keywords interpretation and decision- making in hyperacute
TRANSCRIPT

Central Journal of Neurological Disorders & Stroke
Cite this article: Ward KM, Charmley A, Haughton SJ, White RP (2021) The Ultimate Stroke Mimic: Familial Hemiplegic Migraine and Acute CT Perfu-sion Changes. Implications for Image Interpretation and Decision-Making in Hyperacute Stroke. J Neurol Disord Stroke 8(2): 1177. 1/4
Abstract
Effective management of hyperacute stroke requires rapid decision making, utilizing clinical evaluation supported by imaging. Stroke mimic misdiagnosis may be associated with exposure to inappropriate reperfusion therapies. Recent imaging developments such as cerebral perfusion imaging improve patient selection, but are incompletely understood by clinicians.
Hemiplegic-migraine is a classic stroke mimic characterized by unilateral motor weakness as an aura manifestation, consequent of uncoupling of cerebral blood flow and metabolism. Complex changes are observed on perfusion sequences which could lead to erroneous interpretation.
We report a case of a 25-year-old male presenting with hyperacute left anterior circulation stroke symptoms with computed tomography (CT) perfusion imaging interpreted as such, with a favorable penumbra to core ratio in the left middle cerebral artery (MCA) territory. The imaging illustrated the poorly appreciated phenomenon of crossed cerebellar diaschisis (CCD). The patient was thrombolysed with complete resolution of symptoms and underwent patent foramen ovale (PFO) closure following extensive negative etiological investigations for his presumed stroke.
Although the patient’s original presentation was thought to be consistent with acute ischemic stroke, a stereotypical re-presentation to hospital informed the final diagnosis of familial hemiplegic migraine.
The clinico-radiologic differential diagnosis of stroke includes hemiplegic migraine in the absence of a proximal vessel occlusion. Imaging findings of hemispheric perfusion defect with CCD may have diagnostic value and is a widely under-recognised phenomenon. As CCD can be seen in both acute ischemic stroke and migraine with aura, hemiplegic migraine remains a convincing stroke mimic.
*Corresponding authorKayla M. Ward, Department of Neurology, Townsville University Hospital, Townsville, Queensland, Australia, Tel: 0413 075 060; Email: [email protected]
Submitted: 23 August 2021
Accepted: 30 August 2021
Published: 31 August 2021
ISSN: 2334-2307
Copyright© 2021 Ward KM, et al.
OPEN ACCESS
Keywords•Stroke mimic•Hemiplegic migraine•Crossed cerebellar diaschisis
Case Report
The Ultimate Stroke Mimic: Familial Hemiplegic Migraine and Acute CT Perfusion Changes. Implications for Image Interpretation and Decision-Making in Hyperacute StrokeKM Ward1*, A Charmley2, SJ Haughton3, RP White4
1Department of Neurology, Townsville University Hospital, Australia 2Department of Neurology, Princess Alexandra Hospital, Australia 3James Cook University, Australia4Department of Neurology, Townsville University Hospital, Australia
INTRODUCTIONStroke mimic describes the presentation of acute neurological
deficits simulating acute ischemic stroke, in the absence of a vascular origin for the symptoms [1]. Stroke mimics represent a significant proportion of code stroke presentations [2]. Thoughtful clinical examination and neuroimaging plays an essential role in stroke mimic recognition. The availability of diffusion weighted imaging (DWI) in acute ED presentations increase early recognition of stroke mimic, but is not feasible in all centers, and not all hyperacute stokes are fit for unventilated magnetic resonance (MR) imaging. Hemiplegic migraine can simulate acute ischemic stroke clinically and on more readily
available imaging modalities such as perfusion imaging, making the challenge of differentiation more difficult.
CASE PRESENTATIONA non-smoking, 25-year-old Caucasian male with no past
medical history, was seen well 90-minutes prior to presentation at a scheduled gym session. Collateral history revealed the sudden onset of dysphasia whilst on the phone calling for aide after developing right-sided weakness.
At presentation he had severe expressive dysphasia and right hemiparesis - National Institute of Health Stroke Scale (NIHSS) score of 5. CT perfusion imaging demonstrated a defect in the
Central
Ward KM, et al. (2021)
J Neurol Disord Stroke 8(2): 1177 (2021) 2/4
left MCA territory in keeping with an area of ischaemia (Figure 1A-D). There was increased Mean Transit Time (MTT) and Time to Peak (TTP) within the left MCA territory (Figure 1A and B) corresponding with a decrease in Cerebral Blood Flow (CBF) and a near normal Cerebral Blood Volume (CBV) (Figure 1C and 1D) suggestive of minimal infarct core with an area of salvageable penumbra. Calculations from the AutoMIStar CT perfusion imaging program revealed a favorable penumbra to core ratio of 80%.
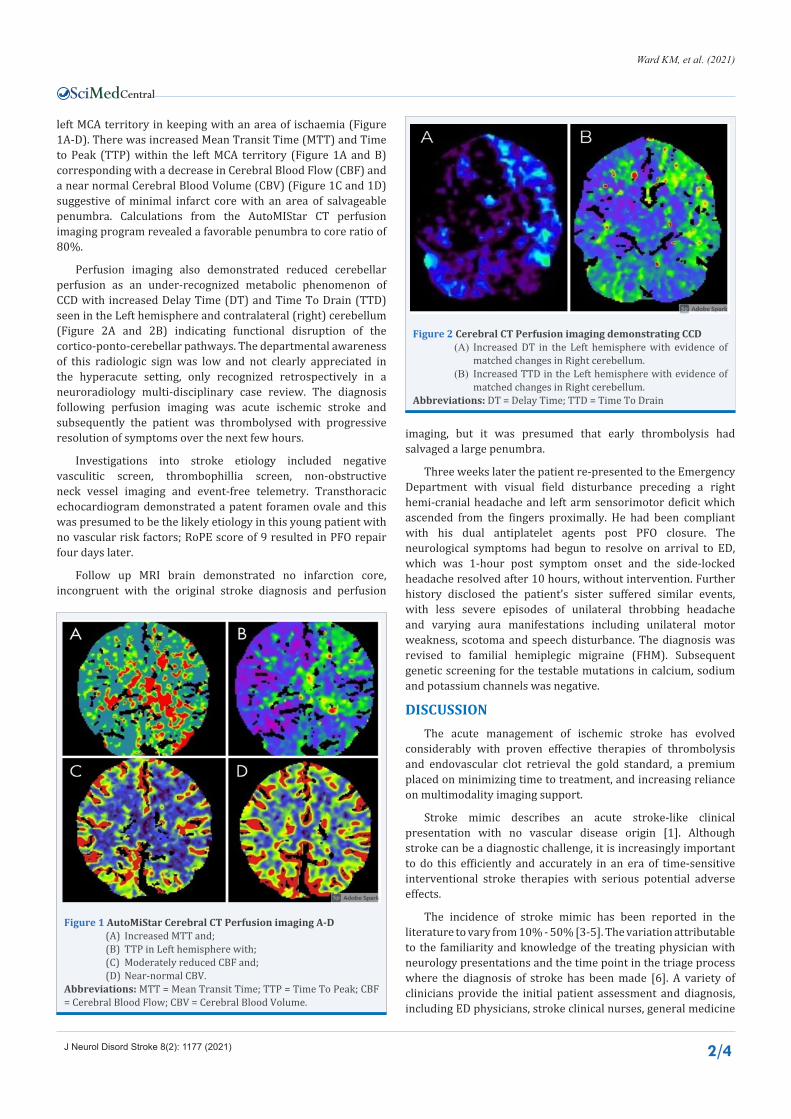
Perfusion imaging also demonstrated reduced cerebellar perfusion as an under-recognized metabolic phenomenon of CCD with increased Delay Time (DT) and Time To Drain (TTD) seen in the Left hemisphere and contralateral (right) cerebellum (Figure 2A and 2B) indicating functional disruption of the cortico-ponto-cerebellar pathways. The departmental awareness of this radiologic sign was low and not clearly appreciated in the hyperacute setting, only recognized retrospectively in a neuroradiology multi-disciplinary case review. The diagnosis following perfusion imaging was acute ischemic stroke and subsequently the patient was thrombolysed with progressive resolution of symptoms over the next few hours.
Investigations into stroke etiology included negative vasculitic screen, thrombophillia screen, non-obstructive neck vessel imaging and event-free telemetry. Transthoracic echocardiogram demonstrated a patent foramen ovale and this was presumed to be the likely etiology in this young patient with no vascular risk factors; RoPE score of 9 resulted in PFO repair four days later.
Follow up MRI brain demonstrated no infarction core, incongruent with the original stroke diagnosis and perfusion
imaging, but it was presumed that early thrombolysis had salvaged a large penumbra.
Three weeks later the patient re-presented to the Emergency Department with visual field disturbance preceding a right hemi-cranial headache and left arm sensorimotor deficit which ascended from the fingers proximally. He had been compliant with his dual antiplatelet agents post PFO closure. The neurological symptoms had begun to resolve on arrival to ED, which was 1-hour post symptom onset and the side-locked headache resolved after 10 hours, without intervention. Further history disclosed the patient’s sister suffered similar events, with less severe episodes of unilateral throbbing headache and varying aura manifestations including unilateral motor weakness, scotoma and speech disturbance. The diagnosis was revised to familial hemiplegic migraine (FHM). Subsequent genetic screening for the testable mutations in calcium, sodium and potassium channels was negative.
DISCUSSIONThe acute management of ischemic stroke has evolved
considerably with proven effective therapies of thrombolysis and endovascular clot retrieval the gold standard, a premium placed on minimizing time to treatment, and increasing reliance on multimodality imaging support.
Stroke mimic describes an acute stroke-like clinical presentation with no vascular disease origin [1]. Although stroke can be a diagnostic challenge, it is increasingly important to do this efficiently and accurately in an era of time-sensitive interventional stroke therapies with serious potential adverse effects.
The incidence of stroke mimic has been reported in the literature to vary from 10% - 50% [3-5]. The variation attributable to the familiarity and knowledge of the treating physician with neurology presentations and the time point in the triage process where the diagnosis of stroke has been made [6]. A variety of clinicians provide the initial patient assessment and diagnosis, including ED physicians, stroke clinical nurses, general medicine
Figure 1 AutoMiStar Cerebral CT Perfusion imaging A-D(A) Increased MTT and;(B) TTP in Left hemisphere with;(C) Moderately reduced CBF and;(D) Near-normal CBV.
Abbreviations: MTT = Mean Transit Time; TTP = Time To Peak; CBF = Cerebral Blood Flow; CBV = Cerebral Blood Volume.
Figure 2 Cerebral CT Perfusion imaging demonstrating CCD(A) Increased DT in the Left hemisphere with evidence of
matched changes in Right cerebellum.(B) Increased TTD in the Left hemisphere with evidence of
matched changes in Right cerebellum.Abbreviations: DT = Delay Time; TTD = Time To Drain

Central
Ward KM, et al. (2021)
J Neurol Disord Stroke 8(2): 1177 (2021) 3/4
registrars, neurology registrars and neurologists. Studies also vary in the timing stroke diagnosis; those including all presumed stroke diagnoses following only initial clinical assessment in ED have shown higher rates of stroke mimic than those where the diagnosis of stroke was assigned after neuroimaging and laboratory investigations were performed [7,8].
In a study by Vroomen et al, of 669 patients admitted by a neurologist with a provisional diagnosis of stroke, only 5% (32 patients) were eventually considered stroke mimics and 15 of those patients were found to have migraine with prolonged aura [5]. Stroke mimic occurred more frequently under 50yrs representing 21% of 87 patients but accounting for only 3% of the 583 patients aged over 50 yrs [5].
Another large cohort study evaluated over 400 patients diagnosed with stroke based on history and examination alone, by different staff members with varying neurology knowledge and experience, resulting in a much higher incidence of stroke mimics [7]. A total of 19% were deemed to be stroke mimics with seizures and postictal deficits (17%), systemic infections (17%), brain tumor (15%), and toxic-metabolic disturbances (13%) the most common mimics [7]. Similar findings were seen in a study by Hand et al, in which 109 of the 350 stroke-like presentations were evaluated to be mimics. Stroke was deemed to be more likely where there was an exact time of onset, definite focal symptoms, lateralizing neurological deficits and findings in keeping with a typical neuroanatomically localized stroke [6].
The case described undertook closure of his PFO as a secondary stroke prevention measure given his extensive negative etiological investigations. In migraine with aura, the presence of PFO has been estimated to be 40-50%. Whilst observational studies suggest migraine with aura responds favorably to PFO closure, randomized controlled trial have not clearly demonstrated a significant benefit of PFO closure in migraine patients [9-11].
Hemiplegic migraine has a reported prevalence of 0.01%, characterized by the presence of unilateral motor weakness as aura [12]. Other typical aura symptoms can occur including visual disturbance, paraesthesia and speech deficits [12-14]. Typically, hemiplegic migraine arises in first to second decade of life and attack frequency declines with age [12]. Hemiplegic migraine occurs sporadically and as a familial syndrome (FHM). FHM is defined by presence of at least one affected first- or second-degree relative with migraine aura and motor weakness on one side of the body as a symptom. In some patients, motor weakness may last weeks and can be difficult to differentiate from stroke or functional neurological disorder, even with advanced neuroimaging. Most patients have an associated side-locked headache, contralateral to their motor weakness. Symptoms usually progress over a 20-30 minute period but occasionally can onset acutely and present like a stroke [12].
FHM is associated in up to 70% of cases, with ion channel-gene mutations; sporadic cases of identical phenotype may reflect new spontaneous mutations, reduced penetrance, or recessive gene disorders. The International Classification of Headache Disorders-3, outlines four subclassifications of FHM based on the associated genetic mutation [8,15]. The CACNA1A gene is associated with FHM1, the most common subtype, accounting for
50% of cases and associated with cerebellar degeneration [14]. FHM2 is associated with ATP1AT gene mutations and FHM3 is associated with SCN1A gene mutations. If no known genetic mutation is identified the patient is diagnosed with FHM4 (25% of cases) [12].
Typically, CT and MR imaging of the brain is normal in FHM but high-quality multimodality Imaging studies including perfusion studies during acute FHM attacks are limited. Several groups have described a range of changes in parameters of cerebral perfusion which are likely to cause confusion in the setting of hyperacute stroke revascularization therapy decision making. A detailed study of perfusion changes in FHM2 with CBF SPECT imaging, demonstrated biphasic changes in cerebral blood flow during attacks with hypoperfusion in the affected cerebral hemisphere followed by hyperperfusion, with the turning point seen at the 18-19 hour mark [16-18]. The hyperperfusion was accompanied by ipsilateral MCA vasodilation demonstrated by MRA in all cases where MRA was performed. This study also demonstrated CCD on CBF- SPECT in 6 of the 11 presentations with FHM. CCD is underrecognized and predominately reported in cases of large hemispheric stroke and epileptic seizures [19-21].
CCD refers to a depression of cerebral blood flow in the cerebellar hemisphere contralateral to a corresponding supratentorial neuronal hypometabolism and represents a functional disruption of the cortico-ponto-cerebellar pathways [19]. White et al demonstrated reduced neuronal metabolic activity in the hemisphere responsible for aura symptoms in a patient with sporadic hemiplegic migraine, as measured by reduced N-acetylaspartate and myoinositol/creatinine area ratio on SV proton magnetic resonance spectroscopy [20]. The early hypoperfusion changes associated with migraine with aura are in keeping with cortical or subcortical spreading depression (CSD), which is the main candidate for aura pathophysiology. CSD is characterized by neuronal hyper-excitability, with a spreading wave of depolarization associated with complex local chemokine neurotransmitter and ion changes followed by an uncoupling of the normal neuronal:CBF relationship [12]. Other neuroimaging studies regarding changes in FHM supported these findings and additionally suggested that cortical swelling and/or hyperintensity of the affected cerebral hemisphere may be seen on T2/FLAIR-weighted MRI [16].
In our case there is radiological evidence of perfusion mismatch in the MCA territory contralateral to the motor weakness with additional CCD.
CCD is a remarkable neurophysiological phenomenon, but the clinical significance has not been established. Kellner-Weldnon et al performed a study on the correlation between CCD in migraine with aura and subsequent cerebellar strokes however no causal relationship was identified [21]. They performed stroke protocol imaging on 98 patients with migraine with aura and 39.1% of patients were found to have CCD [21-23]. None of this cohort demonstrated diffusion restriction on MR imaging indicating that unlike in stroke and seizure, CCD can be considered a benign phenomenon in migraine with aura. Diagnostic sensitivity or specificity of CCD in the differential diagnosis of hyperacute stroke is unknown.

Central
Ward KM, et al. (2021)
J Neurol Disord Stroke 8(2): 1177 (2021) 4/4
Ward KM, Charmley A, Haughton SJ, White RP (2021) The Ultimate Stroke Mimic: Familial Hemiplegic Migraine and Acute CT Perfusion Changes. Implications for Image Interpretation and Decision-Making in Hyperacute Stroke. J Neurol Disord Stroke 8(2): 1177.
Cite this article
Recognition of hemiplegic migraine as a potential stroke mimic and an awareness of how it may present including imaging changes can heighten clinician’s degree of suspicion when assessing stroke patients and potentially aid in the challenging task of recognizing this convincing stroke mimic.
CONCLUSIONThis report details the case of a young, fit man with sudden
onset aphasia and unilateral motor weakness as first presentation of gene negative FHM, with CT perfusion images demonstrating focal cerebral hypoperfusion and CCD. The initial diagnosis of acute ischemic stroke with large penumbra led to thrombolysis and he underwent PFO closure. Repeat hospital presentation with stereotyped features ultimately led to diagnostic revision to FHM. In retrospect, perfusion imaging revealed complex changes including CCD which merits further study as a discriminant marker for stroke versus mimic.
REFERENCES1. Anathhanam S, Hassan A. Mimics and chameleons in stroke. Clin Med.
2017; 17: 156-160.
2. Dupre CM, Libman R, Dupre SI, Katz JM, Rybinnik I, Kwiatkowski T. Stroke chameleons. J Stroke Cerebrovasc Dis. 2014; 23: 374-378.
3. Hosseininezhad M, Sohrabnejad R. Stroke mimics in patients with clinical signs of stroke. Caspian J Intern Med. 2017; 8: 213-216.
4. Wilkins SS, Bourke P, Salam A, Akhtar N, D’Souza A, Kamran S, et al. Functional Stroke Mimics: Incidence and Characteristics at a Primary Stroke Center in the Middle East. Psychosom Med. 2018; 80: 416-421.
5. Vroomen PC, Buddingh MK, Luijckx GJ, De Keyser J. The incidence of stroke mimics among stroke department admissions in relation to age group. J Stroke Cerebrovasc Dis. 2008; 17: 418-422.
6. Hand PJ, Kwan J, Lindley RI, Dennis MS, Wardlaw JM. Distinguishing between stroke and mimic at the bedside: the brain attack study. Stroke. 2006; 37: 769-775.
7. Libman RB, Wirkowski E, Alvir J, Rao TH. Conditions that mimic stroke in the emergency department. Implications for acute stroke trials. Arch Neurol. 1995; 52: 1119- 1122.
8. Kothari RU, Brott T, Broderick JP, Hamilton CA. Emergency physicians. Accuracy in the diagnosis of stroke. Stroke. 1995; 26: 2238-2241.
9. Kumar P, Kijima Y, West BH, Tobis JM. The Connection Between Patent Foramen Ovale and Migraine. Neuroimaging Clin N Am. 2019; 29 :261-
270.
10. Tobis JM, Charles A, Silberstein SD, Sorensen S, Maini B, Horwitz PA, et al. Percutaneous Closure of Patent Foramen Ovale in Patients With Migraine: The PREMIUM Trial. J Am Coll Cardiol. 2017; 70: 2766-2774.
11. Lip PZ, Lip GY. Patent foramen ovale and migraine attacks: a systematic review. Am J Med. 2014; 127: 411-420.
12. Kumar A, Samanta D, Emmady PD, Arora R. Hemiplegic Migraine. StatPearls. Treasure Island (FL): StatPearls Publishing. 2020.
13. Ducros A. [Familial and sporadic hemiplegic migraine]. Rev Neurol (Paris). 2008; 164: 216-224.
14. Jen JC, Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, et al. Familial Hemiplegic Migraine. GeneReviews. Seattle (WA): University of Washington, Seattle. 1993.
15. IHS Classification ICHD-3. International Classification of Headache Disorders 3rd Edition website. 2021.
16. Roth C, Ferbert A, Huegens-Penzel M, Siekmann R, Freilinger T. Multimodal imaging findings during severe attacks of familial hemiplegic migraine type 2. J Neurol Sci. 2018; 392: 22-27.
17. Iizuka T, Tominaga N, Kaneko J, Sato M, Akutsu T, Hamada J, et al. Biphasic neurovascular changes in prolonged migraine aura in familial hemiplegic migraine type 2. J Neurol Neurosurg Psychiatry. 2015; 86: 344-353.
18. Tee TY, Khoo CS, Raymond AA, Syazarina SO. Teaching NeuroImages: Neuroimaging in hemiplegic migraine. Neurology. 2019; 93: e626.
19. Poretti A, Boltshauser E. Crossed cerebro-cerebellar diaschisis. Neuropediatrics. 2012; 43: 53-54.
20. Jacob A, Mahavish K, Bowden A, Smith ET, Enevoldson P, White RP. Imaging abnormalities in sporadic hemiplegic migraine on conventional MRI, diffusion and perfusion MRI and MRS. Cephalalgia. 2006; 26: 1004-1009.
21. Kellner-Weldon F, El-Koussy M, Jung S, Jossen M, Klinger-Gratz PP, Wiest R. Cerebellar Hypoperfusion in Migraine Attack: Incidence and Significance. AJNR Am J Neuroradiol. 2018; 39: 435-440.
22. Allder SJ, Moody AR, Martel AL, Morgan PS, Delay GS, Gladman JR, et al. Limitations of clinical diagnosis in acute stroke. Lancet. 1999; 354: 1523.
23. Han S, Wang X, Xu K, Hu C. Crossed Cerebellar Diaschisis: Three Case Reports Imaging Using a Tri-Modality PET/CT-MR System. Medicine (Baltimore). 2016; 95: e2526.