keeping people with diabetes out of hospital - · pdf file2 primary care diabetes society...
TRANSCRIPT
Keeping People with Diabetes
Out of Hospital
PCDSPrimary Care Diabetes Society
Supported by:
Keeping People with Diabetes Out of Hospital 32 Primary Care Diabetes Society
Contents
Forewords Lord Rennard MBE, Chair of the Working Group ________________________________________________ 6
Dr Paul Downie, Primary Care Diabetes Society ________________________________________________ 8
Caroline Horwood, Sanofi ________________________________________________________________ 9
Dr Roger Gadsby, Member of the Working Group _______________________________________________ 9
1) Recommendations ________________________________________________________________________ 10
2) Scope of the project _______________________________________________________________________ 11
3) Why do people with diabetes end up in hospital? ________________________________________________ 12
a) Complications _______________________________________________________________________ 12
b) Delayed Diagonsis ____________________________________________________________________ 13
c) Vulnerable Groups ____________________________________________________________________ 13
d) Patient Referral ______________________________________________________________________ 15
e) Access to information __________________________________________________________________ 15
f) Patient confidentiality and consent _________________________________________________________ 15
g) Ways of working in the new NHS __________________________________________________________ 16
4) Financial Burden __________________________________________________________________________ 17
5) How to Keep People With Diabetes Out of Hospital _______________________________________________ 19
6) Sharing & adopting best practice _____________________________________________________________ 22
a) Case Study 1: Care Homes Project ______________________________________________________ 23 South Staffordshire Primary Care Trust
b) Case Study 2: Tackling Diabetes Related Emergency Admissions _________________________________ 26 Nottingham NHS
c) Case Study 3: Local Enhanced Service to target pre-diabetes in Primary Care ________________________ 28 NHS Eastern and Coastal Kent
d) Case Study 4: Integrating Community Care for Diabetes ________________________________________ 30 Berkshire West
e) Case Study 5: New Organisations for New Challenges in Long Term Conditions _______________________ 32 Derby PCT
f) Case Study 6: Reducing Hypoglygaemia & hospital admissions in vulnerable patients ___________________ 34 South Staffordshire PCT
g) Case Study 7: Diabetes Inequalities Outreach Project _________________________________________ 36 Clacton-on-Sea
h) Case Study 8: Prevention in admission in vulnerable peoples ____________________________________ 38 Birmingham and Solihull Mental Health Foundation Trust
7) References ___________________________________________________________________________ 40
8) Contacts ___________________________________________________________________________ 41
Insight Public Affairs were employed by Sanofi by way of a grant
to provide secretariat and administrative assistance for this
Primary Care Diabetes Society policy project.
For more information on this project please contact Katie Russell
on 020 7824 1859 or [email protected]

4 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 5
“ How often have you heard about an older patient stuck in hospital
for weeks because there’s nowhere else for them to convalesce? Or
asthmatic and diabetic patients not getting the right support to manage
their condition ending up in A&E before being put on the ward to recover?
We have too many patients, spending too long in hospital, taking too long
to get better.”
Deputy Prime Minister, Rt Hon Nick Clegg MP,
Speech to NHS at University College London Hosptial (May 26 2011)
“ When we are ill, what matters most, is that the NHS is there for us. That
it listens, understands and provides us with the best possible care. The
best outcome. Of course, the best outcome is for people to stay healthy.
But for the many of those who have long-term conditions, the best
outcome is about reducing and minimising the impact of their symptoms,
and wherever possible keeping them out of hospital. For this to happen
there needs to be: a fast and accurate diagnosis; shared decision making
about treatment; and on-going support for self-management.”
Secretary of State for Health, Rt Hon Andrew Lansley CBE MP,
Speech at The Adam Smith Institute, (September 13 2011)
“ We need to help people to manage their diabetes, especially because we
want them to have control over their health care and to spend less time
in hospital.”
Prime Minister, Rt Hon David Cameron MP,
Prime Minister’s Questions (June 15 2011)

6 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 7
Lord Rennard MBEChair of the Working Group
October 2011
Dear Colleague,
It has been my pleasure to Co-Chair this Working Group with my parliamentary colleague, the Lord Harrison, and we are
delighted to launch the findings of the Keeping People With Diabetes out of Hospital Working Group. This report is the
culmination of two ‘deep dive’ roundtables, and a call for evidence from the diabetes clinical community. The Working
Group has scoped out the issue of hospital admissions amongst people with diabetes, proposed a series of practical
recommendations and has strived to identify initiatives that are working to keep people with diabetes out of hospital.
We have been singularly impressed by the innovation and creativity that we have been party to throughout this project;
it is clear that there is a plethora of excellent initiatives taking place across the NHS in England and we hope that this
project will go some way in shining a light on these areas of excellence.
As a member of the All-Party Parliamentary Group on Diabetes, but perhaps more importantly as a person with diabetes,
I am acutely aware of the pressure our diabetes services and clinicians are under in this climate of change in the NHS. Sir
David Nicholson, Chief Executive of the NHS, has set us a challenge – to make £20billlion worth of efficiency savings over
the course of the next three years. This is not just a cost cutting exercise; instead the NHS must continue to improve the
quality of services whilst ensuring that care is delivered in the most efficient way possible. This quality and productivity
challenge is formally embodied in the Department of Health’s QIPP agenda, or Quality, Innovation, Productivity and
Prevention (QIPP).
It is widely understood amongst the diabetes clinical community that people with diabetes are more likely than to be
admitted to hospital than those without the condition. This places a considerable burden on NHS resources, but more
importantly this is often an avoidable and unnecessary worry for the patient, their families and carers. Indeed, Prime
Minister David Cameron himself noted that we need to help people to manage their diabetes better. When addressing the
House of Commons during Prime Minister’s Questions he said, “we want them [people with diabetes] to have control over
their health care and to spend less time in hospital.”2
As a result, the Government is actively encouraging clinicians to find new ways of working to tackle such challenges, whilst
achieving substantial cost savings and utilising existing resources. This project has purposefully taken a solutions focused
approach; bringing together clinical experts to recommend ways to achieve real cost savings whilst improving patient
outcomes.
2 Prime Minister’s Questions, June 15 2011
Critical to meeting this challenge is to break down the barriers between health care professionals and to encourage good, productive dialogue on the ground. What has become clear to us is that doctors, nurses and GPs by their own admission, are not always very good at talking to one another and most importantly, sharing their experiences and insight into their ways of working. This report clearly demonstrates that, in spite of the considerable challenge we face in keeping people with diabetes out of hospital, there is a wealth of expertise on the ground that is driving our diabetes services forward, constantly innovating and consistently striving to deliver and I sincerely hope we can build on this work in the months and years ahead.
I would like to thank my Co-Chair Lord Harrison for his expertise and insight and to Sanofi for their continued support and commitment to improving patient outcomes in diabetes. Finally, I would like to thank the members of the Working Group who have lent their time and expertise to this important project. For our part, we will take these findings to our parliamentary colleagues and continue to speak out for improved diabetes services. We call on you, those on the frontline, to continue to innovate, to continue to share and to continue to strive to attain excellence in diabetes care. Yours faithfully,
Lord Rennard, MBE Chair, Keeping People with Diabetes out of Hospital Working Group

8 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 9
Dr Paul Downie Primary Care Diabetes Society
Caroline HorwoodSanofi
Dr Roger Gadsby MBEProject Working Group
The Primary Care Diabetes Society (PCDS) is delighted to
present this report on behalf of the Keeping People with
Diabetes out of Hospital Working Group. As an organisation
PCDS are constantly striving to support primary care
professionals to deliver high quality clinically effective care, in
order to improve the lives of people living with diabetes. This
project has enabled us to come together with our secondary
and emergency care colleagues and work in partnership on this
critical challenge in diabetes care; how to negate the trend of
high hospital admission rates among those living with diabetes.
This project has presented us with an invaluable opportunity to
assess and reflect on the state of diabetes care, particularly as
we transition into the new NHS. What is clear is that we must
take a holistic, multidisciplinary approach to diabetes care,
striving to provide a fully integrated service.
Jennifer Dixon, director of the Nuffield Trust, noted that
integration is crucial to the future of the NHS and to delivering
the savings that Sir David Nicholson demands. “One of the
areas where there is huge inefficiency is that care is currently
quite fragmented and not proactive enough,” she says. “It
does not reach out to people and there is an enormous divide
between primary and secondary care.” With this project we
have aimed to tackle just this.
The recommendations proposed in this report cover all aspects
of the patient care pathway and are not solely focused on
primary care. Our objective has been to look at the care
pathway in its entirety and identify ways in which we, the
health care professionals, can work with policy makers to
keep people with diabetes healthy and out of hospital. The
revision and improvement of care pathways has proven to be
an effective means of achieving this. Indeed, care pathways
that are less complex, involve fewer appointments or referrals
and are more clearly defined can result in higher quality, more
patient-focused care.
This project has not only set out to review the clinical scenario
in isolation. We have called upon our NHS colleagues to share
any methodology they have followed to tackle admission rates
in their own locality. In our efforts to collate these examples
of best practice we have seen compelling evidence of the
impact that an improved or revised care pathway can have on
patient outcomes. It is imperative that we not only share these
experiences but that we also take these learnings on board and
apply them, where appropriate, in our own settings.
Sanofi are delighted to support the Primary Care Diabetes
Society in this critical area of diabetes care. We are
pleased to work alongside the diabetes clinical community
to assess the diabetes patient care pathway and shine
a light on the plethora of best practice that is currently
taking place in the NHS. This report provides a platform
for health care professionals to learn from their colleagues
across England, and, we hope, will encourage closer ways
of working as we all work to create a more integrated NHS.
At Sanofi, we are committed to working in partnership
with the clinical community and professional associations,
patients and patient groups, managers and policy groups to
facilitate debate, share best practice and improve outcomes
for people with diabetes. In that endeavour, this initiative
under Lord Rennard’s chairmanship is an excellent example
of collaborative working, and I urge for the recommendations
and best practice examples in this publication to be fully
implemented.
On behalf of the members of the Working Group I would
like to thank Lord Rennard and Lord Harrison for their
wholehearted support of this project. We are grateful to them
both for lending their time and expertise, particularly when
both are in such demand. As clinicians with a specialism in
diabetes, we face a considerable challenge in keeping our
patients healthy and out of hospital. In the ever changing
NHS environment we must work together, utilising resources
such as this report, to learn from one another, taking an
innovative eye to the care pathway and consistently striving
for excellence for our patients.

Keeping People with Diabetes Out of Hospital 1110 Primary Care Diabetes Society
Recommendations Scope of the project
The Primary Care Diabetes Society (PCDS) convened a Working
Group of diabetes clinical experts, including GPs with a Special
Interest (GPSIs), diabetologists, Diabetes Specialist Nurses (DSNs),
public health professionals and patient group representatives
to take a closer look at the rate of hospital admissions amongst
people with diabetes with the following objectives in mind:
The Working Group met on two separate occasions in West-
minster in May and July of 2011. The two policy roundtables
were chaired by Lord Rennard MBE, member of the All-Party
Parliamentary Group on Diabetes, and Lord Harrison, Vice Chair
of the All-Party Parliamentary Group on Diabetes and supported
by Sanofi via an unrestricted educational grant.
Members of the Working Group were as follows:
z Lord Harrison, Vice-Chair,
All-Party Parliamentary Group on Diabetes
z Lord Rennard MBE, Member,
All-Party Parliamentary Group on Diabetes
z Adrian Sanders MP, Chair,
All-Party Parliamentary Group on Diabetes
z Dr Belinda Allan, Workstream Lead,
Joint British Diabetes Society
z Sarah Astles, Senior Policy Officer,
Juvenile Diabetes Research Foundation
z Dr Charles Bodmer, Consultant Physician & Diabetologist,
Colchester Hospitals University NHS Foundation Trust
z Louise Brant, Government Affairs Manager,
Sanofi
z Dr Richard Brice, GPSI,
Kent
z Dr David Cartwright, Diabetes Lead,
NHS Lincolnshire
z David Davis, NHS Pathways Development Manager,
South East Coast Ambulance Service NHS Foundation Trust/
College of Paramedics
z Dr Paul Downie, GPSI Diabetes,
Primary Care Diabetes Society
z Elizabeth Dunsford, Public Health Specialist,
NHS Ealing
z John Fellows, Senior Policy Officer,
Diabetes UK
z Dr Roger Gadsby MBE, GP & Associate Clinical Professor,
Warwick Medical School
z Patricia Gilliard, PDSN, King’s College Hospital NHS
Foundation Trust
z Dr David Haslam, Chair, National Obesity Forum
z Jill Hill, Nurse Consultant Diabetes, Birmingham Community
Healthcare NHS Trust
z Fiona Kirkland, Diabetes Nurse Consultant,
South Staffordshire PCT
z Dr Stephen Lawrence, GPSI Diabetes,
Medway NHS Trust
z David Newman, Head of Public Affairs,
Juvenile Diabetes Research Foundation
z Michaela Nuttall, CHD co-ordinator for Bromley PCT,
Primary Care Cardiovascular Society
z Dr Paul O’Hare, Director of Quality Assurance,
Warwick Medical School
z Dr Gerry Rayman, Clinical Lead Diabetes In-Patient Care,
Ipswich Hospital NHS Trust
z Rebecca Reeves, Head of Professional Relations,
Sanofi
z Anna Reid, Nurse Consultant,
Guy’s and St. Thomas’ NHS Foundation Trust
z Sheila Smyth, Lead DSN,
North East Essex NHS
z Stella Valerkou, Senior Policy Officer,
Diabetes UK
z Grace Vanterpool MBE, Consultant Nurse,
Hammersmith and Fulham NHS Foundation Trust
z Dr Chris Walton, Chair,
Association of British Clinical Diabetologists
For the purposes of this report, this group of clinical experts will
be referred to as ‘the Working Group’.
Incentivise GPs to target people with pre-diabetes – a register of patients in a pre-diabetic state (IGT/ IFG/ Gestational diabetes) should be included in the Quality Outcomes Framework (QOF). QOF points should be available to GPs who a) put pre-diabetics onto a register, and b) provide these at-risk patients with the necessary management plan to ensure they prevent or delay the onset of diabetes.
Effective patient referral by ambulance services – after an acute episode of hypoglycaemia, the ambulance services must refer the patient to the appropriate primary/secondary healthcare professional. The ambulance services must look at both the short term and long term management of the patient’s condition including risk management, prevention and avoidance.
Appropriate access to treatments – in the new NHS, the clinical community are under increasing pressure to meet the QIPP challenge of making £20billion worth of efficiency savings. It is imperative that clinicians are not forced to jeopardise or compromise the standard of care that they make available to people with diabetes.
GPs to develop strategies to identify and reach vulnerable groups – GPs should develop out-reach strategies to focus on ‘hard to reach’ groups, to support them in the management of their diabetes and keep them out of hospital.
PCTs to invest in the work force – junior doctors and nurses must be educated and trained in the appropriate discharge procedures for patients with diabetes to avoid further complications and possible readmission.
Access to patient records across the NHS – consideration should be given by PCTs and Ambulance Trusts to the challenge of patient consent and clinical access to patient records across the NHS to help the health care professional, be they GP, DSN, paramedic or diabetologist, to administer care whilst fully informed of the patient’s history.
Specialist care to be made available in all PCTs – integral to optimal diabetes service provision is the availability of specialist care.
Integrated, multi-disciplinary teams – closer working relationships across commissioning groups between community health care professionals, such as podiatrists and dieticians, and secondary care specialists, is vital to ensure that the patient receives a comprehensive and consistent service.
1. To identify why people with diabetes are more likely to be admitted into hospital;
2. To assess the impact this trend has on the patient and the NHS;
3. To propose a series of practical recommendations for primary, emergency and secondary care professionals, managers and commissioners to take into consideration;
4. And to identify where successful hospital avoidance strategies are being implemented in diabetes care across England and highlight the initiatives as best practice.

Keeping People with Diabetes Out of Hospital 1312 Primary Care Diabetes Society
Why do people with diabetes end up in hospital?As Dr Rowan Hillson MBE, National Clinical Director for Diabetes,
observed, “we know what to do, so why aren’t we doing it?”2
National clinical guidance, including a NICE Quality Standard for
Diabetes in Adults, encapsulates the optimal standard of care
that people with diabetes are entitled to. A consensus exists
amongst the diabetes clinical community on what needs to be
done, and yet many people with diabetes are not receiving the
care and support they need to keep them healthy, in control of
their diabetes and out of hospital.
For example, according to the National Institute for Clinical
Excellence (NICE);
“All patients should receive nine crucial tests from their
GP at an annual review of their diabetes management.
These include measurements of weight, blood pressure,
smoking status, a marker for blood glucose called
HbA1c, urinary albumin, serum creatinine, cholesterol,
and tests to assess whether the eyes and feet have been
damaged by diabetes.
These tests are essential to ensure that diabetes is
controlled. If left unchecked, diabetes can lead to
blindness, kidney failure and increase the risk of
developing cardiovascular problems such as heart
attacks and stroke.”3
The National Diabetes Audit for 2009-2010, carried out by NHS
Diabetes, reported that only half of people with Type 2 diabetes,
and less than a third of those with Type 1 diabetes, receive
2 National Diabetes Audit Executive Summary 2009-2010, 2011, NHS Information Centre, p.53 Diabetes care improves, but patients still missing out on key tests, NICE, 2010, www.nice.org.
uk/newsroom/news/DiabetesCareImprovesButPatientsStillMissingOutOnKeyTests.jsp
all nine of the NICE recommended care processes as part of
a complete care bundle. The Audit also reported significant
variation in the individual checks being carried out. For example,
weight measurement and HbA1c checks are carried out most
frequently.4 However, the care processes that check for the
emergence of early complications are not being carried out
to a sufficient level, leaving a large proportion of patients un-
assessed and at risk of developing complications.5
The 2009-2010 Audit also revealed that glucose control levels
in England are not improving. 37% of people with diabetes are
at high risk of future complications due to glucose control above
recommended levels. These results are similar to those found
in the 2006-2007, 2007-2008 and 2008-2009 audits and
therefore demonstrate no improvement.6
What are the key challenges?
The Working Group assessed the current clinical practices and
scoped out the key challenges in keeping people with diabetes
out of hospital. The Working Group discussed the following
issues in detail: complications; delayed diagnosis; social and
demographic circumstances; referral; access to information;
patient confidentiality and consent; and finally the transition into
the new NHS.
a. Complications
Poorly managed diabetes can lead to a range of complications
including amputation, kidney disease, strokes, heart attacks,
depression and blindness. As a result diabetes increases the
chance of a person needing hospital admission by five times.7
This predisposition to complications is further compounded by
the fact that over half of people diagnosed with Type 2 diabetes
already show signs of complications at the point of diagnosis.
This is a widely reported statistic and the Yorkshire and Humber
Public Health Observatory (YHPHO) acknowledge that early
diagnosis and treatment can reduce the risk of complications
that can be found to be well developed at the point of diagnosis.8
However, it was noted by the Working Group that these statistics
4 National Diabetes Audit Executive Summary 2009-2010, 2011, NHS Information Centre, p.115 National Diabetes Audit Executive Summary 2009-2010, 2011, NHS Information Centre, p.116 Ibid, p.147 Turning the Corner: Improving Diabetes Care; A Report from Dr Sue Roberts National Clinical
Director for Diabetes to the Secretary of State for Health, June 2006, Department of Health, p. 138 Diabetes Key Facts, 2006, Yorkshire and Humber Public Health Observatory, p. 15
are dated, and therefore the situation will have almost certainly
improved to an extent, although we lack the evidence to prove it.
The recent National Diabetes Audit noted that the majority of
complications develop after a long period of exposure to high
blood glucose, high blood pressure and high cholesterol. When
coupled with reports that rates of care processes and treatment
target achievement are low, particularly in young people, this
raises concerns for the future. The increasing prevalence of
diabetes will in turn mean that the rate of diabetes related
complications will also increase, negatively impacting on patient
outcomes, and of course on NHS resources.
It is widely acknowledged that a significant proportion of the
NHS diabetes budget is spent on ‘final outcomes of care’,
or complications. Indeed, a report by the NHS Institution for
Innovation and Improvement in 2006 found that diabetic
complications account for almost 20,000 emergency admissions
per year at a cost in excess of £40 million.9
A recent review by NICE of the Clinical Guideline (CG15) – Type
1 Diabetes: diagnosis and management of type 1 diabetes in
children, young people and adults – concluded that the guideline
needs to be updated in order to better reflect the screening
and management of complications such as coeliac disease,
retinopathy, neuropathy and psychosocial aspects.10
b. Delayed diagnosis
Proactive targeting of ‘at-risk’ groups was highlighted by the
Working Group as an important risk management technique.
Such groups might include people who have Impaired Glucose
9 The views of people with diabetes, Key findings from the 2006 survey, 2006, Healthcare Com-mission
10 Review of Clinical Guideline (CG15) – Type 1 Diabetes: diagnosis and management of type 1 diabetes in children, young people and adult, NICE, www.nice.org.uk/nicemedia/live/10944/56133/56133.pdf
Regulation (IGR) or women with gestational diabetes. The
Working Group noted that a high level of resources are currently
concentrated on diabetes registers. It was proposed by the
Working Group that attention should be focused on lifestyle
management of those in a pre-diabetic state (Impaired Glucose
Regulation (IGR) / Impaired Glucose Tolerance (IGT) / Impaired
Fasting Glycaemia (IFG)) to help people avoid developing
diabetes.
It is widely accepted that early diagnosis and treatment can
reduce the risk of complications. The Working Group agreed
that early diagnosis would better enable primary care health
professionals to support patients in avoiding complications, and
ultimately emergency admission.
The Working Group suggested that, as part of the Public Health
Outcomes Framework, a register of people with gestational
diabetes and IGR should be recorded to enable primary care
clinicians to identify those at risk at an early stage in the
development of the condition. The existence of a register alone
is not enough. It must be fully endorsed by the health care
practitioners and those patients on the register must be given
access to the necessary lifestyle management and education
programmes. [See Case Study 2]
c. Vulnerable groups
As part of the process of striving for early diagnosis, it is
important that we identify those groups who are not only
physically at risk of developing diabetes related complications,
but also those whose demography and social circumstances
place them in a vulnerable position. Identification of at-risk
groups by primary and community health care professionals is
part of the solution, however patient awareness and engagement
is also crucial. It was noted that patients need to be aware if they
are at risk, and should be able to identify if they need to visit their
GP and be happy to do so.

14 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 15
BAME Community
When identifying and targeting these ‘at-risk’ groups, the
Working Group noted that any risk management strategies
must be tailored to the demographic and needs of the local
community. For example young people in BAME communities
are particularly at risk of developing Type 2 diabetes, and any
prevention strategies must consider the makeup of the local
patient population and any cultural aspects relevant to care.
For example, it was noted that within the Muslim community
diabetes is a taboo subject, particularly in terms of marriage.
Therefore, to ensure good patient outcomes it is essential that
the patient’s treatment is managed sensitively and appropriately.
The National Diabetes Audit demonstrated that young people in
the BAME community, who also fall in the lower quartile of social
deprivation, are associated with higher risk glucose control.11
The Audit data also clearly demonstrates that all complications
are statistically associated with social deprivation.12
Older People
A report by the Institute of Diabetes for Older People (IDOP)
(2011) noted that the median age of inpatients in more than
200 Acute NHS Trusts was 75 years and the majority had
been admitted as an emergency. This report also found that
factors which increase the likelihood of hospital admission of
older people included care home residency, mis-management
of medication and carer fatigue, among others.13 A report by
Diabetes UK (2010) found that six out of ten care homes in
England, which have residents with diabetes, fail to provide any
training to their staff about the condition. 14 Diabetes UK also
found that only 23% of care homes screen their residents for the
11 National Diabetes Audit Executive Summary 2009-2010, 2011, NHS Information Centre, p.1412 National Diabetes Audit Executive Summary 2009-2010, 2011, NHS Information Centre, p.2113 Keeping Older People with Diabetes out of Hospital – improving outcomes, saving money and
maintaining quality of life and dignity, 2011, Institute of Diabetes for Older People14 Diabetes in care homes – Awareness, screening, training, 2010, Diabetes UK
condition on admission. The report concluded that this missed
screening meant that as many as 13,500 care home residents
could have undiagnosed Type 2 diabetes and were therefore
at increased risk of developing complications.15 All diabetes
complications (excluding Diabetic Ketoacidosis) become more
likely with increasing age and duration of diabetes so it is vital
that this group have their condition closely monitored.
The IDOP report concluded that all older people and their carers
should be educated about the signs and symptoms of diabetes
related complications. The report also recommends that diabetes
care within care homes must be enhanced, with carers supported
in the identification of at-risk patients.16 The Working Group noted
that diabetes care given in care homes is often not appropriate
and that support needs to be available to care workers to ensure
that specialist diabetes care is available where necessary. [See
Case Study 5]
Children & Young People
The Working Group acknowledged that a significant proportion
of children diagnosed with diabetes will have been subject to
a delayed or prolonged diagnosis process. The Working Group
suggested that many of these children present symptoms, which
are sometimes very serious, weeks before they are eventually
diagnosed; and many are only diagnosed after experiencing
complications. The National Diabetes Audit shows that only 4.1%
of children over the age of 12 are receiving all of the NICE key
processes and over 30% of children and young people have
a high risk HbA1c measure, leaving them vulnerable to future
complications.17 The National Diabetes Audit revealed that whilst
social deprivation, gender and the duration of diabetes have
no impact on the likelihood of the nine care processes being
completed, age is a critical variable.
Socio-economic deprivation
Research shows that complications of diabetes such as
retinopathy or cardiovascular disease are more prevalent in areas
of high socio-economic deprivation. Research based on GP
registrations suggests that the prevalence of diabetes in the most
deprived quintile of census output areas was 66% higher than
the most affluent quintile.18 [See Case Study 7]
15 Diabetes in care homes – Awareness, screening, training, 2010, Diabetes UK16 Keeping Older People with Diabetes out of Hospital – improving outcomes, saving money and
maintaining quality of life and dignity, 2011, Institute of Diabetes for Older People17 National Diabetes Audit Executive Summary 2009-2010, 2011, NHS Information Centre, p.2918 Diabetes Key Facts, 2006, Yorkshire and Humber Public Health Observatory (YHPO), p. 11
d. Patient referral
The Working Group noted that the diabetes care pathway can
often be complex and disjointed, and as the patient makes their
way through primary, emergency and secondary care referral
processes, critical information can be miscommunicated,
inaccessible or lost entirely. The Working Group agreed that the
ambulance services and paramedics have a vital role to play in
managing the effective referral of people with diabetes and have
unparalleled access to those most vulnerable to complications.
The National Clinical Quality Improvement Framework for
Ambulance Services have included a pilot marker of “Direct
referral made to an appropriate health professional”, as part of
the Hypoglycaemia Clinical Performance Indicator Audit Cycle
6 – February 2011. This pilot marker has shown wide variation
between ambulance services ranging from 1.9 to 83.9%.
The National Diabetes Support Team (2008) reported that there
are an estimated 100,000 emergency 999 calls every year for
diabetes related emergencies and of them, 35% come from
just 11% of addresses, which clearly points to the existence of
repeat callers.19 The Working Group agreed that the Ambulance
Service is often treated by certain diabetic patients as a
surrogate service, particularly for those patients who are not
good at self management. The Working Group noted that the
Ambulance Service is perhaps ‘too good’ at helping patients with
hypoglycaemia, giving them a short term solution, but not always
facilitating long term management of their condition. Assisting
people with diabetes in the management of their care at home, with
support from community and primary care, would have a significant
impact on patient outcomes and reduce hospital admissions.
One obstacle identified in achieving a consistent referral process,
is that not all patients want to be referred to a secondary care
specialist, or their GP. Crucially though, the Ambulance Service
does have access to hard to reach groups, such as patients with
mental health, drug and alcohol misuse problems i.e. those who
19 Improving emergency and inpatient care for people with diabetes, 2008, National Diabetes Support Team, p.3
may be unable, or choose not to, have a relationship with their
doctor or specialist nurse.
e. Access to information
Limited access to information on what happens to patients
after acute treatment is also very challenging for GPs and poor
communication can effectively hamstring the entire process.
The Working Group cited NICE guidance that states that after a
patient has experienced hypoglycaemia that requires third party
assistance, they ‘ought’ to notify their GP. However, research
shows that this rarely happens. It was agreed that technology
could be used more effectively to manage patient records, and
enable more efficient access to patient information across the
NHS. This would allow GPs, paramedics and specialists to make
informed referral decisions. The introduction of Insulin Passports
was noted by the group but concerns were raised over their
effective implementation.
It was also suggested that stratification of those patients
consistently presenting with hypoglycaemia would enable
clinicians to determine if different treatment regimes or services
would be more appropriate for that patient.
f. Patient Confidentiality and Consent
Patient confidentiality and consent was a recurring area of
contention for the Working Group. The relationship between
the health care professional and the patient is very important,
based on trust and integrity, but there are times when this
can come under strain. If a patient has been admitted due to
hypoglycaemia, they are often reluctant to share this information
with others, for example with the Driver and Vehicle Licensing
Authority (DVLA), as their right to hold a licence can be
withdrawn. This presents health care professionals with a moral
and clinical dilemma.

Keeping People with Diabetes Out of Hospital 1716 Primary Care Diabetes Society
The Working Group acknowledged that patient confidentiality
must be maintained, however, the system should still allow for the
free flow of information between healthcare professionals, where
appropriate and with patient consent. It was suggested that most
patients expect the communication channels to be in place and
fully functioning, and will rarely say no to offering their consent,
but the reality is that the current system does not lend itself to
this fluid exchange of information. It was concluded that the
fear of confidentiality needs to be challenged, in order for a fully
integrated health service to function. 20
g. Ways of working in the new NHS
The Working Group raised concerns over the consistent
delivery of care in the new NHS. NHS Health Checks were
cited as an example where consistent delivery is by no means
guaranteed. These checks present health care professionals
with an invaluable opportunity to identify those at risk of
developing diabetes and to diagnose the condition. However,
the Working Group noted that in each local health economy
they are administered differently. Such inconsistencies and
inequities could become exacerbated in the new NHS, to the
detriment of the healthcare professional’s ability to identify
those with diabetes.
20 Diabetes Key Facts, 2006, Yorkshire and Humber Public Health Observatory (YHPO), p.3
The issue of re-admissions was also raised, in particular, patients
receiving inconsistent care in the primary and acute setting.
For example, when a patient is admitted into hospital after
experiencing hypoglycaemia they are often given standard oral
treatments that contain higher levels of longer acting insulins,
compared to intravenous insulin. If the patient is receiving
medication with higher levels of insulin than they are used to,
they are at risk of suffering complications which can lead to costly
emergency re-admission.
The Working Group was unanimous about the impact of GPs
and hospital doctors working together to achieve good patient
outcomes. It was also agreed that the barriers to this effective
working relationship, are similar to those barriers that stand in the
way of a good patient-doctor relationship.
It was noted that primary, emergency and secondary care
clinicians must have shared goals, and for this to be achieved,
health care professionals need to get better at networking with
one another. This applies to clinicians across the care spectrum:
specialists, GPs, commissioners, diabetes specialist nurses,
podiatrists and dieticians. Will alone is not sufficient, the means
of communication are also vital. It was agreed that improved
communications structures, incorporating new technologies,
would help with this change. However, concerns were voiced
over the future of this peer-to-peer relationship and diabetes
care in the new NHS. It was noted that GP commissioning will
certainly be an effective way of managing resources for short
term procedures, but commissioning for chronic care could be
at risk. It was concluded that high quality care is not possible
without cooperation, which should be at the heart of the Health
and Social Care Bill. It was also noted that the Diabetes Quality
Standard should ensure that services for long term conditions are
commissioned effectively.
It has been estimated that the NHS spends approximately
£25million a day treating people with diabetes, whilst the
estimated percentage of the NHS’ annual budget dedicated
to the treatment of diabetes ranges from 5-10%, depending
on the source. When assessing the cost of diabetes and
its complications, it is important to consider the financial
implications beyond the acute admission. According to the
YPHO, 1 in 20 people with diabetes incur social services
costs, with more than three quarters of these costs associated
with residential and nursing care, whilst home help services
accounted for a further one-fifth.21 A report by the King’s Fund
further noted that the presence of complications increased
social services costs four-fold.22
When it comes to assessing the financial burden of diabetes
on the NHS, there is a notable lack of recent data on which
to calculate a realistic figure. A report from the Yorkshire and
Humber Public Health Observatory (YHPO) in 2006 suggested
that the total annual cost of diabetes care is £1.3 billion. It is
perhaps most concerning that the YHPO also notes that the
presence of diabetic complications “increases NHS costs five-
fold”.23 It is estimated that acute admissions due to diabetic foot
disease alone costs the NHS £252 million per annum.24
21 Diabetes Key Facts, 2006, Yorkshire and Humber Public Health Observatory (YHPO), p. 722 Type 2 diabetes. Accounting for a major resource demand in society in the UK, 2000, King’s Fund.23 Diabetes Key Facts, 2006, Yorkshire and Humber Public Health Observatory (YHPO), p. 624 Improving emergency and inpatient care for people with diabetes, 2008, National Diabetes
Support Team, p.5
These figures are dated, but in light of the National Diabetes
Audit revealing the increasing prevalence of diabetes, particularly
in young people, it would be prudent to assume that the cost of
diabetes and related complications is set to increase dramatically.
In an interview with BBC Radio 4, Dr Bob Young, clinical lead for
the National Diabetes Information Service, noted that the rising
number of young people with Type 2 diabetes will have “huge
cost implications for the NHS”.25 (N.B whilst the prevalence of
diabetes increases annually, we must also consider increased
screening, diagnosis and reporting.)
A report from the Audit Commission and the Association of
Chartered Certified Accountants (ACCA) (2011) attempted to
cost the diabetes care pathway. It acknowledged that the lack of
quality data made it very difficult to evaluate the financial impact
of care pathways that had been actively improved, and whilst it
is widely understood that simpler, patient focused pathways are
more effective, it is hard to quantify the financial benefits.26
25 Today Programme, 2011, BBC Radio 4, http://news.bbc.co.uk/today/hi/today/news-id_9525000/9525601.stm
26 Costing Care Pathways, 2011, Association of Chartered and Certified Accountants (ACCA) and the Audit Commission, p.5
The Financial Burden
The Cost of Acute Care for Diabetes
The Audit Commission and ACCA costed both elective and emergency acute
care for people with diabetes, using Hospital Episode Statistics (HES) and the
Department of Health National Tarriff. The results were as follows:
zz Treatment specifically for diabetes (diabetes mellitus, diabetes with
lower limb complications, diabetes with hypoglycaemic emergency)
accounts for 54% of spending in inpatient care.
zz Treatment for diabetes related conditions (eyes or vascular
system) accounts for 38% of spending in inpatient care.
Source: Costing Care Pathways, 2011, Association of Chartered and
Certified Accountants (ACCA) and the Audit Commission
The Cost of Emergency Care for Diabetes
Between December 2009 and November 2010 the South Central
Ambulance Service NHS Trust carried out the largest UK survey to describe
the incidence of severe hypoglycaemia requiring an emergency attendance.
zz 398,409 emergency calls were received, of which 4081 (1.02%) were
recorded with hypoglycaemia as the ‘chief complaint’.
zz The study concluded that the estimated annual cost of emergency care
for diabetes in England would be equivalent to £16.9million.
Source: Incidence and costs of severe hypoglycaemia in diabetes requiring
attendance by the emergency service in the United Kingdom, 2011, A.J
Farmer, K.J. Brockbank, M.L. Leech et al.
18 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 19
Whilst it would seem intuitive to address the cost of diabetes
related emergency admissions in order to tackle the cost of
diabetes related inpatient care, the Costing Care Pathways report
revealed some interesting data. PCTs that spend the most on
emergency care were not always those spending the most per
patient on inpatient care. It also shows that those trusts spending
more on elective care tend to spend more per patient. ACCA
and the Audit Commission concluded that although reducing
emergency admissions is beneficial in terms of the patient
experience, ‘the cost savings may be less than expected’. 27
It is also important to look at those patients who are admitted
to hospital where diabetes is an additional complication and not
the primary diagnosis. A report by the National Diabetes Support
Team noted that in patients with diabetes stay in hospital longer,
irrespective of the primary cause of admission.28
27 Costing Care Pathways, 2011, Association of Chartered and Certified Accountants (ACCA) and the Audit Commission, p.11
28 Improving emergency and inpatient care for people with diabetes, 2008, National Diabetes Support Team, p.5
Based on the group’s discussions and their clinical experience,
the following recommendations were proposed.
Primary Care
;; It is proposed that as part of the 2012/2013 Quality
Outcomes Framework, an indicator is developed to
incentivise a pre-diabetic register.
;; Further it is proposed that a financial incentive is the most
appropriate course of action.
;; By incentivising GPs, additional resources and capacity
will be made available to maintain a register of pre-
diabetic patients. At-risk patients will be referred on to the
appropriate structured education programmes and provided
with the necessary life-style management techniques.
;; A QOF indicator would not only help incentivise GPs, but
would also raise awareness amongst nurses and other staff
members in the practice on the importance of targeting
these at-risk groups.
The number of people with Type 2 diabetes is increasing
each year, especially in deprived communities.29 Focusing
on those ‘hard to reach groups’ who are more susceptible to
complications as a result of mismanaging their diabetes, will
29 National Diabetes Audit Executive Summary 2009-2010, 2011, NHS Information Centre, p.30
reduce the number of people who are admitted into hospital.
;; ‘Hard to reach’ or ‘vulnerable’ groups could fall into one or
more of the following categories:
• People with diabetes who have a poor or non-existent
relationship with their primary care practitioner (e.g.
patients with mental health, alcohol, drug misuse
problems)
• People with diabetes who are disengaged or unaware of
the risk of complications they could be afflicted with as
a diabetic (e.g. pregnant women)
• People with diabetes who are in care homes, particularly
in the private sector, who do not have access to regular
contact with a diabetes specialist (e.g. older people)
;; It is important to reach these people before they become
unwell. Consideration should be given to a local strategy
whereby healthcare professionals go out into the community
in order to strengthen the relationship between the
healthcare professional and the person with diabetes e.g.
working with ante-natal groups, local pharmacies, private
and public sector care homes.
;; By establishing a level of trust, the person with diabetes is
more likely to engage with their condition; take on board
self-management techniques; and understand when it is
appropriate to seek medical advice.
;; Joint working presents healthcare professionals with an
opportunity to be streamlined and successful in reaching
patients. For example, Diabetes Specialist Nurses working
with Community Psychiatric Specialist Nurses would be
one way of targeting a particularly hard to reach group of
diabetics.
How to keep people with diabetes out of hospital The Working Group’s recommendations
Incentivise GPs to target people with pre-diabetes
- a register of patients in a pre-diabetic state (IGT/ IFG/ Gestational diabetes)
should be included in the Quality Outcomes Framework (QOF). QOF points
should be available to GPs who a) put pre-diabetics onto a register, and
b) provide these at-risk patients with the necessary management plan to
ensure they prevent or delay the onset of diabetes.
GPs to develop strategies to identify and reach vulnerable groups
- GPs should develop out-reach strategies to focus on ‘hard to reach’
groups, to support them in the management of their diabetes and keep
them out of hospital.

20 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 21
General
;; The sharing of specialist knowledge across the clinical
community and across commissioning groups, is critical to
keeping diabetes patients out of hospital.
;; To ensure that this specialist diabetes knowledge in
community, primary and secondary care is fed directly into
the commissioning process, the role of representatives on
Clinical Senates, representing sub-clinical areas, such as
diabetes, should be considered.
95% of diabetes management is self care; therefore patient
education is essential to keeping people with diabetes out of
hospital. According to the Diabetes National Service Framework
educational programmes can prevent or delay the development of
diabetes or its associated complications. Indeed, NICE guidance
suggests that the DAFNE educational programme is associated
with a net cost saving over 10 years of £2679 per patient and a
higher number of quality-adjusted life years.30
;; DESMOND, DAFNE and EXPERT are structured education
programmes already in place, however the volume of places
available to people with diabetes by PCT has yet to be
scoped and in some areas is inadequate.
;; It is important that these programmes are given the
necessary publicity by primary and community healthcare
professionals to ensure people with diabetes are aware of
them and are able to access the resources.
Emergency Care
;; A standardised referral procedure across commissioning
groups would be advisable to establish a continuity of care
in the long-term for patients who are seen by the ambulance
services.
;; It is important that any procedures put in place to
standardise the referral process are kept as simple and
straight forward as possible.
30 Guidance on the use of patient-education models for diabetes, 2003, NICE
;; The issue of consent requires careful planning in order to
protect the patient and maintain an appropriate level of trust
between the patient and the health care professional.
;; Critical to this consideration is consistency – co-ordinating
any access to patient information in primary, emergency and
secondary care must be done across the commissioning
group.
;; Strategies for the sharing of patient information must be
designed to fit the needs of the local health economy.
;; In the early stages of any strategy development, it would
be advisable to pilot any strategy amongst a small group of
vulnerable patients, for example, patients who have poor
self-management of their condition and regularly call on the
ambulance services.
;; Clinical commissioning groups could consider the following:
• Early opt-out consent register – Patients could give their
consent to their GP for information relating to diabetes
episodes to be shared in both directions across the
NHS.
• Voluntary card system – People with diabetes could
be encouraged to carry a small card detailing key
information on their condition, medication, emergency
contact information etc. This would enable paramedics
in particular to make informed decisions about the
patient’s care in an emergency situation.
Secondary Care
;; It is vital that on discharge, both the patient and the clinician
responsible for the ongoing care of that patient are fully
informed as to the type, volume and timing of any treatment
administered.
;; Mechanisms such as a Discharge Checklist are advisable
to ensure that junior doctors and nurses are adhering to a
standardised discharge procedure specifically designed for
patients with diabetes – whether it is the primary cause of
admission, or a secondary condition.
;; The focus must be on patient safety and outcomes, with the
long-term cost benefit of any treatment considered over and
above any short-term gain.
;; Consideration should be given by PCTs, and the emerging
Clinical Commissioning Groups, to the formation of “advisory
hubs” – an informed, multi-disciplinary group of healthcare
professionals who can be referred to for independent advice
and critique on whether seemingly ‘costly’ treatments are
appropriate for patients.
Primary and community healthcare professionals to develop and advertise structured patient education programmes
- GPs to work with community healthcare professionals to provide emotional
and psychological support and self-management techniques, enabling
patients to manage their condition day to day.
Appropriate access to treatments
- in the new NHS, the clinical community are under increasing pressure to
meet the QIPP challenge of making £20billion worth of efficiency savings. It
is imperative that clinicians are not forced to jeopardise or compromise the
standard of care that they make available to people with diabetes.
Specialist care to be made available in all PCTs
- integral to optimal diabetes service provision is the availability of specialist
care. A study into the bed occupancy for in-patients with diabetes before
and after the introduction of a diabetes inpatient specialist nurse service
(DISN) clearly showed that excess bed days can be reduced by 30% when
the correct specialist care is available.Access to patient records across the NHS
- consideration should be given by PCTs and Ambulance Trusts to the
challenge of patient consent and clinical access to patient records across
the NHS to help the health care professional, be they GP, DSN, paramedic or
diabetologist, to administer care whilst fully informed of the patient’s history.
Effective patient referral by ambulance services
- after an acute episode of hypoglycaemia, the ambulance services
must refer the patient to the appropriate primary/secondary healthcare
professional. The ambulance services must look at both the short term
and long term management of the patient’s condition including risk
management, prevention and avoidance.
PCTs to invest in the work force
- junior doctors and nurses must be educated and trained in the
appropriate discharge procedures for patients with diabetes to avoid further
complications and possible readmission.
Integrated, multi-disciplinary teams
- closer working relationships across commissioning groups between
community health care professionals, such as podiatrists and dieticians,
and secondary care specialists, is vital to ensure that the patient receives a
comprehensive and consistent service.
“Diabetes Specialist Nurses preventing acute admission.”
At the University Hospitals of Leicester, a team of diabetes
specialists nurses positioned themselves in A&E and
intervened when a patient presented with a diabetes related
complaint, and where possible, managed to avoid admission
altogether; it was estimated that this exercise saved the
hospital £100,000. This cost saving was then extrapolated
by Diabetes UK, who estimated that this would equate to a
national saving of £100million should the project be rolled
out across the UK.
“ I am aware of [this] excellent beacon of good practice in
Leicester, which is an example that we welcome. It is an
approach that is already being taken in other parts of the
country.”
Earl Howe, Parliamentary Under-Secretary of State for Health, House of Lords (14 July 2011)

Keeping People with Diabetes Out of Hospital 2322 Primary Care Diabetes Society
The value of sharing best practice
During the discussions of the Working Group, it became clear
that there are many examples of good working across the NHS
that are not receiving the publicity they deserve. The Group noted
that if best practice were more widely shared and adopted, the
inconsistencies in service delivery and the resulting ‘post-code
lottery’ in access to healthcare may, in some way, be addressed.
One initiative that falls under the Government’s QIPP agenda is
the NHS Atlas of Variation. In order to provide greater value to the
existing resources within the NHS, the variations in activity and
spend across the NHS need to be addressed. The Atlas maps
the variations in health spending and outcomes across England,
which in the case of diabetes care is considerable; in particular
the implementation of the nine critical tests, which make up the
Annual Review, as recommended by NICE.
These nine tests include measurements of weight, blood
pressure, smoking status, HbA1c, urinary albumin, serum
creatinine, cholesterol, and tests to assess whether the eyes
and feet have been damaged by diabetes. Treating these risk
factors reduces the development of complications, and the early
identification of complications allows patients to receive treatment
to slow the progression of heart disease, stroke, blindness – and
ultimately hospital admission.
For example, recent figures show that provision of podiatric
services is variable, and that a quarter of people with diabetes
were found to be missing out on vital foot checks. Diabetes
results in about 70 amputations a week in England, 80 per cent
of which are potentially preventable. In the National Diabetes
Audit, 19 PCTs recorded the delivery of all nine care processes in
60% of patients, whilst 2 PCTs reported delivering the complete
care bundle to less than 10% of their patients.31 The Audit also
demonstrates significant variation in rates of complications
at both the SHA and PCT level.32 In order to tackle these
inconsistencies it is imperative that where best practice exists,
with outcomes that can be quantified and evaluated, the detail is
shared.
31 National Diabetes Audit Executive Summary 2009-2010, 2011, NHS Information Centre, p.1132 National Diabetes Audit Executive Summary 2009-2010, 2011, NHS Information Centre, p.21
Sharing & adopting best practice
Overview
A bid was submitted to South Staffordshire PCT requesting
funding for a Diabetes Specialist Nurse (DSN) to work in care
homes. It is well documented that people who live in care
homes receive sub optimal care due to problems with access,
participation and a lower standard of understanding of diabetes
amongst the care home staff. It is recognised that people with
diabetes are admitted to hospital twice as often and remain in
hospital twice as long as people without diabetes. It can be seen
that by far the majority of admissions and re-admissions were
aged over 70 and many of these were from care homes.
The bid was successful and the care home project commenced
in September 2004. A district nurse applied for the job and
after 2 months of increasing her awareness of basic diabetes
management and developing skills in diabetes she began the
project with continued professional support.
Objectives
The service aims to improve the knowledge base and availability
of skills of staff in care homes by deploying a part time diabetes
specialist nurse for care homes to provide clinical leadership to
nursing home staff. Resultant improved management of diabetic
patients in nursing homes will reduce the number and duration of
diabetes related admissions.
;z To increase the knowledge base in the staff of care homes.
To allow them to gain an understanding of the reasons
underpinning the care being given.
;z To encourage the staff to develop empowerment skills
enabling residents with diabetes to continue to manage
diabetes themselves wherever possible.
;z To provide ongoing support and facilitation to both care
home staff and residents in the management of their
diabetes.
;z To identify problem areas within the diabetes management.
;z To agree goals with the person with diabetes and plan
interventions jointly wherever possible.
;z To extend skills of appropriate care home staff members in
the testing of blood sugars and giving of insulin injections.
Strategy
Second or recruit a diabetes specialist nurse for care homes
for one day a week to the project extending existing skills in
diabetes. In summary, the intervention is structured around 3
visits to the care home:
Pre-assessment visit
;z Meet with matron / care manager at the home to introduce
self and explain purpose.
;z Meet with those residents with diabetes and ask permission
to assess their diabetes with an aim of improving
management.
;z Ask residents permission to take blood samples.
;z Send letter to GP explaining purpose of visit.
;z Leave personal questionnaires with residents for completion
before 2nd visit date. Includes symptom status and their
areas of concern.
;z Request any hospital / GP notes to inform next visit.
Assessment visit
;z Where possible a small number of staff could be present
depending on individual residents consent, this allows
experiential learning to take place.
;z Go through diabetes questionnaire with resident where
appropriate.
;z Review blood test results.
Case Study 1 – Care Homes ProjectSouth Staffordshire Primary Care Trust
24 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 25
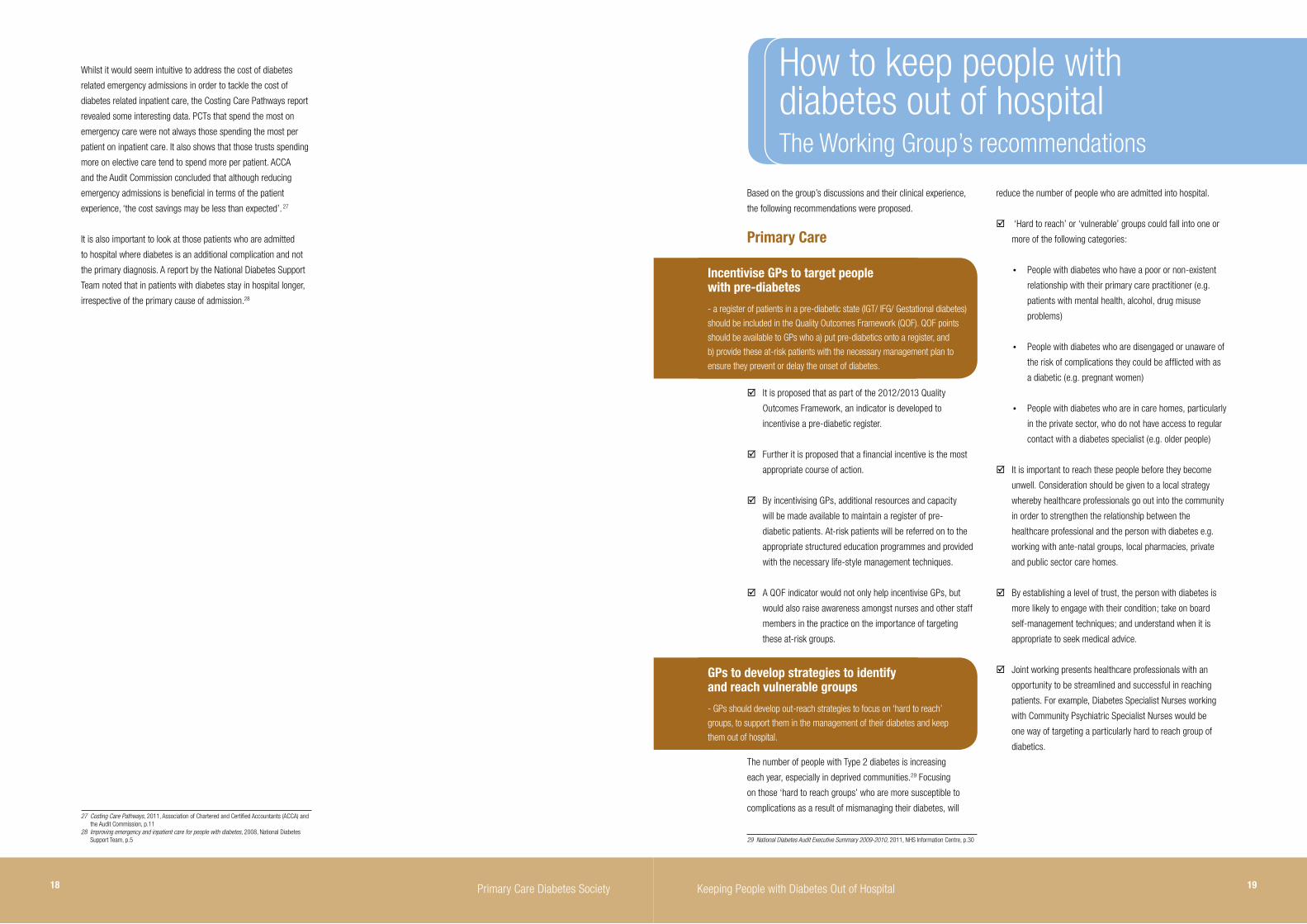
Outcomes
12 months before intervention12 months after intervention
(6 months real time/ 6 months projected)
Number of admissions (elective) 3 0
Number of admissions (emergency) 39 12
Number of bed days spent in hospital 236 116
TOTAL REDUCED ADMISSIONS 71.5%
TOTAL REDUCED BED DAYS 51%
3 residents had died in the 6 month period, one resident stayed for one visit of 40 days in hospital before death – this is included in the figures above*.
Cost savings
The calculation of cost savings, when looking at cost of
admissions, was impossible to determine as the cause of
admission may not be directly due to diabetes and the audit
demonstrated that diabetes is not always documented even
when present. Causes of admission were variable in this group
and often non-specific. Therefore bed days represented a more
accurate financial perspective.
Data taken from 9 care homes visited 6 months post visit:
zz 120 bed days saved = £30,600 (1 bed day = £255)
zz Proportional increase for the total 14 care homes = £47,600
zz Current cost of DSN for care homes + software assessment
tool = £10,000
SAVING PER ANNUM= £37,600
Recommendations
zz Increase DSN hours to 37.5 hours / week to fund a 2 year
secondment
zz 2 days to be spent in care homes, 3 days education,
facilitation and clinical
zz 2 days in care homes potential cost saving = £95,000
MINUS COST OF DSN = £43,000
COST SAVING PER ANNUM = £52,000
Other potential benefits as role continues to develop:
1. Increase the skills of care home staff to give insulin therefore
saving the cost of district nurse visits. These visits can be up
to 3-4 each morning to each home for insulin delivery and
again in the afternoon.
2. This development will also improve diabetes management as
insulin will be given at the correct time for the resident.
3. Allows more appropriate use of district nurse time.
4. Teaching the care home staff monitoring skills so that
changes in blood sugar levels, which could lead to admission
into hospital, are recognised early so reducing risk of
admission.
5. Begin to address those older people in care homes who are
unable to access the service.
6. Improvement in quality of life, increased ability to participate
in activities of daily living.
Achievement of NSF standards through the implementation
of the East Staffordshire Diabetes Strategy - education and
facilitation.
Contact Fiona Kirkland, Consultant Nurse for Diabetes
;z Assess episodes of hyper / hypoglycaemia.
;z Discuss medications, in particular insulin injections and
develop an agreeable programme on support in this area
in line with the UKCCs Scope of practice aiming for staff to
deliver insulin injections.
;z Discuss appropriateness of meal times.
;z Identify level of activity present. Presence of activity sessions
in the home.
;z Assess foot risk and individual foot care - ability to
participate in foot care.
;z Check eyes examined within the last year. Report should be
present.
;z Demonstrate aspects of care to residents and care home
staff.
Post Assessment visit
;z Compile a report for each person with diabetes visited.
Include agreed goals, how these will be worked towards and
any potential obstacles. Copy to home, resident and GP.
;z Compile an overall report to the home identifying areas of
good practice and areas for improvement.
;z Provide supporting literature.
;z Provide care pathways. These will then support care of
people newly admitted to the home who have diabetes.
After 6 months a care home study day is held to maintain
increased awareness in those homes visited.
Evaluation
June 2005
14 homes were identified by looking at the greatest numbers
of people referred to the diabetes centre from each, thereby
identifying a need. This was then followed by requests from the
homes and GPs as awareness of the project increased.
Prior to intervention:
1. Clinical outcomes are generally poor in this group
2. Chronic hypoglycaemia is common, severely affecting quality
of life
3. Admission rates are high
4. Re-admission rates are also high
Following the intervention an audit was carried out in order to
effectively measure the initiative’s impact. A list of people with
diabetes from each home was obtained. Each of these people
were visited on consent. Hospital admissions for each person
over the year previous to the visit were identified, clarified and
noted as follows:
1. Number of visits
2. Number of days spent in hospital for each visit
3. Number of elective admissions
4. Number of admissions directly due to problems with diabetes
[This information was gained from HISS data by looking into
process reports for each patient and admissions and discharge
data.]
Six months following the intervention the same patients visited
had their hospital records examined for the above criteria in the 6
months following the intervention visit.

26 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 27
3. To ensure all patients with diabetes in Nottingham city
are treated in line with current best practice national (i.e.
National Institute for Health and Clinical Excellence) and
local clinical guidelines.
4. To ensure that all activities are developed and implemented
in a way which improves the quality, efficiency and cost
effectiveness of care in line with national Quality, Innovation,
Productivity and Prevention (QIPP) objectives.
Strategy
A steering committee has been established with formal
partnership agreements and terms of reference to ensure
transparency. The project will be split into 4 broad phases:
1. Understanding the problem via an admissions audit;
2. Data analysis / identifying solutions;
3. Implementation of recommendations and solutions;
4. and evaluation.
Once the results of the audit are analysed and understood it will
allow us to identify areas where changes in practice and current
services could lead to a reduction in hospital admissions and
the steering committee will work collaboratively with all local
stakeholders to devise and implement these.
ImplementationPhase 1: Understanding the problem – The Admissions Audit (July 2010 – January 2011)
Patients with a diabetes related unplanned admission to
Nottingham University Hospitals sites between July 1st 2010 and
December 31st 2010 will have their treatment prior to admission
reviewed and benchmarked against best practice national and
local clinical guidelines. A specialist nurse will review the primary
and secondary care medical records of these patients and
through the use of a personalised questionnaire, patients will also
be given the opportunity to describe their own experience of the
care they received prior to admission.
Phase 2: Data Analysis – Identifying the solutions (February 2011 – April 2011)
The data collected via the audit process will be reviewed by
a multi-stakeholder expert group in order to identify common
factors (around patient management and circumstances leading
to the admission) which, if addressed could have the most
significant impact on admissions and patient outcomes. Local
guidelines and care pathways will be revised accordingly in
consultation with stakeholders across the health economy and
current service provision will be reviewed.
Phase 3: Implementation of Recommendations and solutions (May 2011 – December 2012)
Revised guidelines will be disseminated and new care pathways,
service models and services implemented. These will be
supported by a wide programme of education and support for
clinicians and other healthcare professionals working in the
community.
Phase 4: Evaluation (January 2013 – March 2013)
To evaluate the impact of any changes in practice, including
a re-audit and monitoring levels of unplanned admissions,
approximately 12 months after any necessary changes have been
implemented.
Improving the care pathway
There is significant evidence to suggest that proven care models
can reduce the incidence of: hospital admission, excess length
of stay, acute metabolic complications, diabetic foot disease and
amputation.33 However, when sharing and adopting best practice
it is important that outcomes are clearly presented and evaluated.
The Audit Commission and ACCA noted that “community and
outpatient care data is not good enough” and it is clear that
moving forward, the the quality of data collection needs to be
significantly improved.34
Cost efficient and cost effective diabetes care pathways are a
natural priority in light of the Nicholson challenge. However, the
Working Group noted that the fundamental goal must always
be the improvement of the patient experience. The following
initiatives have been identified by the Working Group as leading
the way in improving the patient care pathway, ensuring that the
33 Improving emergency and inpatient care for people with diabetes, 2008, National Diabetes Support Team, p.5
34 Costing Care Pathways, 2011, Association of Chartered and Certified Accountants (ACCA) and the Audit Commission, p.14
person with diabetes receives the right care, at the right time in
the right place, to keep them healthy and out of hospital.
Overview
NIMROD is an innovative collaboration between NHS Nottingham
City, Nottingham University Hospitals NHS Trust, Nottingham
CitiHealth, Diabetes UK and the pharmaceutical industry. The
project is equally funded by NHS Nottingham City and the
pharmaceutical industry and is expected to run for 2 years.
NIMROD will seek to understand why the rates for diabetes
related hospital admissions in Nottingham are higher than
average and then take steps to reduce the rate/number of
avoidable admissions to hospital for people with diabetes and
diabetes related illness.
Objectives
1. To understand why rates for diabetes related hospital
admissions in Nottingham city are higher than the national
average.
2. To reduce the rate/number of avoidable admissions to
hospital for patients with diabetes and diabetes related
illness.
Case Study 2 – Tackling diabetes related emergency admissionsNIMROD: Nottingham NHS and Industry Maximising Resources and Outcomes in Diabetes
The National Diabetes Support Team’s report into improving inpatient and emergency care for people with diabetes, outlines a number of proven
‘best practice’ care models in the UK. These models are cost effective and provide value for money and should therefore for rolled out consistently
across all diabetes care pathways.
These care models are based on specialist diabetes teams commissioned to deliver an enhanced service, which can include:
zz Inpatient diabetic nurse
zz Dietetic and foot care service for high risk patients
zz Educational programmes for all staff
zz Better care pathways between the ambulance service and the specialist diabetes team
Source: National Diabetes Support Team, Improving emergency and inpatient care for people with diabetes, (2008)
The report by the Audit Commission and ACCA notes that “good decisions
cannot be made without knowing how costs will change and whether
value for money will be achieved”. As a result they have developed a
Commissioning Costing tool for PCTs to evaluate spending and to compare
with others. The tool can be found at www.audit-commission.gov.uk/
diabetescostcomparisons.
28 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 29
5. Individual Care Plan. Practices should prepare with the
patient an individual care plan. A comprehensive print-out of
the agreed care plan will be provided for the patient to keep.
6. Record Keeping. Practices are to maintain records
incorporating the fasting sugar levels, blood pressure and
outcomes of cardiac risk assessment.
7. Training. Each practice must ensure that all staff involved
in providing any aspect of care under this service have the
necessary training and skills to do so. Please see ‘Training
and Accreditation’ section for further details.
Contact Dr Richard Brice, GPwSI Diabetes
Overview
The aim of this Local Enhanced Service was to address the
physical healthcare needs of pre-diabetic patients i.e. those with
impaired glucose tolerance (IGT), impaired fasting glycaemia (IFG),
previous gestational diabetes and other relevant type 2 diabetic
patients through recognising and encouraging the development of
the necessary expertise in primary care.
The Quality and Outcomes Framework (QOF) rewards practices
for ensuring that systematic care has been provided for type 2
diabetic patients. However practices are not required to undertake
a regular review for patients identified at risk of developing
diabetes, nor does it incentivise certain critical components of
care to patients with type 2 diabetes.
The specification of this service therefore outlines a more
specialised service to be provided, beyond the scope of essential
services and QOF.
Objectives
By expanding the capacity and skills within primary care this
enhanced service aimed to:
1. Prevent diabetes in those known to be at risk, and where
prevention fails, diagnose early to prevent complications;
2. improve the quality of diabetes care provided in the
community;
3. help deliver the National Service Framework standards; and
4. promote a safe, co-ordinated shift of the delivery of care for
patients from hospital clinics to primary care services.
Strategy Basic Principles
The patient and, where appropriate, their carer should be at the
centre of care and practice staff should support them in self-
management wherever possible.
For patients with IGT, IFG and previous gestational diabetes,
specific responsibilities in delivering this agreement include:
1. The development and maintenance of a register.
Practices must produce up-to-date registers of patients who
are IGT, IFG or who have previous gestational diabetes.
2. Call and recall. Practices will ensure the systematic recall
of all IGT, IFG and previous gestational diabetic patients
using appropriate read codes.
3. Review. Practices will review all patients on the IGT and IFG
registers annually, which must include fasting sugar check,
blood pressure and cardiac risk assessment as a minimum.
Women who have had gestational diabetes and have tested
normal following delivery should be tested 1 year post-
partum and then three-yearly.
A key part of the consultation at review is to emphasise
the message from the DPP (diabetes prevention program)
that the risk of developing diabetes can be reduced by
60% simply by implementing lifestyle changes involving a
better diet and regular exercise. We believe in the positive
reinforcement that patients are “masters of their own
destiny” and they can achieve more by themselves than we
can with drugs.
4. Education of patients. Practices must include education
and lifestyle advice in the annual review.
Case Study 3 – Local Enhanced Service to target pre-diabetes in primary careNHS Eastern and Coastal Kent – Enhanced Service for Diabetes Services

30 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 31
•z The recruitment of Diabetes Specialist Nurses to
cover all the Clinical Commissioning Groups (CCGs)
in Berkshire West would help to support primary care
healthcare professionals in treating complex cases,
reduce variations in care provision and to reduce
inappropriate referrals onto secondary care.
•z The Up-skilling of GP’s and other healthcare
professionals; enhanced capacity of structured
educational programmes for patients [Type 1 & 2]; the
introduction of integrated care; and a dedicated helpline
are other aspects linked to enhanced diabetes nurse
specialist support.
•z Our informatics team are administering a MiQuest audit
in all the GP surgeries, to find out the total numbers of
people actually registered with a diagnosis of diabetes.
•z We are also working with NHS Diabetes and the national
NHS Health Checks team in developing a pre-diabetes
pathway.
•z Locally the Royal Berkshire NHS Foundation Trust
pathology team is trying to identify people with IGT/IFG/
pre-diabetes by proactively following up all those who
have had some type of blood test or screening but who
have not yet been registered on the diabetes registers. A
local GPwSI has been identified to champion the project
including organising road shows in each local area to
raise awareness and lead the WBDC strategy group.
Monitoring
zz Supporting CPD/training and annual validation of skills to
practice diabetes in community.
zz Monitoring the diabetes care through the local strategy
group [WBDC] which has permanent representation from a
patient and Diabetes UK.
zz Monitoring the progress of the pilot through a specialist
sub-group.
Expected Outcomes
Seamless integrated diabetes care pathway across all 4 GP
consortia with high quality, consistent care with reduced variation
in primary care, close to home with multidisciplinary support,
education and self-management.
Contact Dr Onteeru Reddy, Programme Lead – Obesity & Diabetes
Overview
NHS Berkshire West’s Joint Strategic Needs Assessment (JSNA)
demonstrated considerable variation in outpatient and inpatient
referrals to secondary care. The data showed that more patients
were being referred on into secondary care from smaller GP
surgeries located in areas of relative deprivation.
In Berkshire West there are lower rates of people diagnosed
with diabetes (15,517) (QOF) compared to the rates expected
(22,120), in light of a predicted rise to 29,452 by 2020. At any
one time 14% of patients in the Royal Berkshire Hospital have
diabetes, with a further 30% likely to be undiagnosed. It was
also established that whilst 57% of patients with diabetes had
reasonably good control of their condition, the remaining patients
either had poor control (23%) or poor control with complex
needs (15%), with a further 5% of patients requiring referral to
secondary care, but could be managed in primary setting.
In addition, a local GP audit and mapping exercise was used
to identify current capacity and the gaps. This looked at the
recruitment of Diabetes Specialist Nurses (DSNs), identifying
GPwSI/PwSI in each practice and looking at where extra dietetic
and education support was required.
The general consensus from the diabetes strategy group (West
Berkshire Diabetes Care Group, WBDC) and the South Central
SHA was to provide care closer to the patient’s home and to
enhance the patient experience as part of a QIPP pilot.
It was agreed that an integrated care pathway, which links
primary, intermediate and secondary care and ensures the
continuity of a personal care plan, should be established. This
was an opportunity to improve clinical outcomes and financial
efficiency; to reduce the non-elective spend in secondary care;
and help to reinvest in primary care to achieve better patient
outcomes.
Objectives
zz Keep people well and out of hospital via better diabetic
management aiming to avoid unnecessary complications.
zz To improve diabetic management in primary care, looking
to carry out more care in the community, with less hospital
outpatient attendance.
zz To improve the range and quality of care management support
in the community by providing an integrated care system
including specialist support from consultants and nurses.
StrategyPhase 1 – Moving Diabetes Out-Patients (OP) into the Community (StartedOctober 2011)
Moving out of all routine OP diabetes appointments [except
insulin pump patients, pregnant women, teenagers and young
adults] through consultant led community outreach clinics. The
savings from Phase 1 are expected to be reinvested for Phase 2.
Phase 2 – Integrating Community Diabetes Service and Primary Care Diabetes Support (Ongoing)
Phase 2 has several components;
a. Increasing the capacity of diabetes specialist nurse provision;
b. Educational review looking at upskilling GP’s and healthcare
professionals;
c. Therapeutic review looking at the way drugs, including
insulin, are prescribed for each patient;
d. Closely monitoring the provision of personalised care plans
for each patient in primary care, which links with the CQUIN
linked ThinkGlucose project in secondary care;
e. And finally agree on a consistent approach in collecting and
incorporating patient experience feedback into the project.
Case Study 4 – Integrating Community Care for Diabetes-Berkshire WestNHS Berkshire West – QIPP Pilot

32 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 33
Outcomes
QOF data from practices participating in the joint venture show
a 38% improvement in the percentage of patients reducing
their blood sugar glucose levels to target. There was also an
18% increase in the percentage of patients reducing their blood
pressure to target and a 53% improvement in the percentage of
patients achieving their cholesterol target.
Practices served by Integrated Diabetes Services have seen a
15% reduction in new hospital appointments, despite increasing
numbers of diabetics, and a 30% reduction in follow-up
appointments. In contrast, other practices have seen a 15%
increase in new appointments and a 1% increase in follow
ups. 16.4% of new referrals have been not seen directly, but
rather initial advice has been provided to the referrers. To
date, over 85% of practices have been accredited in diabetes
competencies.
There has been a high level of patient satisfaction with the new
organisations created to deliver diabetes care.
Lessons
zz Existing organisational structures of clear divisions into
primary and secondary care may not be suitable to deliver
the proposed government healthcare reforms for integration
of care for long term conditions. However, by GPs and
hospital doctors working together, we demonstrate that
how care for long term conditions is delivered can be
fundamentally restructured, leading to better outcomes at a
lower cost.
zz Shared patient records are a powerful method of speedy
communication between primary and secondary care
clinicians although significant information governance
barriers needed to be overcome. Such communication
is fundamental to saving costs, improving care and the
patient experience.
zz Clinical leadership in primary and secondary care is crucial
to the development of new systems of working. However,
we learnt that clinicians in primary and secondary care
may not fully recognize the different working pressures
experienced by the other clinicians. Time is needed to build
good relationships based on trust, which can then lead to
partnership working.
zz Education of healthcare professionals enables good
professional relationships to develop. This education can be
financially incentivized for practices.
zz Senior managers are key to system change. Often the
data to support the development of services is given a low
priority without senior management support. For instance,
difficulties in obtaining figures to calculate programme
budgeting accurately were helped by senior management
buy in.
Contact Dr Garry Tan
Overview
Without major structural changes to the commissioning and
delivery of care for long term conditions, significant financial
savings cannot be achieved. Fragmenting a patient’s care
pathway by counting and incentivising individual steps will
never be able to provide the efficient continuum of care
needed by patients with long term conditions. This initiative
has redesigned the delivery organisations for a long term
condition (diabetes) to be able to deliver a whole care
pathway for patients, including access to specialist care and
knowledge for all health care professionals and patients.
Patients with long term conditions often attend multiple
locations to see different professionals for their care because
of organizational barriers between primary, community and
secondary care. This project formed integrated multidisciplinary
teams (irrespective of traditional primary or secondary care
barriers) to ensure the patient receives a comprehensive and
consistent service.
Communication between organisations is not optimized, services
are duplicated or are missing, and this fragmentation results in
vulnerable people feeling confused and stranded between care
providers. Current care pathways are generally inefficient which
leads to poor health outcomes. As part of this project, we have
achieved a real-time, unified patient record for our patients (in
both primary and secondary care), based on the patients existing
primary care record.
Objectives
We have removed organizational boundaries and transformed
the structure and delivery of diabetes care to improve clinical
delivery and outcomes. The changes have reduced overall
costs. We have achieved this by forming two new not-for-profit
organisations, each jointly and equally owned by local GPs and
a local NHS Foundation Trust (Derby Hospitals NHS Foundation
Trust) to overcome the financial and governance barriers to
integrated diabetes care. We compared professional and
patient outcomes before and after the implementation of these
partnerships.
Strategy
Consultant clinicians and local GPs drew up a clinical pathway
and defined a diabetes model across primary and secondary
care to deliver this pathway. It included clinical governance,
integrated IT, clinical delivery in GP practices and community
settings, and financial incentives for GP care and healthcare
professional education.
We examined how such “integration” was done elsewhere.
However, it was clear that other models would not remove
traditional “perverse incentives” because the barriers between
primary and secondary care providers would remain. We
therefore developed a novel model to support the clinical
pathway which was predicated on the formation of a new
organization which would deliver diabetes care across
organizational boundaries.
We presented this model to senior management in the PBC
and acute hospital trust to gain support to establish a single
organization to deliver the care pathway. We then bid for, and
won, the contract from the PCT to deliver integrated diabetes
services for the local population in Derby City.
Case Study 5 – New Organisations for New Challenges in Long Term ConditionsDerby Primary Care Trust
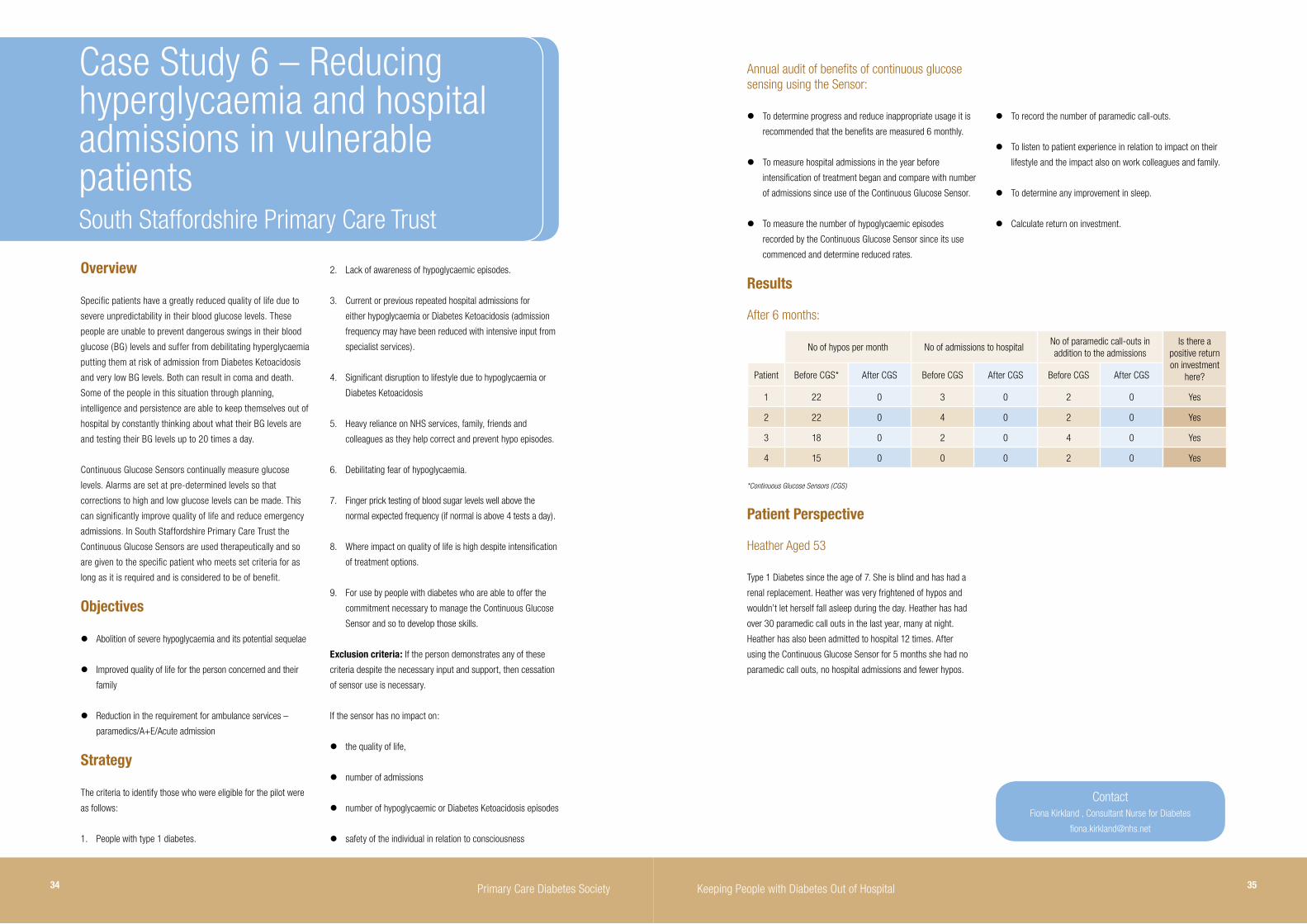
34 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 35
Overview
Specific patients have a greatly reduced quality of life due to
severe unpredictability in their blood glucose levels. These
people are unable to prevent dangerous swings in their blood
glucose (BG) levels and suffer from debilitating hyperglycaemia
putting them at risk of admission from Diabetes Ketoacidosis
and very low BG levels. Both can result in coma and death.
Some of the people in this situation through planning,
intelligence and persistence are able to keep themselves out of
hospital by constantly thinking about what their BG levels are
and testing their BG levels up to 20 times a day.
Continuous Glucose Sensors continually measure glucose
levels. Alarms are set at pre-determined levels so that
corrections to high and low glucose levels can be made. This
can significantly improve quality of life and reduce emergency
admissions. In South Staffordshire Primary Care Trust the
Continuous Glucose Sensors are used therapeutically and so
are given to the specific patient who meets set criteria for as
long as it is required and is considered to be of benefit.
Objectives
zz Abolition of severe hypoglycaemia and its potential sequelae
zz Improved quality of life for the person concerned and their
family
zz Reduction in the requirement for ambulance services –
paramedics/A+E/Acute admission
Strategy
The criteria to identify those who were eligible for the pilot were
as follows:
1. People with type 1 diabetes.
Case Study 6 – Reducing hyperglycaemia and hospital admissions in vulnerable patientsSouth Staffordshire Primary Care Trust
2. Lack of awareness of hypoglycaemic episodes.
3. Current or previous repeated hospital admissions for
either hypoglycaemia or Diabetes Ketoacidosis (admission
frequency may have been reduced with intensive input from
specialist services).
4. Significant disruption to lifestyle due to hypoglycaemia or
Diabetes Ketoacidosis
5. Heavy reliance on NHS services, family, friends and
colleagues as they help correct and prevent hypo episodes.
6. Debilitating fear of hypoglycaemia.
7. Finger prick testing of blood sugar levels well above the
normal expected frequency (if normal is above 4 tests a day).
8. Where impact on quality of life is high despite intensification
of treatment options.
9. For use by people with diabetes who are able to offer the
commitment necessary to manage the Continuous Glucose
Sensor and so to develop those skills.
Exclusion criteria: If the person demonstrates any of these
criteria despite the necessary input and support, then cessation
of sensor use is necessary.
If the sensor has no impact on:
z the quality of life,
z number of admissions
z number of hypoglycaemic or Diabetes Ketoacidosis episodes
z safety of the individual in relation to consciousness
Results
After 6 months:
No of hypos per month No of admissions to hospitalNo of paramedic call-outs in addition to the admissions
Is there a positive return on investment
here?Patient Before CGS* After CGS Before CGS After CGS Before CGS After CGS
1 22 0 3 0 2 0 Yes
2 22 0 4 0 2 0 Yes
3 18 0 2 0 4 0 Yes
4 15 0 0 0 2 0 Yes
*Continuous Glucose Sensors (CGS)
Patient Perspective
Heather Aged 53
Type 1 Diabetes since the age of 7. She is blind and has had a
renal replacement. Heather was very frightened of hypos and
wouldn’t let herself fall asleep during the day. Heather has had
over 30 paramedic call outs in the last year, many at night.
Heather has also been admitted to hospital 12 times. After
using the Continuous Glucose Sensor for 5 months she had no
paramedic call outs, no hospital admissions and fewer hypos.
Contact Fiona Kirkland , Consultant Nurse for Diabetes
Annual audit of benefits of continuous glucose sensing using the Sensor:
z To determine progress and reduce inappropriate usage it is
recommended that the benefits are measured 6 monthly.
z To measure hospital admissions in the year before
intensification of treatment began and compare with number
of admissions since use of the Continuous Glucose Sensor.
z To measure the number of hypoglycaemic episodes
recorded by the Continuous Glucose Sensor since its use
commenced and determine reduced rates.
z To record the number of paramedic call-outs.
z To listen to patient experience in relation to impact on their
lifestyle and the impact also on work colleagues and family.
z To determine any improvement in sleep.
z Calculate return on investment.

36 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 37
Overview
Jaywick is ranked as the 3rd most deprived town in England and
Wales whilst the adjacent coastal neighbourhood of Pier Ward is
the 775th (Indices of Deprivation 2007). According to the North
East Essex Local Delivery Plan (2007) Jaywick area has a higher
than average incidence of cardio-vascular disease and low level
of skills and educational attainment. A high number of people of
working age are receiving unemployment benefits. There are a
high number of people on low incomes, a significant number of
unemployed people of working age and widespread indications of
poor physical and mental health.
During 2009, North East Essex had a slightly higher than national
incidence of diabetes at 3.9%. However, one of practices in
Jaywick had a 7.41% prevalence (2009), more than twice the
national average. Furthermore, the local diabetes service reported
poor clinic attendance for their patients from the Jaywick and Pier
Ward.
Objectives
This new initiative aimed to give extra support to people with
diabetes closer to their homes. The project, addressing the
health inequalities in Jaywick and Pier Wards, was set to run
for 18 months and its key performance indicators included the
management of blood pressure, lipids and diabetes. The initiative
involved joint working with primary and secondary care, Public
Health and local authorities. Data was collected and audited, with
a quarterly assessment of key performance indicators.
Strategy
Four practices were contacted within the designated areas and
meetings set up with either the GP or Practice Nurse. These
meetings identified the first 24 patients as meeting a criteria of
HbA1c >over 10% and those who were excluded from QOF due
to non-attendance.
A letter of introduction was sent to the identified patients asking
if they would like an appointment. The letter also indicated that
further contact would be made. Following the initial letter, 10
patients responded and contact was made. At this time, patients
already under the care of the Primary Care Diabetes Service
but who had a poor attendance record were transferred to the
outreach caseload for closer supervision.
A meeting was held with staff from the Emergency Assessment
Unit at the local Acute Hospital to decide the most effective way
to capture patients who had been admitted into hospital from the
project area and to form a weekly contact. The aim was for the
DSN to be informed of identified admissions and discharges from
the specific postcodes.
Patients were also screened using the interrogation of the
PARR++ tool to identify those who have had frequent admissions
to hospital for diabetes. Cross-functional working with other
community agencies enabled the sharing of ideas and experience
of the best ways to engage with the hard-to-reach patients.
Clinics within a local Pharmacy were successful and delivered on
a weekly basis. This enabled patients to be seen closer to home
which has reduced the DNA rate for clinical appointments. Home
visits are also arranged including care homes, non-attendees and
patients who are too unwell to travel.
It was identified that the clinical management of these patients
required a high level of skill and experience. Many of the patients
are young with type 1 diabetes and had complex needs which
would not normally be managed within primary care (GP) or who
have opted out of the secondary care service. Other patients
were those with complex needs and co-morbidities such as renal
disease, mental health problems, COPD and morbid obesity.
Case Study 7 – Diabetes Inequalities Outreach ProjectClacton-on-Sea
Results
The project has had a significant impact on the local population
in terms of improved clinical outcomes and reaching people with
diabetes who previously did not use the services, thus in turn
improving the lifestyle and motivation of people to self-manage
their long term condition and reengaging with health services.
In six months, the project has resulted in:
zz Caseload 49 patients (12 months)
zz Hospital admissions reduction of 33
zz 4 admission avoidances
zz Improvements in 25 patients HbA1c (Diabetes indicator) with
an average drop of 2.2%
zz Improvements in 10 patients’ lipids results
zz 48 non-medication prescriptions initiated
zz 25 referrals to lifestyle interventions
zz 100% of patients feeling more confident in managing their
diabetes
Recommendations
The key to success was the flexibility of appointment times,
locations and home visits as well as the use of alternative
consulting rooms in pharmacies within the local area at times
convenient for the patient. Ideally appointments were made
on the same day of contact. The contact was made by an
experienced Diabetes Specialist Nurse (DSN) who was able to
work autonomously and make instant changes to medication. The
DSN had instant access to GPs, Practices Nurses and Consultants
for information and support. The patients responded well to the
continuity of care, the DSN gained the trust of individuals who
have come back in to the health care system and enabled them
to feel more confident in managing their diabetes.
Patients reported that one of the most important issues for
them was the continuity of care and that the nurse could make
decisions at the time of the appointment. The pilot project has
shown that intervention health outcomes can be positively
affected. Initially the numbers were small, with a caseload of 49
patients.
The project has now been extended across North East Essex
focusing on patients from deprived post codes who have a high
admission record due to diabetes.
Contact Sheila Smyth, Diabetes Service Manger
38 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 39
Overview
It is now well known that people with severe and enduring mental
health problems have a greater risk, than the general population,
of long-term physical health problems, including diabetes, which
can lead to increased hospitalisation and early mortality.
The need to address this problem was recognised by Birmingham
and Solihull Mental Health Foundation Trust, so not only did it
design and implement a physical health strategy, but it also
created a role to dynamically review diabetes outcomes and
related physical health problems this condition can cause. The
diabetes lead was employed within the mental health trust to
support this vulnerable group of patients in our inpatient units,
ensuring that this condition was recognised as a health and
wellbeing need, and to help support discharge.
The improved communication and enhanced ability to support
these people with their physical health led to a speedier recovery
and the prevention of long-term complications; ultimately
reducing the need for acute diabetes/cardiovascular/kidney
admissions.
Objectives
The key priority for this role was to deliver expert advice and
consultation, to include medication management and where
appropriate to prescribe to any inpatient units and home
treatment environments. This was supported by specialist advice
in the overall management of diabetes. Although there was the
ability to prescribe in the community, this was less frequently
done. Instead, close liaison with the GP or community service
were considered a better option to reduce the risk of too many
practitioners providing the same care. This role was created to
enhance support for the service user, not to replace any existing
services.
The diabetes nurse provided assurance that the staff working
with the service users were able to assess care needs, able
to develop, implement and evaluate programmes of care and
provide educational programmes for patients, families/carers and
other health professionals where needed.
The nurse operated in a self-directed mode in developing
guidance, policy and organisational needs appertaining to
diabetes care management.
Guidance included to date:
;z Development of clear referral guidelines for the most
appropriate diabetes care.
;z Development of clinical guidelines on the treatment of hypo
and hyperglycaemia supporting staff in the management
of these issues; therefore preventing unnecessary acute
hospital visits.
;z Distribution of the ‘Safe Use of Insulin’ educational pack (not
presently promoted in mental health trusts) and reducing the
risk of insulin errors.
;z Promotion of the importance of a good physical health
assessment, identifying vital risk factors.
The strategy was also to establish a diabetes network across
secondary, primary and social care, identifying a range of
opportunities around community diabetes services. Providing the
initial baseline assessments of diabetes care in Birmingham and
Solihull mental health foundation trust would allow quicker access
to these services.
Case Study 8 – Preventing Admission of Vulnerable People with Mental Health Problems Birmingham and Solihull Mental Health Foundation Trust
Strategy
The implementation of an expert practitioner supported the
delivery of care with access to improved community services for
people with severe mental health problems.
Having the knowledge of local diabetes, cardiac and lipid services
ensured prompt referral to appropriate services reducing the need
for reactive hospitalisation in emergency situations.
Additionally the local acute inpatient diabetes team had an
awareness of the additional support available to the service user
and had the ability to refer to us patients for acute follow up once
they were discharged; especially those discharged to one of our
inpatient mental health units.
The baseline of staff knowledge and understanding supported
an educational package to be produced for mental health
practitioners. The package varies for the individual teams’
needs ranging from supporting the Consultant Psychiatrists and
pharmacists to the registered mental health nurses and health
care assistances.
The training supported improved understanding of what care
and treatment to provide in individual situations and prevent the
service user from deteriorating in their physical health, ultimately
avoiding the need for paramedics and acute hospital admission.
The service has also included information updates on the intranet,
regular reporting on important news articles and ad hoc diabetes-
related promotion, all supporting the development of an improved
diabetes service for the service user and carer.
Results
Although only preliminary audits against NICE standard have
been commenced, the subjective evidence is starting to become
apparent.
The staff have greater confidence in the management of diabetes
and emergency admissions to A&E for glycaemia control have
been reduced. Wards are far better equipped with treatment
options and the understanding of treatments which cause
hypoglycaemia or hyperglycaemia and have improved care
planning in place for these issues.
The communication between the acute hospitals in the area and
the mental health trust is progressing with acute trusts being
more confident in the care they will receive if discharged back to
our units, supporting an earlier discharge from the acute hospital
beds.
Mental health practitioners have also highlighted that since
diabetes has been more intensely managed, the ability to improve
the acute mental health conditions has also improved over and
above the norm for each individual patient.
Contact Lyndi Wiltshire, Head of Diabetes Care

Keeping People with Diabetes Out of Hospital 4140 Primary Care Diabetes Society
Association of Chartered and Certified Accountants (ACCA) &
the Audit Commission, Costing Care Pathways; Understanding
the cost of the diabetes care pathway, (2011), http://
www.audit-commission.gov.uk/health/nationalstudies/
financialmanagement/Pages/costingcarepathways.aspx
BBC Radio 4, Today Programme, (2011), http://news.bbc.co.uk/
today/hi/today/newsid_9525000/9525601.stm
Department of Health, Turning the Corner: Improving Diabetes
Care; a Report from Dr Sue Roberts National Clinical Director
for Diabetes to the Secretary of State for Health, (2006), http://
www.dh.gov.uk/en/Publicationsandstatistics/Publications/
PublicationsPolicyAndGuidance/DH_4136141
Diabetes UK, Diabetes in Care Homes – Awareness, screening,
training, (2010), http://www.diabetes.org.uk/Get_involved/
Raising-awareness/World-Diabetes-Day/2010-activities/
Diabetes-in-care-homes---Awareness-screening-training/
Diabetes UK, Diabetes in the UK 2010: Key Statistics on diabetes,
(2010), http://www.diabetes.org.uk/Professionals/Publications-
reports-and-resources/Reports-statistics-and-case-studies/
Reports/Diabetes-in-the-UK-2010/
Farmer, A.J. & Brockbank K.J. et al, Incidence and costs of
severe hypoglycaemia in diabetes requiring attendance by the
emergency service in the United Kingdom, (2011)
Healthcare Commission, The Views of People with Diabetes,
Key Findings from 2006 Survey, (2006), http://www.cqc.org.
uk/_db/_documents/Diabetes_survey_2006_summary.pdf
Institute of Diabetes for Older People (IDOP), Keeping Older
People with Diabetes out of Hospital – improving outcomes,
saving money and maintaining quality of life and dignity, (2011),
http://instituteofdiabetes.org/
The King’s Fund, Type 2 Diabetes – Accounting for a major
resource demand in society in the UK, (2000), http://www.ncbi.
nlm.nih.gov/pmc/articles/PMC1117754/
Map of Medicine, Productivity Considerations for Service Design:
Diabetes, (2011), http://www.mapofmedicine.com/global/pdf/
productivity_considerations_Diabetes.pdf
National Diabetes Support Team, Improving emergency and
inpatient care for people with diabetes, (2008)
NHS Information Service, National Diabetes Audit Executive
Summary 2009-2010, (2011), http://www.ic.nhs.uk/nda
NHS Information Centre for Health and Social Care, Prescribing
for Diabetes in England: 2004/5 to 2009/10, (2010), http://
www.ic.nhs.uk/pubs/prescribingdiabetes0410
NICE, Diabetes care improves, but patients still missing out on
key tests, (2010) http://www.nice.org.uk/newsroom/news/
DiabetesCareImprovesButPatientsStillMissingOutOnKeyTests.jsp
NICE, Review of Clinical Guideline (CG15) – Type 1 Diabetes:
diagnosis and management of type 1 diabetes in children, young
people and adult, (2011), http://www.nice.org.uk/nicemedia/
live/10944/56133/56133.pdf
NICE, Guidance on the use of patient-education models for
diabetes, (2003), http://www.nice.org.uk/nicemedia/pdf/60Pati
enteducationmodelsfullguidance.pdf
Sampson, M.J. & Crowle T. et al, Trends in bed occupancy for
inpatients with diabetes before and after the introduction of a
diabetes inpatient specialist nurse service, Diabetes Medicine,
(2006), http://www.drketandhatariya.com/publications/original_
articles/diabetic_medicine_2006.pdf
Yorkshire and Humber Public Health Observatory (YHPO),
Diabetes Key Facts, (2006), http://www.yhpho.org.uk/resource/
item.aspx?RID=8872
Yorkshire and Humber Public Health Observatory (YHPO),
Diabetes Key Facts; Supplement, (2007), www.yhpho.org.uk/
resource/view.aspx?RID=9743
References

42 Primary Care Diabetes Society Keeping People with Diabetes Out of Hospital 43

Supported by:
PCDSPrimary Care Diabetes Society