large bowel obstructioncdn.cepdtoronto.ca.s3.amazonaws.com/generalsurgery/1045-burnstein.pdf ·...
TRANSCRIPT

M A R C U S B U R N S T E I N
LARGE BOWEL OBSTRUCTION
MCQ
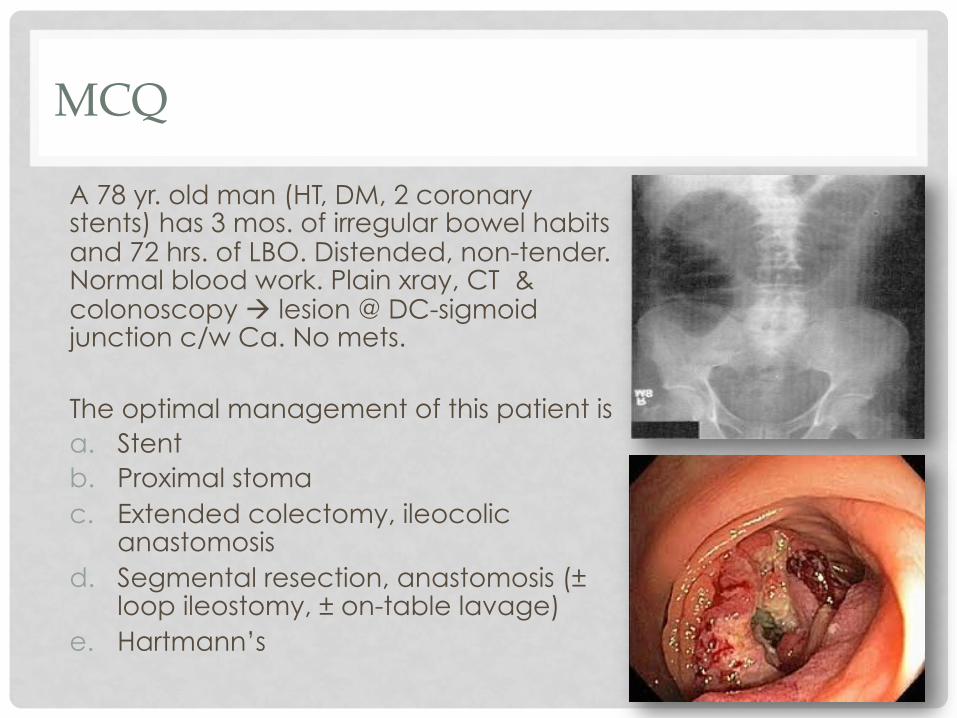
A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray, CT & colonoscopy à lesion @ DC-sigmoid junction c/w Ca. No mets. The optimal management of this patient is a. Stent b. Proximal stoma c. Extended colectomy, ileocolic
anastomosis d. Segmental resection, anastomosis (±
loop ileostomy, ± on-table lavage) e. Hartmann’s
1. MALIGNANT OBSTRUCTION: A practical approach
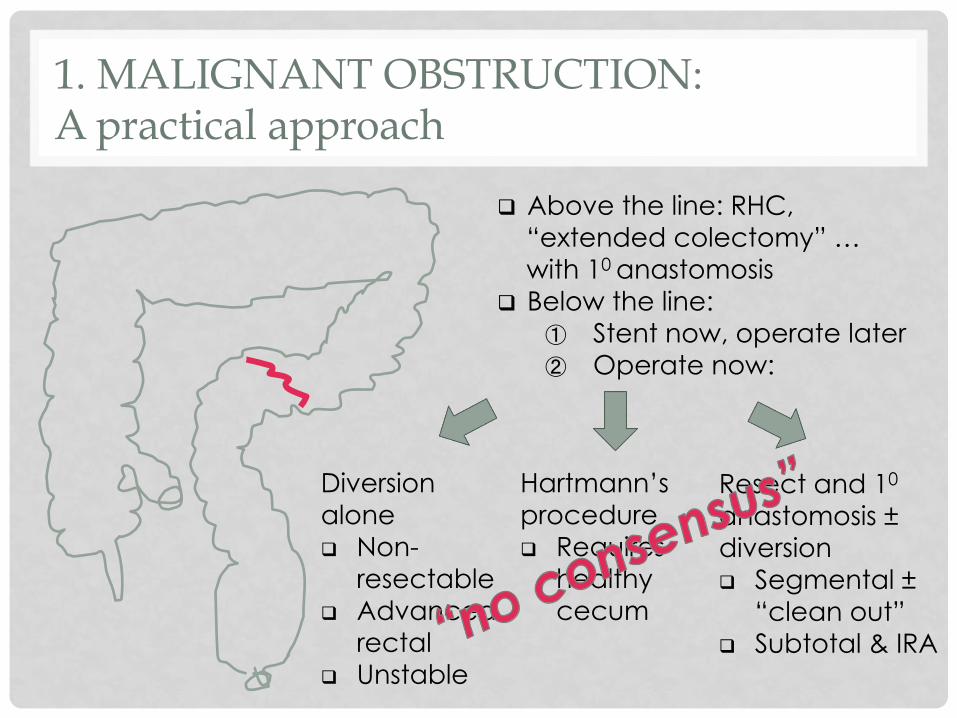
q Above the line: RHC, “extended colectomy” … with 10 anastomosis
q Below the line: ① Stent now, operate later ② Operate now:
Diversion alone q Non-
resectable q Advanced
rectal q Unstable
Hartmann’s procedure q Requires
healthy cecum
Resect and 10 anastomosis ± diversion q Segmental ±
“clean out” q Subtotal & IRA

STENT NOW, OPERATE LATER: A growing consensus?
In expert centres: q Ó10 anastomosis q Ô length of stay q Ô mortality q Ô complications q Cost-effective
In the real world:
Stent Operation p
Stoma 45% 62% 0.02
10 anastomosis 65% 55% 0.003
Complications 48% 55% ns
Mortality 8% 9% ns
Cirocchi R, et al. Surg Onc 2013;22:14-21
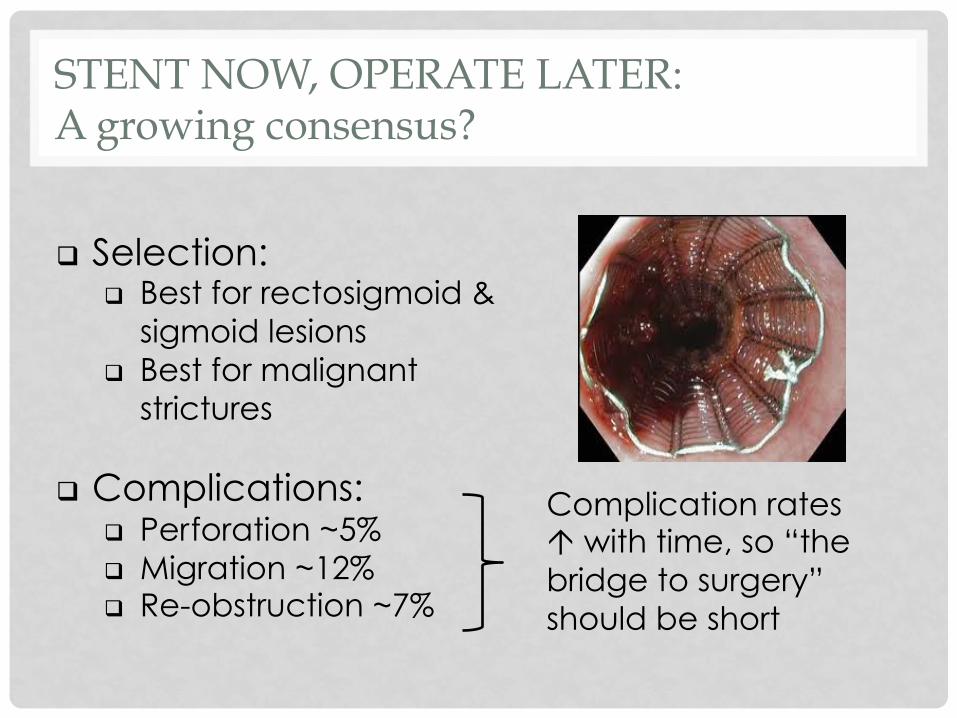
q Selection: q Best for rectosigmoid &
sigmoid lesions q Best for malignant
strictures
q Complications: q Perforation ~5% q Migration ~12% q Re-obstruction ~7%
Complication rates Ó with time, so “the bridge to surgery” should be short
STENT NOW, OPERATE LATER: A growing consensus?

OPERATIONS FOR THE DISTAL LESION (when stent fails)… how do we chose?
Operation + -
Hartmann’s q Safe, easy, quick q Unstable patient q No leaks! q No shame!
q Stoma; >30% not rev’d q Ó reversal morbidity
STC & IRA q Nice anastomosis q Removes the proximal
colon (synchronous lesions; ‘sick’ cecum)
q One stage, no stoma
q Not ’quick & easy’ q Functional disturbance
(ÓBMs, Ô continence) q Anastomotic leak q ± Protecting stoma
Segmental Resection
q Preserves colonic function
q One stage, no stoma
q ?Lavage or manual clean out
q ?Nice anastomosis q Anastomotic leak q ± Protecting stoma
q Weigh the risks and benefits of the various options in the context of: q Patient factors
q General health q ?more likely to get a leak q ?less able to survive a leak
q Bowel function, especially continence
q Disease factors q Degree of distention and fecal
loading q Integrity of cecum q Synchronous lesions q Cancer vs. benign stricture
Good clinical judgement
Careful patient selection
Individualize therapy
Surgeon experience

IN THE ABSENCE OF CONSENSUS… some ‘evidence’ to help us chose
q STC & IRA vs. Segmental Resection with on-table lavage q Mortality: no difference (~10%) q Anastomotic leak: no difference (~5%) q Wound infection: no difference (~15%) q Length of stay: no difference q Quality of life: better after segmental resection
q On-table colonic lavage vs. manual clean-out q No difference in mortality, leak, and wound infection
q Segmental Resection without lavage or manual clean-out q Comparable mortality and leak rates to Segmental Resection
with on-table lavage

SOME TRICKS TO HELP US…
① Deflate the distended colon with an angiocath ② Side to end to overcome luminal discrepancy ③ Don’t do on-table lavage (in general) ④ Scope after anastomosis to deflate, test (±
lavage) ⑤ Still a role for Hartmann’s !!
1.
2. 3. 4.

SIGMOID VOLVULUS
q Diagnosis… think of it q Elderly, institutionalized, medicated q In the rare younger patient, usually part
of colonic inertia ± megacolon q Treatment
q Ischemia/infarction à lap à Hartmann’s vs. 10 anastomosis
q Endoscopic decompression successful ~80%
q Colonoscopy (if no infarction à rectal tube)
q Prep à formal colonoscopy à resect q No resection à Rec Rate up to
70-80% q ?Timing

SIGMOID VOLVULUS
But these patients are old and frail… can we avoid a G.A. and resection?
q Endoscopic decompression prn
q Percutaneous endoscopic colostomy (PEC) tube
q Laparoscopic-assisted PEC tube(s)
q Sigmoidopexy q Sigmoid extra-
peritonealization q Mesosigmoidoplasty
No G.A.
PEC tube
No good
CECAL VOLVULUS
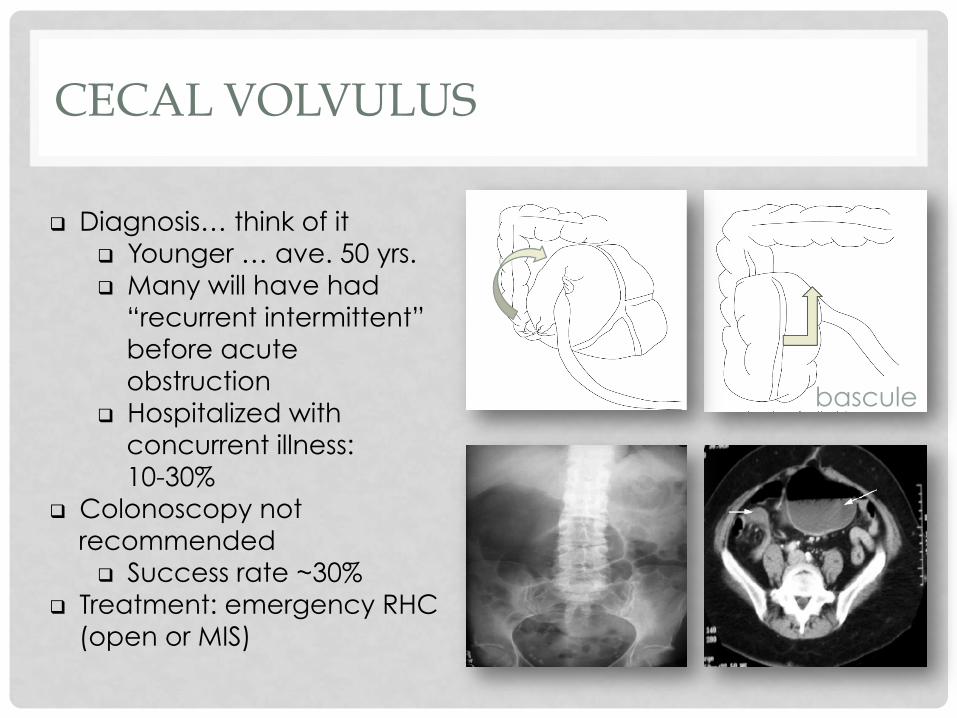
q Diagnosis… think of it q Younger … ave. 50 yrs. q Many will have had
“recurrent intermittent” before acute obstruction
q Hospitalized with concurrent illness: 10-30%
q Colonoscopy not recommended q Success rate ~30%
q Treatment: emergency RHC (open or MIS)
bascule
ACUTE COLONIC PSEUDO-OBSTRUCTION
q ~20 % of LBO are not mechanical
q Elderly, often hospitalized, with a wide spectrum of co-morbidities and medications q Affects 0.5-1% of patients
on ortho, neurosurg & burn units
q Mortality > 15% q cecal perforation

② IV neostigmine: q 1-2mg over 1-5 min q Monitor HR, BP, EKG q Rel CI’d: IHD, COPD,
asthma, β blockers, RF q Success ~80% (repeatable)
① Supportive care: q IV, NGT, RT q Correct lytes q Stop meds: narcs,
anti-chol, Ca++
blockers, laxatives
q Monitor cecum
ACUTE COLONIC PSEUDO-OBSTRUCTION: management algorithm
LBO
Acute CPO
Resolution No Resolution X 48 hrs
No Resolution
④ Tube cecostomy
Resection& stomas
Clinical or Radiologic perforation
CT or WSCE or colonoscopy
③ Colonoscopy q Success ~80% q Perforation ~2%

LARGE BOWEL OBSTRUCTION
• Mechanical obstruction • Proximal to the red line… extended colectomy
with ileocolic anastomosis • Distal to the red line… stent • If no stent expertise or stent failure • Transfer • Operate, but… no consensus on ‘best operation’, &
clinical acumen required
• Sigmoid volvulus… de-tort then discuss • Cecal volvulus… RHC
• Acute CPO… lethal condition