keratosis obturans
TRANSCRIPT

KERATOSIS OBTURANS SRIDHAR L ROLL NO : 4094
1
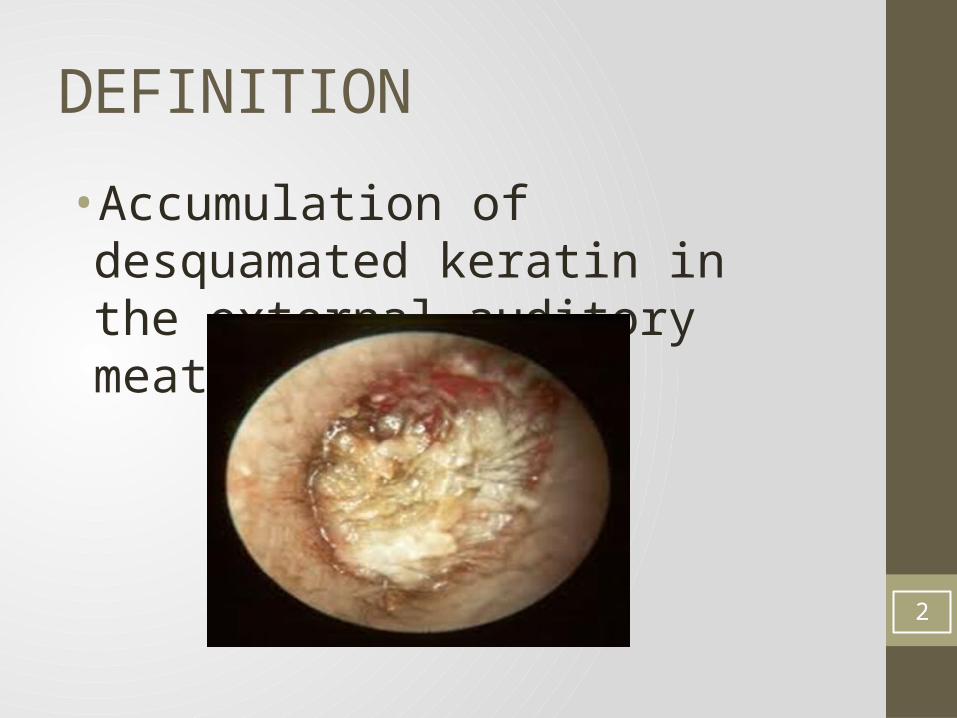
DEFINITION
•Accumulation of desquamated keratin in the external auditory meatus.
2

PATHOLOGY
• The keratin squames are shed from the complete circumference of the deep ear canal forming a lamina.
• Geometrically patterned keratin plug within the lumen of expanded ear canal.
• Normally the epithelium from the tympanic membrane migrates to the posterior meatal wall.
• Failure of this migration or obstruction to the migration by wax/foreign body causes keratosis. 3

SILENT TYPE
• There is no predisposing acute infections involved.
•Caused by abnormal separation of keratin.
•Persists even after removal.4

INFLAMMATORY TYPE
• Due to acute inflammation of the ear canal.
PATHOLOGY
• Causes increased epithelial turn over.• Alteration of epithelial migration. 5

PRIMARY CHOLESTEATOMA OF EAM
• Primarily there is an irregularity/erosion of the bony wall – Post-traumatic or Post surgical.
• Squamous epithelium invades the bone.
• C/F – PAIN , Purulent Otorrhea , No CHL.
• Subjected to histopathology to r/o carcinoma, necrotizing otitis externa etc.
6

7

CLINICAL FEATURES
• 1. Severe ear pain.
• 2. Mild to Moderate conductive hearing loss.
• 3. Associated bronchiectasis / sinusitis /primary ciliary dyskinesia are common.•
• 4. Rarely otorrhoea. 8

EXAMINATION
• The canal is occluded by a plug of white keratin debris which contains a small amount of normal appearing brown cerumen in its centre.
• There may be accompanying granulations and widening of external auditory canal
• CT images of temporal bone will show widening of external canal with bone erosion.
9

10

MANAGEMENT
• Treat the cause- impacted wax-syringing inflammatory type- treat the infection. foreign body- instrumentation.
• Use of keratolytic agents like 2% salicylic acid in alcohol.• Surgical removal under General Anaesthesia.• Canal plasty in recurrent cases.• Mastoidectomy in patients with primary cholesteatoma
of external canal.• Removed specimen should be sent for Histopathology
to rule out malignancy. 11

REFERENCES• K B Bhargava , 9th edition, Sept 2011 , page no. 38, ‘Diseases of
external ear ‘
12

THANK YOU
13