latest trends in hypertension treatment
TRANSCRIPT

Latest Trends in Hypertension Treatment.
Tilak Sirisena, Resident Cardiologist, Teaching Hospital, Kandy.

Proportions of CV Deaths in World (2011) Mendis, S., Puska, P. & Norrving, B. (Eds) Global Atlas on Cardiovascular Disease Prevention and Control. Geneva, World
Health Organization, 2011
Men Women

Hypertension and CV mortality


JNC 8 Guidelines (2014) Endorsed by American Academy of Family Physicians.
Copyright 2014 American Medical Association. All rights reserved.
2014 Evidence-Based Guideline for the Managementof High Blood Pressure in AdultsReport From the Panel Members Appointedto the Eighth Joint National Committee (JNC 8)Paul A. James, MD; Suzanne Oparil, MD; Barry L. Carter, PharmD; William C. Cushman, MD;Cheryl Dennison-Himmelfarb, RN, ANP, PhD; Joel Handler, MD; Daniel T. Lackland, DrPH;Michael L. LeFevre, MD, MSPH; Thomas D. MacKenzie, MD, MSPH; Olugbenga Ogedegbe, MD, MPH, MS;Sidney C. Smith Jr, MD; Laura P. Svetkey, MD, MHS; Sandra J. Taler, MD; Raymond R. Townsend, MD;Jackson T. Wright Jr, MD, PhD; Andrew S. Narva, MD; Eduardo Ortiz, MD, MPH
Hypertension is the most common condition seen in primary care and leads to myocardialinfarction, stroke, renal failure, and death if not detected early and treated appropriately.Patients want to be assured that blood pressure (BP) treatment will reduce their diseaseburden, while clinicians want guidance on hypertension management using the best scientificevidence. This report takes a rigorous, evidence-based approach to recommend treatmentthresholds, goals, and medications in the management of hypertension in adults. Evidencewas drawn from randomized controlled trials, which represent the gold standard fordetermining efficacy and effectiveness. Evidence quality and recommendations were gradedbased on their effect on important outcomes.
There is strong evidence to support treating hypertensive persons aged 60 years or older to aBP goal of less than 150/90 mm Hg and hypertensive persons 30 through 59 years of age to adiastolic goal of less than 90 mm Hg; however, there is insufficient evidence in hypertensivepersons younger than 60 years for a systolic goal, or in those younger than 30 years for adiastolic goal, so the panel recommends a BP of less than 140/90 mm Hg for those groupsbased on expert opinion. The same thresholds and goals are recommended for hypertensiveadults with diabetes or nondiabetic chronic kidney disease (CKD) as for the generalhypertensive population younger than 60 years. There is moderate evidence to supportinitiating drug treatment with an angiotensin-converting enzyme inhibitor, angiotensinreceptor blocker, calcium channel blocker, or thiazide-type diuretic in the nonblackhypertensive population, including those with diabetes. In the black hypertensive population,including those with diabetes, a calcium channel blocker or thiazide-type diuretic isrecommended as initial therapy. There is moderate evidence to support initial or add-onantihypertensive therapy with an angiotensin-converting enzyme inhibitor or angiotensinreceptor blocker in persons with CKD to improve kidney outcomes.
Although this guideline provides evidence-based recommendations for the management ofhigh BP and should meet the clinical needs of most patients, these recommendations are nota substitute for clinical judgment, and decisions about care must carefully consider andincorporate the clinical characteristics and circumstances of each individual patient.
JAMA. 2014;311(5):507-520. doi:10.1001/jama.2013.284427Published online December 18, 2013.
Editorial pages 472, 474, and477
Author Audio Interview atjama.com
Supplemental content atjama.com
CME Quiz atjamanetworkcme.com andCME Questions page 522
Author Affiliations: Authoraffiliations are listed at the end of thisarticle.
Corresponding Author: Paul A.James, MD, University of Iowa, 200Hawkins Dr, 01286-D PFP, Iowa City,IA 52242-1097 ([email protected]).
Clinical Review & Education
Special Communication
507
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jamanetwork.com/ on 10/22/2016

JNC 8 Guidelines.
Blood Pressure medications
Level at which treatment should be
started.Goal of BP
Too low Blood Pressure
Good or Bad ?

Level and Goal
General Population aged 60 years or older.
SBP 150 mmHg
DBP 90 mmHg
Strong Recommendation - Grade A.

Level and Goal.
General Population aged 60 years or older.
If pharmacolgic treatment results in SBP < 140 mmHg,
and treatment is not associated with adverse
effects, treatment does not need to be adjusted.
Expert Opinion - Grade E.

Level and Goal.
General Population aged < 60 years.
SBP* 140 mmHg DBP** 90 mmHg
**For ages 30-59 :Strong Recommendation -Grade A.*/**For ages 18-29 : Expert opinion - Grade E.

Level and Goal.
Population aged > 18 years.
CKD Diabetes Mellitus
SBP 140 mmHg DBP 90 mmHg
Expert opinion - Grade E.

Initial antihypertensive treatment
Non black Population including patients with Diabetes Mellitus
Thiazide type diuretic CCB ACEI ARB
Moderate Recommendation- Grade B.

Initial antihypertensive treatment
Black Population including patients with
Diabetes Mellitus**Thiazide type diuretic
CCB
Moderate Recommendation- Grade B.**Weak Recommendation - Grade C.

Initial or add on antihypertensive treatment
Population > 18 years with
CKD
ACEI ARB
to improve renal outcomes
Moderate Recommendation- Grade B.

Achieve and maintain Goal BP
If Goal is not achieved within a month
Increase the dose of initial drug
Add second or third drug from the recommended list
Do not combine ACEI with ARBS
Referral to Specialist if BP goal is not achieved with 3 drugs.
Add additional medication class (BB, Spironolactone etc)
Expert opinion - Grade E.

Drug Doses Based on RCTs
Copyright 2014 American Medical Association. All rights reserved.
The following important points should be noted. First, manypeople will require treatment with more than one antihyperten-sive drug to achieve BP control. While this recommendation ap-plies only to the choice of the initial antihypertensive drug, the panelsuggests that any of these 4 classes would be good choices as add-onagents (recommendation 9). Second, this recommendation is spe-cific for thiazide-type diuretics, which include thiazide diuretics,chlorthalidone, and indapamide; it does not include loop or potas-sium-sparing diuretics. Third, it is important that medications bedosed adequately to achieve results similar to those seen in the RCTs(Table 4). Fourth, RCTs that were limited to specific nonhyperten-sive populations, such as those with coronary artery disease or heartfailure, were not reviewed for this recommendation. Therefore, rec-ommendation 6 should be applied with caution to these popula-tions. Recommendations for those with CKD are addressed in rec-ommendation 8.
Recommendation 7In the general black population, including those with diabetes, ini-tial antihypertensive treatment should include a thiazide-type di-uretic or CCB.For general black population: Moderate Recommendation – Grade BFor black patients with diabetes: Weak Recommendation – Grade C
Recommendation 7 is based on evidence statements from ques-tion 3. In cases for which evidence for the black population was thesame as for the general population, the evidence statements for thegeneral population apply to the black population. However, thereare some cases for which the results for black persons were differ-ent from the results for the general population (question 3, evi-dence statements 2, 10, and 17). In those cases, separate evidencestatements were developed.
This recommendation stems from a prespecified subgroupanalysis of data from a single large trial (ALLHAT) that was ratedgood.31 In that study, a thiazide-type diuretic was shown to bemore effective in improving cerebrovascular, heart failure, andcombined cardiovascular outcomes compared to an ACEI in theblack patient subgroup, which included large numbers of diabeticand nondiabetic participants (question 3, evidence statements 10,15 and 17). Therefore, the recommendation is to choose thiazide-type diuretics over ACEI for black patients. Although a CCB wasless effective than a diuretic in preventing heart failure in the blacksubgroup of this trial (question 3, evidence statement 14), therewere no differences in other outcomes (cerebrovascular, CHD,combined cardiovascular, and kidney outcomes, or overall mortal-ity) between a CCB and a diuretic (question 3, evidence state-ments 6, 8, 11, 18, and 19). Therefore, both thiazide-type diureticsand CCBs are recommended as first-line therapy for hypertensionin black patients.
The panel recommended a CCB over an ACEI as first-linetherapy in black patients because there was a 51% higher rate(relative risk, 1.51; 95% CI, 1.22-1.86) of stroke in black persons inALLHAT with the use of an ACEI as initial therapy compared withuse of a CCB (question 3, evidence statement 2).32 The ACEI wasalso less effective in reducing BP in black individuals comparedwith the CCB (question 3, evidence statement 2).32 There were nooutcome studies meeting our eligibility criteria that compareddiuretics or CCBs vs β-blockers, ARBs, or other renin-angiotensinsystem inhibitors in black patients.
The recommendation for black patients with diabetes is weakerthan the recommendation for the general black population be-cause outcomes for the comparison between initial use of a CCB com-pared to initial use of an ACEI in black persons with diabetes werenot reported in any of the studies eligible for our evidence review.
Table 4. Evidence-Based Dosing for Antihypertensive Drugs
Antihypertensive Medication Initial Daily Dose, mgTarget Dose
in RCTs Reviewed, mg No. of Doses per DayACE inhibitors
Captopril 50 150-200 2Enalapril 5 20 1-2Lisinopril 10 40 1
Angiotensin receptor blockersEprosartan 400 600-800 1-2Candesartan 4 12-32 1Losartan 50 100 1-2Valsartan 40-80 160-320 1Irbesartan 75 300 1
β-BlockersAtenolol 25-50 100 1Metoprolol 50 100-200 1-2
Calcium channel blockersAmlodipine 2.5 10 1Diltiazem extended release 120-180 360 1Nitrendipine 10 20 1-2
Thiazide-type diureticsBendroflumethiazide 5 10 1Chlorthalidone 12.5 12.5-25 1Hydrochlorothiazide 12.5-25 25-100a 1-2Indapamide 1.25 1.25-2.5 1
Abbreviations: ACE,angiotensin-converting enzyme; RCT,randomized controlled trial.aCurrent recommendedevidence-based dose that balancesefficacy and safety is 25-50 mg daily.
Clinical Review & Education Special Communication 2014 Guideline for Management of High Blood Pressure
514 JAMA February 5, 2014 Volume 311, Number 5 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jamanetwork.com/ on 10/22/2016

Strategies to Dose Antihypertensive drugs
Strategy A
Start one drug, titrate to maximum dose and then add
second drug.
Strategy B
Start one drug and then add a second drug before
achieving maximum dose of second drug.
Strategy C
Begin with 2 drugs at the same time. either as 2
separate pills or as a single pill combination

Why is the change?
JNC 8 Restricted to RCT evidence
No RCT evidence that further lowering of BP provides additional benefit.

Comparison of Guidelines.
Copyright 2014 American Medical Association. All rights reserved.
line was not endorsed by any federal agency or professional societyprior to publication and thus is a departure from previous JNC reports.The panel anticipates that an objective assessment of this report fol-lowing publication will allow open dialogue among endorsing enti-ties and encourage continued attention to rigorous methods in guide-line development, thus raising the standard for future guidelines.
DiscussionThe recommendations based on RCT evidence in this guideline dif-fer from recommendations in other currently used guidelines sup-ported by expert consensus (Table 6). For example, JNC 7 and otherguidelines recommended treatment to lower BP goals in patients withdiabetes and CKD based on observational studies.12 Recently, sev-eral guideline documents such as those from the American DiabetesAssociation have raised the systolic BP goals to values that are simi-lar to those recommended in this evidence-based guideline.37-42 Otherguidelines such as those of the European Society of Hypertension/European Society of Cardiology also recommend a systolic BP goal oflower than 150 mm Hg, but it is not clear at what age cutoff in the gen-eral population this goal specifically applies.37 This changing land-scape is understandable given the lack of clear RCT evidence in manyclinical situations.
History of JNC 8The panel was originally constituted as the “Eighth Joint NationalCommittee on the Prevention, Detection, Evaluation, and Treat-ment of High Blood Pressure (JNC 8).” In March 2008 NHLBI sentletters inviting the co-chairs and committee members to serve on
JNC 8. The charge to the committee was as follows: “The JNC 8 willreview and synthesize the latest available scientific evidence, up-date existing clinical recommendations, and provide guidance to busyprimary care clinicians on the best approaches to manage and con-trol hypertension in order to minimize patients’ risk for cardiovas-cular and other complications.” The committee was also asked toidentify and prioritize the most important questions for the evi-dence review. In June 2013, NHLBI announced its decision to dis-continue developing clinical guidelines including those in process,instead partnering with selected organizations that would developthe guidelines.43,44 Importantly, participation in this process re-quired that these organizations be involved in producing the finalcontent of the report. The panel elected to pursue publication in-dependently to bring the recommendations to the public in a timelymanner while maintaining the integrity of the predefined process.This report is therefore not an NHLBI sanctioned report and doesnot reflect the views of NHLBI.
ConclusionsIt is important to note that this evidence-based guideline has not re-defined high BP, and the panel believes that the 140/90 mm Hg defi-nition from JNC 7 remains reasonable. The relationship betweennaturally occurring BP and risk is linear down to very low BP, but thebenefit of treating to these lower levels with antihypertensive drugsis not established. For all persons with hypertension, the potentialbenefits of a healthy diet, weight control, and regular exercise can-not be overemphasized. These lifestyle treatments have the poten-tial to improve BP control and even reduce medication needs. Al-
Table 6. Guideline Comparisons of Goal BP and Initial Drug Therapy for Adults With Hypertension
Guideline PopulationGoal BP,mm Hg Initial Drug Treatment Options
2014 Hypertensionguideline
General ≥60 y <150/90Nonblack: thiazide-type diuretic, ACEI,ARB, or CCB; black: thiazide-type diureticor CCB
General <60 y <140/90
Diabetes <140/90
CKD <140/90 ACEI or ARB
ESH/ESC 201337 General nonelderly <140/90
Diuretic, β-blocker, CCB, ACEI, or ARBGeneral elderly <80 y <150/90
General ≥80 y <150/90
Diabetes <140/85 ACEI or ARB
CKD no proteinuria <140/90ACEI or ARB
CKD + proteinuria <130/90
CHEP 201338 General <80 y <140/90 Thiazide, β-blocker (age <60y), ACEI(nonblack), or ARBGeneral ≥80 y <150/90
Diabetes <130/80 ACEI or ARB with additional CVD riskACEI, ARB, thiazide, or DHPCCB withoutadditional CVD risk
CKD <140/90 ACEI or ARB
ADA 201339 Diabetes <140/80 ACEI or ARB
KDIGO 201240 CKD no proteinuria ≤140/90ACEI or ARB
CKD + proteinuria ≤130/80
NICE 201141 General <80 y <140/90 <55 y: ACEI or ARB
General ≥80 y <150/90 ≥55 y or black: CCB
ISHIB 201042 Black, lower risk <135/85Diuretic or CCBTarget organ damage
or CVD risk<130/80
Abbreviations: ADA, AmericanDiabetes Association; ACEI,angiotensin-converting enzymeinhibitor; ARB, angiotensin receptorblocker; CCB, calcium channelblocker; CHEP, CanadianHypertension Education Program;CKD, chronic kidney disease; CVD,cardiovascular disease; DHPCCB,dihydropyridine calcium channelblocker; ESC, European Society ofCardiology; ESH, European Society ofHypertension; ISHIB, InternationalSociety for Hypertension in Blacks;JNC, Joint National Committee;KDIGO, Kidney Disease: ImprovingGlobal Outcome; NICE, NationalInstitute for Health and ClinicalExcellence.
Clinical Review & Education Special Communication 2014 Guideline for Management of High Blood Pressure
518 JAMA February 5, 2014 Volume 311, Number 5 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jamanetwork.com/ on 10/22/2016

Is Lower better? SPRINT Trial (2015)
The new england journal of medicine
n engl j med 373;22 nejm.org November 26, 2015 2103
established in 1812 November 26, 2015 vol. 373 no. 22
The members of the writing committee (Jackson T. Wright, Jr., M.D., Ph.D., Jeff D. Williamson, M.D., M.H.S., Paul K. Whelton, M.D., Joni K. Snyder, R.N., B.S.N., M.A., Kaycee M. Sink, M.D., M.A.S., Michael V. Rocco, M.D., M.S.C.E., David M. Reboussin, Ph.D., Mahboob Rahman, M.D., Suzanne Oparil, M.D., Cora E. Lewis, M.D., M.S.P.H., Paul L. Kimmel, M.D., Karen C. Johnson, M.D., M.P.H., David C. Goff, Jr., M.D., Ph.D., Lawrence J. Fine, M.D., Dr.P.H., Jeffrey A. Cutler, M.D., M.P.H., William C. Cush-man, M.D., Alfred K. Cheung, M.D., and Walter T. Ambrosius, Ph.D.) assume re-sponsibility for the overall content and integrity of the article. The affiliations of the members of the writing group are listed in the Appendix. Address reprint requests to Dr. Wright at the Division of Nephrology and Hypertension, Univer-sity Hospitals Case Medical Center, Case Western Reserve University, 1100 Euclid Ave. Cleveland, OH 44106-6053, or at jackson . wright@ case . edu.
* A complete list of the members of the Systolic Blood Pressure Intervention Trial (SPRINT) Research Group is pro-vided in the Supplementary Appendix, available at NEJM.org.
This article was published on November 9, 2015, at NEJM.org.
N Engl J Med 2015;373:2103-16.DOI: 10.1056/NEJMoa1511939Copyright © 2015 Massachusetts Medical Society.
BACKGROUNDThe most appropriate targets for systolic blood pressure to reduce cardiovascular morbidity and mortality among persons without diabetes remain uncertain.
METHODSWe randomly assigned 9361 persons with a systolic blood pressure of 130 mm Hg or higher and an increased cardiovascular risk, but without diabetes, to a systolic blood-pressure target of less than 120 mm Hg (intensive treatment) or a target of less than 140 mm Hg (standard treatment). The primary composite outcome was myocardial infarction, other acute coronary syndromes, stroke, heart failure, or death from cardiovascular causes.
RESULTSAt 1 year, the mean systolic blood pressure was 121.4 mm Hg in the intensive-treatment group and 136.2 mm Hg in the standard-treatment group. The interven-tion was stopped early after a median follow-up of 3.26 years owing to a signifi-cantly lower rate of the primary composite outcome in the intensive-treatment group than in the standard-treatment group (1.65% per year vs. 2.19% per year; hazard ratio with intensive treatment, 0.75; 95% confidence interval [CI], 0.64 to 0.89; P<0.001). All-cause mortality was also significantly lower in the intensive-treatment group (hazard ratio, 0.73; 95% CI, 0.60 to 0.90; P = 0.003). Rates of seri-ous adverse events of hypotension, syncope, electrolyte abnormalities, and acute kidney injury or failure, but not of injurious falls, were higher in the intensive-treatment group than in the standard-treatment group.
CONCLUSIONSAmong patients at high risk for cardiovascular events but without diabetes, target-ing a systolic blood pressure of less than 120 mm Hg, as compared with less than 140 mm Hg, resulted in lower rates of fatal and nonfatal major cardiovascular events and death from any cause, although significantly higher rates of some adverse events were observed in the intensive-treatment group. (Funded by the National Institutes of Health; ClinicalTrials.gov number, NCT01206062.)
a bs tr ac t
A Randomized Trial of Intensive versus Standard Blood-Pressure Control
The SPRINT Research Group*
The New England Journal of Medicine Downloaded from nejm.org on October 22, 2016. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.

Is Lower Better? Yes

Hope 3 Trial (May 2016)
The new england journal of medicine
n engl j med 374;21 nejm.org May 26, 2016 2009
established in 1812 May 26, 2016 vol. 374 no. 21
The authors’ affiliations are listed in the Appendix. Address reprint requests to Dr. Lonn at the Population Health Research Institute and Hamilton Health Sciences, 237 Barton St. E., Hamilton ON L8L 2X2, Canada, or at eva . lonn@ phri . ca.
* Deceased.
†A complete list of the Heart Outcomes Prevention Evaluation (HOPE)–3 trial investigators is provided in the Supple-mentary Appendix, available at NEJM.org.
This article was published on April 2, 2016, at NEJM.org.
N Engl J Med 2016;374:2009-20.DOI: 10.1056/NEJMoa1600175Copyright © 2016 Massachusetts Medical Society.
BACKGROUNDAntihypertensive therapy reduces the risk of cardiovascular events among high-risk persons and among those with a systolic blood pressure of 160 mm Hg or higher, but its role in persons at intermediate risk and with lower blood pressure is unclear.METHODSIn one comparison from a 2-by-2 factorial trial, we randomly assigned 12,705 par-ticipants at intermediate risk who did not have cardiovascular disease to receive either candesartan at a dose of 16 mg per day plus hydrochlorothiazide at a dose of 12.5 mg per day or placebo. The first coprimary outcome was the composite of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke; the second coprimary outcome additionally included resuscitated cardiac arrest, heart failure, and revascularization. The median follow-up was 5.6 years.RESULTSThe mean blood pressure of the participants at baseline was 138.1/81.9 mm Hg; the decrease in blood pressure was 6.0/3.0 mm Hg greater in the active-treatment group than in the placebo group. The first coprimary outcome occurred in 260 par-ticipants (4.1%) in the active-treatment group and in 279 (4.4%) in the placebo group (hazard ratio, 0.93; 95% confidence interval [CI], 0.79 to 1.10; P = 0.40); the second coprimary outcome occurred in 312 participants (4.9%) and 328 partici-pants (5.2%), respectively (hazard ratio, 0.95; 95% CI, 0.81 to 1.11; P = 0.51). In one of the three prespecified hypothesis-based subgroups, participants in the subgroup for the upper third of systolic blood pressure (>143.5 mm Hg) who were in the active-treatment group had significantly lower rates of the first and second copri-mary outcomes than those in the placebo group; effects were neutral in the middle and lower thirds (P = 0.02 and P = 0.009, respectively, for trend in the two outcomes).CONCLUSIONSTherapy with candesartan at a dose of 16 mg per day plus hydrochlorothiazide at a dose of 12.5 mg per day was not associated with a lower rate of major cardio-vascular events than placebo among persons at intermediate risk who did not have cardiovascular disease. (Funded by the Canadian Institutes of Health Research and AstraZeneca; ClinicalTrials.gov number, NCT00468923.)
a bs tr ac t
Blood-Pressure Lowering in Intermediate-Risk Persons without Cardiovascular Disease
Eva M. Lonn, M.D., Jackie Bosch, Ph.D., Patricio López-Jaramillo, M.D., Ph.D., Jun Zhu, M.D., Lisheng Liu, M.D., Prem Pais, M.D., Rafael Diaz, M.D., Denis Xavier, M.D., Karen Sliwa, M.D., Ph.D., Antonio Dans, M.D.,
Alvaro Avezum, M.D., Ph.D., Leopoldo S. Piegas, M.D., Ph.D., Katalin Keltai, M.D., Ph.D., Matyas Keltai, M.D., Ph.D., Irina Chazova, M.D., Ph.D., Ron J.G. Peters, M.D., Ph.D., Claes Held, M.D., Ph.D., Khalid Yusoff, M.D.,
Basil S. Lewis, M.D., Petr Jansky, M.D., Alexander Parkhomenko, M.D., Ph.D., Kamlesh Khunti, M.D., Ph.D., William D. Toff, M.D., Christopher M. Reid, Ph.D., John Varigos, B.Sc., Lawrence A. Leiter, M.D.,
Dora I. Molina, M.D., Robert McKelvie, M.D., Ph.D., Janice Pogue, Ph.D.,* Joanne Wilkinson, B.A., Hyejung Jung, M.Sc., Gilles Dagenais, M.D., and Salim Yusuf, M.B., B.S., D.Phil., for the HOPE-3 Investigators†
The New England Journal of Medicine Downloaded from nejm.org on October 22, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
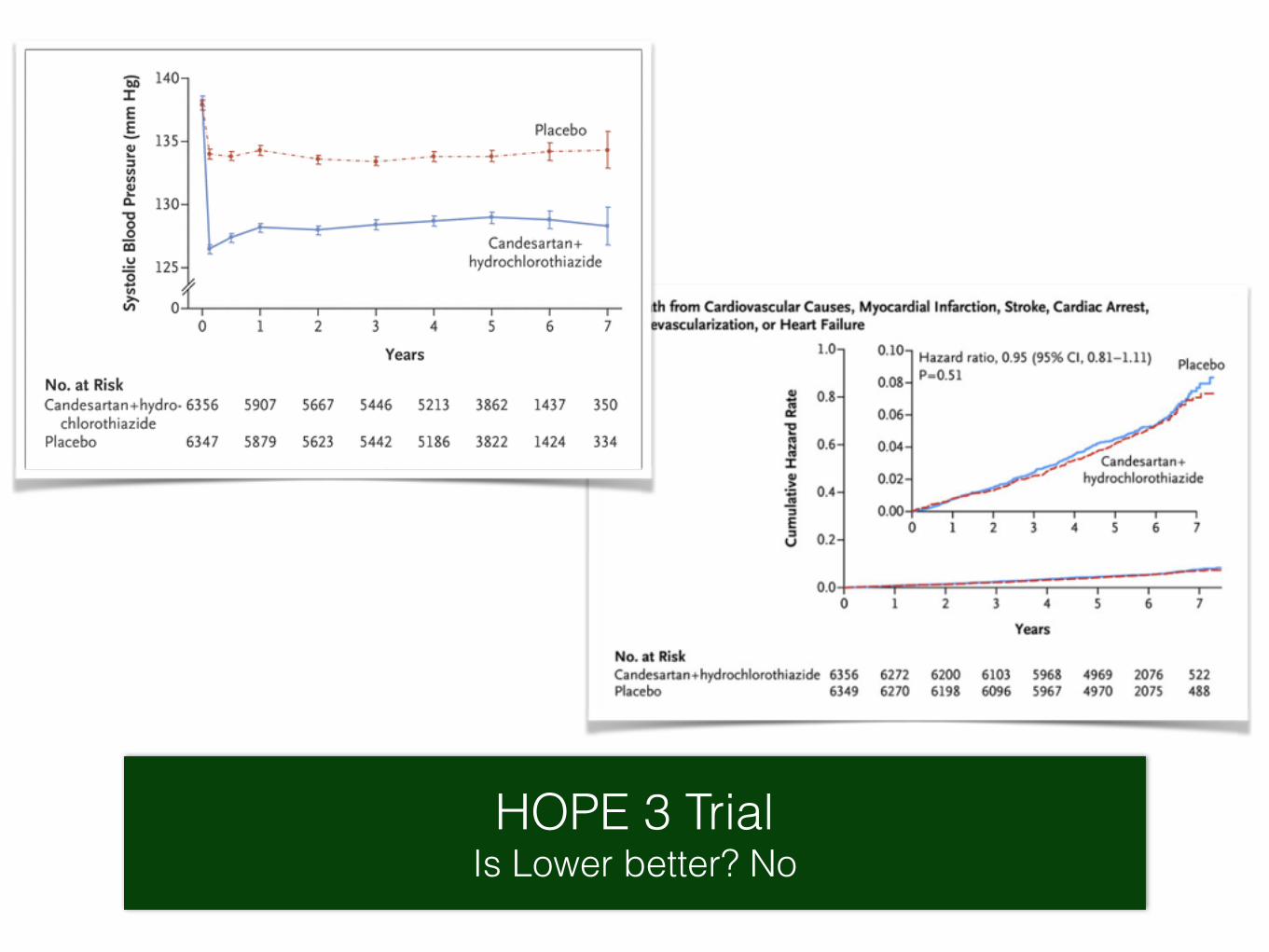
HOPE 3 Trial Is Lower better? No
Different methodology used in two trials.
• In the HOPE-3 trial, conventional blood-pressure measurements at an office visit were used, whereas unattended, automated, office blood-pressure measurements were used in SPRINT.3

Too low Diastolic BP Sub group analysis from ARIC cohort
JACC October 2016
1 1.52.2
Incident CHD and Mortality
DBP 80-89 mmHg DBP 60-69 mmHg DBP < 60 mmHg
Likelihood of having hs Troponin > 14 ng/mL

Will this new data change present Guidelines?
?

Life style

Thank You.
Remember BP Levels and Goals 150/90 mmHg for > 60 Years
140/90 mmHg for < 60 years and patients with CKD and Diabetes
Four main classes of drugs Thiazides. CCB, ACEI and ARB Too low may not be too good