laparoscopic vs. open liver resection for malignant liver disease. a systematic review
TRANSCRIPT
t h e s u r g e on 1 0 ( 2 0 1 2 ) 1 9 4e2 0 1
avai lable at www.sciencedirect .com
The Surgeon, Journal of the Royal Collegesof Surgeons of Edinburgh and Ireland
www.thesurgeon.net
Laparoscopic vs. open liver resection for malignant liverdisease. A systematic review
Ahsan Rao*, Ghaus Rao a, Irfan Ahmed b
Department of Surgery, Ward 31, Foresterhill, Aberdeen Royal Infirmary, Aberdeen AB25 2ZA, United Kingdom
a r t i c l e i n f o
Article history:
Received 13 May 2011
Accepted 28 June 2011
Available online 15 September 2011
Keywords:
Laparoscopic
Open liver resection
Hepatocellular carcinoma
Hepatic malignancy
Meta-analysis
* Corresponding author. Tel.: þ44 (0) 1224 32E-mail addresses: [email protected], a.
(I. Ahmed).a Tel.: þ44 (0) 1224 323224.b Tel.: þ44 (0) 1224 555056, Secretary: þ44 (
1479-666X/$ e see front matter Crown CopyrRoyal College of Surgeons in Ireland. Publishdoi:10.1016/j.surge.2011.06.007
a b s t r a c t
Introduction: Since the introduction of minimally invasive techniques, there is little agree-
ment about use of laparoscopic surgery for malignant liver lesions as compared to open
resection. We aim to analyse all available data comparing both these groups.
Methods: All the studies that compared laparoscopic and open liver resections for malig-
nant lesions were searched on various databases. Data were collected and analysed in
Review Manager RevMan (version 5.0).
Results: There were total of 10 studies (n ¼ 700) that compared laparoscopic (296/700) and
open (404/700) hepatic resections for malignant lesions. Laparoscopic group was associated
with reduced number of patients requiring blood transfusion [Odds ratio 0.35 CI 0.20, 0.60
P<0.001 HG 0.85], decreased number of positive resection margin [Odds ratio 0.34 CI 0.16,
P0.006 HG 0.73] and decrease in overall complication rate [Odds ratio 0.43, CI 0.26, 0.73
P0.002 HG 0.22]. Laparoscopic group was associated with less operative blood loss [WMD
162.6 ml CI �261.79, 73.45 P<0.001] and reduced hospital stay [WMD 4.28 days CI �6.33,
�2.23 P<0.001]; however, there was significant heterogeneity [HG <0.001] between the
studies for these parameters.
Conclusion: The laparoscopic group was associated with reduce overall complication rate,
positive resection margins and number of patients requiring blood transfusion. There is
still need for level I and II data to compare laparoscopic versus open hepatic resection in
malignant lesions.
Crown Copyright ª 2011 Royal College of Surgeons of Edinburgh (Scottish charity number
SC005317) and Royal College of Surgeons in Ireland. Published by Elsevier Ltd. All rights
reserved.
Introduction primary liver cancer worldwide, and a similar number of
Liver cancer is the fifth most common cancer in the world1,2
and it is associated with poor prognosis.2,3 If the tumour is
not removed completely after surgical resection, the survival
rate is usually between 3 and 6 months.1,2 In 1990, it was
estimated that there were more than 400,000 new cases of
0) 1224 551050; fax: þ44ight ª 2011 Royal Collegeed by Elsevier Ltd. All rig
patients died as a result of this disease.4,5
Hepatic tumours of malignant origin are commonly
secondary to metastatic cancer.1 The most common type of
primary hepatic cancer is hepatocellular carcinoma.1 The
treatment options depend on the stage of liver cancer and the
overall condition of the patient.
. Rao), [email protected] (G. Rao), [email protected]
(0) 1224 551236.of Surgeons of Edinburgh (Scottish charity number SC005317) andhts reserved.

t h e s u r g e on 1 0 ( 2 0 1 2 ) 1 9 4e2 0 1 195
First open liver resection was carried out in 1949.6 After the
explanation of functional anatomy of liver by Couinaud,7 its
progress became worldwide. The description of segmental
anatomy immensely assisted in improving surgical techniques.
The concept of minimally invasive surgery gradually crept
into liver surgery after the first laparoscopic resection of liver
was carried out in 1992.8,9 It was initially performed for benign
and cystic lesions that were located at easy accessible loca-
tions. As the surgical techniques became better defined, the
laparoscopic liver resection surgery was carried out for
malignant lesions. With on going technological advance-
ments in laparoscopic techniques, more hepatic resections of
malignant tumours are being carried out.
The evidence of comparison between laparoscopic versus
open hepatic resection of malignant tumours is still scarce.
Some observational studies have directly compared the peri-
and post-operative outcomes of laparoscopic and open liver
resection for hepatic lesions. In the recent years there have
been few comparative studies that investigated the short-
term and long-term effects of laparoscopic and open hepatic
resections for malignant lesions only. There is no level 1 or II
evidence comparing laparoscopic and open liver resection for
malignant lesions. In this study, we will analyse all the
available data of observational studies that compare laparo-
scopic and open liver resections for malignant lesions.
Methods
All the studies that compared laparoscopic vs. open liver
resections for malignant lesions were searched on various
databases that included Medline, Ovid, Embase, and Pubmed.
The following Mesh search terms were used:
“laparoscopy,” “hepatectomy,” “liver resection,” “Open liver
resection,” “Hepatic resection,” “laparoscopic liver resection,”
“segmentectomy,” “sectionectomy,” “comparative study.”
Further, the combinations of these termswere used. The term
like “vs” was used to find comparative studies in particular.
Table 1 e Demographics of the studies included.
Author Year Design No of patients
Lap Open
Mala et al. 2002 R, P(L) 13 14
Laurent et al. 2003 RM(O) 13 14
Kaneko et al. 2005 P(L), R(O) 30 28
Belli 2007 RM 23 23
Cai et al. 2008 RM 31 31
Belli et al. 2009 RM, P(L), RM 54 125
Tranchart et al. 2009 (O) 42 42
Sarpel et al. 2009 RM 20 56
Endo et al. 2009 RM 10 11
Castaing et al. 2009 RM 60 60
L, Laparoscopic; max, maximum; O, open; n/c, not commented; P, prosp
matched.
a 1 age; 2 gender; 3 American Society of Anaesthesiologists (ASA) classifi
7 resection type; 8 cirrhosis; 9 liver metastasis; 10 primary malignancy; 1
b 1 malignancy; 2 tumour location; 3 primary hepatic cancer; 4 only pat
7 resection type.
c 1 benign disease; 2 tumour location; 3 primary hepatic cancer; 4 metas
All the searched abstracts, studies, and citations were
analyzed. All the potential articles were cross-referenced.
There were no language restrictions. The latest date for the
search was 30th January 2010. Two independent researchers,
AR and IA reviewed the selected studies separately.
Inclusion criteria
Studies meeting the following criteria were included in the
systemic review:
(1) Studies that compared peri- and post-operative outcomes
in patients undergoing laparoscopic and open hepatic
resection
(2) Studies reporting at least one of the peri-operative
parameters, post-operative outcome measures or patho-
logical measures
(3) Studies in which all resected lesions were malignant.
Exclusion criteria
Studies were excluded from the analysis if
(1) The outcomes of interest were not reported
(2) It was impossible to extract or calculate the appropriate
data from the published results;
(3) The resected lesions were benign
Outcomes of interest and definitions
The following parameters were identified and reviewed for
each study.
Basic Demographics: first author, year of publication, total
number of patients in laparoscopic and open resection group
in each study, study design, matching criteria, inclusion and
exclusion criteria, and male to female ratio.
Peri-operative parameters: operative time, operative blood
loss, number of patients requiring blood transfusion, use of
portal triad clamping and duration of portal triad clamping.
Matchinga Inclusion criteriab Exclusion criteriac
1e6, 9, 11, 12 1 1, 3
1, 2, 4e8, 10, 12, 1, 3, 4 1, 2, 4
1, 2, 13 1, 3 1, 4
1e3, 5e8 2, 4, 6 1, 5, 6
1, 2, 5, 6, 8 e 1
1e3, 5e8 3, 4e6 1, 5, 6
1e3, 5, 7, 13 1, 4, 5 1
1, 2, 5, 8 3, 5 1
1e7, 1 3, 5 1
1e6, 9, 13 1, 2, 5e7 1
ective; PM, prospective matched; R, retrospective; RM, retrospective
cation; 4 malignancy; 5 mean size of lesion; 6 location of neoplasm;
1 previous operations; 12 neoplasm histology; 13 Child-Pugh grading.
ients with chronic liver disease; 5 ASA classification; 6 tumour size;
tatic cancer, 5 ASA classification; 6 Child-Pugh grading.

Table 2 e Characteristics of the studies included.
Author Conversions Mean age (median) Female (n [%])
n (%) Lap Open Lap Open
Mala et al. 0 68 59 4 (31) 4 (29)
Laurent et al. 2 (15.4) 62.6 65.9 3 (23) 4 (24)
Kaneko et al. 1 (3.3) 59 61 12 (40) 18 (64)
Belli 1 (4.3) 59.5 62.4 10 (43.5) 9 (39.1)
Cai et al. 1 (3.2) 54.2 51.7 7 (22.5) 5 (16.1)
Belli et al. 4 (7) 63.6 61.5 23 (42.5) 47 (37.6)
Tranchart et al. 2 (4.7) 63.7 65.7 15 (35.7) 14 (33.3)
Sarpel et al. 4 (17) 63.8 58.3 5 (25) 11(20)
Endo et al. 0 72 64 2 (20) 3 (29)
Castaing et al. 6 (10) 62 62 23 (28.3) 23 (28.3)
t h e s u r g e on 1 0 ( 2 0 1 2 ) 1 9 4e2 0 1196
Postoperative parameter: time to first oral Intake, duration of
post operative hospital stay and post-operative analgesia
requirement.
Early post operative adverse events: post operative complica-
tions divided into liver resectionerelated (cirrhotic decom-
pensation/ascites, hepatic hemorrhage, biliary leakage, liver
failure) and general complications (chest infection, bowel
perforation, urinary infection, wound infection, cardiac
complications, intra-abdominal abscesses, Clostridium difficile
infection, pleural effusion).
Oncological clearance: Conversion rate, pathologic resection
margin size, positive resection margins, resection margins
<1 cm, and resection margins >1 cm.
Long-term outcomes: Short-term and long-term cost effec-
tiveness, overall complication rate (includes all liver-specific
and general complications), incisional hernia, mortality rate,
5 year and 3 year survival outcome, and recurrence rate.
Statistical analysis
Statistical softwareReviewManager, version 5.0 (TheCochrane
Collaboration, Software Update, Oxford, United Kingdom) was
used toperformtheanalysis.Weightedmeandifference (WMD)
Table 3 e Pathological characteristics of laparoscopic group.
Author No. of procedures n (%) Pathology ofresecte
Mala et al. 15 (52) C ¼ 13
Laurent et al. 13 (48) E ¼ 13
Kaneko et al. 30 (52) E ¼ 30
Belli et al. 23 (50) E ¼ 23
Cai et al. 31 (50) E ¼ 24, G ¼ 4
Belli et al. 54 (30) E ¼ 54
Tranchart et al. 42 (50) E ¼ 42
Sarpel et al. 20 (24) E ¼ 20
Endo et al. 10 (49) E ¼ 10
Castaing et al. 60 (50) C ¼ 60
L, Laparoscopic; n/c, not commented; O, open.
T, three segments resection; LLS, left lateral segmentectomy; RHL, right he
n/c not commented.
a C, malignant metastatic; E, hepatocellular carcinoma; G, gallbladder ca
b W, Wedge resections; S, segmentectomies; B, bisegmentectomies; T, t
hepatic lobectomy; LH, Left hemihepatectomy; PH, partial hepatectomy;
was used to analyse difference among continuous variables.
Odds Ratio (OR) was used to analyse difference in dichotomous
variables. 95% confidence interval (CI) was reported for each
analysed value. To standardize the data on continuous vari-
ables standard deviation (SD) were included. For the studies
that provided the range values for each variable, their range
values were converted to SD and analysed. Continuous vari-
ableswithoutSDwerenot included in theanalysis.Studieswith
no events in a particular outcome for laparoscopic and open
groupswere not included. To assess publication bias, graphical
Exploration with funnel plots were used.
Results
There were total of 10 studies10e19 (n ¼ 700) that compared
laparoscopic (296/700) and open (404/700) hepatic resections
for malignant lesions.
Basic demographics
Tables 1 and 2: The average age for laparoscopic and open liver
resection was 62.84 and 61.15 respectively. The proportion of
lesionsda
Mean size(mm)
Procedures performedb
26 S ¼ 6, B ¼ 7, T ¼ 2
33.5 W ¼ 3, S ¼ 7, B ¼ 3
30 LLS ¼ 10, PH ¼ 20
31 W ¼ 15, S ¼ 3, LLS ¼ 5
, C ¼ 3 39.9 PH ¼ 17, S ¼ 8, LLS ¼ 3, LH ¼ 3
36 W ¼ 21, S ¼ 16, LLS ¼ 14
35.8 RHL ¼ 3, LH ¼ 2, LLS ¼ 9, B ¼ 3,
S ¼ 15, W ¼ 10
43 n/c
30 LLS ¼ 10
33 RHL ¼ 20, S ¼ 5, B ¼ 5, W ¼ 30
patic lobectomy; LH, Left hemihepatectomy; PH, partial hepatectomy;
ncer.
hree segments resection; LLS, left lateral segmentectomy; RHL, right
n/c not commented.

Table 4 e Pathological characteristics of open group.
Author Number of procedures n (%) Pathology of lesionsresecteda
Mean size(mm)
Procedures performedb
Mala et al. 14 (48) C ¼ 14 30 S ¼ 9, B ¼ 3, T ¼ 2
Laurent et al. 14 (52) E ¼ 14 31 W ¼ 4, S ¼ 7, B ¼ 3
Kaneko et al. 28 (48) E ¼ 28 31 LLS ¼ 8, PH ¼ 20
Belli et al. 23 (50) E ¼ 23 32.4 W ¼ 12, S ¼ 5, LLS ¼ 6
Cai et al. 31 (50) E ¼ 26, G ¼ 3, C ¼ 2 36.2 PH ¼ 17, S ¼ 8, LLS ¼ 3, LH ¼ 3
Belli et al. 125 (70) E ¼ 125 60 T ¼ 39
Tranchart et al. 42 (50) E ¼ 42 36.8 RHL ¼ 3, LH ¼ 2, LLS ¼ 7, B ¼ 7,
S ¼ 13, W ¼ 10
Sarpel et al. 5 (76) E ¼ 56 43 n/c
Endo et al. 11 (51) E ¼ 11 41 LLS ¼ 11
Castaing et al. 60 (50) C ¼ 60 44 RHL ¼ 7, S ¼ 10, B ¼ 8 W ¼ 35
L, Laparoscopic; n/c, not commented; O, open.
T, three segments resection; LLS, left lateral segmentectomy; RHL, right hepatic lobectomy; LH, Left hemihepatectomy; PH, partial hepatectomy;
n/c not commented.
a C, malignant metastatic; E, hepatocellular carcinoma; G, gallbladder cancer.
b W, Wedge resections; S, segmentectomies; B, bisegmentectomies; T, three segments resection; LLS, left lateral segmentectomy; RHL, right
hepatic lobectomy; LH, Left hemihepatectomy; PH, partial hepatectomy; n/c not commented.
t h e s u r g e on 1 0 ( 2 0 1 2 ) 1 9 4e2 0 1 197
females in the laparoscopic and open groups was 31.15% and
32.04% respectively.
Six studies10e14,18 were retrospectively matched and one
study17 was retrospectively unmatched. Two studies16,19
included prospective selection of laparoscopic group, which
wasmatchedwithretrospectivedata foropengroup.Twentyone
patients from laparoscopic group were converted to open (7%).
Tables 3 and 4: Seven studies10,11,14e16,18,19 included only
metastatic malignant lesions, 2 studies13,17 only included
hepatocellular carcinoma (HCC) lesions and one study12
included a combination of metastatic malignant lesion, HCC
and gallbladder cancer.
Peri-operative parameters
Eight studies10e12,14e17,19 reported that laparoscopic groupwas
associated with less operative blood loss by 162.6 ml [CI
�261.79, 73.45] than open group ( p < 0.001) but there was
significant heterogeneity between the studies ( p < 0.001).
Six studies10,11,13,16,17,19 reported that laparoscopic group
was associated with reduced number of patients requiring
blood transfusion by 0.35 [CI 0.20, 0.60] than open group
( p < 0.001) and it was not associated with heterogeneity
between studies (p0.85) (Figs. 1 and 2).
Five studies10,11,13,16,19 reported that laparoscopic group
was associated with less use of portal triad clamping by 0.08
Study or Subgroup
Mala et alLaurent et alBelli et alBelli et al.Castaing et alTranchart et al
Total (95% CI)
Total eventsHeterogeneity: Tau² = 0.00; Chi² = 2.03, df = 5 (P = 0.85); I² = 0%Test for overall effect: Z = 3.81 (P = 0.0001)
Events
110694
21
Total
131323546042
205
Events
144
3222
7
70
Total
141423
1256042
278
Weight
3.5%5.3%3.3%
33.2%37.6%17.0%
100.0%
M
Laparoscopic Open
Fig. 1 e Laparoscopic vs open resection: Number
[CI 0.01, 0.46] than open group (p0.005) but it was associated
with significant heterogeneity between the studies (p0.01).
There was no significant difference between the two groups
for operative time (p0.71). Although laparoscopic group was
associated with reduced duration of portal triad clamping
( p < 0.001) but it was only reported by one study.16
Post operative parameters
Eight studies10e12,14e17,19 reported that laparoscopic groupwas
associated with reduced hospital stay by 4.28 days [CI �6.33,
�2.23] than open group ( p < 0.001) but there was significant
heterogeneity between the studies ( p < 0.001).
Three studies12,14,15 reported that laparoscopic group
was associated with reduced time to oral intake by 1.29
days [CI �2.23, �0.35] than open group (p0.007) but there
was significant heterogeneity between the studies (p0.007).
Early post-operative adverse outcomes
� Liver related adverse outcomes:There was no significant
difference between the two groups for cirrhotic decom-
pression/ascites (p 0.39), hepatic haemorrhage (p 0.08),
biliary leakage (p 0.25), and liver failure (p 0.07).
� General complications: There was no significant difference
between the two groups for chest infection (p 0.56), wound
infection (p 0.79) and mortality (p 0.58).
-H, Random, 95% CI
1.08 [0.06, 19.31]0.21 [0.02, 2.18]0.09 [0.00, 1.82]0.36 [0.14, 0.93]0.30 [0.13, 0.74]0.53 [0.14, 1.95]
0.35 [0.20, 0.60]
Year
200220032007200920092009
Odds Ratio Odds Ratio
M-H, Random, 95% CI
0.01 0.1 1 10 100Laparoscopic Open
of patients requiring blood transfusion (n).

0.01 0.1 1 10 100
0
0.5
1
1.5
2OR
SE(log[OR])
Fig. 2 e Laparoscopic vs open resection: Funnel plot of number of patients requiring blood transfusion (n).
t h e s u r g e on 1 0 ( 2 0 1 2 ) 1 9 4e2 0 1198
� Oncological clearance: Three studies11,13,18 reported that
laparoscopic group was associated with reduced number of
positive resection margin by 0.34 [CI 0.16, 0.73] than open
group (p0.006) and it was not associated with heterogeneity
between studies (p0.75) (Fig. 3). There was no significant
difference between the two groups for size of pathological
resection margin (p0.84).
Long term outcomes
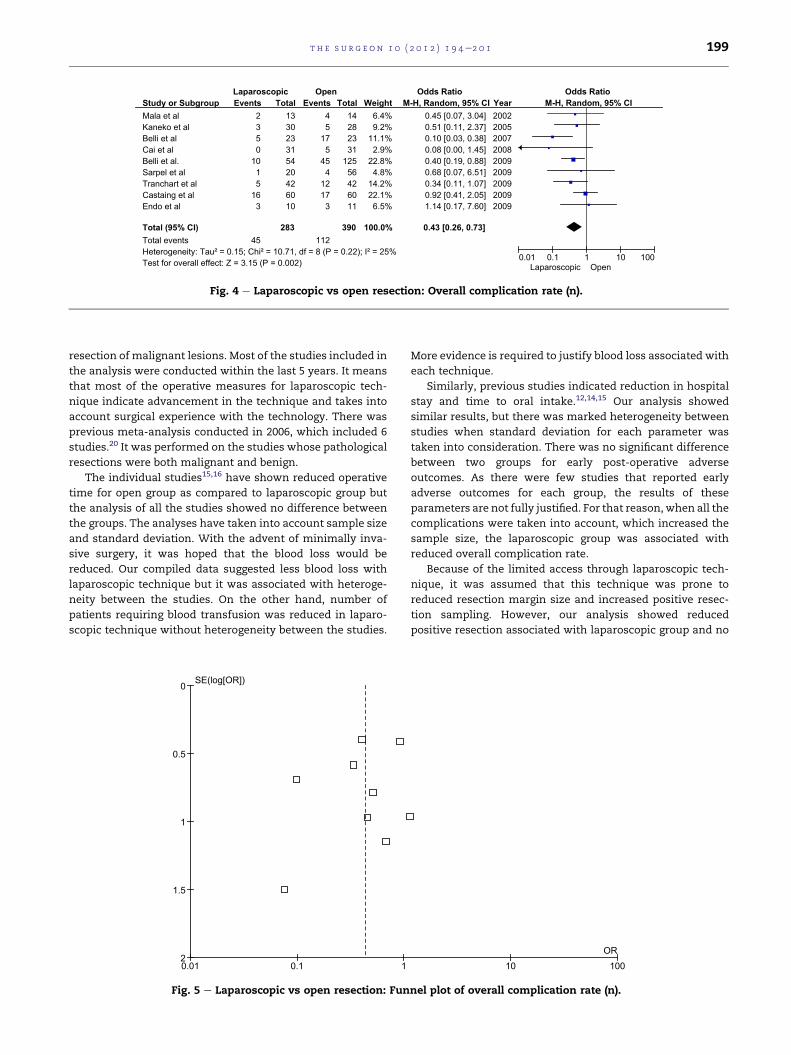
Nine studies10e15,17e19 reported that laparoscopic group was
associated with reduced overall complication rate by 0.43 [CI
0.26, 0.73] than open group (p0.002) and it was not associated
with heterogeneity between studies (p0.22) (Figs. 4 and 5).
There was no significant difference between two groups for
recurrence rate (p0.17), 5-year survival (p 0.10 and 0.07) and 3-
year survival (p 0.17 and 0.26).
Discussion
Overall, laparoscopic group has been favoured over open
group for a few post-operative parameters in our analysis
(Table 5). The laparoscopic group was associated with less
number of patients requiring blood transfusion and reduce
Study or Subgroup
Castaing et alBelli et al.Sarpel et al
Total (95% CI)
Total eventsHeterogeneity: Tau² = 0.00; Chi² = 0.58, df = 2 (P = 0.75); I² = 0%Test for overall effect: Z = 2.75 (P = 0.006)
Events
802
10
Total
605420
134
Events
178
15
40
Total
60125
56
241
Weight
68.7%7.3%
24.0%
100.0%
M
Laparoscopic Open
Fig. 3 e Laparoscopic vs open resection: Nu
positive resection margins. Similarly, laparoscopic group had
decreased overall complication rate than open group. All
these results were significant and not associated with
heterogeneity between the studies. Although, laparoscopic
group was also associated with reduced operative blood loss,
use of portal triad clamping, duration of hospital stay and time
to oral intake, however, this was linked to significant hetero-
geneity between the studies. There was no significant differ-
ence between the two groups for other peri- and post-
operative parameters.
This study is the one of the first meta-analysis to be con-
ducted that compared laparoscopic and open hepatic resec-
tion for malignant lesions. To our knowledge, there has been
no randomised controlled trial or systemic review evaluating
this topic before. The study included 10 observational studies
with a good participants’ size (n ¼ 700). It investigated most of
the peri- and post-operative parameters along with short and
long term adverse outcomes.
The inclusion and exclusion criteria of majority of the
studies were clearly indicated to delineate any discrepancies
in the results and its analysis. Most studies had laparoscopic
and open groups matched for demographics and character-
istics of the patients. It included the patients with cirrhosis
and moderate to severe co-morbidity (ASA grade II and above)
to take into account common factors associated with
-H, Random, 95% CI
0.39 [0.15, 0.99]0.13 [0.01, 2.24]0.30 [0.06, 1.47]
0.34 [0.16, 0.73]
Year
200920092009
Odds Ratio Odds Ratio
M-H, Random, 95% CI
0.01 0.1 1 10 100Laparoscopic Open
mber of positive resection margins (n).
Study or Subgroup
Mala et alKaneko et alBelli et alCai et alBelli et al.Sarpel et alTranchart et alCastaing et alEndo et al
Total (95% CI)
Total eventsHeterogeneity: Tau² = 0.15; Chi² = 10.71, df = 8 (P = 0.22); I² = 25%Test for overall effect: Z = 3.15 (P = 0.002)
Events
2350
1015
163
45
Total
133023315420426010
283
Events
45
175
454
1217
3
112
Total
14282331
12556426011
390
Weight
6.4%9.2%
11.1%2.9%
22.8%4.8%
14.2%22.1%6.5%
100.0%
M-H, Random, 95% CI
0.45 [0.07, 3.04]0.51 [0.11, 2.37]0.10 [0.03, 0.38]0.08 [0.00, 1.45]0.40 [0.19, 0.88]0.68 [0.07, 6.51]0.34 [0.11, 1.07]0.92 [0.41, 2.05]1.14 [0.17, 7.60]
0.43 [0.26, 0.73]
Year
200220052007200820092009200920092009
Laparoscopic Open Odds Ratio Odds Ratio
M-H, Random, 95% CI
0.01 0.1 1 10 100Laparoscopic Open
Fig. 4 e Laparoscopic vs open resection: Overall complication rate (n).
t h e s u r g e on 1 0 ( 2 0 1 2 ) 1 9 4e2 0 1 199
resection of malignant lesions. Most of the studies included in
the analysis were conducted within the last 5 years. It means
that most of the operative measures for laparoscopic tech-
nique indicate advancement in the technique and takes into
account surgical experience with the technology. There was
previous meta-analysis conducted in 2006, which included 6
studies.20 It was performed on the studies whose pathological
resections were both malignant and benign.
The individual studies15,16 have shown reduced operative
time for open group as compared to laparoscopic group but
the analysis of all the studies showed no difference between
the groups. The analyses have taken into account sample size
and standard deviation. With the advent of minimally inva-
sive surgery, it was hoped that the blood loss would be
reduced. Our compiled data suggested less blood loss with
laparoscopic technique but it was associated with heteroge-
neity between the studies. On the other hand, number of
patients requiring blood transfusion was reduced in laparo-
scopic technique without heterogeneity between the studies.
0.01 0.1 1
0
0.5
1
1.5
2
SE(log[OR])
Fig. 5 e Laparoscopic vs open resection: Fun
More evidence is required to justify blood loss associated with
each technique.
Similarly, previous studies indicated reduction in hospital
stay and time to oral intake.12,14,15 Our analysis showed
similar results, but there was marked heterogeneity between
studies when standard deviation for each parameter was
taken into consideration. There was no significant difference
between two groups for early post-operative adverse
outcomes. As there were few studies that reported early
adverse outcomes for each group, the results of these
parameters are not fully justified. For that reason,when all the
complications were taken into account, which increased the
sample size, the laparoscopic group was associated with
reduced overall complication rate.
Because of the limited access through laparoscopic tech-
nique, it was assumed that this technique was prone to
reduced resection margin size and increased positive resec-
tion sampling. However, our analysis showed reduced
positive resection associated with laparoscopic group and no
10 100OR
nel plot of overall complication rate (n).
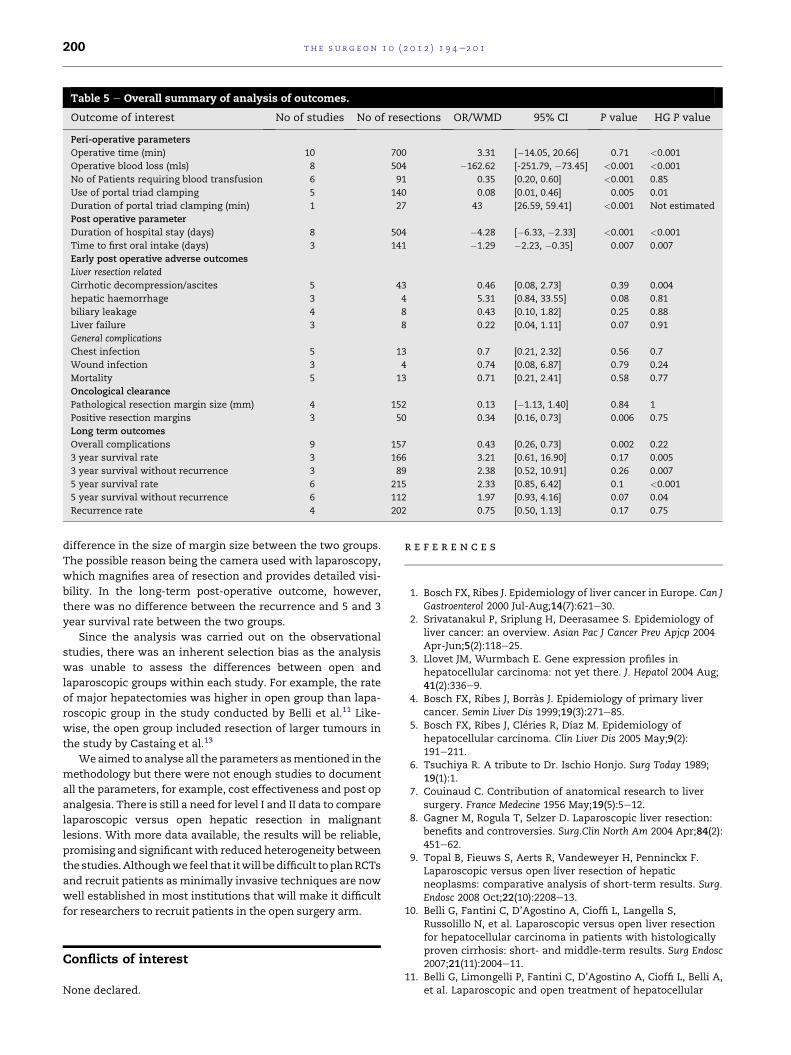
Table 5 e Overall summary of analysis of outcomes.
Outcome of interest No of studies No of resections OR/WMD 95% CI P value HG P value
Peri-operative parameters
Operative time (min) 10 700 3.31 [�14.05, 20.66] 0.71 <0.001
Operative blood loss (mls) 8 504 �162.62 [-251.79, �73.45] <0.001 <0.001
No of Patients requiring blood transfusion 6 91 0.35 [0.20, 0.60] <0.001 0.85
Use of portal triad clamping 5 140 0.08 [0.01, 0.46] 0.005 0.01
Duration of portal triad clamping (min) 1 27 43 [26.59, 59.41] <0.001 Not estimated
Post operative parameter
Duration of hospital stay (days) 8 504 �4.28 [�6.33, �2.33] <0.001 <0.001
Time to first oral intake (days) 3 141 �1.29 �2.23, �0.35] 0.007 0.007
Early post operative adverse outcomes
Liver resection related
Cirrhotic decompression/ascites 5 43 0.46 [0.08, 2.73] 0.39 0.004
hepatic haemorrhage 3 4 5.31 [0.84, 33.55] 0.08 0.81
biliary leakage 4 8 0.43 [0.10, 1.82] 0.25 0.88
Liver failure 3 8 0.22 [0.04, 1.11] 0.07 0.91
General complications
Chest infection 5 13 0.7 [0.21, 2.32] 0.56 0.7
Wound infection 3 4 0.74 [0.08, 6.87] 0.79 0.24
Mortality 5 13 0.71 [0.21, 2.41] 0.58 0.77
Oncological clearance
Pathological resection margin size (mm) 4 152 0.13 [�1.13, 1.40] 0.84 1
Positive resection margins 3 50 0.34 [0.16, 0.73] 0.006 0.75
Long term outcomes
Overall complications 9 157 0.43 [0.26, 0.73] 0.002 0.22
3 year survival rate 3 166 3.21 [0.61, 16.90] 0.17 0.005
3 year survival without recurrence 3 89 2.38 [0.52, 10.91] 0.26 0.007
5 year survival rate 6 215 2.33 [0.85, 6.42] 0.1 <0.001
5 year survival without recurrence 6 112 1.97 [0.93, 4.16] 0.07 0.04
Recurrence rate 4 202 0.75 [0.50, 1.13] 0.17 0.75
t h e s u r g e on 1 0 ( 2 0 1 2 ) 1 9 4e2 0 1200
difference in the size of margin size between the two groups.
The possible reason being the camera used with laparoscopy,
which magnifies area of resection and provides detailed visi-
bility. In the long-term post-operative outcome, however,
there was no difference between the recurrence and 5 and 3
year survival rate between the two groups.
Since the analysis was carried out on the observational
studies, there was an inherent selection bias as the analysis
was unable to assess the differences between open and
laparoscopic groups within each study. For example, the rate
of major hepatectomies was higher in open group than lapa-
roscopic group in the study conducted by Belli et al.11 Like-
wise, the open group included resection of larger tumours in
the study by Castaing et al.13
We aimed to analyse all the parameters asmentioned in the
methodology but there were not enough studies to document
all the parameters, for example, cost effectiveness and post op
analgesia. There is still a need for level I and II data to compare
laparoscopic versus open hepatic resection in malignant
lesions. With more data available, the results will be reliable,
promising and significant with reduced heterogeneity between
the studies.Althoughwe feel that itwill bedifficult toplanRCTs
and recruit patients as minimally invasive techniques are now
well established in most institutions that will make it difficult
for researchers to recruit patients in the open surgery arm.
Conflicts of interest
None declared.
r e f e r e n c e s
1. Bosch FX, Ribes J. Epidemiology of liver cancer in Europe. Can JGastroenterol 2000 Jul-Aug;14(7):621e30.
2. Srivatanakul P, Sriplung H, Deerasamee S. Epidemiology ofliver cancer: an overview. Asian Pac J Cancer Prev Apjcp 2004Apr-Jun;5(2):118e25.
3. Llovet JM, Wurmbach E. Gene expression profiles inhepatocellular carcinoma: not yet there. J. Hepatol 2004 Aug;41(2):336e9.
4. Bosch FX, Ribes J, Borras J. Epidemiology of primary livercancer. Semin Liver Dis 1999;19(3):271e85.
5. Bosch FX, Ribes J, Cleries R, Dıaz M. Epidemiology ofhepatocellular carcinoma. Clin Liver Dis 2005 May;9(2):191e211.
6. Tsuchiya R. A tribute to Dr. Ischio Honjo. Surg Today 1989;19(1):1.
7. Couinaud C. Contribution of anatomical research to liversurgery. France Medecine 1956 May;19(5):5e12.
8. Gagner M, Rogula T, Selzer D. Laparoscopic liver resection:benefits and controversies. Surg.Clin North Am 2004 Apr;84(2):451e62.
9. Topal B, Fieuws S, Aerts R, Vandeweyer H, Penninckx F.Laparoscopic versus open liver resection of hepaticneoplasms: comparative analysis of short-term results. Surg.Endosc 2008 Oct;22(10):2208e13.
10. Belli G, Fantini C, D’Agostino A, Cioffi L, Langella S,Russolillo N, et al. Laparoscopic versus open liver resectionfor hepatocellular carcinoma in patients with histologicallyproven cirrhosis: short- and middle-term results. Surg Endosc2007;21(11):2004e11.
11. Belli G, Limongelli P, Fantini C, D’Agostino A, Cioffi L, Belli A,et al. Laparoscopic and open treatment of hepatocellular

t h e s u r g e on 1 0 ( 2 0 1 2 ) 1 9 4e2 0 1 201
carcinoma in patients with cirrhosis. Br.J.Surg 2009 Sep;96(9):1041e8.
12. Cai XJ, Yang J, Yu H, Liang X, Wang YF, Zhu ZY, et al. Clinicalstudy of laparoscopic versus open hepatectomy for malignantliver tumors. Surg.Endosc 2008 Nov;22(11):2350e6.
13. Castaing D, Vibert E, Ricca L, Azoulay D, Adam R, Gayet B.Oncologic results of laparoscopic versus open hepatectomyfor colorectal liver metastases in two specialized centers.Ann.Surg 2009 Nov;250(5):849e55.
14. Endo Y, Ohta M, Sasaki A, Kai S, Eguchi H, Iwaki K, et al. Acomparative study of the long-term outcomes afterlaparoscopy-assisted and open left lateral hepatectomy forhepatocellular carcinoma. Surg Laparosc Endosc Percutan Tech2009;19(5):171e4.
15. Kaneko H, Takagi S, Otsuka Y, Tsuchiya M, Tamura A,Katagiri T, et al. Laparoscopic liver resection of hepatocellularcarcinoma. Am.J.Surg 2005 Feb;189(2):190e4.
16. Laurent A, Cherqui D, Lesurtel M, Brunetti F, Tayar C,Fagniez PL. Laparoscopic liver resection for subcapsular
hepatocellular carcinoma complicating chronic liver disease.Arch Surg 2003;138(7):763e9. discussion 769; Jul.
17. Mala T, Edwin B, Gladhaug I, Fosse E, Soreide O, Bergan A,et al. A comparative study of the short-term outcomefollowing open and laparoscopic liver resection of colorectalmetastases. Surg.Endosc 2002 Jul;16(7):1059e63.
18. Sarpel U, Hefti MM, Wisnievsky JP, Roayaie S,Schwartz ME, Labow DM. Outcome for patients treatedwith laparoscopic versus open resection of hepatocellularcarcinoma: case-matched analysis. Ann Surg Oncol 2009Jun;16(6):1572e7.
19. Tranchart H, Di Giuro G, Lainas P, Roudie J, Agostini H,Franco D, et al. Laparoscopic resection for hepatocellularcarcinoma: a matched-pair comparative study. J Surg Endosc;2009. doi:10.1007/s00464-009-0745-3 (epub).
20. Simillis C, Constantinides VA, Tekkis PP, Darzi A,Lovegrove R, Jiao L, et al. Laparoscopic versus open hepaticresections for benign and malignant neoplasmsea meta-analysis. Surgery 2007 Feb;141(2):203e11.