large-scale urban disaster drill involving an explosion: lessons learned by an academic medical...
TRANSCRIPT
Lessons Learned
Large-Scale Urban Disaster Drill Involving an Explosion:Lessons Learned by an Academic Medical CenterBrian Sweeney, RN, BSN, MBA, CEN, CFRN, PHRN, CHE, Edward Jasper, MD,and Eleanor Gates, RN, MSN
DMR
Coordinating a successful large-scale hospitaldisaster drill with hundreds of victims requiresextensive planning. The drill must be orga-
nized well to test effectively disaster preparedness andto ensure participants gain the maximum educationalvalue from the exercise.
The lessons learned from this disaster drill areclassified into 6 categories: (1) time management,(2) venue, (3) victim expectations, (4) responder ex-pectations, (5) realistic experience, and (6) recordkeeping/evaluations. Health care organizations thatintend to host disaster drills in the future can learnfrom these experiences and incorporate these lessonslearned into the planning process.
Hospitals and health care organizations are mandat-ed to prepare for mass casualty events and disasters. It isnot uncommon for a hospital to spend countless hoursassessing risk, reviewing emergency managementplans, assessing resources, and training personnel.The investment of resources can be significant anddisaster response planners want to be able to benefitfrom the costs. The purpose of this manuscript is to
Brian Sweeney, RN, BSN, MBA, CEN, CFRN, PHRN, CHE,is Director of JeffSTAT, Patient Transportation, and theEMS Training Center, Coordinator of the disaster drillinitiatives, and Member of the Center for Bioterrorismand Disaster Preparedness at Thomas Jefferson UniversityHospital.
Edward Jasper, MD, is Director of the Center for Bioterrorismand Disaster Preparedness, Attending Physician at theEmergency Department, Medical Director for JeffSTAT, andEMS Director at Thomas Jefferson University Hospital;Clinical Assistant Professor at Thomas Jefferson University;and Faculty at Jefferson Medical College.
Eleanor Gates, RN, MSN, is Vice President of Neuro, Surgery,and Trauma, Co-chairperson of the EmergencyManagement Committee, and overseer of the Center forBioterrorism and Disaster Preparedness atThomas Jefferson University Hospital.
Reprint requests: Brian Sweeney, RN, BSN, MBA, CEN,CFRN, PHRN, CHE, 1020 Sansom St, Suite F-1503,Philadelphia, PA 19107.
Disaster Manage Response 2004;2:87-90.
Copyright � 2004 by the Emergency Nurses Association.
1540-2487/$30.00
doi:10.1016/j.dmr.2004.06.010
July-September 2004
describe the lessons learned from a large-scale drillconducted in a major urban area. See Table 1 for onlineresources that can be used for disaster drills.
Premise of Drill
A regional disaster drill was conducted in May of2003 to test the effectiveness of planned interventionsand to evaluate the preparedness of an organizationand region. The disaster drill scenario involved a seriesof explosions in the city of Philadelphia. The initialmock explosion occurred in northeast Philadelphiaand involved hundreds of victims. The fire departmentwas dispatched and all of the available city emergencymedical services (EMS) units were dispatched to thescene. Approximately 30 minutes later, the policedepartment received multiple reports of an explo-sion occurring at a concert venue near Center CityPhiladelphia. The second explosion also involvedhundreds of injured concert attendees and appearedto be the result of a suicide bomber who drove hisvehicle into the side of the building. This required theresponse of mutual aid ambulance services in thesurrounding counties, because the fire departmentresources were already consumed. An odor similar tomustard was present immediately after the explosion,representing the dispersal of mustard gas.
Tomake the drill more realistic, 240 first yearmedicalstudents were included in the drill and used pre-dominantly as the victims. Medical students wereselected for specific reasons: the students would fulfilla need for a large number of victims, the drill experiencewould give them apatient’s perspective on a health careresponse to disaster, and the students would gainexperience with medical care in disaster situations foruse later in their career. To ensure 100% participation inthe disaster drill, the medical school curriculumcommittee required the students’ participation. Thedrill was incorporated into an introductory course inemergencymedicine and the students received a lectureon terrorism and disaster preparedness prior to the drill.
Lessons Learned
The lessons learned from this disaster drill are listedin Table 2 and are classified into 6 categories: (1) time
Disaster Management & Response/Sweeney et al 87
DMR
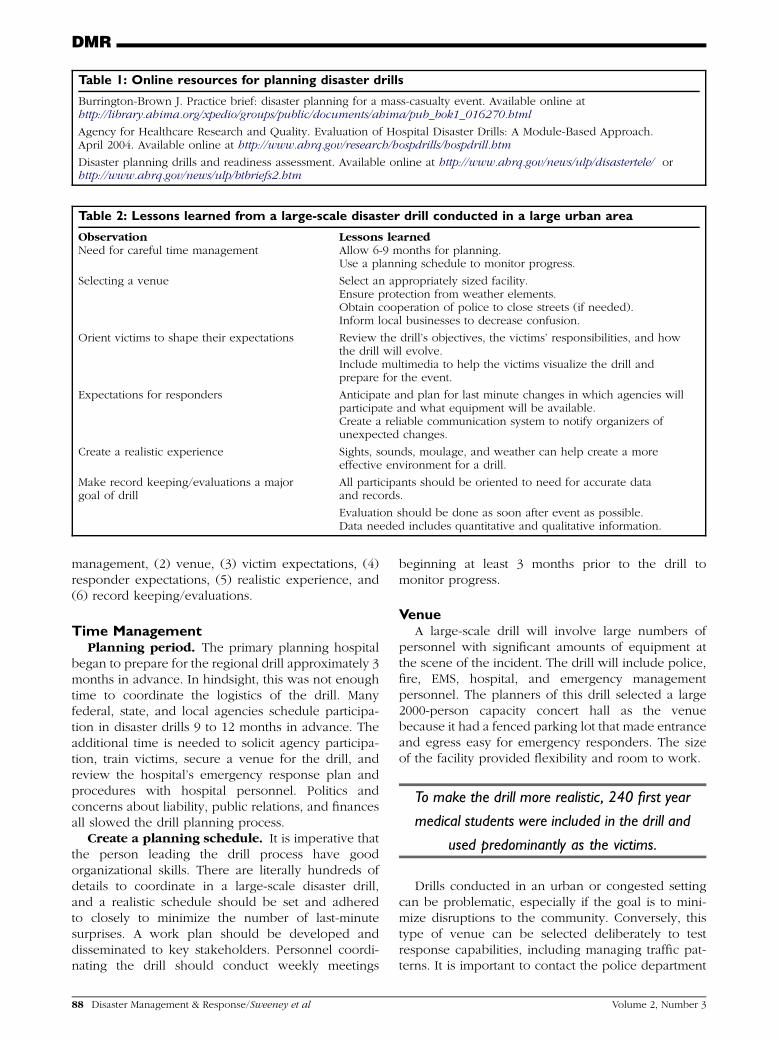
Table 2: Lessons learned from a large-scale disaster drill conducted in a large urban area
Observation Lessons learnedNeed for careful time management Allow 6-9 months for planning.
Use a planning schedule to monitor progress.
Selecting a venue Select an appropriately sized facility.Ensure protection from weather elements.Obtain cooperation of police to close streets (if needed).Inform local businesses to decrease confusion.
Orient victims to shape their expectations Review the drill’s objectives, the victims’ responsibilities, and howthe drill will evolve.Include multimedia to help the victims visualize the drill andprepare for the event.
Expectations for responders Anticipate and plan for last minute changes in which agencies willparticipate and what equipment will be available.Create a reliable communication system to notify organizers ofunexpected changes.
Create a realistic experience Sights, sounds, moulage, and weather can help create a moreeffective environment for a drill.
Make record keeping/evaluations a majorgoal of drill
All participants should be oriented to need for accurate dataand records.
Evaluation should be done as soon after event as possible.Data needed includes quantitative and qualitative information.
Table 1: Online resources for planning disaster drills
Burrington-Brown J. Practice brief: disaster planning for a mass-casualty event. Available online athttp://library.ahima.org/xpedio/groups/public/documents/ahima/pub_bok1_016270.html
Agency for Healthcare Research and Quality. Evaluation of Hospital Disaster Drills: A Module-Based Approach.April 2004. Available online at http://www.ahrq.gov/research/hospdrills/hospdrill.htm
Disaster planning drills and readiness assessment. Available online at http://www.ahrq.gov/news/ulp/disastertele/ orhttp://www.ahrq.gov/news/ulp/btbriefs2.htm
management, (2) venue, (3) victim expectations, (4)responder expectations, (5) realistic experience, and(6) record keeping/evaluations.
Time ManagementPlanning period. The primary planning hospital
began to prepare for the regional drill approximately 3months in advance. In hindsight, this was not enoughtime to coordinate the logistics of the drill. Manyfederal, state, and local agencies schedule participa-tion in disaster drills 9 to 12 months in advance. Theadditional time is needed to solicit agency participa-tion, train victims, secure a venue for the drill, andreview the hospital’s emergency response plan andprocedures with hospital personnel. Politics andconcerns about liability, public relations, and financesall slowed the drill planning process.
Create a planning schedule. It is imperative thatthe person leading the drill process have goodorganizational skills. There are literally hundreds ofdetails to coordinate in a large-scale disaster drill,and a realistic schedule should be set and adheredto closely to minimize the number of last-minutesurprises. A work plan should be developed anddisseminated to key stakeholders. Personnel coordi-nating the drill should conduct weekly meetings
88 Disaster Management & Response/Sweeney et al
beginning at least 3 months prior to the drill tomonitor progress.
VenueA large-scale drill will involve large numbers of
personnel with significant amounts of equipment atthe scene of the incident. The drill will include police,fire, EMS, hospital, and emergency managementpersonnel. The planners of this drill selected a large2000-person capacity concert hall as the venuebecause it had a fenced parking lot that made entranceand egress easy for emergency responders. The sizeof the facility provided flexibility and room to work.
To make the drill more realistic, 240 first year
medical students were included in the drill and
used predominantly as the victims.
Drills conducted in an urban or congested settingcan be problematic, especially if the goal is to mini-mize disruptions to the community. Conversely, thistype of venue can be selected deliberately to testresponse capabilities, including managing traffic pat-terns. It is important to contact the police department
Volume 2, Number 3

DMR
to request road closures or traffic alterations at least6 to 9 months in advance, because the approvalprocess can be lengthy. It is also important to remindthe police of the drill a few weeks in advance and tonotify all local business of the event to avoidunnecessary panic.
Drills conducted in an urban or congested
setting can be problematic, especially if the
goal is to minimize disruptions to the
community.
Unless the drill is intended to test weather-relatedresponses, it is recommended that a venue be selectedthat will protect the participants from rain, wind,and sun. An uncomfortable environment will distractthe victims and the rescuers from the task at hand.Unfortunately, on the day of drill (late spring), con-ditions were cool and damp. The victims complainedrepeatedly of being cold and gradually lost focus onacting and on accurately presenting the signs andsymptoms given to them. As the drill progressed, drillorganizers found that some victims actually changedtheir presenting signs and symptoms and increasedtheir triage tag priority so they would be transportedto the warmth of the hospital sooner. This simplefactor interfered with the ability to test the capabilitiesof various hospitals to handle predetermined numbersof emergent, urgent, and nonurgent victims. Thisalso taught organizers that real victims are able tochange their tags to prioritize treatment and that tagswhich cannot be easily altered should be used in thefuture.
Victims’ ExpectationsMock victims are one of the most important
components of the drill, because they will influencehow realistic and effective the drill will be. The drillcan be significantly influenced by the victims if theydeviate either from the scripted signs and symptomsor from the schedule. Many victims, having neverparticipated in a disaster drill before, will not knowwhat to expect. Some of the victims in this drillbecame agitated while waiting for transportation tothe hospital, especially if their wait time was greaterthan 1 hour. These victims did not understand thatthey were transported last because they requirednonurgent medical care. This misunderstandingcould have been avoided had a more detailedorientation been provided to the victims in advanceof the drill.
In the future, more time will be spent with thevictims to review information such as the drill’sobjectives, the victims’ responsibilities, and a step-
July-September 2004
by-step review of how the drill will evolve. Detailedphotographs, video, and other forms of multimediawill be used to help the victims visualize the drill andprepare for the event.
It is also important that the victims have a genuinewillingness and interest to participate in the drill. Thedrill was held on a weekend. The medical students inthe drill were required to participate and were testedon the experience. These factors were assumed tocontribute to the students’ performance as victims.
Responders’ ExpectationDisasters are chaotic by nature and the drill process
proved to be no different. No matter how muchplanning or training was completed, deviations fromthe script were unavoidable and last-minute planningadjustments had to be made. Several days before thedisaster drill, the police department notified theplanners that a 5-kilometer race was scheduled topass by the selected venue. Planners checked thetimes and were assured the runners would pass beforeaccess to the venue was needed; however, thisinformation was incorrect. While the victims andobservers were en route to the venue, it was learnedthat the road was still closed for the race. The policehad barricades in place and refused to allow thevictims, observers, and organizers to pass until the runwas over. This caused the drill to start 15 minutesbehind schedule.
Not all agencies and organizations in a large-scaledrill may be able to participate as planned. Organizersshould anticipate that some participants will need todrop out at the last minute, and others, even if theycall to confirm their attendance, still may notparticipate in the drill. Planners should schedule extraresources to compensate for last minute changes. It isalso important that participating hospitals have a pre-determined system to notify the drill coordinator ofthe need to withdraw participation if the emergencydepartment becomes inundated with real patients. Adedicated telephone number (ie, a drill hotline)should be distributed to all participants in advanceand used for the purpose of communicating criticalchanges.
Realistic ExperienceIt is important to make the drill as realistic as
possible because participants and victims are morelikely to act seriously when the drill mimics real-lifeevents. Realism will also make the drill a moreeffective test of readiness. Organizers spend hoursdeveloping victim instruction cards with signs andsymptoms for the medical students and even moretime placing gruesome moulage on the victims. At thescene, sound and visual effects were introduced. Thesound of an explosion and smoke from a smoke
Disaster Management & Response/Sweeney et al 89

DMR
machine were used to make the scene seem morerealistic for the initial rescuers.
Having realistic expectations also applies to theparticipants of the drill. It was part of the plan toensure that the resources a hospital has availableduring the drill would be similar to those availableduring a normal workday. For example, instead ofhaving 25 to 50 ambulances sitting in a parking lotnear the scene of the disaster just waiting for the drillto begin, participating ambulances were told torespond from their stations. The ambulances weretold not to use lights and sirens and to obey speedlimits to ensure safety. Unfortunately, this led to oneexperienced drill observer to comment that there werenot enough ambulances immediately on the scene andthe EMS response was not timely. In a real life event,ambulances would arrive from various locations andwould be staggered in their response time.
Not all agencies and organizations in a
large-scale drill may be able to participate
as planned.
Record Keeping/EvaluationsDisaster drills can provide a tremendous amount of
useful information if accurate data is collected. TheAgency for Healthcare Research and Quality (AHRQ)recommend that planners have a detailed evaluationplan in place before the drills begin. Comprehensiveevaluations of the drill using a Likert-scale question-
90 Disaster Management & Response/Sweeney et al
naire were completed by the medical students andobservers. Additional data included triage times,transport times, hospital arrival times, and time tosurgery. This helped to measure the effectiveness andefficiency of the EMS system and hospital operations.
The organizers learned not only how important, buthow difficult it is to keep good records. Some of thedifficulties encountered were collecting triage tags,evaluations, and transport logs, obtaining completeevaluation forms from the victims and observers, andvictims failing to follow the documentation instruc-tions.
It was learned that victims should be given a moredetailed orientation that includes the importance ofdocuments as a tool to evaluate the drill. The drillcoordinators should schedule critique sessions as soonas possible after the drill to ensure the experience isfresh in everyone’s minds. The data collected andlessons learned should be shared with all those whoparticipated to encourage improvement with futureresponses.
Summary
Disaster drills are an effective way to test a hospital’spreparedness for real-life disasters, but an extensiveamount of coordination and time is necessary to hosta successful drill with a large number of victims. Thelessons learned in this drill include a number ofplanning, education, orientation, and follow-up is-sues. It is not realistic to believe that a drill can beperfectly planned and practiced; therefore each drillprovides another opportunity to improve on pastexperience.
Volume 2, Number 3