kevin b. spicer, md, phd, mph antibiotic resistance ... · kevin b. spicer, md, phd, mph antibiotic...
TRANSCRIPT

Kevin B. Spicer, MD, PhD, MPHAntibiotic Resistance Coordinator, HAI/AR Program
Kentucky Department for Public Health

2
Objectives1) Explore relationship between antibiotic use and unintended
consequences2) Review antibiotic resistance, including mechanisms of
resistance3) Discuss importance of antimicrobial stewardship in all
healthcare settings4) Examine the core elements of antimicrobial stewardship,
with discussion of statewide facility data5) Discuss relationship between antimicrobial stewardship and
infection prevention & control

Common Types of Bacteria
Gram positive Most are cocci, “round bacteria” Streptococcus, Staphylococcus,
Enterococcus Clostridium difficile (C. diff) is a Gram
positive rod Gram negative Most are bacilli, “rod-shaped
bacteria” Enterobacteriaceae: E coli, Klebsiella,
Enterobacter, Proteus Pseudomonas, Acinetobacter
4
Terminology
Antibiotic Produced by an organism to kill, or inhibit growth of, another
organism
Antimicrobial Agent able to kill, or inhibit growth of, another organism (can be
natural or synthetic)
Antibacterial An antimicrobial directed towards bacteria
“Antibiotic” often used to refer to an antibacterial agent
“Antibiotics” 101
Antibacterials are grouped into classes based on their structure and activityNarrow-spectrum target a few specific bacteria Broad-spectrum can kill a wide variety of bacteria
Infection prevention programs track certain “bug-drug” combinations for evidence that the bacteria is getting resistantBacteria with resistance can cause patients to have more
severe, costly infections which are harder to treat

6
Time Magazine-Feb 25, 1966
“Nearly all experts agree that (by the year 2000) bacterial and viral diseases will have been wiped out. Probably arteriosclerotic heart disease will also have been eliminated.”

7
Antibiotic Use and Misuse in Hospitals
In a 2011 single-day point prevalence survey in roughly 200 Emerging Infection Program Hospitals, 50% of patients were receiving at least one antibiotic
Approximately 30% of antibiotic use in hospitals is unnecessary or inappropriate
Magill S et al. Oral Presentation Session 37, abstract 114, presented at ID Week 2012. San Diego, CA.

Unintended Consequences of Antibiotic Use
Antibiotic exposure is the single most important risk for Clostridium difficile InfectionsExposure to antibiotics increases the risk of C. diff infection by at
least 3 fold for at least a monthUp to 85% of patients with C. diff infection have antibiotic
exposure in the 28 days before infection
Antibiotics account for nearly 1 in 5 drug-related adverse events>140,000 ER visits/year due to adverse effect of antibioticsAdmission required for 6.1% of adverse events

Antibiotic Use Drives Resistance
Johnson et al. Am J. Med. 2008; 121: 876-84.
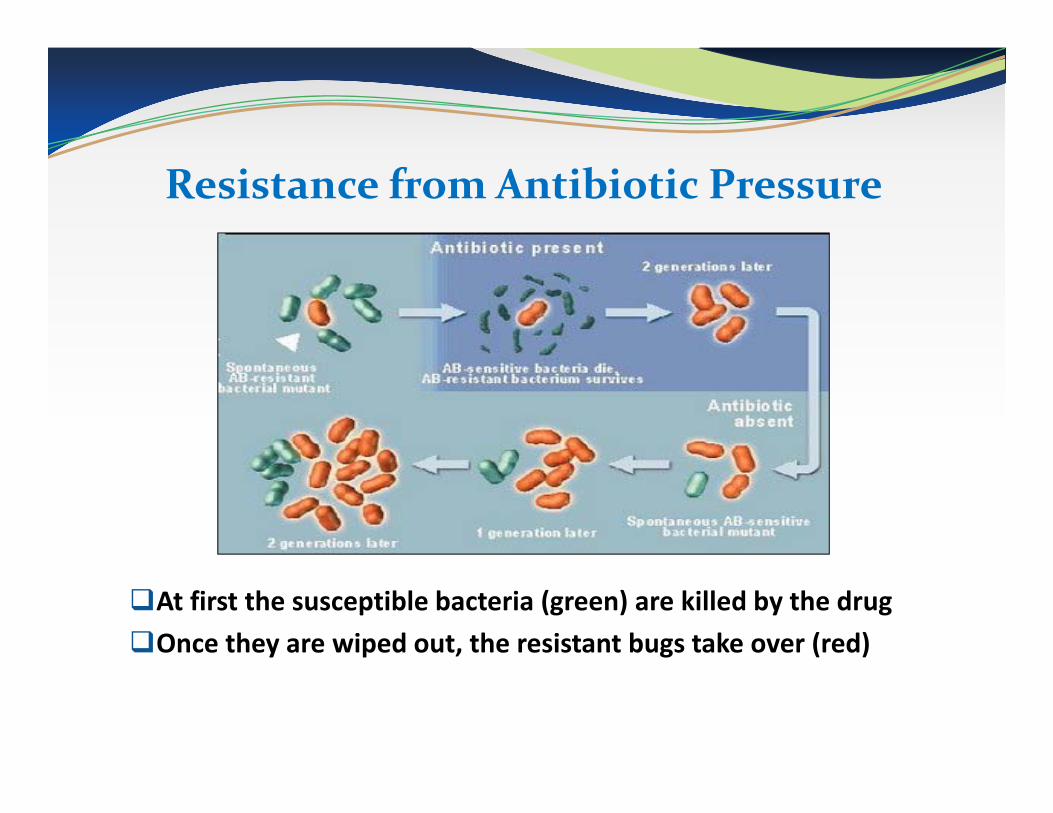
Resistance from Antibiotic Pressure
At first the susceptible bacteria (green) are killed by the drug Once they are wiped out, the resistant bugs take over (red)

11Science 2008;321:356-361.

12Science 2008;321:356-361.

Mechanisms of Antibiotic Resistance
Production of proteins that destroy antibioticsBeta-lactamasesCarbapenemases
Change their cell structure so antibiotics can’t bind and block their function
Reduce their antibiotic exposurePump drugs out Increase cell barriers to
keep drug outhttp://bioinfo.bact.wisc.edu/themicrobialworld/bactresanti.html
New York TimesFebruary 26, 2010
Rising Threat of Infections Unfazed by Antibiotics


History of Antimicrobial Use
2000 B.C. “Here, eat this root.”
1000 A.D. “That root is heathen. Here, say this prayer.”
1850 A.D. “That prayer is superstition. Here, drink this potion.”

History of Antimicrobial Use
1940 A.D. “That potion is snake oil. Here, take this penicillin; it’s a miracle
drug.”1985 A.D.
“Penicillin is worthless. Here, take this new antibiotic; it’s bigger and better.”
2010 A.D. “Those antibiotics don’t work any more. Here eat this root.”
2000 B.C. “Here, eat this root.”
1000 A.D. “That root is heathen. Here, say this prayer.”
1850 A.D. “That prayer is superstition. Here, drink this potion.”

Antimicrobial Resistance and Patient Outcomes
Increase in mortality, morbidity, length of hospitalization, and cost of careStaphylococcus aureusEnterococciGram-negative bacilli
Delays in therapy or severity of illness likely contribute to the worse outcomes
Cosgrove SE, CID, 2006;42 Suppl 2:S82-9.
Defining Multidrug-Resistance
Resistant to treatment by several antibiotics from unrelated classes
Sometimes just one key drug resistance will define an important MDRO, for example, methicillin-resistance in Staphylococcus aureus
Bacteria sometimes acquire resistance to several classes, often seen in Gram negative rodsCephalosporin-resistance is a big concern in bacteria like
E coli/Klebsiella which often cause UTIsPseudomonas can be resistant to fluoroquinolones,
penicillins, cephalosporins, and carbapenems

ABC’s of MDROsBacteria Abbrev. Antibiotic Resistance
Staphylococcusaureus
MRSA Methicillin-resistant
Enterococcus(faecalis/faecium)
VRE Vancomycin-resistant
Enterobacteriaceae(E coli/Klebsiella, etc)
CRE (KPC)
Carbapenem-resistant
Pseudomonas/Acinetobacter
MDR Many drug classes

21
Carbapenem-resistance in Gram Negative Bacteria
Growing threat in the treatment of infectionsBacteria in the family Enterobacteriaceae are commonKlebsiella spp. and E. coli are examples of
EnterobacteriaceaeColonize the human GI tractOften cause infections in both the community and
healthcare settingsCurrently CRE has been limited to people with high
exposure to healthcare
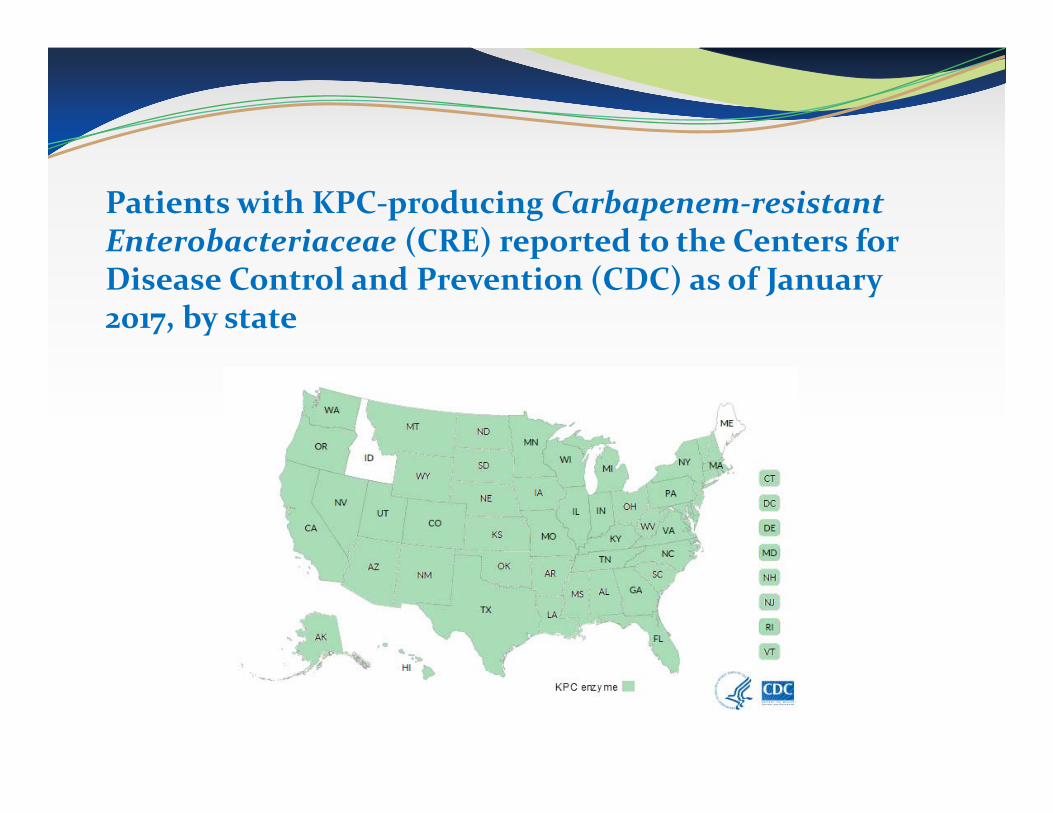
Patients with KPC-producing Carbapenem-resistant Enterobacteriaceae (CRE) reported to the Centers for Disease Control and Prevention (CDC) as of January 2017, by state

Patients with NDM-producing Carbapenem-resistant Enterobacteriaceae (CRE) reported to the Centers for Disease Control and Prevention (CDC) as of January 6, 2017, by state

Patients with VIM-producing Carbapenem-resistant Enterobacteriaceae (CRE) reported to the Centers for Disease Control and Prevention (CDC) as of January 6, 2017, by state

25
MDROs in the Healthcare Setting DEVELOPMENT Antibiotic pressure Most common predictor of antibiotic resistance is prior
exposure Device utilization Biofilm formation on central lines, urinary catheters, etc.
SPREAD Patient to patient transmission via healthcare workers Environmental / equipment contamination Role of colonization pressure on acquisition

“Good Antimicrobial Stewardship”
“is the optimal selection, dose, and duration of an antimicrobial that results in the best clinical outcome for the treatment or prevention of infection, with minimal toxicity to the patient and minimal impact on subsequent resistance.”
Gerding DN, Jt Comm J Qual Improv, 2001;27:403-4.
27
APIC-SHEA Position PaperAntimicrobial stewardship: a collaborative partnership between
infection preventionists and health care epidemiologistsAssist with early identification of infected patientsSurveillance of problematic organismsEmphasis upon compliance with standard and transmission-
based precautionsEducation and promotion of infection prevention strategies
Hand hygiene Care bundles Roles of staff, patients, and visitors in potential spread of
infections
Moody et al., Am J Infect Control, 2012;40:94-5.

28
Antimicrobial Stewardship and Infection Prevention
Complementary components to improving antimicrobial use and potentially limiting development of antimicrobial resistance
Infection control programs rely on stewardship programs toMinimize inappropriate and/or excessive antibiotic exposure Decreases likelihood that patients may acquire a multidrug-resistant
organismAntimicrobial stewardship programs rely on IPC programs to
Minimize spread of multidrug-resistant organisms between patients Decreases use of broad-spectrum antibiotics
Nagel et al., Infect Dis Clin N Am, 2016;30:771-84.

29
AID Stewardship Model
Antibiotic stewardshipInfection prevention stewardshipDiagnostic stewardship
Dik et al., Future Microbiol, 2015;11:93-102.

30
Infection Prevention Stewardship
Close surveillance of multidrug-resistant organisms (MDROs)
Early detection of infections with MDROsEmphasis of transmission precautions and limiting spread
of infections/organismsIncreased response with any possible transmission of an
MDROEnhanced intra- and inter-facility communication to limit
transmission of infections with patient movement
Dik et al., Future Microbiol, 2015;11:93-102.

What is Antibiotic Stewardship?A set of commitments and actions
designed to optimize the treatment of infections while reducing the adverse events associated with antibiotic use
Antimicrobial stewardship interventions can lead to: Improved individual resident outcomes Prevention of the emergence of
antibiotic resistance Saving healthcare dollars

32
Antibiotic Stewardship Programs
Antibiotic stewardship ensures that the patient only receives an antibiotic when needed AND the right drug, dose, and duration is prescribed
CDC recommends that all hospitals should have antimicrobial stewardship programsPrograms will look different in various hospitals,
depending on the size and complexity of the patient population
Fridkin SK, Srinivasan A. Clin Infect Dis. 2013 Oct 25.

Strategies and Challenges to Improving Antibiotic Use
Convince prescribers that their actions are linked to resistanceSurvey and focus group studyResistance was national problem more than
institutional or practice (95% vs. 77% vs. 65%)Convince patients and the public that their actions are
linked to resistanceState the vision for these activities as improving
rather than controlling or restricting use
Giblin TB et al., Arch Intern Med, 2004;164:1662-8.

Potential Benefits of Antimicrobial Stewardship
Decreased antimicrobial resistance More discriminate use of new agentsImproved quality of careImproved patient outcomes Improved physician educationCost containment

35
Eight Proposed Principles of Antibiotic Therapy
1) Antibiotics are prescribed only when there is clear rationale (e.g., clinical signs of a bacterial or fungal infection are present)
2) When empirical therapy is necessary (i.e., the organism has not been identified), reasonable, evidence-based prescribing guidelines are followed
3) Specimens are routinely sent for culture4) Antibiotic treatment is tailored promptly according to the laboratory results5) The appropriate dose is prescribed at the correct frequency of administration
(including continuous infusion when necessary)6) Antibiotic therapy is not prolonged unnecessarily7) Antibiotics with overlapping spectrum of activity are avoided unless there is
clear rationale8) The change from IV to oral therapy is made as early as possible
Best Care Always, 2011, http://www.bestcare.org.za/file/view/Antibiotic+Stewardship+Getting+Started+Guide+v1.pdf

Core Elements of Hospital Antibiotic Stewardship Programs
Leadership Commitment
Accountability
Drug expertise
Action to improve use
Tracking
Reporting
Education
http://www.cdc.gov/getsmart/healthcare/pdfs/core-elements.pdf

Core Contributors to Stewardship Programs (in addition to physicians and pharmacists)
•Risk assessment and prevention planning skills•Collect, analyze and report antibiotic-related data
Infection Preventionists
• Input into specimen collection and proper use of relevant tests
•Review information flow of results to clinicians•Create and interpret a facility antibiotic resistance report
Laboratory
•Review medications as part of their routine duties•Could contribute through prompting discussions of antibiotic
treatment, indication, and durationNursing
•Create ways integrate guidelines and policies with decision support at point of care
•Track antibiotic use through medication administration records
Information Technology (IT)

National Healthcare Safety NetworkAntibiotic Stewardship Programs
Stewardship questions were added to NHSN for first time in 2015 >4,000 hospitals
respondentsQuestions applied to
calendar year 2014cc
http://www.cdc.gov/nhsn/forms/57.103_pshospsurv_blank.pdf

NHMARICTNJDEMDDC
58%
19%
21%
50%
39% 13%
23%44%
VT55%
36%
36%
50%
52% 56%
54% 30%
37%
21%
24%
36% 38%41%
24%
43%29%
28%
21% 37%
49%
48%
41%
47%
50%
29%30%
29%
31%
35%
33%
29%
7 – 28%29 – 35%36 – 48%49 – 58%
42%
HIPR
33%
28%58%30%27%49%50%50%13%
7%
25%AK
Hospitals Meeting all Core Elements
Overall percentage was 39.2% (1642 of 4,184)
Data: NHSN 2015 Annual Facility Survey

29, 43%
15, 22%
24, 35%
2015 Core ElementsState Data
(68 facilities)
7
5,6
<5
Core Elements Met
Kentucky Hospitals Meeting Core Elements - 2015

41, 60%
18, 27%
9, 13%
2016 Core ElementsState Data
(68 facilities)
7
5,6
<5
Core Elements Met
Kentucky Hospitals Meeting Core Elements - 2016

KY – Medicaid Regions

9, 29%
11, 36%
11, 35%
2015 Core ElementsMedical Regions 1-4
(33 facilities)
75,6<5
CoreElements
Met
Hospitals Meeting Core Elements – 2015Medicaid Regions 1-4

18, 55%
9, 27%
6, 18%
2016 Core ElementsMedicaid Regions 1-4
(33 facilities)
75,6<5
CoreElements
Met
Hospitals Meeting Core Elements – 2016Medicaid Regions 1-4

20, 57%
4, 12%
11, 31%
2015 Core ElementsMedicaid Regions 5-8
(35 facilities)
75,6<5
CoreElements
Met
Hospitals Meeting Core Elements – 2015Medicaid Regions 5-8

23, 66%
9, 26%
3, 8%
2016 Core ElementsMedicaid Regions 5-8
(35 facilities)
75,6<5
CoreElements
Met
Hospitals Meeting Core Elements – 2016Medicaid Regions 5-8

Antimicrobial Use in NHs
Over 4 million individuals receive care in nursing homes/skilled nursing facilities (NH) every year The majority are coming directly from hospitals to receive
skilled nursing care/rehabilitation
Antimicrobials are frequently prescribed in NHs Over the course of a year, 50-70% of residents will receive a
systemic antimicrobial
25-75% of antimicrobial use in NHs may be inappropriate
Daneman N et al. JAMA Int Med 2013;173:673-82 Benoit et al. JAGS 2008;56: 2039-2044Nicolle LE et al. ICHE 2000;21:537-545

48
Nursing Homes are Reservoirs of MDROs
NH residents colonized with MDR-Gram Negative Rods (~20% prevalence)O’Fallon et al. Infect Control Hosp Epidemiol 2009; 30: 1172-1179
NH residents colonized with MRSA (40-50% prevalence)Mody et al. Clin Infect Dis 2008; 46(9): 1368-73 Stone et al. Infect Control Hosp Epidemiol 2012; 33(6): 551-7
NH residents colonized with VRE (5-10% prevalence) Pop-Vicas et al J Am Geriatr Soc. 2008 56(7):1276-80 Benenson et al. Infect Control Hosp Epidemiol. 2009 30:786-9

49
Long Term Care Facilities and Antimicrobial Resistance
Fewer or limited resources Personnel, including those devoted to infection prevention Laboratory/diagnostic services Access to prescribing medical providers Access to infectious disease consultation
Consequences of limited resources Potential increased misuse of antimicrobial agents Frequent transfer of residents to acute-care hospitals
Giannella et al., Exp Rev Anti-Infect Ther, 2016;14:219-30.

50
Nurses in LTCFs
Particularly influential in terms of antimicrobial use and resistance
Bedside careDecision to testEscalation to health care provider prescribers

Spotlight on Infection Prevention in NHs Sept. 2012 – CDC released the LTCF infection reporting
component within NHSN Oct. 2012 – Updated infection surveillance definitions for LTC
published by CDC/SHEA
April 2013 – Dept. of Health and Human Services (HHS) released the National Action Plan to Prevent Healthcare-associated Infections in LTCF NHSN reporting from nursing homes was #1 priority
Feb 2014 – Office of the Inspector General released report on adverse events and harms in skilled nursing facilities 1 in 5 post-acute residents experienced an adverse event within
the first 30 days of their admission

Spotlight on Antibiotic Stewardship in NHs
Sept. 2014 – The White House announces an Executive Order to develop an Action Plan to Combat Antimicrobial Resistance
March 2015 – The White House releases the National Action Plan for Combating Antimicrobial Resistance
Call to action for implementing antibiotic stewardship programs and activities in all healthcare settings, including long-term care
July 2015 – CMS proposes new Federal Regulations for Long-term care facilities including new infection prevention and antibiotic stewardship activities
September 2015 – CDC releases the Core Elements of Antibiotic Stewardship for Nursing Homes


Nursing Home Antimicrobial Stewardship Guide
The Agency for Healthcare Research and Quality recently updated its NH antimicrobial stewardship guide that includes toolkits on: Starting and monitoring an antimicrobial stewardship program Communication and decision making for suspected infections Using an antibiogramMaterials for resident and family engagement and education
http://www.ahrq.gov/nhguide/index.html

CDC Core Elements of Antibiotic Stewardship for Nursing Homes
Provide a framework for assessing current and new antibiotic stewardship activities, and for monitoring and improving antibiotic use: Leadership Commitment Accountability Drug Expertise Action Tracking Reporting Education
http://www.cdc.gov/longtermcare/prevention/antibiotic-stewardship.html

Nursing Home Core Elements: Appendix A
Evidence-based examples of policies, actions and interventions that to improve antibiotic prescribing
http://www.cdc.gov/longtermcare/pdfs/core-elements-antibiotic-stewardship-appendix-a.pdf

Other Partners Who Support Stewardship
Infection prevention and control coordinator: Tracking antibiotic starts as part of infection surveillance Monitoring adherence to evidence-based published criteria on
evaluation and management of infections Reviewing antibiotic resistance and CDI as part of surveillance
Consultant laboratory: Developing a process of notifying the facility if certain antibiotic
resistant organisms are identified Providing education for NH staff on use of diagnostic tests Creating a summary report of antibiotic susceptibility patters (i.e.,
antibiogram) State and local health departments:
Proving educational support and resources Engaging facilities in coordinated activities (e.g., stewardship
collaboratives) to promote shared learning

Education-Staff Provide education about antibiotic stewardship to clinicians and nursing staff
May be the first element implemented to establish support among staff Different mechanisms (flyers, newsletters..), strongest evidence for academic
detailing (i.e. face-to-face interactive workshops) Address staff concerns and barriers to changing antibiotic use practices
http://www.health.state.mn.us/divs/idepc/dtopics/antibioticresistance/asp.ltc/
http://www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/nh-aspguide/module1/index.htm
https://nursinghomeinfections.unc.edu/

Colonization versus Infection The presence of bacteria is normal and expected in certain parts
of the human body Especially those parts exposed to the environment Skin, nose, mouth, throat, intestinal tract, urogenital tract (especially
with older age) Medical devices allow bacteria access and increase risk of
colonization, e.g., urinary catheters and tracheostomies Many of the normal colonizing bacteria are helpful to our system
Digest and absorb nutrients; protect us from invasion from harmful bacteria (e.g., C. difficile in the GI tract)
Presence of bacteria in a culture specimen not necessarily indicative of infection Signs and symptoms of inflammation are important to distinguish
colonization from infection

Make Antibiotic Use Decisions Well-informed
Understand and address the knowledge, attitudes and perceptions of the clinical providers, staff and residents Promote antibiotic use guidelines and training Share provider specific antibiotic use data Educate and empower front-line NH staff Educate residents, families and NH staff on the risks of
antibiotic use

Evaluate the discrepancies between surveillance data and clinical/MDS data as a process improvement exercise
Ask for their input in identifying the reasons why events treated with antibiotics don’t meet surveillance (or other practice guideline) criteria
Identify ways to improve: Assessments Documentation Diagnostic testing Follow-up after antibiotics have been initiated
Explore the Gaps with Clinical Providers to Improve Antibiotic Use

Snapshot of Resistance Patterns: Facility Antibiograms
A yearly summary of the common bacteria from facility cultures and their susceptibility patterns to antibioticsAllows you to see trends in resistance over timeAsk your microbiology lab about it

TrackingMonitor at least one process measure and at least one outcome measure from antibiotic use in your facility
Prescribing process measures Adherence to documenting prescribing elements Completeness of resident assessment documentation Appropriateness of antibiotic selection (based on facility
guidelines) Antibiotic use measures
Point prevalence of antibiotic use Antibiotic starts/ 1,000 resident days Days of antibiotic therapy/ 1,000 resident days
Outcome measures C.difficile and multidrug-resistant organisms Adverse events and/or costs related to antibiotic use

Action-Broad Practice Improvements
Broad practice improvements Standardize the assessment of patients
suspected of an infection and the communication between onsite nursing and offsite providers Ask providers’ and nurses’ input on barriers
and opportunities for improvement Ensure staff is communicating all the
relevant data to make appropriate treatment decisions
Consider using Standard Assessment and Communication Tools i.e. SBAR
http://www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/nh-aspguide/module1-toolkit1/utisbar-form.html

65
Released March 27, 2015Outlines steps to
implement the National Strategy and address policy recommendations
Significant outcomes expected by 2020
National Action Plan for Combating Antibiotic-Resistant Bacteria
(CARB)
65

66
National Action Plan for Combating Antibiotic-Resistant Bacteria
(CARB)
Objective 1.1: Implement public health programs and reporting policies that advance antibiotic resistance prevention and foster antibiotic stewardship in healthcare settings and the community.Goal: Reduction of inappropriate antibiotic use by
50% in outpatient settings and by 20% in inpatient settings.




NHSN Antimicrobial Use Option
Objective: Measure antibiotic use to provide risk-adjusted inter- and intra-facility comparisons
Antibiotic resistance surveillance option also available
NHSN AU Protocol
http://www.cdc.gov/nhsn/acute-care-hospital/aur/index.html
71
Action Items1) Learn about your facility’s antimicrobial stewardship
program (ASP) and how the Infection Prevention team can be involved
2) Increase awareness of staff (medical, nursing, etc.) regarding the 8 principles of antibiotic therapy
3) Review your facility’s antibiogram to understand local problematic organisms (especially occurrence of carbapenem-resistant organisms)
4) Encourage and support your facility’s use of NHSN and the NHSN antibiotic use and resistance (AUR) module

72
Acknowledgements(for use of selected slides)
Lauri Hicks, DOCDC, Director, Office of Antibiotic Stewardship
Kurt Stevenson, MD, MPHThe Ohio State University Medical Center
Nimalie Stone, MD, MSCDC, Division of Healthcare Quality Promotion
Theo Zaoutis, MD, MSCEThe Children’s Hospital of Philadelphia

Resources - 1
https://www.cdc.gov/longtermcare/prevention/antibiotic-stewardship.html
http://www.ahrq.gov/nhguide/index.html
http://www.health.state.mn.us/divs/idepc/dtopics/antibioticresistance/asp/ltc/
https://www.gnyha.org/whatwedo/quality-patient-safety/infection-control-prevention/antimicrobial-stewardship
http://www.mi-marr.org/LTC_toolkit.php
https://www.cdph.ca.gov/programs/hai/Pages/ASPinNursingHomesWebinarSeries2016.aspx
Resources - 2
http://www.rochesterpatientsafety.com/tools-for-long-term-care-facilities.html
https://nursinghomeinfections.unc.edu/
https://robinjump.coursesites.com/
http://www.choosingwisely.org/patient-resources/antibiotics-for-people-with-catheters/
http://www.choosingwisely.org/patient-resources/antibiotics-for-urinary-tract-infections-in-older-people/

Resources - 3
Advancing Excellence in America’s NH campaign, Infections Goal: http://www.nhqualitycampaign.org
CDC Get Smart for Antibiotic Use in Healthcare: http://www.cdc.gov/getsmart/healthcare/
CDC/SHEA Infection surveillance definitions for LTC http://www.jstor.org/stable/10.1086/667743
CDC’s resources for LTC (update coming soon): http://www.cdc.gov/HAI/settings/ltc_settings.html
CDC’s infection reporting system for LTCFs: http://www.cdc.gov/nhsn/ltc/

Supplemental, Informational Slides

Unintended Consequences of Antibiotic Use: Antibiotic Resistance
Some of the reasons for this are out of our controlThe ability of bacteria to mutate to resist antibiotics
BUT- some of the most important ones are very much in our controlOveruse of antibioticsSpread of resistant organisms in healthcare settings
through poor infection control practices

Do Antimicrobial Agents Cause Resistance?
5
4
3
2
1
01988 1989
5
4
3
2
1
01990 1991 1992 1993 1994 1995 1996 1997 1998
6
Pneumococci withReduced Susceptibilityto Fluoroquinolones (%)
No. of Prescriptions per 100 persons
Chen DK et al., N Engl J Med, 1999;341:233-9.

80
Urinary Tract Infections andPrevious Exposure to Antibiotics
Children age 6 months to 6 yearsFirst diagnosis of urinary tract infection (UTI)Recent exposure to amoxicillin (i.e., within 30 days) was
associated with increased resistance of identified organism to ampicillin and amoxicillin-clavulanate
Paschke AA et al., Pediatrics, 2010;125:664-72.

Observed Association between Antimicrobial Useand the Emergence of Resistance
Changes in use are paralleled by changes in resistanceResistance more prevalent in healthcare-associated
infections (HAI)Patients with HAI are more likely to have received
antibioticsAreas with high use also have high resistanceIncreased duration of use increases likelihood of
colonization with resistant organisms
Dellit TH et al., CID, 2007;44:159-77.

C. difficile Infection (CDI) and Antibiotics
McDonald LC et al Emerg Infect Dis 2006; Simor AS, J Am Geratrc Soc. 2010.
CDI is the most common cause of acute diarrhea in LTC Antibiotics are a major driver of C. difficile acquisition and infection Fluoroquinolone antibiotics have
been associated with CDI with a more severe strain of C. difficile
Longer antibiotic exposure carries higher risk

83
Mechanisms of Resistance
Cross-resistance to structurally unrelated antimicrobial agents occurs primarily through 1 of 2 mechanisms:1) Efflux pumps that can remove a variety of antimicrobials from the bacterial cell2) Presence of resistance “islands” without the genetic material of the organism that confer resistance to a variety of antimicrobials through diverse mechanisms
Nagel et al., Infect Dis Clin N Am, 2016;30:771-84.

84
ESKAPE Pathogens
E – vancomycin-resistant Enterococcus spp (VRE)S – methicillin-resistant Staphylococcus aureus (MRSA)K – Klebsiella pneumoniaA – Acinetobacter baumanniiP – Pseudomonas aeruginosaE – Enterobacter spp.Bad Bugs, No Drugs2004, Infectious Diseases Society of American campaign
Boucher et al., CID, 2009;48:1-12.

85
Healthcare Facilities as Source of MDROs
Sengstock DM, et al. Clin Infect Dis. 2010 50(12): 1611-1616.

http://emerald.tufts.edu/med/apua/news/news-newsletter-vol-29-no-3-2.shtml
87
Shifting The Way We Approach Improving Antibiotic Use
We need to learn from the successful model of hospital infection control
For decades, preventing infections in hospitals was viewed as the primary responsibility of the infection control program
Preventing infections is increasingly viewed as the primary responsibility of all healthcare providersSystems approach
Surveillance

Antimicrobial Stewardship Active Interventions
Prospective audit with intervention and feedback (A-I)Direct interaction with infectious disease physician
or clinical pharmacist trained in IDFormulary restriction and preauthorization
(A-II)Antibiotic approvals by Infectious Diseases
physicians or PharmD’sRestricted drugs at start of use

Antimicrobial Stewardship Supplemental Strategies
Guidelines and clinical pathways (A-I)Dose optimization (A-II)Streamlining or de-escalation of therapy (A-II)Education (A-III)Parenteral to oral conversion (A-III)Antibiotic order forms (B-II)Antimicrobial cycling (C-II)Combination therapy (C-II)

90
Harm from Infections among SNF Residents
Infections were among the most common causes of harm; accounting for 26% of adverse events
Hospitalizations from infections were estimated to cost ~83 million dollars (the most expensive cause of harm)
Type of Harm Events related to infection
Infection events deemed preventable
Transfers to hospital from infection event
Adverseevents (n=148)
39 (25.8%) 22 (59%) 34 (87.2%)
Temporary (n=113)
20 (16.8%) 9 (45%) NA
OIG report: Adverse Events in Skilled Nursing Facilities: National Incidence Among Medicare Beneficiaries (OEI-06-11-00370), February 2014

Gaps/Opportunities to Prevent Infections Better recognition of the problem
Recognizing and documenting changes in clinical status Standardize the way infections are defined and reported to monitor
the burden of the problem Improved documentation of the response
Inadequate documentation of actions leads to incomplete information and missed opportunities
Provide guidance and standards for implementing best practices Improve communication across care transitions
Increased accountability for prevention Facility practices to prevent infection should be monitored for
adherence and impact Implement consistent methods for assessing the effectiveness of
infection prevention activities

92
CMS Proposed Regulations for Infection Prevention and Control Programs (IPC)
Cross-cutting IPC regulations: Facility risk assessment of resident
population (§483.70) Integrating IPC into QAPI activities
(§483.75) Required review and update of IPC
program, policies/procedures (§483.80) Designated IPC Officer with specific
training (§483.80) IPC-specific education and training for all
staff (§483.80)

93
CMS Proposed Regulations for Antibiotic Stewardship
Antibiotic stewardship integrated within pharmacy and infection prevention and control (IPC): Expanding pharmacy medication reviews
to include antibiotics for monthly review; reviews also occur for all new admissions/re-admissions, (§483.45)
Antibiotic use protocols and monitoring included in IPC (§483.80)
Integrating IPC and stewardship into QAPI activities (§483.75)
Richards et al. JAMDA 2005; 6: 109–112.

Accountability Antibiotic stewardship leads can utilize existing resources
Infection prevention and control coordinator Tracking antibiotics, monitoring adherence to prescribing practices
Consultant Laboratory Alerting facilities if antibiotic resistant organisms are identified Education about differences in diagnostic testing (i.e. different test for
C. difficile) Creating antibiograms to help with empiric antibiotic selection and
monitor for resistance State and local health departments Educational support and resources on antibiotic stewardship and
infection prevention by the Healthcare-Associated Infections prevention programs

Resources for Leadership Education
Utilize existing campaigns and resources to make facility staff and residents more aware of safe antibiotic use
http://www.cdc.gov/getsmart/healthcare/

Resources for Clinician Education
www.cdc.gov/longtermcare/

Education-ResidentsDevelop resources and tools to engage residents and families to in
stewardship education efforts, this will reduce barrier of resident and family expectations in improving antibiotic prescribing
Start the conversation early with residents and their families
http:www.rochesterpatientsafety.com/tools-for-long-term-care-facilities.html
http://www.cdc.gov/longtermcare/prevention/antibiotic-stewardship.html

Resources for Consumer Education
www.choosingwisely.org/doctor-patient-lists/

Use Evidence-based Practice Guidelines to Create Management Algorithms
Infect Control Hosp Epidemiol 2001; 22:120-124
Clin Infect Dis 2009; 48:149-171

Wang L. et al. Eur J Clin Microbiol Infect Dis. 2012. 31(8):1797-804.
Gap between MD Diagnosis and Surveillance Criteria
146 infections, UTI or pneumonia were diagnosed and treated by clinicians
33/146 (23%) were also identified by applying either McGeer or Loeb minimum criteria

Action-Policy Implement at least one policy or practice
to improve antibiotic use, ideally in a stepwise fashion
Antibiotic prescribing and use policies Documentation of dose, route, duration
and indication for every antibiotic course Develop facility specific treatment
guidance for common infections based on practice guidelines
Ouslander et al, Consensus-Derived Interventions to Reduce Acute Care Transfer (INTERACT)-Compatible Order Sets for Common Conditions Associated with Potentially Avoidable Hospitalizations, JAMDA, 2015
http://www.rochesterpatientsafety.com/tools-for-long-term-care-facilities.html

Reporting
Provide regular feedback on antibiotic use and resistance to prescribing clinicians, nursing staff and other relevant staff
Monitoring and feedback to providers and staff on the impact of their efforts is critical to sustaining improvements
Provider specific feedback is one of the most effective ways to change prescribing behaviors
Any measure being tracked as part of monitoring antibiotic use should have a mechanism for reporting the results back to appropriate staff in the facility
Having antibiotic use data to share with staff, residents and families especially improvement in clinical outcomes (e. g., decreased CDI) can increase support of stewardship activities

Education
Provide educational resources to clinicians, nursing staff, residents and families about antibiotic resistance and opportunities for improving antibiotic use
Education may be one of the first elements implemented to establish support among facility providers and staff
Effective and sustained change doesn’t happen without education
Use educational events as an opportunity to engage providers and staff in identifying ways to improve current practices
Address staff concerns and barriers to changing antibiotic use in your facility
Work with facility staff to develop resources/tools to educate residents/families on stewardship efforts in your facility