations, which internal audit willsupport. The committee discussed training in some detail. The committeesupported in principle de-coupling these, but wanted to understand in more detailon what the emphasis of the audit work will be and how this would fit with theother work being undertaken. It was agreed that Mrs Hanwell would report backto Mrs Tankard prior to the next meeting in order to progress this decision.
DH
DH
14/095 Audit of the completion of care plans / aftercare plans in preparation forFirst Tier Tribunals and Mental Health Act Managers’ Hearings (Action logNo. 44) (agenda item 8)
The committee raised a concern that only 69% of local authority representativescontributed to service users’ care plans and that there had not been an audit trailof the process staff undertook to ensure local authority representatives attendtribunals/hearings. In response to this, Mr Butler agreed to send a copy of thereport to colleagues in Adult Social Care in both Leeds and York.
Further, the committee expressed concern at the recommendation to not re-audit,particularly given the lack of local authority representation. The committeeagreed that a clinical audit review of the case notes would be conducted withinsix months to look at this matter specifically after which the outcome of the reviewwould be brought back to the committee.
CB
ED
14/098 Duty of Candour Action Plan (agenda item 11)
The committee considered how the actions would be monitored and agreed thatthey could be brought back to the committee in six months’ time. It was agreedthat this would be added to the committee’s work plan.
AD

1
Agenda item 15.1
LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
Minutes of the Finance and Business Committee27 October 2014 at 1.20 pm, Meeting Room 1 & 2, Trust Headquarters
Present: Dr Gill Taylor, Non-Executive Director, Chair of CommitteeMrs Dawn Hanwell, Chief Financial OfficerMr Chris Butler, Chief Executive
In attendance: Ms Lynn Parkinson, Deputy Chief Operating Officer (on behalf of JillCopeland)Mr David Brewin, Assistant Director of FinanceMr Carl Starbuck, Information and Knowledge Manager (minutenumber 14/044 only)Mrs Cath Hill, Head of Corporate GovernanceMs Keisha Allen, Governance Support Assistant (minutes)
Observers: Mrs Jenny Roper (Governor Observer Public: Leeds)Ms Priyanka Kumari (Graduate Trainee)
Action14/041 Welcome and Introduction
Dr Taylor welcomed everyone to the meeting including Ms Kumari, aManagement Trainee who was observing the meeting.
14/042 Apologies for Absence (agenda item 1)
Apologies were received from members of the committee: Ms Jill Copeland,Chief Operating Officer; Mrs Julie Tankard, Non-executive Director; and fromthose who attend the meeting: Mr Mark Powell, Assistant Director of Finance;Mr Keith Rowley, Managing Director of the Commercial ProcurementCollaborative (CPC) and Ms Heather Cook, Head of Information andKnowledge.
14/043 Members and attendees’ declaration of any conflict of interest in anyagenda items (agenda item 2)
No one present at the meeting declared a conflict of interest in any of theitems to be discussed at the meeting.
14/044 Draft Minutes of the Information Governance Committee meeting held 23September 2014 (agenda item 15.1)
Mr Carl Starbuck attended the meeting to present the minutes of theInformation Governance Committee and drew attention in particular to anumber of information governance / confidentiality breaches identified withinthe services in York. Mr Starbuck noted that these services have hadbreaches in the past and indicated that the minutes from the September

2
meeting noted these breaches up to a point time and that since then theincidents that had occurred had started to filter through the system and had infact shown there to be 5 breaches during that period, but noted that within thelast 12 months there had been a total of seven breaches from within theCAMHS service in York.
Mr Starbuck outlined the type of breaches that had taken place includingincidences of letters being posted to the wrong house on a particular streetnoting that these letters related to mental health data including children’smental health data and that breaches in respect of such data place thesebreaches at the highest level, and consequently they reach the threshold forreporting to the Department of Health and the Information Commissioner’sOffice.
Mr Butler noted his concern in respect of these breaches, noting that fivebreaches in a relatively small service was highly unsatisfactory and that hehad contacted the Associate Director for specialist services seekingassurance that this will be addressed as a matter of urgency.
Mr Starbuck informed the committee that in order to address previousbreaches members of the Information Governance Team had assisted staff inthe service in designing their own processes which they had then owned as aprocess. However, Mr Starbuck advised that during an unannounced visit theIG Team had found that staff in the service were not following their ownprocedure and that further breaches had subsequently occurred.
It was noted that as there were a large number of breaches, there was thepotential for a financial penalty to be imposed on the Trust by the InformationCommissioner’s Office, and that as information about breaches is likely to bein the public domain commissioners and service users may be concerned atoccurrences of this nature.
The committee noted that the matter would be reported to the Board by thechair of the committee and that clarification be provided by Mr Starbuck withregard to the precise number of breaches that had occurred within the lastyear.
The committee also asked for there to be an update of the matter to the nextmeeting.
The committee noted that whilst the minutes of the IG Committee meetingsmade reference to concerns about breaches the cover sheet did not draw outthe seriousness of the situation to the committee. It was noted that moreattention needs to be paid by document authors as to what is included onfront sheets. Mrs Hill agreed to remind all document authors.
CS
HC
CH
The committee noted the contents of the draft minutes of the InformationGovernance Committee meeting held 23 September 2014 and expressedconcern at the number of IG breaches in the CAMHS service in York andrequested further information to the next Finance and Business Committeemeeting.

3
14/045 Minutes of Committee Meeting held 17 July 2014 (agenda item 3.1)
The minutes of the meeting held on 17 July 2014 were accepted as a truerecord of the meeting.
14/046 Matters Arising (agenda item 4)
14/046.1 - Estate Strategy Update / Training Services Review (min 14/031) DrTaylor asked for an update relating to the Estates Strategy with particularreference to the training service review. Mrs Hanwell advised the committeethat a specification had been received from the training services as to theestates they would require in order for them to provide physical (rather thanvirtual) training to staff but that in her opinion this was predicated on a trainingmodel being identified, which was still awaited.
Mrs Hanwell outlined the current proposals which were to withdraw from TheExchange as it was not meeting the needs of the training team or staff andthat there was work in hand to look at providing interim accommodation whichwould allow the training team time to undertake a thorough review of needsand to consider a number of possible options. Mrs Hanwell also reported thatthere was a need for more project manager support within the estatesdepartment and that she was looking at this.
Dr Taylor asked about the timetable for developing the training model. MrsHanwell responded that Susan Tyler and Beverly Murphy were responsiblefor developing this but that irrespective of what the training model might looklike, PMVA would always require some level of physical space even if thiswas underutilised. Mrs Hanwell also noted that there had been considerationas to whether the Trust could enter into collaboration with another mentalhealth trust to share physical estate for such training.
The committee agreed to discuss the estate strategy in respect of the trainingservices review at its next meeting in January 2015, but that before the nextmeeting asked for an update to be provided by Susan Tyler with regard to thetimetable for the development of the training model and conclusion of theestates requirement.
14/046.2 – Committee Terms of Reference (min 14/037). With respect to theTerms of Reference, Mrs Hill asked about the committee’s view as to whichstaff should be attending the committee meetings noting it was unclear in theTerms of Reference. Mrs Hanwell outlined those staff within her area of workwho should attend each meeting. Mrs Hill agreed to consider attendees infurther detail with Mrs Hanwell and to advise people accordingly.
ST
CH
4
14/047 Cumulative Action Log (agenda item 4.1)
Mrs Hill presented to the committee the cumulative action log for those itemsthat have been asked to come back to future meetings, and those actions thathave been passed into the management route. Mrs Hill noted that it showedthose items still outstanding and those that have been completed since thelast meeting.
The committee received the cumulative action log and noted the progresswith the actions.
14/048 Financial Performance Quarter 2 (agenda item 5)
Mr Brewin presented the report and noted that this provides a detailedassessment of the financial position as at quarter 2 for 2014/15. Mr Brewinnoted that in terms of a forward look the financial position was robust and theTrust was expected to maintain a Continuity of Services risk rating of aminimum of 3 for the next 12 months.
Mr Brewin drew attention to the income and expenditure position noting a netsurplus of £1.814 m, which was £1.483 m above plan. Mr Brewin explainedfactors contributing to the surplus as set out in the paper and provided a moredetailed explanation of each of these in turn noting in particular that theWomen’s Low Secure service in York had generated an under spend ofaround £0.4m in quarter 2 as a result of estate savings and clinical and non-clinical staff savings, noting that these savings are non-recurrent; and therebeing a contingent reserve of £363k as a result of controlling spend againstreserves.
Mr Brewin explained that there was an overall slippage of 38% onperformance against the Cost Improvement Programme (CIPs) noting that thedelay had been in part the redesign of the acute care pathway and theestablishment of the Crisis Assessment Unit and that this delay had been dueto the Trust awaiting confirmation from commissioners in respect of theongoing revenue support for this service. Mr Brewin noted that confirmationhad now been received and that there is an expectation that this will start todeliver recurrently in the following financial year. Mr Brewin also noted thatanother key element to the slippage related to a scheme to reduce the timefor handover periods and that this is expected to start to deliver savings in thefourth quarter; and also the implementation of the new on-call arrangements,noting that everything is now in place for these to start to deliver savings. Interms of slippage Mr Brewin assured the committee that this had been offsetby some items of non-recurrent income and that it was not having adetrimental effect on the overall financial position.
With regard to the forward look Mr Brewin noted that the Trust expects tomaintain a strong Continuity of Service Risk Rating of 3 in the next 12 monthsand that the financial forecast would have to deteriorate by £25.8m before thecontinuity risk rating is reduced to 2. The committee noted that whilst thefinancial position is extremely robust there are some concerns emergingaround CIP slippage and delays with the capital programme.

5
The committee noted from the report the issues and risks identified andreceived assurance of a strong financial position over the next twelve months.However, the committee further sought assurance that the slippage in CIPswill not deteriorate any further. Mrs Hanwell gave assurance as to themonitoring in place and also noted that the revenue generation schemes candeliver recurrently and that the expected funding from the Leeds CCGs wouldoffset any CIP shortfall. Mrs Parkinson assured the committee about theprogress with the Crisis Assessment Unit, noting that this is being closelymonitored to ensure progress.
The committee accepted the recommendation and thanked Mr Brewin for thereport. Dr Taylor asked if in future the paper could have a percentage againsteach variance. Mr Brewin agreed to do this.
DB
The committee considered the quarter two position for 2014/15, including theissues and risks identified; it was assured that the Trust anticipates achievinga good overall financial risk rating assessment at year end; and noted theassurance received to allow it to support the Board of Director’s requirementto confirm to Monitor that the Trust will continue to maintain a Continuity ofService Risk Rating of at least 3 over the next 12 months.
14/049 Financial Plan Forecast Out-turn (agenda item 6)
Mr Brewin presented the Financial Plan Forecast Out-turn report whichoutlined the preliminary assessment of the forecast out-turn financial plan for2014/15.
With regard to the income and expenditure position, Mr Brewin gave a reporton the Trust’s financial forecast position noting a potential net surplus of£3.9m which was £3.2m above plan. Mr Brewin indicated that the reportexplained the variance from the plan noting that the forecast out-turn is basedon both recurrent and non-recurrent factors and that the planned surplus ismade up of two elements; £1.323m underlying surplus and £623k non-recurrent pressure. Mr Brewin indicated that as a result of these factors, bythe end of the financial year the Trust will have maintained approximately£1.5m underlying surplus.
Mr Brewin added that there were plans to conduct a thorough review ofcapital spend and a review of the use of provisions in particular themanagement of change provision as both these factors have a significantimpact on the forecast. Mr Brewin also noted that there was a timing mis-match with regard to funding from commissioners against expenditure andthat this time difference will be taken into account for the next financial year.The committee accepted the recommendations in the report noting that thematter will be discussed at the next meeting of the committee.
The committee discussed the financial out-turn forecast and noted that whilstthe Trust is expecting to be ahead of plan there is still the potential for ashortfall in respect of projected CIPs.

6
The committee considered the forecast financial position 2014/15, includingthe issues and risks identified; it was assured that the Trust anticipatesachieving a good overall financial risk rating assessment at year end.
14/050 Estates Strategy Update (agenda item 7)
Mrs Hanwell introduced the Estates Strategy Update report. Mrs Hanwellupdated the committee on the Yorkshire Centre for Psychological Medicine(YCPM) noting that on 10 October 2014 the project group had been asked toconsider a proposal in respect of the location for this service.
Mrs Hanwell stated that whilst a solution for location is being considered byYCPM that discussions were still ongoing with Leeds Teaching Hospitals NHSTrust (LTHT) but noted that at some point it may be necessary to considerwhether to relocate the service on Trust premises in the short-term orcontinue to wait for a solution from LTHT.
Dr Taylor asked about the deadline by which the YCPM will assess thefeasibility of an interim solution. Mrs Hanwell reported that the outcome ofthese considerations should be concluded by the end of quarter 4. Mr Butlerstated that with regard to the timetable, there are a number of importantevents to be mindful of including any findings from Care Quality Commissionannounced inspection in September 2014.
Mrs Hanwell assured the committee of good progress in respect of theEstates Strategy and the estates capital expenditure although she notedsome concerns around spend in respect of IT. Mrs Hanwell noted that therehad been a mini-summit to refresh the Estates Strategy and that it would befurther refreshed in January. Mrs Hanwell also assured the committee that allschemes agreed for this financial year are progressing well and that there areno significant risks identified.
Dr Taylor asked about the project management resources cited in the reportand Mrs Hanwell responded that there had been a temporary project managerappointed, noting that Cherry Tree House and Lime Trees would not havemade such good progress without the Trust having appointed a projectmanager. Mrs Hanwell commented that the sustainability of continuing tohave a project manager is questionable in the long-term but there was anacknowledgement that there was still a lot of other work to be done aroundthe York estates for which there needs to be oversight of the work to ensurethis is carried out and remains on track.
With regard to the Leeds estate Mrs Hanwell informed the committee that shewas considering recruiting a permanent resource to support the projectmanagement of these schemes. Following Mrs Hanwell’s response, thecommittee considered that the capacity and project management expertiseshould be registered as a risk on the risk register. Mrs Hanwell agreed toprovide a further update to the committee at its next meeting in January. DH

7
The committee noted the progress made to the Estate Strategy and noted thecontents of the Estates Strategy Update report.
14/051 Informatics strategy update (agenda item 8)
Dr Taylor firstly commented that the content of the paper had been difficult tounderstand and requested more narrative in respect of the projects, theirprogress and any issues. Mrs Hanwell agreed to feed this back.
Mrs Hanwell presented the Informatics Strategy Update to the committeenoting firstly the issues around the PARIS roll-out programme in Yorkindicating that although it was agreed that it would be completed byDecember 2014 that this would now be delayed. The committee noted thatthere was a new proposed roll-out schedule which had been agreed by theCare Group and the Paris Development Team.
Mrs Hanwell outlined some of the issues encountered including the difficultyin putting the IT infrastructure into some of the buildings. The committee wasadvised that the programme was now likely to be completed by end ofFebruary / beginning of March 2015 for mainstream services, with somespecialised services being picked up following this. Dr Taylor asked for thetimescales to be looked at again outside of the meeting and if there was ashift in the proposed dates for this to be advised by email to all members ofthe committee before the next committee meeting.
Mrs Hanwell raised an issue about the handheld devices and there not beinga ‘one-size fits all’ solution and suggested there will need to be a pilot schemeto assess the appropriate technology to use in differing settings andcircumstances.
Mrs Hanwell advised the committee about the Civica contract and the expirydate for the contract. Mrs Hanwell also outlined to the committee thediscussions that had taken place about the delivery of the high level businessrequirements.
HC
DH
The committee noted the current status of the informatics strategic projects.
14/052 Procurement Strategy Update (agenda item 9)
Mrs Hanwell gave an update on the Procurement Strategy and drew attentionto the work-plan and deadlines set out in the report.
Mrs Hanwell reported that a deputy had been appointmed to support theHead of Procurement. Mrs Hanwell noted the rigor around procurement bothin terms of systems and processes as well as the added value that betterprocurement provides. Mrs Hanwell noted that the Procurement Strategy willbe launched at the Senior Leaders’ Forum in November 2014 in order to havehigh level engagement and for senior managers to be sighted on the changesin procurement processes.

8
The committee noted the progress being made in respect of the ProcurementStrategy and requested a further update be made to the committee at its nextmeeting in January.
DH
14/053 Revival Holdings (agenda item 10)
Content commercial in confidence – see confidential appendix.
14/054 Update on the Mental Health Payments System (agenda item 11)
Mr Brewin presented the Mental Health Payments System report whichprovided an update on the Trust’s progress with the implementation of MentalHealth Payments System (formerly PbR). Mr Brewin noted that the reportsummarised the proposed requirements for 2015/16 and outlined the possibledirection for the Mental Health Payments system.
Mr Brewin reported the trajectory for the percentage of services clusteredwithin the review period as agreed with the Leeds Commissioners for thecontract period for 2014/15 was: Quarter 1 – 58%; Quarter 2 – 62%; Quarter3 -68%; Quarter 4 -75%. Mr Brewin outlined some of the actions beingundertaken to complete this work within the required timescales as per thecontract. In York Mr Brewin noted that only 48.9% of York and NorthYorkshire services had an in-date cluster allocation, but that there are not thesame penalties attached to the contract.
A discussion followed regarding the effectiveness of using a cluster-basedmodel for mental health services, and how this might support the objective ofdelivering high quality care and ensuring outcomes are achieved. It wasacknowledged that a clinical outcome framework was not yet available. Thecommittee also noted the need for the Executive Team to ensure thatclustering targets are met. Mr Butler noted the need for there to be anemphasis in respect of ensuring consultants are on board with this and MrButler agreed to pick this up through the Executive Team. CB
The committee considered the progress to date in respect of theimplementation of the mental health payments system and also noted that thenational context and that key drivers for development will become clearer asfurther guidance is issued for 2015/16.
14/055 Board Assurance Framework (BAF) (agenda item 12)
Mrs Hill presented the Board Assurance Framework to the committee noting arefreshed format to the document and that there was an assurance frameworkworkshop which had about thirty senior managers in attendance.
Mrs Hill noted that the document has been streamlined and the key controlsfocussed on high level strategic risks and noted that the BAF adopted thestrategic risks from the Strategic Risk Register. She noted the refresheddocument lists those committees, including the Finance and Business
9
Committee that are responsible for receiving assurance in respect of theeffectiveness of those key controls.
The committee was of the view that the BAF would be a useful document forthe committee with regard to agenda setting and informing its cycle ofbusiness and Mrs Hill commented that the document may be useful ingenerating actions for the committee. The committee was pleased with thedocument and noted the benefit of using this as a live document.
Having reviewed the framework it was agreed that a report would be broughtto the next committee in respect of contract income and the status and risks inrespect of all the contracts.
DH
The committee noted the contents of the report.
14/056 Ratification of the Declaration of Interest Procedure (agenda item 13)
The committee reviewed the procedure for Declarations of Interest andsought assurance about the groups of staff that would be covered by it andwho would need to make a declaration. Mrs Hill noted that the proceduresought to identify those staff who could have influence over the use ofresources.
The committee received and ratified the Declaration of Interest Procedure.
14/057 Approval of the Governors’ Expenses Procedure (agenda item 14)
The committee received the governors’ Reimbursement of ExpensesProcedure for approval ahead of being ratified by the Council of Governors atits November meeting. It was noted that the procedure has been returned tothe committee for approval due to the inclusion, in the main, of the payment ofa passenger rate of 5p per mile for any governor who gives a lift to anothergovernor in the course of their official duties.
The committee received and approved the governors’ reimbursement ofexpenses procedure, noting the amendments made to this iteration
14/058 Forward Meeting Dates and the Cycle of Business for the Committee(agenda item 16)
Mrs Hill presented the dates and the cycle of business for the committee andagreed to circulate the dates of future committee meetings to members of thecommittee. The committee was asked to note its cycle of business and formembers of the committee to provide information about any other regularstanding items to be added, and to confirm that the timing of the reports to thecommittee to ensure it fits in with other business cycles and timetables.
ALL

10
The committee noted the cycle of business and noted that meeting dates willbe circulated to all members and that the meeting date of 23 January 2015has already been scheduled.
14/059 Committee Effectiveness Review (agenda item 17)
The committee considered the Committee Effectiveness Review paper and DrTaylor asked each member of the committee to complete the questionnaireoutside of the meeting and that the information be collated into a report withthe outcome of the questionnaire being brought back to the committee at itsnext meeting.
ALL/CH
The committee noted the contents of the report and requested the outcomeof the questionnaire be brought to the committee at its next meeting.
14/060 Any Other Business (agenda item 18)
There were no items of other business.
The date of the next meeting is 23 January 2015 at 9.30 am in Meeting Rooms 1&2at Trust Headquarters

11
Finance and Business CommitteeAction summary
Meeting held 27 October 2014
MINUTE ACTIONLEAD
PERSON
14/044 Draft Minutes of the Information Governance Committeemeeting held 23 September 2014 (agenda item 15.1)
The committee noted that the matter would be reported to theBoard by the chair of the committee and that clarification beprovided by Mr Starbuck with regard to the precise number ofbreaches that had occurred within the last year.
The committee also asked for there to be an update of the matterto the next meeting.
The committee also noted that whilst the minutes of the committeemade reference to concerns about breaches the cover sheet didnot draw out the seriousness of the situation to the committee. Itwas noted that more attention needs to be paid by documentauthors as to what is included on front sheets. Mrs Hill agreed toremind all document authors.
CS
HC
CH
14/046 Matters Arising (agenda item 4)
14/046.1 - Estate Strategy Update / Training Services Review(min 14/031)The committee agreed to discuss the estate strategyin respect of the training services review at its next meeting inJanuary 2015, but that before the next meeting asked for anupdate to be provided by Susan Tyler with regard to the timetablefor the development of the training model and conclusion of theestates requirement.
14/046.2 – Committee Terms of Reference (min 14/037). Withrespect to the Terms of Reference, Mrs Hill asked about thecommittee’s view as to which staff should be attending thecommittee meetings noting it was unclear in the Terms ofReference. Mrs Hanwell outlined those staff within her area ofwork who should attend each meeting. Mrs Hill agreed toconsider attendees in further detail with Mrs Hanwell and to advisepeople accordingly.
ST
CH
14/048 Financial Performance Quarter 2 (agenda item 5)
The committee accepted the recommendation and thanked MrBrewin for the report. Dr Taylor asked if in future the paper couldhave a percentage against each variance. Mr Brewin agreed to dothis.
DB

12
MINUTE ACTIONLEAD
PERSON
14/050 Estates Strategy Update (agenda item 7)
With regard to the Leeds estate Mrs Hanwell informed thecommittee that she was considering recruiting a permanentresource to support the project management of these schemes.Following Mrs Hanwell’s response, the committee considered thatthe capacity and project management expertise should beregistered as a risk on the risk register. Mrs Hanwell agreed toprovide a further update to the committee at its next meeting inJanuary.
DH
14/051 Informatics strategy update (agenda item 8)
Dr Taylor firstly commented that the content of the paper hadbeen difficult to understand and requested more narrative inrespect of the projects, their progress and any issues. MrsHanwell agreed to feed this back.
Mrs Hanwell outlined some of the issues encountered includingthe difficulty in enter some premises in order to put the ITinfrastructure into the building. The committee was advised thatthe programme was now likely to be completed by end ofFebruary / beginning of March 2015 for mainstream services, withsome specialised services being picked up following this. DrTaylor asked for the timescales to be looked at again outside ofthe meeting and if there was a shift in the proposed dates for thisto be advised by email to all members of the committee before thenext committee meeting.
DH
DH
14/052 Procurement Strategy Update (agenda item 9)
The committee noted the progress being made in respect of theProcurement Strategy and requested a further update be made tothe committee at its next meeting in January.
DH
14/054 Update on the Mental Health Payments System (agenda item11)
A discussion followed regarding the effectiveness of using acluster-based model for mental health services, and how thismight support the objective of delivering high quality care andensuring outcomes are achieved. It was acknowledged that aclinical outcome framework was not yet available. The committeealso noted the need for the Executive Team to ensure thatclustering targets are met. Mr Butler noted the need for there tobe an emphasis in respect of ensuring consultants are on boardwith this and Mr Butler agreed to pick this up through theExecutive Team.
CB

13
MINUTE ACTIONLEAD
PERSON
14/055 Board Assurance Framework (BAF) (agenda item 12)
Having reviewed the framework it was agreed that a report wouldbe brought to the next committee in respect of contract incomeand the status and risks in respect of all the contracts.
DH
14/058 Forward Meeting Dates and the Cycle of Business for theCommittee (agenda item 16)
Mrs Hill presented the dates and the cycle of business for thecommittee and agreed to circulate the dates of future committeemeetings to members of the committee. The committee wasasked to note its cycle of business and for members of thecommittee to provide information about any other regular standingitems to be added, and to confirm that the timing of the reports tothe committee to ensure it fits in with other business cycles andtimetables.
ALL
14/059 Committee Effectiveness Review (agenda item 17)
The committee considered the Committee Effectiveness Reviewpaper and Dr Taylor commented that in her opinion, each memberof the committee should complete the questionnaire outside of themeeting and that the information should be collated into a reportwith the outcome of the questionnaire being brought back to thecommittee at its next meeting.
ALL/CH

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Integrated Quality & Performance Report and Quarter 3 2014/15monitoring returns/self-certification
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Anthony Deery, Interim Director of Nursing& Quality
STRATEGIC:
PAPER AUTHOR: Clare Blackburn, Quality AssuranceSupport Manager
GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)
G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)
SO1 We provide excellent quality, evidence-based, safe care that involves people and promotesrecovery and wellbeing
SO2 We work with partners and local communities to improve health and lives
SO3 We value and develop our workforce and those supporting us SO4 We provide efficient and sustainable services SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individuals
Matters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
16

SUMMARY:
The integrated quality and performance report is provided as a regular agenda item to the board ofdirectors.
The report details performance against national, regulatory, contractual and local improvementtargets. The January 2015 report is based on December 2014 data and also reflects Quarter 3performance. As this is a quarter end report, it also includes reports from; Workforce, MedicalRevalidation, Mental Health Act information and performance against the Mental Health PaymentScheme (PbR).
The report details performance broadly in keeping with anticipated trends with performance againstthe majority of measures indicating consistently high quality services.
Exception reporting is detailed on page 2.
All NHS Foundation Trusts are required to provide in-year reports for Monitor on a quarterly basis,this paper relates to Quarter 3 2014/15.
In Quarter 3 the Trust’s financial position is robust, with a Continuity of Service Risk Rating of ‘4’.The Trust was inspected between 29 September and 5 October 2014 as part of the Care QualityCommission’s comprehensive inspection programme. The inspection team looked at the Trust as awhole and in more detail at 11 core services including inpatient mental health wards andcommunity-based mental health, crisis response and learning disability services. The Trust hasbeen given five “compliance actions” by the Care Quality Commission across the organisation whichmeans these are areas that require immediate attention to address essential standards of qualityand safety. The Trust has already taken action to address some of these concerns.
For 2014/2015 the Board of Directors are also asked to confirm there are no matters requiring anexception report which have not already been reported to Monitor.
RECOMMENDATIONS:
The Trust Board of Directors is asked to:
Consider the position against both non-financial and financial targets and to comment on thedegree to which it feels assured regarding both current performance and future trajectories.
Confirm that the board anticipates maintaining a continuity of service risk rating of at least 3over the next 12 months, as required by Monitor, and sign the attached declaration.
Confirm that the board is satisfied that plans in place are sufficient to ensure on-goingcompliance with all existing targets (after the application of thresholds) as set out inAppendix B of the Compliance Framework and, a commitment to comply with all knowntargets going forwards and sign the attached declaration.
Confirm that there are no matters arising in the quarter requiring an exception report toMonitor (per Compliance Framework) which have not already been reported and sign theattached declaration.

INTEGRATED QUALITY & PERFORMANCE REPORT – JANUARY 2015 (December 2014 & Quarter 3 Data)Contents
Exception Reporting
Strategic Goal 1 – People achieve their agreed goals for improving health and improving lives
Strategic Goal 2 – People experience safe care
Strategic Goal 3 – People have a positive experience of their care and support
Service User & Carer Feedback
Financial Summary
Appendix A Sickness Absence and Staff Turnover
Appendix 1 Continuity of Service Risk RatingAppendix 2 Statement of Comprehensive IncomeAppendix 3 Cost Improvement Plans & Revenue Generations Scheme 2014/15Appendix 4 Statement of Financial PositionAppendix 5 Cash Flow AnalysisAppendix 6 Capital Programme
This report shows the Trust’s current compliance with national and local performance requirements which are aligned to the Trust’s three StrategicGoals. Each performance requirement has been RAG rated to demonstrate compliance.
compliant partially compliant non-compliant

Exception Reporting
Adherence to Cluster Review/Mental Health Payment System – Leeds Contract Measure (Quarter 3 target 68%). For Quarter 3, performance was 66.4%against a target of 68%. The criteria for calculating the service users who should be clustered has been aligned to the Mental Health & Learning Disabilitiesdata set which resulted in an increase in this number of service users. Leeds service have 66.4% of in date clusters and continue to move in an upwardstrajectory. Although the Quarter 3 target was not met, actions are in place to ensure increase in clustering continues to be implemented.
York services have 40.4% of in date clusters. There are data quality issues with the CPD information system and York services are currently undergoingmigration to the PARIS information system which will impact on the cluster data
Increasing awareness of Autism in registered mental health nurses – Leeds Contract Measure (Quarter 3 target 39%). Although the Trust is below the targetof 39% with performance at 31.5%, training figures have improved since September 2014 (16.6%). Improvements with compliance are being activelymanaged within the care group.
Healthcare Associated Infections, C.difficile – National Target (0). During December 2014, the Trust reported one incident of C.difficile within LeedsServices. One service user on the Yorkshire Centre for Psychological Medicine ward was tested toxin positive. The service user was at home at the time ofthe result, treatment was sent out and the course completed whilst the service user was at home. Post treatment tests indicate the service user is nowC.difficile negative.
Improving the implementation action goals following a serious untoward incident which relates to a suspected suicide – Leeds Contract Measure (90%). InDecember 2014, the Trust’s performance was 66.7% against the target of 90%. Although the Trust were made aware on the same day as the incidentoccurred, the Risk Management department were not informed until the day after (Friday). Therefore, the incident was not reported externally until fourworking days after the incident occurred (Monday).
Trigger to Board – Local Measure. During December 2014, there were three Trigger to Board events. One related to an incident of unlawful detention. Theother two incidents related to inpatient suspected suicides (one Leeds Services and one York Services). In all case, immediate actions has been taken andfull investigations have been completed.
Appraisals – Local Measure (90%). Appraisal performance is continually moving towards the new 2014/15 target of 90% by March 2015.
Compulsory Training – Local Measure (90%). Although the Trust has not achieved the target of 90%, currently 80.1%, there has been a steady increase inperformance from September 2014 (77.6%).
Waiting Times Access to Memory Services – Leeds Contract Measure (70%). During Quarter 3, the Trust’s performance was 44.1% against the target of70%. Within the Quarter, there have been a few referrals where it has not been possible to offer an appointment within six weeks due to the service userbeing unavailable or the referral being incomplete.
Complaints – Local Measure. During January 2015, a pilot phase of a new Complaints Management process within the Leeds Care Group will commence.Following evaluation of the pilot, new improved processes will be rolled out across other Care Groups during Quarter 2014/15 and reflected in a revisedprocedural document.

AT A GLANCE PERFORMANCE SUMMARY
Page No Actual Target
Strategic Goal 1
6 Delayed Transfers of Care (Monitor) 1.4% <7.5%
6 Crisis Resolution Service Gatekeeping (Monitor) 97.5% >=95.0%
7 Care Programme Approach Reviews within 12 months (Monitor) 95.4% >=95.0%
7 Data Completeness – Identifiers (Monitor) 99.4% >=97.0%
8 Bed Occupancy rates for Leeds Inpatient Services (Leeds Contract) 90.5% < 98.0%
8 Bed Occupancy rates for York Acute Inpatient Services (Local) 95.4% <98.0%
9 Inpatient Length of Stay – Adult Mental Health Inpatient Units Adult Wards (Leeds Contract) 42.96 N/A
9Inpatient Length of Staff – Adult Mental Health Inpatient Units Older People’s Wards (Leeds
Contract)73.58 N/A
10Incidence of Inpatient Length of Stay – Adult Mental Health Inpatient Units - <3 days or >90
(Leeds Contract)17 N/A
10 Inpatient Length of Stay – Adult Acute Mental Health Wards (Local - York) 35.42 N/A
11Readmissions to Adult and Older People’s Mental Health Inpatient Units – Cumulative (Leeds
Contract)12 N/A
11Readmissions to Adult and Older Peoples Mental Health Inpatient Units – Median days (Leeds
Contract)14 N/A
12 Emergency readmissions within 28 days – Adult Acute Mental Health Wards (Local) 4.7% N/A
12 Adherence to Cluster review periods (Leeds Contract) 66.4% >= 68.0%
13 Learning Disability Services Inpatient Admissions and Length of Stay (Leeds Contract) 4 N/A
13 Referral and Receipt of a Diagnosis with LADs Service (Leeds Contract) 53 N/A
14 Percentage of people in settled accommodation (Leeds Contract) 73.8% >= 0.0%

Page No Actual Target
16 Mental Health Payment System (Leeds Contract) 66.4% >68.0%
Strategic Goal 2
17 Dual Diagnosis Training (Leeds Contract) 72.9% >= 39.0%
17 Increasing awareness of Autism in registered mental health nurses (Leeds Contract) 31.5% >= 39.0%
18 7 Day Follow Up (Monitor) 95.9% >=95.0%
18 Healthcare Associated Infections (Leeds & York) – C.difficile 1 = 0
19 Healthcare Associated Infections (Leeds & York) – MRSA 0 = 0
19Percentage of people with a Crisis Assessment Summary and formulation plan in place within 24
hours (Leeds Contract)100% >=95.0%
20Improving the implementation of action goals following a serious untoward incident which relates
to a suspected suicide (Leeds Contract)66.7% >=90.0%
21 Never Events (National) 0 = 0
21 Trigger to Board (Local) 3 = 0
22 NHS Safety Thermometer (Leeds & York) Harm Free Care 97.2% >=95.0%
22 Appraisals (Leeds & York) 70.9% >=90.0%
23 Compulsory Training (Local) 80.1% >= 90.0%
25 Incidents of Unlawful Detentions 1 = 0
25 Controlled Drugs Quarter 3 Report
27Information Governance Incident Reports & Information Governance Incidents Requiring
Investigations
27 Medical Revalidation
Strategic Goal 3 28 Data Completeness Indicator for Mental Health Outcomes for CPA Patients (Monitor) 72.9% >=50.0%

Page No Actual Target
28 Access to Healthcare for People with a Learning Disability (Monitor) N/A
29Waiting times for Community Mental Health Teams for face to face contact within 14 days
(Leeds Contract)80.7% >= 80.0%
29 Meeting commitment to serve new psychosis cases by Early Intervention Teams (Monitor) 46 >= 25.5
30 Total number Out of Area placements by bed days (Leeds & York) 331 N/A
30 Waiting times access to Memory Services (Leeds Contract) 44.1% >= 70.0%
31 Timely Communication with GPs notified in 10 days (Leeds Contract) 41.6% >= 80.0%
32 CAMHS to Adult Mental Health Services Transition (Leeds Contract) 0% N/A
33 Number of complaints responded to that met the response target of 30 days 50% 100%
Appendix A38 Staff Turnover 13.5% <= 15.0%
38 Sickness Absence 5.0% <= 4.2%

Strategic Goal 1 : People achieve their agreed goal for improving health and improving livesDelayed Transfers of Care (Monitor)
Target < 7.5%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 3.0% 2.9% 3.5% 2.4% 2.5% 2.4% 2.2% 1.6% 1.5% 1.2% 1.1% 1.4%
Leeds 1.2% 1.3% 1.4% 1.8% 1.7% 1.7% 1.8% 1.8% 1.7% 1.5% 1.4% 2.0%
York & N.Yorkshire
6.5% 6.9% 8.0% 3.6% 4.4% 3.7% 2.9% 1.3% 1.0% 0.7% 0.5% 0.2%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 3.5% 2.4% 1.5% 1.4%
Leeds 1.4% 1.7% 1.7% 2.0%
York & N.Yorkshire
8.0% 3.7% 1.0% 0.2% 0.0%
2.0%
4.0%
6.0%
8.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...York &...Target
Crisis Resolution Service Gatekeeping (Monitor)
Target >= 95.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 96.9% 100.0% 98.0% 100.0% 100.0% 100.0% 97.8% 100.0% 100.0% 100.0% 100.0% 97.5%
Leeds 97.5% 100.0% 97.6% 100.0% 100.0% 100.0% 97.4% 100.0% 100.0% 100.0% 100.0% 97.1%
York & N.Yorkshire
94.1% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 98.3% 100.0% 99.1% 99.1%
Leeds 98.3% 100.0% 99.0% 99.0%
York & N.Yorkshire
98.0% 100.0% 100.0% 100.0% 94.0%
95.0%
96.0%
97.0%
98.0%
99.0%
100.0%
101.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...York &...Target

Strategic Goal 1 : People achieve their agreed goal for improving health and improving livesCare Programme Approach Reviews within 12 months (Monitor)
Target >= 95.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 95.8% 95.4% 96.0% 95.6% 95.3% 96.1% 96.7% 95.1% 95.7% 94.9% 96.0% 95.4%
Leeds 95.8% 95.3% 96.4% 95.6% 95.2% 96.5% 96.5% 94.9% 95.8% 94.7% 96.3% 95.4%
York & N.Yorkshire
95.7% 95.7% 94.9% 95.4% 95.6% 95.1% 97.1% 95.7% 95.5% 95.3% 95.0% 95.4%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 96.0% 96.1% 95.7% 95.4%
Leeds 96.4% 96.5% 95.8% 95.4%
York & N.Yorkshire
94.9% 95.1% 95.5% 95.4% 94.5%
95.0%
95.5%
96.0%
96.5%
97.0%
97.5%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...York &...Target
Data Completeness – Identifiers (Monitor)
Target >= 97.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 99.5% 99.8% 98.9% 99.6% 99.6% 99.6% 99.6% 99.6% 99.4% 99.4% 99.5% 99.4%
Leeds 99.3% 99.8% 98.5% 99.6% 99.5% 99.5% 99.5% 99.5% 99.2% 99.3% 99.4% 99.3%
York & N.Yorkshire
99.9% 99.9% 99.9% 99.9% 99.9% 99.9% 99.9% 99.9% 99.9% 99.7% 99.7% 99.4%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 98.9% 99.6% 99.4% 99.4%
Leeds 98.5% 99.5% 99.2% 99.3%
York & N.Yorkshire
99.9% 99.9% 99.9% 99.4% 97.0%
97.5%
98.0%
98.5%
99.0%
99.5%
100.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...York &...Target

Strategic Goal 1 : People achieve their agreed goal for improving health and improving livesBed occupancy rates for Leeds inpatient services (Leeds Contract)
Target < 98.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 96.1% 95.8% 95.5% 93.6% 95.2% 97.2% 98.3% 95.0% 92.8% 93.3% 95.1% 90.5%
Leeds 96.1% 95.8% 95.5% 93.6% 95.2% 97.2% 98.3% 95.0% 92.8% 93.3% 95.1% 90.5%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 95.8% 95.3% 95.4% 92.9%
Leeds 95.8% 95.3% 95.4% 92.9%
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...Target
Bed occupancy rates for York acute inpatient services (Local)
Target < 98.0%
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 93.0% 97.1% 97.0% 97.6% 97.8% 96.3% 98.6% 97.4% 95.4%
York & N.Yorkshire
93.0% 97.1% 97.0% 97.6% 97.8% 96.3% 98.6% 97.4% 95.4%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 95.7% 97.2% 97.1%
York & N.Yorkshire
95.7% 97.2% 97.1%
93.0%
94.0%
95.0%
96.0%
97.0%
98.0%
99.0%
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...York &...Target

Strategic Goal 1 : People achieve their agreed goal for improving health and improving livesInpatient Length of Stay – Adult Mental Health Inpatient Units Adult Wards (Leeds Contract)
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 34.05 29.33 40.16 40.04 35.33 37.04 31.26 41.71 42.96
Leeds 34.05 29.33 40.16 40.04 35.33 37.04 31.26 41.71 42.96
0.0
10.0
20.0
30.0
40.0
50.0
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...Target
Inpatient Length of Stay – Adult Mental Health Inpatient Units Older People's Wards (Leeds Contract)
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 82.44 72.9 101.31 82.97 61.7 113.83 89.5 78.35 73.58
Leeds 82.44 72.9 101.31 82.97 61.7 113.83 89.5 78.35 73.58
0.0
20.0
40.0
60.0
80.0
100.0
120.0
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...Target

Strategic Goal 1 : People achieve their agreed goal for improving health and improving livesInpatient Length of Stay – Adult Mental Health Inpatient Units - <3 days or >90 (Leeds Contract)
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 12 17 19 20 17 21 18 16 17
Leeds 12 17 19 20 17 21 18 16 17
0.0
5.0
10.0
15.0
20.0
25.0
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...Target
Inpatient Length of Stay – Adult Acute Mental Health Wards (Local - York)
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 20.96 26.46 22.9 39.52 25.56 23.94 26.94 30.48 35.42
York & N.Yorkshire
20.96 26.46 22.9 39.52 25.56 23.94 26.94 30.48 35.42
0.0
10.0
20.0
30.0
40.0
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...York &...Target

Strategic Goal 1 : People achieve their agreed goal for improving health and improving livesReadmissions to Adult and Older peoples Mental Health In Patient Units - Cumulative (Leeds Contract)
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 10 13 12
Leeds 10 13 12
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 10 13 12
Leeds 10 13 12
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target
Readmissions to Adult and Older peoples Mental Health In Patient Units - Median days (Leeds Contract)
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 12.5 9.5 14
Leeds 12.5 9.5 14
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 12.5 9.5 14
Leeds 12.5 9.5 14
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target

Strategic Goal 1 : People achieve their agreed goal for improving health and improving livesEmergency Readmissions within 28 Days - Adult Acute Mental Health Wards (Local)
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 5.7% 7.7% 3.8% 6.6% 5.4% 4.9% 9.9% 2.7% 4.7%
Leeds 5.1% 6.2% 5.1% 7.7% 5.0% 6.6% 10.4% 2.4% 6.1%
York & N.Yorkshire
8.3% 14.3% 0.0% 3.1% 6.7% 0.0% 8.6% 3.7% 0.0%
2014/2015 Q1 2014/2015 Q2
LYPFT 5.8% 12.0%
Leeds 5.5% 6.5%
York & N.Yorkshire
6.8% 3.0% 0.0%
5.0%
10.0%
15.0%
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...York &...Target
Adherence to cluster review periods (Leeds Contract)
Target >= 68.0%
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 64.9% 65.7% 66.4%
Leeds 64.9% 65.7% 66.4%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 64.9% 65.7% 66.4%
Leeds 64.9% 65.7% 66.4%
58.0%
60.0%
62.0%
64.0%
66.0%
68.0%
70.0%
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target

Strategic Goal 1 : People achieve their agreed goal for improving health and improving livesLearning Disability Services Inpatient Admissions and Length of Stay (Leeds Contract)
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 5 4 4
Leeds 5 4 4
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 5 4 4
Leeds 5 4 4
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target
Referral and Receipt of a Diagnosis within LADs Service (Leeds Contract)
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 52 48 53
Leeds 52 48 53
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 52 48 53
Leeds 52 48 53
0.0
10.0
20.0
30.0
40.0
50.0
60.0
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target

Strategic Goal 1 : People achieve their agreed goal for improving health and improving livesPercentage of people in settled accommodation (Leeds Contract)
Target >= 0.0%
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 74.4% 76.9% 73.8%
Leeds 74.4% 76.9% 73.8%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 74.4% 76.9% 73.8%
Leeds 74.4% 76.9% 73.8%
0.0%
20.0%
40.0%
60.0%
80.0%
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target

Additional Data: Strategic Goal 1Learning Disability Services Inpatient Admissions and Length of Stay (Leeds Contract)
Actual Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
Learning Disability Services Inpatient Length of Stay (< 4 weeks)
3 1 2
Learning Disability Services Inpatient Length of Stay (5 - 8 weeks)
1 2 0
Learning Disability Services Inpatient Length of Stay (9 - 12 weeks)
0 0 1
Learning Disability Services Inpatient Length of Stay (12 weeks+)
1 1 1
Percentage of people in employment (Leeds Contract)Actual Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
People in employment - Employed 77 64 68
People in employment - Retired 25 23 27
People in employment - Education 14 9 8
People in employment - Volunteer 2 2 0
People in employment - Other 646 649 670
People in employment - referred to the employment service
113 137
Referral and Receipt of a Diagnosis within LADs Service (Leeds Contract)Actual Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
Time from Referral to Receipt of a Diagnosis within LADs Service (% 20 - 26 weeks)
7.7% 16.7% 22.6%
Time from Referral to Receipt of a Diagnosis within LADs Service (% 26 - 32 weeks)
9.6% 22.9% 13.2%
Time from Referral to Receipt of a Diagnosis within LADs Service (% 32 - 38 weeks)
15.4% 16.7% 11.3%
Time from Referral to Receipt of a Diagnosis within LADs Service (% 38+ weeks)
67.3% 33.3% 45.3%
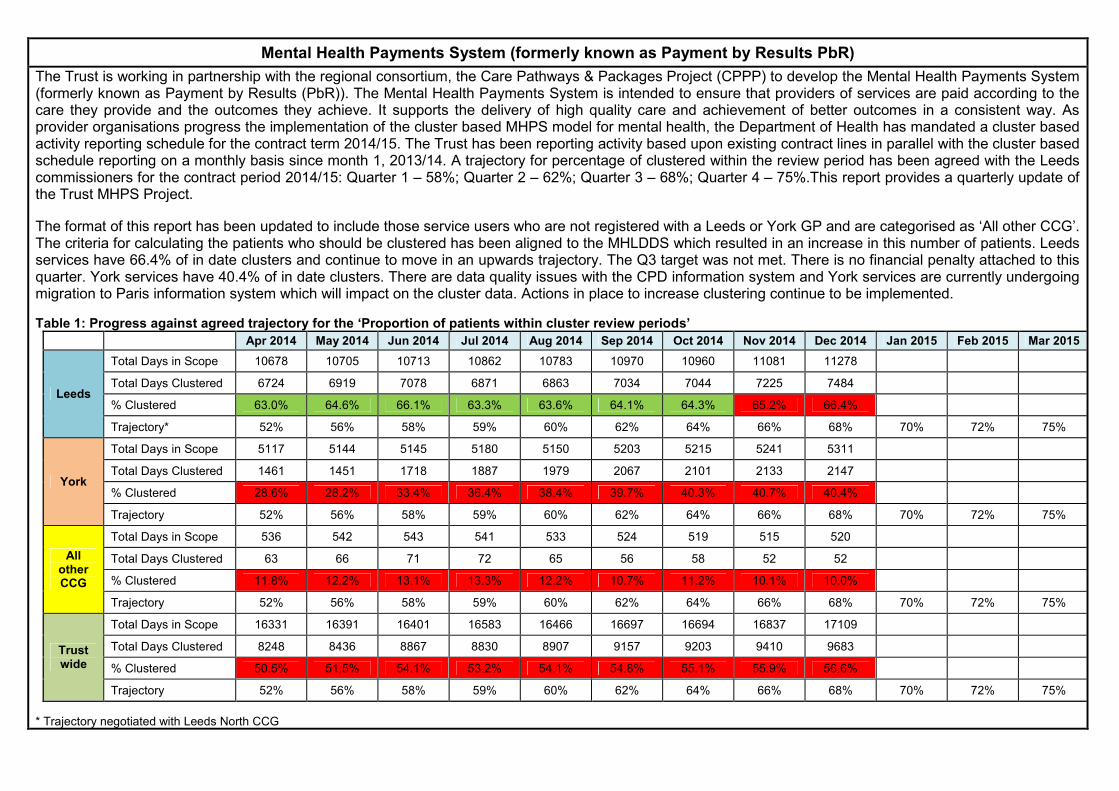
Mental Health Payments System (formerly known as Payment by Results PbR)
The Trust is working in partnership with the regional consortium, the Care Pathways & Packages Project (CPPP) to develop the Mental Health Payments System(formerly known as Payment by Results (PbR)). The Mental Health Payments System is intended to ensure that providers of services are paid according to thecare they provide and the outcomes they achieve. It supports the delivery of high quality care and achievement of better outcomes in a consistent way. Asprovider organisations progress the implementation of the cluster based MHPS model for mental health, the Department of Health has mandated a cluster basedactivity reporting schedule for the contract term 2014/15. The Trust has been reporting activity based upon existing contract lines in parallel with the cluster basedschedule reporting on a monthly basis since month 1, 2013/14. A trajectory for percentage of clustered within the review period has been agreed with the Leedscommissioners for the contract period 2014/15: Quarter 1 – 58%; Quarter 2 – 62%; Quarter 3 – 68%; Quarter 4 – 75%.This report provides a quarterly update ofthe Trust MHPS Project.
The format of this report has been updated to include those service users who are not registered with a Leeds or York GP and are categorised as ‘All other CCG’.The criteria for calculating the patients who should be clustered has been aligned to the MHLDDS which resulted in an increase in this number of patients. Leedsservices have 66.4% of in date clusters and continue to move in an upwards trajectory. The Q3 target was not met. There is no financial penalty attached to thisquarter. York services have 40.4% of in date clusters. There are data quality issues with the CPD information system and York services are currently undergoingmigration to Paris information system which will impact on the cluster data. Actions in place to increase clustering continue to be implemented.
Table 1: Progress against agreed trajectory for the ‘Proportion of patients within cluster review periods’
Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep 2014 Oct 2014 Nov 2014 Dec 2014 Jan 2015 Feb 2015 Mar 2015
Leeds
Total Days in Scope 10678 10705 10713 10862 10783 10970 10960 11081 11278
Total Days Clustered 6724 6919 7078 6871 6863 7034 7044 7225 7484
% Clustered 63.0% 64.6% 66.1% 63.3% 63.6% 64.1% 64.3% 65.2% 66.4%
Trajectory* 52% 56% 58% 59% 60% 62% 64% 66% 68% 70% 72% 75%
York
Total Days in Scope 5117 5144 5145 5180 5150 5203 5215 5241 5311
Total Days Clustered 1461 1451 1718 1887 1979 2067 2101 2133 2147
% Clustered 28.6% 28.2% 33.4% 36.4% 38.4% 39.7% 40.3% 40.7% 40.4%
Trajectory 52% 56% 58% 59% 60% 62% 64% 66% 68% 70% 72% 75%
AllotherCCG
Total Days in Scope 536 542 543 541 533 524 519 515 520
Total Days Clustered 63 66 71 72 65 56 58 52 52
% Clustered 11.8% 12.2% 13.1% 13.3% 12.2% 10.7% 11.2% 10.1% 10.0%
Trajectory 52% 56% 58% 59% 60% 62% 64% 66% 68% 70% 72% 75%
Trustwide
Total Days in Scope 16331 16391 16401 16583 16466 16697 16694 16837 17109
Total Days Clustered 8248 8436 8867 8830 8907 9157 9203 9410 9683
% Clustered 50.5% 51.5% 54.1% 53.2% 54.1% 54.8% 55.1% 55.9% 56.6%
Trajectory 52% 56% 58% 59% 60% 62% 64% 66% 68% 70% 72% 75%
* Trajectory negotiated with Leeds North CCG

Strategic Goal 2 : People experience safe careDual Diagnosis Training (Leeds Contract)
Target >= 39.0%
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 0.0% 46.9% 72.9%
Leeds 0.0% 46.9% 72.9%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 0.0% 46.9% 72.9%
Leeds 0.0% 46.9% 72.9%
0.0%
20.0%
40.0%
60.0%
80.0%
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target
Increasing awareness of Autism in registered mental health nurses (Leeds Contract)
Target >= 39.0%
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 0.2% 16.6% 31.5%
Leeds 0.2% 16.6% 31.5%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 0.2% 16.6% 31.5%
Leeds 0.2% 16.6% 31.5%
0.0%
10.0%
20.0%
30.0%
40.0%
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target

Strategic Goal 2 : People experience safe care7 Day Follow Up (Monitor)
Target >= 95.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 95.4% 95.2% 95.7% 95.6% 96.0% 96.6% 96.2% 97.2% 95.5% 93.8% 96.0% 95.9%
Leeds 94.6% 93.8% 94.7% 94.4% 96.5% 95.6% 97.7% 97.6% 97.1% 96.4% 96.0% 95.6%
York & N.Yorkshire
100.0% 100.0% 100.0% 95.5% 94.7% 96.0% 87.5% 95.5% 89.3% 86.2% 96.0% 96.9%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 95.4% 96.0% 96.2% 95.2%
Leeds 94.4% 95.5% 97.4% 96.0%
York & N.Yorkshire
100.0% 95.5% 90.5% 93.0% 85.0%
90.0%
95.0%
100.0%
105.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...York &...Target
Healthcare Associated Infections (Leeds & York) – C.difficile
Target = 0
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 0 0 1 0 0 0 1 1 0 0 0 1
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 1 0 1 1
0.0
1.0
2.0
3.0
4.0
5.0
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Target

Strategic Goal 2 : People experience safe careHealthcare Associated Infections (Leeds & York) – MRSA
Target = 0
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 0 0 0 0 0 0 0 0 0 0 0 0
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 0 0 0 0
0.0
1.0
2.0
3.0
4.0
5.0
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Target
Percentage of people with a Crisis Assessment Summary and formulation plan in place within 24 hours (Leeds Contract)
Target >= 95.0%
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 100.0% 99.1% 100.0% 100.0% 100.0% 100.0% 98.2% 98.0% 100.0% 100.0%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 100.0% 99.6% 99.5% 99.3%
94.0%
95.0%
96.0%
97.0%
98.0%
99.0%
100.0%
101.0%
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Target

Strategic Goal 2 : People experience safe careImproving the implementation of action goals following a serious untoward incident which relates to a
suspected suicide (Contract)
Target >= 90.0%
Apr 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 100.0% 0.0% 100.0% 100.0% 0.0% 0.0% 100.0% 66.7%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 100.0% 100.0% 88.9%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
Apr 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Target

Strategic Goal 2 : People experience safe careNever Events (National - Leeds & York)
Target = 0
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 0 0 0 0 0 0 0 0 0 0 0 0
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 0 0 0 0
0.0
1.0
2.0
3.0
4.0
5.0
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Target
Trigger to Board Events (Local - Leeds & York)
Target = 0
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 0 0 1 0 1 1 1 1 2 1 0 3
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 1 2 4 4
0.0
1.0
2.0
3.0
4.0
5.0
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Target
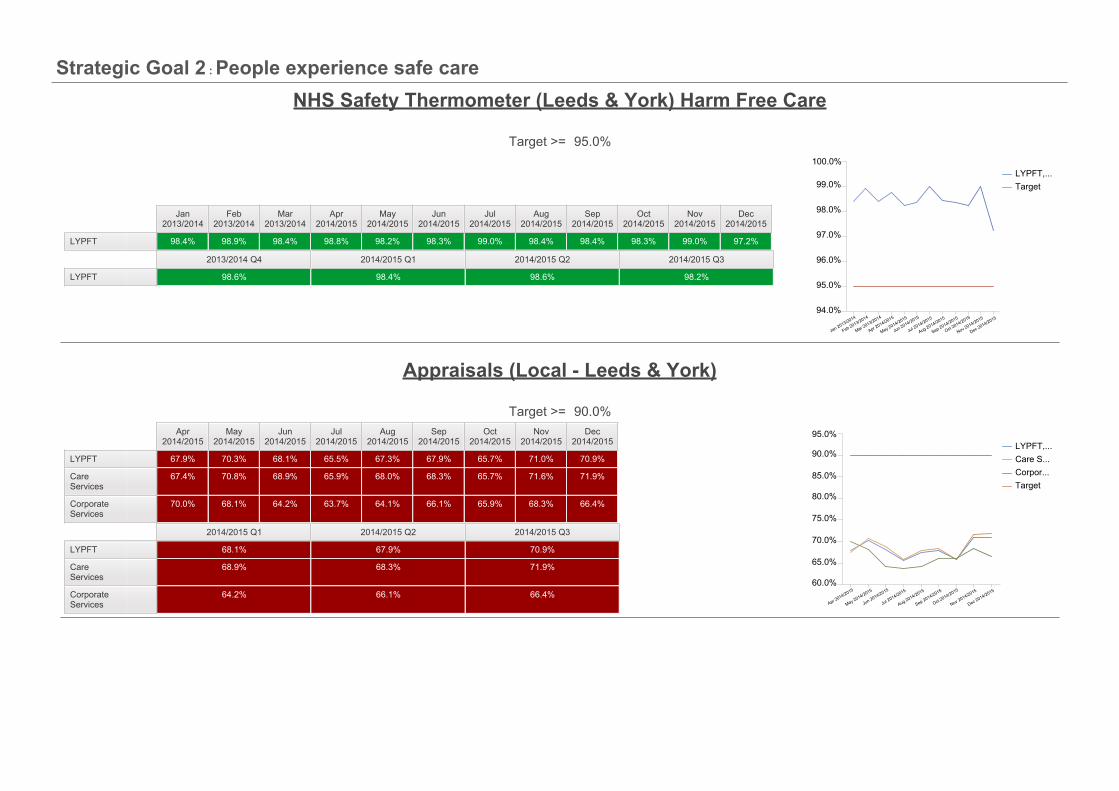
Strategic Goal 2 : People experience safe careNHS Safety Thermometer (Leeds & York) Harm Free Care
Target >= 95.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 98.4% 98.9% 98.4% 98.8% 98.2% 98.3% 99.0% 98.4% 98.4% 98.3% 99.0% 97.2%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 98.6% 98.4% 98.6% 98.2%
94.0%
95.0%
96.0%
97.0%
98.0%
99.0%
100.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Target
Appraisals (Local - Leeds & York)
Target >= 90.0%Apr
2014/2015May
2014/2015Jun
2014/2015Jul
2014/2015Aug
2014/2015Sep
2014/2015Oct
2014/2015Nov
2014/2015Dec
2014/2015
LYPFT 67.9% 70.3% 68.1% 65.5% 67.3% 67.9% 65.7% 71.0% 70.9%
Care Services
67.4% 70.8% 68.9% 65.9% 68.0% 68.3% 65.7% 71.6% 71.9%
Corporate Services
70.0% 68.1% 64.2% 63.7% 64.1% 66.1% 65.9% 68.3% 66.4%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 68.1% 67.9% 70.9%
Care Services
68.9% 68.3% 71.9%
Corporate Services
64.2% 66.1% 66.4%60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Care S...Corpor...Target

Strategic Goal 2 : People experience safe careCompulsory Training (Local)
Target >= 90.0%Jun
2014/2015Sep
2014/2015Dec
2014/2015
LYPFT 78.0% 77.6% 80.1%
Care Services
74.9% 78.0% 80.3%
Corporate Services
79.7% 75.0% 79.0%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 78.0% 77.6% 80.1%
Care Services
74.9% 78.0% 80.3%
Corporate Services
79.7% 75.0% 79.0% 70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Care S...Corpor...Target

Additional Data: Strategic Goal 2Memory Services - Time from Referral to Diagnosis (Leeds Contract)
Actual Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
Memory Services – Time from Referral to Diagnosis (0 - 6 weeks)
2 3 3
Memory Services – Time from Referral to Diagnosis (6 - 12 weeks)
5 5 8
Memory Services – Time from Referral to Diagnosis (12 - 18 weeks)
18 19 51
Memory Services – Time from Referral to Diagnosis (18 - 24 weeks)
41 37 34
Memory Services – Time from Referral to Diagnosis (24+ weeks)
42 29 39

Incidents of Unlawful Detentions – December 2014
Date of Incident Description of Fault Action Taken18/12/2014 It became apparent on this date that the Section 37 for a
service user on Westerdale (Clifton) had not been renewed bythe date of expiry (17/11/14). The renewal date had beenmissed by the Mental Health Act office in York and by theward.
The service user was informed by the ResponsibleClinician of the error and in writing also by the MentalHealth Legislation Lead.
The service user was re-assessed but as they wereapproaching discharged, was not deemed to meet thecriteria and remained as an informal service user.
Administrative processes are being reviewed in the YorkMental Health Act office. The ward is considering howbest to ensure expiry dates are clearly available.
Controlled Drugs – Quarter 3 2014/15
The key activities relating to the management of Controlled Drugs performed in Quarter 3 were:-
Quarterly audit of Controlled Drugs held on wards and departments Trust-wide Prescription pads security information Errors, incidences or occurrences reported through the IR1 system Prescribed Controlled Drugs information (analysis of prescribing; quantities and trends)
The findings reported by exception are:-
Receipt of Controlled Drugs requisitions not signed for on some occasions at Millside, Ward 2 Bootham Park Hospital and Worsley Court.
Weekly stock checks; no evidence of stock checks being carried out, on some occasions, at Ward 2 Bootham Park Hospital and WorsleyCourt.
Authorised signature lists require updating on; Oakrise, Bluebell Ward (Clifton House), Meadowfields, Rose Ward (Clifton House),Riverfields Ward (Clifton House), Ward 6 (Bootham Park Hospital), Whitehorse View, Westerdale Ward (Clifton House), Wards 2, 3, 4 and 5at Newsam Centre and, PICU.

The following incidents reported via the IR1 system with regards to Controlled Drugs in Quarter 3:-
(i) Newsam Centre Ward 1; 2 x 5mg Nitrazepam tablets unaccounted for in November, investigation inconclusive, no further discrepanciessince
(ii) Newsam Centre Ward 2; PRN Zopiclone administered more than prescribed dose in 24 hours (7.5mg admin, prescribed 3.75mg in 24hours)
(iii) Newsam Centre Ward 5; Clonazepam 125mcg administered but not recorded on drug chart(iv) Becklin Centre Ward 1; Lorazepam prescribed TDS , administered BD, not recorded on T3(v) Becklin Centre Ward 4;
Tramadol 50mg x 4 tablets unaccounted for & Codeine Phosphate 23 tablets unaccounted for during this period. Full investigation,unresolved.
Administration error with Tramadol, immediate release prescribed but MR administered on 10 occasions Prescription for Lorazepam oral/IM PRN, max dose ‘29’ Dr informed and prescription rewritten.
(vi) ICS; Incorrect documentation, MST tablets recorded on two pages in the register(vii) Yorkshire Centre for Psychological Medicine;
4 counts of patients own medication (Temazepam, Diazepam, Tramadol & Morphine) being found in patient’s bedroom or inpatient’s possession (found post leave, removed immediately)
Patient administered 2 x 100mg Tramadol, prescription was for 1 x 100mg Tramadol. Sevredol administered to patient but not recorded on drug chart
(viii) Mount Ward 4; 2 x Buprenorphine patches found in bedside locker, relative brought in, did not inform nursing staff

Information Governance Incident Reports & Information Governance Incidents Requiring Investigation (Leeds & York)
2014/15 Quarter 1 2014/15 Quarter 2 2014/15 Quarter 3 2014/15
Near Miss 75 41 34 19
Level 0 12 3 9 2
Level 1 8 4 4 6
Level 2 1 1 0 5
Level 3 0 0 0 0
Level 4 0 0 0 0
Near Miss incidents differ from level zero incidents in that level zero is a breach, but one where the sensitivity factors indicate low or negligible perceivedimpact.
Minor updates were made to the grading regime “sensitivity factors” in November 2014. This will result in more level 1 than level zero incidents beingreported, although these are still non-SIRI grade incidents. Grading of incidents is now Near Miss, Level 0 and 1 (non-SIRI) and Level 2 (reportable SIRI).
The level 2 incidents reported in Quarter 3 have been escalated to the Information Commissioner’s Office via the national reporting tool and we now awaittheir contact.
Medical Revalidation
On 3 December 2012, Medical revalidation was formally launched by the General Medical Council (GMC). It is the process by which all doctors with alicence to practise in the UK will need to satisfy the GMC, at regular intervals that they are fit to practise and should retain their licence. The first cycle ofrevalidation will take until 2017 to complete.
Year zero January 2013 to March 2013 1 recommendation made Recommendation approved
Year one April 2013 to March 2014 24 recommendations made24 recommendations approved(22 for revalidation, 2 deferments)
Year twoApril 2014 to March 201534 scheduled for the year
Quarter 1 April to June4 recommendations made
Seven recommendations approved
Quarter 2 July to September Eight recommendations approvedQuarter 3 October to December Ten recommendations approved
During Quarter 3, the Trust’s Responsible Officer has made ten recommendations for revalidation and no non-engagement reports to the GMC.
Due to doctors starting, leaving or changing their roles within the Trust the numbers scheduled for revalidation may alter from quarter to quarter.

Strategic Goal 3 : People have a positive experience of their care and supportData Completeness Indicator for Mental Health Outcomes for CPA Patients (Monitor)
Target >= 50.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 60.2% 60.8% 62.0% 63.8% 64.5% 67.9% 72.9% 73.9% 74.5% 71.3% 70.5% 72.9%
Leeds 70.2% 70.7% 71.7% 74.0% 75.0% 74.4% 73.6% 73.5% 73.1% 66.1% 65.4% 65.4%
York & N.Yorkshire
48.0% 49.2% 51.0% 51.1% 52.9% 61.0% 72.2% 74.4% 75.8% 76.2% 75.3% 79.7%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 62.0% 67.9% 74.5% 72.9%
Leeds 71.7% 74.4% 73.1% 65.4%
York & N.Yorkshire
51.0% 61.0% 75.8% 79.7% 40.0%
50.0%
60.0%
70.0%
80.0%
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...York &...Target
Access to Healthcare for People with a Learning Disability (Monitor)
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT

Strategic Goal 3 : People have a positive experience of their care and supportWaiting times for Community Mental Health Teams for face to face contact within 14 days (Leeds Contract)
Target >= 80.0%
Mar 2013/2014
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 61.8% 64.4% 77.5% 80.7%
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 61.8% 64.4% 77.5% 80.7%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
Mar 2013/2014 Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Target
Meeting commitment to serve new psychosis cases by Early Intervention Teams (Monitor)
Target >= 25.5
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 44 47 50 2 5 8 19 24 31 36 45 46
2013/2014 Q4 2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 50 8 31 46
0.0
10.0
20.0
30.0
40.0
50.0
60.0
Jan 2013/2014
Feb 2013/2014
Mar 2013/2014
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Target

Strategic Goal 3 : People have a positive experience of their care and supportOut of Area placements by bed days (Leeds & York)
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT 202 254 298 579 382 467 585 658 331
Leeds 47 13 54 343 179 62 51 100 110
York & N.Yorkshire
155 241 244 236 203 405 534 558 221
0.0
200.0
400.0
600.0
800.0
Apr 2014/2015
May 2014/2015
Jun 2014/2015
Jul 2014/2015
Aug 2014/2015
Sep 2014/2015
Oct 2014/2015
Nov 2014/2015
Dec 2014/2015
LYPFT,...Leeds,...York &...Target
Waiting Times Access to Memory Services (Leeds Contract)
Target >= 70.0%
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 30.9% 45.3% 44.1%
Leeds 30.9% 45.3% 44.1%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 30.9% 45.3% 44.1%
Leeds 30.9% 45.3% 44.1%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target
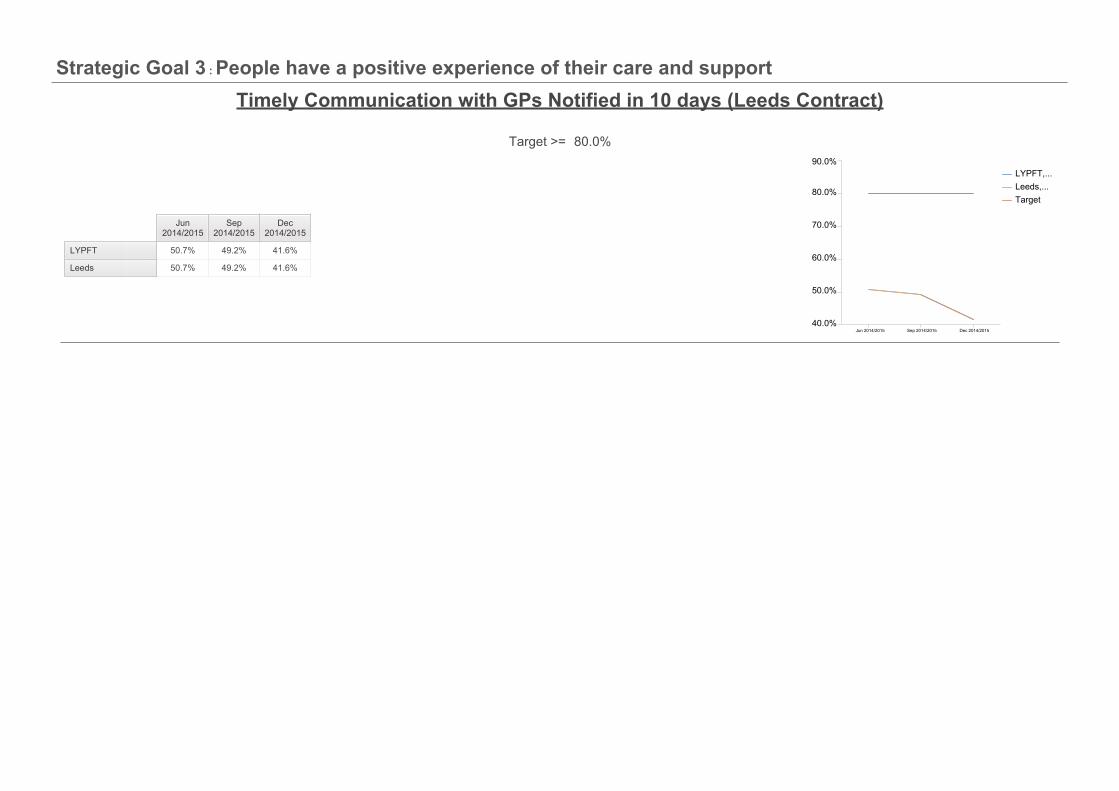
Strategic Goal 3 : People have a positive experience of their care and supportTimely Communication with GPs Notified in 10 days (Leeds Contract)
Target >= 80.0%
Jun 2014/2015
Sep 2014/2015
Dec 2014/2015
LYPFT 50.7% 49.2% 41.6%
Leeds 50.7% 49.2% 41.6%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Leeds,...Target

Additional Data: Strategic Goal 3Number of CAMHS service user’s transitioning to Adult Mental Health services in Leeds (Leeds Contract)
Actual Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
CAMHS to AMHS transition (% with services after 3 months)
50.0% 50.0% 0.0%
CAMHS to AMHS transition (% with services after 6 months)
33.3% 0.0% 0.0%
CAMHS to AMHS transition (% with services after 9 months)
0.0% 0.0% 0.0%
Waiting Times Access to Memory Services (Leeds Contract)Actual Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
Waiting Times to Access Memory Clinic Services (0 - 6 Weeks)
30.9% 45.3% 44.1%
Waiting Times to Access Memory Clinic Services (6 - 12 Weeks)
32.4% 25.7% 27.0%
Waiting Times to Access Memory Clinic Services (12 - 18 Weeks)
28.1% 7.8% 4.9%
Waiting Times to Access Memory Clinic Services (18+ Weeks)
1.8% 0.3% 0.0%

Complaints Summary Report: December 2014
MeasureQuarter 32014/15
December2014
Further Detail
Total number of open complaints at month end 23 23 New complaints received in December (7) were significantlylower than November (29) and lower than the mean average.
Of the new complaints received, 3 relate to the Leeds CareGroup and 4 to the York Care Group. There is no obvioustrend or theme.
Our performance in complaints responses has improved:
We continue to achieve 100% response rate in sendingacknowledgement letters within 3 working days, which isa regulatory requirement.
We met our local 30-day response standard in 50% ofcomplaints responses.
Of the responses that were overdue, 7 were up to onemonth overdue. A new timescale has been agreed for theremaining complaint.
On 12th January 2015 we began a pilot phase of a newComplaints Management process within the Leeds CareGroup. We have agreed a number of improved processes, inline with best practice guidelines, to include:
Making it easier to provide feedback, comments,suggestions and raise concerns, as well as making formalcomplaints;
Grading of complaints according to severity, with tailoredmanagement processes according to level of severity;
Individually tailored complaints timescales agreed withcomplainants;
A clear complaints management escalation process.
Following evaluation of the pilot, new improved processes willbe rolled out across other Care Groups during Q4 of 2013/14;and reflected in a revised procedural document.
Total number of open complaints with the Ombudsman at monthend
0 0
Total number of open complaints which have been reactivated atmonth end
1 1
Number of new complaints received within the month 49 7
Number of complaints closed within the month 43 16
Number & Percentage of complaints responded to that met the 30day response target
14(32%)
8(50%)
Number & Percentage of complaint responses up to one monthoverdue
24(55%)
7(43%)
Number & Percentage of complaint responses up to two monthsoverdue
3(6.9%)
0
Number & Percentage of complaint responses more than twomonths overdue
2(4.6%)
1(6%)
Number & Percentage of complaint responses where a newtimescale had been agreed
14 3
Number & Percentage of acknowledgement letters sent within 3working days (regulatory requirement)
49(100%)
7(100%)
Number of complaints upheld within the month 20 7
Number of complaints partially upheld within the month 1 1
Number of complaints not upheld within the month 22 8

Service User & Carer Feedback
The following patient ‘stories’ have been either published on the Patient Opinion website, NHS Choices or received directly by our staff. Patient storiesrelating to LYPFT can be found at http://www.patientopinion.org.ukor www.nhs.uk. The Trust continues to promote feedback and are committed to usingthe experiences of our service users and carers to further improve our services.
Author story: (Posted on 10 January 2015 via NHS Choices)
“Nice Modern Facilities
Own RoomTV RoomDinning RoomVery professional staff.”
LYPT response: (Posted on 12 January 2015)
Thank you for your review of the Mount, we were very pleased to hear that it met your needs and you clearly felt it to be helpful. It is good to hearwhen things go well and your experience is a positive one.
Kind regardsAndrew Howorth, Head of Patient Experience
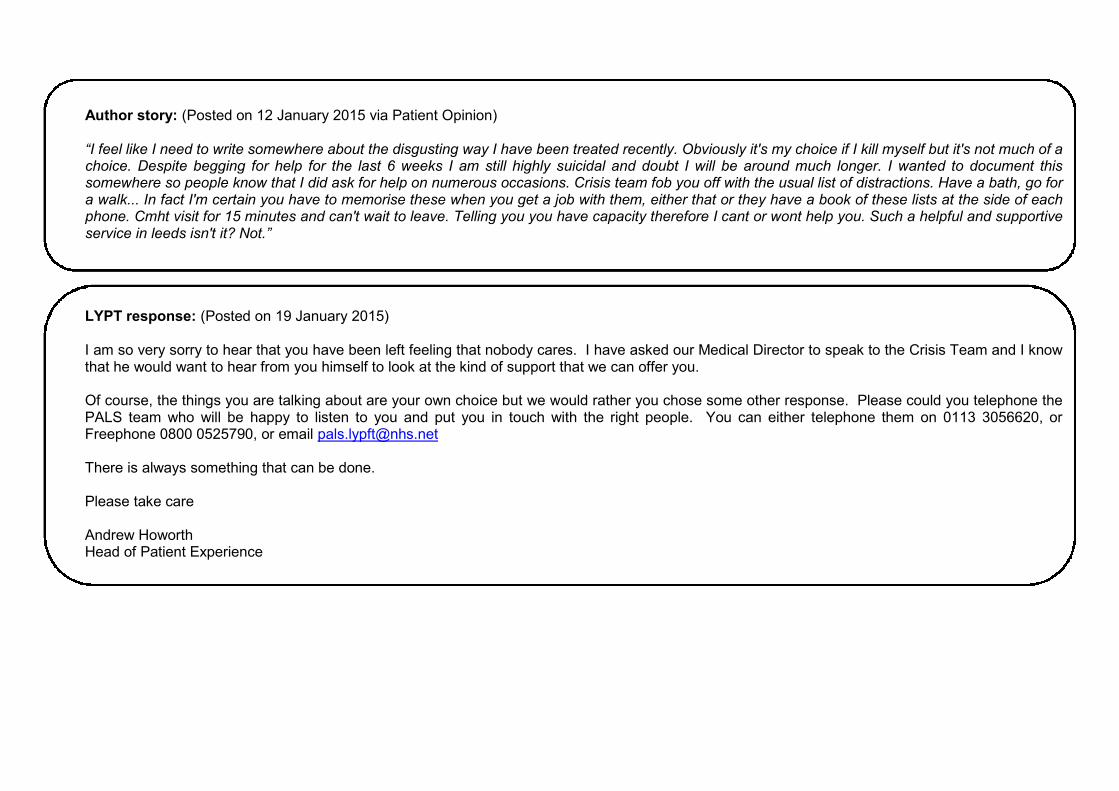
Author story: (Posted on 12 January 2015 via Patient Opinion)
“I feel like I need to write somewhere about the disgusting way I have been treated recently. Obviously it's my choice if I kill myself but it's not much of achoice. Despite begging for help for the last 6 weeks I am still highly suicidal and doubt I will be around much longer. I wanted to document thissomewhere so people know that I did ask for help on numerous occasions. Crisis team fob you off with the usual list of distractions. Have a bath, go fora walk... In fact I'm certain you have to memorise these when you get a job with them, either that or they have a book of these lists at the side of eachphone. Cmht visit for 15 minutes and can't wait to leave. Telling you you have capacity therefore I cant or wont help you. Such a helpful and supportiveservice in leeds isn't it? Not.”
LYPT response: (Posted on 19 January 2015)
I am so very sorry to hear that you have been left feeling that nobody cares. I have asked our Medical Director to speak to the Crisis Team and I knowthat he would want to hear from you himself to look at the kind of support that we can offer you.
Of course, the things you are talking about are your own choice but we would rather you chose some other response. Please could you telephone thePALS team who will be happy to listen to you and put you in touch with the right people. You can either telephone them on 0113 3056620, orFreephone 0800 0525790, or email [email protected]
There is always something that can be done.
Please take care
Andrew HoworthHead of Patient Experience

Author story: (Posted on 12 January 2015 via Patient Opinion)
“I felt as though I was expected to know exactly what type of support I wanted to receive and when I became quite distressed because I clearly neededmore guidance, I received none. There seemed to be no intuition and no sensitivity on the part of the assessor, as though they did not understand thedifficulty that some of the questions were posing on me. Some of the things that were said made me feel unworthy of receiving mental health servicesand greedy and as though I was blowing my own problems out of proportion compared to some other people.
I was told to refer myself to a counselling organisation in Leeds (which is currently not accepting referrals) or to go to my University's counsellingservice. As I have been diagnosed with Bipolar Disorder, I was told by my GP to book an initial assessment with a view to receive some sort of therapythat would give me insight into my illness and help me to cope with other traumas from my past. Although I am willing to attend counselling sessions atuniversity, I feel that counselling will not be sufficient to do all of this and that a psychotherapy would be more appropriate initially.
I feel the opposite of supported now and felt a severe distrust in the mental health services of the NHS when I left the building, which I know is mainlydue to lack of funding and support from this government but it was a real shock. I feel very alone and unsure of where to go next.”
LYPT response: (Posted on 19 January 2015)
I was so very sorry to hear about your experiences. Please will you telephone PALS on 0113 3056620, or email them on [email protected] to discussthis so that we can make sure that you get the proper help that you need.
Thank you.
Andrew HoworthHead of Patient Experience
Author story: (Posted on 16 January 2015 via Patient Opinion)
“Admitted to you hospital for medication themn to the Newsome centre ward 4 for rehabilitation”
LYPT response: (Posted on 20 January 2015)
Thank you for posting on this site, I do hope that you have found the help offered on Ward 4 to be of help? We are always keen to hear about people’sexperience and to learn from them.
If there is more that you want to tell us please do, or speak to somebody in our PALS office, by emailing: [email protected].
With very best wishes for a speedy recovery.
Andrew HoworthHead of Patient Experience

Appendix A :
Staff Turnover
Target < 15.0%Jun
2014/2015Sep
2014/2015Dec
2014/2015
LYPFT 12.9% 13.8% 13.5%
Care Services
10.9% 11.6% 11.9%
Corporate Services
21.1% 23.0% 20.2%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 12.9% 13.8% 13.5%
Care Services
10.9% 11.6% 11.9%
Corporate Services
21.1% 23.0% 20.2% 10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
22.0%
24.0%
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Care S...Corpor...Target
Sickness Absence
Target < 4.2%Jun
2014/2015Sep
2014/2015Dec
2014/2015
LYPFT 4.5% 4.7% 5.0%
Care Services
4.9% 5.0% 5.4%
Corporate Services
3.1% 3.4% 3.2%
2014/2015 Q1 2014/2015 Q2 2014/2015 Q3
LYPFT 4.5% 4.7% 5.0%
Care Services
4.9% 5.0% 5.4%
Corporate Services
3.1% 3.4% 3.2% 3.0%
3.5%
4.0%
4.5%
5.0%
5.5%
Jun 2014/2015 Sep 2014/2015 Dec 2014/2015
LYPFT,...Care S...Corpor...Target

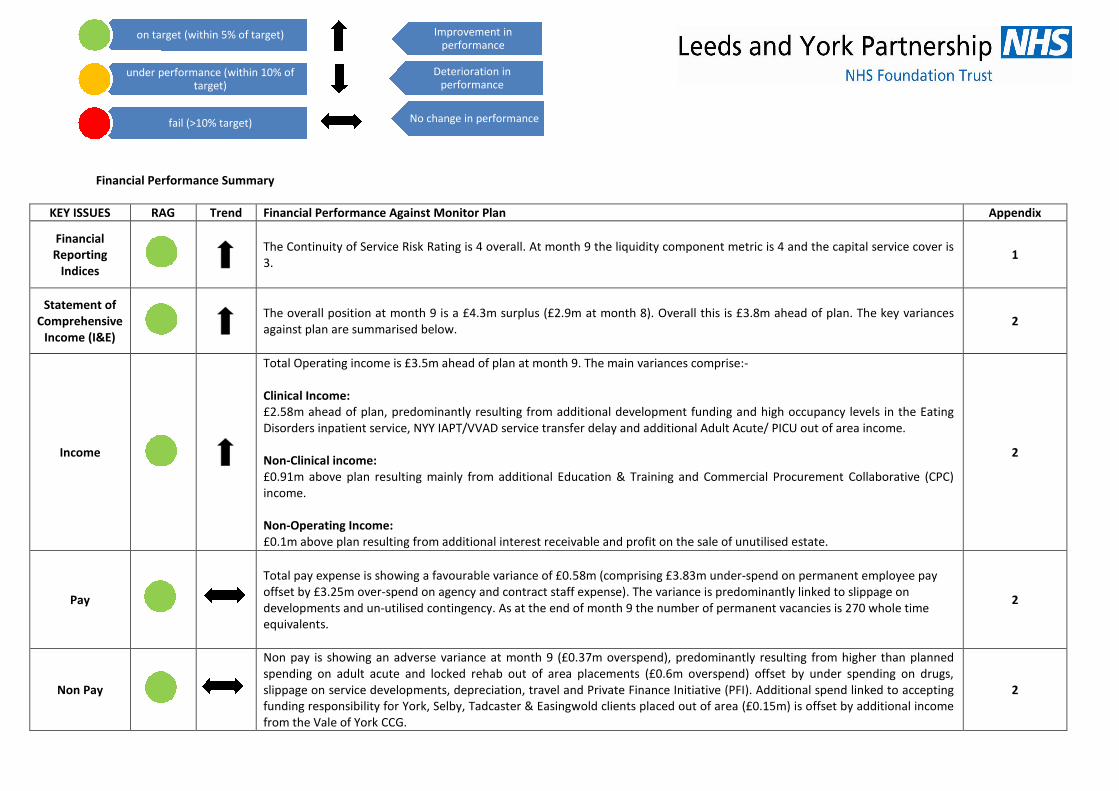
Financial Performance Summary
KEY ISSUES RAG Trend Financial Performance Against Monitor Plan Appendix
FinancialReporting
Indices
The Continuity of Service Risk Rating is 4 overall. At month 9 the liquidity component metric is 4 and the capital service cover is3.
1
Statement ofComprehensive
Income (I&E)
The overall position at month 9 is a £4.3m surplus (£2.9m at month 8). Overall this is £3.8m ahead of plan. The key variancesagainst plan are summarised below.
2
Income
Total Operating income is £3.5m ahead of plan at month 9. The main variances comprise:-
Clinical Income:£2.58m ahead of plan, predominantly resulting from additional development funding and high occupancy levels in the EatingDisorders inpatient service, NYY IAPT/VVAD service transfer delay and additional Adult Acute/ PICU out of area income.
Non-Clinical income:£0.91m above plan resulting mainly from additional Education & Training and Commercial Procurement Collaborative (CPC)income.
Non-Operating Income:£0.1m above plan resulting from additional interest receivable and profit on the sale of unutilised estate.
2
Pay
Total pay expense is showing a favourable variance of £0.58m (comprising £3.83m under-spend on permanent employee payoffset by £3.25m over-spend on agency and contract staff expense). The variance is predominantly linked to slippage ondevelopments and un-utilised contingency. As at the end of month 9 the number of permanent vacancies is 270 whole timeequivalents.
2
Non Pay
Non pay is showing an adverse variance at month 9 (£0.37m overspend), predominantly resulting from higher than plannedspending on adult acute and locked rehab out of area placements (£0.6m overspend) offset by under spending on drugs,slippage on service developments, depreciation, travel and Private Finance Initiative (PFI). Additional spend linked to acceptingfunding responsibility for York, Selby, Tadcaster & Easingwold clients placed out of area (£0.15m) is offset by additional incomefrom the Vale of York CCG.
2
on target (within 5% of target)
under performance (within 10% oftarget)
fail (>10% target)
Improvement inperformance
Deterioration inperformance
No change in performance

Efficiency:Cost
Improvement
The Cost Improvement Plan (CIP) for month 9 is £1.0m (40%) below plan, with £1.6m achieved compared to £2.6 plan. The mainunder achievement relates to Leeds Care Group plan (£1m).
3Efficiency:Revenue
Generation
The revenue generation plan for month 9 is £0.43m (37%) above plan resulting from high occupancy levels in the EatingDisorders inpatient service.
Statement ofFinancialPosition
(Balance Sheet)
Note - The statement of financial position in the Monitor plan for 2014-15 was, for the first time, based on forecast outturnrather than the actual year–end position. This has had a significant impact on opening balances and consequently some of thevariances below, due to timing differences and assumptions made at that time. The main statement of financial positionvariances (excluding cash and capital) are:
Property, plant and equipment and PFI property, plant and equipment – £1.36m total variance. There is an offsetting varianceof £0.9m on the opening value of each line due to the breakdown of the annual valuation. Slippage in the capital programme of£1.3m is offset by reduced depreciation of £0.23m and the delayed sale of Malham House £0.55m.
Non NHS trade receivables - £0.95m variance caused mainly by a delay in raising invoices due to the conversion of the FinanceIT systems in December 2014 (now complete). This is partially offset by an increase in accrued income.
Accrued income - £1.19m variance caused mainly by NHS England funding not yet received for forensic beds (£0.09m),distinction awards (£0.32m) and LCRN funding for nine months (£2.3m). There is also an increase due to the conversion of theFinance IT systems which is offset by a reduction in receivables.
Provisions (current £1.8m and non-current £1.0m) - £2.8m total variance being the phasing of provisions for Management ofChange, NYY Estate and Dilapidation costs.
Accruals, current - £0.35m variance. This is due to a reduction in PFI life cycle costs accrued following payment of £0.78m. Thisis offset by an increase in accruals due to the conversion of the Finance IT systems.
Deferred income - £0.85m variance – this is mainly due to the contract variations in the Leeds block for the Crisis AssessmentUnit (CAU) and Rehabilitation & Recovery (R&R) (£6.7m), Personality Disorder (PD) project (£0.17m) and the PD Women’sintensive RMS income as the service has not yet started (£0.14m).
Capital payables - £0.94m variance caused by active schemes such as Asket R&R, East North East Hub and Millfield as well asthe Equitix dispute over air conditioning for £0.17m.
4
Cash
The cash position of £47.0m is £6.6m ahead of Monitor plan at the end of month 9. This is mainly caused by the increasedsurplus YTD of £3.8m. Other items include an increase in working capital of £4.9m and an increase of £1.8m from investingactivities (capital schemes) however; these are offset by a decrease in the opening cash position of £3.7m as per the statementof financial position above.
Liquidity increased to 66 days operating expenses at the end of December 2014 (64 days at 30 November 2014).
5
Capital
Capital expenditure was £2.72m at the end of month 9, which is 88% of the re-forecast capital programme. The main items ofslippage are estates and IT operational schemes, which are now anticipated to be later in the year.
The capital programme for 2014-15 was re-forecast at Q1 with the planned programme now £5.2m.
6
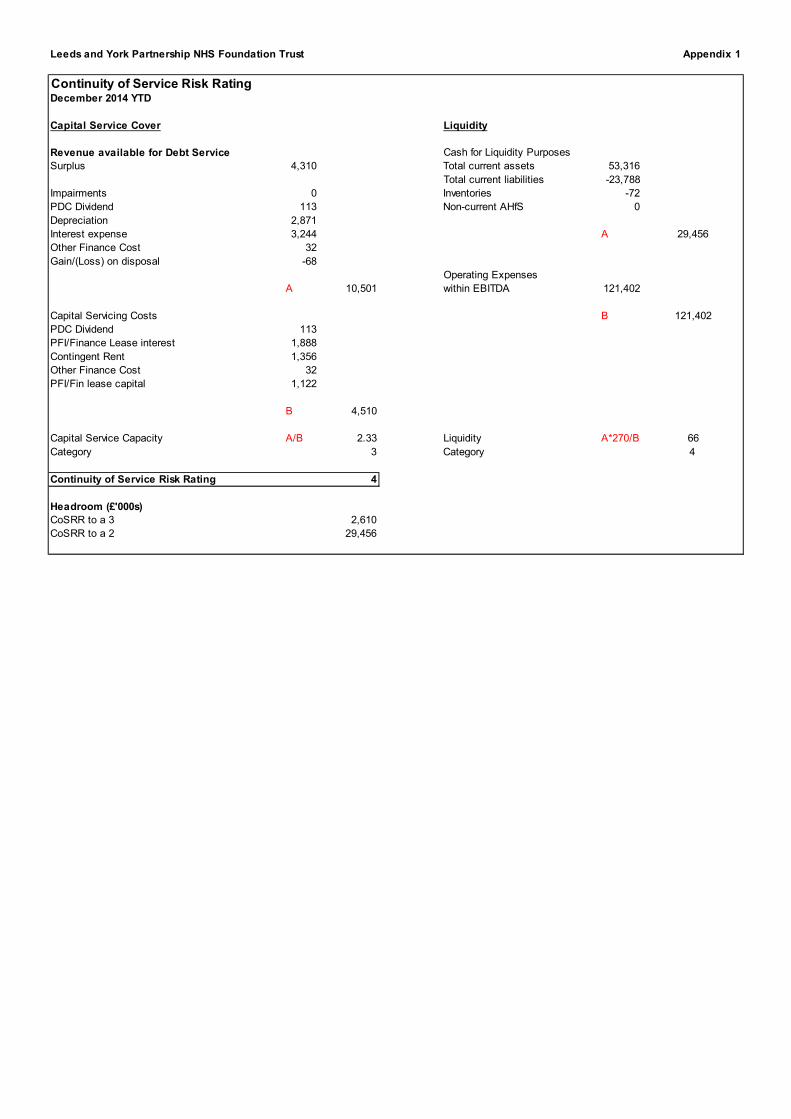
Leeds and York Partnership NHS Foundation Trust Appendix 1
Continuity of Service Risk RatingDecember 2014 YTD
Capital Service Cover Liquidity
Revenue available for Debt Service Cash for Liquidity Purposes
Surplus 4,310 Total current assets 53,316
Total current liabilities -23,788
Impairments 0 Inventories -72
PDC Dividend 113 Non-current AHfS 0
Depreciation 2,871
Interest expense 3,244 A 29,456
Other Finance Cost 32
Gain/(Loss) on disposal -68
Operating Expenses
A 10,501 within EBITDA 121,402
Capital Servicing Costs B 121,402
PDC Dividend 113
PFI/Finance Lease interest 1,888
Contingent Rent 1,356
Other Finance Cost 32
PFI/Fin lease capital 1,122
B 4,510
Capital Service Capacity A/B 2.33 Liquidity A*270/B 66
Category 3 Category 4
Continuity of Service Risk Rating 4
Headroom (£'000s)
CoSRR to a 3 2,610
CoSRR to a 2 29,456

Leeds and York Partnership NHS Foundation Trust Appendix 2
Statement of Comprehensive Income at December 2014
Monitor Actual Variance Variance
Plan Monitor
YTD YTD YTD @ Month 8
£'000 £'000 £'000 £'000
Operating
NHS Mental Health activity Income
Other - Cost and Volume Contract Income 3,261 3,700 438 373
Block Contract Total 103,135 105,101 1,966 1,098
Clinical Partnerships providing mandatory services (including S31 agreements) 5,726 5,771 46 49
Other clinical income from mandatory services 3,157 3,291 134 114
NHS Mental Health activity Income, Total 115,278 117,863 2,584 1,633
Other Operating income
Research and Development income 635 630 -5 11
Education and Training income 2,738 3,032 294 238
Grants received in cash & to fund Operating Expenses 35 35 0 0
Parking revenue 0 0 0 0
Catering revenue 40 50 10 8
Revenue from non-patient services to other bodies 1,508 1,569 61 61
Misc. Other Operating Income 8,038 8,591 553 464
Other Operating income, Total 12,994 13,906 913 781
Operating Income, Total 128,272 131,769 3,497 2,414
Operating Expenses
Raw Materials and Consumables Used
Drugs -2,033 -1,674 359 231
Clinical supplies -1,177 -1,199 -22 -37
Non-clinical supplies -1,144 -1,484 -340 -330
Raw Materials and Consumables Used, Total -4,354 -4,357 -3 -135
Cost of Secondary Commissioning of mandatory services -1,410 -2,160 -751 -543
Employee Benefits Expenses, permanent staff -94,584 -90,751 3,832 3,282
Employee Benefits Expenses, agency & contract staff -2,064 -5,315 -3,251 -2,735
Employee Benefits Expenses, Total -96,648 -96,067 582 548
Research and Development expense -724 -746 -22 -34
Education and training expense -490 -531 -41 -41
Consultancy Expense -16 -102 -86 -56
Misc. Other Operating expense -12,865 -12,580 285 21
PFI operating expenses -4,949 -4,858 91 82
Depreciation and Amortisation
Depreciation and Amortisation - owned assets -1,907 -1,705 202 182
Depreciation and Amortisation - assets held under finance leases -25 -2 24 21
Depreciation and Amortisation - PFI assets -1,094 -1,164 -70 -62
Depreciation and Amortisation, Total -3,026 -2,871 156 142
Impairment (Losses) / Reversals net 0 0 0 0
Operating Expenses, Total -124,483 -124,272 211 -17
Profit (Loss) from Operations 3,789 7,497 3,708 2,398
Non Operating
Non-Operating income
Interest Income 90 134 44 38
Profit/Loss on Asset Disposal 0 68 68 69
Non-Operating income, Total 90 202 112 107
Non-Operating expenses
Finance Costs [for non-financial activities]
Interest Expense
Interest Expense on Finance leases (non-PFI) -190 -172 18 15
Interest Expense on PFI leases & liabilities -1,779 -1,716 63 53
Interest Expense, Total -1,969 -1,888 81 68
PDC dividend expense -106 -113 -7 -15
Other Finance Expenses -40 -32 8 8
Finance Costs [for non-financial activities], Total -2,114 -2,032 82 62
Non-Operating PFI Costs (e.g. Contingent Rent) -1,250 -1,356 -106 -94
Non-Operating expenses, Total -3,364 -3,388 -24 -33
Surplus (Deficit) before Tax 515 4,310 3,795 2,472
Income Tax (expense)/ income 0 0 0 0
Surplus (Deficit) After Tax 515 4,310 3,795 2,472
2014/15

Appendix 3
2014-15
CIP THEMES & REVENUE GENERATION Plan Plan Actual Variance Variance
£'000 £'000 £'000 £'000 %
Leeds Mental Health Care Group 1,688 1,266 221 (1,045) -82.5%
York & North Yorkshire Mental Health Care Group 34 26 26 0 0.0%Specialist & Learning Disability Care Group 595 446 348 (98) -22.0%Providing services from fit-for-purpose, cost effective buildings 422 317 387 70 22.1%Delivering cost effective corporate services 727 545 577 32 5.9%Revenue Generation 1,542 1,156 1,583 427 36.9%
TOTAL 5,009 3,756 3,142 (614) -16.3%
Pay 2,077 1,558 947 (611) -39.2%Non Pay 1,390 1,042 612 (430) -41.3%
Total CIP 3,467 2,600 1,559 (1,041) -40.0%
Income 1,542 1,156 1,583 427 36.9%
TOTAL 5,009 3,756 3,142 (614) -16.3%
Leeds & York Partnership NHS Foundation Trust
Cost Improvement Plans & Revenue Generation Schemes 2014-15
Year to Date

Leeds and York Partnership NHS Foundation Trust Appendix 4
Statement of Financial Position at December 2014
Monitor Actual Variance
Plan
December December December
£'000 £'000 £'000
Assets
Assets, Non-Current
Intangible Assets, Net 182 239 57
Property, Plant and Equipment, Net 32,776 31,417 -1,359
PFI: Property, Plant and Equipment, Net 18,636 19,478 842
Other Receivables, Non-Current 0 0 0
Prepayments, Non-Current 3,242 3,251 9
Assets, Non-Current, Total 54,837 54,385 -452
Assets, Current
Inventories 72 72 0
Trade and Other Receivables, Net, Current
NHS Trade Receivables, Current, Gross 1,000 950 -50
Non NHS Trade Receivables, Current, Gross 2,300 1,346 -954
Other Receivables, Current, Gross 550 537 -13
Impairment of Receivables, Current ( for bad & doubtful debts ) -217 -459 -242
Trade and Other Receivables, Net, Current, Total 3,633 2,373 -1,260
Accrued Income 1,500 2,690 1,190
Prepayments, Current 1,200 1,172 -28
Cash 40,433 47,009 6,577
Non-Current Assets held for sale 0 0 0
Assets, Current, Total 46,837 53,316 6,478
Total Assets 101,674 107,701 6,027
Liabilities
Liabilities, Current
Deferred Income, Current -3,094 -3,943 -849
Provisions, Current -209 -2,014 -1,805
Trade and Other Payables, Current
Trade Payables, Current -5,366 -5,070 296
Other Payables, Current -4,500 -4,314 186
Capital Payables, Current -200 -1,137 -937
Trade and Other Payables, Current, Total -10,066 -10,522 -456
Other Financial Liabilities, Current
Accruals, Current -6,000 -5,651 349
Finance Leases, Current -253 -286 -33
PFI leases, Current -1,260 -1,338 -78
PDC dividend payable, Current -35 -34 2
Other Financial Liabilities, Current, Total -7,549 -7,309 239
Liabilities, Current, Total -20,917 -23,788 -2,871
NET CURRENT ASSETS (LIABILITIES) 25,920 29,528 3,608
Liabilities, Non-Current
Provisions, Non-Current -1,555 -2,560 -1,005
Other Financial Liabilities, Non-Current
Finance Leases, Non-current -1,550 -1,521 29
PFI leases, Non-Current -26,653 -26,585 68
Other Financial Liabilities, Non-Current, Total -28,203 -28,106 97
Liabilities, Non-Current, Total -29,758 -30,666 -908
TOTAL ASSETS EMPLOYED 50,999 53,247 2,248
Taxpayers' and Others' Equity
Public dividend capital 19,119 19,119 0
Retained Earnings (Accumulated Losses) 25,140 27,609 2,469
Revaluation Reserve 7,391 7,170 -221
Miscellaneous Other Reserves -651 -651 0
TAXPAYERS EQUITY, TOTAL 50,999 53,247 2,248
TOTAL ASSETS EMPLOYED 50,999 53,247 2,248
2014/15

Appendix 5
Leeds Partnerships NHS Foundation Trust
Cashflow Analysis as at December 2014
Monitor Actual Variance
Plan
YTD YTD YTD
£'000 £'000 £'000
Surplus/(deficit) after tax 515 4,310 3,795
non-cash flows in operating surplus/(deficit)
Finance income/charges 3,129 3,110 -19
Other operating non-cash movements 0 0 0
Depreciation and amortisation, total 3,026 2,871 -156
Impairment losses/(reversals) 0 0 0
Gain/(loss) on disposal of property plant and equipment 0 -68 -68
Gain/(loss) on disposal of intangible assets 0 0 0
PDC dividend expense 106 113 7
Other increases/(decreases) to reconcile to profit/(loss) from operations 0 0 0
Non-cash flows in operating surplus/(deficit), Total 6,261 6,025 -236
Operating Cash flows before movements in working capital 6,776 10,336 3,560
Increase/(Decrease) in working capital
(Increase)/decrease in inventories 0 0 0
(Increase)/decrease in NHS Trade Receivables -250 916 1,166
(Increase)/decrease in Non NHS Trade Receivables -700 2,090 2,790
(Increase)/decrease in other receivables 200 1,714 1,514
(Increase)/decrease in accrued income -750 -2,018 -1,268
(Increase)/decrease in prepayments 0 -120 -120
(Increase)/decrease in other assets 0 0 0
Increase/(decrease) in Deferred Income 847 2,097 1,251
Increase/(decrease) in provisions -1,758 -942 816
Increase/(decrease) in post-employment benefit obligations 0 0 0
Increase/(decrease) in Trade Payables 1,782 789 -993
Increase/(decrease) in Other Payables 0 190 190
Increase/(decrease) in accruals 790 382 -408
Increase/(Decrease) in workling capital, Total 161 5,098 4,937
Net cash inflow/(outflow) from operating activities 6,936 15,434 8,497
Net cash inflow/(outflow) from investing activities
Property, plant and equipment expenditure -4,200 -1,961 2,238
Proceeds on disposal of property, plant and equipment 1,100 643 -457
Net cash inflow/(outflow) from investing activities, Total -3,100 -1,319 1,781
Net cash inflow/(outflow) before financing 3,836 14,115 10,278
Net cash inflow/(outflow) from financing activities
Public Dividend Capital received 0 0 0
Public Dividend Capital repaid 0 0 0
PDC Dividends paid -119 -146 -28
Interest element of finance lease rental payments - other -232 -219 13
Interest element of finance lease rental payments - On-balance sheet PFI -2,986 -3,024 -38
Capital element of finance lease rental payments - other -190 -186 4
Capital element of finance lease rental payments - On-balance sheet PFI -945 -936 10
Interest received on cash and cash equivalents 90 134 44
Movement in Other grants/Capital received 0 0 0
(Increase)/decrease in non-current receivables -250 -258 -8
Increase/(decrease) in non-current payables 0 0 0
Other cash flows from financing activities 0 0 0
Net cash inflow/(outflow) from financing activities, Total -4,632 -4,636 -3
Net increase/(decrease) in cash and cash equivalents -796 9,479 10,275
Opening cash and cash equivalents 41,228 37,530 -3,698
Effect of exchange rates 0 0 0
Closing cash and cash equivalents 40,433 47,009 6,577

CAPITAL PROGRAMME - at 31st DECEMBER 2014 Appendix 6
Monitor Actual YTD
Re-forecast Spend Variance
£'000 £'000 £'000
OPERATIONAL CAPITAL
Estates
Health & Safety /Fire 87 54 -33
Planned Annual Commitments 150 -150
Backlog Maintenance 102 -102
Replacement Vehicles 35 35 0
Sub-Total 373 89 -284
IT/Telecomms
Additional Server/Storage 25 -25
Virtual Desktop Infrastructure 30 -30
IT-Voice Telecoms Network 15 -15
IT-NCRS/N3 Infrastructure 20 39 19
Dashboard Professional 7 -7
Additional Cognos Licences + Server 44 58 14
PC Replacement Programme (Leeds) 167 177 10Additional Server/Storage Capacity 19 18 -1Trust WAN Upgrade (Leeds & York) 250 47 -203
Medical Devices Management System 25 -25Videoconferencing (York) 20 -20Additional IT Infrastructure 92 -92Single Sign-On System 40 -40Unified Communications 0 7 7
Sub-Total 755 347 -408Other Equipment
Vehicles 29 -29
Woodland Square CCTV 11 -11
ECG Machine (X2) 15 -15
Physio Equipment Newsam 19 -19
Sub-Total 73 0 -73
2013/14 Completed Schemes -2 -6 -3
Estimated Slippage -442 442
TOTAL OPERATIONAL CAPITAL 757 430 -327
STRATEGIC DEVELOPMENTS
Estate
ENE Hub 708 476 -232
Cafés At The Mount / Becklin Centre 25 -25
Dementia Care At The Mount 0 11 11
Seclusion Room - Newsam Centre 99 109 10
Asket Croft R&R 325 518 193
LD In-Patient Reprovision 0 69 69
HQ relocation/ St Marys House 92 95 3
Millfield (Contingency) 84 92 8
Mount / Asket House Air Con (contingency) 32 33 1
Asket House Nursecall / Maglock (contingency) 6 6 0
Becklin Car Park Barrier 60 66 6
PFI OOH Access 13 -13
YNY - fixtures and fittings for ML and CTH 170 33 -137
Vacate Malham House 75 0 -75
Sub-Total 1,689 1,508 -180
IT
Tablets Wards Pilot 36 1 -35
Electronic Prescribing 60 -60
Migration of York IT infrastructure to LYPFT 225 289 65
EPR System Developments 45 75 30
PC Replacement & Upgrade (York & NY) 253 291 38
Laptops for Students 0 116 116
Sub-Total 618 772 154
TOTAL STRATEGIC CAPITAL 2,307 2,280 -26
Contingency Schemes 0 0
CPC Telephone System 20 11 -9
TOTAL CONTINGENCY 20 11 -9
TOTAL CAPITAL PROGRAMME 3,083 2,722 -362

1
1. INTRODUCTION
Prior to 2010/2011 for both annual risk assessment and in-year monitoring,Monitor assigned a risk rating in three areas - finance, governance andmandatory goods and services. From 2010 onwards the provision ofmandatory goods and services is included in the governance risk rating.
Monitor uses these risk ratings to guide the intensity of its monitoring and tosignal to the NHS Foundation Trust its degree of concern with the specificissues identified and evaluated.
The table below shows the Trust’s risk ratings to date. The previous amber-redrisk ratings have been due to compliance actions received by the Care QualityCommission as a result of inspections. All compliance actions have beenaddressed in a timely and effective manner.
Riskratings
Atauthorisation
At Q22007/08
At Q32007/08
At Q42007/08
Risk ratingat 2007/08year end
Financial 3 3 3 4 4Governance Green Green Green Green GreenMandatoryservices
Green Green Green Green Green
Riskratings
At Q12008/09
At Q22008/09
At Q32008/09
At Q42008/09
Risk ratingat 2008/09year end
Financial 3 3 3 3 3Governance Green Green Green Amber AmberMandatoryservices
Green Green Green Green Green
Riskratings
At Q12009/10
At Q22009/10
At Q32009/10
At Q42009/10
Risk ratingat 2009/10year end
Financial 4 4 4 4 4Governance Green Green Green Green GreenMandatoryservices
Green Green Green Green Green
Riskratings
At Q12010/11
At Q22010/11
At Q32010/11
At Q42010/2011
Risk ratingat 2010/11year end
Financial 4 5 5 4 4Governance Green Green Green Green Green

2
Riskratings
At Q12011/12
At Q22011/12
At Q32011/12
At Q42011/12
Risk ratingat 2011/12year end
Financial 4 4 4 4 4Governance Amber Red Amber Red Amber Red Green Green
Riskratings
At Q12012/13
At Q22012/13
At Q32012/13
At Q42012/13
Risk ratingat 2012/13year end
Financial 4 4 4 4 4Governance Green Green Green Green Green
Riskratings
At Q12013/14
At Q22013/14
At Q32013/14
At Q42013/14
Risk ratingat 2013/14year end
Financial 4 4 4 4 4Governance Green Green Green Green Green
Riskratings
At Q12014/15
At Q22014/15
At Q32014/15
At Q42014/15
Risk ratingat 2014/15year end
Financial 4 4 4Governance Green Green Green
FINANCIAL COMMENTARY PERIOD 1st APRIL 2014 TO 31st DECEMBER 2014
2.1 Introduction
This report describes the financial position of the Trust as at Quarter 3.
It also provides assurance to support confirmation that the Trust anticipatesmaintaining a Continuity of Service Risk Rating of at least 3 over the next 12months, as required by Monitor.
2.2 2014/15 Financial Position
The financial position as at the end of quarter 3 is robust, with higher thanplanned Income Statement surplus (Income and Expenditure). The Continuityof Service Risk Rating is ‘4’.
Year to 31st
December 2014 COSRR Score Category
Capital Service Cover 2.33 3
Liquidity 66 4
Continuity of Service Risk Rating 4
The overall income and expenditure surplus is £4.3m against a planned surplusof £0.52m, a positive variance of £3.8m. Overall, the variance is predominantlydriven by non-recurrent income and the level of under-spend on pay expenses(inclusive of unutilised contingency reserve and development slippage).

3
2.3 Income
At 31st December 2014 overall operating income is £3.5m above plan.
Clinical Income is £2.6m ahead of plan, predominantly resulting from additionaldevelopment funding and high occupancy levels in the Leeds Eating Disordersinpatient service. A presentational variance due to the delay in a servicetransfer to another provider as agreed with Vale of York commissioners (thishas a corresponding expenditure variance c£0.5m see below) is contributing tothe income position.
Other Operating Income was £0.91m above plan linked primarily to additionalconfirmed education and training tariff income and Commercial ProcurementCollaborative income.
2.4 Pay
Pay expenditure is showing a favourable variance of £0.58m (comprising£3.83m under-spend on permanent employee pay offset by £3.25m over-spendon agency and contract staff expense). The net position includes:
Pay CIP slippage £(0.61)m. Delayed transfer of IAPT, VVADS & Eating Disorders services £(0.44)m. Slippage on development posts and unutilised contingency reserves
£0.60m. Other vacancies £1.03m.
2.5 Non Pay
Non pay is showing an adverse variance at month 9 (£0.37m overspend),predominantly resulting from higher than planned spending on adult acute andlocked rehab out of area placements (£0.6m overspend). This is offset by underspending on drugs, slippage on service developments, depreciation, travel andPrivate Finance Initiative (PFI). Additional spend linked to accepting fundingresponsibility for York, Selby, Tadcaster & Easingwold clients placed out ofarea (£0.15m) is offset by additional income from the Vale of York CCG.
2.6 Non-Operating Income / Expenses
No significant variances in Quarter 3.
2.7 Cost Improvement Plans & Revenue Generation Schemes
The Cost Improvement Plan for quarter 3 is £1.04m (40%) below plan, with£1.56m achieved compared to £2.60m plan. The main under achievementrelates to Leeds Care Group acute pathway redesign delays. There isoverachievement on delivering cost effective corporate services and revenuegeneration. Revenue generation schemes exceeding plan by £0.43m and thisequates to a surplus of 37%. The overall shortfall on CIPs and revenue

4
generation schemes is £614k (16%). Contingency reserves are offsetting theoverall level of slippage.
2.8 Statement of Financial Position (Balance Sheet)
Cash
The cash position of £47.0m is £6.6m ahead of Monitor plan at the end ofmonth 9. This is mainly caused by the increase in surplus YTD of £3.8m,increase in working capital of £4.9m and an underspend on investmentactivities of £1.8m, offset by a decrease in the opening cash position of £3.7m.
It is important to note that the opening cash position shows as £3.7m behindplan. The reason for the variance is because two significant receipts totalling£2.5m were received after the year-end (1 and 15 April 2014) and payments toNHS Property Services were made prior to the year-end, ie earlier thanforecast. These would not normally cause a variance as the Monitor plan isusually based on the actual closing cash position. However, the 2014-15Monitor plan was required in advance of the year-end and was therefore basedon the 2013-14 forecast out-turn position, which did not foresee the timingissues identified above.
Liquidity increased slightly to 66 days operating expenses in Quarter 3 (61 daysat Quarter 2 2014-15).
Provisions
Provisions were increased in the Trusts final accounts for 2013-14. Theincrease was not envisaged in the plan with the Bootham and Lime Treesprovision being included after the draft accounts were submitted. Theseprovisions are categorised as current and non-current as appropriate. The mainprovisions are Management of Change, Bootham and Lime Trees andDilapidation costs.
The utilisation of these provisions is not currently in line with plan. It isanticipated that any unutilised provision will be carried forward to 2015-16.
2014-15
CIP THEMES & REVENUE GENERATION Plan Plan Actual Variance Variance
£'000 £'000 £'000 £'000 %
Leeds Mental Health Care Group 1,688 1,266 221 (1,045) -82.5%York & North Yorkshire Mental Health Care Group 34 26 26 0 0.0%Specialist & Learning Disability Care Group 595 446 348 (98) -22.0%Providing services from fit-for-purpose, cost effective buildings 422 317 387 70 22.1%Delivering cost effective corporate services 727 545 577 32 5.9%Revenue Generation 1,542 1,156 1,583 427 36.9%
TOTAL 5,009 3,756 3,142 (614) -16.3%
Pay 2,077 1,558 947 (611) -39.2%Non Pay 1,390 1,042 612 (430) -41.3%
Total CIP 3,467 2,600 1,559 (1,041) -40.0%
Income 1,542 1,156 1,583 427 36.9%
TOTAL 5,009 3,756 3,142 (614) -16.3%
Year to Date

5
However, any unutilised provision not carried forward would need to bereversed, which would increase the 2014-15 surplus.
2.9 Capital Expenditure
As at quarter 3, capital expenditure was £2.7m, which is 88% of the re-forecastcapital plan.
The re-forecast Capital Plan for 2014-15 is £5.2m from the original plan of£5.9m. The re-forecast spend for the remainder of the current financial yearconsiders scheme slippage where appropriate.
2.10 Forecast Financial Performance over the next 12 Months
The Trust is required to confirm that it anticipates maintaining a Continuity ofService Risk Rating of at least 3 over the next 12 months. To support thisdeclaration a 12 month forward look including cash flow is produced. Theforecast Continuity of Service Risk Rating of ‘3’ as at 31 December 2015 isbased on the following assumptions:
2014/15 I&E surplus estimated at c£5.8m (based on current run rateestimates).
Cumulative Quarter 3 2015/16 I&E position as per first draft annual plan. Capital expenditure plans as per the five year forecast submitted to Monitor
in January 2015, which reflects an early assessment of requirements forestate and technology.
Cash balance of £40.9m as at 31 December 2015.
The table below shows a strong forecast Continuity of Service Risk Rating of 3in the next 12 months with EBITDA forecast above current plans.
January 2015 - December 2015
Capital Service Cover Liquidity
Revenue available for Debt Service Cash for Liquidity Purposes
Surplus 129 Working capital facility 0
Total current assets 47,069
Impairments 0 Total current liabilities -22,559
Restructuring Costs 0 Inventories -72
PDC Dividend 161 Derivatives 0
Depreciation 3,888 Financial AHfS 0
Interest expense 4,115 PFI prepayments 0
Other Finance Costs 23 Non-current AHfS 0
Gain/(Loss) on disposal 0 Current AHfS by charity 0
Capital grants/donations 0 Current LHfS by charity 0
A 8,316 A 24,438
Capital Servicing Costs Operating Expenses
PDC Dividend 161 within EBITDA 168,825
Bank interest 0
Loan interest 0
Other Finance Costs 23
PFI/Finance Lease interest 2,440
Contingent Rent 1,675
Other Finance Costs 23
PDC repayment 0
Loan repayment 0
PFI/Fin lease capital 3,139
B 7,460 B 168,825
Capital Service Cover A/B 1.11 Liquidity A*360/B 52
Category 1 Category 4
Continuity of Service Risk Rating 3

6
In terms of sensitivity analysis this forecast position could deteriorate by£24.4m before the Continuity of Service Risk Rating reduced to a ‘2’. Thisrepresents a significant level of tolerance to mitigate unplanned risks.
2.11 Summary
The Trusts financial position as at Quarter 3 is robust, with a Continuity ofService Risk Rating of 4. The Income & Expenditure position is ahead of planyear to date (largely due to non-recurrent issues) and revised capitalexpenditure is broadly on plan.
Forecasting ahead the Trust envisages maintaining an overall Continuity ofService Risk Rating of ‘3’ throughout the next 12 months, with significanttolerance. However, there are some real risks emerging in relation tocommissioning procurement exercises. The Trust is working through a detailedimpact analysis of the potential loss of contracts, but is confident it can managethe short term financial consequences.
The other key risks remain continued deliverability of sustainable CIP targetsand realistic capital investment plans.
The Board of Directors are asked to confirm that the board anticipates that theTrust will continue to maintain a Continuity of Service Risk Rating of at least 3over the next 12 months and sign the attached declaration.
3. GOVERNANCE DECLARATION
NHS Foundation Trust Boards must confirm that the board is satisfied thatplans in place are sufficient to ensure; on-going compliance with all existingtargets (after the application of thresholds) as set out in Appendix B of theCompliance Framework; and a commitment to comply with all known targetsgoing forwards.
No breach has been identified in any national target during Quarter 3 2014/15,for Leeds and York Partnership NHS Foundation Trust where thresholds havebeen published by Monitor. Plans are in place to ensure continued compliancewith all existing targets and all known targets going forward.
Plans are in place to continue to respond to the Care Quality Commission’sregulatory framework. It should be noted that the Trust self-assessment againstthe Information Governance Toolkit was “not satisfactory” as at 31st March2013. This is because of a weakness in the access controls for the CPDapplication (which is utilised by services in North Yorkshire and York) wasidentified; a full action plan is in place which mitigates the risk of non-compliance. The action plan includes a plan for York and North Yorkshireservices to be migrated to the ‘PARIS Vision’ system by the end of financialyear 2014/15. This assessment has led the Trust to review overall compliancewith CQC essential standards outcome 21, and declare yellow (outcome mostlymet), until the CPD application is replaced.

7
The Trust was inspected between 29 September and 5 October 2014 as part ofthe Care Quality Commission’s comprehensive inspection programme. Theinspection team looked at the Trust as a whole and in more detail at 11 coreservices including inpatient mental health wards and community-based mentalhealth, crisis response and learning disability services.
The Trust has been given an overall rating of “requires improvement”.
The Trust has been given five “compliance actions” by the CQC across theorganisation which means these are areas that require immediate attention toaddress essential standards of quality and safety. These include:
Safety and suitability of premises Systems for identifying, handling and responding to complaints Ensuring staff receive appropriate training, supervision and appraisals Ensuring there are enough suitably qualified, skilled and experienced staff
at all times to meet patients’ needs Eliminating mixed sex accommodation
The Trust has already taken action to address some of these concerns. Thisincludes:
Moving inpatient children’s mental health services in York into newlyrefurbished accommodation at Mill Lodge in Huntington
Working with staff at the Worsley Court elderly care unit in Selby to improvethe quality of nursing care – this unit has recently reopened following atemporary closure
Addressing mixed sex accommodation issues by designating Worsley Courtas a male-only facility and making the Meadowfields elderly inpatient unit inYork a female-only unit.
The CQC has set the Trust 19 “must do” actions and 23 “should do” actionsacross its clinical services. The Trust will now agree an action plan whichaddresses the key concerns highlighted in the report as its Trust Board meetingon 29 January 2015.
The implications of the Trust’s overall rating of “requires improvement” hasbeen discussed with Monitor and the Trust’s Governance Risk Rating will bemaintained as “Green”.
3.1 Monitor’s Quality Governance Framework
NHS Foundation Trust Boards must confirm that they are satisfied that, to thebest of their knowledge and using their own processes and having assessedagainst Monitor’s Quality Governance Framework (supported by Care QualityCommission information, its own information on serious incidents, patterns ofcomplaints, and including any further metrics it chooses to adopt), its NHSFoundation Trust has, and will keep in place, effective arrangements for thepurpose of monitoring and continually improving the quality of healthcareprovided to its patients.

8
The Board of Directors is asked to approve the signing of the in yearGovernance Declaration which is attached.
4. REPORTS ON ANY CHANGES TO THE BOARD OF DIRECTORS ANDCOUNCIL OF GOVERNORS
4.1 Changes to the Board of Directors
Executive Team
A competitive interview process took place in early November 2014 for the postof Director of Nursing although no substantive appointment was made;however, Anthony Deery continues in post as the Interim Director of Nursing.
The Nominations Committee will meet again to agree a process for this post tobe filled substantively.
Non-executive Team
During Quarter 3 of 2014/15 there have been no changes to the composition ofthe Non-executive Directors on the Board of Directors.
4.2 Changes to the Council of Governors
Elected Governors
Excluding the new governors listed below, during Quarter 3 there have beenthree other changes to the elected governors on the Council of Governors:
Paul Cockcroft: Staff, Non-clinical Leeds and York & North Yorkshirestepped down 14 October 2014
Jenny Roper: Public, Leeds stepped down on 31 December 2014 Karl Roberts: Public, York and North Yorkshire stepped down on the 8
January 2015
Appointed Governors
During Quarter 3 there was one change to the appointed governors on theCouncil of Governors:
• Cllr Helen Douglas, City of York Council stepped down on 25 October 2014
4.3 Elections concluded during Quarter 3 2014/15
On Friday 27 Novmember 2014 we concluded the latest round of elections toour Council of Governors. At the end of the election period the following peoplewere elected to our Council:
Karl Roberts: Public, York and North Yorkshire (elected unopposed)

9
Laura Phipp: Service User, York and North Yorkshire (elected unopposed) Libby Rowlands: Service User, York and North Yorkshire (elected
unopposed) Becky Oxley: Service User, Leeds (elected by ballot)
5. EXCEPTION REPORTS
NHS Foundation Trusts must report risks to compliance with the licence on anexception basis. Examples of these include:
Unplanned significant reductions in income or significant increases in costs Failure to comply with the NHS Foundation Trust Annual reporting Manual Significant third party investigations that suggest material issues with
governance Performance penalties to commissioners Outcomes or findings of Care Quality Commission responsive or planned
reviews. Patient Safety issues which may impact the Authorisation Enforcement notices from other bodies implying potential or actual
significant breach of any other requirement in the Authorisation
No matters have arisen in Quarter 3 2014/15 which require an exception reportto Monitor.
The Board of Directors is asked to confirm that there are no matters arising inthe quarter requiring an exception report to Monitor (per ComplianceFramework) which have not already been reported and sign the attacheddeclaration.

Worksheet "Governance Statement"
In Year Governance Statement from the Board of [MARSID]
The board are required to respond "Confirmed" or "Not confiirmed" to the following statements (see notes below)
For finance, that: Board Response
4
For governance, that:
11
Otherwise
Signed on behalf of the board of directors
Signature Signature
Name Name
Capacity [job title here] Capacity [job title here]
Date Date
3Notes:
A
B
C
The board anticipates that the trust will continue to maintain a continuity of service risk rating of at least 3 over the next 12 months.
The board is satisfied that plans in place are sufficient to ensure: ongoing compliance with all existing targets (after the application of
thresholds) as set out in Appendix A of the Risk Assessment Framework; and a commitment to comply with all known targets going
forwards.
The board confirms that there are no matters arising in the quarter requiring an exception report to Monitor (per Compliance
Monitor will accept either 1) electronic signatures pasted into this worksheet or 2) hand written signatures on a paper printout of this declaration
posted to Monitor to arrive by the submission deadline.In the event than an NHS foundation trust is unable to confirm these statements it should NOT select 'Confirmed’ in the relevant box. It must
provide a response (using the section below) explaining the reasons for the absence of a full certification and the action it proposes to take toThis may include include any significant prospective risks and concerns the foundation trust has in respect of delivering quality services and
effective quality governance.Monitor may adjust the relevant risk rating if there are significant issues arising and this may increase the frequency and intensity of monitoring for
the NHS foundation trust.
The board is unable to make one of more of the confirmations in the section above on this page and accordingly responds:

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Safer Staffing paper November and December 2014
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Anthony Deery, Interim Director ofNursing
STRATEGIC:
PAPER AUTHOR: Linda Rose, Assistant Director ofNursing GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)
G1 People achieve their agreed goals for improving health and improving lives
G2 People experience safe care
G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)
SO1 We provide excellent quality, evidence-based, safe care that involves people and promotesrecovery and wellbeing
SO2 We work with partners and local communities to improve health and lives
SO3 We value and develop our workforce and those supporting us
SO4 We provide efficient and sustainable services
SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individuals
Matters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
17

SUMMARY:
This is the standing report produced to monitor staffing capacity and capability. The Boardand services require assurance that staffing is sufficient to provide safe care.
Leeds and York Partnership NHS Foundation Trust (LYPFT) has a total of 37 Inpatient unitsand will report by exception any ward that achieves less than an 80% fill rate againstplanned staffing and highlight any exceptionally high fill rates.
RECOMMENDATIONS:
The Board of Directors is asked to
Receive the report and note the contents Discuss any issues raised by the content.

1
Report to the Board of Directors
Safer Staffing November and December 2014
1 Purpose
This paper forms the 7th monthly review of nurse staffing in line with the commitment and recommendations in the Hard Truths document, 2014. Ithas been produced to ensure that there is a clear system in place to monitor staffing capacity and capability.
This report and its narrative will also be published on the Trust’s website, and uploaded onto the relevant hospital webpage on NHS Choices.
LYPFT has previously reported on a total of 38 Inpatient units across Leeds and York.
This report excludes data from the older person’s unit Worsley Court, Selby as it remained temporarily closed through this reporting period andreopened on the 11
thJanuary 2015.
This data collection period covers two months: 1st
November to 30th
November 2014 and the 1st
December 2014 to the 31st
December 2014.
2 Updates
Millside Community Unit and Towngate House (Rehabilitation and recovery) closed on the 5 and the 6th
January respectively. They now operate as asingle unit at Asket Croft.
The new erostering system is going live on 26th
January 2015.
Workforce reviews are in progress.

2
3 Planned and actual staffing on a shift by shift basis reported to the Board of Directors
Any incidence of staffing reported at <80% of planned staffing continues to be noted as exception with a narrative summary of the reasons for the reportedexception.
In addition the requirement has been added to also note shifts that exceed a 120% fill rate. For this report exceptions apply to 33 of the 37 inpatient units.
November Unify Data
Hospital Name Hospital SiteCode
Ward Name Type Planned RegHours Day
Actual RegHours Day
PercentReg Day
Planned RegHours Night
Actual RegHours Night
Percent RegNight
ACOMB GARTH RGDT1 York - Recovery Unit AcombGables
HCW 1,323 955.52 72.22% 660 649 98.33%
Nursing
876 792.5 90.47% 352.5 352.5 100.00%
ASKET HOUSE RGDAP Asket House Inpatient HCW 897 765.5 85.34% 330 660.5 200.15%
Nursing
450 603.5 134.11% 330 331 100.30%
BECKLIN CENTRE RGDBL Becklin Ward 1 HCW 834 1,235 148.08% 660 781 118.33%
Nursing
1,278 900.5 70.46% 660 638 96.67%
Becklin Ward 3 HCW 813 1,066.51 131.18% 660 730 110.61%
Nursi 1,353 1,103.83 81.58% 660 632.5 95.83%
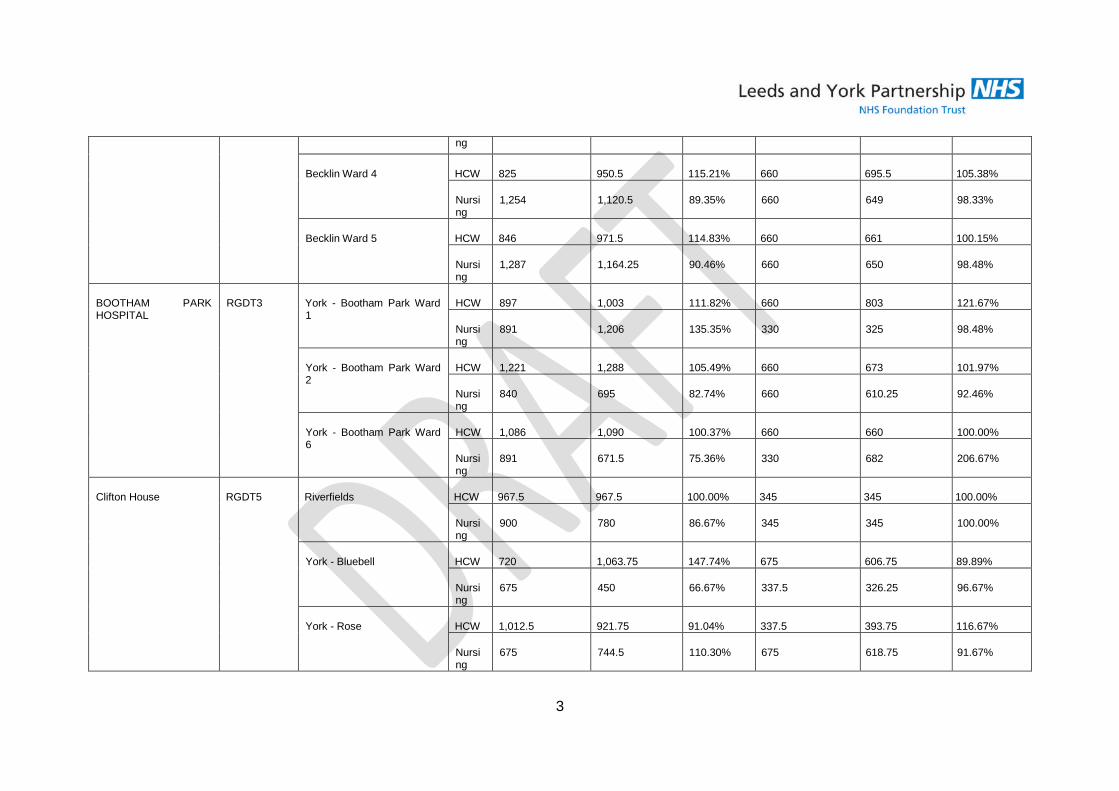
3
ng
Becklin Ward 4 HCW 825 950.5 115.21% 660 695.5 105.38%
Nursing
1,254 1,120.5 89.35% 660 649 98.33%
Becklin Ward 5 HCW 846 971.5 114.83% 660 661 100.15%
Nursing
1,287 1,164.25 90.46% 660 650 98.48%
BOOTHAM PARKHOSPITAL
RGDT3 York - Bootham Park Ward1
HCW 897 1,003 111.82% 660 803 121.67%
Nursing
891 1,206 135.35% 330 325 98.48%
York - Bootham Park Ward2
HCW 1,221 1,288 105.49% 660 673 101.97%
Nursing
840 695 82.74% 660 610.25 92.46%
York - Bootham Park Ward6
HCW 1,086 1,090 100.37% 660 660 100.00%
Nursing
891 671.5 75.36% 330 682 206.67%
Clifton House RGDT5 Riverfields HCW 967.5 967.5 100.00% 345 345 100.00%
Nursing
900 780 86.67% 345 345 100.00%
York - Bluebell HCW 720 1,063.75 147.74% 675 606.75 89.89%
Nursing
675 450 66.67% 337.5 326.25 96.67%
York - Rose HCW 1,012.5 921.75 91.04% 337.5 393.75 116.67%
Nursing
675 744.5 110.30% 675 618.75 91.67%

4
York - Westerdale HCW 843 1,762 209.02% 690 1,584 229.57%
Nursing
690 768.75 111.41% 345 391.25 113.41%
LEEDS GENERALINFIRMARY
RGD03 YCPM LGI HCW 240 562.5 234.38% 0 262.5 262.50%
Nursing
870 1,257.16 144.50% 630 634 100.63%
MEADOWFIELDS CUE RGDVC York - Meadowfields HCW 1,851 1,840.5 99.43% 690 713 103.33%
Nursing
810 1,135.25 140.15% 345 345 100.00%
MILLSIDE CUE RGD76 Millside Inpatient HCW 894 815.92 91.27% 330 337.75 102.35%
Nursing
450 536.49 119.22% 330 308 93.33%
NEWSAM CENTRE RGDAB Newsam Ward 1 PICU HCW 1,416 1,782 125.85% 660 1,195.5 181.14%
Nursing
1,284 981 76.40% 660 495 75.00%
Newsam Ward 2 Forensic HCW 828 1,095 132.25% 967.5 666.5 68.89%
Nursing
852 662 77.70% 322.5 354.75 110.00%
Newsam Ward 2 WomensServices
HCW 867 1,078 124.34% 322.5 526.75 163.33%
Nursing
867 812.5 93.71% 645 440.75 68.33%
Newsam Ward 3 HCW 882 987.5 111.96% 645 645 100.00%
Nursing
891 743 83.39% 408.5 322.5 78.95%
Newsam Ward 4 HCW 1,278 1,190 93.11% 660 712.5 107.95%

5
Nursing
1,044 904 86.59% 660 627 95.00%
Newsam Ward 5 HCW 1,293 1,319 102.01% 660 651.5 98.71%
Nursing
855 1,176 137.54% 660 650 98.48%
Newsam Ward 6 EDU HCW 900 1,166.99 129.67% 630 935.5 148.49%
Nursing
894 1,594.66 178.37% 315 443 140.63%
Oak Rise RGDT2 York - Oak Rise HCW 879 875.3 99.58% 645 645 100.00%
Nursing
882 1,087.81 123.33% 322.5 322.5 100.00%
PARKSIDE LODGE RGDPL Parkside Lodge HCW 1,323 1,977.67 149.48% 945 1,070.75 113.31%
Nursing
867 1,232 142.10% 315 356.25 113.10%
Peppermill Court RGDVG York - Peppermill Court HCW 2,013 979 48.63% 345 388.5 112.61%
Nursing
897 214.5 23.91% 345 391 113.33%
ST MARY'S HOSPITAL RGD17 2 Woodland Square HCW 669 698 104.33% 315 420 133.33%
Nursing
624 674 108.01% 315 315 100.00%
3 Woodland Square HCW 900 906.33 100.70% 315 472.5 150.00%
Nursing
450 348.5 77.44% 315 325.25 103.25%
THE MOUNT RGD05 Mother and Baby The Mount HCW 438 443 101.14% 330 473 143.33%
Nursi 894 821.5 91.89% 660 529.5 80.23%

6
ng
The Mount Ward 1 HCW 1,521 1,844.5 121.27% 967.5 1,333 137.78%
Nursing
1,155 1,036.5 89.74% 322.5 322.5 100.00%
The Mount Ward 2a HCW 1,494 2,049.5 137.18% 967.5 1,776.75 183.64%
Nursing
1,155 1,087.5 94.16% 322.5 322.5 100.00%
The Mount Ward 3a HCW 1,098 1,694.08 154.29% 660 1,001 151.67%
Nursing
897 937.99 104.57% 330 317.5 96.21%
The Mount Ward 4a HCW 1,557 1,907.92 122.54% 660 990.5 150.08%
Nursing
900 877.5 97.50% 330 330 100.00%
TOWNGATE HOUSE RGD75 Towngate Inpatient HCW 447 646.5 144.63% 630 630.58 100.09%
Nursing
480 552.58 115.12% 315 315 100.00%
WHITE HORSE VIEW RGDVA York - White Horse View HCW 1,791 1,592 88.89% 645 645 100.00%
Nursing
450 499 110.89% 322.5 323.75 100.39%
York - Fieldview RGDT8 York - Field View HCW 609 780 128.08% 345 218.5 63.33%
Nursing
658.5 430.5 65.38% 253 322 127.27%
YORK - LIME TREES(CAMHS)
RGDT9 York - Limetrees HCW 897 1,013.18 112.95% 352.5 341.58 96.90%
Nursing
750 919.75 122.63% 705 668 94.75%

7
December Unify Data
Hospital Name Hospital SiteCode
Ward Name Type Planned RegHours Day
Actual RegHours Day
PercentReg Day
Planned RegHours Night
Actual RegHours Night
Percent RegNight
ACOMB GARTH RGDT1 York - Recovery Unit AcombGables
HCW 1,374 986 71.76% 682 649 95.16%
Nursing
903 822.25 91.06% 364.25 360.5 98.97%
ASKET HOUSE RGDAP Asket House Inpatient HCW 924 757 81.93% 341 561 164.52%
Nursing
456 633.5 138.93% 341 341 100.00%
BECKLIN CENTRE RGDBL Becklin Ward 1 HCW 870 1,247 143.33% 682 761 111.58%
Nursing
1,359 1,034 76.09% 682 673.5 98.75%
Becklin Ward 3 HCW 847.5 1,057.75 124.81% 682 682 100.00%
Nursing
1,396.5 1,149 82.28% 682 671 98.39%
Becklin Ward 4 HCW 876 850.5 97.09% 682 748 109.68%
Nursing
1,281 1,260 98.36% 682 660 96.77%
Becklin Ward 5 HCW 894 1,015 113.53% 682 692.5 101.54%

8
Nursing
1,329 1,071.84 80.65% 682 660.5 96.85%
BOOTHAM PARKHOSPITAL
RGDT3 York - Bootham Park Ward1
HCW 915 944 103.17% 682 671 98.39%
Nursing
900 1,106.5 122.94% 341 396 116.13%
York - Bootham Park Ward2
HCW 1,272 1,364 107.23% 682 649 95.16%
Nursing
843 664 78.77% 682 605 88.71%
York - Bootham Park Ward6
HCW 1,129.5 1,122 99.34% 682 671 98.39%
Nursing
918 741 80.72% 341 703.5 206.30%
Clifton House RGDT5 York - Bluebell HCW 768.75 1,219.5 158.63% 697.5 742.5 106.45%
Nursing
712.5 681.75 95.68% 348.75 337.5 96.77%
York - Riverfields HCW 899 1,148 127.70% 356.5 782 219.35%
Nursing
502.5 728.5 144.98% 356.5 356.5 100.00%
York - Rose HCW 1,046.25 1,083.5 103.56% 348.75 583.75 167.38%
Nursing
697.5 920 131.90% 697.5 710.25 101.83%
York - Westerdale HCW 829.5 2,484.75 299.55% 713 2,354.5 330.22%
Nursing
768 701.5 91.34% 356.5 353.25 99.09%
LEEDS GENERALINFIRMARY
RGD03 YCPM LGI HCW 232.5 651.5 280.22% 325.5 294 90.32%
Nursi 1,371 1,218.92 88.91% 651 666.75 102.42%

9
ng
MEADOWFIELDS CUE RGDVC York - Meadowfields HCW 1,945.5 1,847.55 94.97% 713 621 87.10%
Nursing
825 1,359.75 164.82% 356.5 345 96.77%
MILLSIDE CUE RGD76 Millside Inpatient HCW 927 849.25 91.61% 341 343 100.59%
Nursing
462 523.67 113.35% 341 341 100.00%
NEWSAM CENTRE RGDAB Newsam Ward 1 PICU HCW 1,507.5 1,809 120.00% 682 1,062.5 155.79%
Nursing
1,323 1,137.5 85.98% 682 618 90.62%
Newsam Ward 2 Forensic HCW 882 1,066.5 120.92% 999.75 967.5 96.77%
Nursing
867 771 88.93% 333.25 365.5 109.68%
Newsam Ward 2 WomensServices
HCW 912 1,252 137.28% 333.25 515.75 154.76%
Nursing
912 752 82.46% 666.5 494.5 74.19%
Newsam Ward 3 HCW 924 1,129.5 122.24% 666.5 677.25 101.61%
Nursing
912 661 72.48% 333.25 333.25 100.00%
Newsam Ward 4 HCW 1,341 1,345 100.30% 682 748 109.68%
Nursing
1,099.5 936 85.13% 682 663 97.21%
Newsam Ward 5 HCW 1,353 1,591.83 117.65% 682 832 121.99%
Nursing
888 1,033.5 116.39% 682 656 96.19%

10
Newsam Ward 6 EDU HCW 918 949.5 103.43% 651 808.75 124.23%
Nursing
930 1,777.5 191.13% 325.5 409.5 125.81%
Oak Rise RGDT2 York - Oak Rise HCW 915 869.55 95.03% 666.5 664.25 99.66%
Nursing
915 1,113.52 121.70% 333.25 333.25 100.00%
PARKSIDE LODGE RGDPL Parkside Lodge HCW 1,350 2,072.92 153.55% 976.5 1,302 133.33%
Nursing
906 1,313 144.92% 325.5 325.5 100.00%
Peppermill Court RGDVG York - Peppermill Court HCW 2,053.5 1,821.25 88.69% 356.5 828 232.26%
Nursing
903 1,058.75 117.25% 356.5 506 141.94%
ST MARY'S HOSPITAL RGD17 2 Woodland Square HCW 694.5 564.5 81.28% 325.5 483 148.39%
Nursing
634.5 670.5 105.67% 325.5 304.5 93.55%
3 Woodland Square HCW 930 1,044.92 112.36% 325.5 514.5 158.06%
Nursing
465 512 110.11% 325.5 315 96.77%
THE MOUNT RGD05 Mother and Baby The Mount HCW 462 419 90.69% 341 583 170.97%
Nursing
903 747.25 82.75% 682 429.5 62.98%
The Mount Ward 1 HCW 1,563 1,731.97 110.81% 999.75 1,161 116.13%
Nursing
1,194 1,107.5 92.76% 333.25 344 103.23%
The Mount Ward 2a HCW 1,557 1,937.5 124.44% 999.75 1,421 142.14%

11
Nursing
1,200 1,167 97.25% 333.25 333.25 100.00%
The Mount Ward 3a HCW 1,138.5 1,641.5 144.18% 682 1,001 146.77%
Nursing
921 1,008.67 109.52% 341 342 100.29%
The Mount Ward 4a HCW 1,606.5 1,882.1 117.16% 682 977 143.26%
Nursing
927 922.18 99.48% 341 341 100.00%
TOWNGATE HOUSE RGD75 Towngate Inpatient HCW 459 529.17 115.29% 651 602.25 92.51%
Nursing
495 594.5 120.10% 325.5 325.5 100.00%
WHITE HORSE VIEW RGDVA York - White Horse View HCW 1,860 1,686.75 90.69% 666.5 666.5 100.00%
Nursing
462 508.25 110.01% 333.25 344 103.23%
York - Fieldview RGDT8 York - Field View HCW 555 742.5 133.78% 356.5 322 90.32%
Nursing
549 432.25 78.73% 356.5 345 96.77%
YORK - LIME TREES(CAMHS)
RGDT9 York - Limetrees HCW 930 870.16 93.57% 364.25 365.25 100.27%
Nursing
801 1,137.02 141.95% 728.5 706.83 97.03%

12
Hospital Name Hospital Site Code Ward Name Type Planned Reg HoursDay
Actual Reg HoursDay
Percent RegDay
Planned Reg HoursNight
Actual Reg HoursNight
Percent RegNight
ACOMB GARTH RGDT1 York -RecoveryUnit AcombGables
HCW 1,374 986 71.76% 682 649 95.16%
Nursing 903 822.25 91.06% 364.25 360.5 98.97%
ASKET HOUSE RGDAP Asket HouseInpatient
HCW 924 757 81.93% 341 561 164.52%
Nursing 456 633.5 138.93% 341 341 100.00%
BECKLINCENTRE
RGDBL Becklin Ward1
HCW 870 1,247 143.33% 682 761 111.58%
Nursing 1,359 1,034 76.09% 682 673.5 98.75%
Becklin Ward3
HCW 847.5 1,057.75 124.81% 682 682 100.00%
Nursing 1,396.5 1,149 82.28% 682 671 98.39%
Becklin Ward4
HCW 876 850.5 97.09% 682 748 109.68%
Nursing 1,281 1,260 98.36% 682 660 96.77%
Becklin Ward5
HCW 894 1,015 113.53% 682 692.5 101.54%
Nursing 1,329 1,071.84 80.65% 682 660.5 96.85%
BOOTHAMPARKHOSPITAL
RGDT3 York -BoothamPark Ward 1
HCW 915 944 103.17% 682 671 98.39%
Nursing 900 1,106.5 122.94% 341 396 116.13%
York -BoothamPark Ward 2
HCW 1,272 1,364 107.23% 682 649 95.16%
Nursing 843 664 78.77% 682 605 88.71%
York -BoothamPark Ward 6
HCW 1,129.5 1,122 99.34% 682 671 98.39%
Nursing 918 741 80.72% 341 703.5 206.30%
Clifton House RGDT5 York - HCW 768.75 1,219.5 158.63% 697.5 742.5 106.45%
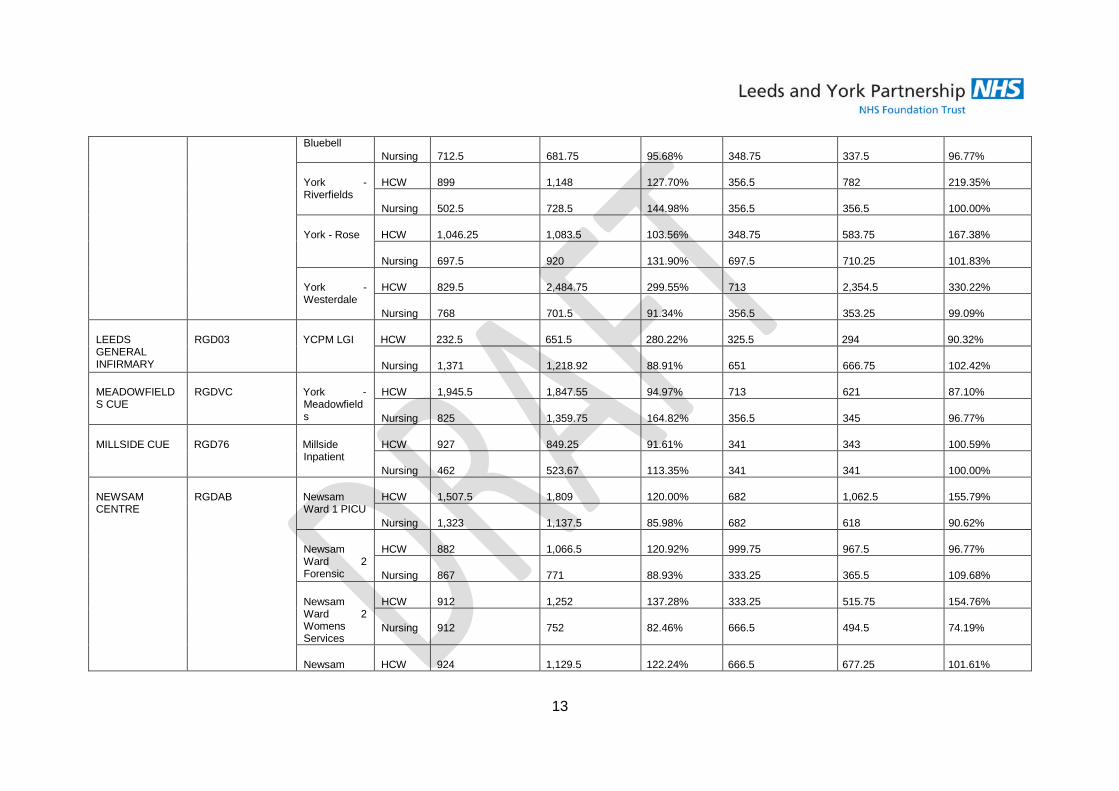
13
BluebellNursing 712.5 681.75 95.68% 348.75 337.5 96.77%
York -Riverfields
HCW 899 1,148 127.70% 356.5 782 219.35%
Nursing 502.5 728.5 144.98% 356.5 356.5 100.00%
York - Rose HCW 1,046.25 1,083.5 103.56% 348.75 583.75 167.38%
Nursing 697.5 920 131.90% 697.5 710.25 101.83%
York -Westerdale
HCW 829.5 2,484.75 299.55% 713 2,354.5 330.22%
Nursing 768 701.5 91.34% 356.5 353.25 99.09%
LEEDSGENERALINFIRMARY
RGD03 YCPM LGI HCW 232.5 651.5 280.22% 325.5 294 90.32%
Nursing 1,371 1,218.92 88.91% 651 666.75 102.42%
MEADOWFIELDS CUE
RGDVC York -Meadowfields
HCW 1,945.5 1,847.55 94.97% 713 621 87.10%
Nursing 825 1,359.75 164.82% 356.5 345 96.77%
MILLSIDE CUE RGD76 MillsideInpatient
HCW 927 849.25 91.61% 341 343 100.59%
Nursing 462 523.67 113.35% 341 341 100.00%
NEWSAMCENTRE
RGDAB NewsamWard 1 PICU
HCW 1,507.5 1,809 120.00% 682 1,062.5 155.79%
Nursing 1,323 1,137.5 85.98% 682 618 90.62%
NewsamWard 2Forensic
HCW 882 1,066.5 120.92% 999.75 967.5 96.77%
Nursing 867 771 88.93% 333.25 365.5 109.68%
NewsamWard 2WomensServices
HCW 912 1,252 137.28% 333.25 515.75 154.76%
Nursing 912 752 82.46% 666.5 494.5 74.19%
Newsam HCW 924 1,129.5 122.24% 666.5 677.25 101.61%

14
Ward 3Nursing 912 661 72.48% 333.25 333.25 100.00%
NewsamWard 4
HCW 1,341 1,345 100.30% 682 748 109.68%
Nursing 1,099.5 936 85.13% 682 663 97.21%
NewsamWard 5
HCW 1,353 1,591.83 117.65% 682 832 121.99%
Nursing 888 1,033.5 116.39% 682 656 96.19%
NewsamWard 6 EDU
HCW 918 949.5 103.43% 651 808.75 124.23%
Nursing 930 1,777.5 191.13% 325.5 409.5 125.81%
Oak Rise RGDT2 York - OakRise
HCW 915 869.55 95.03% 666.5 664.25 99.66%
Nursing 915 1,113.52 121.70% 333.25 333.25 100.00%
PARKSIDELODGE
RGDPL ParksideLodge
HCW 1,350 2,072.92 153.55% 976.5 1,302 133.33%
Nursing 906 1,313 144.92% 325.5 325.5 100.00%
Peppermill Court RGDVG York -PeppermillCourt
HCW 2,053.5 1,821.25 88.69% 356.5 828 232.26%
Nursing 903 1,058.75 117.25% 356.5 506 141.94%
ST MARY'SHOSPITAL
RGD17 2 WoodlandSquare
HCW 694.5 564.5 81.28% 325.5 483 148.39%
Nursing 634.5 670.5 105.67% 325.5 304.5 93.55%
3 WoodlandSquare
HCW 930 1,044.92 112.36% 325.5 514.5 158.06%
Nursing 465 512 110.11% 325.5 315 96.77%
THE MOUNT RGD05 Mother andBaby TheMount
HCW 462 419 90.69% 341 583 170.97%
Nursing 903 747.25 82.75% 682 429.5 62.98%
The Mount HCW 1,563 1,731.97 110.81% 999.75 1,161 116.13%
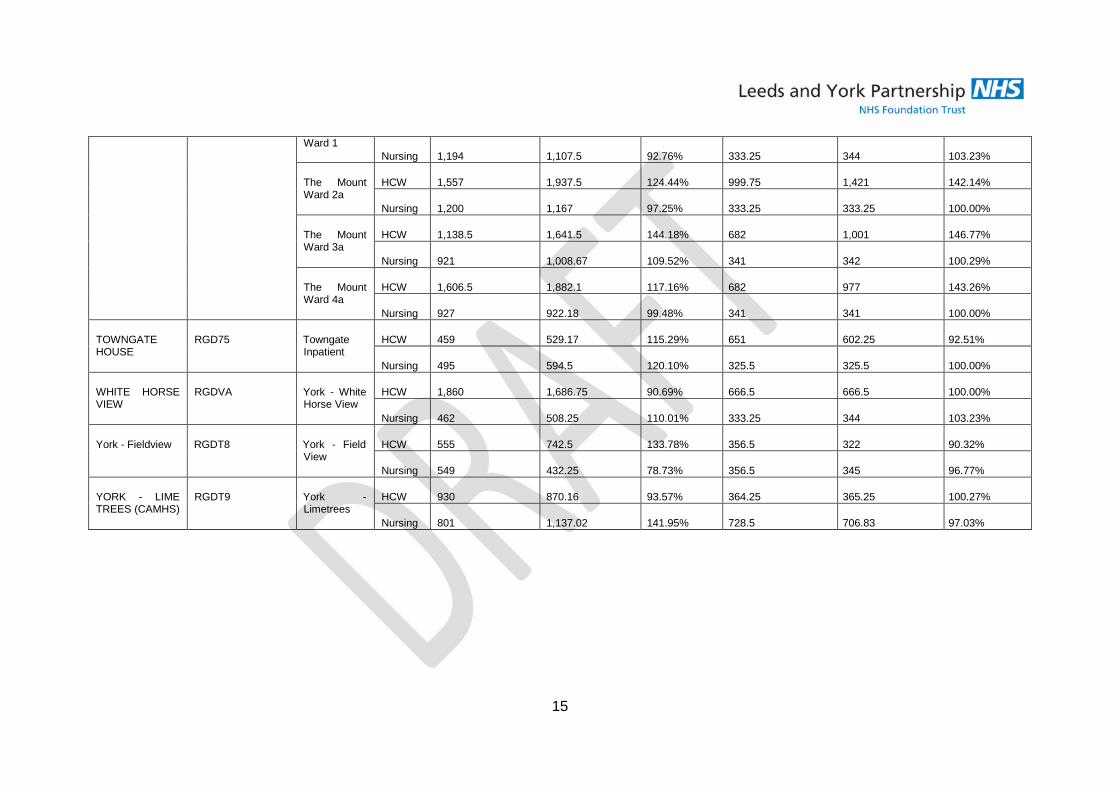
15
Ward 1Nursing 1,194 1,107.5 92.76% 333.25 344 103.23%
The MountWard 2a
HCW 1,557 1,937.5 124.44% 999.75 1,421 142.14%
Nursing 1,200 1,167 97.25% 333.25 333.25 100.00%
The MountWard 3a
HCW 1,138.5 1,641.5 144.18% 682 1,001 146.77%
Nursing 921 1,008.67 109.52% 341 342 100.29%
The MountWard 4a
HCW 1,606.5 1,882.1 117.16% 682 977 143.26%
Nursing 927 922.18 99.48% 341 341 100.00%
TOWNGATEHOUSE
RGD75 TowngateInpatient
HCW 459 529.17 115.29% 651 602.25 92.51%
Nursing 495 594.5 120.10% 325.5 325.5 100.00%
WHITE HORSEVIEW
RGDVA York - WhiteHorse View
HCW 1,860 1,686.75 90.69% 666.5 666.5 100.00%
Nursing 462 508.25 110.01% 333.25 344 103.23%
York - Fieldview RGDT8 York - FieldView
HCW 555 742.5 133.78% 356.5 322 90.32%
Nursing 549 432.25 78.73% 356.5 345 96.77%
YORK - LIMETREES (CAMHS)
RGDT9 York -Limetrees
HCW 930 870.16 93.57% 364.25 365.25 100.27%
Nursing 801 1,137.02 141.95% 728.5 706.83 97.03%

16
Leeds Mental Health Care Group
Asket House (Rehabilitation and Recovery Service)
The report shows a Health support worker fill rate of 200.15% during the night in November 2014 and a Registered Nurse fill rate of 134.11% during the day.This unit is funded for two members of staff at night but a third staff member was required to meet clinical demand as an exception. The Registered Nurseover compliment has now been reviewed in line with the R&R service review.
In the December 2014 reporting period the Health support worker fill rate at night is 164.52% and the Registered Nurse fill rate during the day is 138.93%.
The erostering team created new rosters for the newly opened (5 January2015) Asket Croft R&R Service in November. This may have created duplication asthe paper rosters indicate that minimum staffing levels maintained throughout all of December.
Newsam Ward 5 (Secure Rehabilitation and Recovery Service)
The report shows a Registered Nurse fill rate of 137.54% during the day in November 2014. The new ward manager has confirmed that a review of theeroster template is required to accurately reflect staffing levels. This has been arranged with the eroster team, Ward manager and Band 6 staff.
Towngate House (Rehabilitation and Recovery Service)
The report shows a Health support worker fill rate of 144.63% during the day in November 2014.A contributory factor to the increase in hours is in response toa service user being cared for on within eyesight observations who also required support from two staff for hourly personal care.
Towngate House closed on the 6th
January 2015 (Millside on the 5th
January 2015) and now both function at Asket Croft.
Becklin Ward 1 (Female acute inpatient service)
The report shows a Health support worker fill rate of 148.08% during the day and a Registered Nurse fill rate of 70.46% during the day in November 2014.
The December 2014 report shows a Health support worker fill rate during the day of 142.47% and a Registered Nurse fill rate during the day of 76.09%.
The exceptions relate to the adjusting of skill mix in response to Registered Nurse vacancy and sickness. Acuity in relation to management of ECT patient andincreased within eyesight observations was also a contributory factor. The low Registered Nurse fill rate is not an indication of non-compliance with having aRegistered Nurse on duty, but a reflection of the amendment required for the eroster template.

17
Becklin Ward 3 (Male acute inpatient service)
The report shows a Health support worker fill rate of 131.18% during the day in November 2014. The service has confirmed that this was in response tomanaging two patients on within eyesight observations.
In December 2014 the Health Support worker fill rate during the day is 124.81%. The increase is in response to acuity and clinical need.
Becklin ward 5 (Female acute inpatient service)
In November 2014 the health support worker fill rate during the day was 148.08%. The Registered nurse fill during the day was 70.46 %.
The increase in Health support worker hours has been confirmed as a response to acuity and clinical need. There was no shift without Registered Nursecover. The underfill reflects the amendment required on the erostering template.
Newsam Ward 1 (Psychiatric intensive care unit)
The report shows a Health support worker fill rate of 125.85% during the day in November 2014 and 181.14% during the night. The Registered Nurse fill rateduring the day in November 2014 was 76.40% during the day and 75.00% during the night. The service has confirmed that the increase in the use of Healthsupport workers supplemented the Registered Nurse shortage, but there was no occasion when there was not registered Nurse on duty. The RegisteredNurse shortage related to sickness and graded returns. This area also had two staff members who were not included in the staffing numbers (supernumery)due to temporary PMVA role restriction.
The December 2014 report shows a Health support worker fill rate of 155.79% at night. This service has described having a clinical situation where they wererequired to provide staff for each shift, to look after a patient at St James’s Hospital, in addition to providing staffing on ward 1 Newsam for patients on levelsof observation.
Mount Ward 1 (OPS Dementia care)
The report shows a Health support worker fill rate of 121.27% during the day in November 2014 and 137.78% during the night. This is in response to clinicalneed and a sickness rate of 6.47%. For the entirety of November there were a minimum 2 patients on within eyesight observations and this rose to x3patients for five days during this period.

18
Mount Ward 2 (OPS Dementia care)
The report shows a Health support worker fill rate of 137.18% during the day in November 2014 and 183.64% during the night. The service has confirmed anincrease in clinical need (within eyesight observations); escorting service users to LTHT; occupancy of 95% and sickness at 13%.
During December 2014 the Health support worker fill rate during the day is 122.44% and 142.14% at night. This is a similar position to the previous month inthat Ward 2 averaged out at 1 patient on within eyesight/arm’s length observations on any given shift and some of this was escorted at LTHT. Othercontributory factors are that occupancy ran at approx. 95% and sickness increased to 14%.
Mount Ward 3 (OPS Mental health)
The report shows a Health support worker fill rate of 154.29% during the day in November and 151.67% at night. The service has confirmed that this is inrelation to increased acuity and complex physical health needs.
During December 2014 the Health support worker fill rate during the day is 144.18% and 146.77% at night. As previously discussed Health support workerstaffing numbers are raised in response to on-going high acuity and complex physical care needs.
Mount ward 4 (OPS Mental health)
The report shows a Health support worker fill rate of 122.54% during the day in November 2014 and 150.00% at night.
During December the Health support worker fill rate at night is 143.26%.
The high percentage increase in use of Health support workers is due to an increase of patients on within eyesight level of observations and 10 to 15 minuteintermittent observations. The number of patients requiring physical care and physical observations also increased. A further contributory factor was a highlevel of staff sickness during December.
York and North Yorkshire Mental Health Care Group
Bootham Ward 1 (Female acute Inpatient Service)
The report shows a Health support worker fill rate of 121.67% during the night in November 2014 and a Registered Nurse fill rate of 135.35% during the day.The service has confirmed that this is in response to high acuity levels and increased within eyesight observations.

19
During December 2014 the Registered Nurse fill rate during the day is 122.94%. This service reports high acuity throughout the month and back filling ofshifts for RN’s involved in a tragic incident on the ward. Extra Registered Nurses were brought in to facilitate special leave for these staff members.
Bootham Ward 2 (Male acute inpatient service)
During December 2014 the Registered Nurse fill rate during the day is 78.77%. There was no occasion where there was no Registered Nurse cover howeverthere occasions where there was only had one qualified nurse on shift instead of two.
Bootham Ward 6 (OPS assessment unit)
The report shows a Registered Nurse fill rate of 75.36% during the day in November 2104 and a Registered Nurse fill rate of 206.67% during the night. Theservice has confirmed that the shortfall during the day is in relation to sickness, maternity leave and training but all shifts have been covered by a RegisteredNurse. There is also an on-going request for a second Registered Nurse (over budget spend) to provide cover across service as required at night, howeverthis is billed to Ward 6 as instructed by the Management Team.
During December 2014 the Registered Nurse fill rate during the night is 206.30% and again this is accounted for via the operational and managerialagreement to have a second registered nurse to provide response cover across the service.
Acomb Garth (Rehab and recovery CUE)
The report shows a Health support worker fill rate of 72.22% during the day in November 2014. This service has confirmed that there was an excess ofannual leave authorised for this group of staff.
The report shows a Health support worker fill rate of 71.6% during the day in December 2014. Allocated numbers were on all shifts but there is a discrepancywith the availability of extra shifts which are not being used. This will be amended on the template with the eroster team.
Meadowfields (CUE)
The report shows a Registered Nurse fill rate of 140.15% during the day in November 2014. During December 2014 the report shows a Registered Nurse fillrate of 164.8% during the day.
This service has a long day shift pattern which accounts for one Registered nurse filling 6 shifts per week as opposed to the usual five. In addition there wereperiods when Registered Nurses backfilled for Health support worker absence. Long days will be reflected in the review of the template.

20
Specialist and Learning Disabilities Care Group
Bluebell Ward (Forensic service)
The report shows a Health support worker fill rate of 147.74% during the day in November 2014 and a Registered Nurse fill rate of 66.67% during the day.One Registered Nurse is not accounted for in the numbers as she is currently supernumery as a newly employed Preceptee. There is also a band 6 vacancy.
Additional Health support worker hours have been engaged to support the Registered Nurse gap in hours. All duties in November were covered with a
Registered Nurse on duty.
During December 2014 the report shows a Health support worker fill rate during the day of 162.54%. The additional hours again have been used to fill theRegistered Nurse vacancy.
This service has also report no Registered Nurse cover on the night of the 20th
December 2014 due to sickness unavailability. The service put a request outto Bank on the 19
thDecember 2014 and attended all wards at Clifton House to seek cover- including offering overtime. Two Agencies were then contacted
but neither could fill the shift. The ward was covered with a registered Nurse from Rose ward to administer 2200hrs medication and the Charge Nurse onRiverfields provided supported to the staff on duty during the rest of the night. The risks on Blue bell ward were assessed as low at this time. The issue wasescalated to the Matron.
Rose Ward (Forensic service)
During December 2014 the report shows a health support worker fill of 167.38% during the night and a Registered Nurse fill rate of 131.90% during the day.The increase in clinical activity is attributed to an increase in self-harming and the use of use of seclusion over the Christmas period. The increase inRegistered Nurse hours is due to no sickness or annual leave being taken during this period.
Westerdale Ward (Forensic service)
The report shows a Health support worker fill rate of 209.02% during the day in November 2014 and 229.57% during the night. The service has confirmedthat this reflects significant levels of seclusion and special observations running concurrently.
During December 2014 the report shows a Health support worker fill rate of 297.80% during the day and a Health support worker fill rate of 330.22% duringthe night. Westerdale report exceptional levels of both seclusion and within eyesight / within arm’s reach observations throughout December culminating inhigh Health support worker fill rates. This was this escalated through to the Matron, Associate Director and Clinical Directors. This was a particularly difficultperiod for the service.

21
Fieldview (Forensic service)
The report shows a Health support worker fill rate of 128.08% during the day and 63.33% at night. There is a discrepancy with the agreed figures but theservice has confirmed that staff were loaned to cover Westerdale Ward and that there were 3.5 hours which were not covered by a Registered Nurse. AHealth support worker was in phone contact with a Registered Nurse at Clifton House for this period until a Registered Nurse arrived. The Erostering teamhave confirmed the template and timing issue has been corrected for this service report.
During December 2014 The Registered Nurse fill rate during the day is 78.73% and the Health support worker fill rate is 133.78%. All shifts in December werecovered with qualified staff and Health support workers only worked their contracted hours. The figures provided by the erostering require templateadjustment.
Riverfields (Forensic service)
The December 2014 report shows a Health support worker fill of 127.7% hours during the day and 219.35% during the night. Registered Nurse fill during theday is 144.98%.
This area also has template issues that are contributing the credibility of the reported numbers. This is currently being adjusted.
4-6 Oak Rise (LD Acute assessment and treatment)
The report shows a Registered nurse fill rate of 123.33% during the day in November 2014. The service has confirmed that this in in response to increasedacuity and having x3 service users on within eyesight observations.
Peppermill Court (OPS Challenging behaviour unit)
The report shows a Health support worker fill rate of 48.63% during the day in November 2014 and a Registered Nurse fill rate of 23.91% during the day. Thisservice confirmed that all shifts were covered by a Registered Nurse but that they are actively recruiting to x6 Band 5 Vacancies. The numbers do not reflectan accurate picture of staffing as there has been an issue with data collection for this service.

22
Parkside Lodge (LD Acute assessment and treatment)
The report shows a Health support worker fill rate of 149.48% during the day in November 2014 and a Registered Nurse fill rate of 142.10% during the day.This area has confirmed that staffing reflects levels of acuity on the ward necessitating increased staffing levels to facilitate safe observations for patientsrequiring enhanced obs (e.g. 1:1; and 2:1 for community activity). Staff are also flexibly deployed across 3 Woodland square to cover acuity when the needarises as these teams are managed within one larger team.
Similarly in December 2014 the report shows a Registered Nurse fill rate during the day of 144.92%. in response to the level of acuity on the ward. The
Health support worker fill of 153.55% during the day and 133.33% during the night has been provided to facilitate safe care for patients requiring enhancedobservations. Parkside is an isolated unit and higher staffing levels are required to respond to any incidents that occur to maintain safety of patients andothers.
2 Woodland Square (LD Respite for complex physical health)
The report shows a Health support worker fill of 133.33% during the night in November 2014. The service has confirmed that this is in response to a clientbeing cared for on within eyesight observations.
The December 2014 report also reflects clinical need with a Health support worker fill rate of 148.39% at night.
3 Woodland Square (LD Continuing Care and rehabilitation / health respite)
The report shows a health support worker fill of 150.00% during the night in November 2014 and a Registered Nurse fill of 77.44% during the day. The nighthours reflects occupancy within the respite service and the need for 3 night staff as opposed to the established 2. The Registered Nurse fill reflects thevacancy factor. Recruitment process has yielded additional staff. Staff are deployed across this unit and Parkside Lodge.
During December 2014 the Health support worker fill rate at night is 158.06%. Contributory factors to over establishment during this period is annual leave isnot sanctioned over Christmas and New Year weeks except for exceptional circumstances; and also in response to clinical need as the profile of the serviceuser group in respite is changing.
Newsam Ward 2 (Forensic male)
The report shows a Health Support Worker fill rate of 132.25% during the day in November 2014 and 68.89% during the night. The Registered Nurse fill rateis 77.70% during the day. There were two occasions where there was no Registered Nurse on duty but both duties were filled by a Registered Nurse fromWard 2N(f). The shortfall of Registered Nurse hours was also covered by an increase in health support worker hours. On-going vacancies and long termsickness continue to be contributory factors and are being managed.

23
Newsam 2 (Forensic female)
The report shows a Health Support Worker fill rate of 124.34% during the day in November 2014 and 163.33% during the night. The Registered Nurse fill rateis 68.33% during the day. There are no reports of shifts without a registered Nurse on duty but the shortfall is accounted for by one Registered Nurse beingon duty where they are established for two. Registered nurse hours have been backfilled by Health support workers on day and night duties.
The December 2014 report shows the Health support worker fill rate during the day as 137.28% and 154.76% during the night. The Registered Nurse fill rateat night was 74.19%. The increase in health support workers is backfill for Registered Nurse hours. All duties were covered by a Registered Nurse. On-going
vacancies and long term sickness continue to be contributory factors and are being managed.
Newsam Ward 3 (Forensic)
The report shows a Registered Nurse fill rate of 78.95% during the night in November 2014.The service has confirmed that all shifts were covered with aRegistered Nurse.
The December 2014 report shows a Registered Nurse fill rate of 72.48% during the day. The service has confirmed that all shifts were staffed with at leastone qualified nurse but have two vacant Registered Nurse posts.
Newsam Ward 6
The report shows a Health support worker fill rate of 129.67% during the day in November 2014 and 148.49% during the night.The report also shows a registered Nurse fill rate of 178.37% during the day in November 2014 and 140.63% during the night.The service has confirmed that higher staffing levels are in response to increased acuity in terms of users of the service requiring staffing of 2:1; staff onrestricted duties and all service users on naso gastric feeding requiring within eyesight observations whilst feeds are running.
The December 2014 report shows a Registered Nurse fill rate of 191.13% during the day and 125.81% during the night. The Health support worker fill duringthe night is 124.23%. The service has confirmed that the increase remains due to 2 patients needing within eyesight / within arm’s reach levels of observation(including one patient nursed at a ratio of 2:1). A health support worker is also on maternity leave.
Ward 5 Mount (Perinatal)
The report shows a Health support worker fill of 143.33% during the night in November 2014. The service has confirmed that vacant Registered nurse postswere backfilled with Health support worker staff that knew the unit to ensure safe care for mothers and infants. This was due to clinical need and increasedobservations.

24
In December 2014 the Health support worker fill rate during the night is 170.97% and the Registered Nurse fill rate at night is 62.98%. Of the 4.6 RMNvacancies in this service, 3.6 were successfully recruited into in December and are awaiting H/R clearance. Sickness absence in December was also acontributory factor in December as a result of a sickness bug. The high Health support worker fill rate is as a result of backfilling some of the vacantRegistered Nurse hours. All shifts were covered with a Registered Nurse.
YCPM (Ward 40 LGI)
The report shows a Health support worker fill rate of 234.38% during the day in November 2014 and 262.50% during the night. The report also shows aRegistered Nurse fill rate of 144.50% during the day.
During the month of December 2014 the report shows Health Support Worker hours of 280.22% during the day.
The fill rates are affected by increased recruitment - new posts for health care support worker (2.5 WTE) and Band 5 nurses (3.0 WTE) over the year and toincreased patient need over this period also. The templates have not yet been updated to reflect these changes.
Limetrees (Camhs)
The report shows a Registered Nurse fill rate of 122.63% during the day in November 2014. The service has confirmed that there are template issues whichwill be picked up with the erostering team.
In December 2014 the Registered Nurse fill rate during the day is 137.89%. Awaiting response from this service in regards to the context.
4. Benefits / Risks
The National Institute for Health and Care Excellence (NICE) has developed safe staffing guidance (July 2014). However this covers adult inpatient wards inacute hospitals only.
Mental health is still without an evidenced based tool to support workforce reviews but work is in progress with NICE in terms of scoping the framework formental health settings. Consultation on the draft guidance is due October 2015 and expected date of issue is October 2015.
Of benefit in terms of the 6 monthly workforce reviews all care groups have gone through the process of reviewing staffing in terms of CIP’s, quality andservice requirements and have provided assurance of this work. The revised profiles are being directly signed off through the management teams firstly and

25
then will be escalated through to the Director of Nursing for assurance. The reviews and supporting information will be stored centrally in a shared folderaccessible to Executives, Non-executives and Directors.
We know from data collection and workforce reviews that the that the erostering templates are not yet where we require them to be and this will beprogressed through version 10 erostering training in conjunction with every inpatient Ward manager and Matron. Getting the establishments right will ensurethat we are not using bank or agency staff to cover annual leave and provide further assurance of a rigorous process in terms of going outside of fundedestablishments. The benefits of version 10 erostering will have a positive impact on data accuracy and management of staffing from April 2015.
Acuity and clinical need features as a theme in many of the exception reports where staffing is over the 100% -making reference to increased observations.We know that for most areas this happens when the establishment has to manage more than one patient with this need at the same time. We also know thatwhere the staffing establishment at night is funded for two staff the only option is to go outside of the funded establishment. In a number of cases wherestaffing appears to be under filled and overfilled there is also evidence that the eroster templates are the issue.
The safe staffing escalation process has been clearly defined and agreed by all Matrons for every inpatient area. The Assistant Director of Nursing hascommunicated to senior operational leads that the escalation process must also be publicised and disseminated to all relevant staff. In addition, the escalationprocess for each area will be added to the on call folder as an aide for on call managers.
5. Next steps
The 26th
January will see the implementation of the new V.10 rostering system.
Between 2nd
February and 1st
April, every manager in the inpatient safe-staffing group will have their roster recalibrated with:
Accurate budgeted establishment. Removal of optional duties. 17% annual leave tolerance activated. Bespoke Auto-Roster facility for each unit manager.
The eroster system currently has an additional duties function. In order to graduate the implementation of the new process for requesting duties outside of thebudgeted establishment, additional duty activity will be monitored by the erostering team from the 2
ndFeb – 1
stApril. On the 1st April a report will be run to
accurately determine how many duties have been requested over and above the budgeted establishment across all areas of the organisation.
This will give us some indication of how many, and to what extent managers are looking outside their budgets to staff clinical areas. It will also serve todetermine the extra resource demand.

26
6. RecommendationsThe Board are asked to receive the report for information and to note the work that is taking place to review ward nursing establishments and the
corresponding actions that are taking place with erostering version 10 training and management to improve nurse staffing .
Linda RoseAssistant Director of Nursing21
stJanuary 2015

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Complaints Summary Report
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Anthony Deery, Director of NursingSTRATEGIC:
PAPER AUTHOR: Melanie Hird, Head of ClinicalGovernance
GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)
G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)
SO1 We provide excellent quality, evidence-based, safe care that involves people and promotesrecovery and wellbeing
SO2 We work with partners and local communities to improve health and lives SO3 We value and develop our workforce and those supporting us
SO4 We provide efficient and sustainable services
SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individuals
Matters exempt under the Freedom of Information Act (quote section number)
SUMMARY:This is the quarterly report on complaints to the Board of Directors. It includes a summaryof the changes we are making to the complaints management process; together withexpected benefits
AGENDAITEM
18

RECOMMENDATIONS:The Board is asked to:
note the content of the attached report; be assured of the actions taken to improve the complaints procedure and that these
are being progressed appropriately.
Complaints Report
January 2015

Page 1 of 5
1. Introduction
This report provides a summary of complaints data year to date to the Board of Directors. Thisis produced on a quarterly basis, with a brief summary provided monthly. In addition, asummary of the changes we are making to the complaints management process is included;together with expected benefits.
2. Number of complaints received
The table below shows numbers of complaints received each quarter in 2014, by care group.From Q3 we are also measuring numbers of reactivated complaints. New complaints receivedin December (7) were significantly lower than November (29) and lower than the meanaverage.
2014 Q1 Q2 Q3 Year to dateLeeds Care Group 27 42 27 96York Care Group 9 17 14 40Specialist and LD Care Group 10 4 8 22Total: 46 63 49 158
Table 1: numbers of complaints received April – December 2014
3. Response times
The chart below shows numbers of complaints closed each month in 2014, by care group.
Chart 1: Complaints responses (April to December 2014)

Page 2 of 5
Quarter 3 performance overall is disappointing. In October we did not meet the 30 dayresponse standard for any closed complaints, the main delay point being the time taken forcare groups to return the draft response to the complaints team (in 14 of 15 cases). InNovember and December performance improved and we achieved our 30-day standard in50% of responses.
Following a review of capacity within the complaints team, additional resource will be madeavailable for a fixed term (initially 12 months) to improve performance. Further detail is givenin section 8.
4. Complaints acknowledgement letters
We continue to achieve 100% response rate in sending acknowledgement letters within 3working days, which is a regulatory requirement. It is important to note that this is the onlystandard set in regulation; other standards are locally set.
Chart 2: complaint acknowledgement timescales
5. Number of Complaints Upheld
Table 2 shows outcomes of closed complaints by quarter.
Outcome Q1 Q2 Q3 Year todate
Upheld 5 7 21 33Partially upheld 8 4 1 13Not upheld 23 29 25 77Total: 36 40 47 123
Table 2
0%
20%
40%
60%
80%
100%
Q1 Q2 Q3 YTD
Complaint AcknowledgementTimescales 2014
On Time
1 day over
2 days over

Page 3 of 5
6. Themes
We have reviewed the way in which we capture themes from complaints, moving away fromsix broad themes to a larger number of more specific themes. Main themes year to date areshown in table 3 below.
Issues with clinical care and treatment continue to be the highest rated theme. Staff attitude isalso a consistently high factor in complaints received. The Head of Clinical Governance isworking with the Head of Organisational Development and the Head of Learning and PeopleDevelopment to link training for complaints investigators and values-based customer caretraining for the wider workforce.
Q1 Q2 Q3 Ytd
Admission, discharge and transfer arrangements 4 0 2 6Aids, appliances, equipment and premises 0 0 0 0All aspects of clinical treatment 18 29 23 70Appointments – delay 4 1 1 6Attitude 5 2 12 19Communication to patients/carers 2 3 4 9Hotel Services, including food 1 1 2Other 2 2 2 6Patients Property 1 1Policy and commercial decisions of the TrustService User - privacy, dignity and confidentiality 2 2Service user's records 2 2Violence/abuse
Total 36 40 47 123Table 3
7. Complaints Actions
The corporate complaints team now holds a rolling log of complaints actions, with identifiedleads and timescales for each action; and will seek assurance that actions have beencompleted. Capacity issues within the complaints team, together with the high number ofprocess changes that we are currently implementing, mean that we have not yet fullyembedded the process for completing and reporting on actions arising from complaints. Table4 illustrates the total number of actions recorded on the central log, of which the majority havebeen captured during Q3.
Total actions 63
Total open actions 36
Actions raised during Q3 2014 40
Actions closed during Q3 2014 15
Table 4

Page 4 of 5
8. Next Steps
We are making a number of changes to the way in which we manage complaints, aimed atimproving the process for service users. Key improvements are as follows:
Named contacts. Each complaint will have an allocated ‘owner’ who will be responsiblefor maintaining contact with the service user, providing a more personal experience andthe benefits of a single point of contact.
Severity assessments. Complaints will be severity assessed, so that more senior andexperienced staff members can be allocated to investigate more serious complaints.
Tailored complaint resolution timelines. In line with national guidance and bestpractice, the new process will allow for resolution timelines that are agreed with theservice user and are tailored to the nature of the complaint.
Locally managed process. A new ‘locally managed’ process will be introduced forlower severity complaints, to allow local staff to resolve issues directly and respond tothe complainant personally, rather than always having to go via the central complaintsteam which in some instances can add an unnecessary step in our process. Allcomplaints will still be recorded and reported; and the corporate team will continue tooversee local complaints management.
Reporting. Improved complaints reporting will allow better quantitative and qualitativeanalysis, allowing us to identify common themes and look at trends at (for example)care group level.
Learning lessons. We are engaging with leads from each care group to ensure thatthey have processes in place to manage complaints actions through to completion – it islikely that this will be managed through existing care group clinical governance groups.
Investigator training. We are collaborating with Leeds Independent Health ComplaintsAdvocacy (LIHCA) to provide training for complaints investigators.
Policy document revision. We will make guidance much clearer for staff tounderstand, improving the service user experience by addressing processinconsistencies. This will include the creation of an easily accessible customer-facingprocess document.
Clarified signposting for feedback. Ways of providing feedback to the Trust are beingupdated in line with the new process. This includes reviews of written materials (leaflets,posters), the Trust website and raising staff awareness about the correct ways forservice users or those acting on their behalf to provide feedback. It also encompassesreferrals to the PALS service (for advice and concerns) and Compliments processes.
Datix Web. We are implementing a new system for recording and monitoringcomplaints. This offers a number of benefits in terms of reporting and the platform isused nationally by a number of Trusts, opening up the possibility of comparing ourperformance with that of others nationally.

Page 5 of 5
Telephone feedback. Currently our final complaints response letter asks complainantsto give us feedback on the way their complaint has been handled; however we receivevery few responses to this request. Our new process will include a routine telephonecall to complainants at a set time after their complaint response letter has been sent, toseek verbal feedback to a short series of set questions. This will enable us tocontinuously learn from feedback.
To help to deliver these improvements we have secured further capacity within the ComplaintsManagement Team, initially on a fixed term basis.
The Complaints team needs to be able to respond more quickly to ensure that expected timescales are achieved. A new Complaints Manager post, supported by the existing post ofComplaints Administrator, will enable a speedy response to the (less serious) severity 1 and 2complaints, and much needed support for the clinical investigators handling the more serious(severity 3 – 5) complaints. The new post will also lead on essential investigation training,which is currently not provided. We will be able to maintain contact with complainantsthroughout the complaints investigation, advising them of any slippage or delay, and workingmore closely with the various independent advocacy services.
Clarity of reporting will improve through having a dedicated Complaints Manager. This willfacilitate better governance of our responses and reporting on outcomes. Thematic analysiswill be carried out objectively and split by service to help identify trends and enable thedissemination of lessons learnt across the group. We will be able to evidence the sharing oflessons learnt and will maintain a full record for audit purposes. In the recent CQC inspection itwas highlighted that in many cases local records of complaints learning are not maintained;the Complaints Manager will have a clear role in improving awareness and oversight.
The additional resource will create networks with other NHS organisations and will liaise withexternal agencies e.g. Healthwatch, Advocacy (LIHCA) etc. to improve our ability tobenchmark against other organisations and improve our processes in line with best practice.
9. Recommendations
The Board is requested to:
Note the content of the report
Be assured of the actions taken in respect of complaints and that these are being
progressed appropriately.

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Signing up to safety
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Jim Isherwood & Carl ThompsonSTRATEGIC: √
PAPER AUTHOR: Jim IsherwoodGOVERNANCE: √
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)G1 People achieve their agreed goals for improving health and improving lives √ G2 People experience safe care √ G3 People have a positive experience of their care and support √
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)SO1 We provide excellent quality, evidence-based, safe care that involves people and promotes
recovery and wellbeing√
SO2 We work with partners and local communities to improve health and lives √ SO3 We value and develop our workforce and those supporting us √ SO4 We provide efficient and sustainable services √ SO5 We govern our Trust effectively and meet our regulatory requirements √
STATUS OF PAPER
To be taken in the public session (Part A) √
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individualsOther – not yet a public documentMatters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
19

SUMMARY:The Quality Committee agreed, in October 2014, to recommend that the Trust Boardconsider signing up to safety following the invitation from Jeremy Hunt to all Trusts. TheTrust Board, through its workshop on 14.11.14, agreed the final action plan that wasapproved at the Quality committee on 11.12.14 and is contained within this paper. Insigning up to safety the Board is committing to the five given pledges.
RECOMMENDATIONS:The Trust Board is asked to;1. Approve the final version of the action plan.2. Sign up to safety.

Sign Up To Safety
1
Sign up to Safety – Final Version
This draft follows review of the feedback received following dissemination of draft 1, discussion at
the Trust Board workshop on 14.11.14 and approval at the Trust’s Quality Committee on 11.12.2014.
Underlying Principles
Actions must be relevant to what we know we need to do already (and must not, therefore,
simply increase the number of action plans already in progress).
Actions must, as far as is possible, not require additional resource unless the need for that
resource has already been identified
The number of actions must be manageable
Actions must be SMART (measurable in the sense that we will know whether they have been
achieved)
Wherever possible the impact of actions should be measurable, particularly in demonstrating
that quality of care and/or safety for patients and staff is improving (this includes
demonstrable learning)
Revised Action Plan for each of the 5 Pledges
1. Put safety first; Commit to reduce avoidable harm in the NHS by half and make public the
goals and plans developed locally.
The Trust will develop plans for specific serious harms;
o To reduce the likelihood of suicide by people with mental health problems by
training staff to work collaboratively using recognised approaches to safety planning
and risk management such as the Connecting with People approach.
o To support people in crisis through the development of liaison psychiatry teams
o To improve the physical health of people who use our services through the
promotion of academic posts and networks.
o To address known deficiencies in communication with primary care and to specify
responsibility for physical health monitoring.
The Trust will develop specific plans to eliminate never events;
o By developing and implementing a continuous system of inspection of our ward
environments to eliminate fixed ligature points from our inpatient services.
o By implementing a system of electronic prescribing and training our staff in its use to
reduce the likelihood of medication errors.

Sign Up To Safety
2
2. Continually learn; Make the organisation more resilient to risks by acting on the feedback
from patients and by constantly measuring and monitoring how safe the services are.
The Trust will seek simple but routine feedback from all patients, carers and family on exit
from care to better understand what was good or could have been done better?
The Trust will encourage staff to report their concerns directly during leadership walkabouts.
On hearing such concerns, Directors will be required to respond to the staff that raised
concerns following discussion with officers of the Trust.
The Trust will enhance and reorganise the risk management team so that it has capacity to
undertake thematic analyses of complaints, incidents, claims and other relevant information
and to monitor the implementation of action plans.
o The risk management team will be trained and equipped to be capable of
undertaking thematic analysis and developing SMART and prioritised action plans.
3. Honesty; be transparent with people about the progress to tackle patient safety issues and
support staff to be candid with patients and their families if something goes wrong.
The Trust will cascade training to improve communication skills for staff who need to
apologise and explain to patients and their carers what has gone wrong and why.
The Trust will publish safety and quality indicators including;
o The friends and family test, patient & staff surveys, participation in the National
Confidential Inquiries
o Significant National and local clinical audits
o Patient Reported Outcome Measures
o The Trust will publish themed data from complaints, incidents, claims and other
relevant information and associated action plans in Public Board papers and on its
website.
4. Collaborate; take a leading role in supporting local collaborative learning, so that
improvements are made across all of the local services that patients use.
The Trust will seek membership of a local steering group to include the voluntary sector.
The Trust will participate in a shared learning network with NHS Mental Health Providers
and Primary Care.
The Trust will share its learning with CCGs and NHS England and seek support and advice
where barriers occur in attempts to improve safety.

Sign Up To Safety
3
The Trust will seek research opportunities in collaboration with local Universities to improve
patient safety and the quality of care.
5. Support; help people understand why things go wrong and how to put them right. Give
staff the time and support to improve and celebrate the progress.
The Trust will commit to a culture that allows staff to feel comfortable reporting incidents,
raising concerns and suggesting improvements.
o The starting point of any investigation into an untoward incident will be to
determine what happened and what lessons can be learned.
o Resources will be made available to support staff to learn from untoward incidents
and to address those circumstances that prohibit the delivery of safe care.
The Trust will commit to supporting each member of staff that raises concerns about poor
practice in the Trust, including those that report their own errors.
o So that our approach is consistent with the Nursing Times’ ‘Speak Out Safely’
campaign.
o Through the appointment of safety champions.
o By introducing a support line for staff involved in untoward incidents or serious
complaints
The Trust will expect all staff to contribute to its determination to provide safe care and, in
doing so, to uphold the statutory duty of candour and to meet the responsibilities
articulated in their professional standards.
The Trust will create Trust Awards to reflect and celebrate commitment to open reporting
culture, for example;
o The team or individual that addressed a safety issue through their own initiative and
shared learning across the Trust.
o The clinical audit that had greatest impact on safety.
o The research project that had the greatest impact on safety.
Professor Carl Thompson, Non-Executive DirectorDr Jim Isherwood, Medical Director
(11.12.2014)

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: National Confidential Inquiry into Suicide and Homicide by Peoplewith Mental Illness
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Jim IsherwoodSTRATEGIC:
PAPER AUTHOR: Jim IsherwoodGOVERNANCE: √
INFORMATION: √
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)G1 People achieve their agreed goals for improving health and improving lives √ G2 People experience safe care √ G3 People have a positive experience of their care and support √
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)SO1 We provide excellent quality, evidence-based, safe care that involves people and promotes
recovery and wellbeing√
SO2 We work with partners and local communities to improve health and lives √ SO3 We value and develop our workforce and those supporting us √ SO4 We provide efficient and sustainable services √ SO5 We govern our Trust effectively and meet our regulatory requirements √
STATUS OF PAPER
To be taken in the public session (Part A) √
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individualsOther – not yet a public documentMatters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
20

SUMMARY:
The National Confidential Inquiry into Suicide and Homicide by People with Mental Illnesspublished its annual report in July 2014. This was reported to the Board at its publicmeeting in the Chief Executive’s update the same month. The Board asked for a paperdescribing the work of the Inquiry, the actions taken by the Trust in response to its findingsand the implications of some of its recommendations.
RECOMMENDATIONS:
The Trust Board is asked to;
1. Note the work and recommendations of NCISH and the activities of the Trust inresponse to the findings of the Inquiry.
2. Consider the implications for the Trust if all the recommendations of NCISHbecome national policy.
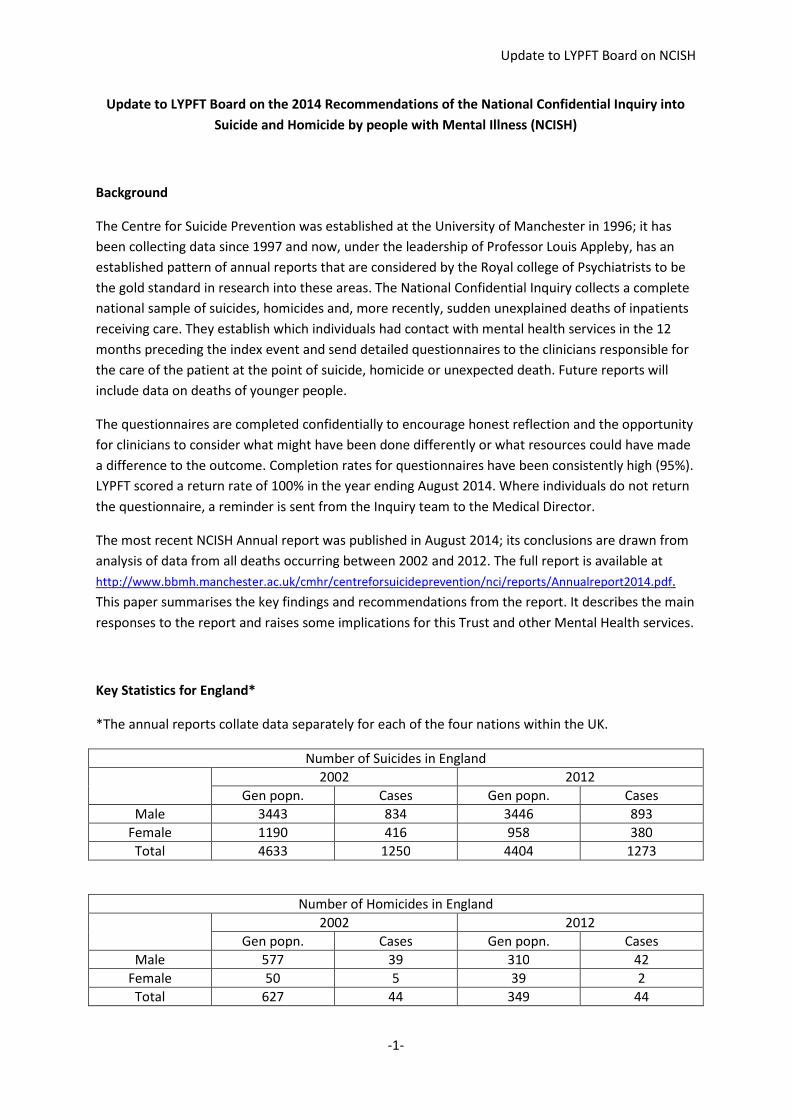
Update to LYPFT Board on NCISH
-1-
Update to LYPFT Board on the 2014 Recommendations of the National Confidential Inquiry into
Suicide and Homicide by people with Mental Illness (NCISH)
Background
The Centre for Suicide Prevention was established at the University of Manchester in 1996; it has
been collecting data since 1997 and now, under the leadership of Professor Louis Appleby, has an
established pattern of annual reports that are considered by the Royal college of Psychiatrists to be
the gold standard in research into these areas. The National Confidential Inquiry collects a complete
national sample of suicides, homicides and, more recently, sudden unexplained deaths of inpatients
receiving care. They establish which individuals had contact with mental health services in the 12
months preceding the index event and send detailed questionnaires to the clinicians responsible for
the care of the patient at the point of suicide, homicide or unexpected death. Future reports will
include data on deaths of younger people.
The questionnaires are completed confidentially to encourage honest reflection and the opportunity
for clinicians to consider what might have been done differently or what resources could have made
a difference to the outcome. Completion rates for questionnaires have been consistently high (95%).
LYPFT scored a return rate of 100% in the year ending August 2014. Where individuals do not return
the questionnaire, a reminder is sent from the Inquiry team to the Medical Director.
The most recent NCISH Annual report was published in August 2014; its conclusions are drawn from
analysis of data from all deaths occurring between 2002 and 2012. The full report is available at
http://www.bbmh.manchester.ac.uk/cmhr/centreforsuicideprevention/nci/reports/Annualreport2014.pdf.
This paper summarises the key findings and recommendations from the report. It describes the main
responses to the report and raises some implications for this Trust and other Mental Health services.
Key Statistics for England*
*The annual reports collate data separately for each of the four nations within the UK.
Number of Suicides in England
2002 2012
Gen popn. Cases Gen popn. Cases
Male 3443 834 3446 893
Female 1190 416 958 380
Total 4633 1250 4404 1273
Number of Homicides in England
2002 2012
Gen popn. Cases Gen popn. Cases
Male 577 39 310 42
Female 50 5 39 2
Total 627 44 349 44

Update to LYPFT Board on NCISH
-2-
Number of Sudden Unexplained deaths among Inpatients
2002 2012
Gen popn. Cases Gen popn. Cases
Male nr 22 nr 14
Female nr 19 nr 9
Total nr 41 nr 23
There has been no significant trend in the total number of suicides of people with mental illness in
England over the 10 year period but the proportion of male suicides is rising.
The number of cases of homicide peaked during 2006 – 2008 and there has been a steady but
sustained reduction since then. A great majority are committed by men.
The total number of Sudden Unexplained Deaths in Mental Health In patients is small and has been
steady since2009. Higher figures before 2006 are likely to reflect a change in the data collection
criteria.
Key Findings from Related Research undertaken at University of Manchester
In addition to its annual reports NCISH publishes findings and recommendations from related
studies; relevant key findings are listed below;
1. Those services that did not implement recommendations from previous reports had little
reduction in suicide (ref 1).
2. From the 2006 study, provision of 24 hour crisis care was associated with the biggest fall in
suicide rates (ref 1).
3. Local policies on patients with dual diagnosis and multidisciplinary review after suicide were also
associated with falling rates (ref 1).
4. Removal of ligature points was associated with large reductions in inpatient suicide and assertive
outreach teams seemed to reduce suicide in those with a history of missed contact with services
(ref 1).
5. Among patients treated by crisis resolution home treatment services, the average rate of suicide
seemed higher than the average rate among psychiatric inpatients (ref 2).
6. Among patients treated by crisis resolution home treatment services, living alone and
undergoing a major life event were associated with suicide; one third of patients treated by
CRHT who committed suicide did so within 3 months of discharge from inpatient care (ref 2).
7. Risk assessment and management should be individual to each patient, should assess current
and past risk factors and should include a management plan that follows from the risk
assessment (ref 3).
8. Risk assessment and management should not ignore past history, equate the completion of a
checklist with good formulation and management and should not rely on a generic plan of
clinical management.
Update to LYPFT Board on NCISH
-3-
Key Findings and Recommendations from the 2014 Annual Report
1. The first 3 months (and particularly the first 2 weeks) after discharge from in patient care
remains a time of particularly high risk for suicide. Suicide in the first two weeks after discharge
is linked to admissions lasting less than 7 days and adverse life events. Despite early
improvements with the introduction of CRHT the picture has not improved since 2006.
a. Care of patients on discharge from hospital should be a priority.
b. Effective care planning (CPA) is needed including for patients who discharge themselves.
c. Early follow up should be routine: NCISH suggest that suicide within 3 days of discharge
should be considered an NHS ‘never event’.
d. Adverse events that precede admission should have been addressed before discharge.
e. The benefits if reducing length of stay should be balanced with risks and it should not be
an aim in itself.
2. Hanging remains the commonest method of suicide in both the general and patient populations.
a. The portrayal of hanging in the media should be re-examined so that it is not seen as
quick and painless.
3. Suicide by patients receiving CRHT is now substantially more common than in inpatient care.
Living alone is a common antecedent of suicide by patients under CRHT.
a. CRHT should be a priority setting for suicide prevention in mental health services.
b. CRHT may not be suitable for patients at high risk or those who do not have adequate
family or social support: services should review the criteria for its use.
4. Higher suicide rates from 2008 have been linked to the economic crisis – but the impact is varied
across regions, countries and age groups.
a. Services should recognise the economic pressures patients might be facing and offer
help with employment, housing and debt, working with relevant agencies.
5. Figures for intimate partner homicides have fallen but remain a serious problem, 77% involve
male perpetrators and female victims. 13% of perpetrators were mental health patients (similar
to the general population).
a. Mental health services should play a stronger role in protecting victims of domestic
violence by ensuring perpetrators receive treatment for mental disorder including
substance misuse.
b. Mental health services should also play a full part in multi-agency collaboration through
information sharing and joint review.
6. The previous fall in patient homicides has been maintained – this is related to better care for
people with mental illness and substance misuse – but there has been no further fall.
a. Services should continue to address patients’ comorbidities through better provision for
alcohol and drug misuse and ‘dual diagnosis’.

Update to LYPFT Board on NCISH
-4-
7. Annual figures for deaths within 24 hours of restraint are low (24 in England and Wales between
2002 and 2012) but 6 occurred within 1 hour of restraint. It is not known whether restraint is
causal in these sudden unexplained deaths.
a. Services should implement the approach to restraint described in the 2014 report by the
DoH on reducing the need for restrictive interventions.
b. Deaths and serious injuries caused by restraint should be considered an NHS ‘never
event’.
What additional measures the Trust is taking in response to recommendations from the report
It is not the purpose of this paper to describe all service development and improvement activity that
is on-going within services provided by LYPFT but three programmes are highlighted that have
particular relevance to the findings from NCISH and learning from untoward events;
1. Research
Dr Andria Hanbury has been seconded from the University of York for two years to analyse key
processes within the Trust that may have barriers to successful implementation. Prominent
among these is the delivery of the Care Programme Approach. It is hypothesised that better
performance in the delivery of CPA will improve a variety of patient outcomes besides self-harm
and suicide. These include partnership working with non-health sectors, management of
multiple diagnoses and physical health care.
2. Removal of Fixed Ligature Points from Inpatient Settings
Training is underway across inpatient services to ensure all inpatient areas are subject to regular
risk assessment audit using the Manchester Ligature Risk Assessment Tool (ref 4). It is proposed
that as many staff as possible (including members of the Board) undertake this training so that
whenever a potential ligature risk is identified the matter may be reported, recorded and acted
upon expediently.
3. Review of Clinical Risk Training
The review of clinical risk training, involving clinical staff from all care groups, was completed in
clinical risk training will focus on collaboration with patients, consultation with carers and other
relevant parties and co-production of a safety plan based on the assessment of clinical risk. This
approach is consistent with the work already underway in the promotion of a recovery model.
A new on-line e-learning package is now available for all staff and this is followed by a face-to-
face training session. The content and style of training is delivered through membership of
‘Connecting with People’, a network led by Dr Alys Cole-King. This work has a strong evidence
base. As a member organisation we are able to cascade training from our own trainers and will
have access to updates in training as new evidence for effective risk management of patients in
crisis becomes available.

Update to LYPFT Board on NCISH
-5-
4. Review of SIs at LYPFT
The Director of Nursing has already discussed the feasibility of Professor Appleby’s team
undertaking a review of all serious incident reports related to deaths during the last twelve
months with a Senior Research Fellow from NCISH. The terms of reference of the review will be
finalised by the Directors of Nursing and Medicine and it is intended that the results would be
submitted to the Board of Directors and Council of Governors.
Further Implications for LYPFT
The author proposes that the Board may wish to consider the findings and recommendations of the
work of NCISH, not least the following two further implications;
1. Service Design
In associated research and the most recent report there has been a consistent theme warning
against practices and service models that drive home treatment and early discharge rather than
admission to hospital. Limited bed availability has been noted frequently across many types of
mental health service in recent years. These recommendations advise caution against the use of
home treatment for some patient groups and under some circumstances. Commissioners and
providers may need to reconsider how services are designed in future and this may have
implications for savings plans.
2. Never Events
NCISH has proposed additions to the list of NHS ‘never events’ so that suicides within 3 days of
discharge from hospital or deaths caused by restraint will be reported in future. Any death
involving restraint demands rigorous investigation, as does any suicide, but (especially in the
case of suicides after discharge) it is foreseeable that there will be a small increase in reported
never events. It is important that if such deaths are reported as never events, the response from
the Trust is fair and consistent and entirely in line with the pledges that the Board intends to
make in its commitment to ‘Sign up to Safety’. At the presentation that accompanied the launch
of the 2014 Annual report, Professor Appleby stressed the difficulties faced by clinicians in
mental health services. It is right to raise the profile of the needs of people with mental health
problems and this is the intention of these proposals.
References
1. D While et al (2012) Implementation of mental health service recommendations in England and Wales and suicide rates, 1997 -2006:
a cross-sectional and before-and-after observational study. The Lancet Published online February 2, 2012. www.thelancet.com
2. IM Hunt et al (2014) Safety of Patients under the care of crisis resolution home treatment services in England; a retrospective
analysis of suicide trends 2003 to 2011. The Lancet Published online June 18, 2014. www.thelancet.com/psychiatry
3. The National Confidential Inquiry into Homicide and Suicide by People with Mental Illness (NCISH) (2013) Quality of Risk Assessment
Prior to Homicide: A Pilot Study.
4. Manchester Mental Health and Social Care Trust and Manchester City Council (2013) Ligature Risk Assessment Policy.

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Serious Untoward Incidents Update and Lessons Learntfollowing the Trust Incident Review Group meetings held:12/11/2014, 10/12/2014, 14/01/2015
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Jim IsherwoodMedical Director
STRATEGIC:
PAPER AUTHOR: Christine WoodwardHead of Risk Management
GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)
G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)
SO1 We provide excellent quality, evidence-based, safe care that involves people and promotesrecovery and wellbeing
SO2 We work with partners and local communities to improve health and lives
SO3 We value and develop our workforce and those supporting us
SO4 We provide efficient and sustainable services SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individuals
Matters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
21

SUMMARY:
The attached paper is a briefing for the Board of Directors following the Trust IncidentReview Group meetings held: 12/11/2014, 10/12/2014, 14/01/2015.
The report is broken down as below:PART A – Serious Untoward Incidents UpdatePART B – Serious Untoward Incidents Lessons Learnt.
RECOMMENDATIONS:
Note the content of the report. Be assured that the actions in respect of the lessons learnt are being progressed
appropriately through the committee (or organisation).

Following the Trust Incident Review Group Meeting Held: 12/11/2014, 10/12/2014,14/01/2015
Part A:Serious UntowardIncidents Update

Page 2 of 17
1 Purpose
The purpose of this paper is to provide the Board with information relating to new incidentsthat are subsequently categorised as Serious Untoward Incidents (SUI).
2 Executive Summary
The paper details the following information: TABLE 1 – Breakdown of Serious Untoward Incidents –
October/November/December 2014 TABLE 2 – Overview of Serious Untoward Incidents by Directorate –
October/November/December 2014. TABLE 3 – Number of Final reports of STEIS(Strategic Executive Information
System) incidents submitted to TIRG within 12 week/details of overduecases/reasons for delay
TABLE 4 – Schedule of cases to be presented to Trust Incident Review Group
3 Background
The following table shows a brief flow of action: from incident occurring to presentation atthe Trust Incident Review Group (TIRG).
All incidents that are agreed as Serious Untoward Incidents and STEIS reported arepresented at TIRG.Following review of the fact find information, a Root Cause Analysis Investigation can berequired even though the incident is not STEIS reported. In these cases the report ispresented to TIRG at the discretion of the Directorate and TIRG Chair.
Final Report to the Trust Incident Review Group
The report is submitted to TIRG within 45 working days. Once agreed the report is sent to Leeds West ClinicalCommissioning Group for final review and closure.
Incident agreed as Serious Untoward Incident
Incident is reported via STEIS and a full Root Cause Analysis Investigation is commenced.
Review by Risk Management
Risk Management reviews the information on the fact find and agrees the level of investigation with the DeputyDirector of Care Services and Deputy Director of Nursing/Head of Clinical Governance.
Incident Occurs - Incident Report Form (IR1) Completed
Due to the severity rating /type of incident a Fact Find report is completed.

Page 3 of 17
TABLE 1 – Breakdown of Serious Untoward Incidents (SUI)
TABLE 2 – Overview of SUI’s by Care Group
Care GroupIncident
DateIncident Type
IncidentNumber
Severity Rating Service
Leeds 23/10/2014 Assault leading to injury (SU to SU) 168386 5 W2 The Mount
York 04/10/2014 Death - Overdose 165330 5 AOT
Leeds 03/11/2014 Death - Hanging* 87972 5 CMHT Millfield
Leeds 06/11/2014 Self Injury – Stabbed* 138158 4 ICS South
Leeds 08/11/2014 Serious Assault on member of staff* 146695/8535 4 W4 Becklin
Leeds 12/11/2014 Overdose* 157906 5 CMHT WNW
Leeds 25/11/2014 Death - Hit by train* 101796 5 CMHT SSE
Leeds 27/11/2014 Death – Hanging* 134216 5 CMHT WNW
Leeds 26/11/2014 Death – Hanging* 101797 5 CMHT SSE
York 18/11/2014 Death – Found in River* Not listed 5CAS Home Based
Treatment
York 06/11/2014 Death - Jumped from height* 173901 5 South West CAS
Leeds 28/12/2014 Death – HangingWEBINC-
29105 W4 Becklin
York 16/12/2014 Unexpected inpatient death*WEBINC-
27805 W1 Bootham
SS/LD 03/12/2014 Unexpected Death - jumped from height* 165266 5 LAU
Period:Leeds Care
Group
Specialist andLD CareGroup
YorkNorth Yorkshire
Care GroupTOTAL
NUMBER OF INCIDENTS REPORTED VIA
STEIS – Oct 2014 1 0 1 2
NUMBER OF INCIDENTS REPORTED VIA
STEIS – Nov 2014 7 0 2 9
NUMBER OF INCIDENTS REPORTED VIA
STEIS – Dec 2014 1 2 2 5
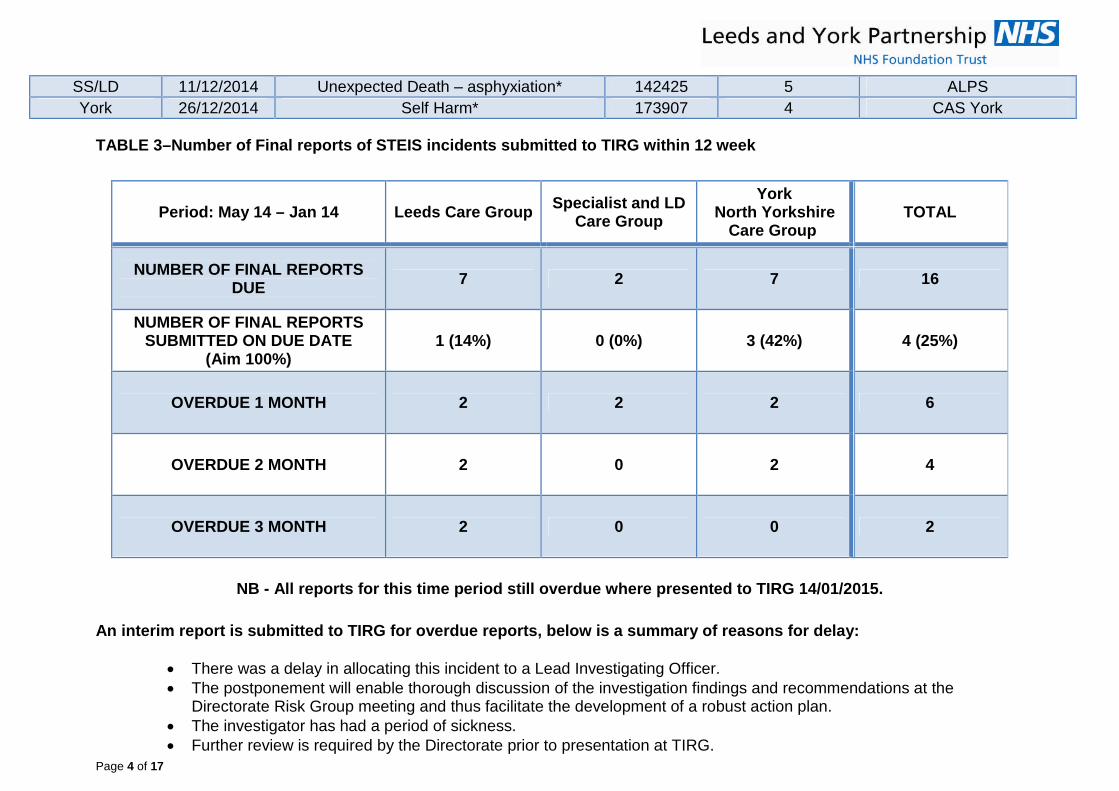
Page 4 of 17
SS/LD 11/12/2014 Unexpected Death – asphyxiation* 142425 5 ALPS
York 26/12/2014 Self Harm* 173907 4 CAS York
TABLE 3–Number of Final reports of STEIS incidents submitted to TIRG within 12 week
NB - All reports for this time period still overdue where presented to TIRG 14/01/2015.
An interim report is submitted to TIRG for overdue reports, below is a summary of reasons for delay:
There was a delay in allocating this incident to a Lead Investigating Officer. The postponement will enable thorough discussion of the investigation findings and recommendations at the
Directorate Risk Group meeting and thus facilitate the development of a robust action plan. The investigator has had a period of sickness. Further review is required by the Directorate prior to presentation at TIRG.
Period: May 14 – Jan 14 Leeds Care GroupSpecialist and LD
Care Group
YorkNorth Yorkshire
Care GroupTOTAL
NUMBER OF FINAL REPORTSDUE
7 2 7 16
NUMBER OF FINAL REPORTSSUBMITTED ON DUE DATE
(Aim 100%)1 (14%) 0 (0%) 3 (42%) 4 (25%)
OVERDUE 1 MONTH 2 2 2 6
OVERDUE 2 MONTH 2 0 2 4
OVERDUE 3 MONTH 2 0 0 2

Page 5 of 17
Due to unforeseen circumstances the investigation was reallocated.
TABLE 4 – Schedule of cases to be presented to Trust Incident Review Group

Page 6 of 17
Date ofincident
Type of Incident Care Group STEIS/IR1LYPFT
RefCCG Due
Date
Reportpresented
on duedate
Proposed Date to TIRG
27/07/2014 Self Harm - Jumped from 2nd floor Leeds 2464107-
14.1508/10/2014 NO
14/01/2015
01/08/2014 Death - Hanging Leeds 2523608-
14.1508/10/2014 NO
14/01/2015
18/08/2014 Death - Drowning Leeds 2784911-
14.1512/11/2014 NO 14/01/2015
28/09/2014 Accident or deliberate harm to self Leeds 3200514-
14.1510/12/2014 NO
14/01/2015
29/09/2014 Fire leading to full evacuation Specialist & LD 3203815-
14.1510/12/2014 NO
14/01/2015
04/10/2014 Death - Overdose York 3247116-
14.1510/12/2014 NO
14/01/2015
23/10/2014Assault leading to injury Leeds 36402
17-14.15 11/02/2015
11/02/2015
06/11/2014Death - Jumped from height York 36407
18-14.15 11/02/2015
11/02/2015
03/11/2014Death - Hanging
Leeds36447
19-14.15 11/02/2015
11/02/2015
06/11/2014Self Injury – Stabbing
Leeds36451
20-14.15 11/02/2015
11/02/2015
08/11/2014Serious Assault on member of staff
Leeds36902
21-14.15 11/02/2015
11/03/2015
12/11/2014Death - Overdose
Leeds37541
22-14.15 11/02/2015
11/03/2015
18/11/2014Death – Drowning York 37915
23-14.15 11/02/2015
11/03/2015
01/02/2014Suspected Suicide - Overdose Leeds 38770
24-14.15 11/02/2014
11/03/2015
25/11/2014Death - Hit by train Leeds 38787
25-14.15 11/02/2015
08/04/2015
27/11/2014 Death –Hanging Leeds 38937 26- 11/02/2015 08/04/2015

Page 7 of 17
Please note: The CCG have been advised of the above schedule and have granted extensions on all the reports.
14.15
26/11/2014Death –Hanging Leeds 39054
27-14.15 11/02/2015
08/04/2015
30/11/2014Death - Hanging York 10234
28-14.15
11/03/201508/04/2015
03/12/2014Death - jumped from height Leeds 39407
29-14.15
11/03/201508/05/2015
28/11/2014Self Harm Specialist & LD 39944
30-14.15
11/03/201508/05/2015
11/12/2014Death Specialist & LD 40672
31-14.15
11/03/201508/05/2015
16/12/2014Death York 41010
32-14.15
08/04/201508/05/2015
28/12/2014Death - hanging Leeds 42064
33-14.15
08/04/201510/06/2015
26/12/2014Self Harm York 42473
34-14.15
08/04/201510/06/2015

Page 8 of 17
Following the Trust Incident Review Group Meeting Held: 12/11/2014, 10/12/2014,14/01/2015
Part B:Serious UntowardIncidents Lessons Learnt

Page 9 of 17
1 Purpose
Summary of lessons learnt from Serious Untoward Incidents. Sharing of good practice highlighted from reports. Conclusions of any thematic reviews that were undertaken. Results of any trend analyses. Summary of major actions that have been implemented.
2 Executive Summary
Learning from experience is critical to the delivery of safe and effectiveservices in the NHS. To avoid repeating mistakes organisations need torecognise and learn from them, to ensure that the lessons are communicatedand shared and that plans for improving safety are formulated and actedupon. The findings and learning from any adverse event within the Trust mayhave relevance and valuable learning for the local team and also other teamsand services. This paper outlines the identified lessons learnt following theTrust Incident Review Group meetings 12/11/2014, 10/12/2014 and14/01/2015.
3 Background
The purpose of the Trust Incident Review Group is to review the investigationreports to ensure that all serious untoward incidents have been investigatedthoroughly, to agree recommendations and action plans that are relevant andachievable, to oversee the implementation of those action plans and toidentify trends and patterns of untoward incidents that may require furtherinvestigation.
This activity supports LYPFT to be an organisation with a memory, to assistlearning from incidents and to continue the drive towards safer therapeuticcare for all service users.
Findings from the meetings held:12/11/2014, 10/12/2014 and 14/01/2015
4 Outline of Lessons Learnt from Serious Untoward Incidents
Older People Units in York
A Root Cause Analysis (RCA) investigation has been completed to specificallyinvestigate the nursing care afforded to a service user in the immediate daysleading to her unexpected death. In order to manage any risks to service usersthe scope of the RCA was limited to ensure a quick turnaround.
As recommended within the RCA review, a mapping exercise has beenundertaken to understand the knowledge and skill base mix of the nursing staffat all Older People Units in York.

Page 10 of 17
A training programme has been developed to focus on the following factors:
Rationale and frequency for conducting physical observations Interpretation of physical observations and requesting further
investigations Medications and effects on physical observations Pressure area care including regular repositioning Screening tools for risk of pressure area breakdown Management of continence Fluid and diet intake How to promote fluids
TIRG were confident that the incident had been investigated thoroughlyhowever to ensure further assurance all the work completed on this issue willbe pulled together and presented to TIRG within one report - including theQuality Improvement Plan which is in place to address the concerns aboutsome aspects of care delivery.
MEWS
A Trustwide notice has been circulated to support an RCA recommendation thatan up to date baseline MEWS is available at all times for patients residing in ourunits. All inpatients in the trust must have a MEWS completed on admission sothat we have a baseline – this should be updated each week, as it has beenrecognised that some of our service users can be with us for long periods oftime. For example in one case, it was found that a patient had been with us for6 months and only had 1 set of observations done on their admission (nonesince). The concern with this is that a person’s physical health can changemassively over 6 months, especially with some of the medications used.
7 Day Follow Up
All patients discharged to their place of residence, care home, residentialaccommodation or non-psychiatric care must be followed up within 7 days ofdischarge. The seven-day period should be measured in days not hours andshould start on the day after the discharge.
Exemptions to the above are:
Patients who die within 7 days of discharge may be excluded Where legal precedence has forced the removal of a patient from the
country Patients transferred to NHS psychiatric inpatient ward CAMHS (child and adolescent mental health services) are not included.
The Trust has a very clear policy on 7 day follow up which is a national qualityindicator. There is some confusion with practitioners about the standard forfollow up at discharge being 3 days as a measure of “good practice” - there isno evidence that this is written into policy or local working instructions.Clarification will be circulated to make this clearer.

Page 11 of 17
Carer Involvement who are not listed as the next of kin
A service user’s parents raised a point during a Serious Incident Review thatthey did not feel involved in the care planning or delivery of care afforded totheir son. The service user’s family had arranged a “rota” of visitors and feltthat they may have benefitted from one of the family members being a “singlepoint of contact” on behalf of them all.
This recommendation will be discussed at the Acute Inpatient LeadershipForum in order to inform the review of current procedures.
External involvement with RCA investigations
The group discussed the involvement of an external counselling and therapyservice, in particular any specific questions we have asked of them as part ofthe RCA (Root Cause Analysis) investigation. We had been informed that theyhad not completed an internal review following the incident but due to thepersistence of our reviewer, their Governance Lead has advised that an internalreview would now take place and any subsequent information would be sharedwith the Coroner. TIRG agreed this was disappointing and showed reluctanceon their part to identify any learning from this very sad incident.
TIRG agreed that if we have another case with these issues in the future we willraise with the Learning Lessons Review Meeting via the Leeds or York SeriousCase Review Board.
This topic will also be included within all future LYPFT Root Cause Analysistraining to ensure our reviewers know of their options and jurisdiction.
Initial Review of Serious Incidents in Nov 2014
During the month of November 2014, 9 incidents have been reported as seriousvia STEIS [Strategic Executive Information System]. Due to this high number,which compares with 1 serious incident reported within the same period in2013, Risk Management provided a briefing paper to identify any initialcommonalities – none were evident.
Anthony Deery advised the Group that the number of incidents reflects thenational picture.
Obtaining information from carers and relatives
TIRG discussed the confidentiality issues raised within an RCA report whichhighlighted sharing information with carers and relatives of service users.TIRG commented that staff should be reminded that although they are unableto share information they should still be asking questions and gaining as muchknowledge as possible from those directly involved with the service user.It was agreed that this report be discussed at the Information GovernanceTeam meeting. Following the Information Governance meeting the below “mythbuster” was circulated Trustwide.

Page 12 of 17
Getting it RightListening to Carers & Relatives
As providers of mental health and learning disabilityservices, we are often approached by our service users’carers and relatives who wish to share information with usabout their family members or those they care for. There isa bit of a myth doing the rounds that this is something wemay not listen to or record due to "confidentiality" rules.Please accept the Trust's blessing to listen to, engage withand record this information.
The nature of our work occasionally means that our service users are not themost reliable source of information about their wellbeing. Carers, relatives andother 3rd parties often have valuable insight and factual information that isessential in seeing the full picture of what is going on in the lives of our serviceusers. If, during the course of your work, you hear from a carer, relative orsomeone else who wishes to tell you something then please engage. It issometimes the case that in doing so we will help the carer or relative as well asthe service user, by making them feel they have contributed to the wellbeing ofthose they care for.
If anything, this is the "opposite of confidentiality" - and we should not be citingconfidentiality or information governance as a reason not to do this. You cangive an assurance that we will hold that information in confidence and notdisclose it to the patient unless it is necessary or appropriate, and we will neverdisclose this under a "Subject Access Request".
Pilot Scheme
A recommendation from an RCA was that the Crisis Assessment Service andAcute Liaison Psychiatry Service teams will follow up any recommendations forreferral (specific to drugs and alcohol) to other services within the trust.
The Care Group discussed this recommendation and agreed that the resultingaction would be linked to an existing Pilot which was originally driven to reduceattendance at Accident and Emergency Units. The agreed action:Pilot harm reduction workers to follow up service users with substance misuseissues directly from CAS or ALPS service as an integrated service.
TIRG agreed that this was a positive action and a creative use of resources.
Translation Needs
An RCA report recommended that the needs of carers are considered inrelation to translating needs and that translating services are organised toattend at key points in the service user’s care and treatment. Throughout theRCA review the language barrier with the service user’s husband and hisunderstanding of her treatment and future plans had not been addressed.
The Care Group actioned that the standards for the use of translators within

Page 13 of 17
acute services in relation to service users and their carers are agreed anddisseminated.
Policy/Procedure Awareness
The inpatient unit staffs lack of awareness of the guidance within theMissing service user/patients Procedure resulting in the following:
The nursing team did not seek Senior Management/Senior Medicalsupport in a timely manner when concerns were raised regarding theservice users risk of harm to self and the response adopted by thePolice.
CCTV footage was not reviewed at the time of the service user’sdisappearance.
The service user was not categorized formally, as the procedureguidance, as a missing person.
The review recommended that the Ward team familiarise themselves with theLYPFT procedures “Patients leave of absence procedure” and the “Missingservice user/patients procedure” and ensure that they understand their role andresponsibilities.
Yorkshire Ambulance Service
On the day that a service user died, she was attended by paramedics from theYorkshire Ambulance Service while staff from the Assertive Outreach Team(AOT) were present. It is documented that one of the paramedics expressedconcern at the state of the lady’s house directly challenging AOT staff.This made an already distressing situation more difficult to deal with for theAssertive Outreach Team staff member involved.
Dr Isherwood has written to the Head of Quality at YAS and expressed onbehalf of the Trust that although we are sure no insult was intended by theparamedic, we would ask that this matter be raised at the Yorkshire AmbulanceService to make health colleagues aware of the difficulties faced by staff inCommunity Mental Health Services who face the dilemma of supporting peoplewith severe mental illness, often in very difficult circumstances, while attemptingto maintain collaboration without exacerbating symptoms of illness. Colleaguesin the Ambulance Service maybe unaware that mental health staff have nopower to insist that people maintain their houses in a clean and tidy fashionunless there is an immediate threat to life or safety.
TIRG requested that the staff involved with this service user are commendedand advise that the letter has been sent to YAS due to the criticism levelled atthem unjust.
5 Areas of Good Practice
“This is Me”
The inpatient service encouraged a service user’s daughter to complete the“This is Me” document. This Royal College of Nursing/Alzheimer Society paper
Page 14 of 17
allows the carer to give an insight into the patient’s life and past history.
Inter- Agency Working
Contact made to the Crisis and Access Service by a police officer was apositive step and an example of good inter-agency good practice. This contactallowed an early opportunity for intervention and assessment.
Inpatient Service
A significant amount of good practice was evident within a Root Cause Analysisconcerning a service user who had spent a period of time being cared for withinan inpatient ward at The Becklin Centre. The good practice included:
The approach to safeguarding regarding the service users wife had beencomprehensive and thorough.
The interface with community services and the implementation of theCare Programme Approach demonstrated good practice.
The risk assessment of the service user was consistent andcomprehensive.
The assessment and care of the service user as an inpatient was in-depth and sustained over the full 28 day period of his detention underSection 2 of the Mental Health Act 1983. The team made full use of thetime to fully assess the service user and engage him in working thoughhis problems and support him in finding ways to adapt to the forthcomingchanges in his life.
Crisis Assessment Service
The shift coordinator of the service used initiative to maximise time resourceand requested that the late shift colleagues began their shift at the PoliceStation.
The assessing clinicians spent approximately three hours attending to theassessment and had four separate contacts with the service user.
CAMHS Service
The below good practice points were highlighted within a review followingthe sad death of a service user:
A letter was written to the parents the day after the death to offersupport to them and the service user’s brother.
CAMHS contacted the service user’s parents and explained theinvestigatory process; offering support to help them to have a greaterunderstanding.
The Early Intervention Team (EIT) were given time with the CAMHSstaff on duty and offered use of the Community Links Health Mattersassistance programme.
CAMHS invited EIT to a joint debrief with their service.

Page 15 of 17
East North East – Intensive Community Services (ENE ICS)
ENE ICS developed a well-constructed recovery plan that was informedby thorough FACE Risk Assessment.
ENE ICS made a number of support calls to the service user. The needs of the service user’s children were clearly considered, good
interworking with other agencies was evident.
Efforts to locate a missing service user
The nursing team on the unit put considerable effort into trying to locate amissing service user by ringing around his friends and family and evencontacting the kennels where his dog was being kept. They persisted in makingcontact with the police and reiterating their concerns about his risk of suicide.
The Crisis Assessment Service responded to the concerns expressed by thenursing team by carrying out a welfare check and kept in regular contact withthe Ward throughout the night.
Mother & Baby Unit
There were areas of good practice evident throughout a review concerning anincident which occurred on the Mother and Baby unit:
Timely and appropriate staff actions to prevent further risk from effects offire and smoke inhalation.
Excellent application of business continuity plan to ensure the ongoingdelivery of safe and appropriate care to all unit Service users.
Excellent support provided by all staff responders across the Mount unit Good leadership and use of initiative in identifying alternative care
options for Service users whilst unit was closed for the 12 hour period.
Recommendations
The Board is requested to: Note the content of the report Be assured that the actions taken in respect of the lessons learnt are
being progressed appropriately through the organisation.

Page 16 of 17
GLOSSARY OF DEFINITIONS
The following definitions are of relevance to this document:
Definition Meaning
Case Conference Meeting to discuss complex cases that are very serious or have amulti-agency aspect and that may include criminal offences andpossible organisational failures.
CPA Care Pathway Approach
ICS Intensive Community Services
Incident For the purpose of the Trust’s incident reporting system, an incident isdefined as: -‘any event, untoward or unusual, which is a deviation from the normalpattern of activity or therapeutic well-being or smooth running of theworkplace (e.g. ward/ department, client’s home, etc.), which involvesservice users and/or staff and/or visitors, and which may adverselyaffect their health and/or safety and/or welfare and/or confidentialitythen or later’.
LYPFT Leeds and York Partnerships Foundation Trust
MDT Multi Disciplinary Team - A group composed of members with variedbut complimentary experience, qualifications, and skills that contributeto the achievement of the specific objectives.
PARIS Electronic patient information record system.
RCA Root Cause Analysis.
Risk A risk is characterised by both the likelihood/probability of harm orinformation security breach actually occurring (e.g. low, medium orhigh) and the impact/severity of the harm (e.g. slight injury, majorinjury, death).
The level of risk to health increases with the impact/severity of thehazard and the duration and frequency of exposure to the hazard.
Section 17 Leave Section 17of the Mental Health Act 1983 makes provision for patientswho are liable to be detained under various other sections of the Act tobe granted leave of absence.Section 17 applies to patients who are detained under ss.2, 3, 37, or47 of the Act.
Serious untowardincident (SUI)
A serious untoward incident is defined as ‘any accident or incidentwhere a service user, member of staff (including those in thecommunity), or member of the public suffers serious injury, majorpermanent harm or unexpected death, (or the risk of death or injury),

Page 17 of 17
on hospital, other health service premises or other premises wherehealth care is provided, or where actions of health services staff arelikely to cause significant concern’.
STEIS Strategic Executive Information SystemThis is the Trust’s mechanism for reporting serious untoward incidentsto the Clinical Commissioning Group.
TIRG Trust Incident Review Group
MEWS Modified Early Warning System
CAMHS Child and Adolescent Mental Health Services
LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Duty of Candour regulatory requirements
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Anthony Deery, Director of NursingSTRATEGIC:
PAPER AUTHOR: Melanie Hird, Head of ClinicalGovernance
GOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)
G1 People achieve their agreed goals for improving health and improving lives
G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)
SO1 We provide excellent quality, evidence-based, safe care that involves people and promotesrecovery and wellbeing
SO2 We work with partners and local communities to improve health and lives
SO3 We value and develop our workforce and those supporting us
SO4 We provide efficient and sustainable services
SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individuals
Matters exempt under the Freedom of Information Act (quote section number)
SUMMARY:
On 27 November 2014 the new Regulation 20: duty of candour of the Health and SocialCare Act 2008 came into force and all NHS bodies (including Foundation Trusts) must nowmeet its requirements. This paper summarises the main elements of the regulation; how
AGENDAITEM
22
the CQC will assess our compliance; how we are currently meeting the new regulation; andwhat further action needs to be taken.
RECOMMENDATIONS:
The Board is asked to be assured that the Trust meets the new Regulation 20 and thatareas for improvement are being addressed.

1
Board of Directors’ Meeting 29 January 2015
The Health and Social Care Act 2008 (Regulated Activities) Regulations 2014Regulation 20: Duty of Candour
1. Introduction
On 27 November 2014 the new Regulation 20: duty of candour of the Health and SocialCare Act 2008 came into force and all NHS bodies (including Foundation Trusts) must nowmeet its requirements. This new regulation has also been incorporated into the CQC’sinspection regime.
The introduction of regulation 20 is a direct response to the Francis Inquiry report, which
recommended that a statutory duty of candour be imposed on healthcare providers. Prior to
November 2014, we were already subject to a contractual duty of candour under Standard
Condition 35 of the NHS Standard Contract.
The aim of the regulation is to ensure that health service bodies are open and transparentwith the ‘relevant person’ (as defined in the regulation) when certain notifiable incidentsoccur. These incidents are defined as those which result in moderate harm; severe harm;death; and prolonged psychological harm.
This paper summarises the main elements of the regulation; how the CQC will assess ourcompliance; how we are currently meeting the new regulation; and what further action needsto be taken.
2. Responsibilities of the Trust
To meet the requirements of Regulation 20, the Trust must:
Act in an open and transparent way with ‘relevant persons’ in relation to care andtreatment provided. The ‘relevant person’ is defined as the service user and, incertain situations, those acting lawfully on their behalf, for example where a serviceuser under 16 is not competent to make decisions about their care and treatment, orwhere a service user lacks capacity to make decisions about their care andtreatment.
Tell the relevant person, in person, as soon as reasonably practicable after becoming
aware that a notifiable safety incident has occurred; and provide support to them in
relation to the incident, including when giving the notification.
Provide an account of the incident which, to the best of our knowledge, is true of all
the facts we know about the incident at the date of notification.
Advise the relevant person what further enquiries we believe are appropriate.
Offer an apology.
Follow this up by giving the same information in writing; and providing an update on
the enquiries.
Keep a written record of all communication with the relevant person.
If the relevant person cannot be contacted or declines to speak to us, we must keep
a written record of our attempts to contact or speak to the relevant person.

2
Appendix 1 maps how the Trust is currently meeting these requirements and what furtheraction needs to be taken.
3. Responsibilities of the Care Quality Commission
The CQC will check and monitor the extent to which the Trust meets regulation 20 duringinspection processes. Two specific key lines of enquiry (KLOEs) under the ‘safe’ and ‘well-led’ questions are relevant:
S2: Are lessons learned and improvements made when things go wrong?Are people who use services told when they are affected by something that goeswrong, given an apology and informed of any actions taken as a result?
W3: How does the leadership and culture reflect the vision and values,encourage openness and transparency and promote good quality care?Does the culture encourage candour, openness and honesty?
Information that CQC receives from a member of the public or a staff member relating to thestatutory duty of candour will be dealt with in line with their safeguarding and whistleblowingprotocols.
4. The Trust’s Response
An initial benchmarking exercise has been undertaken to ensure that the Trust is meetingthe requirements of the regulation (see Appendix 1). Further improvements are required toour systems and processes to embed the requirements into routine practice; to ensure thatwe can always demonstrate that we have met the Duty; to ensure that all staff are fullyaware of requirements; and to ensure that there is an organisational culture of openness andtransparency which is followed by all staff.
A Task and Finish Group has now been established to undertake further mapping againstthe detailed elements of the guidance, which CQC say we must consider. This will involve:
• The Head of Clinical Governance• The Head of Corporate Governance• The Deputy Chief Operating Officer• Assistant Director of Nursing (Compliance)• The Head of Risk Management• The Head of Organisational Development• The Head of Learning and People Development
The Group will develop an action plan to address any areas for improvement and willcontinue to meet until confident the Duty is embedded throughout the Trust.
5. Recommendation
The Board is asked to be assured that the Trust meets the new Regulation 20 and that areasfor improvement are being addressed.
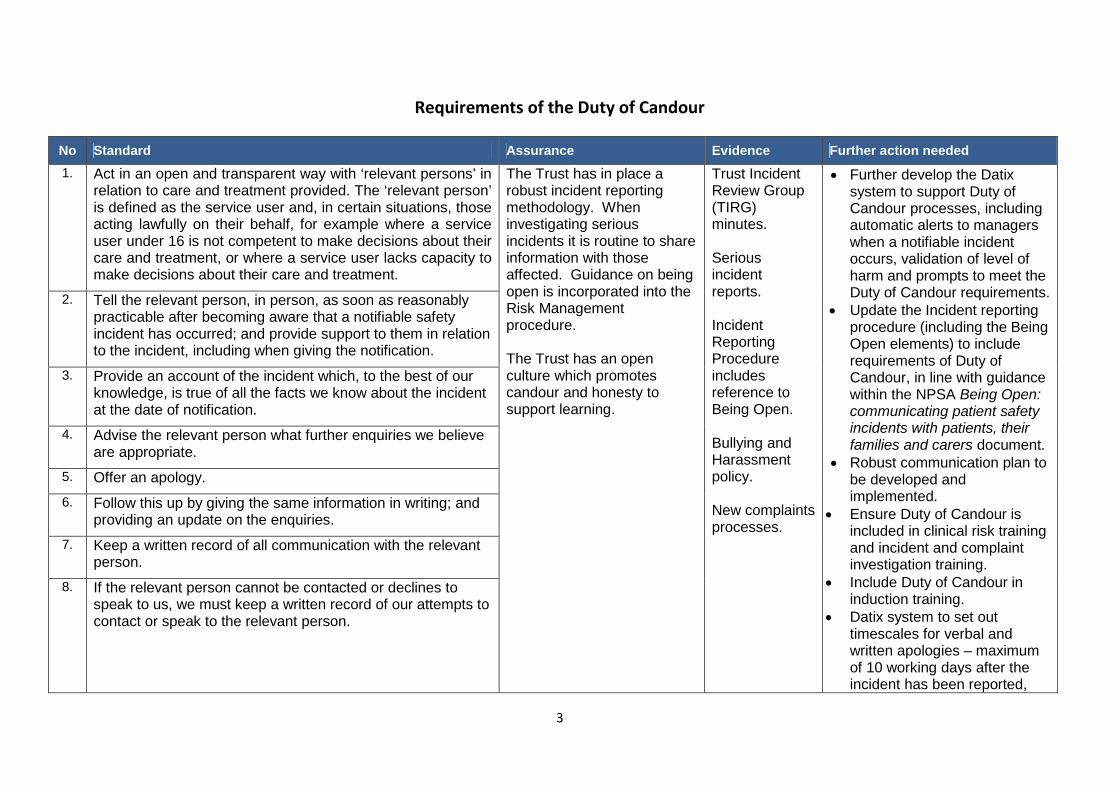
3
Requirements of the Duty of Candour
No Standard Assurance Evidence Further action needed
1. Act in an open and transparent way with ‘relevant persons’ inrelation to care and treatment provided. The ‘relevant person’is defined as the service user and, in certain situations, thoseacting lawfully on their behalf, for example where a serviceuser under 16 is not competent to make decisions about theircare and treatment, or where a service user lacks capacity tomake decisions about their care and treatment.
The Trust has in place arobust incident reportingmethodology. Wheninvestigating seriousincidents it is routine to shareinformation with thoseaffected. Guidance on beingopen is incorporated into theRisk Managementprocedure.
The Trust has an openculture which promotescandour and honesty tosupport learning.
Trust IncidentReview Group(TIRG)minutes.
Seriousincidentreports.
IncidentReportingProcedureincludesreference toBeing Open.
Bullying andHarassmentpolicy.
New complaintsprocesses.
Further develop the Datixsystem to support Duty ofCandour processes, includingautomatic alerts to managerswhen a notifiable incidentoccurs, validation of level ofharm and prompts to meet theDuty of Candour requirements.
Update the Incident reportingprocedure (including the BeingOpen elements) to includerequirements of Duty ofCandour, in line with guidancewithin the NPSA Being Open:communicating patient safetyincidents with patients, theirfamilies and carers document.
Robust communication plan tobe developed andimplemented.
Ensure Duty of Candour isincluded in clinical risk trainingand incident and complaintinvestigation training.
Include Duty of Candour ininduction training.
Datix system to set outtimescales for verbal andwritten apologies – maximumof 10 working days after theincident has been reported,
2. Tell the relevant person, in person, as soon as reasonablypracticable after becoming aware that a notifiable safetyincident has occurred; and provide support to them in relationto the incident, including when giving the notification.
3. Provide an account of the incident which, to the best of ourknowledge, is true of all the facts we know about the incidentat the date of notification.
4. Advise the relevant person what further enquiries we believeare appropriate.
5. Offer an apology.
6. Follow this up by giving the same information in writing; andproviding an update on the enquiries.
7. Keep a written record of all communication with the relevantperson.
8. If the relevant person cannot be contacted or declines tospeak to us, we must keep a written record of our attempts tocontact or speak to the relevant person.
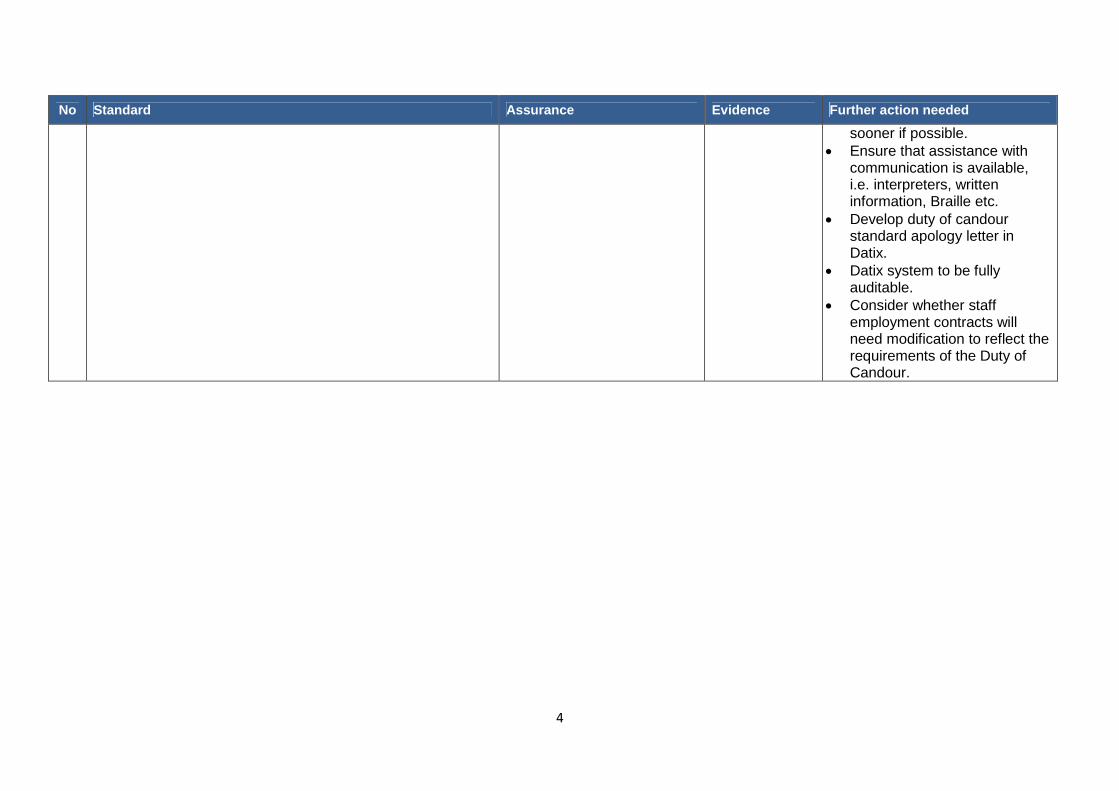
4
No Standard Assurance Evidence Further action needed
sooner if possible. Ensure that assistance with
communication is available,i.e. interpreters, writteninformation, Braille etc.
Develop duty of candourstandard apology letter inDatix.
Datix system to be fullyauditable.
Consider whether staffemployment contracts willneed modification to reflect therequirements of the Duty ofCandour.

LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Regulation 5: Fit and Proper Persons: Directors (FPPR)
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Susan Tyler, Director of WorkforceDevelopment
STRATEGIC:
PAPER AUTHOR: Cath Hill, Head of Corporate GovernanceGOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)SO1 We provide excellent quality, evidence-based, safe care that involves people and promotes
recovery and wellbeingSO2 We work with partners and local communities to improve health and lives
SO3 We value and develop our workforce and those supporting us SO4 We provide efficient and sustainable services
SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individualsOther – not yet a public documentMatters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
23

SUMMARY:
On 27 November 2014 the new Regulation 5: fit and proper persons: directors (part of theregulations relating to the Health and Social Care Act 2008) came into force and all NHSbodies (including Foundation Trusts) must now meet its requirements. This new regulationhas also been incorporated into the CQC’s inspection regime under the ‘well led’ domainand Trusts will now need to not only comply with the regulation, but provide evidence of thisto the CQC so as not to be found in breach of its conditions of registration or licence.
This paper seeks to summarise the main regiments of the regulation; outline the Trust’sobligations under the regulation; set out how the CQC will seek to ensure the Trust isapplying the regulation effectively (following the publication of their guidance also on 27November 2014); and assure the Board as to how the Trust is meeting the new regulationand what further action needs to be taken.
RECOMMENDATIONS:
The Board is asked to be assured of the action taken to ensure the Trust meets the newRegulation 5 and to be assured that any gaps are being addressed by the Director ofWorkforce Development and the Head of Corporate Governance.

1
Board of Directors’ Meeting 29 January 2015
The Health and Social Care Act 2008 (Regulated Activities) Regulations 2014Regulation 5: Fit and Proper Persons: Directors (FPPR)
1. Introduction
On 27 November 2014 the new Regulation 5: fit and proper persons: directors (part of theregulations relating to the Health and Social Care Act 2008) came into force and all NHSbodies (including Foundation Trusts) must now meet its requirements. This new regulationhas also been incorporated into the CQC’s inspection regime under the ‘well led’ domain andTrusts will now need to not only comply with the regulation, but provide evidence of this tothe CQC so as not to be found in breach of its conditions of registration or licence.
The aim of the regulation is to ensure that the individuals who are responsible for the overallquality and safety of care are fit and proper to carry out their role. It applies to Board levelappointments (executive and non-executive, permanent, interim and associate positions)irrespective of their voting rights. The regulation also applies to any governor of a foundationtrust if they sit on the Board of Directors as a governor representative. (This is notapplicable to LYPFT).
The Board is reminded that there is also a requirement for directors (and all governors) tomeet a Fit and Proper Person’s test in Monitor’s Provider Licence and the Trust has alreadyobtained evidence of directors’ and governors’ fitness through the declaration of interestprocess (annually and on appointment). However, the Monitor test is less demanding thanthe new test and the Board will need to assure itself that the Trust is in a position to meet thenew regulation.
This paper seeks to summarise the main regiments of the regulation; outline the Trust’sobligations under the regulation; set out how the CQC will seek to ensure the Trust isapplying the regulation effectively (following the publication of their guidance also on 27November 2014); and assure the Board as to how the Trust is meeting the new regulationand what further action needs to be taken.
This paper builds on the presentation to directors at the Board workshop on 13 November2014.
2. Responsibilities of the Trust
The Trust has always had a general obligation to: ensure that it only employs individualswho are fit for their role; that it has in place an ongoing process of appraisal anddevelopment; and under exceptional circumstances the ability to remove an individualdirector from the Board if they are not fit for the role. This regulation does not change thatobligation nor the current HR practices in obtaining evidence of suitability when appointingan individual; however, it places a greater burden of providing evidence to the CQC that theprocesses and procedures have been administered; it widens the scope of the backgroundchecks that will need to be made by the Trust; and requires a specific declaration to bemade that new Board members are fit and proper against a set of more detailed criteria.
In addition to the usual requirements of good character, health, qualifications, skills andexperience the regulation goes further by excluding people who have been responsible for,been privy to, contributed to or facilitated any serious misconduct or mismanagement(whether unlawful or not) in the course of carrying on a regulated activity or providing a

2
service elsewhere. This even relates to times when the individual was working in a morejunior capacity or working outside England.
It is the responsibility of the Chair of the Trust to discharge the requirements placed on theTrust in respect of newly appointed director. The Chair will need to confirm to the CQC thatthe fitness of all new directors has been assessed in line with the regulations and declare tothe CQC in writing that they are satisfied that they are fit and proper individuals for that role.
To meet the requirements of Regulation 5 the CQC requires the Trust to:
Be aware of the various guidelines available and to have implemented procedures inline with this best practice
Provide evidence to the CQC that appropriate systems and processes are in place toensure that all new directors and existing directors are, and continue to be, fit, andthat no appointments meet any of the unfitness criteria set out in Schedule 4 of theregulation
Make every reasonable effort to assure itself about an individual by all meansavailable
Make specified information about Board directors available to CQC when asked
Where a board member no longer meets the fit and proper persons requirement,inform the regulator in question where the individual is registered with a health careor social care regulator, and take necessary action to ensure the position is held by aperson meeting the requirements.
Appendix 1 sets out more detailed information about how the CQC expect NHS bodies toimplement the regulation. It also shows how the Trust is currently meeting theserequirements and what further action needs to be taken.
3. Responsibilities of the Care Quality Commission
The CQC will check and monitor the extent to which the Trust meets the regulation:
a) during an inspection;b) where there is a serious systemic failure of the Trust; orc) on receipt of any concerning information.
The CQC will not undertake a fit and proper person’s test of a director or determine what isserious mismanagement or misconduct, but will examine how the provider has dischargedits responsibility under the new regulation and will triangulate information received with anythey may hold.
a) During an inspection:
During the inspection process the CQC will assess whether the Trust is deliveringgood quality care. The specific key line of enquiry (KLOE) and prompts that arerelevant for the FPPR are under the ‘well-led’ domain.
Using the ‘well-led’ domain the CQC will confirm that the Trust has undertakenappropriate checks and is satisfied that, on appointment and subsequently, all new

3
and existing directors are of good character and are not unfit. This may involvechecking personnel files and records and the Trust may be required to providespecifc information listed in Schedule 3 of the regulation. The inspection team willwant to check the providers’ awareness of the various guidelines and that they haveimplemented procedures in line with best practice.
If following its enquiries the CQC find there has been a breach of the regulation it willconsider what enforcement action to take in accordance with CQC’s JudgementFramework and Enforcement Policy.
b) Serious systemic failure:
Where there is a serious systemic failure of a provider the CQC will carry out afocused inspection, including the FPPR aspects of corporate failure, and will use theevidence of such an inspection to inform its judgements about Regulation 5 and anybreaches that may have taken place.
They will not use the fact that a provider is in special measures as evidence or anindication that a director is unfit. However the CQC will, if necessary because ofspecial measures, assess the effectiveness and robustness of the processes for theappointment of directors.
The CQC will also have regard to any other information that it holds or obtains aboutdirectors in line with current legislation on when convictions, bankruptcies or similarmatters are to be considered ‘spent’. Where a director is associated with seriousmisconduct or responsibility for failure in a previous role, they will have regard to theseriousness of the failure, how it was managed, and the individual’s role within that.
c) Receipt of concerning information about the fitness of an existing Boardmember:
The CQC has set out a protocol for dealing with information received from a memberof the public or Trust staff about an existing Board member. This will be dealt with inline with the CQC’s safeguarding and whistle blowing protocols where relevant. Theprocess will be carried out by a panel led by the Chief Inspector of Hospitals and willinvolve the director and the Trust concerned.
It will be for the panel to assess if due process has been followed in respect ofassessing ‘fit and proper’, or if there is a need for further dialogue with the provideras to what action needs to be taken in respect of the director, or to assess ifenforcement action needs to be taken in respect of any breach.
Further guidance about how the CQC will ensure the regulation is being applied is containedin the CQC Regulation 5: fit and proposer persons: directors (guidance for NHS bodies)November 2014, which is available on the CQC website.
4. The Trust’s Response to the New Regulation
A benchmark exercise has been undertaken to ensure that the Trust is meeting therequirements of the regulation (as set out by the CQC) in respect of any new appointmentsand on an ongoing basis for existing directors (See Appendix 1). The actions taken so far toaddress the new requirements:

4
The Trust’s solicitors have reviewed the executive director contract and non-executive director appointment letter to ensure these meet the new requirements(these will be presented to the Remuneration Committee for executive directors andthe Appointments and Remuneration Committee for non-executive directors forapproval)
A self declaration form has been devised that will be used for new appointments andannually thereafter for all existing directors (this will be completed alongside theDeclaration of Interests form)
Further actions include:
Ensure the procedures for appointing executive and non-executive directors takeaccount of the checks under the FPPR proper on appointment
Values based questions to be included in all interviews Expand the background check carried out on candidates prior to the interview and
incorporate a process for asking questions at the interview about any mattershighlighted by these checks
Update of the Annual Declaration of Interests Procedure to include reference to thenew annual declaration for ongoing checks to be made
NED and ED appraisal processes to be amended to allow the assessment of thetemperament, character and empathy of directors.
5. In conclusion
The Fit and Proper Person’s Regulation (Regulation 5) came into effect on 27 November2014 which is a more substantial check than has been carried out previously. As this nowsits within the NHS legislative framework the Trust must not only abide by regulation butmust be able to provide evidence that it is doing so. The CQC will check and monitor theextent to which the Trust meets the regulation through three possible channels: during aninspection; where there is a systemic failure; or on receipt of concerning information about adirector and will decide whether or not to take regulatory action, and what action to take if itconsiders there has been a breach of the regulation.
In order to meet the new regulation the Trust has benchmarked itself against therequirements and taken action to address any gaps. This is set out at Appendix 1.
The Board is asked to be assured of the action taken to ensure the Trust meets the newRegulation 5 and to be assured that any gaps are being addressed by the Director ofWorkforce Development and the Head of Corporate Governance.
6. Sources of further information
Statutory Instrument 2014 No 2936 The Health and Social Care Act 2008 (RegulatedActivities) Regulations 2014 (Part 3, Section 1, Regulation 5; and Schedule 4, Part 1and Part 2)
CQC Regulation 5: fit and proposer persons: directors (guidance for NHS bodies)November 2014.

5
Requirements of the Fit and Proper Person’s Regulation andhow the Trust intends to assure itself of the suitability of individuals
(Executive and Non-executive Directors)
No Standard Assurance Evidence
ASSURANCES AT APPOINTMENT
1 Regulation 5(3)(a)
Providers should make every effort to ensure that allavailable information is sought to confirm that theindividual is of good character as defined in Schedule 4,Part 2 of the regulations.
Schedule 4 Part 2: Whether the person has been convicted in the
United Kingdom of any offence or beenconvicted elsewhere of any offence which, ifcommitted in any part of the United Kingdom,would constitute an offence.
Whether the person has been erased, removedor struck-off a register of professionalsmaintained by a regulator of health care orsocial work professionals.)
Employment checks are undertaken in accordance withNHS Employers’ Pre-employment Check Standards andinclude:
Two references, one of which must be most recentemployer
Qualification and professional registration checks
Right to work checks
Identity checks
DBS check.
Further action:
Self-declarations of fitness to be completed bycandidates (declaration form has been devised)
Consequences of false or inaccurate or incompleteinformation included in recruitment packs
NED appointment process
References
Documentation from pre-employmentchecks carried out as part of the standardHR appointment process
DBS checks where appropriate
Signed declarations from applicants
Register search results
Information held on the HR file.

6
No Standard Assurance Evidence
2 Regulation 5(3)(a)
Where a provider deems the individual suitable despitenot meeting the characteristics outlined in Schedule 4,Part 2 of these regulations (as listed above), the reasonsshould be recorded and information about the decisionshould be made available to those that need to beaware.
This would be the subject of discussion at theNominations Committee (for EDs) and at theAppointments and Remuneration Committee (forNEDs). The minutes would record such discussionand decisions.
Report and recommendations to the Council ofGovernors (for NEDs) or the Board of Directors (forEDs)
Decisions and reasons for decisions recorded inminutes
The Chair would take advice from internal andexternal advisors as appropriate.
Minutes of meetings.
Board/Council/committee agenda papers
Outcome of advice taken from advisors.
3 Regulation 5(3)(b)
Where specific qualifications are deemed by the provideras necessary for a role, the provider must make thisclear and should only employ those individuals that meetthe required specification, including any requirements tobe registered with a professional regulator.
Details of qualifications required is included withinthe job description / personal specification forrelevant posts
Request for any registration details are asked for onthe application form – the registers are checked byHR
Checks carried out as part of the pre-employmentchecks and through references.
Checks are made of the qualifications stated on theapplication form, particularly where are specificallyrequired for a particular post.
NED appointment process
Job description
Person specification
Application form
References
Recruitment / appointment process
Information held on HR files includingcopies of qualification certificates.

7
No Standard Assurance Evidence
4 Regulation 5(3)(b)
The provider should have appropriate processes forassessing and checking that the individual holds therequired qualifications and has the competence, skillsand experience required, (which may includeappropriate communication and leaderships skills and acaring and compassionate nature), to undertake the role;these should be followed in all cases and relevantrecords kept.
Employment checks include the verification ofcandidate’s qualifications particularly where theseare applicable to the role
Employment references.
The recruitment process also includes qualitativeassessment for executive directors
Decisions and reasons for decisions recorded innotes of the interview and shortlisting panels.
Further action:
Values-based questions will be included as standardin all ED and NED interviews (question set to beupdated)
NED appointment process
Application form
Job description
Person specification
Recruitment / appointment policy andprocedure
Values-based questions
Shortlisting and interview documentation.
5 Regulation 5(3)(b)
The provider may consider that an individual can beappointed to a role based on their qualifications, skillsand experience with the expectation that they willdevelop specific competence to undertake the role withina specified timeframe.
This would be the subject of discussion at theNominations Committee (for EDs) and at theAppointments and Remuneration Committee (forNEDs). The minutes would record such discussionand decisions.
Discussion and decisions would take place at theBoard of Directors (EDs) and Council of Governors(NEDs)
Actions would be subject to follow-up as part ofongoing review and appraisal for the individual.
Board / Council / committee agendapapers
Minutes of meetings
NED appraisal framework
ED appraisal framework

8
No Standard Assurance Evidence
6 Regulation 5(3)(c)
When appointing relevant individuals the provider hasprocesses for considering a person’s physical andmental health in line with the requirements of the role.
(People in a position of control must be physically andmentally fit. This does not mean that people who have along-term condition, a disability or mental illness cannotbe in such a position. This aspect of the regulationrelates to the ability to sustain the managementfunction).
Self declaration to be made on the OccupationalHealth form
All post-holders are subject to clearance byOccupational Health as part of the pre-employmentprocess.
Self declaration Occupational Health form
Occupational Health clearance.
7 Regulation 5(3)(c)
Wherever possible, reasonable adjustments are made inorder that an individual can carry out the role.
Self declaration of adjustments required
This is already included in the Trust’s disabilitypolicy.
Self declaration Occupational Health form
Advice from Occupational Health
Disability policy.
8 Regulation 5(3)(d)
The provider has processes in place to assure itself thatthe individual has not been at any time responsible for(see glossary), privy to (see glossary), contributed to, orfacilitated, any serious misconduct or mismanagement(see glossary) in the carrying on of a regulated activity(see glossary); this includes investigating any allegationof such potential behaviour.
Where the individual is professionally qualified, it mayinclude fitness to practise proceedings and professionaldisciplinary cases.
Two references one of which must be most recentemployer
Further action:
Self declaration of fitness including explanation ofpast conduct / character issues where appropriateby candidates.
Consequences of false or inaccurate or incompleteinformation to be included in recruitment packs
Pre-interview background checks on the individualand the organisations with which they have been
Recruitment Information pack
Pre-employment declaration
Reference Request for ED/NED
Outcome of the background checks carriedout
Interview documentation
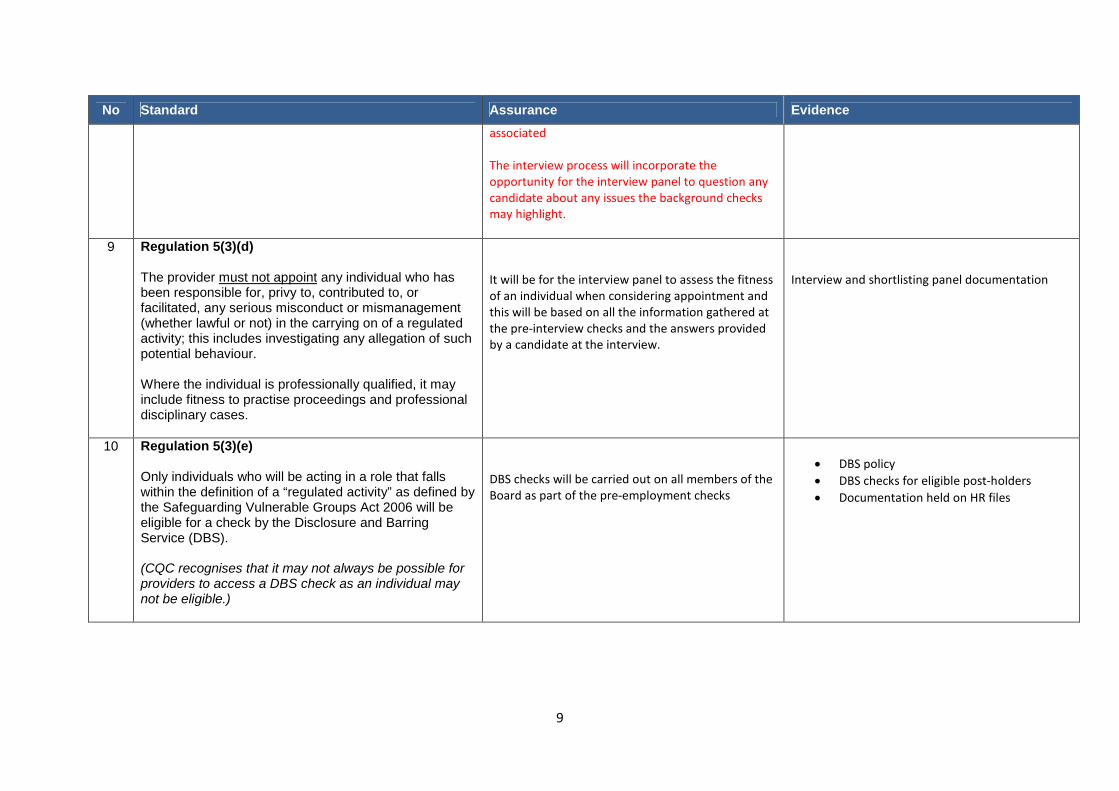
9
No Standard Assurance Evidence
associated
The interview process will incorporate theopportunity for the interview panel to question anycandidate about any issues the background checksmay highlight.
9 Regulation 5(3)(d)
The provider must not appoint any individual who hasbeen responsible for, privy to, contributed to, orfacilitated, any serious misconduct or mismanagement(whether lawful or not) in the carrying on of a regulatedactivity; this includes investigating any allegation of suchpotential behaviour.
Where the individual is professionally qualified, it mayinclude fitness to practise proceedings and professionaldisciplinary cases.
It will be for the interview panel to assess the fitnessof an individual when considering appointment andthis will be based on all the information gathered atthe pre-interview checks and the answers providedby a candidate at the interview.
Interview and shortlisting panel documentation
10 Regulation 5(3)(e)
Only individuals who will be acting in a role that fallswithin the definition of a “regulated activity” as defined bythe Safeguarding Vulnerable Groups Act 2006 will beeligible for a check by the Disclosure and BarringService (DBS).
(CQC recognises that it may not always be possible forproviders to access a DBS check as an individual maynot be eligible.)
DBS checks will be carried out on all members of theBoard as part of the pre-employment checks
DBS policy
DBS checks for eligible post-holders
Documentation held on HR files
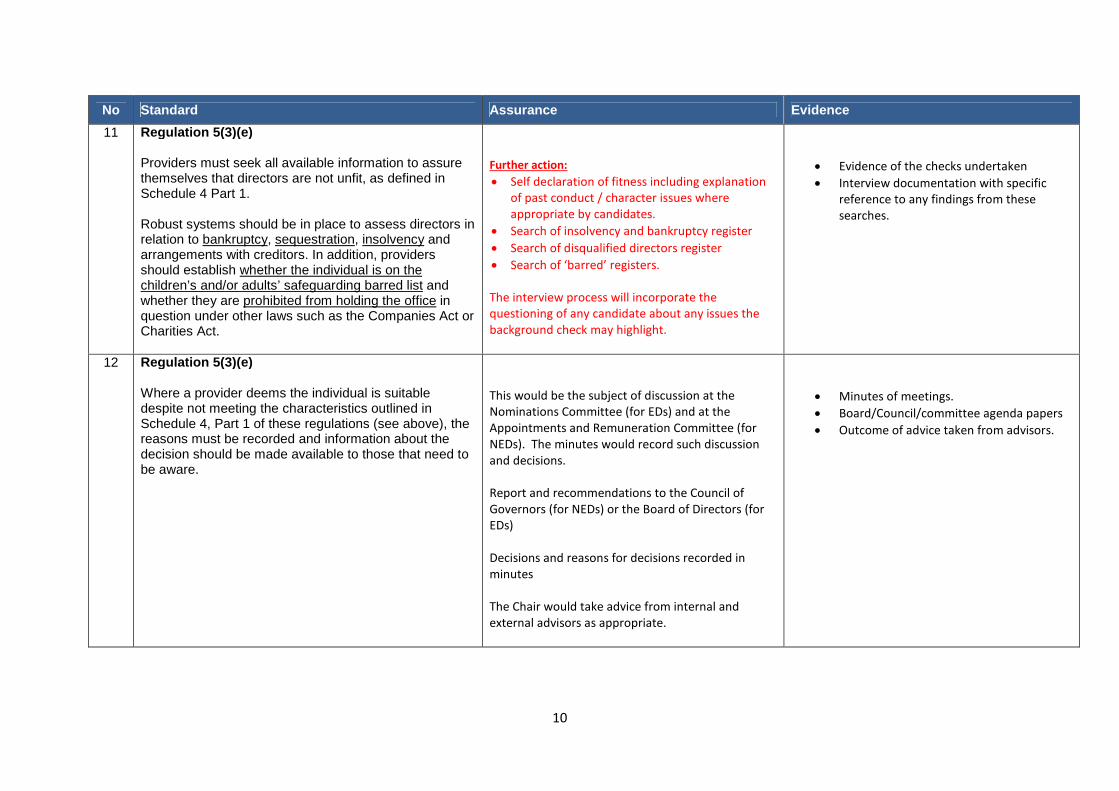
10
No Standard Assurance Evidence
11 Regulation 5(3)(e)
Providers must seek all available information to assurethemselves that directors are not unfit, as defined inSchedule 4 Part 1.
Robust systems should be in place to assess directors inrelation to bankruptcy, sequestration, insolvency andarrangements with creditors. In addition, providersshould establish whether the individual is on thechildren’s and/or adults’ safeguarding barred list andwhether they are prohibited from holding the office inquestion under other laws such as the Companies Act orCharities Act.
Further action:
Self declaration of fitness including explanationof past conduct / character issues whereappropriate by candidates.
Search of insolvency and bankruptcy register
Search of disqualified directors register
Search of ‘barred’ registers.
The interview process will incorporate thequestioning of any candidate about any issues thebackground check may highlight.
Evidence of the checks undertaken
Interview documentation with specificreference to any findings from thesesearches.
12 Regulation 5(3)(e)
Where a provider deems the individual is suitabledespite not meeting the characteristics outlined inSchedule 4, Part 1 of these regulations (see above), thereasons must be recorded and information about thedecision should be made available to those that need tobe aware.
This would be the subject of discussion at theNominations Committee (for EDs) and at theAppointments and Remuneration Committee (forNEDs). The minutes would record such discussionand decisions.
Report and recommendations to the Council ofGovernors (for NEDs) or the Board of Directors (forEDs)
Decisions and reasons for decisions recorded inminutes
The Chair would take advice from internal andexternal advisors as appropriate.
Minutes of meetings.
Board/Council/committee agenda papers
Outcome of advice taken from advisors.

11
No Standard Assurance Evidence
On-going Assessment
13 Regulation 5(3)(a)
Robust systems must be in place to ensure continuousassessment of the temperament, character and empathyof staff. It is not possible to outline every character traitan individual should have but among them we wouldexpect to see that the diligence processes take accountof honesty, trust and respect.
Further action:
NED and ED appraisal process will need to beupdated to take account of this requirement.
NED appraisal process documentation
ED appraisal process documentation
14 Regulation 5(3)(a)
If a provider discovers information that suggests anindividual is not of good character, as defined inSchedule 4, Part 2 of the regulations, after they havebeen appointed to a role the provider must takeappropriate and timely action to investigate and rectifythe matter.
Schedule 4 Part 2: Whether the person has been convicted in the
United Kingdom of any offence or beenconvicted elsewhere of any offence which, ifcommitted in any part of the United Kingdom,would constitute an offence.
Whether the person has been erased, removedor struck-off a register of professionalsmaintained by a regulator of health care orsocial work professionals.)
Annual self declaration of FPPR to be carried out
Any information provided from a third party wouldbe investigated under the whistle blowing /safeguarding procedures (dependent on the natureof the information received)
Disciplinary procedure may also be applicabledepending on the outcome of any investigation.
Revised contracts allow for termination in the eventof non-compliance with regulations and otherrequirements.
Self declaration forms
Contracts of employment (for EDs anddirector-equivalents)
Terms and conditions of service in theappointment letters (for NEDs)
Disciplinary policy and procedure
Whistle blowing procedure
Safeguarding procedure
Outcome of any investigation.

12
No Standard Assurance Evidence
15 Regulation 5(3)(e)
If a provider discovers information that suggests anindividual is unfit (in relation to Schedule 4 Part 1) afterthey have been appointed to a role, the provider musttake appropriate and timely action to investigate andrectify the matter.
Schedule 4 Part 1In relation to bankruptcy, sequestration,insolvency and arrangements with creditors. Inaddition, providers should establish whether theindividual is on the children’s and/or adults’safeguarding barred list and whether they areprohibited from holding the office in questionunder other laws such as the Companies Act orCharities Act.
Annual self declaration of FPPR to be carried out
Any information provided from a third party wouldbe investigated under the whistle blowing /procedure
Disciplinary procedure may also be applicabledepending on the outcome of any investigation
Revised contracts allow for termination in the eventof non-compliance with regulations and otherrequirements.
Self declaration forms
Contracts of employment (for EDs anddirector-equivalents)
Terms and conditions of service in theappointment letters (for NEDs)
Disciplinary policy and procedure
Whistle blowing procedure
Outcome of any investigation
16 Regulation 5(3)(e)
Where a provider deems the individual is suitabledespite not meeting the characteristics outlined inSchedule 4, Part 1 of these regulations (see above), thereasons must be recorded and information about thedecision should be made available to those that need tobe aware.
This would be the subject of discussion at theNominations Committee (for EDs) and at theAppointments and Remuneration Committee (forNEDs). The minutes would record such discussionand decisions.
Report and recommendations to the Council ofGovernors (for NEDs) or the Board of Directors (forEDs)
Decisions and reasons for decisions recorded inminutes
The Chair would take advice from internal andexternal advisors as appropriate.
Minutes of meetings.
Board/Council/committee agenda papers
Outcome of advice taken from advisors.

13
No Standard Assurance Evidence
17 Regulation 5(6)
The provider must regularly review the fitness ofdirectors to ensure that they remain fit for the role theyare in. The provider must determine how often to reviewfitness based on the assessed risk to business deliveryand / or to the people using the service posed by theindividual and / or role.
Post-holders undertake annual declarations offitness to continue in post.
Annual declaration forms
Outcome of the checks undertaken
18 Regulation 5(6)(a)
The provider has arrangements in place to respond toconcerns about a person’s fitness (as per paragraph 3 ofthe regulations) after they are appointed to a role,identified by itself or others, and these are adhered to.
Annual self declaration of FPPR to be carried out
Any information provided from a third party wouldbe investigated under the whistle blowing /safeguarding procedures (dependent on the natureof the information received)
Disciplinary procedure may also be applicabledepending on the outcome of any investigation.
Revised contracts allow for termination in the eventof non-compliance with regulations and otherrequirements.
Self declaration forms
Contracts of employment (for EDs anddirector-equivalents)
Terms and conditions of service in theappointment letters (for NEDs)
Disciplinary policy and procedure
Whistle blowing procedure
Safeguarding procedure
Outcome of any investigation.
19 Regulation 5(6)(a)
The provider investigates, in a timely manner, anyconcerns about a person’s fitness or ability to carry outtheir duties, and where concerns are substantiated,proportionate, timely action is taken; the provider mustdemonstrate due diligence in all actions.
As above As above

14
No Standard Assurance Evidence
20 Regulation 5(6)(a)
Where a person’s fitness to carry out their role is beinginvestigated, appropriate interim measures may berequired to minimise any risk to service users.
This would be picked up as part of the disciplinaryprocedure
Disciplinary procedure
21 Regulation 5(6)(b)
The provider informs others as appropriate aboutconcerns/findings relating to a person’s fitness; forexample, professional regulators, CQC and otherrelevant bodies, and supports any relatedenquiries/investigations carried out by others.
This will done as and when required Documentation relating to the report thatneeds to be made will be held on the HRfile of the individual.

15
Glossary
“timely” As soon as can be achieved in order to minimise harm or potential harm to people receiving services. We would assess action taken on a case by casebasis, but would expect providers to take immediate action to protect people from harm and introduce and complete investigations quickly,evidencing reasons for any delay that any reasonable trust would avoid.
“Seriousmisconduct ormismanagement”
Behaviour that would constitute a breach of any legislation/enactment that CQC deems relevant to meeting these regulations or their componentparts. “Serious misconduct” might be expected to include assault, fraud and theft. “Mismanagement” might be expected to include mismanaging fundsand/or not adhering to recognised practice, guidance or processes regarding care quality within which the individual is meant to work. These are notexhaustive lists.
“Responsible for,contributed to orfacilitated”
There is evidence that a person has intentionally, or through neglect, behaved in a manner that would be considered to be, or would have led to,serious misconduct or mismanagement
“Privy to” There is evidence that could lead the provider to reasonably conclude that a person was aware of serious misconduct or mismanagement but did not
take the appropriate action to ensure it was addressed
“RegulatedActivity”
Activities set out in Schedule 1, Regulated Activities of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014. Schedule 1 covers
the provision of: personal care; accommodation for person who require nursing or personal care; accommodation for person who requires treatment
for substance misuse; treatment of disease, disorder or injury assessment or medical treatment for person detained under the 1983 Act; surgical
procedures; diagnostic and screening procedures; management of supply of blood and blood derived products etc.; transport services, triage and
medical advice provided remotely; maternity and midwifery services.; termination of pregnancies; services in slimming clinics; nursing care; family
planning services.
LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
PAPER TITLE: Draft Minutes from the Council of Governors’ meeting 4 November2014
DATE OF MEETING: 29 January 2015 CATEGORY OF PAPER(please tick relevant box)
LEAD DIRECTOR: Frank Griffiths – Chair of the TrustSTRATEGIC:
PAPER AUTHOR: Cath Hill – Head of Corporate GovernanceGOVERNANCE:
INFORMATION:
IMPACT ON THE TRUST’S STRATEGIC GOALS (please tick relevant box)G1 People achieve their agreed goals for improving health and improving lives G2 People experience safe care G3 People have a positive experience of their care and support
IMPACT ON THE TRUST’S STRATEGIC OBJECTIVES (please tick relevant box)SO1 We provide excellent quality, evidence-based, safe care that involves people and promotes
recovery and wellbeingSO2 We work with partners and local communities to improve health and lives
SO3 We value and develop our workforce and those supporting us
SO4 We provide efficient and sustainable services
SO5 We govern our Trust effectively and meet our regulatory requirements
STATUS OF PAPER
To be taken in the public session (Part A)
To be taken in private session (Part B) - If the paper is to be taken in the private session pleaseindicate which criterion is applicable:
Legal advice relating to legal proceedings (actual or possible)Negotiations in respect of employee relations where they are of a confidential natureProcurement processes and contract negotiationsInformation relating to identifiable individuals or groups of individualsOther – not yet a public documentMatters exempt under the Freedom of Information Act (quote section number)
AGENDAITEM
25

SUMMARY:
It is good governance for the Board of Directors and Council of Governors to share theirminutes and this paper presents the draft minutes from the Council of Governors’ meetingheld on 4 November for information. These minutes are still in draft and will be presentedto the Council at its meeting on 18 February 2015 for approval.
RECOMMENDATIONS:
The Board of Directors is asked to receive the draft minutes from the Council of Governorsand be informed of the matters discussed at the meeting.

1
Agenda item 25
LEEDS AND YORK PARTNERSHIP NHS FOUNDATION TRUST
Minutes of the Public Meeting of the Council of Governorsheld at 14:45 on Tuesday 4 November 2014, in the Large function
Room, St George’s Centre, Leeds LS1 3BR
PRESENT:
Frank Griffiths – Chair of the Trust
Public Governors Service User GovernorsJenny Roper Ann ShuterPhilip Jones Claire Woodham
Jackie Ainsley-StringerRichard BrownSteve Howarth
James Morgan
Carer Governors Staff GovernorsAnnie Dransfield Gary MatfinJulia Raven Andrew JohnsonAndy Bottomley Mark Wills
Alan Procter Pamela Morris
Appointed GovernorsAnt HanlonColin Clark
IN ATTENDANCE:Chris Butler, Chief ExecutiveJill Copeland, Chief Operating OfficerSusan Tyler, Director of Workforce DevelopmentAnthony Deery, Interim Director of NursingGill Taylor, Non-executive DirectorCarl Thompson, Non-executive DirectorMargaret Sentamu, Non-executive DirectorGary Bouch, PR and Communications ManagerCath Hill, Head of Corporate Governance (secretariat)Keisha Allen, Governance Support Assistant (minutes)1 member of the public

2
Action14/080 Welcome and Introductions (agenda item 1)
The Chair opened the public session of the meeting at 14:30 andwelcomed everyone.
14/081 Apologies (agenda item 2)
Apologies were received from, Maria Trainer (Service User:Leeds Resident); Heather Simpson, (Clinical Staff, Leeds andYork & North Yorkshire); Andrew Marran (Public: Leeds); andNiccola Swan (Public: Rest of England and Wales).
14/082 Governors’ Declaration of Interests (agenda item 3)
No member of the Council declared a conflict of interest inrespect of any item on the agenda.
14/083 Opportunity to Receive Comments or Questions fromMembers of the Public (agenda item 4)
There were no questions from members of the public.
14/084 Minutes of the Public Meeting held on 2 September 2014(agenda item 5.1)
The minutes of the public Council of Governors’ meeting held on2 September 2014 were agreed as an accurate record.
14/085 Minutes of the Annual Members’ Meeting held 23 September2014 (agenda item 5.2)
The minutes of the Annual Members’ Meeting held 23 September2014 were agreed as an accurate record.
14/086 Meeting the Needs of People who are Deaf or Hard ofHearing (agenda item 6.1)
Mrs Tyler presented a paper on the needs of people who are deafor hard of hearing to the Council noting that this was in response

3
to an item that had come to the last Council of Governors’meeting where a question had been raised regarding whatprovision was in place to ensure staff were trained in British SignLanguage (BSL).
Mrs Tyler reported that where following a training needs analysisit has been identified that staff would be required to use BSL itwould be possible for them to access a programme provided bythe Leeds Society for Deaf and Blind People. Mrs Tyler reportedthat so far the Trust had provided four training sessions to staffand that currently fifty staff had undertaken the training. Mrs Tylernoted that staff were trained in basic skills and that it was not afull BSL accredited programme but that it will provide staff with anawareness of how to support service users who have deaf relatedconditions.
Mrs Tyler noted that the other aspect of the paper sets outinterpretation services and that the Leeds Society for Deaf andBlind People come into the Trust to provide a lip-speak service.Mrs Tyler indicated that a protocol had been implemented withinthe Trust which guides staff as to when it would be necessary toseek services from the society.
Mrs Tyler commented on the suggestion as to whether theprogramme should be available to all staff indicating that theTrust was not currently seeking to roll out the programme to allstaff but that the training programme was specifically tailored tothe needs of the individual employees and the role they fulfilwithin the Trust.
Mr Griffiths asked for the views of the Council. Ms Woodhamstated that it was a good training programme thus far but that inthe summary of the paper regarding the current training it wasnoted that staff were trained to interpret basic words and phrasesbut not whole conversations. Ms Woodham commented thatservice users often need someone to talk to particularly if theyare in distress and if no one is available to understand theirconcerns this could be detrimental to their recovery. Shesuggested that if an interpreter is unavailable when the individualis in need of one that a member of staff should be on call andhave sufficient skills to support that individual.
A discussion followed with regard to the small number of stafftrained to provide support to service users with hearing related

4
conditions and it was noted that another way they can haveconversations with service users is via the use of a computer ortext messages and that sign language skills are not necessarilyalways required. However, it was noted that although technologymay be an alternative for some service users it was necessary tobear in mind the needs of elderly service users who may not beable to communicate in such a way.
With respect to providing support to service users a number ofquestions were raised such as; the number of service users whowere profoundly deaf; whether there was signage at serviceusers’ bedsides to indicate they have a hearing loss; and whetherthere were facilities to repair and/or replace the batteries ofhearing aids.
With regard to the number of service users within our serviceswho have hearing difficulties, Mrs Tyler replied that she wasunable to provide the answer at this time but that she wouldascertain the information and report back to governors. In respectof having signage by the bedside Mrs Tyler noted that any needswould be recorded in the service users’ notes.
In regard to the training programme Mrs Tyler responded that ifthere were specific training needs in a particular clinical area itwould first need to be identified within the team and the Trustwould then respond to this need to ensure service users areprovided with adequate support.
Ms Shutter commented that she knows someone who uses signlanguage and speaks to people who are deaf and that she wouldprovide further details of this. Mrs Hill agreed to speak to MsShutter and obtain the details.
Mr Griffiths also responded that the discussion had drawnattention to a range of issues including what provision was inplace at the Mental Health Act hearings noting the need for thereto be more than basic information conveyed and that in theseinstances there would be a need for a full translation service.
Mr Griffiths also noted the separate matter of language andcultural issues noting that there have been some issues withregard to our ability to engage effectively with service users. Inaddition, Dr Willis noted that some service users with autisticspectrum disorder would value some form of sign language
ST
CH
5
support.
The Council of Governors received and noted the informationabout the provision of BSL training within the Trust.
14/087 Cumulative Actions – Actions Outstanding from PreviousCouncil of Governors’ Meetings (agenda item 7)
Mrs Hill presented the action log which showed those actionsagreed by the Council at previous meetings; those that had beenrecently completed; and those that were still outstanding.
Mrs Hill reported that in respect of log number 56 there was nowa new refreshed membership of the Appointments andRemuneration Committee which would be confirmed at a laterpoint in the agenda and that the procedure will go to its meetingin January.
With regard to log number 66 Mrs Hill reported that she hadchecked with the complaints team and that the matter is currentlybeing dealt with noting that when it is concluded an update onany lessons learnt will be brought back to the Council through theIntegrated and Quality Performance Report.
The Council of Governors noted the actions outstanding fromprevious meetings and was assured of progress.
14/088 Chair’s Report (agenda item 8)
Mr Griffiths presented to the Council the Chair’s report noting theresignation of Mr Paul Cockcroft, non-clinical staff governor forLeeds and York & North Yorkshire, who stepped down on the 14October 2014. The Council thanked Paul for his hard work andcontribution as a staff governor. Mr Griffiths indicated that hewould write to Paul to express the Council’s appreciation.
Mr Griffiths reminded the Council of the resignation the ChiefNurse and Director of Quality Assurance, Ms Beverly Murphy,and advised the Council that Mr Anthony Deery commenced withthe Trust on 1 November as the Interim Director of Nursing toensure there was no vacancy on the Board in respect of thisstatutory role.
FG

6
Mr Griffiths advised the Council that there is currently an electionprocess underway. Mrs Hill stated that even though the electionhad not concluded she was very pleased with the response andthat a final update of the elections process would be published onthe Trust’s website. Mrs Hill noted that she would keep theCouncil updated of progress and report on the outcome once theelection comes to an end.
Mr Griffiths reported that the Care Quality Commission inspectionwhich had commenced on 29 September 2014 had been verydemanding on those staff involved and had lasted for more than aweek. Mr Griffiths indicated that it was likely that feedback fromthe inspection would highlight areas where there is need forimprovement but overwhelming the early feedback had beenpositive. The Council was advised that a Quality Summit meetingis scheduled to be held in December where the final outcome ofthe inspection will be reported. Mr Griffiths indicated that in hisview there was noticeably a great deal of good practice takingplace in the Trust particularly in view of the positive way in whichservices had been described by the CQC at the early feedbackstage. Mr Griffiths also indicated that all staff, governors, non-executive, executives and carers should feel proud of theircontribution to the way services are provided and for the hardwork undertaken to ensure the inspection achieved a successfuloutcome.
CH
The Council received the Chair’s Report and noted the content.
14/089 Proposals for Bootham Park Hospital and Lime Trees –update on progress (agenda item 9)
Ms Copeland presented a paper to the Council which provided anupdate on the service improvements in York with regard to theestate noting that the inpatient services for CAMHS at Lime Treeswill be relocated to Mill Lodge in the week beginning 15December and that work is expected to be completed within theagreed timescale. It was noted that the capital funding for CherryTree House has been approved by NHS England and that on the17 November work will begin on site with the 9 April being thedate scheduled for when services will commence at the unit.
With regard to Bootham Park Hospital Ms Copeland reported that

7
the plans for the refurbishment for Ward 1 and Ward 6 which areto become the new female and male wards have been agreed byNHS Property Services Ltd (NHSPS) and that this had inlcudedinput from clinicians in the service to ensure there is the rightconfiguration with regard to the rooms and therapy space. MsCopeland reported that the Vale of York Clinical CommissioningGroup (VoY CCG) and NHSPS are completing the business caseand once completed they will be forwarded to NHS England forapproval and for the funding to be released. Ms Copelandreported that as yet there is not a detailed timetable for therefurbishment from NHSPS but that a meeting was schedulednext week with the Bootham Park Programme Board and thatMrs Hanwell would be attending and would seek assurance withregard to a detailed timetable for the refurbishment.
Ms Copeland advised the Council that there were risks arounddelivery noting that the main risk is with regard to getting thecapital funding signed off by NHS England in respect of thechanges in Bootham Park Hospital. Ms Copeland also noted thatthere was a risk with regard to the work clinical staff will have toundertake with service users at a time when the Trust will betendering for mental health services for York.
Ms Copeland noted that at the last Council of Governors’ meetingshe was asked about service users involvement and indicatedthat this had now been detailed in the paper.
Dr Willis asked about the estate developments that would takeplace following the move from Lime Tress to Mill Lodge, inparticular the location for a new South West Locality Hub, notingits importance in the community service redesign. Ms Copelandassured the Council that it had been raised with NHSPS and theVoY CCG as the next priority, but that as yet no timescales hadbeen identified.
The Council of Governors received the paper, noted the contentand was assured of the progress made.
14/090 Non-executive Director Presentation in respect ofPerformance (agenda item 10 and 10.1 )
Prof Thompson gave an update on the quality of services and theperformance of the Board of Directors. He noted that the Trust

8
was performing relatively well but that as chair of the QualityCommittee he considered that there was consistentunderperformance in some key areas. In particular he expressedconcern that compulsory training was not being completed by allstaff; that about one third of staff were not being appraised in ameaningful way; that the complaints process was not meeting itstarget for responding; that with regard to the care programme,some service users were not always involved in their care plansand neither were all plans being reviewed. Prof Thompson notedthat the executive directors were concerned about progress inthese areas.
Prof Thompson noted that whilst there were plans in place toaddress these matters there was probably the need to do somethings differently and reported that to support this, the Trust hadseconded someone with expertise in organisational behaviouralchange.
With regard to the financial position of the Trust, Prof Thompsonreported that whilst the Trust was in a relatively sound positionthere were foreseeable challenges which the Board will have toaddress in the coming months; in particular underperformanceagainst cost improvement plans noting that the Board waschallenging this.
Prof Thompson went on to discuss the uncertainty around theprocess for the tender for the York services and the implication itwould have on the Trust if it was decided not bid for theseservices. He stated the Board would need to discuss theproposed course of action and look at the pros and cons ofbidding for the services.
Prof Thompson briefly spoke about the Trust’s regulators. Inrespect of the Care Quality Commission inspection and theQuality Summit meeting in December noting the praise receivedabout the services but also the areas highlighted forimprovement. He also advised the Council that the Trust hadreceived an amber rating from Monitor in respect of the StrategicPlan and that the Board will be discussing this in more detail.
Prof Thompson also advised the Council that following MsMurphy’s resignation that interviews for a replacement would takeplace shortly and that the Council would be informed when anappointment was made.

9
Prof Thompson updated the Council on two informationinitiatives. The first being accessible indicators for ward teams toshow how well they are doing as an individual team and also incomparison to other teams, noting that this will be launchedwithin the next few months; and the second being a qualitywebsite which would be accessible through the Trust’s website.
Prof Thompson lastly assured the Council that although there arechallenges, the core business of the Trust is to deliver safe,effective, quality care and treatment to service users and that hewas assured that the Trust was doing that and that it wasperforming very well.
Mr Howarth asked about staffing levels noting that the reportindicates a shortage of staff in some areas and asked if there was alink to the low uptake of staff appraisals and compulsory trainingnoting that inadequate staffing levels could affect the completionof appraisals and compulsory training. Prof Thomson replied thatthe aspect of appraisal and training is a complex one. However,with regard to safe staffing levels versus therapeutic staffinglevels Prof Thompson noted the need to first ensure the overallsafety of service users and when this was met to then look atwhat further resources were needed to achieve levels to providetherapeutic activities. However Prof Thompson noted that therewas a need to recognise there are only finite resources and thatany such initiative may impact on resources elsewhere.
Ms Woodham noted that the performance report showed that theperiod before re-admission following an inpatient episode wasonly 9.5 days. Prof Thompson noted that this related to a smallnumber of people overall. The Council also noted that this wasnot clear from the report and suggested further narrative could beadded to the report. Mrs Morris asked about the seven dayfollow-up and noted that where a service user refuses to engagewith the Trust following discharge that this counts against theTrust. Ms Copeland acknowledged that this was the case andexplained that this is why the Monitor target is not set at 100%.
Ms Copeland assured the Council with regard to the costimprovement plans noting that it was not that these would not bedelivered but that there had been some delays as a result of theTrust waiting for approval from the Leeds Clinical CommissioningGroup to set up a crisis unit at the Becklin Centre. Ms Copeland

10
also reported that extra income had been received and thatoverall the financial position was good.
With regard to therapeutic staffing levels Ms Copeland advisedthe Council that this is being reviewed and outlined an example ofwhere this had occurred, but noted that the Trust is only currentlyasked to report on safe staffing levels.
With regard to the York tender, Ms Copeland assured the Councilthat although the Board has not made a final decision with regardto how to proceed that work was on-going in preparation ahead offurther tender information being released by the Vale of YorkCCG.
The Council received the report from the non-executive directorsand noted the assurances received as to how they areindividually and collectively challenging the executive directors onthe performance of the Board including are areas of lowperformance.
14/091 Annual Report from the Audit Committee – 2013/14 (agendaitem 11)
Dr Taylor presented to the Council the Annual Report from theAudit Committee on behalf of Mrs Julie Tankard (the chair of theAudit Committee) noting that the work the committee does isindependent of the management of the Trust because it needs tobe in a position to give an objective view on matters in order toprovide assurance to the Board. She explained that the meetingswere well attended and the committee sets and agrees theannual work plan for both internal and external auditors and forclinical audit.
Dr Taylor indicated that the purpose of the report is to set out thework undertaken in 2013/14 and she briefly outlined the mainareas covered by the committee as set out in the report.
Mr Jones asked whether the Council should be made aware ofthe level of fraud that occurs within the Trust, and also receive areport in respect of the recent fraud case. Mr Griffiths informedthe Council that reports on the current case will be in the publicdomain within the next few days but that until the case iscompleted information cannot be released and that the Trust

11
must be careful not to adversely affect the proceedings. TheCouncil was given assurance that when the final outcome of thecase is known it would be kept informed. He also advised theCouncil that the Audit Committee receives up to date reports oncounter fraud from the Local Counter Fraud Sepcialist. Mr Butleralso sets out the local and national processes for identifying andinvestigating fraud.
Mr Bottomly asked about the timescale for the Council receivingthe report. Mrs Hill explained why the annual report takes time tocome to the Council of Governors, noting that it sets out the workof the committee for a financial year and is written after the end ofthat year; that it has to go to the Board of Directors first and to theCouncil of Governors following that. Mrs Hill advised that theAnnual Reporting Manual (ARM) issued by Monitor has nowasked for further information to be included in the Trust’s AnnualReport and for the Audit Committee annual report to go to theBoard in May; that this has shifted the timeline which will meanthe Council of Governors should receive the report in July.
The Council of Governors received the 2013/14 Annual Reportfor the Audit Committee.
14/092 Update on progress with the Governors’ TrainingProgramme (Evolve) (agenda item 12)
Mrs Tyler presented a paper regarding an update on progresswith the governors’ training programme. Mrs Tyler reported thatNatasha Furness who was responsible for putting together thegovernors’ training programme had resigned from her post inSeptember 2014 and that work going forward will be covered byRichard Ellis, from the Learning and Development Team.
Mrs Tyler noted that following a training needs analysis whichwas issued to all governors, that a number of training needs havebeen identified. Mrs Tyler noted that it is envisaged that theremay be some opportunity for cross party working with otherregional and local foundation trusts in order to share resources.
The Council noted the update on progress with the Governors’Training Programme.

12
14/093 Ratification of the Governors’ Expenses Procedure (agendaitem 13)
Mrs Hill presented the governors’ reimbursement of expensesprocedure for ratification noting that this relates only to electedgovernors and that the procedure was seen at the Membershipand Development Committee and also the Finance and BusinessCommittee. Governors were reminded that they are entitled toclaim expenses and can do so via the governance office. Mrs Hillagreed to write to all members of the Council regarding this andwould enclose a supply of expenses claim form.
CH
The Council received the governors’ reimbursement of expensesprocedure and ratified the amended procedure.
14/094 Draft minutes from the Appointments and RemunerationCommittee meeting held 2 September 2014 (agenda item 14)
The Council of Governors received the draft minutes from theAppointments and Remuneration Committee meeting held 2September 2014, noted the contents and was assured of thework of the committee as set out in its Terms of Reference.
14/095 Outcome of the elections to the Appointments andRemuneration Committee (agenda item 14.1)
The Council of Governors approved the appointment of JuliaRaven and Steve Howarth to the Appointments andRemuneration Committee and noted that there is still one vacantseat for appointed governors on the committee.
14/096 Ratification of the Terms of Reference for the Appointmentsand Remuneration Committee (agenda item 14.2)
The Council received and ratified the refreshed Terms ofReference for the Appointments and Remuneration Committee
14/097 Appointment of the Deputy Chair of the Trust (agenda item15)

13
The Council received a paper which recommended that StevenWrigley-Howe should be appointed for a period of one year witheffect from 6 November 2014 as Deputy Chair of the Trust. TheCouncil approved this appointment and thanked Mr Woodhousefor his contributions to the role of Deputy Chair within the lasttwelve months.
The Council appointed Steven Wrigley-Howe for a period of oneyear with effect from 6 November 2014.
14/098 Approval of Membership Campaign 2015/16 (agenda item 16)
Mr Howorth presented a paper on the proposed four themes forthe 2015/16 membership campaign noting that members at theAnnual Members Day were asked to vote on the preferred themeand they suggested one relating to men’s health: the “Man-UP”campaign. It was noted that the Membership and Engagementteam had met with a small group of governors to agree theprogramme for next year.
The Council of Governors was asked to support the “Man-UP”campaign as recommended by the small governor working group.
The Council of Governors noted the contents of the paper; andapproved the “Man Up?” campaign for 2015-16.
14/099 Engagement with people whose views are not fullyrepresented (agenda item 17)
Mr Howorth introduced a paper regarding the engagement withpeople whose views are not fully represented, noting that thistopic derived from a previous Council of Governors’ meeting andwas discussed at the Membership and Development Committee.Mr Howorth suggested that a small task and finish group be setup to include governors to look at some of the suggestionsidentified and collate ideas which would be discussed at theFebruary’s Council of Governors’ meeting for ratification.
Mr Howorth briefly outlined the groups that the task and finishgroup would look at namely: people with learning disabilities;people with dementia and young people and children. Mr Hanlonnoted that people from Black and Ethnic Minority Communities

14
(BMEs) were excluded from the paper even though there was ahigh number of BMEs (21% approximately in the Leedscommunity) with mental illnesses. Mr Griffiths responded thatindeed Leeds was a diverse city with various communities and MrHoworth agreed with the observation noting that he had onlybeen asked to look specifically at the three groups outlined in thepaper. Members of Council were keen to get involved in a taskand finish group with the objective of considering how better toengage with these groups. Mr Howorth asked for the governorvolunteers to contact him if they would like to be involved.
COG
The Council considered the contents of the paper and agreed tosetting up a task and finish group of governors in order torepresent the views of these groups and report back to theFebruary Council meeting.
14/100 Ratification of the percentage uplift for non-executivedirectors (agenda item 14.3)
Mr Griffiths declared an interest in this item and handed the chairto Mrs Roper.
Mrs Roper noted that the Appointments and RemunerationCommittee had agreed that the uplift for non-executive directorswould be in line with the 1% uplift awarded to those Trust staff onAgenda for Change who were not in receipt of an annualincrement.
Mr Johnson asked how this 1% increase would affect the pensionfor non-executive directors. Mrs Hill assured the Council that non-executive directors do not make pension contributions from theirremuneration and as such the uplift is on the same footing as thenon-consolidatied payment to staff.
The Council ratified the recommendation from the Appointmentsand Remuneration Committee that a 1% uplift in respect of theChair of the Trust and other non-executive directors be applied andbe backdated to 1 April 2014.
14/101 Minutes of the meetings of the Board of Directors held on 31July 2014 (agenda item 18)

15
The Council received and noted the Minutes of the meetings ofthe Board of Directors held on 31 July 2014.
14/102 Any Other Business (agenda item 19)
There was no other business discussed at the meeting.
14/103 Question / comments from Members of the Public (agendaitem 20)
A member of the public raised a concern with regard to peoplewith a personality disorder not being represented in the Council,in particular males with a personality disorder. Mr Howorth repliedthat these views would be fed into the task and finish group whichwill look at engaging with people whose views are not fullyrepresented and agreed to liaise with the gentleman. AH
The chair of the meeting closed the public meeting of the Council of Governors ofLeeds and York Partnership NHS Foundation Trust at 16:20 and thanked governors
and members of the public for their attendance.

16
COUNCIL OF GOVERNORS’ ACTION SUMMARY(PUBLIC MEETING)
Meeting held 4 November 2014
MINUTE ACTION SUMMARY (PUBLIC MEETING) LEAD
14/086 Meeting the Needs of People who are Deaf or Hard ofHearing (agenda item 6.1)With regard to the number of service users within ourservices who have hearing difficulties, Mrs Tyler repliedthat she was unable to provide the answer at this time butthat she would ascertain the information and report backto governors. In respect of having signage by the bedsideMrs Tyler noted that any needs would be recorded in theservice users’ notes.
Ms Shutter commented that she knows someone whouses sign language and speaks to people who are deafand that she would provide further details of this. Mrs Hillagreed to speak to Ms Shutter and obtain the details.
ST
CH
14/088 Chair’s Report (agenda item 8)
The Council thanked Paul for his hard work andcontribution as a staff governor. Mr Griffiths indicated thathe would write to Paul to express the Council’sappreciation.
Mr Griffiths advised the Council that there is currently anelection process underway. Mrs Hill noted that she wouldkeep the Council updated of progress and report on theoutcome once the election comes to an end.
FG
CH
14/093 Ratification of the Governors’ Expenses Procedure(agenda item 13)
Mrs Hill presented the governors’ reimbursement ofexpenses procedure for ratification. Governors werereminded that they are entitled to claim expenses and cando so via the governance office. Mrs Hill agreed to writeto all members of the Council regarding this and wouldenclose a supply of expenses claim form.
CH

17
MINUTE ACTION SUMMARY (PUBLIC MEETING) LEAD
14/099 Engagement with people whose views are not fullyrepresented (agenda item 17)
Members of Council were keen to get involved in a taskand finish group with the objective of considering howbetter to engage with these groups. Mr Howorth asked forthe governor volunteers to contact him if they would like tobe involved.
COG
14/103 Question / comments from Members of the Public(agenda item 20)
A member of the public raised a concern with regard topeople with a personality disorder not being representedin the Council, in particular males with a personalitydisorder. Mr Howorth replied that these views would befed into the task and finish group which will look atengaging with people whose views are not fullyrepresented and agreed to liaise with the gentleman.
AH