kims presentation web edit
TRANSCRIPT

1
Cardiac Surgery at KIMS
Mr. Inderpaul BirdiConsultant Cardiac Surgeon

2
Plan
• Who am I?
• Surgical revascularisation in stable ischaemic heart disease
– PCI or CABG
– Special circumstances
– Off-pump or On-pump
• Cardiac surgery at KIMS
– Who, What, When, Where

3
Who am I?
• Cardiac Surgeon
– Papworth Hospital and Royal Brompton Hospital
– Consultant since 2003
• Essex Cardiothoracic Centre 2007 (NEW SERVICE)
– Clinical Governance Lead 2007 to 2013
– Surgical Lead 2013 to date
– SCTS Unit Representative
– CQC Specialist Advisor
• Lead Clinician at The Keyhole Heart Clinic

4
Death rates with medical therapy
2013 ESC Guidelines
The more severe the coronary disease the less likely medical therapy is effective

5
Cardiac mortality and extent of ischaemia
2013 ESC Guidelines
Presence of ischaemia is also important

6
PCI versus CABG
• More than 20 trials of PCI versus CABG – No survival benefit
• <10% eligible population
• 0ne-/two- vessel disease
• Normal ventricular function
• Propensity matched Registry data – Consistent survival benefit for surgery
• Registries can be susceptible to confounding
• SYNTAX TRIAL – ‘all comers’ trial
• Benefit of surgery over PCI in certain subgroups
• Higher incidence of repeat procedures in PCI group
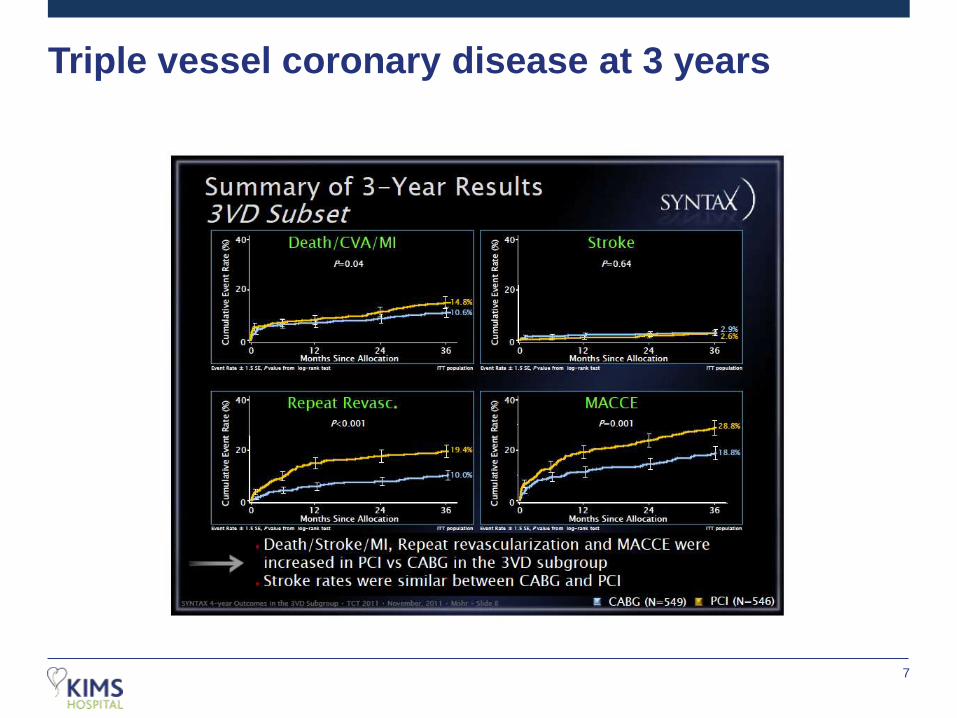
7
Triple vessel coronary disease at 3 years

8
Triple vessel coronary disease at 4 years
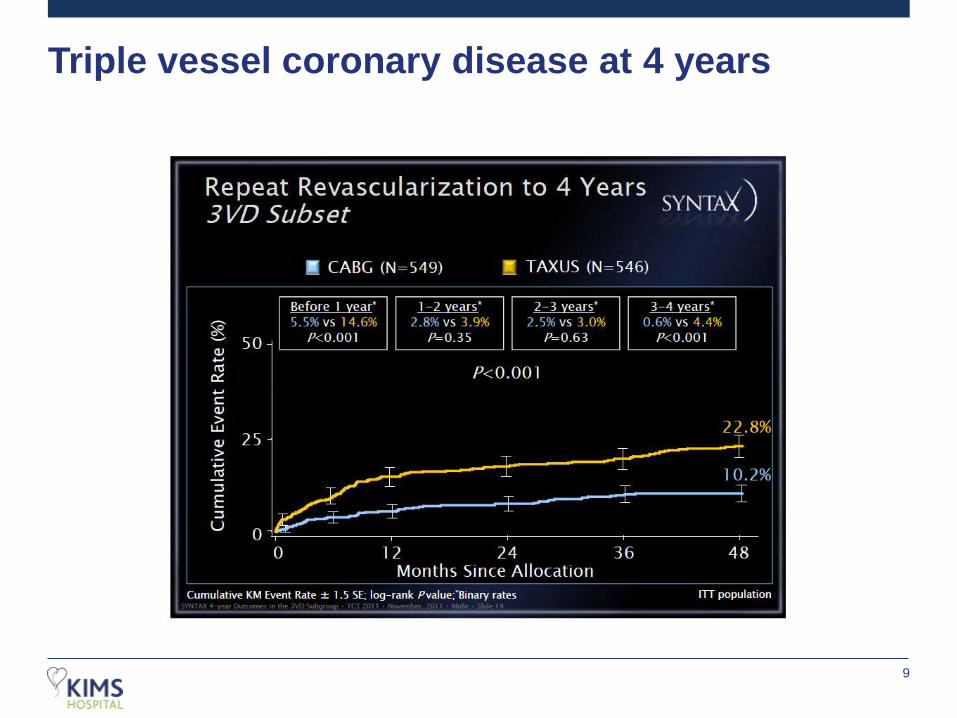
9
Triple vessel coronary disease at 4 years

10
Method of revascularisation
2013 ESC Guidelines

11
Special Situations
• Diabetes
– Complex lesions often predicate a preference for surgery especially in multi-vessel disease
• Elderly
– Balance of risk benefit ratio and influence of prognosis becomes difficult to establish
• Chronic renal disease
– Higher risk of renal injury associated with surgery
• Hybrid therapies (MIDCAB and PCI)
– Rebalancing between evidence base and patient preference

MIDCAB / MULTI-MIDCAB
• Acc Left Minithoracotomy(No costal cartilage or bone excision)
Lima to LAD
95% 10 year patency
Home 3.3 days versus 8 days for sternotomy
(more than £1000 cost saving per case)
Ideal patients:Single LAD lesion
Some multi-vessel lesions
Hybrid revascularisation

13
Off-Pump or On-Pump
• Off-Pump surgery performed in 20% of CABG patients
• Polarised views (Asia – 60-100% performed Off-pump)
• Afilalo et al Eur Heart J 2012
– Metanalysis of 59 trials (9000pts)
• Significant reduction in stroke in Off-Pump group (1.4 v 2.1; rr0.77)
• Lamy et al N Engl J Med 2012
– Randomised trial looked at 30 day outcomes
• Off-Pump group bled less, required reduced transfusions, and suffered reduced respiratory and renal complications

14
Off-Pump or On-Pump continued
• Several large patient Registries suggest:
– Reduction in mortality, stroke and major morbidities
– Less complete revascularisation
– increased incidence of repeat procedures reducing the early mortality benefit
• Real reduction in application of Off-pump surgery since Lamy 2012
• MIDCAB remains extremely attractive either as isolated LAD therapy or
as part of a hybrid protocol with PCI.

15
Summary
• High ischaemic burden indicates prognostic need for revascularisation over
medical therapy
• PCI and CABG offer a complimentary package of interventional and surgical
therapies for the correction of myocardial ischaemia
• Off-pump vs On-pump debate continues
• Hybrid revascularisation may offer a rebalancing of clinical benefit and
patient preference

16
Cardiac Surgery at KIMS

17
Cardiac Surgery at KIMS
• Superb Infrastructure (award winning building; superb theatre space and
specifications; spacious rooms; infection control built in to the design)
• Diagnostic capabilities (CT and MRI; onsite Cardiology support)
• Proximity of services for patients and families is of immeasurable benefit
• CONSULTANT LED SERVICE

18
Surgeons - Deployment
• No existing surgical platform in Kent
– Multi-professional team based care delivery
• Daily Consultant ward rounds
• Daily MDT decision making
• Rapid deployment of clinical care
• Combined experiences from three major centres for Cardiac Surgery covering
the whole of the South of England East to West
• Over 90 combined years of experience in cardiac surgery
• Surgical backup for Percutaneous Intervention ON-SITE
– Unique for any PCI service in Kent and in line with infrastructure design found in most tertiary centres

SCTS outcome data
Data For period April 2010 - March 2013
Risk adjusted In Hospital Mortality Rate
National Average
Ris
k -A
dju
ste
d M
ort
alit
y R
ate
Number of operations
1.63%1.54%
2.79%
2.21%
3.67%
2.83%
2.43%
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
3.50%
4.00%
0 1,000 2,000 3,000 4,000 5,000 6,000
ECTC
Papworth
Royal Brompton
Barts
Harefield
Guys and StThomas
UCLH
Essex Cardiothoracic Centre
20
Surgeons - Expertise
• All types of adult cardiac surgery
• Complete arterial grafting (Beating heart and standard CPB)
• Aortic and Mitral valve repair / replacement
• Surgery for Atrial Fibrillation
• Keyhole heart surgery (MIDCAB : Mini AVR : Mini Mitral)
21
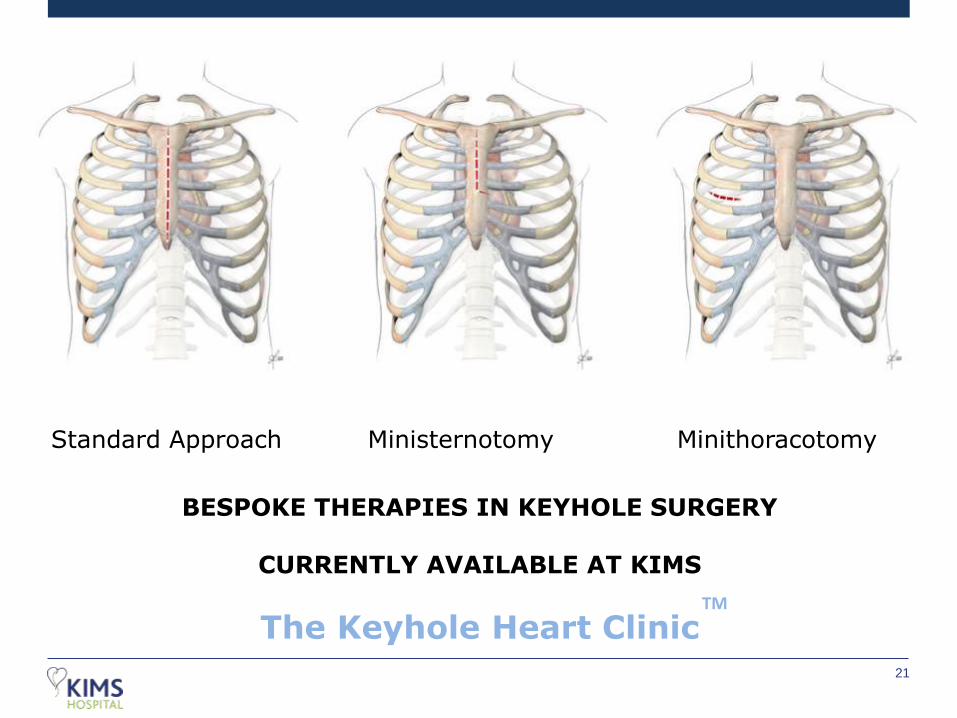
Standard Approach Ministernotomy Minithoracotomy
BESPOKE THERAPIES IN KEYHOLE SURGERY
CURRENTLY AVAILABLE AT KIMS
The Keyhole Heart ClinicTM

22
Minithoracotomy
No broken boneHeals in 10 daysLess painEarly return to activitiesFacilitates later surgeryCosmetically more appealing
Sternotomy
Broken bone12 weeks to heal

AHA/ACC Guidelines
Chronic Severe Mitral Regurgitation
No Symptoms
Class I
LV Dysfunction
Class IIa
New Onset AFPulmonary HT
Class IIaMitral Valve repair may be performed in asymptomaticpatients if performed by an experienced surgical team andThe likelihood of successful MV repair is > 90%
Keyhole approach makes
early surgery more
acceptable to patients

Additional Resources offered by The KHC
www.thekeyholeheartclinic.com
https://m.youtube.com/channel/UC-
WPe3ECVAApb_XiI-s5Avg
Practice based education and training for Primary
care clinicians an their teams
Clinical partnership in the cardiac patient pathways
especially screening