“keys for housing the homeless
TRANSCRIPT
10-Year Plan to End Chronic Homelessness
Monroe County, Florida
June 01, 2005
“KEYS for Housing the Homeless”
Revised June 10, 2005 SEB

2

3

4
Myth: Establishing Services for the homeless will cause homeless people from all over the country to
migrate to Key West. “If we build it…they will come.”
Fact: Homeless people who move to new areas do so because they are searching for work, have family or
friends in the area, for the climate, or for other reasons not related to services. Homeless services in Key West and Monroe County have dramatically increased since 2002 and the number of homeless
has decreased 55%!

5
EXECUTIVE SUMMARY-Rev. Stephen E. Braddock, Ph.D. Chairman Monroe County Homeless Continuum-of-Care Approximately 1,000 men, women and children experience homelessness in Monroe County at a given point in time during the course of each year. Thousands more live cramped together in the homes of family and friends, in rundown trailers, on derelict vessels, or are in imminent risk of homelessness, living in substandard or overcrowded housing they cannot afford. KEYS for Housing the Homeless is a long-range, comprehensive plan to help homeless people in the Florida Keys return to healthy and stable lives in permanent housing. It is a collaborative effort by homeless service providers, elected government officials and administrators, housing developers, community leaders, clergy, homeless, and formerly homeless people. The recommendations that follow are evidence-based, and draw from the best practices of innovative programs and initiatives throughout the United States. KEYS for Housing the Homeless is intended to end long-term, or “chronic homelessness.” The United Stated Department of Housing and Urban Development (Hereinafter “HUD”) defines the chronic homeless as “an unaccompanied individual with a disabling condition who has been homeless for a year or longer or had four episodes of homelessness in three years.” This emphasis on chronic homelessness reflects a growing body of research demonstrating that members of the chronic homeless population are poorly served for the long-term by existing efforts, even though they use a disproportionate share of emergency services and resources. In Monroe County this year, 48% of the total homeless population have been homeless for over a year and are considered to be chronically homeless. Research supports the idea that the chronic homeless population is best served by utilizing a Housing First/Housing Plus model, this model focuses on moving people out of homelessness and into housing as soon as possible; and then addressing their other needs. Housing First/Housing Plus projects across the country are reporting impressive results. After five years, as many as 90% of participants have remained in permanent housing. Under the leadership of the United States Interagency Council on Homelessness, a national consensus has emerged that all levels of government must focus on improving efforts to house chronically homeless individuals and families.

6
KEYS for Housing the Homeless is consistent with, and complimentary to, the federal government’s initiatives in this area to solve what it has called a “national disgrace.” The strategies presented are drawn from three homeless summits held in Key West since 2002, as well as concepts developed by the National Alliance to End Homelessness, and specific action steps already initiated through Monroe County CoC planning process. The State of Florida, through its Office on Homelessness established in 2001, and the Governor’s Council on Homelessness, coordinates statewide efforts with federal programs and local homeless continuum-of-care (CoC) plans. Hereinafter, federal, state, and local plans must compliment each other, because each level of government needs to play an integral part in implementation of effective strategies to end homelessness. The scope of KEYS for Housing the Homeless is not limited to chronic homelessness alone, but also addresses the needs those who experience situational homelessness. When implemented over the next decade, the policy recommendations will also result in a significant reduction of all types of homelessness, including among families, youth, workers, victims of abuse, elderly and disabled adults. Successful implementation of KEYS for Housing the Homeless will depend on funding availability at the local, state, and especially, federal levels. This plan does not detail exact sources or methods of funding, or how much is required. Local funding decisions will be left to the elected officials who embrace KEYS for Housing the Homeless, in consultation with the Southernmost Homeless Assistance League (hereinafter, SHAL) board of directors, and members of the 10-Year Plan Steering Committee. KEYS for Housing the Homeless is intended to end chronic homelessness and reduce all types of homelessness over the next decade by investing our resources in a coordinated, sustained effort that addresses the underlying causes of homelessness and avoids duplication of services. This anti-homelessness initiative will: *Reduce the number of people who become homeless in Monroe County. *Reduce the number of people who are currently homeless in Monroe County. *Decrease the length of homeless episodes. *Provide community based services and support that prevents homelessness before it happens. *Diminish opportunities for homelessness to recur. *Reduce the burden on law enforcement and costs to the taxpayers.

7
These goals will be accomplished through the following approach: *Leading the Way: The Southernmost Homeless Assistance League (SHAL), Monroe County’s federal and state recognized entity responsible for the jurisdiction’s homeless continuum-of-care (CoC), will oversee implementation of the plan in consultation with local units of government.
*Developing the Homeless Management Information System: (HMIS)- a Homeless Management Information System (HMIS) will be utilized to link all services, screen for program eligibility, identify gaps in services; gather data needed to monitor progress of implementation, and generate annual progress reports for HUD and other funding sources. *Prevention: Steps must be taken to stop individuals and families from becoming homeless. These steps include better coordination of financial assistance and discharge planning for people leaving public institutions, and creating affordable workforce housing. *Housing First: Development and implementation of a county-wide Housing First program that will include permanent housing for all homeless. *Housing Plus: Necessary supportive services must be provided to ensure that homeless individuals and families placed in permanent housing can remain housed long-term.
Myth: Charitable groups will always be able to take care of the homeless.
Fact: The growth of homelessness has far exceeded
the capacity of local charitable groups and inadequate funding is threatening their ability to
even sustain the current level of services. Homelessness is a societal problem that requires a
partnership between private charities and the government, with active public support.
8
Introduction: Of the 80-thousand people who live in Monroe County, at least 1,000 people are known to be homeless at any given point in time. Most are concentrated in Key West and the lower Keys. Visitors and residents of the Keys cannot miss the small groups of homeless people that gather throughout the day before many seek refuge at the Keys Overnight Temporary Shelter (KOTS) on Stock Island. Every afternoon, homeless individuals and families line up at St. Mary’s Soup Kitchen in Key West, or Higher Love Mission Outreach in Marathon, for a hot meal. Dozens file in and out of the Florida Keys Outreach Coalition’s (FKOC) trailer at the rear of the Key West Police Department for a shave and shower. Homelessness costs our community millions of dollars annually; the human cost of homelessness is immeasurable. In response to urgent recommendations from the United States Interagency Council on Homelessness, the United States Department of Housing and Urban Development, the Florida Office on Homelessness, the Mayor of Key West and the Chairman of the Southernmost Homeless Assistance League formed a steering committee to oversee a 10-year strategic plan to end homelessness in Monroe County. The committee is comprised of local business, law enforcement, homeless service providers, medical professionals, non-profit organizations, faith-community and government leaders.
Strategic Planning Committee Members Millie Andreasen AIDS Help
Greg Artman Monroe County Sheriff’s Office
Julio Avael City Manager City of Key West
Deb Barsell National Director of Development West Care Corporation
Reverend Stephen Braddock, Ph.D. Chairman of SHAL Monroe County of CoC
Charlie Bradford Chairman Key West Chamber of Commerce
Veronica Brown Formerly Homeless
Manuel Castillo Executive Director Key West Housing Authority
Russ Draper Key West Park Ranger
Chad Duncan Florida Keys Children’s Shelter SHAL Board Member
Frances England Monroe County School District Children’s Homeless Intervention Project
Hon. Rosemary Enright Florida State Public Defender SHAL Board Member
Diana Flenard Secretary of SHAL Monroe County CoC
Jay Gewin Assistant to the Key West Mayor and City Commissioners
Jan Goes Homeless Middle Keys
Very Reverend Michael Hartney Middle Keys Faith Community SHAL Board Member

9
Elena Herrera, Administrator Department of Children and Families SHAL Board Member
Captain Phil Heyl U.S. Coast Guard Key West
Louise Hubbard Chairwoman Florida Coalition for the Homeless
John Jones, Assistant City Manager City of Key West SHAL Board Member
Honorable Mark Kohl Florida State Attorney SHAL Board Member
Justine Kraft Homeless Lower Keys
Elmira Leto Vice-Chair of SHAL Monroe County CoC
Pastor Debbie Maletic Higher Love Homeless Outreach Middle Keys Service Provider
Dr. Duncan Matthewson Monroe County School Board SHAL Board Member
Chief Bill Mauldin Key West Police Department
Hon. Margie Mearns Councilwoman City of Marathon
Clare Murray Formerly Homeless
Honorable Sony McCoy Monroe County Commissioner
Margy McMennamy Grants Acquisition Manager Monroe County
Mary Miles Special Assistant to SHAL Chairman
Reverend Len Millison Key West Interfaith Council
Randy Osipow Key West Innkeepers Association & Restaurant and Bar Association
Virginia Panico President Key West Chamber of Commerce
Gina Pecora Business Manager Florida Keys Outreach Coalition, Inc
Trixie Phelan Contract Manager Department of Children and Families
Sandy Pearce Public Defender’s Office
Tom Pierce Executive Director Florida Office on Homelessness
Honorable Rick Roth Sheriff of Monroe County
Hon. Dixie Spehar Mayor of Monroe County
Tom Sterner Formerly Homeless
Dr. Tom Taylor Florida Conflict Resolution Consortium
Officer Steve Torrence Key West Police Department
Catherine Vogel, Esq. Assistant State Attorney
Hon. Jimmy Weekley Mayor of Key West
Dr. Niki Will Lower Keys Medical Center
10
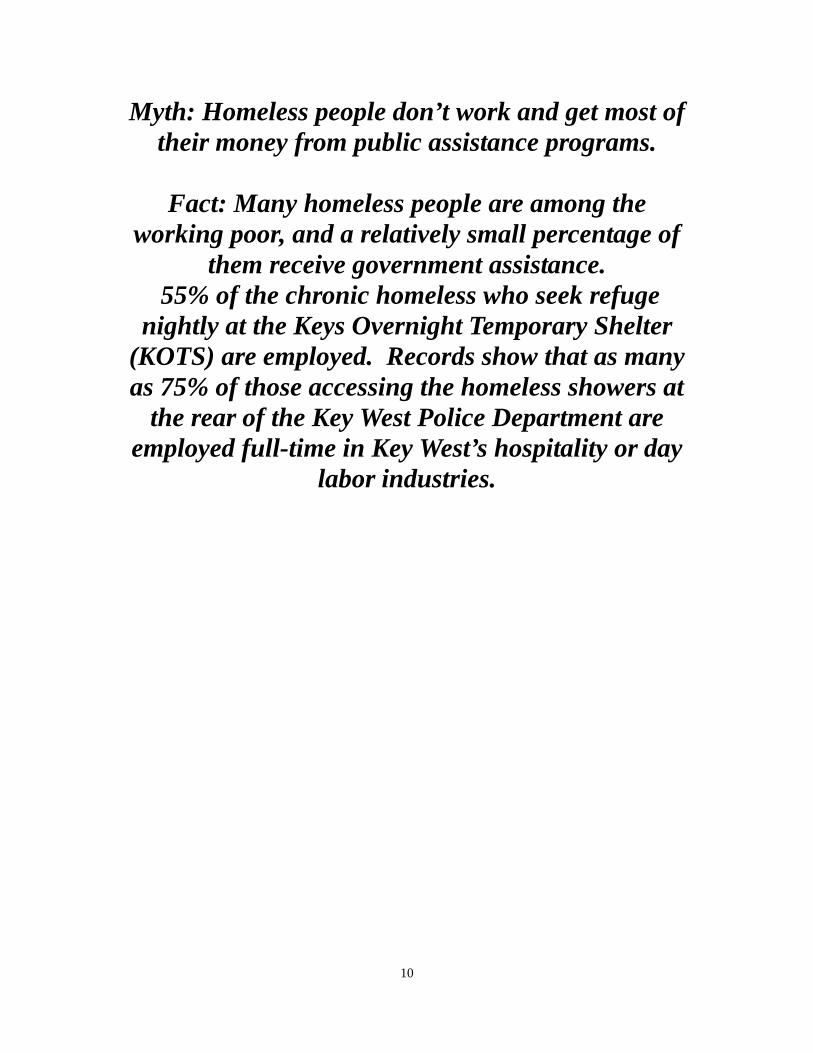
Myth: Homeless people don’t work and get most of their money from public assistance programs.
Fact: Many homeless people are among the
working poor, and a relatively small percentage of them receive government assistance.
55% of the chronic homeless who seek refuge nightly at the Keys Overnight Temporary Shelter
(KOTS) are employed. Records show that as many as 75% of those accessing the homeless showers at
the rear of the Key West Police Department are employed full-time in Key West’s hospitality or day
labor industries.

11
Homelessness in Monroe County Currently, services and shelter for the homeless are provided through the agency and governmental members of the Southernmost Homeless Assistance League (hereinafter “SHAL”), an incorporated federal 501 (c) (3) tax-exempt organization that meets monthly to plan and prioritize around homeless issues. Once a year, SHAL conducts a point-in-time census to count and document the number of homeless people in the county. The last census was held January 26, 2005 and found a total of 981 homeless, a 55% decrease since 2002. The decrease in homelessness is evidence that programs currently in place are working. Especially, the full utilization Poinciana Plaza, former Navy property that transferred to the City of Key West and now offers transitional and permanent residential facilities for homeless individuals and families with special needs. The chart below shows the breakdown of the sub-populations:
Gender:
Male 78.5%
Female 21.5%
Age:
Under 18-years 8.4%
18-60 years 73.9%
60-years and older 17.7%
Race:
Asian 5.6%
Black/African American 9.6%
White 84.8%
Hispanic or Latino: 13%
Veteran: 12%
Family Status:
Single, no minor children 75.5%
Single, with minor children 6%
Married, no minor children 18.5%
12
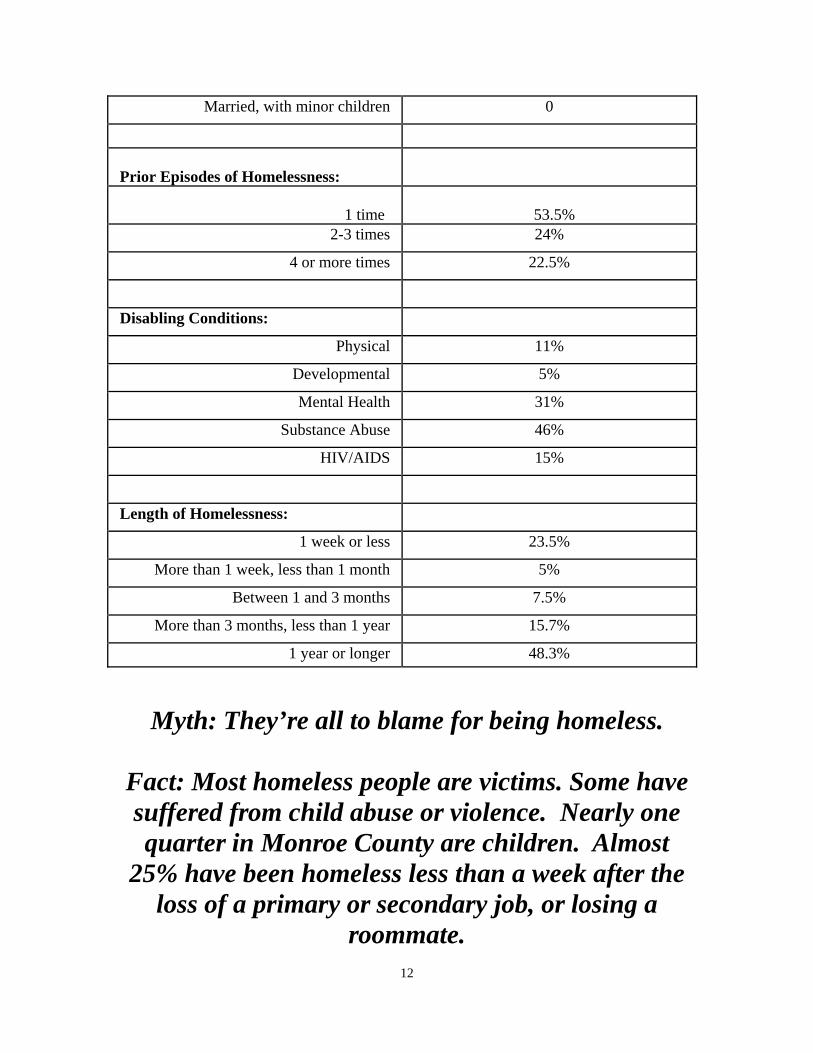
Married, with minor children 0
Prior Episodes of Homelessness:
1 time
53.5%
2-3 times 24%
4 or more times 22.5%
Disabling Conditions:
Physical 11%
Developmental 5%
Mental Health 31%
Substance Abuse 46%
HIV/AIDS 15%
Length of Homelessness:
1 week or less 23.5%
More than 1 week, less than 1 month 5%
Between 1 and 3 months 7.5%
More than 3 months, less than 1 year 15.7%
1 year or longer 48.3%
Myth: They’re all to blame for being homeless.
Fact: Most homeless people are victims. Some have suffered from child abuse or violence. Nearly one quarter in Monroe County are children. Almost
25% have been homeless less than a week after the loss of a primary or secondary job, or losing a
roommate.
13
The point-in-time census is only a one day “snapshot” of homelessness in the Florida Keys. Programs offered by the Florida Keys Outreach Coalition (hereinafter “FKOC”), for example, serve many more homeless people over the course of a year than the census revealed in the one day count. In addition to the annual point-in-time count, a detailed survey was initiated in January 2005 to gather detailed demographic information and identify who is chronically homeless in our community. The vast majority of the chronic homeless suffer from some type of mental illness, and/or a substance abuse problem. In 2005, SHAL’s point-in-time census revealed that at least 48% of homeless surveyed met the statutory definition of chronic homelessness. This is almost four times greater than the national average. What is particularly significant about the chronically homeless population is the percentage of resources they consume. Nationwide, approximately 80% of homeless individuals and families are homeless for a very short period of time. They obtain the services needed and move-on to stable affordable housing. The next 10% stay in the homeless system a while longer, but they too, obtain the services they need and are re-housed. The chronic homeless population, (on national average), representing approximately 10% of the homeless population, uses more than 50% of the available resources. The percentages are much higher and costs even greater in Monroe County. Finding more cost-efficient ways to serve this population will make more resources available for the other homeless individuals and families. Within the chronic homeless population, a smaller group of homeless men and women are constantly causing problems for downtown businesses, residents and tourists, and are frequently arrested for minor offenses. The 2005 Key West City survey established the issue of homelessness as a primary concern of the citizens. The community cost of this subpopulation will be examined in the next section. Some recommendations in this plan are specifically for this population. A Change in Approach Services are currently delivered to the homeless through the SHAL’s Continuum of Care (CoC) using a "housing readiness" approach. The CoC model stretches all levels of housing on a continuum, beginning with emergency shelter, then transitional housing with supportive services, and ending with permanent housing. People move along the continuum when they are "ready" for a specific type of housing, usually by articulating a desire for change, or completing one phase and progressing to the next. The housing readiness model requires compliance with service and treatment plans. Services are only available as long as a person lives at the program site, adhering to certain requirements such as employment, sobriety, attending life skills classes, receiving case management and working toward self-sufficiency and independence. The chronic homeless do not move along the continuum, because they are "never ready".

14
The mentally ill chronic homeless are focused on surviving from one day to the next, often not even realizing the existence of their illness. They cannot move along the continuum, off the street, into transitional or permanent housing using the traditional components of the CoC, with the high demand for cooperative, goal oriented, and consistent behaviors. A different service model has to be utilized to house the chronic homeless population. The collaborative effort between Monroe County, the City of Key West, Monroe County Sheriff’s Office, SHAL and FKOC to establish the Keys Overnight Temporary Shelter (KOTS) has been a good start and provides an excellent opportunity for outreach and intervention, but much more needs to be done. A Housing First/Housing Plus model will seek to assist persons at the KOTS, and on the streets, to exit homelessness as quickly as possible by placing them in permanent housing as soon as possible and linking them to needed services. This approach assumes that the factors that have contributed to a person's homelessness can best be remedied once the individual is housed rather than in emergency shelters or transitional housing facilities. It also accepts the fact that for some, life long support may be required to prevent the reoccurrence of homelessness. Hence, it seeks to maximize utilization of mainstream resources. The model also seeks long term self-sufficiency, promoted through a wrap- around service philosophy. Housing First/Housing Plus Within this Housing First model, two core principles define permanent housing: • Choice regarding location and type of housing. • No predetermined limit on the length of time that the individual or family can
remain in the housing unit. Accordingly, the form of permanent housing will vary according to the needs and desires of each individual or family.

15
The Cost of Homelessness Because homeless people have no regular place to stay, they use a variety of public systems in an inefficient and costly way. People who are homeless are more likely to access costly health care services by utilizing emergency rooms instead of primary care physicians. They also spend more time in jail or prison, often for crimes such as loitering, camping, panhandling, open container or public drunkenness, which is tremendously expensive. Homelessness both causes and results from serious health care issues, usually including addictive disorders. Treating homeless people for drug and alcohol related illness in less than optimal conditions is expensive and ineffective. Substance abuse increases the risk of incarceration and also HIV exposure. Fifteen percent of the homeless surveyed in SHAL's 2005 census reported they were HIV positive. This is, in itself, a substantial cost to our medical system. • *Jail During 2004, 418 homeless individuals were arrested in Monroe County, for a total of 966 bookings. Some of these individuals were arrested as many as 5, 10, 20 or 30 times! One individual was arrested 36 times in 12 months! 966 bookings at an assumed average length of incarceration for 29 days at a cost of $80.00 per day totals $2,241,120.00 $2,241,120 divided by 418 individuals equals an average cost of $5,361.53 per homeless person arrested. These figures do not include costs related to police time, prosecution, defense, probation, parole or health care needs while in custody. The total cost to taxpayers for the arrests and incarceration of homeless individuals is enormous. Most arrests are the result of illegal behaviors related to mental illness, substance abuse, and “quality of life” infractions. The American Bar Association’s Commission on Homelessness and Poverty has agreed to assist SHAL in evaluating the possibility of establishing a “homeless court.” Homeless Courts are being created in communities across the country and may be one strategy that would ease the burden on our criminal justice system. Homeless Courts are special court sessions held in a local shelter or other community site designed for homeless citizens to resolve outstanding misdemeanor criminal warrants (principally “quality of life” infractions such as disorderly conduct, open container, public drunkenness, blocking a sidewalk, sleeping on a beach or in a park after hours, public urination, etc.) Resolution of outstanding warrants not only meets a fundamental need of homeless people but also eases court case-processing backlogs and reduces vagrancy.

16
Homeless people tend to be fearful of attending court, yet their outstanding warrants limit their reintegration into society, deterring them from using social services and impeding their access to employment. They are effectively blocked from obtaining driver’s licenses, job applications, rental agreements, and even entry into transitional housing for the homeless at Poinciana Plaza. The founder of the country’s first homeless court, San Diego Assistant Public Defender, Steve Binder, will visit Key West in summer 2005 to meet with law enforcement, judicial officials, and homeless service providers, to offer technical assistance and advice on creating such a program for Monroe County. • *Hospitals and Health Care Poor health is closely associated with homelessness. For families struggling to pay the rent, a serious illness or disability can start a downward spiral into homelessness, beginning with a lost job, depletion of savings to pay for care, and eventual eviction. The rates of both chronic and acute health problems are extremely high among the homeless population. Conditions which require regular, uninterrupted treatment, such as tuberculosis, HIV/AIDS, diabetes, hypertension, chronic obstructive pulmonary disease, addictive disorders, mental illness, and infections like staphylococcus, are extremely difficult to treat or control among those without adequate housing. Furthermore, when the homeless seek health care services, it is often at an expensive, inpatient, acute level, as preventative care was not obtained. As well, the homeless may be Baker Acted, or involuntarily committed, to a mental health facility on a revolving door process. Many homeless people have multiple health problems, have physiological and mental illnesses, and are dual diagnosed persons. For example, leg and foot ulcers and upper respiratory infections are frequent, often the direct result of homelessness. Homeless people are also at greater risk of trauma resulting from muggings and beatings. Homelessness precludes good nutrition, good personal hygiene, and basic first aid, adding to the complex health needs of homeless people. Fortunately, there is no reason for any person in Key West, or Marathon, to go without a daily meal and hot shower. St. Mary’s Soup Kitchen serves the homeless and poor a hot meal every afternoon at 4:00pm, and the Florida Keys Outreach Coalition operates a 12-stall shower facility at the rear of the Key West Public Safety building every weekday evening and Saturday mornings. This shower facility, and the one at KOTS, have helped to dramatically reduce the spread of Methicillin-Resistant Staphylococcus Aureus (MRSA) that was spreading easily among the homeless population. Higher Love Homeless Outreach provides meals and showers to homeless in the Middle Keys. All programs currently providing basic food, personal hygiene, and shelter must continue to be supported as means to prevent illness and unnecessary health care costs. In addition, some homeless people with mental disorders may use drugs or alcohol to self-medicate, and those with addictive disorders are also often at risk of HIV and other communicable diseases.

17
People who are homeless are overwhelmingly uninsured and often lack access to the most basic health care services for their complex health care needs. Lower Keys Medical Center (LKMC) reports of the 20,000 plus visitors to its emergency room last year (15% of whom were admitted) a whopping 3635% were indigent or uninsured. This fact alone is causing physicians to rethink their ability to maintain a practice where the cost of living continues to escalate. The reimbursement for physician services has fallen to an all time low, with Medicaid reimbursing at ten (10) cents on the dollar, and self pay being no-pay. Increased malpractice insurance rates, high costs associated with retaining quality support staff ,and increased taxes on their professional offices are just a few of the reasons for dissatisfaction sited. Physicians that have left the community site the high cost of living and the low return for services rendered. The emergency room is dependent on the services of “on call” specialty physicians for services needed by the patients who frequent the emergency room. The hospital in Key West must financially subsidize key physician specialties in order to cover the Emergency Department due to the high level of uncompensated patients. Combined with the cost of living in the Keys, it is often difficult to recruit physicians because of the poor payor mix and higher levels of uncompensated care. The Lower Keys Medical Center is projected to provide $20 million dollars in uncompensated and charity care in fiscal year 2006. Currently, a comprehensive primary and preventive care program does not exist. The emergency room is utilized as a clinic for the sickest patients, with the highest cost of care, due to lack of medical attention in the earliest stages. This current situation exists for long-term, contributing residents of the community, as well as those who are homeless. Under a Health Care for the Homeless application, Monroe County would only be eligible for a maximum of $100,000 a year. This would not even begin to address the need, as not even a physician can be retained under those financial limitations, let alone provide for a facility, supplies and support staff necessary to meet all the Federal regulations required to sustain a medical practice. Currently, the Lower Keys Hospital District Board covers the cost of one full-time physician who treats the homeless at the indigent health clinic Monday through Friday 9am-5pm. In addition, limited funds annually are available to physicians who choose to

18
participate in a program of caring for the indigent who live south of the Seven Mile Bridge. Rural Health Network of Monroe County (RHNMC) operates two Medi-Vans and a clinic at St. Mary’s Soup Kitchen. 284 homeless individuals were treated during a total of 638 visits county-wide. Attempts by RHNMC to secure federal funding for a Community Health Center have thus far been unsuccessful but RHNMC is committed to continue to attempt to obtain CHC status. Additional funding is urgently needed to adequately care for the healthcare of the homeless and working poor of Monroe County. Lack of housing greatly impacts efforts to provide health care to homeless persons: housing is the first form of treatment for homeless people with medical problems, preventing many illnesses and making it possible for those who remain ill to recover. Access to affordable, high-quality and comprehensive health care is also essential in the fight to end homelessness. A fully funded health care for the homeless system would reduce homelessness and, more significantly, help to prevent future episodes of homelessness, as well as ease the pain -- and even prevent unnecessary deaths -- of those on the streets. A health system for the homeless would also reduce the fiscal impact and social cost of communicable diseases and other illnesses. • *Emergency Shelter Low demand emergency shelter, such as the KOTS, is a costly alternative to permanent housing. While it is necessary for short-term crises, by offering a humane alternative to sleeping in places not suitable for human habitation, and contributes greatly toward protecting the environmentally sensitive lands from being destroyed by homeless encampments, it has also, predictably, become long-term housing for some. Many are too mentally ill or addicted to live peaceably in available transitional housing with others, or independently in permanent housing. The degree of mental health and substance abuse care that is required is not presently available to them even if they want it. Others are working full-time, or more, and simply cannot afford housing in a community with the highest cost of living in the State of Florida. The men’s sleeping quarters at the KOTS are surplus Navy tents, made of canvass that will need to be replaced as they dry rot. Replacing all the canvass with fiberglass panels is an option being explored by city management and FKOC. The City has included the creation of a more permanent facility as part of its own 2005-2010 Strategic Plan.
19
Myth: The Homeless are dangerous and they break the law.
Fact: In general, the homeless are among the
least threatening group in our society and are more likely to be victims of crime. Although they are more likely to commit non-violent and non-destructive crimes, they are
less likely to commit crimes against person or property.
Guiding Principles for KEYS to Housing the Homeless: The ongoing development of this plan will guided by these principles: • Recognition that homelessness and near homelessness are growing problems in
Monroe County - and that a severe shortage exists of housing affordable to people with extremely low incomes, low incomes and even moderate incomes.
• Commitment to the belief that more can be done to prevent homelessness and to more effectively serve people in need.
• Recognition that the vast majority of homeless people are not homeless by choice, even though their own actions may have contributed to and perpetuated their homelessness.
• Support for the concept that better coordination among agencies is needed to address the multiple factors that contribute to homelessness, including poverty, domestic violence, substance abuse, and lack of education and job skills.
• Agreement that mainstream organizations - not just groups that serve only homeless people- must become more involved to develop an effective community response. People in need will be better served if the justice; mental health and welfare systems; child protective services; employment assistance programs; housing developers; neighborhood organizations; and other areas of the public and private sectors do more, individually and collectively, to eliminate homelessness.
• A belief that homeless and near homeless should become as independent as possible, for their own dignity, to contribute as much as they can to society, and to

20
limit the cost homelessness places on society. To assist them in reaching this goal, people in need should receive appropriate support services.
• Agreement that realistic goals must be set for assisting homeless and near-
homeless people to move out of crisis and toward self-sufficiency. In addition, mechanisms should be established to evaluate progress toward meeting these goals.
• Recognition that the plan we are developing should not become a document gathering dust on a shelf. This steering committee should establish recommendations for providing oversight to ensure the 10-year plan is carried out and to provide adjustments to the plan as needed.
KEYS for Housing the Homeless has four major components:
1. Leading the way: Designation of SHAL as lead agency. 2. Developing the Homeless Management Information System (HMIS) 3. Closing the front door: Prevention 4. Opening the back door: Housing First/Housing Plus
Myth: Homeless people are all mentally ill or
substance abusers.
Fact: Nationwide about 25% of the homeless are estimated to be mentally ill, about 40% are alcohol or substance abusers, and about 15% suffer from
both disabilities. One percent may need long-term hospitalization.
LEADING THE WAY: SHAL as Lead Agency To ensure the progress toward the goal of ending homelessness in Monroe County, SHAL will coordinate implementation of the plan and be accountable to the community, homeless service providers and local government. SHAL has a track record of quality service, advocacy, grant writing and grant management, and institutional accountability.

21
SHAL has relationships with service providers, funding sources, elected officials, law enforcement agencies and other stake holders. As a non-profit, rather than a government entity, SHAL can ensure that the realization of the plan's goals transcends electoral cycles. SHAL has strong and diverse board membership and leadership. SHAL is a volunteer driven organization. Immediate funding is needed for SHAL to be able to hire full-time administrative support. This support should include expertise in grant writing, management, homelessness, and access to mainstream resources. The function of SHAL: Managing HMIS (HMIS is described in the next section.) Working with service providers to better coordinate and communicate through using
HMIS. Helping agencies increase their capacities to implement HMIS. Producing periodic reports and monitoring the results of service providers. Identifying and obtaining additional public and private resources, and consulting with
local philanthropies and governments about gaps and services, and funding priorities. Coordinating service provider agencies and local government efforts. Acting as
liaison to local, state and federal government. Providing regular progress reports to the community.
Developing the Homeless Management Information System (HMIS) Each jurisdiction has been mandated by HUD (an unfunded mandate) to begin using an HMIS system no later than October 2004. That deadline has already been missed due to lack of funding. HMIS, at the very least, is a computer software system that collects a variety of information on homeless people and compiles data. Ideally, the system can be used to coordinate services, link resources, centralize intake, manage housing placement and monitor wrap-around services. Numerous communities across the nation have successfully implemented this for their entire social services network and many have integrated it with a 211 system. SHAL is in the process of implementing a pilot program created by DOMUS. The pilot system will be operational no later than June 8, 2005. Anticipated funding through a capacity building grant from the Health Foundation of South Florida will allow the system to fully be operational by all service providers in the CoC by October 2005.
Strategies and goals for HMIS:
Fully fund and implement HMIS by the end of 2005 and link it to 211. Establish a “no-wrong door” entry into the homeless network. Link all intake forms, service plans, referral protocols, and housing resources with
HMIS. Use HMIS to screen for program service and eligibility, and to identify gaps in
services.

22
Myth: Homeless in the Keys are all single men that just need to get a job.
Fact: Families constitute a large and growing
percentage of the homeless population nationwide and in Monroe County. Monroe County has only two units designated for homeless intact families.
55% of the men at KOTS work full-time. CLOSING THE FRONT DOOR: Prevention The most humane strategy for addressing homelessness is to prevent its occurrence in the first place. Prevention efforts include strategies such as one-time, short-term rent or mortgage assistance, legal assistance programs, representative payee and direct payment programs, and housing placement services. They also include more systemic strategies that seek to prevent homelessness by ensuring that people leaving institutions such as jails, prisons, or treatment facilities are not discharged to the streets or shelter system, as well as strategies that seek to forestall homelessness in cases of family crisis such as domestic violence. By far, the most common prevention approach is the provision of one- time or short-term financial assistance, such as was established by Key West Mayor, Jimmy Weekley, this past year to offer “move-in financial assistance” to needy individuals and families. Such programs assist persons at risk of becoming homeless by providing one-time rental assistance payments and funds for security and utility deposits. Strategies to prevent homelessness: 1. Better coordinate and expand legal assistance and housing resources available for
one- time, short- term and transitional financial assistance that can be used to avert eviction. Legal services, SHAL members, Monroe County Social Services, Key West Housing Authority, and Monroe County Local Land Authority will work together to better utilize their services and resources.
2. Increase linkage to permanent housing and services for people leaving institutions through the creation of a mobile 24-hour discharge team that can collaborate on placements upon discharge. This discharge team will include representatives of

23
discharging institutions, the SHAL membership, and housing providers. 3. Set up zero tolerance policy for discharge to homelessness policy including hospitals,
jail, prison, foster care shelters, recovery programs, transitional programs and halfway houses.
4. Fund, implement and fully utilize 211 for referrals and link it to HMIS. 5. Refer individuals assisted by prevention programs to mainstream resources to support
their sustainability. Receipt of assistance will trigger eligibility assessment for mainstream resources.
6. Provide landlord education of homelessness and services available to homeless. This strategy will be accomplished by SHAL in cooperation with the Key West Landlord Tenant Association, the Key West Housing Authority, Monroe County Housing Authority, Key West Affordable Housing Task Force, The Florida Keys Assisted Care Coalition, and others.
7. Fully fund and develop a health care for the homeless system. 8. Establish more mental health & crisis counseling services 9. Provide better education of existing help and resources. 10. Develop alternative diversion programs for mentally ill to relieve the jail issue,
possibly a halfway house/sheltering facility 11. Have the Housing Authority Community Development Agency serve as the central
agency to manage prevention rental assistance. 12. Pursue state and federal grants for prevention initiatives. 13. Explore voluntary donations on Waste Management bills to fund homeless services. 14. Encourage voluntary donations on utility bills OPENING THE BACKDOOR: Housing First Housing First must be utilized for those who are already homeless or for whom homelessness cannot be prevented. For Monroe County, this approach will ultimately result in a fundamental shift in our shelter strategy and policies away from the current system, to a model in which short-term housing is provided for the minimum time needed to access permanent housing. Services will be focused on immediate and comprehensive needs assessment, resource acquisition, and housing placement. Upon entry into the homeless service system, each individual and family will be assessed for eligibility of mainstream resources. Housing placement and job training services will be provided along with primary healthcare, mental health and substance abuse services. Case management will be provided as necessary. Any and all of these services will follow the family or individual into permanent housing and will be available as long as necessary, even indefinitely. (Although HUD funding currently limits such follow up to six months.) An excellent example of a Housing First program opened on April 29, 2005. St. Bede’s permanent housing program at 2700 Flagler Avenue in Key West, offers permanent supportive housing for ten elderly and/or disabled chronically homeless

24
adults. The Don Moore Apartments is another Housing First model. This housing program is sponsored by the Monroe Association for Retarded Citizens and provides twelve developmentally disabled homeless individuals with immediate permanent housing and supportive services for an indefinite period of time in order to make sure that they stay housed. AIDS Help recently acquired site control, under a long-term lease agreement with the City of Key West, for a piece of land at Poinciana Plaza specifically set aside for homeless housing. The “Helping Hands Housing Project” envisions the construction of up to 50 Housing First/Housing Plus 500 sq. ft. modular units for homeless individuals with HIV/AIDS. Agencies operating transitional housing programs at Poinciana, especially the Florida Keys Outreach Coalition, with its 120-transitional beds in five buildings, have begun to explore the feasibility of converting some of those transitional units into Housing First permanent units. While this plan will not mandate that existing shelter programs transition into Housing First, this plan does recognize that over the course of ten years, as current shelter residents are moved into permanent housing, the need for emergency and transitional shelter is expected to be reduced. Existing emergency shelters and transitional housing facilities will revise their programming in order to better serve our homeless population. The wide range of services currently in place will be better coordinated and expanded to ensure that the formerly homeless people remain in their housing units.
Short-Term Strategies (2005 to 2007) for Implementing Housing First
1. Provide Housing First accommodation for chronic elderly and disabled homeless in St. Bede’s Housing Project sponsored by Catholic Charities. Participants to be selected by a committee of community representatives and members of SHAL.
2. Support and assist AIDS Help in creating at least 10 new Housing First units for homeless men and women living with HIV/AIDS.
3. Support and assist Samuel’s House and other providers in proposals to create new Housing First units for women and women with children throughout the Keys.
4. Develop a plan for creating at least 5 Housing First units for families and an additional 10 for individuals each year.
5. Maximize use of existing funding sources, especially Florida State’s Homeless Housing Assistance Program and HUD’s Samaritan Initiative to create new permanent housing for the chronically homeless.

25
Long-Term Strategies for Continued Implementation of Housing First 1. Create new permanent supportive housing units with project based housing subsidies
for homeless persons with serious and persistent disabilities. 2. Create Single Room Occupancy (SRO) units for permanent housing for
unaccompanied adults (shared living facility). 3. Utilize existing housing markets by making public housing more accessible and
affordable and working with landlords toward further acceptance of rental subsidies. 4. Use local public funding to create or subsidize more housing units for homeless
individuals, families, and youth. 5. Develop more rental subsidies utilizing tax incentives (with covenants). 6. Develop appropriate Housing First models for intact homeless families. 7. Initiate intensive outreach for homeless populations, particularly campers in our
environmentally sensitive areas throughout the Keys. 8. Landlord education on homelessness and services available to the homeless. 9. Fund and construct an additional upper level on some of the 11 homeless special
needs buildings at Poinciana Plaza for use as permanent housing. 10. Seek ROGO exemption for affordable housing. 11. Release additional ROGO permits based on permanent residency. 12. Create a land trust to funnel funds to purchase land. 13. Identify vacant commercial properties potentially convertible to residential housing. 14. Explore Habitat for Humanity Involvement. 15. Consider easing height restrictions and density in some areas. 16. Link developer incentives to long-term affordable housing requirement (deed
restrictions) with enforcement. 17. Find ways to work with developers and landowners to build affordable housing.

26
Myth: Homeless people are a fixed population who are usually homeless for long periods of time.
Fact: The homeless population is quite diverse relative to their length of homelessness and the
number of times they cycled in and out of homelessness. SHAL’s 2005 homeless census
revealed that 25% of the homeless were homeless one week or less, 5% were homeless more than one week but less than one month, 7.5% between one and three months, 15.7% more than three months but less than a year, and 48.3% were homeless for one year or longer, meeting HUD’s definition of
chronically homeless.

27
SUPPORTIVE SERVICES Housing Plus Housing Plus, also known as wrap-around or supportive services, is the key to keeping a formerly homeless person or family in housing. These supports include: Affordable health care with mental health and substance abuse services; livable wage employment and/or other income supports; and for families, childcare. The Housing First approach is a comprehensive service provision model that guarantees that any and all services needed by an individual or family are integrated through a cohesive, individualized service plan that guides a service provision. This service approach should be used in all components of the homeless service delivery system. Currently, service referral is a component of most homeless service providers, but in the absence of more active and integrated case management, referral-based case management often results in fragmented care, and fails altogether when the homeless person does not persist in seeking it. The implementation of a wrap-around services approach will mean that case managers across agencies must work together to develop one plan of action, with each agency contributing, according to its strengths and resources, to support the individual or family in achieving housing stability and long-term self-sufficiency, with or without the client’s active cooperation. Because service intensity is determined upon client need, this may mean that initially an agency provides daily or weekly contacts, which may shift to monthly or on-call assistance for an extended period of time. For some, service will always remain an integral part of the residential environment. For others, this support will be transitional, sufficient to ensure that employment and community based resources, such as health care, schools, social services, civic organizations, and communities of faith are secured.
Short-Term Strategies (2005 – 2007) for Implementing Housing Plus:
1. Create a designated local revenue stream to support the Homeless CoC. 2. Fund and implement HMIS. 3. Pursue all available state and federal funding including, but not limited to, taking
aggressive steps to have HUD appropriate an adequate level of funding under the Supportive Housing Program and the Samaritan Initiative by adjusting Monroe County’s “pro-rata need” determination.
4. Appoint a task force to explore possible establishment of a Health Center for the Homeless (HCH).
5. Identify funding sources for homeless health care.

28
Long-Term Strategies to Implement Housing Plus:
1. Expand the provision of community based case management services that embody a wrap-around services approach with a team of people who provide site visits, medication intervention, shopping and other intervention services.
2. Develop formal systems integration strategies between the Housing First system and the main stream service systems, such as public entitlements (TANF, Medicaid, Social Security and Food Stamps), employment training and placement, public health, community mental health and substance abuse, to ensure that formerly homeless individuals and families have streamlined access to the array of formal supports available in the community at large.
3. Establish a working group to identify alternative resources to fund targeted supportive services for persons with severe and permanent disabilities and/or substance abuse disorders placed in supportive permanent housing. Priorities should include: Funding for services for substance abuse disorders, and development of a wide range of teams offering population-appropriate services.
4. Initiate planning for an emergency detoxification center for homeless people in conjunction with law enforcement.
5. Prepare homeless people for discharge from institutions to permanent housing and supportive services.
6. Coordinating with health providers so that non-emergency services are available 24/7. 7. Purchase property in Miami-Dade, i.e. Homestead, to initiate housing plus. This
would also provide affordable housing for the staff needed to manage housing plus. 8. Provide housing through the county land trust where people can lease to own, with
the objective to own the property within ten years.
29
Looking forward to 2015: Ten years from now the KEYS for Housing the Homeless plan should be complete. What will be the results? No homeless people living on the streets, in camps, under bridges, on beaches, on
derelict vessels, etc. Sharply reduce the number of dormitory style emergency or transitional shelter beds.
Thousands of formerly homeless individuals and families living independently with varying levels of support services.
Day programs offering social activities for the disabled and elderly. Transitional housing for individuals and families who are temporarily homeless
because of economic crisis, family breakdown or abuse. Multiple entry points into a system with coordinated services for people who become
homeless or need help to prevent homelessness. Measurably reduced burden on courts, police, jail, EMS, and emergency rooms
throughout Monroe County, including an established homeless court and health center for the homeless (HCH).
Integration of HMIS with a county-wide 211 system. Availability of detoxification beds for the homeless. Accessible county-wide health care for the homeless.
"There is a troubling misconception in our community about our
local homeless population. The most visible individual may be the aggressive panhandler on Duval Street.
However, we must remember that a majority of our homeless work
in our restaurants, construct our buildings, and landscape our properties and are therefore tightly woven into the social fabric of
Key West.
The implementation of a long-term plan to end homelessness is not only something a humane and just society should do, but will allow us to better utilize the abilities of our city's greatest resource - its
people." Hon. Jimmy Weekley Mayor of Key West

30
Keys to Housing the Homeless Approach Matrix
Homeless Group Approach Strategies A. Those who lose a job or roommate, divorce, get sick
Closing the front door - Prevention
Rent or mortgage payments Housing placement Move-in assistance Landlord education
B. Those released from jails, mental hospitals, foster care, etc.
Closing the front door - Prevention
Assure those released from mainstream institutions are housed not homeless
Homeless court and legal assistance
Same as A above C. Transitionally (short-term) homeless
Opening the back door – Housing First
High-demand emergency housing and services
Assess service eligibility Job training and placement Create worker SROs Develop affordable apts More rental subsidies
D. Domestic Violence Victims
Opening the back door – Housing First
Secure abuse shelter See C above
E. Chronic homeless who are willing and able to work
Opening the back door – Housing First
Homeless court Case mgt. & monitoring 2nd story on Poinciana See C above
F. Chronic and episodically homeless who are willing and able to work but need supportive housing
Opening the back door – Housing Plus
Create new supportive housing
Affordable basic and mental health & abuse services
G. Chronic homeless who are not willing and able to work
Opening the back door – Housing Elsewhere
Low demand “wet” facility Send to home community Send to lower-cost facility

31
A COVENANT OF PARTNERSHIP TO END HOMELESSNESS
Southernmost Homeless Assistance League, Inc. Monroe County, Florida
The Board of Directors and membership of the Southernmost Homeless Assistance League (SHAL) and our other Covenant Partners reflect a diverse array of stakeholders including the public, private, non-profit, and faith-based sectors, as well as representation from the homeless population residing in Monroe County. As Covenant Partners, we hereby commit to a leadership role in a countywide collaborate effort to end homelessness, particularly chronic homelessness within ten years. Now, as leaders in this initiative to end homelessness, we declare our intention to strengthen our partnership with one another to this end. We will aggressively explore and implement strategies that will create a visible, measurable, and quantifiable reduction of chronic homelessness on our streets, in our programs, and in our shelters with the intent of ending this national disgrace.
Our objective is to hasten the achievement of our collective goal by establishing successful, replicable
practices that lead to ending homelessness countywide.
We will pursue in common efforts to reduce homelessness in our community.
• We will be guided by research and data, results and performance. • We will seek the most innovative initiatives in cities across our country and the world.
We will serve as leaders for other communities that seek to follow our example. • We will commit to creating strategies to reduce deaths of homeless people and prevent
violence from being perpetrated upon them. • We will ensure that the chronically homeless are prioritized in our individual
and collective efforts.
To advance these efforts, we covenant with one another: • To design a common methodology for conducting repetitive counts of street homelessness,
to establish a baseline number, to monitor results, and to share that information with each other; • To implement and participate in a web-based Homeless Management Information System (HMIS) • To advance productive partnerships that establish a central, cross-agency record
of persons experiencing homelessness, their involvement with public and private agencies, and the resources that can assist with their housing placement;
• To share with one another on a regular basis our progress in placing persons experiencing homelessness into housing;
• To develop and maintain mental health, substance abuse, life skills, and other resources that engage and support individuals and end homelessness;
• To test and advance new messages to reframe the issue of homelessness in our community through a coordinated public education/communications campaign; and
• To meet monthly to review our progress in achieving our goal and to study together the latest developments that will support our direction and commitment.
We further covenant to assist each other in implementing these measures; to report openly on our learning and progress; to explore other complementary and replicable strategies to prevent and end homelessness; and to welcome additional partners into our collaboration.

32
Keys Community-Homeless Covenant Partner Expectations Participation in the Keys Community-Homeless Partnership is based, in part, on these desired outcomes. These expectations guide partnership strategies and provide a basis for evaluating the success in addressing the interests of each partner. The Homeless’ Partnership Expectations
1. Ability to perform life sustaining functions without breaking the law 2. Privacy, security and respect 3. Lifestyle freedom 4. Convenient to shopping and other services 5. Access to jobs and job training 6. Community tolerance of homelessness and assistance, rather than resistance. 7. Relocation assistance 8. Help with security deposits 9. Access to physical, medical, substance abuse and mental health services 10. A living wage 11. An address they can use to receive services 12. Education about services 13. Food 14. Translation for foreign speakers 15. Removal of suitability impediments (legal, credit, rent issues, etc.). 16. Address special needs of homeless children 17. Child care 18. Transportation 19. Access to a continuum of housing 20. Address youth aging out of foster care
Residents’ Partnership Expectations
1. Less loitering, panhandling and other undesirable behavior 2. Minimize negative personal experiences with the homeless 3. Protection of property values 4. Protection of the environment 5. Ability to use the park and beach without intimidation
Business Interests’ Partnership Expectations
1. Improved image of the Keys 2. Education, training, hygiene/healthcare, self-esteem and housing services for the
homeless so they can be working members of our community 3. Less loitering and panhandling 4. Minimize negative customer experiences with the homeless 5. No harassment of employees 6. Limit homeless living in parks, etc.
33
7. Clean up of human wastes (odors) in public spaces. 8. Opportunities for productive involvement in helping the homeless, e.g. providing
affordable housing for their own employees and in-kind services 9. Seeing a business plan showing how resources are efficiently used to produce
measurable results
Homeless Service Providers’ Partnership Expectations
1. Community is educated about homelessness 2. Homeless people are given respect 3. Needed services are available and affordable 4. Adequate (more) funding for programs 5. Identify sources of funds 6. Facility and services for mental health cases that do not meet existing program’s
criteria, e.g. person with mental problems that can’t be “Baker acted” 7. Partners with more business experience 8. Agreement with other counties to provide services for special needs, e.g. utilize
Dade County programs. 9. Service locations that are convenient for the homeless 10. Need providers in the upper keys 11. Homeless people are aware of services available to them 12. Homeless people trust they can obtain services without harassment 13. Community link of services via Homeless Management Info. System, HMIS
General Service Providers’ Partnership Expectations Hospitals, EMS, DOH, DCF, School Board, Housing Authority, employment assistance, etc.
1. Reduced demand for indigent services 2. Coordinated service delivery 3. Community link of services via Homeless Management Info. System, HMIS
Law Enforcement’s Partnership Expectations
1. Enforceable laws (can offer shelter as required by the Pottinger case) 2. Violations are minimized 3. Actions are supported by residents, businesses and the homeless 4. Incarceration and prosecution time and expense minimized 5. Services are accessible and are used by homeless people without being forced by
police action. 6. Need solutions to the homeless problem to reduce case load 7. Involvement of law enforcement in developing strategies for dealing with the
homeless, representation at the table 8. Training in protocols for dealing with the homeless 9. A designated liaison between homeless programs and law enforcement

34
10. Include criminal background checks with homeless intake process, with the exception of at KOTS.
11. Support for substance abuse treatment to reduce violations. 12. Coordinate medical and mental health treatment to save everyone money 13. Help people access Medicaid, Medicare, Food Stamps, TANAF and other
mainstream benefits. 14. Immediate stress relief for police officers 15. A directory of homeless services that officers can give out 16. Provide education about the difficulties of being homeless in the keys, i.e.: costs
of living 17. Homeless court on legal and mental health issues 18. Assistance with Baker Act and Marchman Act situations
County and City Governments’ Partnership Expectations
1. Fewer “homeless” related complaints 2. Minimize impacts on visitors, residents and businesses 3. Establish a reputation for humane, successful treatment of the homeless 4. Minimize time and cost of addressing homeless related problems 5. Minimize problems and liability through careful provision of services 6. Funding for homeless services, including Homeless Management Information
System, HMIS 7. Ability to raise funds from new sources without being penalized by other funding
sources. 8. Environmental protection 9. Homeless people and residents of Monroe County are more compassionate toward
each other 10. Specific legislation allowing funding formula adjustments that currently make it
difficult for Monroe County to compete for funds, e.g. rent limits 11. Collaboration of agencies, including providing a consistent message and
coordinated state and federal funding requests 12. More flexibility to use federal land for homeless facilities 13. Hurricane evacuation 14. Ability to provide different solutions for situational and chronic homeless

35
Keys Community-Homeless Covenant Partner Responsibilities Everyone will:
1. Be advocates for their own needs and help others and the community as a whole. 2. Share responsibility for shared action and share the impacts. 3. Allow homeless persons to perform life-sustaining activities without breaking the
law. 4. Provide alternative housing facilities so the homeless can legally be removed
from the street when warranted. 5. Protect the sensitive environment of the Keys. 6. Help the homeless become working contributors to the local economy. 7. Insure all people in our community are able to live peacefully, without threat of
interference or violence. The Homeless will:
1. Not panhandle or interfere with business customers 2. Not trespass on private property 3. Not litter or damage public property 4. Take responsibility for maintaining good physical and mental health 5. Contribute to the community through paid or volunteer work 6. Take as much responsibility as possible for shelter and service costs 7. Relocate if not willing to comply with the community covenant
Homeless Service Providers will: (Government, religious, non-profit, private; homeless programs and facilities)
1. Provide for basic food, hygiene and low demand temporary shelter 2. Provide emergency shelter, transitional and permanent housing and sanitary
facilities 3. Provide screening for needed services and assistance 4. Provide physical and mental health, educational and job referral services 5. Help those who want to leave with transportation and housing/service referrals 6. Share the costs, benefits and responsibilities; across the County and across the
government, business, non-profit and residential sectors General Service Providers will: (New Category with suggested responsibilities) Hospitals, EMS, DOH, DCF, School Board, Housing Authority, employment assistance
1. Provide services in ways that address the special needs of the homeless 2. Coordinate efforts with other Covenant Partners 3. Provide input to the homeless data base, HMIS
36
Businesses will
1. Employ the homeless who are qualified 2. Provide training as appropriate 3. Provide the homeless with information on the compact and services available 4. Support and provide funding needed to implement the community compact 5. Provide employee housing when possible
Residents will
1. Treat the homeless with respect and compassion 2. Provide the homeless with information on the Homeless Compact and services
available 3. Support and provide funding needed to implement the community compact 4. Volunteer and be mentors through religious and non-profit groups.
Law enforcement will
1. Provide training for officers and others 2. Comply with protocols (Pottinger) for interacting with the homeless 3. Enforce panhandling, decency and environmental laws if the homeless are not
willing to go to available shelters
SHAL will: 1. As the lead agency, update the Continuum of Care and ten year plan for public,
non-profit and private efforts 2. Coordinate efforts to work with the homeless 3. Review the overlap of services 4. Develop and implement HMIS 5. Educate the public and government on homeless concerns 6. Coordinate advocacy for adequate funding 7. Monitor legislative activity
Local government leaders will:
1. Partner with service providers to insure success of cost effective, community sensitive homeless services to avoid having a program imposed on Monroe County
2. Adopt an open, fair, facility site selection process and support the results if conducted appropriately
3. Seek outside funding to minimize the cost to local taxpayers 4. Provide incentives for neighborhoods who are impacted by facilities 5. Promote new innovative affordable housing opportunities throughout Monroe
County