knowledge-based treatment planning: an inter-technique and...
TRANSCRIPT

Physica Medica 36 (2017) 38–45
Contents lists available at ScienceDirect
Physica Medica
journal homepage: ht tp : / /www.physicamedica.com
Original paper
Knowledge-based treatment planning: An inter-technique and inter-system feasibility study for prostate cancer
http://dx.doi.org/10.1016/j.ejmp.2017.03.0021120-1797/� 2017 Associazione Italiana di Fisica Medica. Published by Elsevier Ltd. All rights reserved.
⇑ Corresponding author.E-mail addresses: [email protected] (E. Cagni), [email protected]
(A. Botti), [email protected] (R. Micera), [email protected] (M.Galeandro), [email protected] (R. Sghedoni), [email protected](M. Orlandi), [email protected] (C. Iotti), [email protected] (L. Cozzi),[email protected] (M. Iori).
Elisabetta Cagni a, Andrea Botti a,⇑, Renato Micera b, Maria Galeandro b, Roberto Sghedoni a, Matteo Orlandi a,Cinzia Iotti b, Luca Cozzi c, Mauro Iori a
aMedical Physics Unit, Department of Advanced Technology, Arcispedale Santa Maria Nuova, IRCCS, Reggio Emilia, ItalybRadiotherapy Unit, Department of Advanced Technology, Arcispedale Santa Maria Nuova, IRCCS, Reggio Emilia, ItalycRadiotherapy and Radiosurgery Department, Istituto Clinico Humanitas, Rozzano, Milan, Italy
a r t i c l e i n f o
Article history:Received 27 September 2016Received in Revised form 3 March 2017Accepted 7 March 2017Available online 17 March 2017
Keywords:Knowledge basedPlanning AutomationProstateRapidarcTomotherapy
a b s t r a c t
Purpose: Helical Tomotherapy (HT) plans were used to create two RapidPlan knowledge-based (KB) mod-els to generate plans with different techniques and to guide the optimization in a different treatmentplanning system for prostate plans. Feasibility and performance of these models were evaluated.Material and methods: two sets of 35 low risk (LR) and 30 intermediate risk (IR) prostate cancer cases whounderwent HT treatments were selected to train RapidPlan models. The KB predicted constraints wereused to perform new 20 KB plans using RapidArc technique (KB-RA) (inter-technique validation), andto optimise 20 new HT (KB-HT) plans in the Tomoplan (inter-system validation). For each validationmodality, KB plans were benchmarked with the manual plans created by an expert planner (EP).Results: RapidPlan was successfully configured using HT plans. The KB-RA plans fulfilled the clinicaldose-volume requirements in 100% and 92% of cases for planning target volumes (PTVs) and organs atrisk (OARs), respectively. For KB-HT plans these percentages were found to be a bit lower: 90% forPTVs and 86% for OARs. In comparison to EP plans, the KB-RA plans produced higher bladder doses forboth LR and IR, and higher rectum doses for LR. KB-HT and EP plans produced similar results.Conclusion: RapidPlan can be trained to create models by using plans of a different treatment modality.These models were suitable for generating clinically acceptable plans for inter-technique and inter-system applications. The use of KB models based on plans of consolidated technique could be useful witha new treatment modality.
� 2017 Associazione Italiana di Fisica Medica. Published by Elsevier Ltd. All rights reserved.
1. Introduction
Helical and volumetric arc-modulated RadioTherapy (VMAT)employ inverse planning processes that optimise the dose distribu-tion of arc-deliveries according to constraints set by planners ontreatment planning systems (TPS). Since the optimal achievabledosimetry is unknown at the beginning of the optimisation, theability of the planners is a primary factor to obtain a good plan.Moreover, each plan tailored to a specific patient generally requiresmany rounds of trial and error optimisation. Therefore, the finalresult is highly related to experience and planning time of theplanner or institution.
RapidPlanTM (Varian Medical Systems, Palo Alto, USA) is a com-mercially knowledge-based planning solution integrated in EclipseTPS that generates automated constraints based on a model trainedby libraries of specific plans. These models use the geometrical fea-tures of treatment plans included in the library to predict a rangeof achievable OARs DVHs for a new patient plan. Moreover, the sys-tem suggests a list of objectives and penalties to perform aknowledge-based (KB) optimisation process suitable for the opti-misation module of Eclipse. The RapidPlan was investigated andvalidated for clinical practice in several studies [1–8]. These studiesdemonstrated that RapidPlan can produce good quality plans whenemploying the same technique of the model library plans (VMATand fixed-gantry IMRT). It is important to use plans which haveconsistently high quality because the model is based on the meanvalues of dosimetric features of the majority of the training setplans. Therefore, few good plans in the training set are not enoughto obtain a model with good performances [9]. However, not in allinstitutes, a significant number of good quality plans are easily
E. Cagni et al. / Physica Medica 36 (2017) 38–45 39
available, for one particular anatomical region, technique andmodality; the number of patients treated in the institute and theexperience of the individual planner become critical factors, espe-cially when a new radiotherapy techniques are clinically intro-duced in the Institute. KB models, trained with plans createdfrom a consolidated different technique, should be useful to com-pensate for the lack of planning experience. This study investigatedthe potential of RapidPlan applied to different treatment tech-niques and optimisation systems: the capability of two prostatecancer models trained by HT plans to produce knowledge-basedRapidArc (KB-RA) plans and to predict the dosimetry of new HTplans (KB-HT) was tested.
2. Methods and materials
2.1. Knowledge based optimisation engine
RapidPlan was introduced in the Eclipse treatment planningsystem (Varian Medical Systems, Palo Alto, USA) from itsrelease13.5 [9]. In order to configure a model in RapidPlan, a setof geometric and dosimetric information are extracted from agroup of selected available treatment plans (N > 20). A combina-tion of Principal Component Analysis and regression techniques(PCA regression [10]) extracts the features that are used in theautomated model based dose volume objectives prediction tool(DVH estimation phase) [9]. In a second phase, called DVH Estima-tion, the DVH ranges for the structures defined in the model arepredicted for any new patient. These predicted DVH are specificfor the new patient anatomy derived from the features extractedin the model training. The optimization objectives, as line objec-tives, are created from the predicted DVH, following the lowerboundary of the estimate.
2.2. Model’s library
Two models were trained, employing HT prostate treatmentsplans: a model for low risk prostate cancer (LR), using 35 plansdelivering 70 Gy/28 fractions to prostate gland only, and a modelfor intermediate risk prostate cancer (IR) using 30 simultaneousintegrated boost (SIB) plans delivering 70 Gy to prostate gland(PTV1) and 56 Gy to proximal seminal vesicles (PTV2) in 28 frac-tions [11,12]. All the selected HT treatments plans were simulated
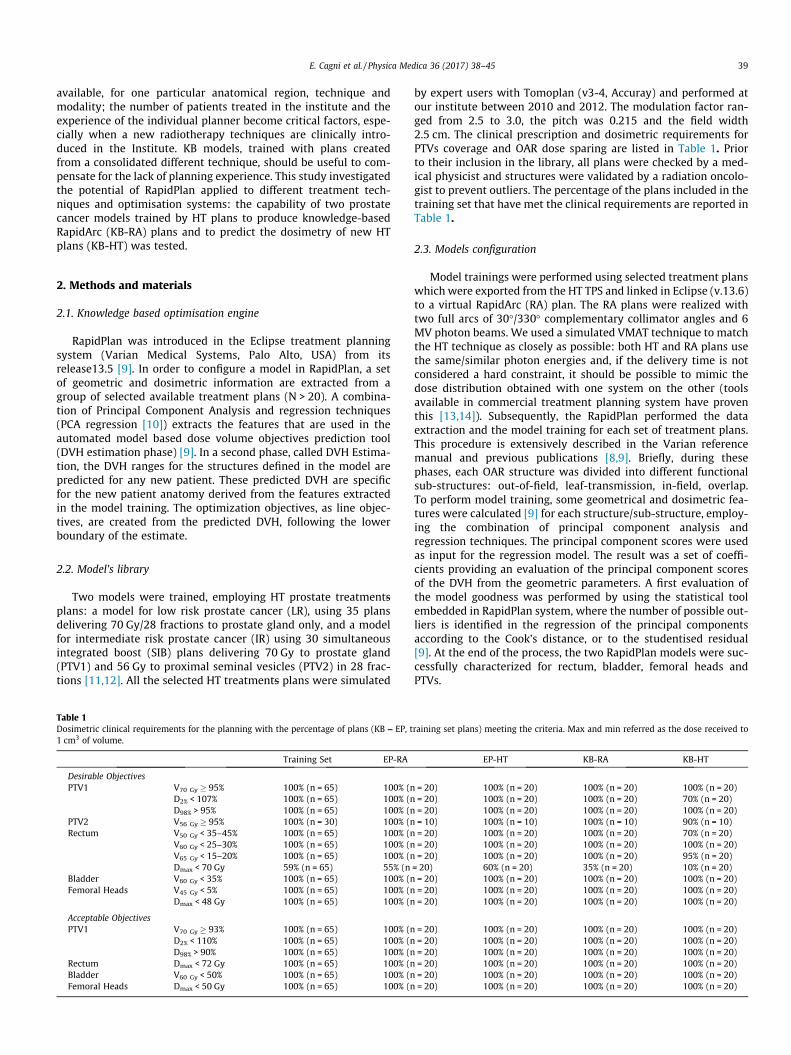
Table 1Dosimetric clinical requirements for the planning with the percentage of plans (KB – EP, t1 cm3 of volume.
Training Set EP-RA
Desirable ObjectivesPTV1 V70 Gy � 95% 100% (n = 65) 100% (n
D2% < 107% 100% (n = 65) 100% (nD98% > 95% 100% (n = 65) 100% (n
PTV2 V56 Gy � 95% 100% (n = 30) 100% (nRectum V50 Gy < 35–45% 100% (n = 65) 100% (n
V60 Gy < 25–30% 100% (n = 65) 100% (nV65 Gy < 15–20% 100% (n = 65) 100% (nDmax < 70 Gy 59% (n = 65) 55% (n
Bladder V60 Gy < 35% 100% (n = 65) 100% (nFemoral Heads V45 Gy < 5% 100% (n = 65) 100% (n
Dmax < 48 Gy 100% (n = 65) 100% (n
Acceptable ObjectivesPTV1 V70 Gy � 93% 100% (n = 65) 100% (n
D2% < 110% 100% (n = 65) 100% (nD98% > 90% 100% (n = 65) 100% (n
Rectum Dmax < 72 Gy 100% (n = 65) 100% (nBladder V60 Gy < 50% 100% (n = 65) 100% (nFemoral Heads Dmax < 50 Gy 100% (n = 65) 100% (n
by expert users with Tomoplan (v3-4, Accuray) and performed atour institute between 2010 and 2012. The modulation factor ran-ged from 2.5 to 3.0, the pitch was 0.215 and the field width2.5 cm. The clinical prescription and dosimetric requirements forPTVs coverage and OAR dose sparing are listed in Table 1. Priorto their inclusion in the library, all plans were checked by a med-ical physicist and structures were validated by a radiation oncolo-gist to prevent outliers. The percentage of the plans included in thetraining set that have met the clinical requirements are reported inTable 1.
2.3. Models configuration
Model trainings were performed using selected treatment planswhich were exported from the HT TPS and linked in Eclipse (v.13.6)to a virtual RapidArc (RA) plan. The RA plans were realized withtwo full arcs of 30�/330� complementary collimator angles and 6MV photon beams. We used a simulated VMAT technique to matchthe HT technique as closely as possible: both HT and RA plans usethe same/similar photon energies and, if the delivery time is notconsidered a hard constraint, it should be possible to mimic thedose distribution obtained with one system on the other (toolsavailable in commercial treatment planning system have proventhis [13,14]). Subsequently, the RapidPlan performed the dataextraction and the model training for each set of treatment plans.This procedure is extensively described in the Varian referencemanual and previous publications [8,9]. Briefly, during thesephases, each OAR structure was divided into different functionalsub-structures: out-of-field, leaf-transmission, in-field, overlap.To perform model training, some geometrical and dosimetric fea-tures were calculated [9] for each structure/sub-structure, employ-ing the combination of principal component analysis andregression techniques. The principal component scores were usedas input for the regression model. The result was a set of coeffi-cients providing an evaluation of the principal component scoresof the DVH from the geometric parameters. A first evaluation ofthe model goodness was performed by using the statistical toolembedded in RapidPlan system, where the number of possible out-liers is identified in the regression of the principal componentsaccording to the Cook’s distance, or to the studentised residual[9]. At the end of the process, the two RapidPlan models were suc-cessfully characterized for rectum, bladder, femoral heads andPTVs.
raining set plans) meeting the criteria. Max and min referred as the dose received to
EP-HT KB-RA KB-HT
= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 70% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 10) 100% (n = 10) 100% (n = 10) 90% (n = 10)= 20) 100% (n = 20) 100% (n = 20) 70% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 95% (n = 20)
= 20) 60% (n = 20) 35% (n = 20) 10% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)
= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)= 20) 100% (n = 20) 100% (n = 20) 100% (n = 20)

Table 2Summary of the KB-HT plan optimisation parameters. The pb value indicatesRapidplan DVH proposed constraint and/or penalty. DVH OARs point constraintswere extracted from the line proposed by Rapidplan, by fixing the dose values.
Structures Optimisation DVHconstraints
Penalty
D (Gy) V(%)
PTV1 67.2 100 13070 95 13070.7 0 130
PTV2 57 100 13056 95 13052.2 0 130
Rectum 20 pb pb506070
Bladder 20 pb pb456070
Right Fem Head Pb 50 pb0
Left Fem Head Pb 50 pb
40 E. Cagni et al. / Physica Medica 36 (2017) 38–45
2.4. KB plan performance evaluation
Forty patients not used for model training, that underwent clin-ical treatment in our Institute between 2010 and 2015, were retro-spectively randomly selected as evaluation groups to test theperformance of RapidPlan; 20 patients (10 LR and 10 IR) for HTtreatments (HT validation group) and 20 patients (10 LR and 10IR) for RA treatments (RA validation group). For each patient, thedefinitive plan that was clinically approved and selected for clinicaltreatment was considered as expert plans (EP). The percentage ofexpert plans, for both modalities, that fulfil the clinical require-ments were reported in Table 1. Prior to their inclusion in the val-idation groups, using the same modality of the training set, allpatients were checked to prevent outliers.
Two validation experiments were performed, (1) the inter-technique and (2) the inter-system validations. The inter-technique validation tested the ability of RapidPlan to generatenew RA plans using KB model based on HT plan technique. Theinter-system validation evaluated the performance of RapidPlanto produce a KB plan with different TPS (KB dose-volume con-straints applied to HT system optimisation). In both cases, a com-bination of different techniques (RA versus HT) and systems(Varian versus Accuray) were used to create KB plans. A schematicrepresentation of the two validation modalities is reported inFig. 1.
2.5. Inter-technique validation
New RapidArc knowledge based (KB-RA) plans were generatedfor each case of RA evaluation group with a single optimizationprocess and without any manual intervention. The KB-RA planswere then compared with the EP-RA plans. All the EP-RA and theKB-RA plans were calculated using the Acuros-XB algorithm witha grid dose resolution of 2.5 mm, Varian HD MLC collimator and2 full arcs of 6 MV photon beam and 30�/330� complementary col-limator angle. The jaw tracking application was used. The planswere normalized to 95% of the PTV1 volume.
2.6. Inter-system validation
New HT plans were created for each patient of the HT evalua-tion group using the KB information of the RapidPlan module
Fig. 1. Schematic workflow of the inter-technique and inter-system validations. A. Thedose distributions were imported in Eclipse (1) and simulated as 2 arcs RA plans. B. Twom(2). C. The predicted KB constraints were used in Eclipse (3) to generate KB-RA new plansconstraints were imported in Tomoplan (4) to guide the optimisation for new KB-HToptimized plans by an expert (EP-RA) (inter-technique validation); KB-HT were compar
(KB-HT). In detail, predicted DVHs for OARs were extracted fromthe RapidPlan model by simulating a RA plan with two full arcs.The proposed OARs DVH endpoints and penalties were set intoTomoplan before starting the optimisation process. The full dosecalculation was programmed after 100 iterations. All KB-HT planswere optimized in a single run without any manual interactionon the OARs constraints. The constraints and penalties used forKB-HT planning are listed in Table 2. Penalty and importance valueadjustments were done only for PTVs to overcome the trend ofRapidPlan to assign low priority to the target volume maximumdose. This corrective strategy was applied in order to obtain a clin-ical acceptable homogenous dose to the PTVs that otherwise wasnot reached. All the other proposed penalties were used withoutmodifications. The line constraints for OARs proposed by theRapidPlan were sampled in four DVH points suitable for the HToptimizer. In this version of Tomoplan, only dose-volume pointconstraints were allowed for OARs with a maximum number of 4for each organ. For rectum and bladder the DVH points were cho-sen in order to control the entire DVH during the optimisation over
training sets of 35HT and 30 HT plans for LR and IR respectively were selected. Theodels (one for LR and the other for IR) were built in RapidPlan using the training setsfor the evaluation group (10 LR and 10 IR prostate cancers). The same predicted KB
plans for the evaluation group. D. KB-RA plans were compared with manually RAed with EP-HT for inter-system validation.
E. Cagni et al. / Physica Medica 36 (2017) 38–45 41
a large range of doses (from low doses (i.e. 20 Gy) to maximumdoses (i.e. 70 Gy) while for Femoral Head only the portion ofDVH higher than D50% was managed. The KB-HT plans were com-pared with the EP-HT. All the HT plans were created using 6MVbeam energy and 2.5 cm field width. The modulation factor was2.8 for the KB-HT plans, while it was in the 2.8–3.0 range for theclinical EP-HT plans. For all plans, the dose calculation was madewith the fine grid (1.9 mm) and the prescription normalized to95% of the PTV1.
2.7. Plans evaluation
A comparison between predicted OARs models versus KB plansfor different DVH endpoints was performed for each risk group andfor each validation experiment. The considered DVH endpointswere: V70Gy, V60Gy, V50Gy and V20Gy for rectum and bladder, themaximum dose DMAX and the dose received by the 50% of the vol-ume (D50%) for femoral heads. All KB plans were evaluated for theirability to fulfil the plan acceptance criteria listed in Table 1 andcompared with EP plans.
As a second step, both sets of KB-plans were compared for theachieved target coverage and normal tissue dose sparing. The tar-get coverage and the target dose uniformity were quantified usingthe conformity index [15] and homogeneity index (HI). The HI isdefined as (D2 � D98)/Dp � 100, where D2 is the minimum doseto 2% of the PTV1, D98 is the minimum dose to the 98% of thePTV1, and Dp is the prescribed dose. Several dose-volume end-points were considered to compare the KB plans with the respec-tive benchmark (EP plans). These include: D98%, D50% and D2% forPTV1; D98% for PTV2; mean doses to individual OARs; V70Gy,V65Gy, V50Gy and V20Gy for rectum; V70Gy, V60Gy and V20Gy for blad-der; the DMAX for femoral heads.
Radiobiological indexes were also considered for comparisonswith the main aim to clinically evaluate the dosimetrical differencebetween plans. Normal Tissue Control probability (NTCP) [16] was
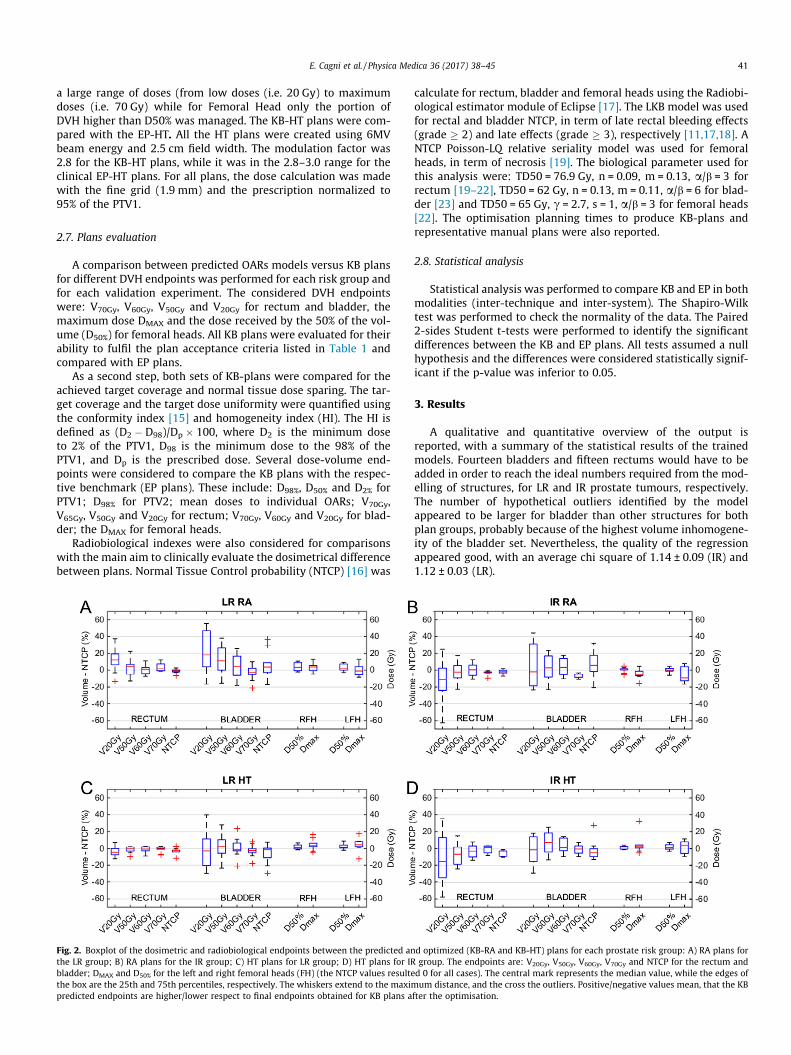
Fig. 2. Boxplot of the dosimetric and radiobiological endpoints between the predicted anthe LR group; B) RA plans for the IR group; C) HT plans for LR group; D) HT plans for IRbladder; DMAX and D50% for the left and right femoral heads (FH) (the NTCP values resultethe box are the 25th and 75th percentiles, respectively. The whiskers extend to the maximpredicted endpoints are higher/lower respect to final endpoints obtained for KB plans a
calculate for rectum, bladder and femoral heads using the Radiobi-ological estimator module of Eclipse [17]. The LKB model was usedfor rectal and bladder NTCP, in term of late rectal bleeding effects(grade � 2) and late effects (grade � 3), respectively [11,17,18]. ANTCP Poisson-LQ relative seriality model was used for femoralheads, in term of necrosis [19]. The biological parameter used forthis analysis were: TD50 = 76.9 Gy, n = 0.09, m = 0.13, a/b = 3 forrectum [19–22], TD50 = 62 Gy, n = 0.13, m = 0.11, a/b = 6 for blad-der [23] and TD50 = 65 Gy, c = 2.7, s = 1, a/b = 3 for femoral heads[22]. The optimisation planning times to produce KB-plans andrepresentative manual plans were also reported.
2.8. Statistical analysis
Statistical analysis was performed to compare KB and EP in bothmodalities (inter-technique and inter-system). The Shapiro-Wilktest was performed to check the normality of the data. The Paired2-sides Student t-tests were performed to identify the significantdifferences between the KB and EP plans. All tests assumed a nullhypothesis and the differences were considered statistically signif-icant if the p-value was inferior to 0.05.
3. Results
A qualitative and quantitative overview of the output isreported, with a summary of the statistical results of the trainedmodels. Fourteen bladders and fifteen rectums would have to beadded in order to reach the ideal numbers required from the mod-elling of structures, for LR and IR prostate tumours, respectively.The number of hypothetical outliers identified by the modelappeared to be larger for bladder than other structures for bothplan groups, probably because of the highest volume inhomogene-ity of the bladder set. Nevertheless, the quality of the regressionappeared good, with an average chi square of 1.14 ± 0.09 (IR) and1.12 ± 0.03 (LR).
d optimized (KB-RA and KB-HT) plans for each prostate risk group: A) RA plans forgroup. The endpoints are: V20Gy, V50Gy, V60Gy, V70Gy and NTCP for the rectum andd 0 for all cases). The central mark represents the median value, while the edges ofum distance, and the cross the outliers. Positive/negative values mean, that the KB
fter the optimisation.

42 E. Cagni et al. / Physica Medica 36 (2017) 38–45
Fig. 2 shows the differences between the predictions andachieved KB plans (predicted-achieved) in terms of dose endpointsand NTCP values of the RA and HT plans by using a box plot. Thevalues considered for the model constraints were the lowest valuesof the predicted range for the RapidArc plans. A positive differencemeans that the prediction provides higher values compared tothose obtained by the KB optimized plans. These differences wereextremely variable in both risk groups. In particular, for RA plans apositive median difference in bladder volume receiving more than20 Gy, 50 Gy and 60 Gy was evident. The NTCP for RA in bladdervolume have showed median positive difference (3.7 ± 16.6%,5.6 ± 14.5% for LR and IR respectively), in contrast for HT the NTCPresulted in a negative median value (-1.7 ± 11.2%, -5.2 ± 11.7% forLR and IR respectively). However, all the NTCP values for bladderpresented extremely large variability. For HT plans, significant dif-ferences were seen in femoral head DVH endpoints, as higher med-ian dose and distribution range. The corresponded NTCP values forfemoral heads resulted zero for all cases (thus these data were notreported in Fig. 2). For the rectum the NTCP difference resultedvery small with negative median value for all cases (for RA1.0 ± 2.5%, -1.9 ± 2.8% for LR and IR respectively; for HT -2.2 ± 3.6%, -3.1 ± 3.6% for LR and IR respectively).
All KB plans demonstrated the ability to achieve the clinicalrequirements (described in Table 1) for both RapidArc and HTtreatment modalities. In details, 100% (n = 70) and 92% (n = 180)of the primary endpoints were achieved by the KB-RA plans forPTVs and OARs, respectively. For the KB-HT plans, these percent-
Fig. 3. Average DVHs of target volumes and OARs that are obtained in the inter-systemanually optimized by the expert (EP), while the blue line indicates the plans optimize
ages were slightly lower, with 90% (n = 70) and 86% (n = 180) ofendpoints fulfilled for the targets and OARs, respectively. However,100% of acceptable endpoints were achieved for KB-RA and KB-HTplans. More details of this comparison are reported in Table 1.
Fig. 3 shows the average comparison of PTVs and OARs DVHs,between the KB and EP plans for the inter-technique and inter-system validations. Corresponding ranges (±1 SD) are also plotted.For both risk groups, the PTV1 DVHs did not differ significantly. Alarger range was found for PTV2 s probably because of their lowervolume. Regarding the OARs, the EP-RA plan data showed a sys-tematic tendency to spare the bladder and, moderately, the rectumfor the inter-technique validation, while KB-HT plans showed amodest but systematic tendency to better spare the rectum inthe LR group of the inter-system case; this tendency is invertedin the IR group. Similar DVH shapes were obtained for the femoralheads.
Table 3 summarizes the quantitative analysis over the entirecohort of patients for the two validation modalities. Mean differ-ences between the KB and EP plans (in term of KB plans -EP plans).together with the SD and ranges were displayed Statistical p valueswere also reported (normal distribution of data was assessed andconfirmed by means for the Shapiro-Wilk test for all sets – signif-icant differences were indicated with (⁄)).
The inter-technique validation tests documented significantendpoint differences in OARs for both LR and IR groups. The rectumdose was found to be significantly higher in KB plans only in the LRgroup. For bladder, KB plans lead to endpoint values higher than EP
m and inter-technique validation experiments. The red line represents the plansd with RapidPlan (KBP).
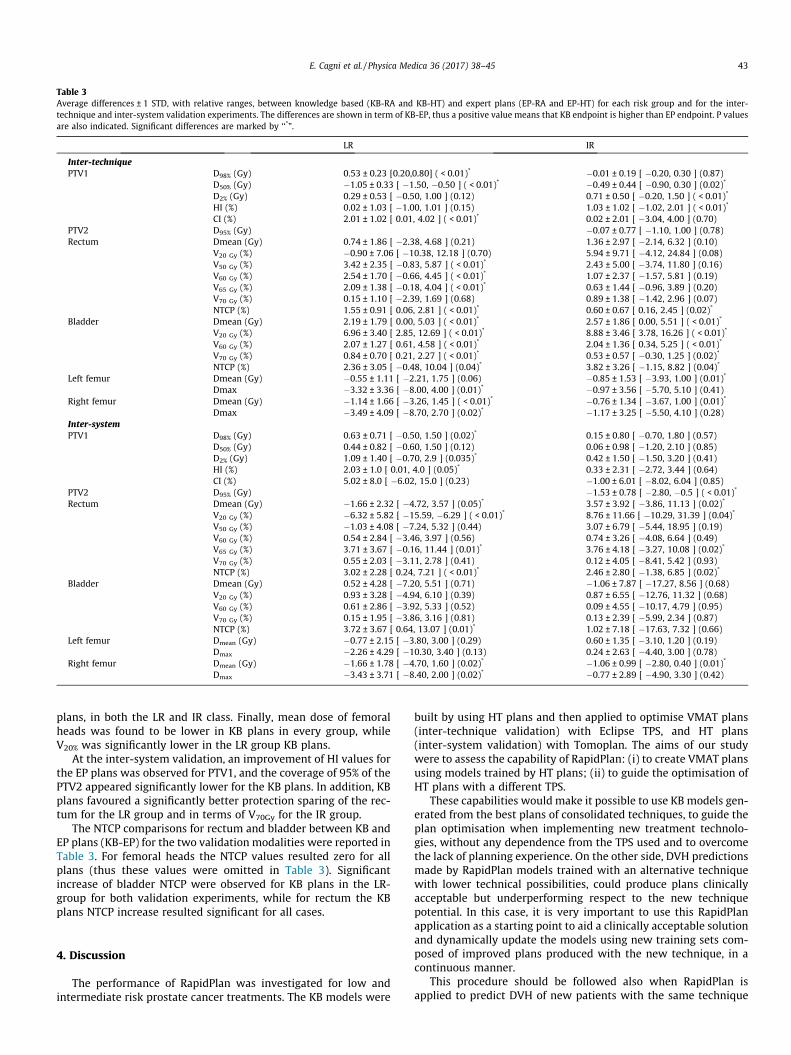
Table 3Average differences ± 1 STD, with relative ranges, between knowledge based (KB-RA and KB-HT) and expert plans (EP-RA and EP-HT) for each risk group and for the inter-technique and inter-system validation experiments. The differences are shown in term of KB-EP, thus a positive value means that KB endpoint is higher than EP endpoint. P valuesare also indicated. Significant differences are marked by ‘‘*”.
LR IR
Inter-techniquePTV1 D98% (Gy) 0.53 ± 0.23 [0.20,0.80] ( < 0.01)* �0.01 ± 0.19 [ �0.20, 0.30 ] (0.87)
D50% (Gy) �1.05 ± 0.33 [ �1.50, �0.50 ] ( < 0.01)* �0.49 ± 0.44 [ �0.90, 0.30 ] (0.02)*
D2% (Gy) 0.29 ± 0.53 [ �0.50, 1.00 ] (0.12) 0.71 ± 0.50 [ �0.20, 1.50 ] ( < 0.01)*
HI (%) 0.02 ± 1.03 [ �1.00, 1.01 ] (0.15) 1.03 ± 1.02 [ �1.02, 2.01 ] ( < 0.01)*
CI (%) 2.01 ± 1.02 [ 0.01, 4.02 ] ( < 0.01)* 0.02 ± 2.01 [ �3.04, 4.00 ] (0.70)PTV2 D95% (Gy) �0.07 ± 0.77 [ �1.10, 1.00 ] (0.78)Rectum Dmean (Gy) 0.74 ± 1.86 [ �2.38, 4.68 ] (0.21) 1.36 ± 2.97 [ �2.14, 6.32 ] (0.10)
V20 Gy (%) �0.90 ± 7.06 [ �10.38, 12.18 ] (0.70) 5.94 ± 9.71 [ �4.12, 24.84 ] (0.08)V50 Gy (%) 3.42 ± 2.35 [ �0.83, 5.87 ] ( < 0.01)* 2.43 ± 5.00 [ �3.74, 11.80 ] (0.16)V60 Gy (%) 2.54 ± 1.70 [ �0.66, 4.45 ] ( < 0.01)* 1.07 ± 2.37 [ �1.57, 5.81 ] (0.19)V65 Gy (%) 2.09 ± 1.38 [ �0.18, 4.04 ] ( < 0.01)* 0.63 ± 1.44 [ �0.96, 3.89 ] (0.20)V70 Gy (%) 0.15 ± 1.10 [ �2.39, 1.69 ] (0.68) 0.89 ± 1.38 [ �1.42, 2.96 ] (0.07)NTCP (%) 1.55 ± 0.91 [ 0.06, 2.81 ] ( < 0.01)* 0.60 ± 0.67 [ 0.16, 2.45 ] (0.02)*
Bladder Dmean (Gy) 2.19 ± 1.79 [ 0.00, 5.03 ] ( < 0.01)* 2.57 ± 1.86 [ 0.00, 5.51 ] ( < 0.01)*
V20 Gy (%) 6.96 ± 3.40 [ 2.85, 12.69 ] ( < 0.01)* 8.88 ± 3.46 [ 3.78, 16.26 ] ( < 0.01)*
V60 Gy (%) 2.07 ± 1.27 [ 0.61, 4.58 ] ( < 0.01)* 2.04 ± 1.36 [ 0.34, 5.25 ] ( < 0.01)*
V70 Gy (%) 0.84 ± 0.70 [ 0.21, 2.27 ] ( < 0.01)* 0.53 ± 0.57 [ �0.30, 1.25 ] (0.02)*
NTCP (%) 2.36 ± 3.05 [ �0.48, 10.04 ] (0.04)* 3.82 ± 3.26 [ �1.15, 8.82 ] (0.04)*
Left femur Dmean (Gy) �0.55 ± 1.11 [ �2.21, 1.75 ] (0.06) �0.85 ± 1.53 [ �3.93, 1.00 ] (0.01)*
Dmax �3.32 ± 3.36 [ �8.00, 4.00 ] (0.01)* �0.97 ± 3.56 [ �5.70, 5.10 ] (0.41)Right femur Dmean (Gy) �1.14 ± 1.66 [ �3.26, 1.45 ] ( < 0.01)* �0.76 ± 1.34 [ �3.67, 1.00 ] (0.01)*
Dmax �3.49 ± 4.09 [ �8.70, 2.70 ] (0.02)* �1.17 ± 3.25 [ �5.50, 4.10 ] (0.28)Inter-systemPTV1 D98% (Gy) 0.63 ± 0.71 [ �0.50, 1.50 ] (0.02)* 0.15 ± 0.80 [ �0.70, 1.80 ] (0.57)
D50% (Gy) 0.44 ± 0.82 [ �0.60, 1.50 ] (0.12) 0.06 ± 0.98 [ �1.20, 2.10 ] (0.85)D2% (Gy) 1.09 ± 1.40 [ �0.70, 2.9 ] (0.035)* 0.42 ± 1.50 [ �1.50, 3.20 ] (0.41)HI (%) 2.03 ± 1.0 [ 0.01, 4.0 ] (0.05)* 0.33 ± 2.31 [ �2.72, 3.44 ] (0.64)CI (%) 5.02 ± 8.0 [ �6.02, 15.0 ] (0.23) �1.00 ± 6.01 [ �8.02, 6.04 ] (0.85)
PTV2 D95% (Gy) �1.53 ± 0.78 [ �2.80, �0.5 ] ( < 0.01)*
Rectum Dmean (Gy) �1.66 ± 2.32 [ �4.72, 3.57 ] (0.05)* 3.57 ± 3.92 [ �3.86, 11.13 ] (0.02)*
V20 Gy (%) �6.32 ± 5.82 [ �15.59, �6.29 ] ( < 0.01)* 8.76 ± 11.66 [ �10.29, 31.39 ] (0.04)*
V50 Gy (%) �1.03 ± 4.08 [ �7.24, 5.32 ] (0.44) 3.07 ± 6.79 [ �5.44, 18.95 ] (0.19)V60 Gy (%) 0.54 ± 2.84 [ �3.46, 3.97 ] (0.56) 0.74 ± 3.26 [ �4.08, 6.64 ] (0.49)V65 Gy (%) 3.71 ± 3.67 [ �0.16, 11.44 ] (0.01)* 3.76 ± 4.18 [ �3.27, 10.08 ] (0.02)*
V70 Gy (%) 0.55 ± 2.03 [ �3.11, 2.78 ] (0.41) 0.12 ± 4.05 [ �8.41, 5.42 ] (0.93)NTCP (%) 3.02 ± 2.28 [ 0.24, 7.21 ] ( < 0.01)* 2.46 ± 2.80 [ �1.38, 6.85 ] (0.02)*
Bladder Dmean (Gy) 0.52 ± 4.28 [ �7.20, 5.51 ] (0.71) �1.06 ± 7.87 [ �17.27, 8.56 ] (0.68)V20 Gy (%) 0.93 ± 3.28 [ �4.94, 6.10 ] (0.39) 0.87 ± 6.55 [ �12.76, 11.32 ] (0.68)V60 Gy (%) 0.61 ± 2.86 [ �3.92, 5.33 ] (0.52) 0.09 ± 4.55 [ �10.17, 4.79 ] (0.95)V70 Gy (%) 0.15 ± 1.95 [ �3.86, 3.16 ] (0.81) 0.13 ± 2.39 [ �5.99, 2.34 ] (0.87)NTCP (%) 3.72 ± 3.67 [ 0.64, 13.07 ] (0.01)* 1.02 ± 7.18 [ �17.63, 7.32 ] (0.66)
Left femur Dmean (Gy) �0.77 ± 2.15 [ �3.80, 3.00 ] (0.29) 0.60 ± 1.35 [ �3.10, 1.20 ] (0.19)Dmax �2.26 ± 4.29 [ �10.30, 3.40 ] (0.13) 0.24 ± 2.63 [ �4.40, 3.00 ] (0.78)
Right femur Dmean (Gy) �1.66 ± 1.78 [ �4.70, 1.60 ] (0.02)* �1.06 ± 0.99 [ �2.80, 0.40 ] (0.01)*
Dmax �3.43 ± 3.71 [ �8.40, 2.00 ] (0.02)* �0.77 ± 2.89 [ �4.90, 3.30 ] (0.42)
E. Cagni et al. / Physica Medica 36 (2017) 38–45 43
plans, in both the LR and IR class. Finally, mean dose of femoralheads was found to be lower in KB plans in every group, whileV20% was significantly lower in the LR group KB plans.
At the inter-system validation, an improvement of HI values forthe EP plans was observed for PTV1, and the coverage of 95% of thePTV2 appeared significantly lower for the KB plans. In addition, KBplans favoured a significantly better protection sparing of the rec-tum for the LR group and in terms of V70Gy for the IR group.
The NTCP comparisons for rectum and bladder between KB andEP plans (KB-EP) for the two validation modalities were reported inTable 3. For femoral heads the NTCP values resulted zero for allplans (thus these values were omitted in Table 3). Significantincrease of bladder NTCP were observed for KB plans in the LR-group for both validation experiments, while for rectum the KBplans NTCP increase resulted significant for all cases.
4. Discussion
The performance of RapidPlan was investigated for low andintermediate risk prostate cancer treatments. The KB models were
built by using HT plans and then applied to optimise VMAT plans(inter-technique validation) with Eclipse TPS, and HT plans(inter-system validation) with Tomoplan. The aims of our studywere to assess the capability of RapidPlan: (i) to create VMAT plansusing models trained by HT plans; (ii) to guide the optimisation ofHT plans with a different TPS.
These capabilities would make it possible to use KB models gen-erated from the best plans of consolidated techniques, to guide theplan optimisation when implementing new treatment technolo-gies, without any dependence from the TPS used and to overcomethe lack of planning experience. On the other side, DVH predictionsmade by RapidPlan models trained with an alternative techniquewith lower technical possibilities, could produce plans clinicallyacceptable but underperforming respect to the new techniquepotential. In this case, it is very important to use this RapidPlanapplication as a starting point to aid a clinically acceptable solutionand dynamically update the models using new training sets com-posed of improved plans produced with the new technique, in acontinuous manner.
This procedure should be followed also when RapidPlan isapplied to predict DVH of new patients with the same technique

44 E. Cagni et al. / Physica Medica 36 (2017) 38–45
and system of the training sets. In fact, the KB training is an itera-tive circular process that aims to produce high quality of KB plansthat could be used as a input plan for a new KB model.
Our results documented that RapidPlan system allows to trainpredictive models, even if by using plans generated with otherTPS and for other techniques, and creates clinically acceptable RAplans, with an overall quality level similar to the EP plans. How-ever, some exceptions have been observed. In the inter-techniquevalidation experiment, the comparison of the RapidPlan predictedDVHs with the final KB plan DVHs showed some differences(Fig. 2). In details, for the bladder the predicted values (in termof DVHs and NTCP) were found to be systematically higher thanthe KB-RA DVHs for both LR and IR groups (Fig. 2). This could becaused by the delivery characteristic of the HT plans that, with afixed field with of 2.5 cm and a pitch of 0.215, produced a lowercranio-caudal dose gradient in comparison with RA technique per-formed with HDMLC and jaw tracking. This delivery features led toHT higher bladder volumes receiving higher mean doses. Conse-quently, the constraints derived from the model and applied toKB plans were not very restrictive for the RA technique. A quanti-tative analysis confirmed the significant under-performance of KB-RA plans in the bladder dose sparing for different endpoints (20 Gy,60 Gy and 70 Gy) in both risks groups (Table 3) respect to clinicalplans. The NTCP values reported the same behaviour and showedpositive mean values. Because of this, we think that the model per-formance to produce high-quality RA plans could be partially lim-ited. In the LR group, KB-RA plans were related to significantlyhigher rectal volumes receiving 50 Gy, 60 Gy and 65 Gy, as wellas NTCP values. Again, these results could be related to the deliverydifferences of the two treatment modalities. On the other hand, forIR no significant differences were observed between KB and EPplans. Our explanation is that in IR prostate cancer the inclusionof seminal vesicles made the beam-eyes-view of RA larger andincluding almost all rectum length, therefore, the rectum dose dis-tribution was not influenced by the dose-gradient shapes related tothe delivery technique.
Published studies have showed that, although VMAT and HTproduced very similar plans, HT generally resulted in more homo-geneous distributions, but also produced higher integral doses[24,25]. In particular, in the study of Davidson et al. [25] theauthors found that although HT resulted in a slightly higher inte-gral dose and mean doses to the OARs, it yielded a lower maximumdose to all OAR examined in the prostate cancer patients includedin the planning study. In a recent study, We et al. [26], used asupine VMAT RapidPlan model to optimise IMRT plans of otherpatient setup orientations for rectal cancer cases. In their conclu-sions, a model trained on a technique and orientation can be usedfor another and KB plans improved organ sparing and quality con-sistency. However, the target-objectives defined for VMAT-optimizer should be readapted to IMRT planning, followed by man-ual hot spot processing.
The NTCP differences observed in the KB-EP comparisonshowed the same behaviour of the dosimetric endpoints for rectumand bladder. In detail, significant NTCP increment in the KB planswere observed for both experiments, with all mean values lessthan 4%. The only case no statistically significant was the bladderNTCP difference for IR group in the inter-system modality.
Recent studies have confirmed that reliable predictive modelsof urinary toxicity are challenging, especially due to the complexityof symptoms, to their evolution with time and their strong depen-dence on baseline characteristics and pre-radiotherapy urinaryfunctionality [21]. Currently, no quantitative models are availablein the literature that satisfactorily describe the observed seriouslate bladder toxicity after radiotherapy, given the lack of a cleardose response for whole-bladder toxicity [27]. More generally, sev-eral studies have showed as the most important toxicity depends
on the fraction of the bladder included in the high doses [21]. Ifwe considered V60 Gy as the better indicator for bladder toxicityin this study, significant underperformances of KB plans wereobserved in the inter-technique validation for both risk groups,with a mean value around 2%. For inter-system experiment, no sig-nificant difference in the V60 Gy for bladder was observed instead.
The DVHs predicted by RapidPlan confirmed its ability to guidethe optimisation in HT TPS (inter-system validation). In fact, theKB-HT respected most of the primary clinical requirements. Somefailures were observed only in the PTV1 and high doses rectumareas. In contrast, significantly lower mean rectal dose wasobserved in the LR group.
The dose distribution has been easily improved with a manualtouch-up or by increasing the penalties of these endpoints duringthe optimisation phase. We believe that the introduction of manualtouch-up after KB optimisation could, in principle, eliminate theobserved bias between KB-HT and EP-HT plans, and more generallybetween KB and EP. However, such investigations were outside thescope of this paper.
Our models validations were performed following an open loop[7] approach for both planning techniques. Close loop validationwas already performed in previous studies [7,11]. The performanceof RapidPlan models for the intra-technique (IMRT (models) vs. RA(plans)) prostate planning was investigated by Fogliata et al. [7].
The inter-technique KB application was previously studied bythe group of Duke University [28] using a theoretical model forhead and neck cancer, similar to Rapidplan. This study evaluatedthe potential of a fixed gantry IMRT model to aid IMRT planningand to predict achievable DVHs with HT. The authors found thatan IMRT fixed gantry model could accurately predict the mediandose of the parotid gland in HT plans. However, that study didnot address the opposite experiment (using HT model to predictIMRT DVHs) and the inter-system application was not investigated,thus a direct comparison with our results it is not possible.
An important point is the fast and easy realisation of a highquality plan when using RapidPlan, without using trial and errorprocedures. As an estimate of the planning time, the generationof the estimated DVHs and the related objectives from the modeltakes less than 1–2 min compared to the common time neededto prepare all the dose volume constraints, that could be of severalminutes [8,29]. The optimization time of the RapidPlan plans wastypically 10 min for prostate case. Similarly, the possibility to usecustom KB objectives for the optimization process of TomoPlanallows to obtain a clinical acceptable solution into 100 iterationsrespect to the 400–500 generally used in a manual trial and errorprocess.
As a feasibility study of the RapidPlan for the inter-techniqueand inter-system application, our models were built using a med-ium size cohort of patient taken from a single institution (35 casesfor LR and 30 for IR). In a recent study [30] the influence of thetraining set size on the accuracy of KB models was investigatedfor the prostate cancer using in one case an approach similar toRapidPlan. The authors concluded that 30 samples were neededto accurately predict the bladder and rectum DVH points (D30 –D50). However, this number depends on the plan quality trainingdata set and on the specific model and endpoint to be predicted.The differences observed in this study between HT and RA seemto be not depended on the lack of statistic of the training data setsbut on a physically difference of the delivered dose distributionbetween the two techniques.
The low and intermediate risk prostate cases present few chal-lenges respect to others more complex cases (i.e. prostate withlimphonodes, head and neck): a small number of OARs (rectum,bladder and femoral heads), a limited number of targets (prostategland, seminal vesicles) and dose prescription levels (whichreaches a maximum number of two for IR), a low variability of

E. Cagni et al. / Physica Medica 36 (2017) 38–45 45
the target size and location respect to the OARs. As a feasibilitystudy of these applications, this treatment cohort was intentionallychosen because it represents a good starting point for testing theRapidPlan capabilities in terms of inter-technique and inter-system validation experiments. Deeper evaluation with more com-plex cases and models built with heterogeneous population interm of dose prescription, is advisable for the generalized interpre-tation of the results. However, in the complex cases, the capabilityof HT to obtain very good performance in term of dose distributioncould avoid the problems related to the cranio-caudal gradientobserved in the low risk prostate cases.
Finally, it must be considered that the quality of the generateddose distribution is dependent on the skills and experience of theplanner, and on allocated time. It is extremely difficult to assesswhether a generated plan is indeed optimal for the unique anat-omy of the individual patient. The prediction accuracy of RapidPlanin this study was investigated using manual plans for both trainingset and benchmarking in the evaluation sets, thus with a possibleimpact plan quality variations related to manual planning. A morerobust analysis should be done using Pareto optimal plans, gener-ated with automated prioritized multi-criteria treatment plan opti-mization, and therefore considered as an unbiased ground truth ofachievable plan quality.
5. Conclusion
RapidPlan was successfully configured by using clinical prostateHT plans and it has proved to be capable of predicting DVHs plan-ning. All the KB plans were clinically acceptable. However, thebladder dose distribution in KB-RA plans seemed to be influencedby the HT modality employed to create the models. A minimaloptimisation touch-up was necessary to achieve the same qualityas EP plans. Therefore, we consider RapidPlan as capable of sup-porting prostate cancer planning for both inter-technique andinter-system solutions. These applications will be particular usefulespecially for clinics in which new modality are activated in orderto supply for the lack of experience.
Conflict of interest notification
Luca Cozzi acts as Scientific Advisor to Varian Medical Systemsand is Clinical Research Scientist at Humanitas Cancer Center. Allother co-authors have no conflicts of interest.
Acknowledgement
Authors are grateful to Francesca Attanasi and Mirco Acerbi,Varian Medical System Team, for the support and cooperation.
References
[1] Chanyavanich V, Das S, Lee W, Lo W. Knowledge based IMRT treatmentplanning for prostate cancer. Med Phys 2011;38:2515–22.
[2] Zhu X, Ge Y, Li T, Thongphiew D, Yin FF, Wu J. A planning quality evaluationtool for prostate adaptive IMRT based on machine learning. Med Phys2011;38:719–26.
[3] Yuan L, Ge Y, Lee W, Yin FF, Kirkpatrick J, Wu J. Quantitative analysis of thefactors which affect the inter-patient organ-at risk dose sparing variation inIMRT plans. Med Phys 2012;39:6868–78.
[4] Good D, Lo J, Lee R, Wu J, Yin FF, Das S. A knowledge based approach toimproving and homogenizing intensity modulated radiation therapy planningquality among treatment centers: an example application to prostate cancerplanning. Int J Radiat Oncol Biol Phys 2013;87:176–81.
[5] Moore K, Brame RS, Low D, Mutic S. Experience based quality control of clinicalintensity modulated radiotherapy planning. Int J Radiat Oncol Biol Phys2011;81:545–51.
[6] Appenzoller L, Michalski J, Thorstad W, Mutic S, Moore K. Predicting dosevolume histograms for organs-at-risk in IMRT planning. Med Phys2012;39:7446–61.
[7] Fogliata A, Belosi F, Clivio A, Navarria P, Nicolini G, Scorsetti M, et al. On thepre-clinical validation of a commercial model-based optimization engine:application to volumetric modulated arc therapy for patients with lung orprostate cancer. Radiother Oncol 2014;113:385–91.
[8] Fogliata A, Wang P, Belosi F, Clivio A, Nicolini G, Vanetti E, et al. Assessment ofa model based optimization engine for volumetric modulated arc therapy forpatients with advanced hepatocellular cancer. Radiat Oncol 2014;9:236.
[9] Eclipse Photon and Electron reference guide v.13.7, Varian Medical System,June 2015, https://www.myvarian.com.
[10] Hastie T, Tibshirani R, Friedman J. The Elements of Statistical Learning: DataMining, Inference, and Prediction. Second edition. Springer. February 2009.
[11] Dal Pra A, Souhami L. Prostate cancer radiation therapy: a physician’sperspective. Physica Med 2016;32(3):438–45.
[12] McVicar N, Popescu IA, Heath E. Techniques for adaptive prostateradiotherapy. Physica Med 2016;32(3):492–8.
[13] Petersson K, Ceberg C, Engstrom P, Knoos T. Beam commissioning andmeasurements validating the beam model in a new TPS that converts helicalTomotherapy plans to step-and-shoot IMRT plans. Med Phys 2011;38:40–6.
[14] Petersson K, Ceberg C, Engstrom P, Benedek H, Nilsson P, Knoos T. Conversionof helical tomotherapy plans to step-and-shoot IMRT plans – Pareto frontevaluation of plans from a new treatment planning system. Med Phys2011;38:3130–8.
[15] Nakamura JL, Verhey LJ, Smith V, et al. Dose conformity of gamma kniferadiosurgery and risk factor for complications. Int J Radiat Oncol Biol Phys2001;51:1313–9.
[16] Lyman JT. Complication probability as assessed from dose–volume histograms.Radiat Res 1985;104:S13–9.
[17] Biological Optimization, Biological Evaluation and Conformal OptimizationInstructions for Use. v.13.7, Varian Medical System, June 2015, https://www.myvarian.com.
[18] Stavrev P, Ruggieri R, Stavreva N, Naccarato S, Alongi F. Applyingradiobiological plan ranking methodology to VMAT prostate SBRT. PhysicaMed 2016;32(4):636–41.
[19] Coates J, El Naqa I. Outcome modeling techniques for prostate cancerradiotherapy: Data, models, and validation. Physica Med 2016;32(3):512–20.
[20] Cicchetti A, Rancati T, Ebert M, Fiorino C, Palorini F, Kennedy A, Joseph D.J.,Denham J.W., et al. Modelling late stool frequency and rectal pain after radicalradiotherapy in prostate cancer patients: Results from a large pooledpopulation. Phys. Medica 2016;32(12):1690–7.
[21] Landoni V, Fiorino C, Cozzarini C, Sanguineti G, Valdagni R, Rancati T.Predicting toxicity in radiotherapy for prostate cancer. Physica Med 2016;32(3):521–32.
[22] Azzeroni R, Maggio A, Fiorino C, Mangili P, Cozzarini C, De Cobelli F, et al.Biological optimization of simultaneous boost on intra-prostatic lesions (DILs):sensitivity to TCP parameters. Physica Med 2013;29:592–8.
[23] Dale E, Hellebust TP, Skjønsberg A, Høgberg T, Olsen DR. Modeling normaltissue complication probability from repetitive computed tomography scansduring fractionated high-dose-rate brachytherapy and external beamradiotherapy of the uterine cervix. Int J Radiat Oncol Biol Phys. 32 2000;47(4):963–971.
[24] Iori M, Cattaneo GM, Cagni E, et al. Dose–volume and biological-model basedcomparison between helical tomotherapy and (inverse-planned) IMAT forprostate tumours. Radiother Oncol 2008;88:34–45.
[25] Davidson MT, Blake SJ, Batchelar DL, et al. Assessing the role of volumetricmodulated arc therapy (VMAT) relative to IMRT and helical tomotherapy inthe management of localized, locally advanced, and post-operative prostatecancer. Int J Radiat Oncol Biol Phys 2011;80:1550–8.
[26] Wu H, Jiang F, Yue H, Zhang H, Wang K, Zhang Y. Applying a RapidPlan modeltrained on a technique and orientation to another: a feasibility and dosimetricevaluation. Radiat Oncol 2016 Aug 18;11(1):108. http://dx.doi.org/10.1186/s13014-016-0684-9.
[27] Akila N. Viswanathan, Ellen D. Yorke, Lawrence B. Marks, Patricia J. Eifel,William U. Shipley. Radiation Dose-Volume Effects Of The Urinary Bladder Int JRadiat Oncol Biol Phys. PMC 2013 Mar 5.
[28] Lian J, Yuan L, Ge Y, Chera B, Yoo D, Chang S, et al. Modeling the dosimetry oforgan-at-risk in head and neck IMRT planning: an inter-technique and inter-institutional study. Med Phys 2013;40:121704.
[29] Tol J, Delaney A, Dahele M, Slotman B, Verbakel W. Evaluation of a knowledgebased planning solution for head and neck cancer. Int J Radiat Oncol Biol Phys2015;91:612–20.
[30] Boutilier JJ, Craig T, Sharpe MB, Chan TC. Sample size requirements forknowledge-based treatment planning. Med Phys 2016 Mar;43(3):1212.

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具