leading population health---a results-based lean approach
TRANSCRIPT

L E A D I N G P O P U L AT I O N H E A LT Htomás j aragón1,2,3*
may 4, 2016
contents
1 Background 2
1.1 Purpose . . . . . . . . . . . . . . . . . . . . . . . 2
1.2 Population health overview . . . . . . . . . . . 2
1.3 Results-based lean management . . . . . . . . 6
2 Transform self and interpersonal relationships 10
2.1 Connect! Building positive relationships . . . . 10
2.2 Think! Leadership intelligence . . . . . . . . . 12
2.3 Decide! Decision intelligence . . . . . . . . . . 13
2.4 Lead! Leader standard work . . . . . . . . . . 14
3 Transform teams and collaboratives 14
3.1 Building teams . . . . . . . . . . . . . . . . . . 14
3.2 Embracing challenges . . . . . . . . . . . . . . 14
3.3 Achieving results . . . . . . . . . . . . . . . . . 15
4 Transform organizations and communities 15
4.1 Transforming organizations . . . . . . . . . . . 15
4.2 Transforming communities . . . . . . . . . . . 15
4.3 Achieving health equity . . . . . . . . . . . . . 15
a The Leading Population Framework 16
b Leadership competencies 17
b.1 How to be: character traits and values . . . . . 17
b.2 What to know: public health knowledge . . . 17
b.3 What to do: 25 essential competencies . . . . . 18
c Trauman informed system core principles 19
c.1 Understanding Trauma and Stress . . . . . . . 19
c.2 Compassion and Dependability . . . . . . . . . 19
c.3 Safety and Stability . . . . . . . . . . . . . . . . 20
c.4 Collaboration and Empowerment . . . . . . . . 20
c.5 Cultural Humility and Responsiveness . . . . 20
c.6 Resilience and Recovery . . . . . . . . . . . . . 21
1 Health Officer, City and County of San Francisco2 Director, Population Health Division, San Francisco Department of Public Health3 Adjunct Faculty, University of California, Berkeley School of Public Health* Address: 101 Grove St., Rm 308, SF, CA 94102; Email: [email protected]
1

background 2
background
Purpose
I am the health officer of the City & County of San Francisco,and director of the Population Health Division at the De-partment of Public Health. As health officer, I exercise lead-ership and legal authority to protect and promote health. AsPHD director, I direct public health services. My passionsare health equity and team leadership development to trans-form organizations and communities into healthy, thriving,learning, healing, and resilient organizations and communi-ties. Why teams? Teams are the smallest operational unitsthat can be trained, deployed, and combined to tackle com-plex adaptive organizational, community, and societal chal-lenges.
This document contains my personal notes summariz-ing the concepts, frameworks, and tools that I rely on andpromote for population health work. This is my strategicroadmap for self, team, and organization development. Itis dynamic and evolving. I share this document so my staffand colleagues understand my thinking and acting; so theycan teach me and support my professional development;and so they can hold me accountable to my values and prin-ciples. I hope others find this useful in their own develop-ment. I welcome critical feedback and questions.
The challenge of leading population health requires sig-nificant amounts of knowledge, skills, and abilities. It canbe overwhelming! No one can master everything! Therefore,we must cultivate and practice relentless humility, curiosity,and courage. Humility is the most important! “Humility isthe noble choice to forgo your status and use your influencefor the good of others before yourself” [1]. The more poweror privilege we have, the more we must cultivate humility.Humility generates trust. Humility generates learning andcontinuous improvement. Humility generates servant lead-ership.
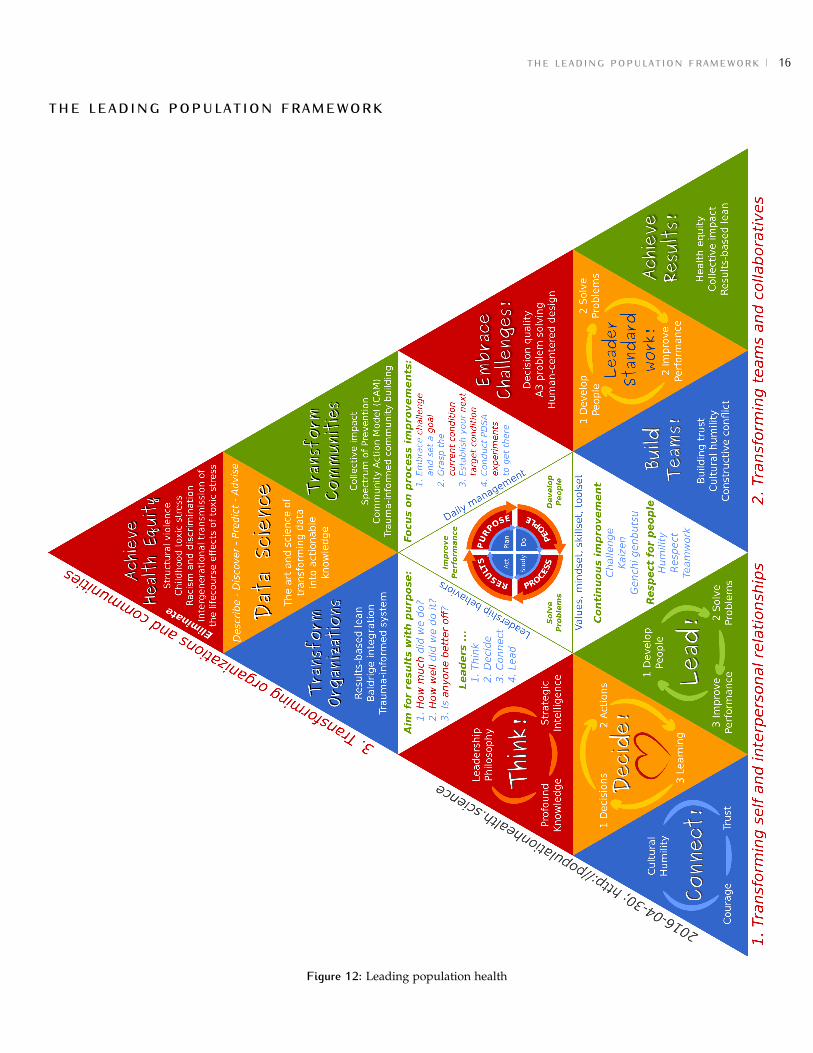
The Leading Population Health framework (Figure 12 onpage 16) has four interdependent components:
1. Transforming self and interpersonal relationships2. Transforming teams and collaboratives3. Transforming organizations and communities4. Improving performance with results-based lean
My underlying premise is that if we cannot optimally trans-form ourselves, our teams, and our organizations, then we will notbe able to partner successfully to optimally transform communities.
An “optimal” transformation is one that results in a team, or-ganization, or community that is healthy, thriving, learning,healing, and resilient. Healthy includes the “Eight Dimen-sions of Wellness,”1 thriving means high performing, learn-ing means continuous improvement, healing means trauma-informed, and resilient means resistant to and rapid recov-ery from serious threats.
These high-level summary notes are mostly in outlineform. Updated versions will be posted here:
Population health overview
We start with some key definitions. “Health is a state of com-plete physical, mental and social well-being and not merelythe absence of disease or infirmity” [2]. “Public health is whatwe, as a society, do collectively to assure the conditions inwhich people can be healthy” [3]. Public health leadershipis “the practice of mobilizing people, organizations, andcommunities to effectively tackle tough public health chal-lenges” [4]. Population health “is a systems framework forstudying and improving the health of populations throughcollective action and learning.”2 Lean thinking and practiceis “to systematically develop people and continuously im-prove processes to provide value for customers and prosper-ity for the organization while consuming the fewest possibleresources.”3 Here are key population health approaches:
Essential population health goals
Essential population health goals must include
1. Protecting and promoting health and equity2. Transforming people and place3. Ensuring a healthy planet4. Achieving health equity
The 4Ps of public health
Public health practice or activities can be categoried into theThe 4Ps of public health:
1. Protect (health protection)2. Promote (health promotion)3. Prevent (disease and injury prevention)4. Prepare (resiliency, risk mitigation, consequence man-
agement, recovery)
1 http://www.samhsa.gov/wellness-initiative/eight-dimensions-wellness2 Source: Tomás Aragón; posted at http://medepi.com3 Source: John Shook from the Lean Enterprise Institute4 Source: Tomás J Aragón; inspired by Bay Area Regional Health Inequities Initiative (BARHII) and Dr. Tony Iton

background 3
The 6Ps of complex social systems
When deploying one or more of the 4P’s of public health wecan target, engage, and mobilize one or more of the 6Ps ofcomplex social systems.4 The 6Ps of complex social systemsalways applies to everyone, everywhere, and in every situa-tion. It is holistic, complete, and dynamic (adapting, evolv-ing).
The 6Ps of complex social systems can be used to mo-bilize a collaborative with mutually-reinforcing activities toaddress a common agenda. This is called collective impact(more on this later).
1. People (belief systems, mental models, norms, ’isms)2. Policy (social and organizational)3. Place (neighborhoods, communities, social networks)4. Program (program, agency, or service system)5. Provider (clinician, teacher, employer)6. Person (patient, student, employee)
The Spectrum of Prevention
A powerful way to use the 4Ps of public health and the 6Psof complex social systems is to deploy the Prevention Insti-tute’s Spectrum of Prevention.5 We use an updated versionfrom Contra Costa Public Health:6
1. Influencing policy and legislation2. Mobilizing neighborhoods and communities3. Changing organizational practices4. Fostering coalitions and networks5. Educating providers
6. Promoting community education7. Strengthening individual knowledge and skills8. Assuring access to quality health care
The Social Determinants of Health
Our health and wellness, our diseases and injuries, arelargely determined by historical, economic, social, and en-vironmental forces that shape our conditions, epigenetics,opportunities, and choices. We call these the “social deter-minants of health.”
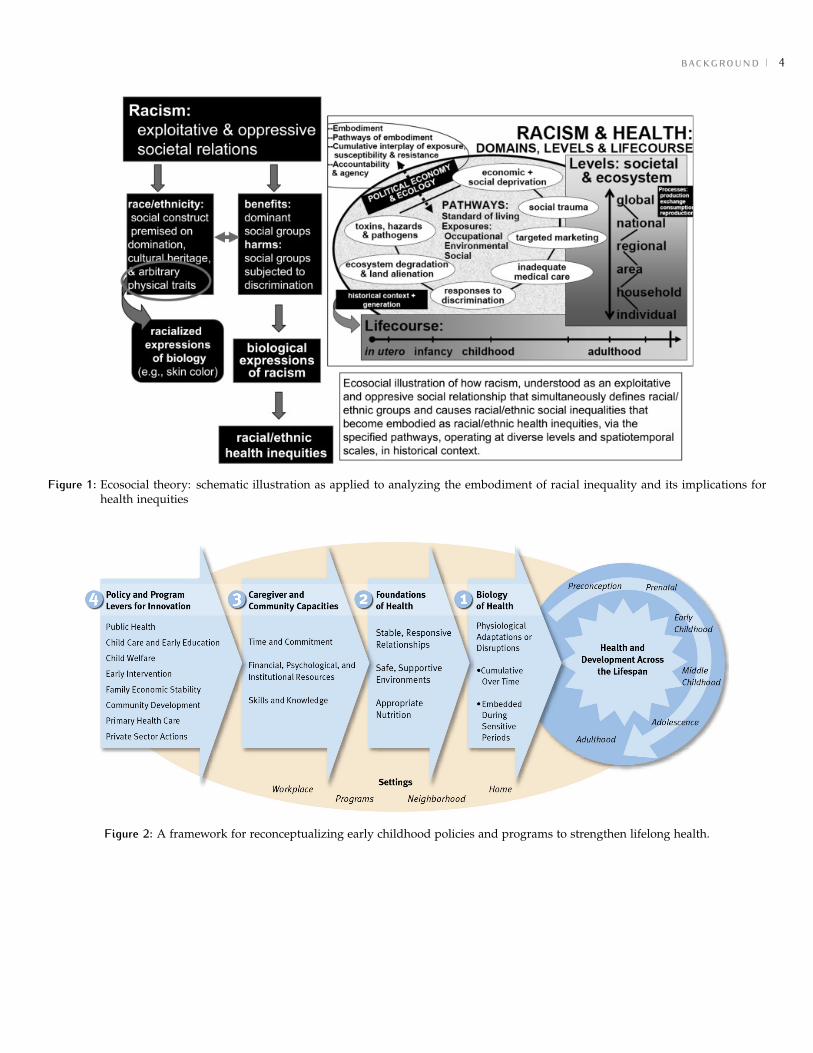
ecosocial theory Nancy Krieger’s ecosocial theorymodel is displayed in Figure 1 on the next page and includesracism and discrimination [5].
two-generational logic model The Center on the De-veloping Child’s two-generational logic model is displayedin Figure 2 on the following page [6].
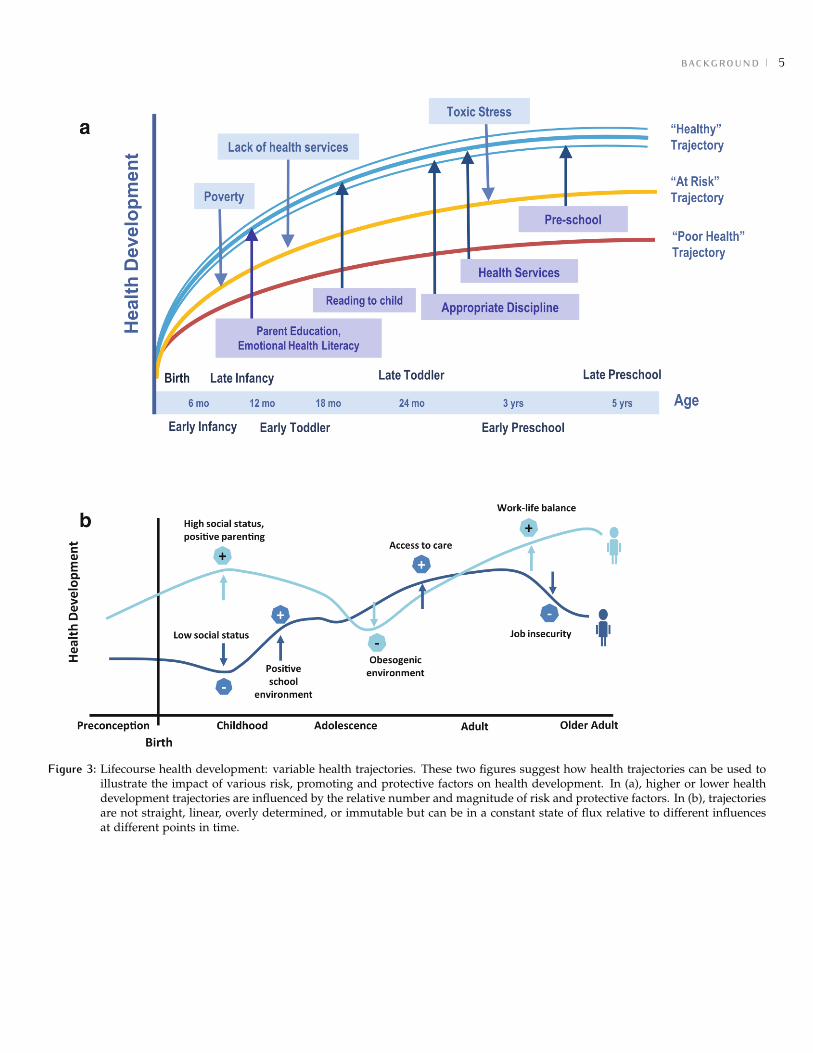
lifecourse health development Neal Halfon’s life-course health development (LCHD) trajectories are depictedin Figure 3 on page 5 [7].
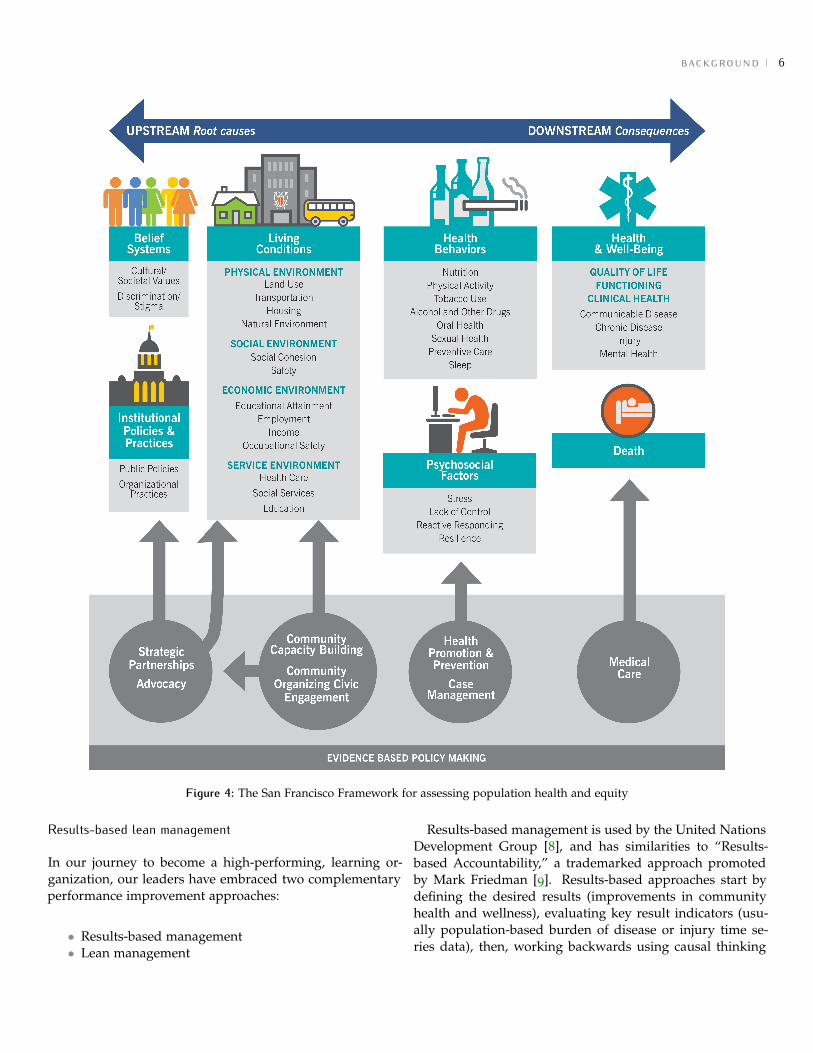
the san francisco framework The San FranciscoFramework (Figure 4 on page 6) for assessing populationhealth and equity was inspired by the Bay Area Health In-equities Initiative (BARHII) framework.7 An important ad-dition is that the San Francisco Framework includes beliefsystems (i.e., the first P in the 6P’s of complex social systems).
5 http://www.preventioninstitute.org6 http://cchealth.org/prevention/spectrum/7 https://www.cdph.ca.gov/programs/mcah/Documents/BARHIIFramework.pdf
background 4
Figure 1: Ecosocial theory: schematic illustration as applied to analyzing the embodiment of racial inequality and its implications forhealth inequities
Figure 2: A framework for reconceptualizing early childhood policies and programs to strengthen lifelong health.
background 5
Figure 3: Lifecourse health development: variable health trajectories. These two figures suggest how health trajectories can be used toillustrate the impact of various risk, promoting and protective factors on health development. In (a), higher or lower healthdevelopment trajectories are influenced by the relative number and magnitude of risk and protective factors. In (b), trajectoriesare not straight, linear, overly determined, or immutable but can be in a constant state of flux relative to different influencesat different points in time.
background 6
Figure 4: The San Francisco Framework for assessing population health and equity
Results-based lean management
In our journey to become a high-performing, learning or-ganization, our leaders have embraced two complementaryperformance improvement approaches:
• Results-based management• Lean management
Results-based management is used by the United NationsDevelopment Group [8], and has similarities to “Results-based Accountability,” a trademarked approach promotedby Mark Friedman [9]. Results-based approaches start bydefining the desired results (improvements in communityhealth and wellness), evaluating key result indicators (usu-ally population-based burden of disease or injury time se-ries data), then, working backwards using causal thinking

background 7
(informed by root-cause and force field analyses) to designstrategies and activities that are informed by scientific andcommunity-based evidence.
We start the collaborative process by convening stakehold-ers who are already contributing to solutions. By aligning,coordinating, and improving existing efforts we attempt toachieve collective impact. It is easier to mobilize partnersby starting with existing activities they are already inspiredto do, and by focusing on the pursuit of a shared vision(desired results). We use two results-based methods:
• Four strategic questions (4SQ)• Results-based management (RBM) questions
The 4SQ are used for daily or short-term action planningnot involving significant problem solving. In contrast, RBMis an extension of 4SQ that includes extensive collaborativeproblem solving. RBM is used for collective impact projects(Table 1).
Table 1: Results-based methods: four strategic questions (4SQ) and results-based management (RBM) questions
Four strategic questions (4SQ) Results-based management (RBM)questions
Comments
1. What are we trying to accomplishand why?
1. What are the goals? Strategic goals (what) and purpose(why)
2. How do we measure success? 2. How are we doing? (includeforecast: consequence continuingof the status quo)
Result indicators: outputs,outcomes, impacts; program orpopulation level
3. What partners can help? Stakeholder analysis, engagement,alignment, coordination,collaboration
4. What are the drivers? (“What’s thestory behind the curve?”*)
Causal evidence, root causeanalysis, community-basedevidence
5. What strategies work? (“Whatworks to turn the curve?”*)
Prioritize: cost-effective, promisingpractices, community-basedevidence
3. What other conditions must exist? 6. What other conditions must exist? Assumptions and riskmanagement
4. How do we get there? 7. How do we get there? Plan-Do-Study-Act (PDSA) cyles*Results-based accountability (RBA) by Mark Friedman
Results-based approaches have their origins incommunity-based public health practice. However, leanexperts are quick to remind us of the dangers of focusingsolely on results. In contrast, lean focuses on prioritizing pro-cess improvements by eliminating waste—processes that do notadd “value” as defined by customers. Here is John Shook’sdefinition of lean thinking and practice: to systematicallydevelop people and continuously improve processes to pro-vide value for customers and prosperity for the organizationwhile consuming the fewest possible resources. Most oftenvalue is defined as what the customer is willing to pay for(the value proposition). Similar to health care systems, inpopulation health we aspire to deliver services that have thehighest level of
• patient experience (safety, quality, satisfaction)• lowest per capita cost.
Beyond this common focus, we aspire to protect and im-prove health and well-being “at the source”—in the commu-nity, upstream (social determinants), and early in the lifecourse. (When health care systems genuinely include thispopulation health focus, it is called the “Triple Aim.” Inour experience, health care and public health generally havedifferent operational definitions of “population health.”)
Therefore, our highest priority is partnering with com-munities and policy makers to improve the social determi-nants of health. This leads to socioecological frameworksand practices that go beyond the scope of most health caresystems. In population health, we go beyond traditional cus-tomer value to include improving population health results(outputs, outcomes, and impacts) and achieving populationhealth goals.

background 8
In our experience, some of our “customers” are not will-ing to pay for social policies that protect and promote healthand well-being (e.g., laws limiting involuntary exposuresto secondhand tobacco smoke, soda tax, mandatory vac-cinations, controlling industrial pollution of the environ-ment). Sometimes we must fight for the health protectionof our most vulnerable populations (low-income, marginal-ized, discriminated, young, elderly, etc.).
Results-based lean philosophy
Lean and results-based approaches are complementary andsynergistic. We have come to realize that we are practicingwhat we call results-based lean (RBL). The RBL LeadershipPhilosophy for organization transformation is displayed inFigure 5. For any challenge we must have the followingsituational mindset:
Figure 5: Results-based lean (RBL) leadership mindset
1. Alignment to purpose: What is the new challenge(problem or opportunity) or goal? How does tacklingthis challenge align with our value-driven purpose?
a) Purpose [why] (+ vision, values, and principles)b) People [who] (communities, patients, and staff)c) Processes [how] (problem solving/improvement)d) Results [what] (outputs, outcomes, impacts) and
Goals (“Is anyone better off?”)
2. PDSA experimentation (scientific problem solving):How do we tackle this challenge?
a) Plan (planning or proposed countermeasures)b) Do (experimenting or project schedule)c) Study (analyzing or interpretation)
d) Act (adjusting or proposed adjustments)
3. Leader standard work: What are the necessary leader-ship behaviors?
a) develop people (coach and mentor)b) embrace challenges (problems or opportunities)c) improve performance (processes and results)
4. Daily management: What daily management systemensures continuous improvement?
5. Culture, values, mindsets, habits: What culture, val-ues, mindsets (thinking), and habits (acting) supportthe RBL transformation? Start with these:
a) Challenge (growth mindset)b) Genchi genbutsu (gemba walk to see/understand)c) Kaizen (daily continuous improvement)d) Humility (forgo status; open heart and mind)e) Respect (for people)f) Teamwork (relentless collaboration)
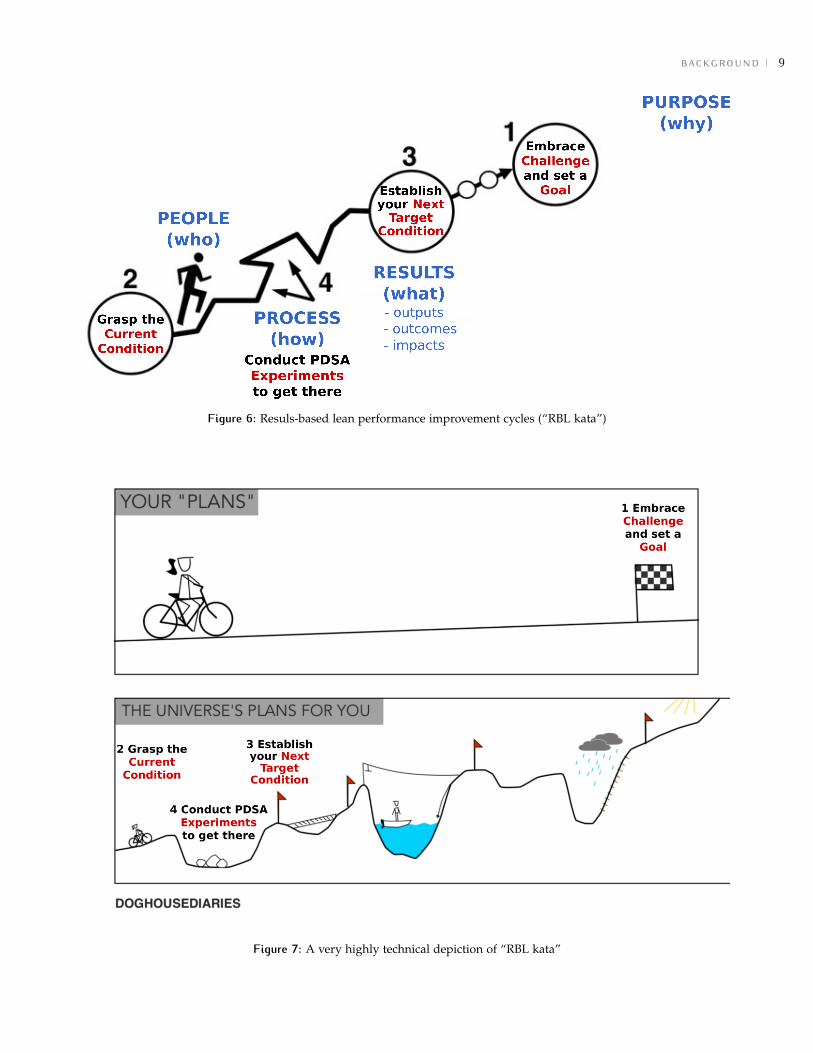
Results-based lean improvement cyles (“RBL kata” )
Inspired by Mike Rother’s Toyota Kata [10], Figure 6 on thenext page graphically depicts the performance improvementcycles (“kata”) of results-based lean. We start by looking for,recognizing, or being assigned a challenge. Challenges areopportunties to make things better; they are improvementopportunities: a problem that needs solving, a new oppor-tunity that needs pursuing, or an assigned goal or objectivethat needs completing. There are four steps:
1. Embrace the challenge
a) Align with organizational purposeb) Set goals (How do we measure success?)
2. Grasp the current condition3. Establish the target condition4. Conduct PDSA experiments to get there
This RBL approach extends the results-based manage-ment approach to include PDSA experiments (scientificproblem solving). A key revelation is that everything we dois an experiment—everything! There is what we expect to hap-pen, and there is what actually happens. Learning occurs whenwe carefully observe and seek to understand why the differ-ence. Adaptation occurs when we combine what we learnedwith change for the future. Ultimately, the adaptation is animprovement if our result metrics improve.
For those who need it, a more technical approach to theseconcepts is depicted in Figure 7 on the following page.
background 9
Figure 6: Resuls-based lean performance improvement cycles (“RBL kata”)
Figure 7: A very highly technical depiction of “RBL kata”
transform self and interpersonal relationships 10
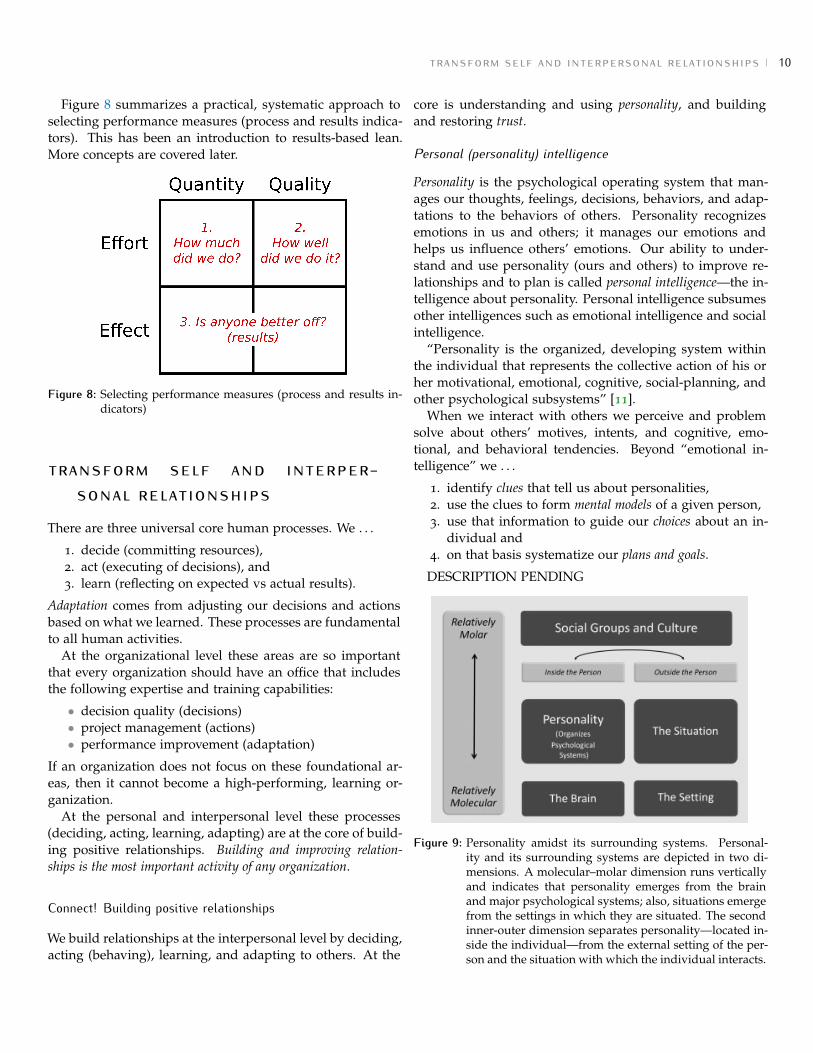
Figure 8 summarizes a practical, systematic approach toselecting performance measures (process and results indica-tors). This has been an introduction to results-based lean.More concepts are covered later.
Figure 8: Selecting performance measures (process and results in-dicators)
transform self and interper-sonal relationships
There are three universal core human processes. We . . .
1. decide (committing resources),2. act (executing of decisions), and3. learn (reflecting on expected vs actual results).
Adaptation comes from adjusting our decisions and actionsbased on what we learned. These processes are fundamentalto all human activities.
At the organizational level these areas are so importantthat every organization should have an office that includesthe following expertise and training capabilities:
• decision quality (decisions)• project management (actions)• performance improvement (adaptation)
If an organization does not focus on these foundational ar-eas, then it cannot become a high-performing, learning or-ganization.
At the personal and interpersonal level these processes(deciding, acting, learning, adapting) are at the core of build-ing positive relationships. Building and improving relation-ships is the most important activity of any organization.
Connect! Building positive relationships
We build relationships at the interpersonal level by deciding,acting (behaving), learning, and adapting to others. At the
core is understanding and using personality, and buildingand restoring trust.
Personal (personality) intelligence
Personality is the psychological operating system that man-ages our thoughts, feelings, decisions, behaviors, and adap-tations to the behaviors of others. Personality recognizesemotions in us and others; it manages our emotions andhelps us influence others’ emotions. Our ability to under-stand and use personality (ours and others) to improve re-lationships and to plan is called personal intelligence—the in-telligence about personality. Personal intelligence subsumesother intelligences such as emotional intelligence and socialintelligence.
“Personality is the organized, developing system withinthe individual that represents the collective action of his orher motivational, emotional, cognitive, social-planning, andother psychological subsystems” [11].
When we interact with others we perceive and problemsolve about others’ motives, intents, and cognitive, emo-tional, and behavioral tendencies. Beyond “emotional in-telligence” we . . .
1. identify clues that tell us about personalities,2. use the clues to form mental models of a given person,3. use that information to guide our choices about an in-
dividual and4. on that basis systematize our plans and goals.
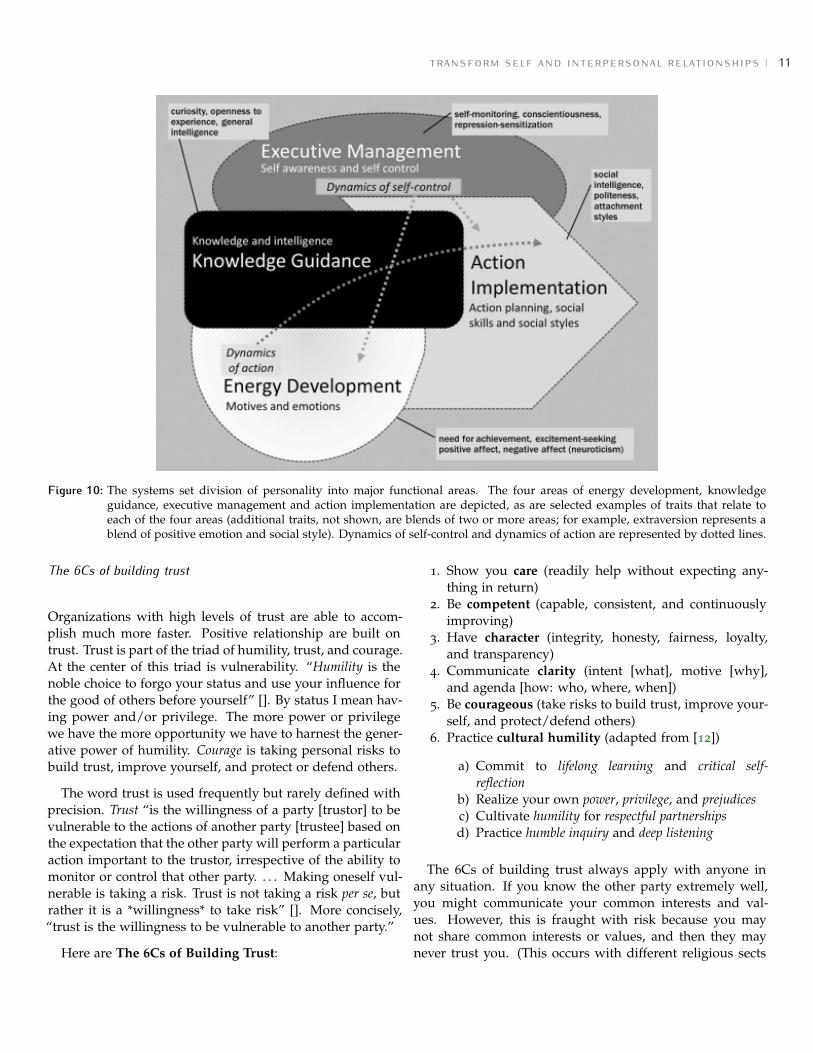
DESCRIPTION PENDING
Figure 9: Personality amidst its surrounding systems. Personal-ity and its surrounding systems are depicted in two di-mensions. A molecular–molar dimension runs verticallyand indicates that personality emerges from the brainand major psychological systems; also, situations emergefrom the settings in which they are situated. The secondinner-outer dimension separates personality—located in-side the individual—from the external setting of the per-son and the situation with which the individual interacts.
transform self and interpersonal relationships 11
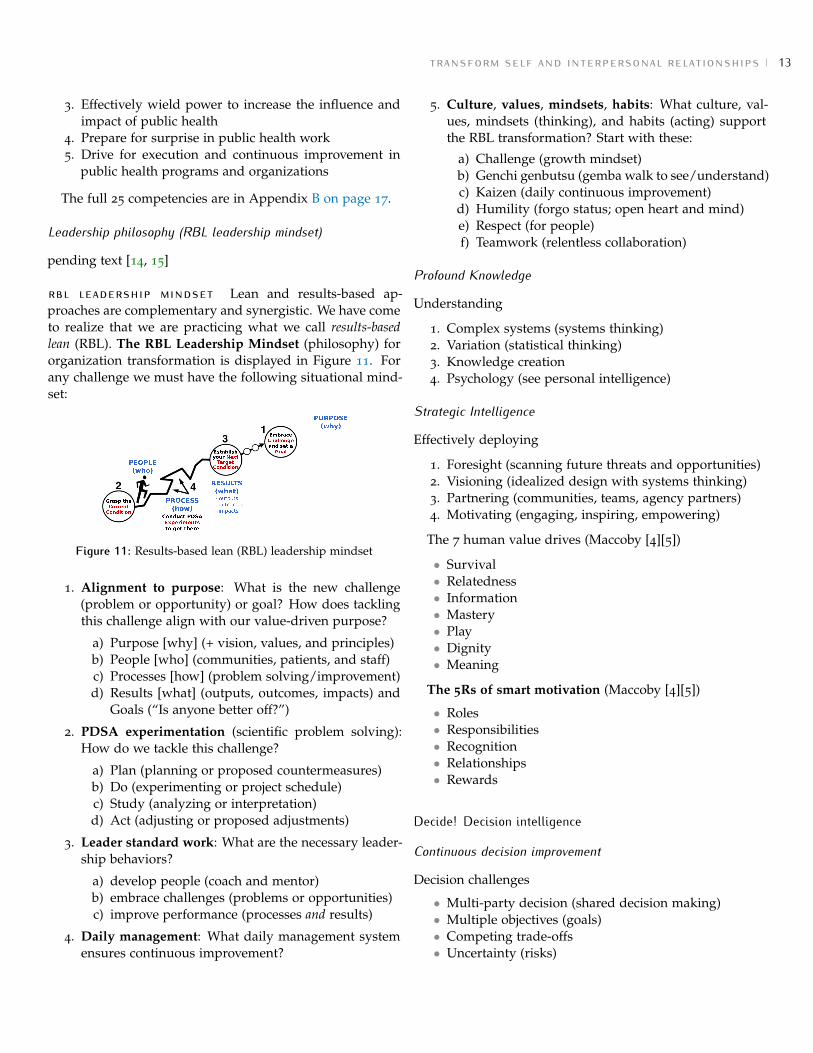
Figure 10: The systems set division of personality into major functional areas. The four areas of energy development, knowledgeguidance, executive management and action implementation are depicted, as are selected examples of traits that relate toeach of the four areas (additional traits, not shown, are blends of two or more areas; for example, extraversion represents ablend of positive emotion and social style). Dynamics of self-control and dynamics of action are represented by dotted lines.
The 6Cs of building trust
Organizations with high levels of trust are able to accom-plish much more faster. Positive relationship are built ontrust. Trust is part of the triad of humility, trust, and courage.At the center of this triad is vulnerability. “Humility is thenoble choice to forgo your status and use your influence forthe good of others before yourself” []. By status I mean hav-ing power and/or privilege. The more power or privilegewe have the more opportunity we have to harnest the gener-ative power of humility. Courage is taking personal risks tobuild trust, improve yourself, and protect or defend others.
The word trust is used frequently but rarely defined withprecision. Trust “is the willingness of a party [trustor] to bevulnerable to the actions of another party [trustee] based onthe expectation that the other party will perform a particularaction important to the trustor, irrespective of the ability tomonitor or control that other party. . . . Making oneself vul-nerable is taking a risk. Trust is not taking a risk per se, butrather it is a *willingness* to take risk” []. More concisely,“trust is the willingness to be vulnerable to another party.”
Here are The 6Cs of Building Trust:
1. Show you care (readily help without expecting any-thing in return)
2. Be competent (capable, consistent, and continuouslyimproving)
3. Have character (integrity, honesty, fairness, loyalty,and transparency)
4. Communicate clarity (intent [what], motive [why],and agenda [how: who, where, when])
5. Be courageous (take risks to build trust, improve your-self, and protect/defend others)
6. Practice cultural humility (adapted from [12])
a) Commit to lifelong learning and critical self-reflection
b) Realize your own power, privilege, and prejudicesc) Cultivate humility for respectful partnershipsd) Practice humble inquiry and deep listening
The 6Cs of building trust always apply with anyone inany situation. If you know the other party extremely well,you might communicate your common interests and val-ues. However, this is fraught with risk because you maynot share common interests or values, and then they maynever trust you. (This occurs with different religious sects

transform self and interpersonal relationships 12
and political parties.) A better approach is to build trustfirst. You want to be trusted in spite of your differences.
Think! Leadership intelligence
Leadership intelligence is intelligence about leadership.“An intelligence represents a group of related abilities—aperson’s mental capacities to correctly solve a broad set ofrelated problems of a particular type that our society recog-nizes as being of importance” [13]. Intelligence enables oneto problem solve in new situations where the path forwardis not readily apparent. We can improve an intelligencethrough study, practice, reflection, and continuous improve-ment.
Leadership intelligence consists of having knowledge,skills, and abilities in the following areas:
1. Leadership competencies2. Leadership philosophy3. Profound knowledge4. Stategic intelligence
Leadership competencies
A competency is defined as the “effective application ofvalues, traits, knowledge, and skills in complex situations”[4]. Leadership competencies can be divided into three cate-gories:
• How to be• What to know• What to do
how to be (part 1/2): Here are the values of effectivepublic health leaders [4]:
• Social justice• Reliance on evidence• Interdependence• Respect• Community self-determination• Requisite role of government• Transparency
The full descriptions are in Appendix B on page 17.
how to be (part 2/2): Here are the character traits ofeffective public health leaders [4]:
• Integrity• Initiative• Empathy• Comfort with ambiguity
• Passion• Courage• Persistence
The full descriptions are in Appendix B on page 17.
what to know (part 1/2): Here is the knowledge baseof effective public health leaders [4]:
• Public health science:
– Analytic / assessment;– Basic public health sciences (biostatistics, epi-
demiology, environmental health, health policyand management, social and behavioral sciences);
– Cultural competency (see cultural humility);– Communication;– Community dimensions of practice;– Financial planning and management;– Leadership and systems thinking;– Policy development / Program planning
• Understanding people (see personal intelligence in sec-tion 2.1.1 on page 10)
– Motivation– Social and emotional intelligence
• Understanding complex systems
– Systems thinking– Focusing on complex adaptive systems
• Changing people, organizations, and communities
– Change management– Culture of innovation– Positive deviance
The full descriptions are in Appendix B on page 17.
what to know (part 2/2): Here are the key characteris-tics of public health knowledge:
• Evidence-based• Dynamic• Prevention-focused• Transdisciplinary• Value-laden
The full descriptions are in Appendix B on page 17.
what to do: Here are the five core competencies of effec-tive public health leaders:
1. Invigorate bold pursuit of population health2. Engage diverse others in public health initiatives
transform self and interpersonal relationships 13
3. Effectively wield power to increase the influence andimpact of public health
4. Prepare for surprise in public health work5. Drive for execution and continuous improvement in
public health programs and organizations
The full 25 competencies are in Appendix B on page 17.
Leadership philosophy (RBL leadership mindset)
pending text [14, 15]
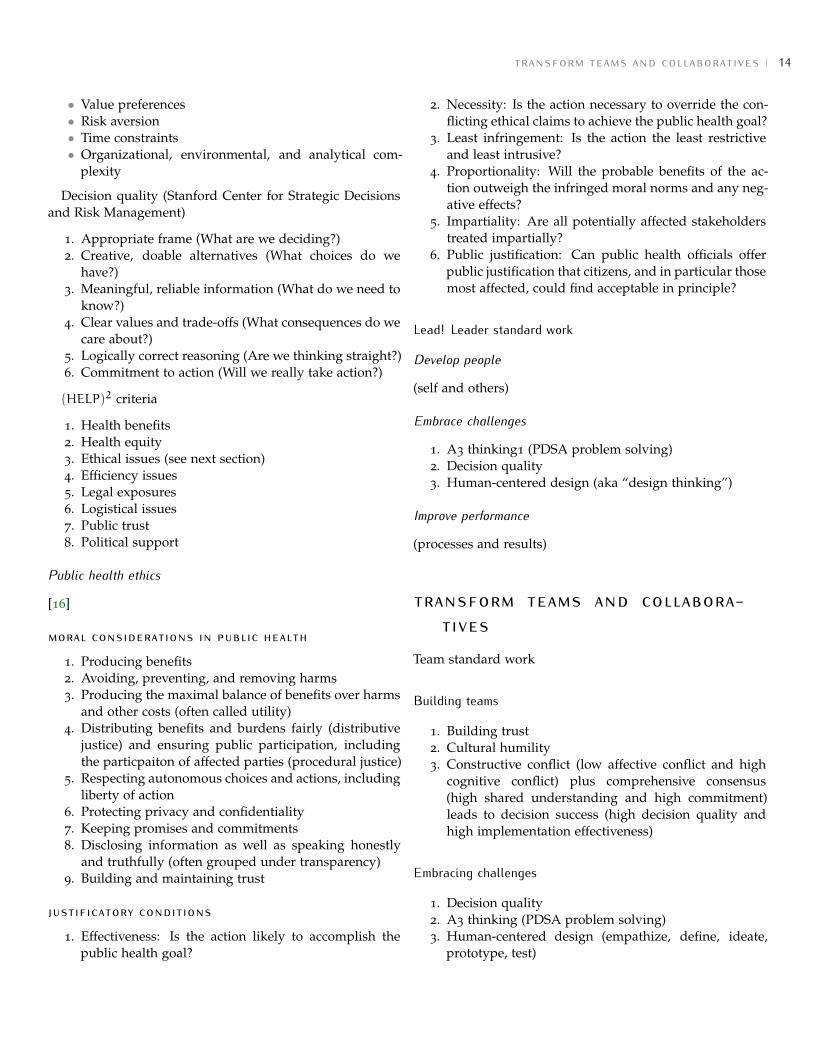
rbl leadership mindset Lean and results-based ap-proaches are complementary and synergistic. We have cometo realize that we are practicing what we call results-basedlean (RBL). The RBL Leadership Mindset (philosophy) fororganization transformation is displayed in Figure 11. Forany challenge we must have the following situational mind-set:
Figure 11: Results-based lean (RBL) leadership mindset
1. Alignment to purpose: What is the new challenge(problem or opportunity) or goal? How does tacklingthis challenge align with our value-driven purpose?
a) Purpose [why] (+ vision, values, and principles)b) People [who] (communities, patients, and staff)c) Processes [how] (problem solving/improvement)d) Results [what] (outputs, outcomes, impacts) and
Goals (“Is anyone better off?”)
2. PDSA experimentation (scientific problem solving):How do we tackle this challenge?
a) Plan (planning or proposed countermeasures)b) Do (experimenting or project schedule)c) Study (analyzing or interpretation)d) Act (adjusting or proposed adjustments)
3. Leader standard work: What are the necessary leader-ship behaviors?
a) develop people (coach and mentor)b) embrace challenges (problems or opportunities)c) improve performance (processes and results)
4. Daily management: What daily management systemensures continuous improvement?
5. Culture, values, mindsets, habits: What culture, val-ues, mindsets (thinking), and habits (acting) supportthe RBL transformation? Start with these:
a) Challenge (growth mindset)b) Genchi genbutsu (gemba walk to see/understand)c) Kaizen (daily continuous improvement)d) Humility (forgo status; open heart and mind)e) Respect (for people)f) Teamwork (relentless collaboration)
Profound Knowledge
Understanding
1. Complex systems (systems thinking)2. Variation (statistical thinking)3. Knowledge creation4. Psychology (see personal intelligence)
Strategic Intelligence
Effectively deploying
1. Foresight (scanning future threats and opportunities)2. Visioning (idealized design with systems thinking)3. Partnering (communities, teams, agency partners)4. Motivating (engaging, inspiring, empowering)
The 7 human value drives (Maccoby [4][5])
• Survival• Relatedness• Information• Mastery• Play• Dignity• Meaning
The 5Rs of smart motivation (Maccoby [4][5])
• Roles• Responsibilities• Recognition• Relationships• Rewards
Decide! Decision intelligence
Continuous decision improvement
Decision challenges
• Multi-party decision (shared decision making)• Multiple objectives (goals)• Competing trade-offs• Uncertainty (risks)
transform teams and collaboratives 14
• Value preferences• Risk aversion• Time constraints• Organizational, environmental, and analytical com-
plexity
Decision quality (Stanford Center for Strategic Decisionsand Risk Management)
1. Appropriate frame (What are we deciding?)2. Creative, doable alternatives (What choices do we
have?)3. Meaningful, reliable information (What do we need to
know?)4. Clear values and trade-offs (What consequences do we
care about?)5. Logically correct reasoning (Are we thinking straight?)6. Commitment to action (Will we really take action?)
(HELP)2 criteria
1. Health benefits2. Health equity3. Ethical issues (see next section)4. Efficiency issues5. Legal exposures6. Logistical issues7. Public trust8. Political support
Public health ethics
[16]
moral considerations in public health
1. Producing benefits2. Avoiding, preventing, and removing harms3. Producing the maximal balance of benefits over harms
and other costs (often called utility)4. Distributing benefits and burdens fairly (distributive
justice) and ensuring public participation, includingthe particpaiton of affected parties (procedural justice)
5. Respecting autonomous choices and actions, includingliberty of action
6. Protecting privacy and confidentiality7. Keeping promises and commitments8. Disclosing information as well as speaking honestly
and truthfully (often grouped under transparency)9. Building and maintaining trust
justificatory conditions
1. Effectiveness: Is the action likely to accomplish thepublic health goal?
2. Necessity: Is the action necessary to override the con-flicting ethical claims to achieve the public health goal?
3. Least infringement: Is the action the least restrictiveand least intrusive?
4. Proportionality: Will the probable benefits of the ac-tion outweigh the infringed moral norms and any neg-ative effects?
5. Impartiality: Are all potentially affected stakeholderstreated impartially?
6. Public justification: Can public health officials offerpublic justification that citizens, and in particular thosemost affected, could find acceptable in principle?
Lead! Leader standard work
Develop people
(self and others)
Embrace challenges
1. A3 thinking1 (PDSA problem solving)2. Decision quality3. Human-centered design (aka “design thinking”)
Improve performance
(processes and results)
transform teams and collabora-tives
Team standard work
Building teams
1. Building trust2. Cultural humility3. Constructive conflict (low affective conflict and high
cognitive conflict) plus comprehensive consensus(high shared understanding and high commitment)leads to decision success (high decision quality andhigh implementation effectiveness)
Embracing challenges
1. Decision quality2. A3 thinking (PDSA problem solving)3. Human-centered design (empathize, define, ideate,
prototype, test)
transform organizations and communities 15
Achieving results
1. Health equity2. Collective impact 2.0 (adapted from http://www.fsg.org)
a) Common agenda (goals)b) Shared measurement (results and processes)c) Mutually-reinforcing activitiesd) Continuous improvement (results-based lean)e) Backbone support and continuous communica-
tion
3. Daily management (results-based lean)
transform organizations and com-munities
Transforming organizations
Design a learning organization
Design a healing organization
• Understanding trauma and stress• Compassion and dependability• Safety and stability• Collaboration and empowerment• Cultural humility and responsiveness• Resilience and recovery
Design an integrated organization
baldrige integration
1. Leadership2. Strategy3. Customers4. Data science (1–3, 4–7)5. Workforce6. Operations7. Results (1–3, 4, 7, finance and markets)
Transforming communities
Collective impact 2.0
Community-based participatory approach
Trauma-informed community building
Achieving health equity
childhood roots of adults health inequities(a) Problem: intergenerational transmission of toxic
stress4; toxic stress alters brain, body, and behavior affectingdecision making, self-regulation, and physiology; life courseof toxic stress from trauma, racism, and discrimination.
(b) Solution: trauma-informed community building andsocial policy (prevent and protect from toxic stress; prepareby building resiliency skills; and promote healthy, enrich-ment opportunities)
the leading population framework 16
the leading population framework
Figure 12: Leading population health

leadership competencies 17
leadership competencies
How to be: character traits and values
Values of effective public health leaders
1. Social justice: Acceptance of health as a universal, fundamental human right for all, and a strong commitment tocorrecting patterns of systematic disadvantage to population subgroups
2. Reliance on evidence: Requirement that evidence informs and challenges decision making, accompanied by ahealthy skepticism about existing practices, mindsets, and outcomes; helps mitigate groupthink among like-mindedpublic health practitioners
3. Interdependence: Recognition of the need to work with and in collaboration with diverse individuals and commu-nities rather than independent pursuits; enhanced by the impact of social determinants on population health
4. Respect: At the personal level, a way of regarding another individual that denotes the individual is important;manifested in soliciting input from the individual, listening, and doing so in a way that is sensitive to the individual’sculture and individuality
5. Community self-determination: Respect for the right and ability of communities to define their own issues andinterventions; serve as a coalition builder rather than the agenda-setter
6. Requisite role of government: Belief in the value of public service and the role of government action to protect thepublic’s health
7. Transparency: Public and other stakeholders have the right to information; develops trust and promotes constructivepolitics
Character traits of effective public health leaders
1. Integrity: Honesty, truthfulness, and consistent action in accord with one’s values; key to credibility and strength inthe face of attack
2. Initiative: Drive to change; willingness to take charge and take risks when necessary3. Empathy: Interest in and ability to relate to people4. Comfort with ambiguity: Comfort with lack of clear boundaries and hierarchy in work settings5. Passion: Deep commitment to values of public health, profession of public health, and service6. Courage: Willingness to take unpopular stands on high-visibility issues and to push harder, to insist more vigorously,
more effectively, and over a longer period of time7. Persistence: Patience with long-term cultural, social, and multi-generational change
What to know: public health knowledge
Knowledge for public health leadership
• Public health science:
– Analytic / assessment;– Basic public health sciences (biostatistics, epidemiology, environmental health, health policy and management,
social and behavioral sciences);– Cultural competency;– Communication;– Community dimensions of practice;– Financial planning and management;– Leadership and systems thinking;– Policy development / Program planning
• Understanding people
– Motivation

leadership competencies 18
– Social and emotional intelligence
• Understanding complex systems
– Systems thinking– Focusing on complex adaptive systems
• Changing people, organizations, and communities
– Change management– Culture of innovation– Positive deviance
Key characteristics of public health knowledge
• Evidence-based
– Correlates with an emphasis on science and scientific research– Uses evidence as a key weapon in tackling public health challenges in political arenas– Grows largely through the accumulation of scientific evidence-based– Empowers societal influence of public health leaders and the field
• 2. Dynamic
– Changes frequently, particularly knowledge connected to scientific disciplines– Invites an attitude of learning by public health leaders– Demands the push for new evidence where it is needed– Requires leaders’ openness to change their minds where compelling evidence is identified
• 3. Prevention-focused
– Directs most public health knowledge toward preventing the emergence of health problems– Compels focus on addressing the root causes of health problems to prevent them– Enables a “return-on-investment” mindset that reflects the shard belief in the value of prevention
• Transdisciplinary
– Driven by problems rather than traditional boundaries of scientific disciplines– Welcomes acceptance of relevant information from other fields and disciplines, as well as their potential limita-
tions– Encourages cross-sector collaboration within and outside clinical and scientific fields
• Value-laden
– Characterized by strongly political nature of field due to value conflict inherent in most population health issues– Raises questions about the allocation of public resources relative to government regulation and intervention,
legal and ethical concerns, and political influences– Requires political debate over both the means and ends for improving population health
What to do: 25 essential competencies
Here are the five core competencies (A–E) expanded into 25 essential competencies (1–25) of effective public healthleaders:
A. Invigorate bold(er) pursuit of population health
1. Critically assess the current state of your program or organization2. Articulate a more compelling agenda3. Enlist others in the vision and invigorate them to drive toward it4. Pursue the vision with rigor and flexibility5. Marshal the needed resources

trauman informed system core principles 19
B. Engage diverse others in public health initiatives
6. Assess local conditions, in ways relevant and credible to the local stakeholders.7. Search widely for the right partners8. Apply a social determinants perspective to planning9. Take time to build relationships, teamwork, and common understanding
10. Clarify roles and governance
C. Effectively wield power to increase the influence and impact of public health
11. Understand and strategically use both positional authority and informal influence12. Analyze a given public health problem and proposed solution in “campaign” terms13. Build coalitions of core supporters, new partners, and issue-specific allies14. Deal effectively with opponents15. Be strategically agile
D. Prepare for surprise in public health work
16. Promote resilience in individuals and communities17. Develop and critique an emergency response plan18. Communicate effectively during surprises19. Execute an emergency response plan with flexibility and learning20. Learn and improve after surprises
E. Drive for execution and continuous improvement in public health programs and organizations
21. Build accountability into public health teams, programs, and organizations22. Establish metrics, set targets, monitor progress, and take action23. Proactively demonstrate financial stewardship of public health funds24. Employ the methods and tools of quality improvement25. Encourage innovation and risk-taking
trauman informed system core principles
Understanding Trauma and Stress
Without understanding trauma, we are more likely to adopt behaviors and beliefs that are negative and unhealthy. How-ever, when we understand trauma and stress we can act compassionately and take well- informed steps toward wellness.
1. Trauma: We understand that trauma is common, but experienced uniquely due to its many variations in form andimpact.
2. Stress: We understand that optimal levels of positive stress can be healthy, but that chronic or extreme stress hasdamaging effects.
3. Reactions: We understand that many trauma reactions are adaptive, but that some resulting behaviors and beliefsmay impede recovery and wellness.
4. Recovery: We understand that trauma can be overcome effectively through accessible treatments, skills, relationships,and personal practices.
Compassion and Dependability
Trauma is overwhelming and can leave us feeling isolated or betrayed, which may make it difficult to trust others andreceive support. However, when we experience compassionate and dependable relationships, we reestablish trustingconnections with others that foster mutual wellness.

trauman informed system core principles 20
1. Compassion: We strive to act compassionately across our interactions with others through the genuine expressionof concern and support.
2. Relationships: We value and seek to develop secure and dependable relationships characterized by mutual respectand attunement.
3. Communication: We promote dependability and create trust by communicating in ways that are clear, inclusive, anduseful to others.
Safety and Stability
Trauma unpredictably violates our physical, social, and emotional safety resulting in a sense of threat and need to managerisks. Increasing stability in our daily lives and having these core safety needs met can minimize our stress reactions andallow us to focus our resources on wellness.
1. Stability: We minimize unnecessary changes and, when changes are necessary, provide sufficient notice and prepa-ration.
2. Physical: We create environments that are physically safe, accessible, clean, and comfortable.
3. Social-Emotional: We maintain healthy interpersonal boundaries and manage conflict appropriately in our relation-ships with others.
Collaboration and Empowerment
Trauma involves a loss of power and control that makes us feel helpless. However, when we are prepared for and givenreal opportunities to make choices for ourselves and our care, we feel empowered and can promote our own wellness.
1. Empowerment: We recognize the value of personal agency and understand how it supports recovery and overallwellness.
2. Preparation: We proactively provide information and support the development of skills that are necessary for theeffective empowerment of others.
3. Opportunities: We regularly offer others opportunities to make decisions and choices that have a meaningful impacton their lives.
Cultural Humility and Responsiveness
We come from diverse social and cultural groups that may experience and react to trauma differently. When we are opento understanding these differences and respond to them sensitively we make each other feel understood and wellness isenhanced.
1. Differences: We demonstrate knowledge of how specific social and cultural groups may experience, react to, andrecover from trauma differently.
2. Humility: We are proactive in respectfully seeking information and learning about differences between social andcultural groups.
3. Responsiveness: We have and can easily access support and resources for sensitively meeting the unique social andcultural needs of others.
trauman informed system core principles 21
Resilience and Recovery
Trauma can have a long-lasting and broad impact on our lives that may create a feeling of hopelessness. Yet, when wefocus on our strengths and clear steps we can take toward wellness we are more likely to be resilient and recover.
1. Path: We recognize the value of instilling hope by seeking to develop a clear path towards wellness that addressesstress and trauma.
2. Strengths: We proactively identify and apply strengths to promote wellness and growth, rather than focusing singu-larly on symptom reduction.
3. Practices: We are aware of and have access to effective treatments, skills, and personal practices that support recoveryand resiliency.
References 22
references[1] Dickson J. Humilitas: A Lost Key to Life, Love, and Leadership. Zondervan; 2011. Available from: http://amzn.com/
0310328624.
[2] World Health Organization. WHO definition of Health. World Health Organization; 1948. Preamble to the Constitu-tion of the World Health Organization as adopted by the International Health Conference, New York, 19-22 June, 1946;signed on 22 July 1946 by the representatives of 61 States (Official Records of the World Health Organization, no. 2, p.100) and entered into force on 7 April 1948. Available from: http://www.who.int/about/definition/en/print.html.
[3] Institute of Medicine, Committee for the Study of the Future of Public Health. The Future of Public Health. NationalAcademy Press; 1988. Available from: http://www.nap.edu/catalog/1091.html.
[4] Begun J, Malcolm J. Leading Public Health: A Competency Framework. 1st ed. Springer Publishing Company; 2014.Available from: http://amzn.com/0826199062.
[5] Krieger N. Methods for the scientific study of discrimination and health: an ecosocial approach. Am J Public Health.2012 May;102(5):936–944.
[6] Center on the Developing Child. InBrief: The Foundations of Lifelong Health. Center onthe Developing Child; 2010. Available from: http://developingchild.harvard.edu/resources/inbrief-the-foundations-of-lifelong-health/.
[7] Halfon N, Larson K, Lu M, Tullis E, Russ S. Lifecourse health development: past, present and future. Matern ChildHealth J. 2014 2;18:344–65.
[8] United Nations Development Group (UNDG). Results-Based Management Handbook. United Nations; 2011. Avail-able from: https://undg.org/wp-content/uploads/2014/06/UNDG-RBM-Handbook-2012.pdf.
[9] Friedman M. Trying Hard Is Not Good Enough: How to Produce Measurable Improvements for Customers and Com-munities. 3rd ed. CreateSpace Independent Publishing Platform; 2015. Available from: http://amzn.com/1516971620.
[10] Rother M. Toyota Kata: Managing People for Improvement, Adaptiveness and Superior Results. McGraw-HillEducation; 2009. Available from: http://amzn.com/0071635238.
[11] Mayer JD. The personality systems framework: Current theory and development. Journal of Research in Personality.2015 June;56:4–14.
[12] Tervalon M, Murray-Garcia J. Cultural humility versus cultural competence: A critical distinction in defining physi-cian training outcomes in multicultural education. J Health Care Poor Underserved. 1998 May;9(2):117–125.
[13] Mayer JD. Personal Intelligence: The Power of Personality and How It Shapes Our Lives. Scientific American / Farrar,Straus and Giroux; 2015. Available from: http://amzn.com/0374535019.
[14] Maccoby M, Norman CL, Norman CJ, Margolies R. Transforming Health Care Leadership. 1st ed. Jossey-Bass; 2013.Available from: http://amzn.com/1118505638.
[15] Maccoby M. Strategic Intelligence: Conceptual Tools for Leading Change. 1st ed. Oxford University Press; 2015.Available from: http://amzn.com/0199682380.
[16] Bernheim RG, Childress JF, Melnick A, Bonnie RJ. Essentials Of Public Health Ethics. 1st ed. Essential Public Health.Jones & Bartlett Learning; 2013. Available from: http://amzn.com/0763780464.