kompetansegruppa for smertebehandling på sunnaas sykehus v/ tor s. haugstad, overlege, prof. dr....
TRANSCRIPT

SmertebehandlingKompetansegruppa for smertebehandling på
Sunnaas Sykehusv/ Tor S. Haugstad, overlege, prof. dr. med.
Tor S. Haugstad Columbia NY

Prevalence of Chronic Pain in Europe - by Country– Based on Complete Screener Data –
14 %
13 %
12 %
17 %
15 %
13 %
19 %
21 %
8 %
13 %
8 %
9 %
4 %
5 %
7 %
4 %
0 % 50 %
5 %
8 %
9 %
10 %
10 %
10 %
7 %
12 %
6 %
6 %
10 %
5 %
5 %
4 %
5 %
6 %
0 % 50 %
Severe
Moderate
Norway (n=2,018)
Poland (n=3,812)
Italy (n=3,849)
Belgium (n=2,451)
Finland (n=2,004)
Austria (n=2,004)
Sweden (n=2,563)
Netherlands (n=3,197)
Germany (n=3,832)
Israel (n=2,244)
Denmark (n=2,169)
Switzerland (n=2,083)
France (n=3,846)
UK (n=3,800)
Ireland (n=2,722)
Spain (n=3,801)
30%
27%
26%
23%
21%
19%
18%
18%
17%
17%
16%
16%
15%
13%
13%
11%
Overall Prevalence = 19% (n=46,394)
Moderate 13% Severe 6%
Tor S. Haugstad Columbia NY Breivik et al, 2006

Mechanism based division of chronic pain (IASP 2008)
Perifere nociceptive
Neuropathic Central non-nociceptive
inflammation/periferal mechanic tissue damage
Damage or affection of periferal/central nerve tissue
Central disturbance in pain processing in CNS (allodynia/hyperalgesia)
NSAID/opioid response
Responds to both periferal and central farmacological treatment
TCA and neurodrugs are most effective
Triggered by stress
Examples:OsteoarthritisRACancer pain
Examples:PolyneuropathyCentral post stroke painPain in MS
Examples:FibromyalgiaIBSCPP
Tor S. Haugstad Columbia NY

Tor S. Haugstad Columbia NY

CP – epidemiologi (1965-2004)Materiale fra EuropaPrevalens har økt til over 2.0 pr. 1000
levendefødteMindre diplegi, økt hemiplegiKognitive utfordringer 23 – 44
%Språkutfordringer 42 – 81 %Synsutfordringer 62 – 71
%Epilepsi 22 – 40 %Langvarige smertelidelser > 25 %
Tor S. Haugstad Columbia NY
Odding et al, 2006

Operativ behandling for skjelettdeformiteter
Kirurgisk behandling for skoliose aktuelt vedBekkenskjevetAffisert sittebalanseTrykksårSmerter når ribbebuen møter hoftebenet
Komplikasjoner i 25 % av tilfelleneVed luksasjoner/malformasjoner i hofteleddet
Fjerne toppen av lårbenet/avstive hoften/totalprotese
Tor S. Haugstad Columbia NY
Hasler, 2013Boldingh, 2014

Resultat av treningsprogramEffekten på smerte og tretthet (fatigue) hoa
voksne med CPSmertereduksjonBedring av energinivåetLivskvalitet bedretFor at effekten skal vare, må programmet gå
kontinuerlig
Tor S. Haugstad Columbia NY
Vogtle, 2013

Tor S. Haugstad Columbia NY
From the Paris School of Neurology to Somatocognitive Therapy
Clockwise from top:1. Charcot lecturing on hysterical
palsies2. Duchenne demonstrating electrical
stimulation of nerves controlling facial muscles
3. Freud developed psychoanalysis – from hysterical palsies to interpretation of dreams
4. Reich developed somatic psychology – ”body language” and ”muscular armor” as expression of psychological defence
5. Mensendieck teaching functional anatomy
6. Beck developed cognitive therapy – based on theory of dysfunctional cognitive schemata

Cognitive therapyDysfunctional cognitive schemata psychological
distressExample – the negative triade of depression:
negative thoughts of SelfWorldFuture
Therapeutic sessions divided in threeGo over experiences since last sessionWork with cognitive schemataNew assignments to be practiced until next
sessionTor S. Haugstad Columbia NY
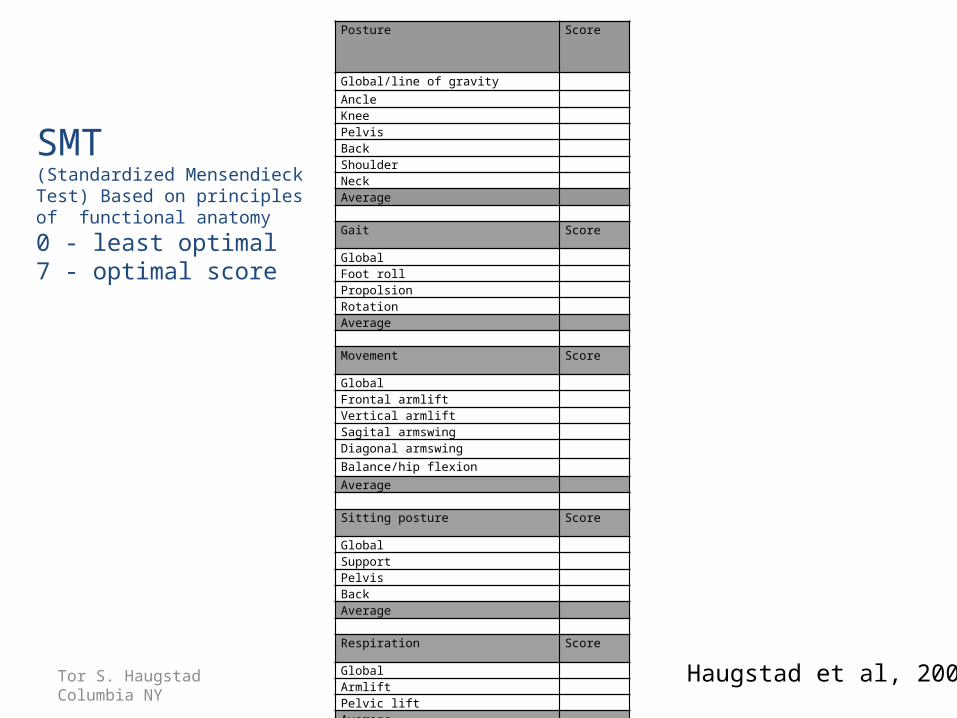
SMT(Standardized Mensendieck Test) Based on principles of functional anatomy
0 - least optimal 7 - optimal score
Tor S. Haugstad Columbia NY
Posture Score
Global/line of gravity
Ancle Knee Pelvis Back Shoulder Neck Average Gait Score
Global Foot roll Propolsion Rotation Average Movement Score
Global Frontal armlift Vertical armlift Sagital armswing Diagonal armswing
Balance/hip flexion
Average Sitting posture Score
Global Support Pelvis Back Average Respiration Score
Global Armlift Pelvic lift Average Haugstad et al, 2006

Somatocognitive therapy Builds on cognitive therapy
and theory Dr. Bess Mensendieck
worked with cognitive elements (1931) – cognitions control movement
Cognitive therapy later developed by Aaron Beck
Short term body oriented therapy - focused on the here and now and thoughts about movements
Likeworthy working alliance beween therapist and patient, built on empathy and dialouge
Body awareness through explorative treatment with functional goals - in daily life
Can be understood as a hybrid between physiotherapy and psychotherapy
3-phased lesson-1.What is learnt and
experienced since last time? In daily life?
2.Treatment- Learning new active movements – challenging dysfunctional thoughts. Work with these in daily activities, they will influence on the respiration, the body awareness, the circulation and the fear of movement
- manual massage that gives new tactile experiences- feel the difference between tension and relaxation
3. New assignments given - the therapy unfolds in the activities of daily living
Tor S. Haugstad Columbia NY

Longstanding pelvic pain - Chronic Pelvic Pain (CPP)Pain persisting in the lower
abdomen for a period exceeding 6 months
Excluded: Pain related to
menstruation only Or only to sex, Or only in the vulva
3.8% of all women between 15 – 73 years
By some authors classified as ICD-10 F45.4 – persistent somatoform pain disorder.
(Zondervan 2001, Grace 2004)
Tor S. Haugstad Columbia NY

The RCT study of women with CPP
60 women with CPP were recruited from the National Hospital, OUS
Pain was evaluated by means of a VAS on a scale from 0 - 10 before and after treatment and after one year
Psychometric assessment GHQ-30 before treatment and after one year
Evaluation of motor patterns with SMT before and after treatment and after one year (7 is optimal function, 0 is least optimal). The evaluator was blinded with respect to whether the SMT was before or after treatment, or after one year
Palpation of the muscles in the pelvic regionA clinical history/interview was taken before and after
treatment
Tor S. Haugstad Columbia NY

CPP - Description of the patientsAverage score for pain experience among the 60 women with
CPP was 6.01The mean age for all 60 were 31 y75 % of all of the 60 had moderate to strong pain under or
after intercourse50 % described the lower abdomen as swollen, and they have
difficulty wearing jeans due to allodynia
• 25 % told that the pain started after an infection in the bladder or in kidney region, or after an abortion
• The CPP patients in the study had previously performed in average two surgical prosedures each (explorative laparoscopies, resection of ovarian cysts, hysterctomy, extirpation of the adnexae, etc.).
Tor S. Haugstad Columbia NY

SMT – movement patterns after 3 months -and at 1 year follow up after therapy
Tor S. Haugstad Columbia NY

VAS after therapy and at 1 year follow up
Tor S. Haugstad Columbia NY

GHQ-30 - Psychological Distress before and 1 year after therapy
GHQ- 30 after 1 y:No change in the STGT group (slightly worse)
In the MSCT group significant improvement in the scores for anxiety (p=0.00) and coping (p=0.01), also improvement in the scores for depression (p=0.06)
Haugstad GK, Haugstad TS, Kirste UM, Leganger S, Malt UF. Continuing improvement of chronic pelvic pain in women after short-term Mensendieck somatocognitive therapy; results of a 1-y follow – up study Am J Obst Gyn 2008 ;199:615.e1-615.e8
Tor S. Haugstad Columbia NY

Comments from editor in American Journal of Gynecology & Obstetrics (2008)
Tor S. Haugstad Columbia NY

Provoked Vestibulodynia PVD
Tor S. Haugstad Columbia NY
• Affecting approximately 12 - 30 % of premenopausal women
• Described as a sharp or burning sensation at the vulvar vestibule
Erythema/hypersensitivity/allodynia of defined area of the vestibulum may occur
Dyspareunia, or painful sexual intercourse, is the most common complaint
May occur even in the absence of relevant visible findings.
(Moyal-Barracco & Lynch 2004, Goldfinger 2009)
Few RCT and follow – up studies;
1. Comparing EMG biofeedback and lidocaine gel – significant increases in vestibulare pain tresholds, quality of life, and sexual funcion (Danielsson 2006).
2. Compare vestibulectomy and group cognitive- behavior therapy and EMG biofeedback for treatment – all three significant pain reduction –after 2.5 y all three group continued to improve (Bergeron 2008).
3. Comparing Cognitve behavioral therapy and supportive Psychotherapy - the CAT group reported greater improvement (Masheb 2009).
PVD and somatocognitive therapy-A follow up study
Follow up study at the Oslo University CollegeNo studies have ever examine the movement
patterns in these patients with PVDPhysiotherapy students, under supervisionPatients were treated for 6 weeks; twice a
week, for 1 hour – 12 hours with somatocognitive therapy
In this study we have treated 25 patients Tested with SMT, VAS, GHQ – 30 and TAMPA
scale of Kinesofobia before and after somatocognitive treatment and after 6 months
Tor S. Haugstad Columbia NY

Some of the elements in somatocognitive treatment of PVD patients
Learning body awareness through; body tension and relaxation in daily movement new experiences of own respiration pattern
Be aware of vulva, get new sensations through; squeeze and relax the pelvic floor gently apply lotion to the vulva apply cold and warm cloths trying carefully the smallest tampon – after a while try
sex again if they have a partner
The patients try these small steps in between the therapy sessions, in the daily life, and share the experiences with therapist.
Tor S. Haugstad Columbia NY

SMT Respiration scores –before and after therapy
Tor S. Haugstad Columbia NY
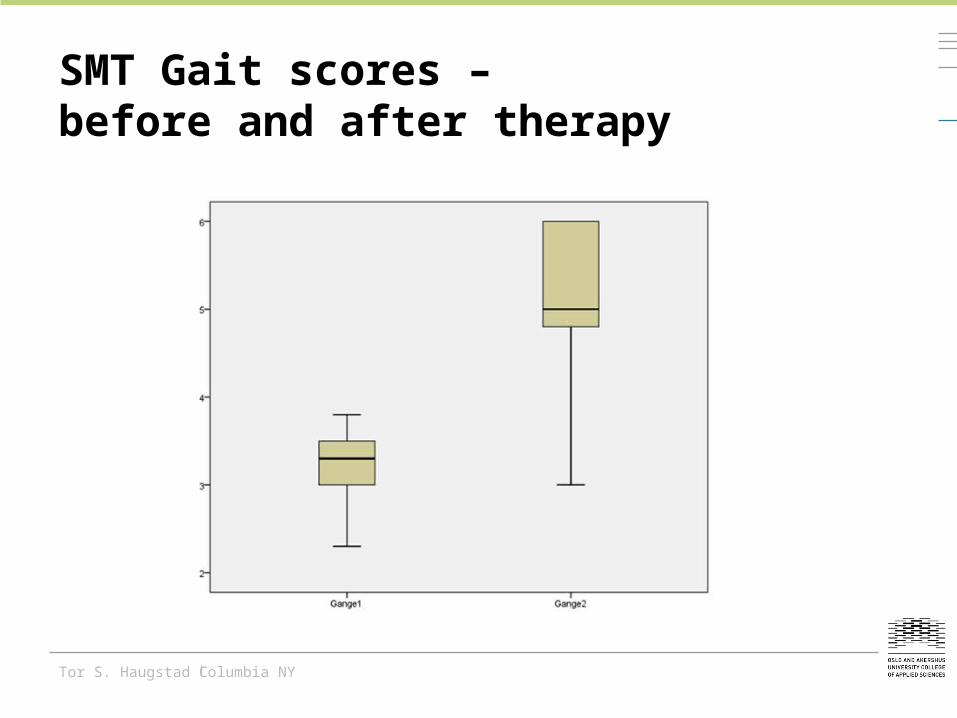
SMT Gait scores –before and after therapy
Tor S. Haugstad Columbia NY

Pain score before and after therapy
Before treatment After treatment After 6 months0123456789
108.75
5.04
1.88
VAS
Tor S. Haugstad Columbia NY

Psychological Distress – GHQ-30 andTAMPA Scale of Kinesophobia 6 months after therapy
GHQ – 30: significantly improved scores for anxiety and depression at 6 months follow up
TAMPA scale of kinesophobia: significantly reduced scores for fear of movement, and fear of pain at 6 months follow up
Tor S. Haugstad Columbia NY

CONCLUSION
Promising results using somatocognitive therapy for these gynecological patients with longstanding pain syndromes
More studies are needed, including other groups of patients (like low back pain, neck and shoulder pain, generalized pain, PTDS) using this new approach combining physiotherapy and psychotherapy
We need to understand the mechanisms behind the development of these longstanding pain syndromes, related to peripheral sensors, peripheral nerves and the central nervous system, as well as the mechanisms behind the effect of somatocognitive therapy
Tor S. Haugstad Columbia NY In lumine Tuo videbimus lumen

Konklusjon:
—Ved CP med langvarig smerte kan operasjon hjelpe i noen tilfeller
—Treningsprogrammer hjelper mot smerter og tretthet så lenge de holdes ved like
—Behandlingsprogrammer basert på innsiktsorienterte og kognitivt baserte teknikker bør utprøves
—Sunnaas har fokus på smertetilstander hos CP-pasienter
Tor S. Haugstad Columbia NY