kenya contextualised theory of change
TRANSCRIPT
Page | 1
KENYA CONTEXTUALISED
THEORY OF CHANGE
25 September 2016
Report Author
Heather Budge-Reid
Contributors
Gavin Stedman-Bryce
Email: [email protected]
Web: www.pamoja.uk.com

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 1
TABLE OF CONTENTS
LIST OF BOXES AND FIGURES ......................................................................................................... 1
ACRONYMS AND ABBREVIATIONS ............................................................................................... 2
EXECUTIVE SUMMARY .................................................................................................................... 3
1. CONTEXT .................................................................................................................................. 4
2. EXAMINING HOW TO CREATE CHANGE IN KENYA .................................................... 10
3. OUTCOMES ............................................................................................................................. 12
APPENDIX 1: PROBLEM TREE EXERCISE RESULTS .................................................................. 17
APPENDIX 2: SPIDER DIAGRAM EXERCISE RESULTS .............................................................. 21
APPENDIX 3: BALLOONS AND STONES EXERCISE RESULTS ................................................ 22
APPENDIX 4: AGENDA ..................................................................................................................... 24
LIST OF BOXES AND FIGURES
Figure 1 Short-, medium- and long-term outcomes Figure 2 Problem tree for 'Low implementation' Figure 3 Balloons and stones diagram for 'County work' Figure 4 Problem tree for 'Health system weakness' Figure 5 Spider diagrams Figure 6 Balloons and stones diagrams Figure 7 Detailed Theory of Change indicating Accountability Threshold
KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 2
ACRONYMS AND ABBREVIATIONS
CSO Civil society organisation
HSA Health Systems Advocacy Partnership
HSS Health system strengthening
SRH Sexual and reproductive health
SRHR Sexual and reproductive health rights
ToC Theory of Change

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 3
EXECUTIVE SUMMARY
Following a three-day residential meeting that focused on group work and plenary
discussions, the Kenya HSA Partnership and guests from a wide range of stakeholder
organisations came to a set of conclusions around a contextualised Theory of Change.
While the theory of change process was new to most in the room, all were open to the idea
of examining the concepts and re-examining previously developed lists of activities in the
light of questions about what change was desired and how that change was going to be
created. This led to the identification of some key contexts for the Kenyan team:
Health policies in Kenya were deemed good health polices but, as in Uganda, there
were challenges around implementation. As a result, work focused on
implementation rather than policy change.
The regions being targeted by the Kenya Partnership are undergoing an exciting
change as a result of the decentralisation process. This change is part of an exciting
moment of opportunity for influence that the HSA Partnership has in Kenya, to
support accountability, empowerment and policy implementation.
Each of the counties being targeted is undergoing a rapid urbanisation as the central
towns grow rapidly into cities and people move from the land to the urban areas. This
puts a particular pressure on the health systems in counties that were previously
rural. This peri-urban setting is not a unique challenge in Africa but by being involved
in this process the HSA team believe they will identify some important lessons.
After much discussion, the following statement summarises the contextualized theory of
change.
If we work at community, county and national levels to create/improve a well-informed space
for dialogue and dissent that improves accountability and empowerment
Then the health system at county level will be strengthened
Because health polices will implemented, financing of health will be more effective, planning
improved, commodities and HR better managed and the county-level decision-makers better
informed.
Figure 1 Short-, medium- and long-term outcomes
Long-term outcome of a sustainable local system of dialogue that continues
to develop accountability and empowerment and thus full implementation of
existing policies
Mid-term outcome of creating an empowerment and accountability space in
peri-urban environments and the research that will inform that space
Short-term outcome of an effective partnership between HSA members and
an effective, integrative approach between all stakeholders

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 4
1. CONTEXT
There remains a challenge in the adaptation of the existing plans developed at the Kampala meeting
for the HSA Partnership and the results of the contextualised Theory of Change. These challenges are
not insurmountable but do illustrate the need to carry out the theory of change development process
before settling to specific plans. There is little evidence that the key contexts in Kenya are included in
the planning of activities. However, it will be straightforward enough to adapt activity lists to the
context as revealed in the three-day workshop.
1.1. Key issues
1.1.1. Implementation not policy change
Key to the context in Kenya is the understanding that there is no perceived need for policy change in
health and thus the activities currently targeted at policy change outcomes do not need to be
undertaken. However, there is a need to address the challenges of implementation – the financial
resources needed for implementation need to be made available, alongside the guidance and approach
necessary to see full implementation of existing policies. The diagram below is the result of group
work and reviews the causes and effects of poor implementation of good health policies in Kenya as
listed here. There is one further aspect of policy analysis that needs to take place – are the policies that
exist appropriate for the rapidly expanding peri-urban nature of growth in Kenya?
Problem tree results for 'Low implementation'
Causes Effects
Lack of guidelines
Poor dissemination of information
No timeframe
Poor formal and informal supervision
Poor allocation of resources
Poor planning
Lack of accountability
Corruption
Lack of public awareness
Misuse of resources
Lack of quality performance
Spread of corruption
Demoralised population
Lack of empowerment
Lack of awareness of rights

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 5
Figure 2 Problem tree for 'Low implementation'
1.1.2. Decentralisation
The HSA Partnership begins work at an exciting moment of decentralisation of decision making and
finance allocations for health, with county-level structures taking local decisions about allocation of
funding and the development of the local health system. This has led to an understanding of the
importance of informing county structures about the value of strengthening health systems as well as
raising their capacities to make decisions in the new county structures. While new people are
becoming decision-makers, health related information needs to reach them about health systems and
health needs as well as the nature of health systems and challenges in their county.
1.1.3. The peri-urban health environment
Health needs change rapidly as an area's population changes from mainly rural to mainly urban, e.g.
the number of traffic accidents increases; population proximity increases TB; and, as structures such
as water and waste systems degrade under pressure, other health dangers alongside population growth
place demands on services that were previously serving a rural area.
There is a need to inform the county-level decision makers about the peri-urban health needs of their
areas. The group drew up a list of five topics of research that would need to be carried out in each
county in order that decision makers are informed about the conditions of the entire health system,
including the for-profit and not-for-profit sectors as well as the government sector.
Research topics:
1. What amount of funding is coming into the area that strengthens the health system?
2. What score does the health system in the area have and what should it have?
3. What is the commodity availability in the area?
4. What is the gap in human resources in the area?
5. What is the level of implementation of existing policies in the area?

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 6
1.1.4. County-level implementation
Work in the chosen counties not only requires access to information but also the communication of
information to decision makers. In addition, county-level work faces some challenges as well as
positive factors. Group work through the Stones and Balloons exercise suggests that the following
issues will be important positives and negatives, and this illustrates why informing policy makers is so
important.
County work
Stones Balloons
High turnover of county leaders
Competing interests/priorities at county
level
Outbreaks of disease or epidemic
Severe unrest
Supportive political will
Existing health structures
Established and interested CSOs
Established and existing community
structures
Figure 3 Balloons and stones diagram for 'County work'
1.2. Identifying change relationships in the context of Kenya
The Problem Tree exercise (see Appendix 1) allowed the group to explore in more detail the causes
and effects surrounding key areas of the health system. The diagram below takes the example of the
weakness of the health system.
Health system weakness
Causes Effects
Lack of prioritisation by government High morbidity rates

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 7
Lack of transparency of supply chain
Inadequate funding
Inadequate human resources for health
Inadequate political goodwill
Poor information flow in every
direction
Poor planning
Stock outs
Burnout and low morale
Misdiagnosis and poor patient
management
High turnover of staff
Uncontrolled population growth
Services that don't respond to
community needs
Figure 4 Problem tree for 'Health system weakness'
During the feedback session, it became clear that, while there was no need for a change in policies,
implementation is the key issue and access to information is going to be a fundamental part of
creating change in a system that has only recently become decentralised.
It was clear that, with the focus on specific counties where rapid urbanisation is going on, there will
need to be a specific target for advocacy work through county structures around implementation and
responses to local needs. While the main focus would be at county level, the issue of financing the
health system throughout the nation remains important and an aspect of work to be undertaken.
In addition, there was a clear need to carry out evidence-based advocacy relating to the needs of
specific areas, as well as increasing the capacity of county-level decision makers to take well-
informed decisions.
The decentralisation process was seen to create an exciting opportunity to develop an inclusive health
system that unites the government, not-for-profit and profit-based service providers in a coherent
system that serves rapidly changing local needs.

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 8
1.3. Estimating the current situation
This work was carried out by using Spider Diagrams to draw out estimates of the current situation
surrounding the priorities of human resources for health, commodities, and the health system itself.
Each group was asked to identify eight areas of influence and then estimate the current situation
giving a score of 0 as very poor and 10 as ideal.
Figure 5 Spider diagrams

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 9
Given that the aim of the programme of work is to address the issues on the spider 'legs' and raise
their score to 10, a clear picture emerged of the target areas for activities, particularly when priorities
were considered in the context of advocacy work rather than work to provide physical infrastructure.
1.4. Assumptions and risk
Throughout the three-day workshop, assumptions and risks were identified – they are brought
together here.
1.4.1. Assumptions
That the policy in place is good policy but lacks implementation
That HSS as a precondition is generally accepted by actors in health but that it is ignored in
strategizing for results
That if county-level decision makers are well informed then they will strengthen the health
system
That lessons can be captured that enable the roll-out of the programme's approach to other
physical areas in Kenya
That finance issues still need to be discussed at the national level
That peri-urban forces create specific health demands
That the decentralisation process has created a positive environment for decision on health
system strengthening.
1.4.2. Risks
That political changes could change the policies on which this work is based
That there will be informal resistance to integrative approaches from private and public health
service providers
That there will be a failure to capture lessons in real time, reducing effectiveness and long-
term impact
That county-level decision makers only focus on government health services.

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 10
2. EXAMINING HOW TO CREATE CHANGE
IN KENYA
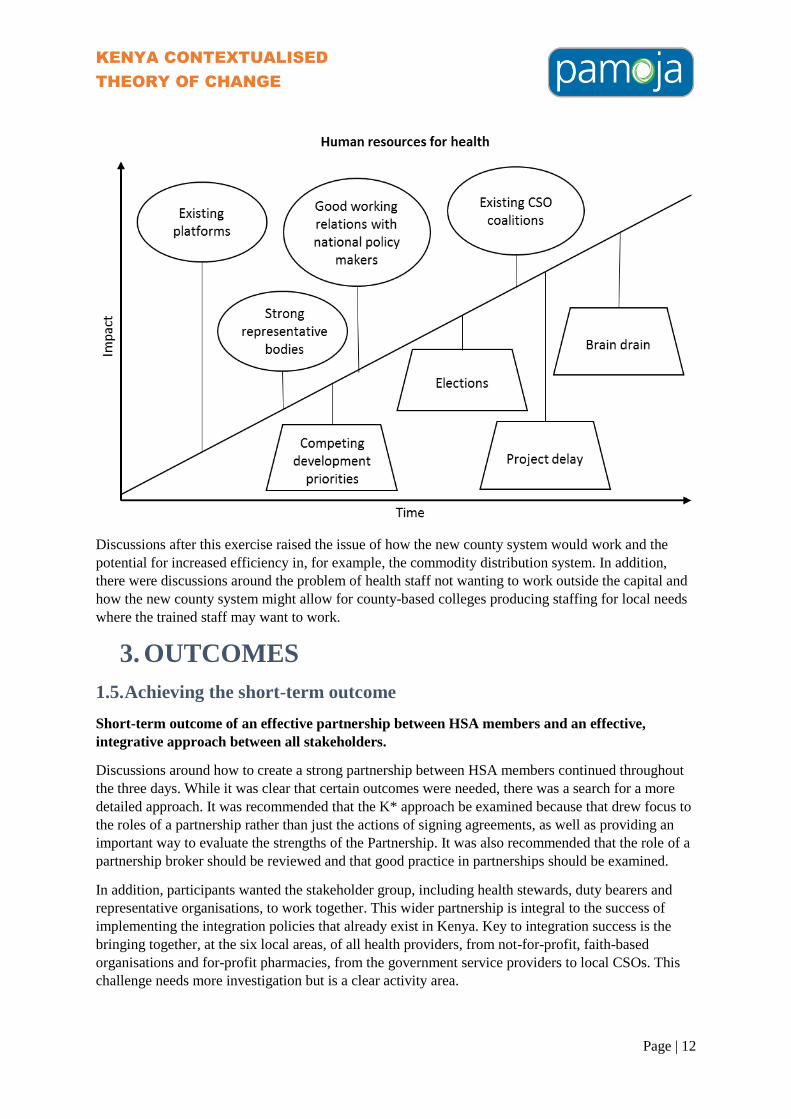
By feeding the results of the Spider Diagram exercise into a Balloons and Stones exercise, it was
possible to identify those issues that would support and hinder success for the Partnership.
Figure 6 Balloons and stones diagrams

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 11
KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 12
Discussions after this exercise raised the issue of how the new county system would work and the
potential for increased efficiency in, for example, the commodity distribution system. In addition,
there were discussions around the problem of health staff not wanting to work outside the capital and
how the new county system might allow for county-based colleges producing staffing for local needs
where the trained staff may want to work.
3. OUTCOMES
1.5. Achieving the short-term outcome
Short-term outcome of an effective partnership between HSA members and an effective,
integrative approach between all stakeholders.
Discussions around how to create a strong partnership between HSA members continued throughout
the three days. While it was clear that certain outcomes were needed, there was a search for a more
detailed approach. It was recommended that the K* approach be examined because that drew focus to
the roles of a partnership rather than just the actions of signing agreements, as well as providing an
important way to evaluate the strengths of the Partnership. It was also recommended that the role of a
partnership broker should be reviewed and that good practice in partnerships should be examined.
In addition, participants wanted the stakeholder group, including health stewards, duty bearers and
representative organisations, to work together. This wider partnership is integral to the success of
implementing the integration policies that already exist in Kenya. Key to integration success is the
bringing together, at the six local areas, of all health providers, from not-for-profit, faith-based
organisations and for-profit pharmacies, from the government service providers to local CSOs. This
challenge needs more investigation but is a clear activity area.

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 13
1.5.1. Activities
Initial
Discover the legal context of partnership
Carry out capacity analysis of partnership members at national and county levels
Discover how to make partnership meetings work
Schedule a set of meetings
Develop a shared vision.
Then
Sign MOU
Set budget
Put in place a conflict resolution system
Clearly define responsibilities
MEI plans for Partnership and its activities
Communication systems designed and implemented
Create a joint work plan
Increase relevant partner capacities.
Having created transparency and trust these two aspects will create commitment, harmonised
understanding of the project and the capacity development of partners.
1.6. Achieving the medium-term outcome
Medium-term outcome of creating an empowerment and accountability space in peri-urban
environments and the research that will inform that space.
It was recognised that an empowerment and accountability space needs to be put in place that mirrors
the county system. There was also a focus on the need to inform both the space in which
empowerment and accountability takes place, and county-level decision makers. Therefore, research
and communication of evidence has taken a high priority in activities.
Initial
Inform the decision makers on health system strengthening
Inform decision makers about the results of research:
o Research into the amount of funding coming into the area that strengthens the health
system
o Research into what score the health system in the area has and should have
o Research into commodity availability in the area
o Research into the gap in HR in the area
o Research into the level of implementation of existing policies in the area
Develop a county-level coordination mechanism inclusive of government, for-profit and not-
for-profit health providers
Create a comprehensive Kenya-wide and county-level review of financing for health system
strengthening
Develop the tools for social accountability, e.g. citizen scorecard, community and health unit
self-assessment.
Then

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 14
Advocate for evidence-based health system strengthening approaches
Advocate for efficient and effective county-level HRH and commodity approaches
Facilitate a county-wide dialogue space inclusive of communities and all health service
providers
Apply scorecard approach to monitoring.
1.7. Achieving the long-term outcome
Long-term outcome of a sustainable local system of dialogue that continues to develop
accountability and empowerment and thus full implementation of existing policies.
Create a sustainable mechanism for informing new decision makers at county level as they
come to power
Sensitise the community about health rights and responsibilities
Develop a sustainable community-based monitoring system for implementation levels
Develop and implement an exit strategy
Capture lessons learnt and start a roll-out process to one other county
Develop scorecard results dissemination for sustainability.
Figure 7 Detailed Theory of Change indicating Accountability Threshold

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 15

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 16

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 17
APPENDIX 1: PROBLEM TREE EXERCISE
RESULTS
Low implementation
Causes Effects
Lack of guidelines
Poor dissemination of information
No time frame
Poor formal and informal supervision
Poor allocation of resources
Poor planning
Lack of accountability
Corruption
Lack of public awareness
Misuses of resources
Lack of quality performance
Spread of corruption
Demoralised population
Lack of empowerment
lack of awareness of rights

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 18
Lack of advocacy for HSS
Causes Effects
Poor information management
Lack of skills
Misconception about advocacy
Poor coordination of advocacy efforts
Competition among actors
Weak health system
Inadequate funding for HSS
Weak advocacy platform
Weak health leadership
Weak governance
Poor stewardship

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 19
Health system weakness
Causes Effects
Lack of prioritisation by government
Lack of transparency of supply chain
Inadequate funding
Inadequate human resources for health
Inadequate political goodwill
Poor information flow in every
direction
Poor planning
High morbidity rates
Stock outs
Burnout and low morale
Misdiagnosis and poor patient
management
High turnover of staff
Uncontrolled population growth
Services that don't respond to
community needs.

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 20
Poor SRH services
Causes Effects
Lack of accountability
Attitude of workers and population
Culture
Lack of enforcement on law
Religion
Poor legislation laws
Poor policy implementation
Poor supplies
Poor equipment
Low capacity of workers
Lack of information for the public
Distance to health services
Early pregnancies
Counterfeit or fake drugs
Fake health staff
Corruption
Harmful cultural practises
Poor quality of services
Poverty
Slow economic growth

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 21
APPENDIX 2: SPIDER DIAGRAM EXERCISE
RESULTS
The data below is presented as diagrams in Chapter 1.
Human resources
Staff retention 2
Career progression opportunities 6
Terms and conditions 4
Standardisation across public/private 2
Distribution of staff 2
Social accountability 3
Training 5
Numbers of staff 2
Commodities
Community perception 3
Access 2
Finance 3
Supply chain 3
Information availability to population 2
Information from health units to support
planning
2
Policy implementation 5
Human resource capacity 5
Health system
Policy implementation 4
Health systems delivery 2
Information about health systems 2
Financing for health systems 7
Social accountability 3
Governance and leadership at high levels 3
Commodity availability 5
Governance and leadership at service delivery
level
4

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 22
APPENDIX 3: BALLOONS AND STONES
EXERCISE RESULTS
The data below is presented as diagrams in Chapter 2.
Health system strengthening
Stones
o Poor political will
o Inadequate budget allocation
o Culture and perceptions
o Poor policy implementation
Balloons
o Existing community structures
o Favourable policies
o Enabling conducive environment
o Coordinated management structures for the Partnership
Commodities
Stones
o Weak distribution system
o Poor storage
o Infiltration of counterfeit drugs
o Inadequate implementation policies
Balloons
o Existing policies
o Synergy within the Alliance
o Community commitment
o Goodwill of duty bearers
County work
Stones
o High turnover of county leaders
o Competing interests/priorities at county level
o Outbreak of disease or epidemic
o Severe unrest
Balloons
o Supportive political will
o Existing health structures
o Established and interested CSOs
o Established and existing community structures
Human resources for health
Stones
o Competing development priorities
o Elections
o Project delay
o Brain drain
Balloons

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 23
o Existing platforms
o Strong representative bodies
o Good working relations with national policy makers
o Existing CSO coalitions

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 24
APPENDIX 4: AGENDA
Learning goals Outputs Shared understanding of ToC methodology Contextualised theory of change
Shared understanding of Indicators First draft indicators for contextualised theory
of change
Summary
Day 1 – Overall Theory of Change, identifying the change desired and understanding the details
of the problem.
Day 2 – Context, the logic of change and advocacy in the Theory of Change.
Day 3 – Activities, assumptions, indicators.
Day One: 4th
July
Timing Session Detail
09.00 – 09.15 Arrival
Tea and coffee will be available
09.15 – 09.45 Welcome and introductions
09.45 – 10.30
Working together
Individual brainstorm and vote exercise – What makes a good partnership?
10.30 – 11.30 Introducing Theory of Change
Presentation – An introduction to the Theory of Change approach and its relevance in
good impact practice
11.30 – 11.50 Comfort Break
11.50 – 12.30
Looking at the HSAP Theory of Change
Group work card sort exercise to aid understanding the current overall Theory of Change
12.30 – 13.00
Looking at a contextualised Theory of Change
Group work card sort with the example of the Netherlands Theory of Change
13.00 – 14.00 Lunch Break
14.00 – 14.30
The change the programme wants to achieve
Individual headline success stories exercise
Shout-out exercise and group work to support the articulation of goals
14.30 – 15.30
Problem analysis
Group work around the problem trees to develop understanding of the problem the
programme seeks to address
15.30 – 15.50 Comfort Break
15.50 – 16.50
Problem analysis (continued)
Breaking the cycle of cause and effect for the problem the Partnership is seeking to
address
16.50 – 17.00
Reflections and wrap up
17.00 Close

KENYA CONTEXTUALISED
THEORY OF CHANGE
Page | 25
Day Two: 5th
July
Timing Session Detail
09.00 – 09.15 Arrival
Tea and coffee will be available
09.15 – 10.00
Welcome back
Time to reflect on the session from Day One
10.00 – 11.30
The context of the Partnership's work
A Spider Diagram Exercise to help articulate the influences on the project that the
Kenyan context imposes
11.30 – 11.50 Comfort Break
11.50 – 13.00
Power analysis An exercise to help identify the outcomes for the programme to create the change it wants
13.00 – 14.00 Lunch Break
14.00 – 14.30
Identifying the logical flow of change
If-Then-Because exercise
14.30 – 15.00
Overview of advocacy activities
Presentation
15.00 – 15.30
Conversations that create change
Fish bowl exercise
15:30 – 15.50 Comfort Break
15.50 – 16.45 The evidence basis
Exercise to support research planning in the advocacy context
16.45 – 17.00 Wrapping up
17.00 Close
Day Three: 6th
July
Timing Session Detail
09.00 – 09.15 Arrival
Tea and coffee will be available
09.15 – 09.45
Remembering where we have got to
09.45 – 10.30 Understanding outputs, outcomes and impacts
Presentation
10.30 – 11.30
Activities and outcomes
Exercise to develop activity plans
11.30 – 11.50 Comfort Break
11.50 – 12.30
Indicators and baselines
Presentation
12.30 – 13.00
Creating indicators
Exercise to define indicators
13.00 – 14.00 Lunch Break
14.00 – 15.00
Assumptions and Risks exercise
Plenary discussion
15.00 – 15.30
Headline success exercise
What will success look like?
15.30 – 15.50 Comfort Break
15.50 – 16.30
Reviewing the contextualised Theory of Change
16.30 Close