laboratory markers of alcohol abuse - icadts … the search for more objective laboratory markers of...
TRANSCRIPT

Laboratory Markers of Alcohol Abuse
Pekka Sillanaukee
Alcohol Related Diseases, Pharmacia & Upjohn Diagnostics AB, Sweden, and University of
Tampere, Medical School, Finland
Alcohol consumption in many parts of Europe has increased considerably in the past 25
years, and with it alcohol-related problems have risen sharply. Consequently, more patients
seen in clinical practice as well as among drunk drivers have an underlying alcohol problem.
The need for accurate methods for detection and monitoring of alcohol abuse in different
health care settings is huge.
Despite the need there is no exact clinical finding or symptom in a patient history, in an
interview or in a clinical status that is sufficiently sensitive and specific to detect alcohol
abuse in its early phase. The clinical signs o f alcohol abuse are rather minimal in the early
phase o f alcohol abuse while most o f the signs arise later, after several years o f excessive
drinking. Alcohol consumption is usually under-reported in interviews. Alcohol abusers tend
to underestimate their drinking even more than the social drinkers (Poikolainen, 1995). For
example, in our study among heavy drinkers who were willing to participate in a brief
intervention treatment the typical first self-reported alcohol consumption was only 124
g/week among males and 73 g/week among females (Sillanaukee, 1995). The reliability of
personal interviews about alcohol consumption is difficult. This is especially true when the
individual is trying to get feedback about his/her excessive drinking.
The reasons for using biological laboratory markers are that they give objective information
about alcohol consum ption and changes in drinking habits. Consequently, laboratory tests are
useful in screening heavy drinking; in decision making about the role of alcohol as an
etiologic factor o f disease; in follow-up and monitoring changes in alcohol consumption; in
m otivating patients to change their drinking habits by showing alcohol-induced changes in
their bodies; and, finally, in picking up patients who are sensitive for alcohol-induced
problems.
- 217 -

Thus, the search for more objective laboratory markers of alcohol abuse has been active.
Several laboratory abnormalities based on hematological characteristics, liver enzyme
activities, lipids, immune function factors, hormones, neurological factors have been
observed to be associated with alcohol abuse (Holt et al, 1981; Cushman et al, 1984; Watson
et al, 1986; Salaspuro, 1986 and 1989; Nilssen and Huseby, 1992; Mihas and Tavassoli,
1992; Stibler, 1992; Allen et al, 1994).
Blood, urine or breath ethanol analyses (5HTOL) and creatinine or 5-hydroxyindoleactic acid
(HIAA) in urine have been proposed to be a specific short-term marker for alcohol
consumption (Voltaire et al, 1992; Helander et al, 1995). 5HTOL stays elevated 6-20 hours
after ethanol disappearance. False positive values have been reported in patients using drugs
inhibiting aldehyde dehydrogenase. If the 5HTOL ratio to creatinine (instead of HIAA) is
used also serotonine rich food may cause false positive values. The marker seems to be
promising, having high sensitivity and specificity for detecting recent alcohol consumption.
The measurement is based on GC-MS technique or HPLC with electrochemical detection
(Helander, 1992) and thus the problem is the difficulty o f routine application today.
Elevated serum levels of membrane-bound enzyme, eamma-elutamvl transferase (GGT) have
been widely used as a marker of alcohol abuse. The sensitivity of GGT in detecting alcohol
abuse has been reported to vary between 34% and 85%. GGT is not increased after acute
alcohol intake but needs probably alcohol consumption of 80-200 g/day for one or several
weeks. The half-life o f elevated GGT is between two and three weeks. In addition to alcohol
abuse increased GGT is frequently found in non-alcoholic liver disease, diabetes, obesity,
pancreatitis, hyperlipidemia, heart failure, severe trauma, and in subjects using barbiturates,
antiepileptics or anticoagulants. Despite its poor specificity, 50-72% of elevated GGT values
can be explained by an excessive alcohol consumption (Kristenson et al, 1980; Penn et al,
1981; Suokas, 1992).
Mean corpuscular volume (MCV) is an index of red blood cell size. Increased MCV values
have been observed in 34-89% of alcohol abusers (Wu et al, 1974; Unger and Johnson, 1974;
Chick et al, 1981). Increased MCV values are also found in vitamin B12 and folic acid
deficiency, liver diseases, several hematological diseases, hypothyroidism, reticulocytosis, in
users o f antiepileptics, as well as among smokers. Alcohol abuse has been found to explain
- 2 1 8 -

increased MCV values in 89% of men and 56% of women in general practice (Seppa et al,
1991). MCV responds slowly to abstinence and up to 40% may have an elevated MCV value
even after three months o f abstinence (Morgan et al, 1981).
Other widely used markers are serum aspartate aminotransferase (ASAT) and alanine
aminotransferase (ALAT). The intracellular enzymes are more indicative for liver damage
than for alcohol abuse. The pooled sensitivity o f ASAT has been estimated to be 35% as a
marker of alcohol abuse (Rosman and Lieber, 1991). The sensitivity for ALAT may be even
poorer. Increased values are also found in non-alcoholic liver diseases (ASAT, ALAT), in
muscle disorders (ASAT), and in myocardial infraction (ASAT).
One of the recently developed routine laboratory tests for alcohol abuse is serum
carbohydrate-deficient transferrin (CDT). The marker consists o f a-, mono-, and
disialoisoforms of transferrin that are deficient in their terminal trisaccharide. In a recent
review by Helena Sdbler (1992) summarizing 2500 individuals in different studies, a total
clinical sensitivity was 82% and specificity 97%. False positives have been reported in
patients with severe liver diseases (mainly in primary biliary chirrosis, chronic hepatitis C,
hepatic malignities), in patients with genetic D-variant of transferrin, and in patients with an
inborn error of glycoprotein metabolism. In a more recent study Anton and Moak (1994)
reported a sensitivity o f 79% and a specificity of >90% among males who drank more than
60 g/day before admission. During abstinence the CDT values normalize with a mean half-
life o f 14-17 days. Females have higher normal values of CDT than males, possibly due to
asialo- and monosialotransferrin.
CDT has now been shown to have high specificity and a sensitivity that is at least equal to
that of the conventional laboratory markers. CDT values seem to increase after 10 days of
drinking at 50-80 grams of ethanol per day. It has also a relatively good correlation with self-
reported alcohol consumption but not with conventional markers. This combination makes it
suitable for routine work in the detection of alcohol abuse and monitoring either abstinence or
relapse during treatment. Additionally, by following relative changes in CDT and GGT from
each individual’s baseline values, rather than using the conventional population-based cut
offs, one may improve the detection of relapses in a monitoring situation (Borg et al, 1995;
- 21 9 -
Helander et al, 1996). In one study CDT detected relapses even before self-report among
male subjects (Rosman et al, 1995).
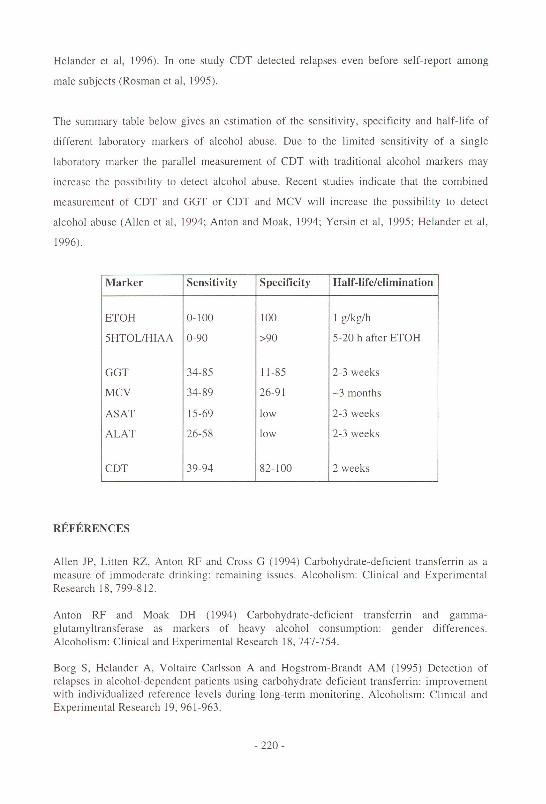
The summary table below gives an estimation of the sensitivity, specificity and half-life o f
different laboratory markers of alcohol abuse. Due to the limited sensitivity o f a single
laboratory marker the parallel measurement of CDT with traditional alcohol markers may
increase the possibility to detect alcohol abuse. Recent studies indicate that the combined
measurement of CDT and GGT or CDT and MCV will increase the possibility to detect
alcohol abuse (Allen et al, 1994; Anton and Moak, 1994; Yersin et al, 1995; Helander et al,
1996).
Marker Sensitivity Specificity Half-life/elim ination
ETOH 0 - 1 0 0 1 0 0 1 g/kg/h
5HTOL/HIAA 0-90 >90 5-20 h after ETOH
GGT 34-85 11-85 2-3 weeks
MCV 34-89 26-91 -3 months
AS AT 15-69 low 2-3 weeks
ALAT 26-58 low 2-3 weeks
CDT 39-94 82-100 2 weeks
REFERENCES
Allen JP, Litten RZ, Anton RF and Cross G (1994) Carbohydrate-deficient transferrin as a measure o f immoderate drinking: remaining issues. Alcoholism: Clinical and Experimental Research 18,799-812.
Anton RF and Moak DH (1994) Carbohydrate-deficient transferrin and gamma- glutamyltransferase as markers of heavy alcohol consumption: gender differences. Alcoholism: Clinical and Experimental Research 18, 747-754.
Borg S, Helander A, Voltaire Carlsson A and Hogstrom-Brandt AM (1995) Detection of relapses in alcohol-dependent patients using carbohydrate-deficient transferrin: improvement with individualized reference levels during long-term monitoring. Alcoholism: Clinical and Experimental Research 19, 961-963.
- 22 0-

Chick J (1981) Mean cell volume and gamma-glutamyltranspeptidase as markers o f drinking in working men. Lancet i, 1249-1251.
Cushman P, Jacobson G, Barboriak JJ and Anderson AJ (1984) Biomedical markers for alcoholism: sensitivity problems. Alcoholism: Clinical and Experimental Research 8 , 253- 257.
Helander A, Beck O and Borg S (1992a) Determination of urinary 5-hydroxytryptophol by high-performance liquid chromatography with electrochemical detection. Journal of Chromatography 579, 340-345.
Helander A, Beck O and Jones AW (1992b) Urinary 5HTOL/5HIAA as biochemical marker o f postmortem ethanol synthesis (letter). Lancet 340, 1159.
Helander A, Voltaire Carlsson A and Borg S (1996) Longitudinal comparison of carbohydrate-deficient transferrin and gamma-glutamyltransferase complementary markers of excessive alcohol consumption. Alcohol and Alcoholism 31, 101-107.
Holt S, Skinner HA and Israel Y (1981) Early identification of alcohol abuse: 2: Clinical and laboratory indicators. Canadian Medical Association Journal 124, 1279-1294.
Kristenson H, Ohrn J, Trell E and Hood B (1980) Serum gamma-glutamyltransferase at screening and retrospective sickness days (letter). Lancet i, 1141.
M ihas AA and Tavassoli M (1992) Laboratory markers of ethanol intake and abuse: a critical appraisal. American Journal o f Medical Sciences 303, 415, 428.Morgan MY, Camil ME, Luck W, Sherlock S and Hoffbrand AV (1981) Macrocytosis in alcohol-related liver disease: its value for screening. Clinical Laboratory Haematology 3, 35- 44.
National Council on Alcoholism (1972) Criteria for the diagnosis of alcoholism by the Criteria Committee. American Journal of Psychiatry 129, 127-135.
Nilssen O, Huseby NE, Hoyer G, Brenn T, Schirmer H and Forde OH (1992) New alcohol markers— how useful are they in population studies: the Svalbard Study 1988-1989. Alcoholism: Clinical and Experimental Research 16, 82-86.
Penn R, W orthington LJ, Clarke CA and Whitfiel AGW (1981) Gamma- glutam yltranspeptidase and alcohol intake. Lancet i, 849.
Poikolainen K (1985) Underestimation of recalled alcohol intake in relation to actual consumption. British Journal on Addiction 80, 215-216.
Rosman AS and Lieber CS (1992) An overview of current and emerging markers of alcoholism. In: Measuring alcohol consumption, Litten R and Allen J, eds. The Humana Press Inc., NJ, USA.
- 221 -

Rosman AS, Basu P, Galvin K and Lieber CS (1995) Utility o f carbohydrate-deficient transferrin as a marker o f relapse in alcoholic patients. Alcoholism: Clinical and Experimental Research 19, 611-616.
Salaspuro M (1986) Conventional and coming laboratory markers o f alcoholism and heavy drinking. Alcoholism: Clinical and Experimental Research 10, 5s-12s.
Salaspuro M (1989) Characteristics o f laboratory markers in alcohol-related organ damage. Scandinavian Journal o f Gastroenterology 24, 769-780.
Seppa K, Laippala P and Saarni M (1991) Macrocytosis as a consequence of alcohol abuse among patients in general practice. Alcoholism: Clinical and Experimental Research 15, 871 - 876.
Sillanaukee P (1995) Brief intervention in primary health care. In: Lahti-project, Holmila M, ed., in press.
Stibler H (1991) Carbohydrate-deficient transferrin in serum: a new marker o f potentially harmful alcohol consumption reviewed. Clinical Chemistry 37, 2029-2037.
Suokas A (1992) B rief intervention of heavy drinking in primary health care: Hameenlinna study. University Printing House, Helsinki.
Unger KW and Johnson D Jr (1974) Red blood cell mean corpuscular volume; a potential indicator of alcohol usage in a working population. American Journal o f Medical Sciences 267,281-289.
Voltaire A, Beck O and Borg S (1992) Urinary 5-hydroxytryptophol: a possible m arker of recent alcohol consumption. Alcoholism: Clinical and Experimental Research 16, 281-285.
W atson RR, Mohs ME, Eskelson C, Sampliner RE and Hartmann B (1986) Identification of alcohol abuse and alcoholism with biological parameters. Alcoholism: Clinical and Experimental Research 10, 364-385.
Wu A, Chanarin I and Levi AJ (1974) Macrocytosis of chronic alcoholism. Lancet i, 829- 831.
Yersin B, Nicolet JF, Decrey H, Burnier M, van Melle G and Pecoud A (1995) Screening for excessive alcohol drinking. Comparative value of carbohydrate-deficient transferrin, gamma- glutamyltransferase, and mean corpuscular volume. Archives o f Internal Medicine 155, 1907- 1911.
- 2 2 2 -