lee v. lumen food corp., et al index of medical records ... food corp., et al index of medical...
TRANSCRIPT

Lee v. Lumen Food Corp., et alIndex of Medical Records
Sharon Lee
DOA: 1/8/02
Records Summarized:
Parkview Regional HospitalPalestine Regional Medical Center
Northwest Regional Hospital
Date Provider Complaint Treatment
1/8/02 Parkview RegionalHospital
History & Physical
Charles Smith, D.O.
Abnormal uterinebleeding
History: Patient with long history ofabnormal uterine bleeding; she has been onmultiple birth control pills in an attempt tocontrol the heavy bleeding and crampingwith little help; she now states she ispassing large clots with severe cramping.
Exam: Neck supple; heart rate regular;lungs clear; normal vagina and cervix.
Impression: Abnormal uterine bleeding withsevere dysmenorrhea (pain) andhypermenorrhea (length of period).
Plan: Total abdominal hysterectomy andpossible left salpingo oophorectomy.
1/8/02 Parkview RegionalHospital
Operative Report
Rory Lewis, M.D.
Left wrist pain Pre and Post-operative Diagnosis: Left wristdorsal ganglion cyst, symptomatic.
Operation: Excision left wrist dorsalganglion cyst.
Procedure: Patient tolerated procedure welland was turned over to Dr. Smith who wasscheduled to do a hysterectomy.

Date Provider Complaint Treatment
1/8/02 Parkview RegionalHospital
Operative Report
Charles Smith, D.O.
Abnormal uterinebleeding
Pre and Post -operative Diagnosis:Hypermenorrhea, dysmenorrhea and pelvicpain.
Operation: Abdominal hysterectomy, lysis ofadhesions and left salpingo-oophorectomy.
Procedure: “The shape of the pelvis wasdeep and the patient was felt to be at riskfor possible enterocele (intestinal prolapseinto the vagina) or rectocele (rectal prolapsewith protrusion into the vagina) in the futureso the cul-de-sac was closed by bringingthe uterosacral ligaments into the midline;there was some oozing around the bladderflap and so some Surgicel was put in thisarea and the peritoneum was then closedover the Surgicel.”
1/8/02 Parkview RegionalHospital
R a d i o l o g yDepartment
A b d o m i n a lhysterectomy
Abdominal X-ray: There are 2 drains overthe lower abdomen/pelvis; there is an ovalshaped structure possibly reflecting a drainreservoir projecting over the lower pelvis;there was some faint radiopaque rows ofsutures seen in the lower pelvis.
Foreign bodies as described are felt to berelated to post surgical drains and sutures;I cannot see any additional foreign matterbut clinical correlation is requested as I amuncertain as to what was misplaced insurgery.
1/9/02 Parkview RegionalHospital
Progress Notes
Charles Smith, D.O.
A b d o m i n a lhysterectomy
Subjective: Patient sore; passing gas;hungry.
Objective: Afebrile; abdomen soft; dressingdry.
Assessment: Stable.
Plan: Per orders.
1/10/02 Parkview RegionalHospital
Progress Notes
Charles Smith, D.O.
A b d o m i n a lhysterectomy
Subjective: Patient tolerating regular diet;c/o urinary retention.
Objective: Afebrile; abdomen soft.
Assessment: Stable.
Plan: Per orders.

Date Provider Complaint Treatment
1/11/02 Parkview RegionalHospital
Progress Notes
Charles Smith, D.O.
A b d o m i n a lhysterectomy
Subjective: Patient doing okay; c/o bladderspasms.
Objective: Afebrile; abdomen soft; JacksonPratt drain removed; incision looks good.
Assessment: Stable.
Plan: Home.
1/11/02 Parkview RegionalHospital
Discharge Summary
Charles Smith, D.O.
A b d o m i n a lhysterectomy
History: Patient with long history ofabnormal uterine bleeding, dysmenorrhea(pain) and hypermenorrhea (length ofperiod); she failed conservativemanagement.
Hospital Course: Patient underwent totalabdominal hysterectomy, lysis of adhesions& left salpingo-oophorectomy on 1/8/02;post-operative course was uncomplicated;she has had normal return of bowel andbladder function, has ambulated well andtolerated regular diet well.
She is discharged in stable condition; post-operative instructions were given; to follow-up in office in 4 weeks.
1/12/02 Parkview RegionalHospital
Progress Notes
Charles Smith, D.O.
A b d o m i n a lhysterectomy
Subjective: Patient has episode ofdecreased pO2, dizziness, nausea &vomiting last p.m.
Objective: Afebrile; highest temp 102; BP95/55; lungs clear-shallow; abdomen withminimal distension; bowel soundsdecreased but present; KUB showsincreased gas in colon; chest x-ray showsatelectasis vs pneumonia; hemoglobindecreased from 12.8 to 9.3 to now 7.9.
Assessment: Atelectasis vs. pneumonia;post op bleed.
Plan: Will watch hemoglobin; if continues todrop will consider transfusion; possiblelaparotomy.
Date Provider Complaint Treatment
1/12/02 Parkview RegionalHospital
Consultation Report
Kenneth Russell,M.D.
Abnormal uterinebleeding
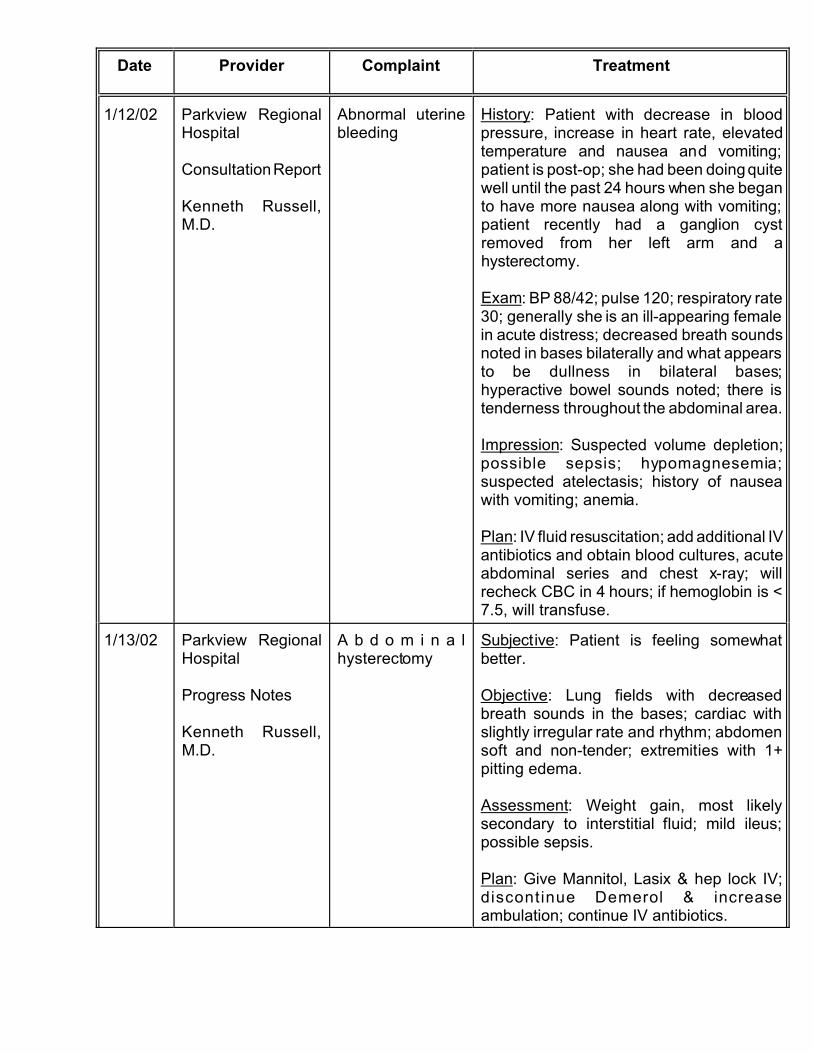
History: Patient with decrease in bloodpressure, increase in heart rate, elevatedtemperature and nausea and vomiting;patient is post-op; she had been doing quitewell until the past 24 hours when she beganto have more nausea along with vomiting;patient recently had a ganglion cystremoved from her left arm and ahysterectomy.
Exam: BP 88/42; pulse 120; respiratory rate30; generally she is an ill-appearing femalein acute distress; decreased breath soundsnoted in bases bilaterally and what appearsto be dullness in bilateral bases;hyperactive bowel sounds noted; there istenderness throughout the abdominal area.
Impression: Suspected volume depletion;possible sepsis; hypomagnesemia;suspected atelectasis; history of nauseawith vomiting; anemia.
Plan: IV fluid resuscitation; add additional IVantibiotics and obtain blood cultures, acuteabdominal series and chest x-ray; willrecheck CBC in 4 hours; if hemoglobin is <7.5, will transfuse.
1/13/02 Parkview RegionalHospital
Progress Notes
Kenneth Russell,M.D.
A b d o m i n a lhysterectomy
Subjective: Patient is feeling somewhatbetter.
Objective: Lung fields with decreasedbreath sounds in the bases; cardiac withslightly irregular rate and rhythm; abdomensoft and non-tender; extremities with 1+pitting edema.
Assessment: Weight gain, most likelysecondary to interstitial fluid; mild ileus;possible sepsis.
Plan: Give Mannitol, Lasix & hep lock IV;discontinue Demerol & increaseambulation; continue IV antibiotics.

Date Provider Complaint Treatment
1/13/02 Parkview RegionalHospital
Progress Notes
Charles Smith, D.O.
A b d o m i n a lhysterectomy
Subjective: Feels better; + BM.
Objective : Afebrile; abdomen soft;extremities with some swelling; weight up10 lbs. since admission.
Assessment: Improving.
Plan: Per orders.
1/14/02 Parkview RegionalHospital
Progress Notes
Charles Smith, D.O.
A b d o m i n a lhysterectomy
Subjective: + BM.
Objective: Afebrile; abdomen soft; still someswelling noted of extremities.
Assessment: Improving.
Plan: Per orders.

Date Provider Complaint Treatment
1/14/02 Parkview RegionalHospital
A d d e n d u m t oDischarge Summary
Charles Smith, D.O.
Abnormal uterinebleeding
History: Patient was prepared for dischargeon 1/11/02; however, that day shedeveloped a post-operative fever prior todischarge and her discharge was canceled.
She was started on Unasyn; the followingday, 1/12/02, the patient had an episode ofdizziness with nausea and vomiting; shewas made NPO and an abdominal seriesand CBC were obtained; the abdominal filmshowed a possible ileus; she developedsome shortness of breath with decrease inoxygen saturation.
Consultation was obtained with Dr. Russell;due to the patient’s post-operative ileus, anasogastric (NG) tube was placed; patient’sx-rays also showed some basilarconsolidations and possible pleural effusionin the lungs; Magnesium Citrate was givenvia NG tube in an attempt to get the bowelsfunctioning; the next day she did havebowel functioning and was feeling better; on1/14/02, the patient was having bowelfunction but continued to have somedistension of the abdomen that was soft; arepeat abdominal film at that time revealedextensive distension of the small bowel withair fluid levels, possible ileus vs. mechanicalobstruction.
CT of the abdomen was performed, whichshowed a blood clot in the cul-de-sac, witha possible partial mechanical small bowelobstruction.
This was explained to the patient and shewas given the option of continuedobservation with a liquid diet andambulation vs. exploratory laparotomy withevacuation of the hematoma.
The patient stated she would like to gohome; post-operative instructions weregiven; she was to be followed up in theoffice in 2 days; if she developed furtherproblems, she would be re-admitted.

Date Provider Complaint Treatment
1/15/02 Parkview RegionalHospital
Progress Notes
Kenneth Russell,M.D.
A b d o m i n a lhysterectomy
Subjective: Patient is alert; is somewhatdepressed.
Objective: After evaluation, it is obvious thepatient has at least a partial small bowelbowel obstruction, whether this issecondary to hematoma or whether this issecondary to other, it is unsure; I had a longdiscussion with Dr. Smith today; patient wasgiven the option of staying and letting Dr.Smith open her up vs. simply going home;patient demands to go home at this point intime; risks and benefits have been given.
Assessment: Ileus; decreased oral intake.
Plan: Patient fully understands that sheneeds to increase her oral intake; risks andbenefits have been given of not doing so;she accepts this at this point in time; willdefer that to Dr. Smith.
1/15/02 Parkview RegionalHospital
Progress Notes
Charles Smith, D.O.
A b d o m i n a lhysterectomy
Subjective: Bowels working.
Objective: Afebrile; abdomen soft; goodbowel sounds; less edema of extremities.
Assessment: Stable.
Plan: Small bowel follow through; if okay,home.
1/15/02 Parkview RegionalHospital
Progress Notes
Charles Smith, D.O.
A b d o m i n a lhysterectomy
Objective: Small bowel CT scan-___ bloodclot in cul-de-sac & possible partialmechanical bowel obstruction; explainedoptions to patient; patient wants to gohome.
Plan: Instructed in full liquid diet; will ___daily & will re-admit if problems develop.

Date Provider Complaint Treatment
1/18/02 Palestine RegionalMedical Center
History and Physical
Stephen Bates,M.D.
Abdominal pain,r e p e t i t i v evomiting, diarrhea
History: Patient arrived to the ED at 0400on the morning of admission c/o repetitivevomiting since the evening of 1/17/02 &increasing lower abdominal pain andcontinuous watery stools.
She underwent total abdominalhysterectomy and lef t salpingo-oophorectomy in Mexia on 1/8/02; on 3rd or4th postop day she began having nausea,vomiting, fever, bladder spasms and drop inhemoglobin down to 7.7; she states shewas diagnosed with an ileus; she initiallyimproved but when she was about to bedischarged she again had nausea andvomiting and was again diagnosed with anileus; states a CT scan was done but shenever heard the findings; she stated shestrongly wanted to go home, as she wasvery dissatisfied with the nursing care.
Despite the concern about ileus andconstipation, she was having 10 or morewatery stools per day; she has not eatenany solid food since surgery; she has notedan odorous vaginal discharge.
Patient lives in Buffalo with her mother; sheis a registered nurse who used to work atPalestine Regional Medical Center over ayear ago but for the past year has been amed-surg nurse at Parkview in Mexia.
Exam: Abdomen moderately tender in bothlower quadrants, right > left; bowel soundsare present but extremely sluggish; whenexamining the vagina, the cuff appears tobe partially open; there is a watery yellow-gray exudate over the cuff surrounded by alinear margin of erythema; bimanual examreveals a firm fairly fixed mass posteriorand superior to the vaginal cuff.
Abdominal pelvic CT done; I have been toldthere are 1-2 abscesses in the pelvis.

Date Provider Complaint Treatment
1/18/02 Palestine RegionalMedical Center
History and Physical
Stephen Bates,M.D.
Abdominal pain,r e p e t i t i v evomiting, diarrhea
(Continued)
Assessment: Postoperative pelvic abscess;appears to be walled off; she does not havean acute surgical abdomen at this time; shehas secondary vomiting and waterydiarrhea with hypokalemia.
Plan: Admission; broad spectrumantibiotics; will review CT with radiologist; ifIV antibiotics do not take care of theproblem, she may require surgicalexploration and drainage.
1/19/02 Palestine RegionalMedical Center
Progress Note
Stephen Bates,M.D.
Abdominal pain,r e p e t i t i v evomiting, diarrhea
Subjective: Patient feels much better today;has had no vomiting or diarrhea sinceadmission.
Objective: Lungs are clear; is very mildlytender to abdominal palpation.
Reviewed x-ray and CT films from Parkviewbrought in by family members; on 1/15/02,abdominal x-ray and CT showed a partialsmall bowel obstruction, the same fluidcollections in the pelvis that we had seenwere evident at that time; we have certainlyseen complete resolution of her partialsmall bowel obstruction by the time of thisadmission.
Assessment: Pelvic abscess or infectedhematoma with secondary ileus and partialsmall bowel obstruction and repetitivevomiting; certainly seems to be respondingto IV antibiotics; actually her small bowelobstruction had already resolved by thisadmission; she has been afebrile and herwhite blood count is declining; she has hadresolution of vomiting and diarrhea; herappetite is returning and overall clinicallyshe looks to be responding to conservativemanagement.
Plan: Continue IV antibiotics; advance clearliquid diet; if she continues to do well, willadvance her to solid diet tomorrow; willrepeat CT in 2-3 days.

Date Provider Complaint Treatment
1/20/02 Palestine RegionalMedical Center
Progress Note
Stephen Bates,M.D.
Abdominal pain,r e p e t i t i v evomiting, diarrhea
Subjective: Patient feels much better today;she is hungry and would like to eat; she hadone bowel movement which was loose, butthere was some formed stool present; sheis ambulating without difficulty.
Objective: Abdomen soft, not distended andvery minimally tender to abdominalpalpation in the right lower quadrant.
Assessment: Clinically appears to continueto improve although her white blood countdid not decrease further from yesterday.
Plan: Advance to regular diet; change IV toheparin lock and discontinue Morphine;continue IV antibiotics; will repeat CT in 2days.
1/21/02 Palestine RegionalMedical Center
Progress Note
Stephen Bates,M.D.
Abdominal pain,r e p e t i t i v evomiting, diarrhea
Subjective: The patient feels well; she atesome regular diet throughout the dayyesterday with no nausea or vomiting; sheis still passing gas but has not had anotherbowel movement; she feels like she ishaving some mild gas pains; patient statesshe feels like she is having some urinaryfrequency, like her bladder will not hold asmuch.
Objective: Abdomen is soft and does notappear distended; she is minimally tenderto deep palpation.
Assessment: Overall doing well on IVantibiotics; her bladder symptoms may bedue to compression by the pelvic mass.
Plan: After next voiding, will get in and outcath for residual; otherwise continue samemanagement; will repeat lab and CTtomorrow.

Date Provider Complaint Treatment
1/22/02 Palestine RegionalMedical Center
Progress Note
Stephen Bates,M.D.
Abdominal pain,r e p e t i t i v evomiting, diarrhea
Subjective: The patient was doing well untilsometime during the night, when she beganto have nausea; this morning she began tohave repeated vomiting; late this morningshe appears weak and lethargic, althoughstill oriented.
Objective: Lungs clear; abdomen is soft butsignificantly more tender to deep palpationin the right lower quadrant; bowel soundsare rare.
Patient’s white blood count is increasingagain; CT scan is worrisome, showingmultiple dilated loops of small bowel; thelarger mass high in the pelvis is larger; thegallbladder is more distended andgallstones are again evidenced.
Assessment: Appears to be suddenlydeveloping a partial small bowelobstruction, very likely due to the largermass high in the pelvis; I believe this is ahematoma, although abscess is stillconsidered; cholelithiasis.
Plan: Have reviewed the case and films withradiologist and Dr. Rodriguez, a generalsurgeon; will decompress the bowel with anNG tube, give IV fluid hydration andtransfuse because I believe she is stillsignificantly anemic; will attempt to drain thelarger mass percutaneously tomorrow aftershe is rehydrated and her bowel hasdecompressed somewhat.

Date Provider Complaint Treatment
1/23/02 Palestine RegionalMedical Center
Consultation Report
Dirk Rodriguez,M.D.
Abdominal painand vomiting
Consultation Diagnoses: Postoperativein t raabdomina l f l u id co l lec t ion;postoperative ileus with possible bowelobstruction; extrinsic mass effect on thebladder by this intraabdominal mass.
Consultation Recommendations: NGdecompression with IV fluid resuscitation;CT scan-directed drainage of this fluid-filledcollection; transfusion.
Exam: No bowel sounds heard; nodistension noted; white blood count isslightly elevated; films show the presence ofan ileus with multiple fluid-filled loops ofbowel; she has a 6 centimeterintraabdominal mass that in comparison toanother CT scan shows an increase in size;it is compressing the bladder and appearsto be compressing the small bowel.
Plan: Have discussed findings with thepatient and she understands all this; sheunderstands she has about a 15-25%chance of requiring repeat intraabdominalsurgery if this is a septic process.
1/23/02 Palestine RegionalMedical Center
Progress Note
Stephen Bates,M.D.
Abdominal pain,r e p e t i t i v evomiting, diarrhea
Subjective: The patient has felt much bettersince the placement of the NG tube.
Objective: Abdomen is soft but lessdistended; mildly to moderately tender inthe right lower quadrant; bowel sounds arefairly normal.
Patient completed transfusion of 2 units ofpacked cells yesterday; hemoglobin is up to11.2 today.
Assessment: Status post partial small bowelobstruction, due to what I believe to be apelvic or intra-abdominal hematoma, vs.abscess.
Plan: Is scheduled to go down this morningfor attempted percutaneous drainage of thefluid collection.

Date Provider Complaint Treatment
1/23/02 Palestine RegionalMedical Center
Progress Note
Dirk Rodriguez,M.D.
Abdominal pain,r e p e t i t i v evomiting, diarrhea
Subjective: The patient states Dr. Smithused some type of solution during surgeryto try and help with bleeding; this may havebeen fibrin glue or some other type ofhemostatic agent.
Objective: Drainage of mass via CT wasunsuccessful.
Assessment: Suspect she has a walled offhematoma that is causing her ileus,possibly the source of her drop in bloodcount and producing the urgency.
Plan: I have explained by recommendationfor surgery; has agreed to proceed; will alsoplace a central line.

Date Provider Complaint Treatment
1/24/02 Palestine RegionalMedical Center
Operative Report
Dirk Rodriguez,M.D.
Abdominal painand vomiting
Preop Diagnoses: Intraabdominalhematomas from a separate hysterectomyand left salpingo-oophorectomy performedat Parkview Regional Hospital; small bowelobstruction.
Postop Diagnoses: Intraabdominalhematomas from a separate hysterectomyand left salpingo-oophorectomy performedat Parkview Regional Hospital; small bowelobstruction; enlarged right ovarian cyst,likely reactive.
Operation: Exploratory laparotomy; lysis ofadhesions; drainage of postoperative intra-abdominal hematomas; right salpingo-oophorectomy.
Indication and Judgement: Patientunderwent abdominal hysterectomy in earlyJanuary by Dr. Smith in Mexia; she had noconflict with Dr. Smith, however, due tonursing and care issues, she requestedtransfer to Palestine Regional MedicalCenter; patient underwent conservativesurgical care without success; patient wasbrought to OR for exploration.
Findings: Dense adhesions from priorsurgeries noted, most of them collectingdown in the pelvis; there was a rightperirectal hematoma; there was a largeright paracecal hematoma which had drawnin the omentum of the transverse colon, thesmall bowel as well as the appendix and theright tube and ovary which were left behindfrom the prior surgery; the right ovary had avery large 4-6 cm cyst which was drawn intothe inflammatory process and could not beseparated from it.
1/23/02 Palestine RegionalMedical Center
Progress Note
Dirk Rodriguez,M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: The patient is doing well; shehas had a tough time with some itching andwas in pain but apparently got the PCAadjusted; she had a vasovagal symptomearly today but we have picked up on hervolume.
Plan: Will leave in ICU for today andtransfer out tomorrow.

Date Provider Complaint Treatment
1/25/02 Palestine RegionalMedical Center
Progress Note
Dirk Rodriguez,M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: The patient is doing well; NGtube has been removed; color looks good;spirits appear good as well.
Objective: She has a few bowel sounds;abdomen soft; lab work looks good;tolerating TPN (Total Parenteral Nutrition).
Plan: Will reduce maintenance IV; will leaveFoley cath in place due to the inflammationin that area; will transfer to the floor; and willincrease her physical activity.
1/25/02 Palestine RegionalMedical Center
Progress Note
Stephen Bates,M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: The patient is doing much bettertoday; she started diuresing today, puttingout 200-400 cc’s per hour of urine.
Objective: NG tube has been discontinued;abdomen is soft and not distended.
Assessment: Doing well postoperatively;she is now mobilizing her third space fluid;she really seems to be turning the corner.
Plan: She is on TPN; Dr. Rodriguez plans tostart clear liquids this evening.
1/26/02 Palestine RegionalMedical Center
Progress Note
Don Jackson, M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: The patient seems in betterspirits today; she has been up walkingaround the unit but still somewhat in aweakened state.
Objective: Lungs clear bilaterally; abdomensoft with hypoactive bowel sounds.
Assessment: Patient is progressing well;has had good urine output.
Plan: Will transfuse 2 units of packed cells;continue ambulation; will give Dulcolax tostimulate bowel function.
Date Provider Complaint Treatment
1/27/02 Palestine RegionalMedical Center
Progress Note
Don Jackson, M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
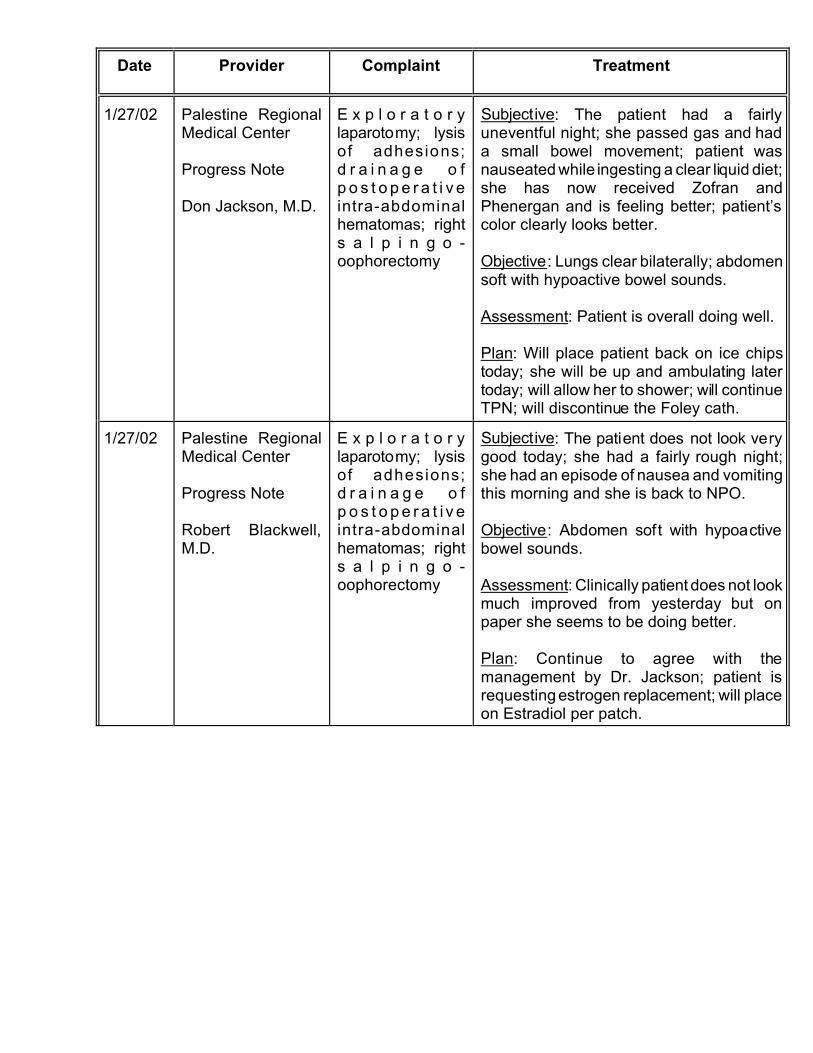
Subjective: The patient had a fairlyuneventful night; she passed gas and hada small bowel movement; patient wasnauseated while ingesting a clear liquid diet;she has now received Zofran andPhenergan and is feeling better; patient’scolor clearly looks better.
Objective: Lungs clear bilaterally; abdomensoft with hypoactive bowel sounds.
Assessment: Patient is overall doing well.
Plan: Will place patient back on ice chipstoday; she will be up and ambulating latertoday; will allow her to shower; will continueTPN; will discontinue the Foley cath.
1/27/02 Palestine RegionalMedical Center
Progress Note
Robert Blackwell,M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: The patient does not look verygood today; she had a fairly rough night;she had an episode of nausea and vomitingthis morning and she is back to NPO.
Objective: Abdomen soft with hypoactivebowel sounds.
Assessment: Clinically patient does not lookmuch improved from yesterday but onpaper she seems to be doing better.
Plan: Continue to agree with themanagement by Dr. Jackson; patient isrequesting estrogen replacement; will placeon Estradiol per patch.

Date Provider Complaint Treatment
1/28/02 Palestine RegionalMedical Center
Progress Note
Stephen Bates,M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: Yesterday the patient had anepisode of emesis in the morning aftertaking clear liquids; she was made NPOand has had no further nausea or vomiting;she had a bowel movement this morning.
Objective: Abdomen soft with active bowelsounds.
Assessment: Patient is progressing well;has had good urine output.
Plan: I am concerned the patient seemed tohave a setback yesterday, but she hasdone well NPO; it may be time to graduallyadvance her diet a little bit if Dr. Rodriguezthinks it is appropriate.
1/28/02 Palestine RegionalMedical Center
Progress Note
Dirk Rodriguez,M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: The patient is doing better; shewas hungry and ate a regular diet becauseshe wanted to; she has been passing gasand having bowel movements; she threw uplater this afternoon but it was liquid, not herfood.
Objective: Abdomen soft with good bowelsounds.
Assessment: I had an extensiveconversation with the patient regarding thefindings of her operation.
Plan: Will leave her on TPN until she cantolerate a regular diet.
1/29/02 Palestine RegionalMedical Center
Progress Note
Stephen Bates,M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: Patient is still having somenausea and vomiting; at lunch she wasactually able to keep down solid food; she ishaving frequent watery stools, about 10 sofar.
Objective: Abdomen soft, not distended andminimally tender.
Plan: The dietitian is adjusting the patient’sdiet to try to help her keep down solid food;her TPN is being tapered.

Date Provider Complaint Treatment
1/29/02 Palestine RegionalMedical Center
Progress Note
Dirk Rodriguez,M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: Patient is doing a little bit better;she is tired of being her; she has had a littlenausea.
Plan: Will taper TPN and allow her to havesmall meals.
1/30/02 Palestine RegionalMedical Center
Progress Note
Stephen Bates,M.D.
E x p l o r a t o r ylaparotomy; lysisof adhesions;d r a i n a g e o fp o s t o p e r a t i v eintra-abdominalhematomas; rights a l p i n g o -oophorectomy
Subjective: Patient is doing better; she willthrow up after a meal, particularly if it is alarge meal, but she handled the smallmeals well; she is tired of being here andwe will let her go home; she has bowelactivity and the diarrhea is going away.
Objective: Abdomen soft with active bowelsounds; lungs clear.
Plan: Patient is c/o some dyspnea; will sendhome on Prilosec.
1/30/02 Palestine RegionalMedical Center
History and Physical
Stephen Bates,M.D.
Abdominal pain,r e p e t i t i v evomiting, diarrhea
Admission Diagnoses: Intra-abdominalpostoperative hematoma after TAH/BSO atParkview in Mexia; intra-abdominalpostoperative adhesions resulting in apostoperative bowel obstruction; persistentanemia; malnutri tion secondary topostoperative inanition (condition of beingempty).
Therapeutic Procedures Performed:Abdominal CT scan with attemptedpercutaneous intra-abdominal fluidcollection drainage; exploratory laparotomywith lysis of adhesions and extraction ofright ovary with large ovarian cyst andextraction and drainage of intra-abdominalhematomas (the appendix was notremoved).
Plan: Keep wound dry and clean with soapand water; resume regular diet and followup in 1-2 weeks.

Date Provider Complaint Treatment
1/28/03 Northwest RegionalHospital
Operative Report
Juan Villarreal, M.D.
Pelvic pain Preoperative Diagnosis: Pelvic pain;dyspareunia (painful intercourse); peritonealadhesions.
Postoperative Diagnosis: Pelvic pain;dyspareunia (painful intercourse); peritonealadhesions; foreign body in the pelvis.
Name of Procedure: Exploratorylaparotomy; lysis of adhesions; removal offoreign body in peritoneal cavity;vaginectomy.
Specimens: Some foreign bodies werefound in the peritoneal cavity attached tothe vaginal cuff consisting of what appearedto be suture material and staples.
Procedure: We took the incision down tothe fascia where we encountered numerousinterrupted figure-of-eight sutures ifpermanent suture material; these had to beindividually removed....the patient had beenpositioned in a frog-leg position and wewere able to introduce an EEA dilator intothe vagina and push up and visualize thevaginal cuff; of note, there was a staple limeon the right side where some vascularstaples had been laid...on the vaginal cuffthere were not visible staples...we wereable to palpate around the vaginal mucosaon the inside and were not able to feel anydistinct staples or any other foreign bodiesat the apex of the vagina.
1/30/03 Northwest RegionalHospital
Discharge Summary
Juan Villarreal, M.D.
Pelvic pain Admit Diagnosis: Pelvic pain; dyspareunia(painful intercourse); peritoneal adhesions.
Procedure Performed: Exploratorylaparotomy; lysis of adhesions; removal offoreign bodies in peritoneal cavity frompervious surgery.
Hospital Course: Patient is doing wellpostop; she is tolerating diet andambulating.
Plan: Discharge home; no heavy lifting,strenuous activity or anything in the vagina;follow up in 2 weeks.


History:
Exam:
Impression:
Plan: