leaving no one behind- casting a wider net …...leaving no one behind- casting a wider net to...
TRANSCRIPT

LEAVING NO ONE BEHIND- CASTING A WIDER NET TO INTEGRATE HCV CARE INTO PRIMARY CARE
Stacey B. Trooskin MD PhDDirector of Viral Hepatitis ProgramsPhiladelphia FIGHT Community Health CentersClinical Assistant Professor of MedicinePerelman School of Medicine, University of Pennsylvania

Treatment cascade for people with chronic HCV infection
Yehia B. PLoS One. 2014; 9(7) e101554.
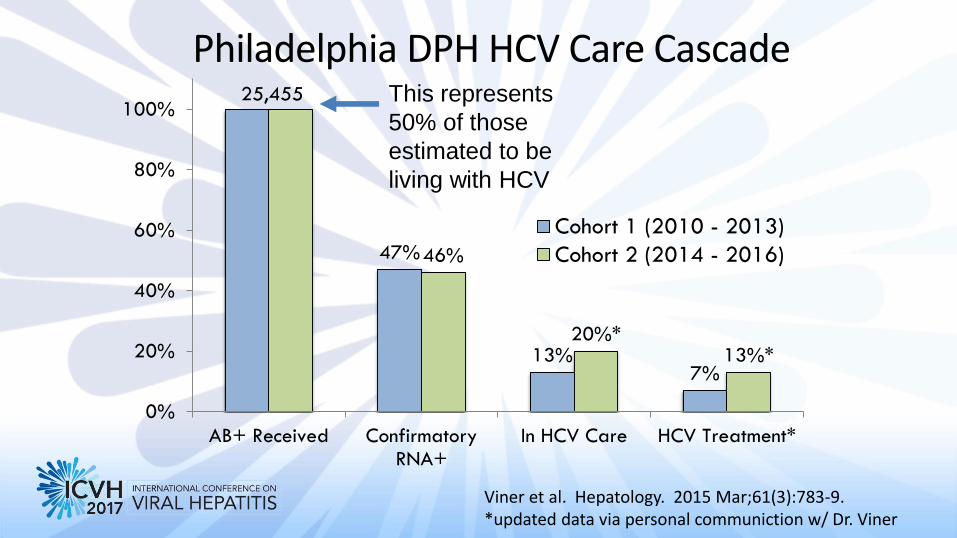
25,455
47%
13%7%
46%
20%*13%*
0%
20%
40%
60%
80%
100%
AB+ Received ConfirmatoryRNA+
In HCV Care HCV Treatment*
Cohort 1 (2010 - 2013)
Cohort 2 (2014 - 2016)
Philadelphia DPH HCV Care Cascade
Viner et al. Hepatology. 2015 Mar;61(3):783-9. *updated data via personal communiction w/ Dr. Viner
This represents
50% of those
estimated to be
living with HCV

Testing and Linkage to Care ProtocolOraQuick® rapid HCV antibody test reactive
HCV RNA Detected
HCV RNA Not
Detected
Patient Navigator
notifies patient and
provides counselingPatient Navigator notifies patient and
provides counseling + insurance
assessment
Insured with a primary care
provider
Insured with no known
primary care provider
Patient Navigator facilitates
PCP acquisition
Uninsured
Patient Navigator facilitates
appointment with clinical social
worker
Blood draw for confirmatory HCV PCR
PCP Visit
Obtain Referral to subspecialist

Do One Thing Campaign HCV Testing and Linkage to Care Cascade n=1,301
58%
Trooskin S et al. JGIM. 2015 Jul;30(7):950-7.

Strategies for Enhanced Testing in Academic Primary Care Clinics
– EMR modifications
– Integration into clinic work flow
– Antibody with Reflexive confirmatory testing only
– Automated ordering

Impact of EMR Prompts on Type of HCV Screening Test Ordered
2014
Reflexive confirmatory testing
Other HCV test orders

0.00%
10.00%
20.00%
30.00%40.00%
50.00%
60.00%
70.00%
80.00%90.00%
100.00%
Practice1
Practice2
Practice3
Practice4
Practice5
Practice6
Total
%ag
e o
f El
igib
le P
atie
nts
te
sted
for
HC
V
*EMR prompts added July 2014
Jan '14-Jun '14 Jul '14-Dec '14
Impact of EMR prompts on Percentage of Eligible Baby Boomers Tested for HCV

Philadelphia FIGHT
The Jonathan Lax Treatment CenterThe Youth Health Empowerment Project
The John Bell Health Center
COMMUNITY BASED TESTINGSyringe Exchange ProgramDrug Treatment Programs
Homeless sheltersOpioid substitution programsPhiladelphia Dept of Prisons

Strategies for Enhanced Testing in the FQHC Primary Care Clinic
– High risk population consider universal annual testing
– Visit notes with prepopulated orders for HIV and HCV testing
– Provider education
– Quality control and improvement
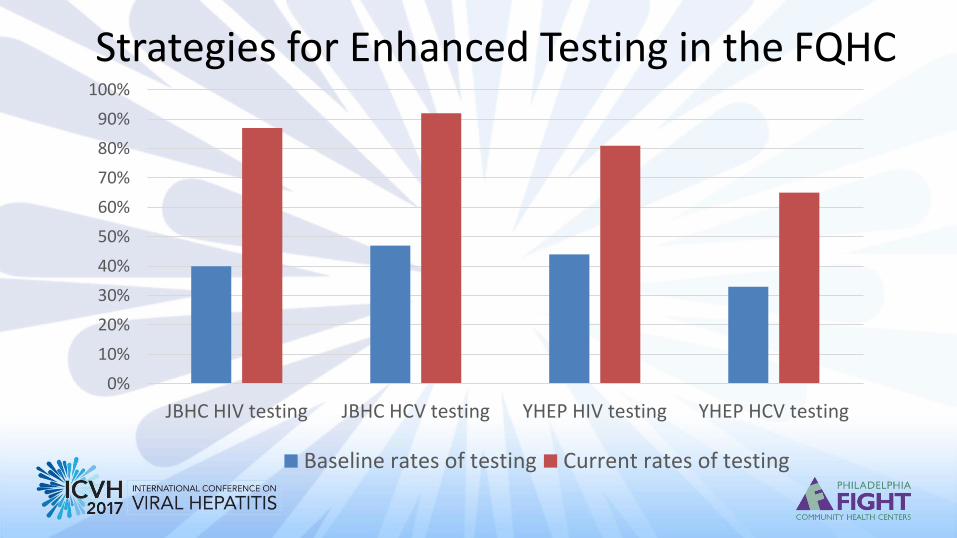
Strategies for Enhanced Testing in the FQHC
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
JBHC HIV testing JBHC HCV testing YHEP HIV testing YHEP HCV testing
Baseline rates of testing Current rates of testing

Coyle, C. Pub Health Rep. 2016, sup 2, Vol 131.

Primary Care HCV Treatment

Primary Care Provider HCV Treatment Outcomes
Arora, S. 2011. NEJM. 364, 23

AASLD/IDSA: Who should be treated?
www.hcvguidelines.org
Treatment is recommended for all patients with chronic HCV infection, except those with short life expectancies that cannot be
remediated by treating HCV, by transplantation, or by other directed therapy. Patients with short life expectancies owing to liver disease
should be managed in consultation with an expert.Rating: Class I, Level A

Current Challenges in HCV Care in the US
• Restrictive criteria for drug approval for many payers– Sobriety requirement
– Prescriber requirement
– Disease severity requirement
– HIV may not be a mitigating factor
• Arduous prior authorization process for providers
Barua S et al., Ann Intern Med. 2015;163(3):215-223Canary LA et al., Ann Intern Med. 2015;163(3):226-228

Clary, R & Greenwald, R. The State of Medicaid Access, AASLD, The Liver Meeting, November 14 2016.
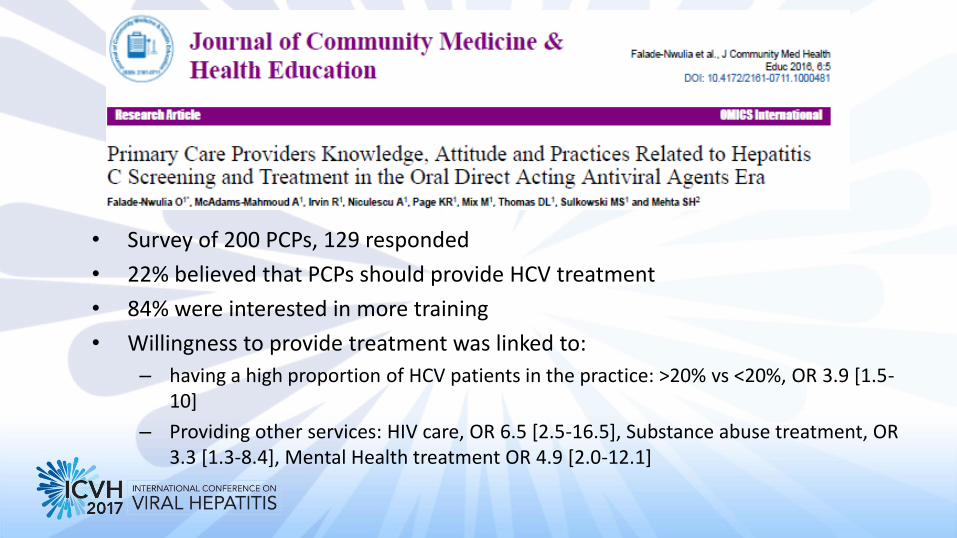
• Survey of 200 PCPs, 129 responded
• 22% believed that PCPs should provide HCV treatment
• 84% were interested in more training
• Willingness to provide treatment was linked to:
– having a high proportion of HCV patients in the practice: >20% vs <20%, OR 3.9 [1.5-10]
– Providing other services: HIV care, OR 6.5 [2.5-16.5], Substance abuse treatment, OR 3.3 [1.3-8.4], Mental Health treatment OR 4.9 [2.0-12.1]
Current Challenges in HCV Care in the US
• Restrictive criteria for drug approval for many payers– Sobriety requirement
– Prescriber requirement
– Disease severity requirement
– HIV may not be a mitigating factor
• Arduous prior authorization process for providers
Barua S et al., Ann Intern Med. 2015;163(3):215-223
Canary LA et al., Ann Intern Med. 2015;163(3):226-228
Training, support, education- HCV treatment in people actively using drugs- Harm reduction

Thank you!
• C a Difference Team, Philadelphia FIGHT– Lora Magaldi, C a Difference Project Coordinator– Carla Coleman, Linkage Coordinator– Ta-Wanda Preston, Lead Outreach specialist– Ricardo Rivera, HIV/HCV tester and educator– Nabori Brown, HIV/HCV tester and educator– Students, volunteers, community partners– Patients
• Do One Thing– Amy Nunn, ScD
• HepCAP members and leadership– Alex Shirreffs & Jack Hildick- Smith
• Prevention Point Philadelphia• Gilead FOCUS and Prevent Cancer Foundation•