key findings of air pollution health effects and its...
TRANSCRIPT

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Key findings of air pollution health effects and its application
Recent results from the WHO systematic review
Jürgen Schneider Jürgen Schneider Project MangerProject Manger
WHO ECEH, Bonn, GermanyWHO ECEH, Bonn, Germany
CAFE Steering GroupCAFE Steering Group(Brussels, 17(Brussels, 17--18 May 200418 May 2004))

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Content
•• IntroductionIntroduction•• Findings Findings •• OutlookOutlook
CAFE Steering GroupCAFE Steering Group(Brussels, 17(Brussels, 17--18 May 200418 May 2004))

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Published reports: Health aspects of air pollution with particulate matter, ozone and nitrogen dioxide Health aspects of air pollution – answers to follow-up questions form CAFEMeta analysis of time-series studies and panel studies op particulate matter and ozone
In preparation:Impact of air pollution on children’s health (2nd draft internally available)Short summary report (in preparation)
Complementary are the reports on the 6th and 7th meetings of thejoint WHO/UN ECE Task Force on Health
Introduction - Products

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Process:
Background document on epi evidence
Background document on tox evidence
Draft answersincl rationale
Review and revisions by
SAC
External peerreview
WHO WG meeting
Revision and additional
review
Finalisation, editing, print
WHO Review - process
WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
A full risk assessment comprises:
Hazard identification: Review of relevant evidence (epidemiologic, toxicologic, etc. to determine wether the agent poses a hazard
Exposure response function: Quantifying the relationship betweenexposure and adverse health effects
Exposure assessment: Determination of the magnitude, duration androute of exposure
Risk characterication: An integration of the above three leads to an estimation of the health budren of the hazard. The approach, assumptions and uncertaintiesshould be highlighted
Key findings

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Key findings
Hazard identification
• Short term versus long term• Hot spot versus urban background• Epi versus tox evidence (susceptibility)• Thresholds for ozone• WHO AQG for NO2• Coarse PM• (Other pollutants)

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key finings
Relevance of exposure to peaks versus long term
Peak versus long-term:Ozone: ‘As there are usually many more days with mildly elevated ozone
levels than days with very high peaks, the largest burden of disease might be expected with the many days with mildly elevated levels and not with the few days with very high levels’
PM: ‘…the public health significance of the long-term effects clearly outweighs the public health significance of the short term effects. This obviously does not diminish the significance of the short-term effects of PM, which consist of very large numbers of attributable deaths and cardiovascular and respiratory hospital admissions in Europe.’

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Relevance of exposure at hot spots; exposure to peaks - Hot-spot versus urban background
• A policy which aims at a significant reduction of the overall health burden caused by air pollution will have to aim at a reduction of the exposure of the general population. This is in particular true for pollutants/health endpoints with (a) no threshold of effects and (b) a linear relationship between exposure and response.

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Relevance of exposure at hot spots; exposure to peaks - Hot-spot versus urban background
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
10 15 20 25 30 35 40 45 50 55
PM10 µg/m3, JMW
Pop
ulat
ion
expo
sed
base case No exceedance'General reduction

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Relevance of exposure at hot spots versus urban background
• However, some studies have documented that subjects living close to busy roads experience more short-term and long-term effects of air pollution than subjects living further away. In urban areas, up to 10% of the population may be living at such “hot spots”. The public health burden of such exposures is therefore significant. Unequal distribution of health risks over the population also raises concerns of environmental justice and equity.

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Consistency of epi and tox evidence in the defining thresholds - General remark
• For a uniform population with specific exposures, thresholds for certain pairs of pollutant/health endpoints may be detectable
• At a population level, susceptibility and exposure vary over a wide range. Large differences in individual exposure-response curves may lead to a disappearance of thresholds at a population level.
Taking into account these differences, the evidence coming from the epidemiological and toxicological studies is not contradictory.

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Consistency of epi and tox evidence in the defining thresholds - PM
• Most epidemiological studies on large populations have been unable to identify a threshold concentration below which ambient PM has no effect on mortality and morbidity. It is likely that within any large human population, there is a wide range in susceptibility so that some subjects are at risk even at the low end of current concentrations.

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Consistency of epi and tox evidence in the defining thresholds - Ozone:
• Statistical significant associations between ozone and mortality have been demonstrated at places with low ozone levels
• Sophisticated statistical analysis applied to address the question of thresholds for PM have not been applied to the same degree for O3
• There remain uncertainties about the shape of the CR function, in particular at the lower end of the ambient range
• Although there is evidence that associations exist well below the current guideline value, the confidence in the existence of associations with health outcomes decreases as concentrations decrease.

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Consistency of epi and tox evidence in the defining thresholds - Ozone:
A recent paper (Kim et al., 2004) applied a linear model, a natural spline model and a threshold model to a dataset in Seoul and found that the threshold model, with a threshold at 56 µg/m3 (28 ppb) 1 hour average for effect son mortality, gave the best fit. However, the slope above the threshold was steeper than in the linear model. The authors conclude: that models that not take thresholds into consideration, could underestimate the true risk of ozone effects on mortality.
L e v e l s L e v e l s
E f f e c t s E f f e c t s

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Contribution of different sources to PM related health effects
Epi studies: Combustion sources are particularly important for health effects. Tox studies:• Primary, combustion-derived particles have a higher toxic potency. These
are often rich in transition metals and organics, in addition to their relatively high surface area
• Other single components of the PM mix are lower in toxicity in laboratory studies e.g. ammonium salts, chlorides, sulphates, nitrates and wind-blown crustal dust such as silicate clays.
Despite these differences among constituents studied under laboratory conditions, it is currently not possible to quantify the contributions from different sources and different PM components to health effects from exposure to ambient PM.

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Coarse particles and health
• There is limited evidence that coarse particles are associated independently of PM2.5 with mortality in time series studies.
• One study has investigated the effect of long-term exposure to coarse particles on life expectancy without producing evidence of altered survival.
• There is evidence that coarse particles are independently associated with morbidity endpoints such as respiratory hospitalizations in time-series studies.
There is sufficient concern about the health effects of coarse particles to justify their control.

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Basis for maintaining the WHO AQG for NO2
• New toxicological studies show that LT exposure to NO2 at concentrations higher than current ambient concentrations have adverseeffects.
• Uncertainty remains over the significance of NO2 as a pollutant with a direct impact on human health at current ambient air concentrations
• NO2 has been associated with adverse health effects even when theannual average NO2 concentration is within a range that includes 40 µg/m3
It is recommend that the WHO annual specific guideline value of 40 µg/m3
should be retained or lowered.
WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings
Effects of air pollution on children’s health
• There are several factors which potentially increase children’s susceptibility to adverse effects of air pollution
• There is solid evidence for effects of air pollution (PM) on infant mortality
• Poor air quality effects lung development of children • Air pollution is associated with increased upper and lower respiratory
symptoms in children• Air pollution may increase bronchitis, cough and aggravates asthma
symptoms• There are uncertainties whether ambient air pollution at current levels
causes cancer in children

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
The evidence is sufficient to recommend strongly furtherpolicy action to reduce levels of air pollutants includingPM, NO2 and ozone; it is reasonable to assume that a reduction of air pollution will lead to considerable healthbenefits.
Systematic Review – key findings

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key finings
Meta-analysis of time-series studies
• Set-up of a Task Group upon recommendation of a WHO WG• Development of a strict protocol• Bibliographic database of time-series studies at St. George’s
Hospital/London• Summary estimates for different health outcomes related to PM and
ozone• Outcome in RR per 10 µg/m3 increase in pollution level• Analysis of possible publication bias

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key finings
European studies on ozone and and all-cause mortality
Bar
celo
na
Mad
rid
Val
enci
a
Le H
avre
Lyon
Par
is
Rou
en
Stra
sbou
rg
Toul
ouse
Wes
t Mid
land
s
Lond
on
Net
herla
nds
Am
ster
dam Rom
e
Turin
Sum
mar
y es
timat
e
0.97
0.98
0.99
1
1.01
1.02
1.03
RR
for a
10
µg/m
3 in
crea
se in
dai
ly o
zone
leve
ls

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key finings
RR for all-cause mortality – PM and ozone
Relative risks (RR) for mortality endpoints related to a 10 µg/m3 increase in pollution including 95 % confidence intervals; left part: PM10, black smoke (BS) and ozone from European studies; right part:
PM2.5 from North American studies
all c
ause
resp
irato
ry
card
iova
scul
ar
all c
ause
resp
irato
ry
card
iova
scul
ar
all c
ause
resp
irato
ry
card
iova
scul
ar
all c
ause
resp
irato
ry
card
iova
scul
ar
0.99
0.995
1
1.005
1.01
1.015
1.02
1.025
1.03PM10 BS Ozone PM2.5
European studies American studies
RR

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key finings
RR for all-cause mortality – publication bias
Relative Risk for all-cause mortaility, 10 µg/m3 increase inpollution level, without and with correction for publication bias
all c
ause
all c
ause
cor
r.
all c
ause
all-c
ause
cor
r.
all c
ause
all-c
ause
cor
r.
0.999
1.001
1.003
1.005
1.007
1.009
RR
PM10 BS Ozone
WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key finings
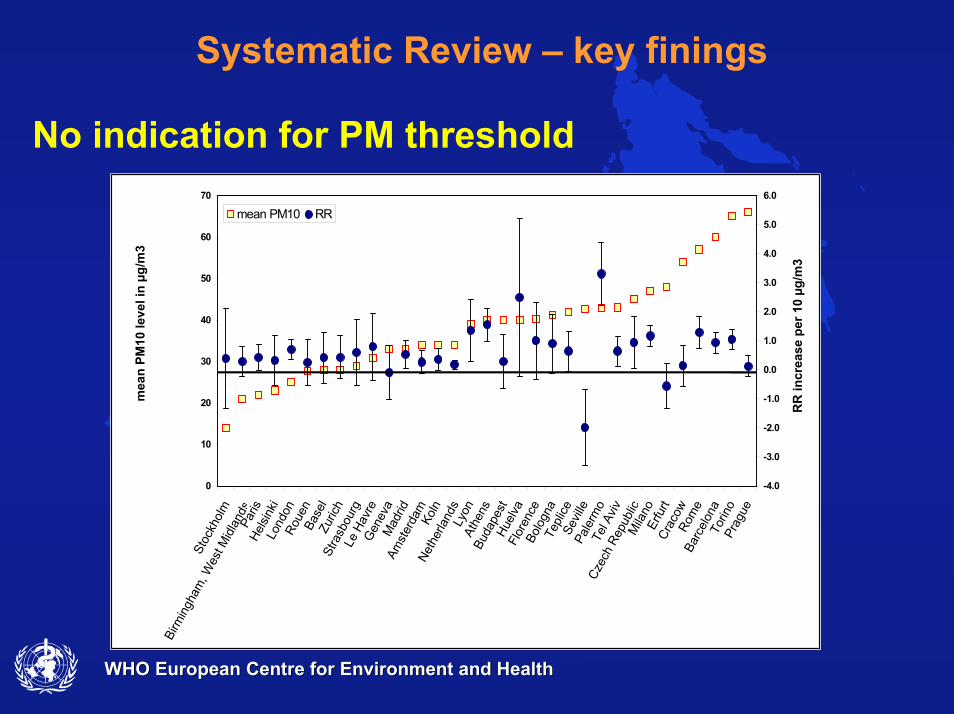
No indication for PM threshold
0
10
20
30
40
50
60
70St
ockh
olm
Birm
ingh
am, W
est M
idla
nds
Paris
Helsi
nki
Lond
onRo
uen
Base
lZu
rich
Stra
sbou
rgLe
Hav
reG
enev
aM
adrid
Amst
erda
mKo
lnNe
ther
land
sLy
onAt
hens
Buda
pest
Huel
vaFl
oren
ceBo
logn
aTe
plice
Sevil
lePa
lerm
oTe
l Aviv
Czec
h Re
publ
icM
ilano
Erfu
rtCr
acow
Rom
eBa
rcel
ona
Torin
oPr
ague
-4.0
-3.0
-2.0
-1.0
0.0
1.0
2.0
3.0
4.0
5.0
6.0
mean PM10 RR
mea
n PM
10 le
vel i
n µg
/m3
RR
incr
ease
per
10
µg/m
3

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – key findings

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Develop recommendations on the approach to model health impacts within RAINS
Health impact assessment: Science-basedNo cookbook approach yetSeveral assumptions and choices – transparency is needed‚Conservative approach‘CBA complementory
7th Meeting of the TF Health

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Ozone effects:
Health endpoint: attributable mortalityCausal relationship between ozone exposure and mortalityIndependent of PMRR from WHO meta-analysis of European studies:The relative risk for all-cause mortality is 1.003 (C.I. 1.001, 1.004) for a 10 µg/m3 increase in the daily maximum 8-hour mean.
7th Meeting of the TF Health - Ozone

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Ozone effects:
A linear concentration response function is assumed. The principle metric for assessing effects of ozone on mortality should be the daily maximum eight-hour mean. Current evidence is insufficient to derive a level below which ozone has no effect on mortality. The use of a cut-off for IAM at 35 ppb is recommeded
7th Meeting of the TF Health - Ozone

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
0
10
20
30
40
50
60
70
80
daily
max
8-h
r mea
n
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36
0
10
20
30
40
50
60
70
80
daily
max
8-h
r mea
n
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Why use a cut-off?
There remain uncertainties about the shape of the CR function, in particular at the lower end of the ambient range
20 to 40 ppb is the hemispheric background – main purpose is to analyseEuropean abatement optionsThere are difficulties of state-of-the-art dispersion models to simulate low ozone situations in urban areas. Titration becomes important at low levels
Ozone

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
This recommendation is based on the application of a very conservative approach for integrated assessment modelling and takes account of uncertainties in relation to the evidence in health studies and lowerconfidence in model performace at low ozone levels. It is recommended to make a sensitivity analysis applying no cut-off. This estimate would outline an upper estimate of the attributable effects of ozone on mortality.
The Task Force also stressed that the approach did not yield an overall quantification of all effects related to exposure to ozone. Important effects which were currently not covered, but should be taken into account in CBA, including morbidity outcomes.
Ozone

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Ozone
Levels Levels
Effects Effects

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Particulate matter
PM effects:Use annual mean of PM2.5 as indicator for PM related mortality (this also implies the use of one factor for different PM constituents)RR from cohort studyLinear CR function Health outcome: Reduction of life expectancyEffect for explained anthropogenic contribution only
‘Most epidemiological studies on large populations have been unable to identify a threshold concentration below which ambient PM has no effect on mortality and morbidity. It is likely that within any large human population, there is a wide range in susceptibility so that some subjects are at risk even at the low end of current concentrations.’

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
Systematic Review – outlook
Follow-up actions
• Finalisation of the reports• Dissemination of main results• Keep contact with CAFE• Revision of WHO Air Quality Guidelines (PM, ozone)

WHO European Centre for Environment and HealthWHO European Centre for Environment and Health
For further information see:
http://www.euro.who.int/air
CAFE Steering GroupCAFE Steering Group(Brussels, 17(Brussels, 17--18 May 200418 May 2004))