journal of nurse life care planning - c.ymcdn.com · aanlcp journal of nurse life care planning...
TRANSCRIPT
JOURNAL OF
NURSE LIFE CARE PLANNINGFall 2017 vol XVII, no.3
T H E A M E R I C A N A S S O C I A T I O N O F N U R S E L I F E C A R E P L A N N E R S
P E E R - R E V I E W E D E X C E L L E N C E I N L I F E C A R E P L A N N I N G S I N C E 2 0 0 6
Back and Spine
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
JOURNAL OF NURSE LIFE CARE PLANNINGFALL 2017
TABLE OF CONTENTS
DEPARTMENTS
15 Chronic Low Back Pain: Impact on the Life Care Plan Emma W. White, PT, DPT, OCS
22 Alternative Treatments for Individuals with a Spinal Cord Injury Erin T. OConnell, MSN, MBA, RN-BC, CNL, CNLCP®
28 Platelet-Rich-Plasma: Life Care Planning Considerations Dawn Cook, RN, LNCP-C, CLCP, CLNC
3 From the Editor
4 Information for Authors
6 A Message from the President
8 Contributors to this Issue
9 Upcoming Issues
10 Aging and Back and Spine Issues Resource List
12 Dear Carole
34 Issue Index
®®
American Association of NurseLife Care Planners 125 Warrendale Bayne Rd. #375Warrendale, PA 15086PH: 801.274.1184FX: 724.935.1560Website: www.aanlcp.org/
BOARD OF DIRECTORS
PresidentDenise W. Wrenn, MSHA, BSN, RN, CCM, COHN-S, CWCP, CMSP, CLCP, ALNC
President-ElectLori Moore Dickson, MSN, RN, MSCC, CLCP, CNLCP®
Past PresidentPatricia Rapson, RN CCM, CNLCP®, CLCP, LNCC, CBIS, MSCC
SecretaryBeth Wood, RN MMA, MIS, CCM, CNLCP®
TreasurerCynthia Towne, BSN, RN-BC, CCM, CNLCP®
JOURNAL OF NURSE LIFE CARE PLANNING
Editor Mariann F. Cosby, DNP, MPA, RN, PHN, CEN, NE-BC, LNCC, CCM, MSCC
Journal Committee Chair
Kelly K. Campbell, RN, BSN, CP, CLNC, CLCP
Journal Committee for This Issue:
Barbara Bate, RN-BC, CCM, CRRN, CNLCP®, LNCC, MSCC
Kelly K. Campbell, RN, BSN, CP, CLCN, CLCP
Jenn Craigmyle, RN, BSN, CLNC, LNCP-C, CLCP
Chris Ann Daniel, RN, BSHS, CCM, CNLCP®, MSCC, LNC, CBIS
Wendie Howland, MN, RN-BC, CRRN, CCM, CNLCP®, LNCC
Linda Husted, MPH, RN, CNLCP®, LNCC, CCM, CDMS, CRC
Shelly Kinney, MSN, RN, CCM, CNLCP®
LaToya Lowery, RN, BSN, MBA, CCM, CNLCP®
Kathy Pouch, MSN, RN-BC, CCM, CNLCP®, LNCC
Carole Upman, RN, MA, CCM, CRC, CDMS/R, CNLCP®
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 3
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Welcome to the Fall 2017 issue! As Denise Wrenn so
eloquently conveys in her President’s message, this month
brought challenges to many of our colleagues who were
impacted by the recent hurricanes. It is with heartfelt
care, concern, and hope that their innate resiliency and
resourcefulness as nurses, fosters their speedy return to
normalcy in their personal and professional life.
This issue includes three articles regarding different aspects of the back and spine
for life care planning consideration. Dr. Emma White dispels three common myths
about chronic lower back pain and provides information on the “red and yellow
flags” that the life care planner should consider. Erin OConnell discusses the current
and potential alternative therapies for persons with spinal cord injuries including cell
transplantation, functional electrical stimulation, and lower extremity exoskeleton.
Dawn Cook provides an overview, case study, and costing tips regarding the use
of platelet-rich plasma. Natasha Davis provides tips for success in overcoming six
business challenges as the guest writer of the Dear Carole column.
As with the seasonal change, the Journal Committee is experiencing change with
the resignations of the two Co-Chairs: Jenn Craigmyle and Kelly Campbell. Although
they plan to continue to be committee members; their leadership, dedication, and
drive to keep the ideas flowing and articles coming for the last year will be missed.
As the Editor, I wish them much success in their future endeavors! Please check out
the upcoming issue themes and consider submitting a short piece on your costing
methods or case studies for next year!
As always, the Journal Committee welcomes your feedback and input. Please send
your comments to the Editor.
Fro
m t
he E
dit
or
Mariann F. Cosby, DNP, MPA, RN, PHN, CEN, NE-BC, LNCC, CLCP, CCM, MSCC
Editor, [email protected]
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 4
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
AANLCP® invites interested nurses and allied professionals to submit article queries or manuscripts that educate and inform the Nurse Life Care Planner about current clinical practice methods, professional development, and the promotion of Nurse Life Care Planning within the medical-legal community. Submitted material must be original. Manuscripts and queries may be addressed to the Editorial Committee. Authors should use the following guidelines for articles to be considered for publication. Please note capitalization of Nurse Life Care Plan, Planning, etc.
Text Manuscript length: 1500 – 3000 words ◾ Use Word© format (.doc, .docx) or Pages (.pages) ◾ Submit only original manuscript not under consideration by other publications ◾ Put the title and page number in a header on each page (using the Header feature in Word) ◾ Use Times New Roman 12 point font ◾ Place author name, contact information, and article title on a separate title page, so author name can be blinded for editorial review ◾ Use APA style (Publication Manual of the American Psychological Association 6th Ed)
Art, Figures, Links All photos, figures, and artwork should be in JPG or PDF format (JPG preferred for photos). Line art should have a minimum resolution of 1000 dpi, halftone art (photos) a minimum of 300 dpi, and combination art (line/tone) a minimum of 500 dpi. Each table, figure, photo, or art should be on a separate page, labeled to match its reference in text, with credits if needed (e.g., Table 1, Common nursing diagnoses in SCI; Figure 3, Time to endpoints by intervention, American Cancer Society, 2003) Live links are encouraged. Please include the full URL for each.
Editing and Permissions The author must accompany the submission with written release from: ◾ Any recognizable identified facility for the use of name or image ◾ Any recognizable person in a photograph, for unrestricted use of the image ◾ Any copyright holder, for copyrighted materials including illustrations, photographs, tables, etc.
All authors must disclose any relationship with facilities, institutions, organizations, or companies mentioned in their work. All accepted manuscripts
are subject to editing, which may involve only minor changes of grammar, punctuation, paragraphing, etc. However, some editing may involve condensing or restructuring the narrative. Authors will be notified of extensive editing. Authors will approve the final revision for submission. The author, not the Journal, is responsible for the views and conclusions of a published manuscript. Submit your article as an email attachment, with document title articlename.doc, e.g., wheelchairs.doc
All manuscripts published become the property of the Journal. Manuscripts not published will be returned to the author. Queries may be addressed to the care of the Editor at: [email protected]
Manuscript Review Process Submitted articles are peer reviewed by Nurse Life Care Planners with diverse backgrounds in life care planning, case management, rehabilitation, and the nursing profession. Acceptance is based on manuscript content, originality, suitability for the intended audience, relevance to Nurse Life Care Planning, and quality of the submitted material. If you would like to review articles for this journal, please contact the Editor.
Information for Authors
Journal of Nurse Life Care Planning is the official peer-reviewed publication of the American Association of Nurse Life Care Planners. Articles, statements, and opinions contained herein are those of the author(s) and are not necessarily the official policy of the AANLCP® or the editors, unless expressly stated as such. The Association reserves the right to accept, reject, or alter manuscripts or advertising material submitted for publication. The Journal of Nurse Life Care Planning is published quarterly in spring, summer, fall and winter. Members of AANLCP® receive the Journal subscription electronically as a membership benefit. Back issues are available in electronic (PDF) format on the association website. Journal contents are also indexed at the Cumulative Index of Nursing and Allied Health Literature (CINAHL) at ebscohost.com. Please forward all email address changes to AANLCP® marked “Journal-Notice of Address Update.” Contents and format copyright by the American Association of Nurse Life Care Planners. All rights reserved. For permission to reprint articles, graphics, or charts from this journal, please request to AANLCP® headed “Journal-Reprint Permissions” citing the volume number, article title, author and intended reprinting purpose. Neither the Journal nor the Association guarantees, warrants, or endorses any product or service advertised in this publication nor do they guarantee any claims made by any product or service representative. In order to make safe and effective judgments using NANDA-I nursing diagnoses it is essential that nurses refer to the definitions and defining characteristics of the diagnoses listed in this work.
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 5A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 5

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 6
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
I was a resident of Louisiana in 2005 when Hurricane Katrina decimated New Orleans. I was fortunate in that my home, located about three hours away, was undamaged. But I didn't think twice about leaving the safety of my community to travel with co-workers into the heart of the devastation to provide help. Once there, I worked many hours triaging front-line workers who were striving to re-build the city's destroyed infrastructure.
Why did I go? Because I am a nurse, and I was needed, and this is what we do. We don't think - we act. When others are in need, our passion drives us to respond. And
this September, we have seen great need. Many of our members are now facing the challenge of rebuilding their lives both at home and at work in the aftermath of hurricanes Harvey and Irma. Many other first responders - many of them healthcare workers - have put their lives on hold to serve those who have lost so much. As nurses who are Life Care Planners, events like these remind us that our work is important, and that life's trajectory can change in an instant.
AANLCP is here to provide a community of education, collaboration and support to our members, who may be called to duty in response to crisis, or who may be called to the witness stand to defend a patient's life care plan. AANLCP also strongly supports the work of nurses like Alex Wubbels, who was recently arrested at The University of Utah Hospital by a Salt Lake City detective
for refusing to let police draw blood from an unconscious ER patient.
As advocates for patient rights, our work is grounded in the mission that every person deserves to live to their highest quality of life. It is an inspiration to me how often nurses put their own professional and personal lives on the line to uphold the rights of others.
In this month that has often known tragedy, from natural disasters to the acts of terrorism experienced on September 11, 2001, I believe we must be mindful, thoughtful and prayerful in our power as nurses to give others hope for the future.
Denise W. Wrenn, MSHA, BSN, RN, CCM, COHN-S, CWCP, CMSP, CLCP, ALNCPresident, AANLCP [email protected]
A Message from the President

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 7
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 3 5
S P R I N G 2017 P E E R - R E V I E W E D E XC E L L E N C E I N L I F E C A R E P L A N N I N G S I N C E 20 0 6 V O L . X V I I N O. 1
Evidenced-based practice begins with research.If you write life care plans you already do research.No fear! Lighten the load! Strengthen the practice!
Come join us as we find the evidence to support our practice!
Participate: email [email protected]
Phone 732-261-1761
Together we can learn the scoopshare knowledgebuild a body of evidence by life care plannersfor nurse life care planners
Show Them The Evidence
… curious about how and why the nursing process supports our specialty
practice of Nurse Life Care Planning? Are you in a formal education/practice program and need ideas for a research project and paper? Let’s talk!
Your Research Committee is currently studying how and why Nurse Life
Care Planners put case management services into life care plans. We need help doing literature reviews and identifying tools to determine variables in using case management services.
Are you…
… already working on research in a formal advanced education/practice
program? Did you know that AANLCP would love to know about your research project?! Tell us about it!
~ Colleen Manzetti, DNP, RN, CNLCP, CNEChair, AANLCP Research Committee

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 8
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Contributors to this Issue
EMMA W. WHITE PT, DPT, OCS
Dr. Emma White is a Clinical Assistant Professor, Department of Physical
Therapy, Winston Salem State University. Dr. White received her PT degree from the Medical College of Virginia in 1978.
Dr. White brings 30 years of clinical experience with 16 of those years
owning an orthopedic private practice in Thomasville, NC (1991-2007) working
extensively in the management of patients presenting with musculoskeletal
spine and extremity conditions, both surgical and non-surgical. Dr. White
received her clinical doctorate in physical therapy from the University of North
Carolina at Chapel Hill in 2008, and her ABPTS certification in Orthopedics in 2014. Dr. White joined the WSSU DPT faculty in 2011. Dr. White is very active and a passionate member of the North Carolina Physical Therapy Association
serving as the Director at Large for Reimbursement. Dr. White’s research interest: conservative management of LBP, quantifying forward head postural
dysfunction and exploring its relationship to fall risk in older adults, and injury
prevention in athletes and sports enhancement.
DAWN COOK RN, LNCP-C, CLCP, CLNC
Dawn Cook has been a life care planner since 2012 and has completed
over 250 expert reports, and has qualified to testify in Nevada,
California, New Mexico and at Federal Court. Dawn has been a
Registered Nurse since 1979 when she graduated as the Valedictorian of her Nursing class in Victoria, British Columbia. She has worked in Home Care and Acute Hospital facilities for over 30 years. Dawn is certified as a
Lifetime Nurse Care Planner, Certified Nurse Life Care Planner and Certified
Life Care Planner.
Dawn developed a special interest in platelet rich plasma (PRP) therapy because she has seen the benefits for pain reduction and healing for injured knees when she worked at a hospital at a California ski resort
and as a life care planner with patients receiving PRP for pain. Dawn has been a speaker at the
American Association of Legal Nurse Consultants, the Executive Forum of Nurse Life Care Planners, the Society
of Pain Management Nursing, the American Association of Nurse Life
Care Planners, the International Symposium of Life Care Planners and the International Transplant
Nurse Society.
ERIN T. OCONNELL, MSN, MBA, RN-BC, CNL, CNLCP®
Erin OConnell has had over a decade of clinical nursing experience in a multitude
of nursing areas including the ICU, telemetry, emergency, long-term care,
rehabilitation, and same day/PACU. Her career has afforded her a diverse set of experiences. It has also deepened her appreciation for the field as a whole.
She currently works as the Clinical Nurse Leader in the long-term care setting. She
is compelled to continuously learn and stay involved. She currently serves on the
AANLCP’s research committee, whose goal is to enrich resources for Nurse
Life Care Planners. She is also Webinar Committee Chair of the AALNC West
Virginia Upper Ohio Valley Chapter. In her free time, she enjoys hiking, backpacking,
biking, kayaking, downhill skiing and cross country skiing. She recently moved
to Seattle and is loving every minute.

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 9
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
UPCOMING ISSUES
Winter 2017Mobility, Extremity Function
Spring 2018Costing Methods
Summer 2018Case studies
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 0
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Aging and Back and Spine Issues Resource List Compiled by: Kelly K. Campbell, RN, BSN, CP, CLNC, CLCPJenn Craigmyle, RN, BSN, CLNC, LNCP-C, CLCP
1. Back and neck pain in seniors—prevalence and impacthttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC3489453/
2. The impact of chronic low back pain on older adultshttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC2065872/
3. Healing Hands: Massage May Ease Chronic Back Pain: People over 50 tended to respond best, study findshttps://medlineplus.gov/news/fullstory_164647.html
4. Chiropractic Associated with Protective Effect in Spinal Health of Medicare Beneficiarieshttps://nccih.nih.gov/research/results/spotlight/091614
5. Tai Chi and Your Health: A Modern Take on an Ancient Practice https://newsinhealth.nih.gov/issue/dec2016/feature2
6. Spinal stenosis: Recent clinical studies. Etiology. Diagnosis. Therapy. Prognosis. Clinical Prediction Guides. Recent Systematic Reviews.https://www.ncbi.nlm.nih.gov/medgen/20907
7. Clinician’s Guide to Prevention and Treatment of Osteoporosishttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC4176573/
8. Degenerative changes in the spine: Is this arthritis?http://www.mayoclinic.org/diseases-conditions/osteoarthritis/expert-answers/arthritis/faq-20058457
9. Arthritis Prevalence Rising as Baby Boomers Grow Older: Osteoarthritis Second Only to Chronic Heart Disease in Worksite Disabilityhttps://www.niams.nih.gov/News_and_Events/Press_Releases/1998/05_05.asp
10. Neck pain in the elderly: a management review. Part I. : Degenerative disease of the spine.https://www.ncbi.nlm.nih.gov/pubmed/3803929
JENN CRAIGMYLE, RN, BSN, CLNC, LNCP-C, CLCPJenn Craigmyle is a bachelor’s prepared Registered Nurse with experience as a clinical nurse in neurology and critical care, nursing educator for an ADN school of nursing, legal nurse consultant, life care planner, and care manager. She earned her certification in life care planning in 2012 and is the one owner of Craigmyle Legal Nurse Services, LLC based out of Southern California.
KELLY K. CAMPBELL, RN, BSN, CP, CLNC, CLCPKelly K. Campbell earned her Bachelor of Science degree in Nursing from Penn State University in 1996 and a certificate of Perfusion from Texas Heart Institute in 1998. In 2013 she earned her Legal Nurse Consultant certification and 2014 she completed her Life Care Plan education from Capital University Law School. In addition to Chair Journal of Nurse Life Care Planning, she is an author for revision of AALNC Principles and Practice 4th Edition. Her specialty interests include Medical Device, Brain Injury, Amputation, Chronic Pain and Cardiac.
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 1
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
This online program will prepare you to work in a variety of areasincluding child/elder abuse, domestic violence intervention, lifecare planning, sexual assault examination, case management,mass disaster response, and death investigation.
Forensic Nursing MSN
monmouth.edu/GRNU_info
WEST LONG BRANCH, NJ732-571-3452
39-credit 100% online program
Allows specialization such as Care Managementor Interpersonal Violence
Individualized mentoring for Practicum & Seminarexperiences
IAFN SANE Clinical Skills Lab Site
Inquiretoday!
Applications accepted year-round!
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 2
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Overcoming the Six Main Challenges of Starting and Growing a BusinessNatasha E. Davis, MBA-M, RN-BSN
Starting a business and growing a business both come with their own challenges. Entrepreneurship brings the entrepreneur personal and professional development. The arena of business will grow the owner to levels beyond their wildest dream. Here are six of the greatest challenges every business must overcome in order to reach heightened places of success. 1) Leadership Skills... Developing strong leadership skills will give the business a strong competitive edge. These skills not only provide the business an opportunity to position themselves for years of success, it will also position them as industry experts. When you discipline yourself to learn to be a phenomenal leader you offer your company another valuable competitive edge. You actually move from being an entrepreneur into being a real CEO. 2) Sales... Developing a Sales strategy is one of the most important areas that businesses must excel in. Getting products and services in the hands of customers by way of monetary exchange is a focus that should never been forgotten. Learn and Develop a strong sales model for your company that you can teach your team...speaking of teams!........
3) Staffing... Building a reliable team of people to help move your company forward is critical to your growth factor. There is no business that grows without a supportive team. The CEO can not do it alone! Make it a point to hire your weakness and capitalize on your strengths.

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 3
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
4) Research & Development (Change Management) ...This is an area that many small businesses have problems with. The value of R & D takes back seat in the small business community. The smaller the business, the less value is placed on R &D. This may be because the perceptions of R & D are frightening and often times incorrect. Extreme value comes from R & D for every size business. R & D can be as simple as doing an online survey asking your customers what they like and don’t like about your products/service. 5) Training ...Unfortunately, new Entrepreneurs are more concerned with networking every where instead of networking with a plan and trying to figure out this thing called being a CEO. Ongoing education and training has proven to be one of the greatest advancing tools successful businesses have used. The more you learn is the better you’ll earn...Never stop learning. Never stop teaching your team. Never stop teaching your customers. 6) Not Asking For Help!!!! Man cannot live by bread alone and Businesses cannot survive by CEO alone...Asking for help can feel like the most uncomfortable thing to do because it exposes all your vulnerable sides. However asking for help early, will prevent years of long suffering. Ask and you just might receive. Take these tips and apply them to your Business today. Manage and overcome the six main challenges of starting and growing your business.. It’s time to enjoy the experience of #OwningMyEdge.
If you have any questions or want guidance in overcoming business growth challenges, you are invited to contact Natasha at Impact Branding via 678-390-2681 or via [email protected].
DISCLAIMER: The content of this column is intended as a brief introduction to general business concepts and has no legal or accounting expertise implied or suggested. The members of the journal committee and the invited contributors recommend the readers seek their own legal counsel and financial advice for guidance on their business requirements.
Please keep the questions coming to: [email protected]

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 4
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 4 8
S P R I N G 2017 P E E R - R E V I E W E D E XC E L L E N C E I N L I F E C A R E P L A N N I N G S I N C E 20 0 6 V O L . X V I I N O. 1
Coming!Summer 2018
Core Curriculum for Nurse Life Care Planning
2nd edition
To contribute, contactAANLCP
801-274-1184
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 5
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Introduction:When thinking about major health conditions that drive people to the doctor what comes to mind are complex medical conditions such as diabetes, heart disease, and hypertension. Surprisingly however low back pain (LBP) is consistently reported as one of the top five reasons to seek medical care (Chou et al., 2007; Ladeira, 2011). Low back pain is the most common musculoskeletal condition seen by physical therapists in the United States (Beattie, 2011; Fritz, Cleland, & Childs, 2007). The lifetime incidence of an acute episode of LBP ranges from 60% to 90%, and 30% of those may develop chronic LBP (Philadelphia Panel, 2001; Delitto et al., 2012; van Tulder et al., 2006).
Chronic low back pain (CLBP) can have devastating consequences from an inability to participate in daily activities, to declining work productivity, and decreased tolerance for recreational pursuits (Chou et al., 2007; Delitto et al., 2012; Nguyen, 2007). Many of the theories about low back pain may perpetuate false beliefs about how
best to manage this condition. Physical therapists commonly hear statements such as: “you should rest until the back pain stops”, “exercise is bad for my back”, and “x-rays and MRI’s are needed to show the true source of the back pain”. Patients are often led to believe that medications can “fix” the problem which perpetuates their dependence on the healthcare system. It is no wonder then that the success in managing LBP has been less than optimal.
Having a firm understanding of these misconceptions or myths should help guide the nurse decision-makers when developing a life care plan (LCP) for persons with CLBP that may be secondary to other medical conditions or as the sole reason for a person’s disability. The purpose of this article is to discuss and provide evidence that refutes these myths including the importance of exercise for people dealing with CLBP, medications and their role, and the purpose of diagnostics for this population. Additionally this article will discuss elements that the life care planner should consider when developing a plan.
Myth #1: Rest and Medication will Cure LBP. It was a common belief that long periods of rest was needed to resolve symptoms causing LBP (Waddell, 1987). Current evidence however, has proven this theory to be inaccurate (Chou et al., 2007). There may be situations when brief periods of bed rest is warranted following an acute episode of LBP or even following an acute exacerbation of a chronic lower back condition (Dahm, Brurberg, Jamtvedt, & Hagen, 2010). During an acute first-time episode or an acute exacerbation, the soft tissues involved undergo a natural process whereby acute inflammatory markers or signs are present. These may include redness, heat, swelling, decreased range of motion (ROM), and pain at the affected area. Inflammation is part of the body’s normal immune response. During this period (particularly the first 48 hours) rest, especially from the offending activities, is recommended as the body attempts to heal itself (Kuritzky, & Samraj, 2012; Nordqvist, 2015).
The problem with too much rest is that muscles weaken and joints stiffen causing
CHRONIC LOW BACK PAIN:
IMPACT ON THE LIFE CARE
PLAN
EMMA W. WHITE, PT, DPT, OCS

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 6
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
reduced spinal mobility and range of motion which can lead to a loss of spine stability (Beattie, 2011; Delitto et al., 2012; Belavy, Armbrecht, Richardson, Felsenberg, & Hides, 2011; Bortz II, 1984; Koes, van Tulder, Ostelo, Burton, & Waddell, 2001; O’Sullivan, Twomey, & Allison, 1997). O’Sullivan, Twomey, and Allison (1997) and Hides, Richardson, and Jull (1996) demonstrated that following an acute episode of LBP, the muscles primarily responsible (lumbar multifidus) for the segmental stability of the lumbar spine were not automatically “turned back on”. In other words these muscles were no longer functioning properly even when the person no longer reported LBP (O’Sullivan et al., 1997; Hides, Richardson, & Jull, 1996; Hides, Stokes, Saide, Jull, & Cooper, 1994). This finding was eye-opening for many healthcare practitioners as the lack of a response from these muscles has been tied to frequent LBP exacerbations (O’Sullivan et al., 1997; Hides et al. 1996; Hides, Stokes, Saide, Jull, & Cooper, 1994).
Medications commonly prescribed to manage LBP include: nonsteroidal anti-inflammatory drugs (NSAIDs) opioids, and antidepressants. Short term use of acetaminophen or NSAIDs have been used to reduce acute inflammatory signs early on in the injury process or following an acute exacerbation of a chronic condition (Chou et al., 2007; White, Arnold, Norvell, Ecker, & Fehlings, 2011; Wong et al., 2017). White, Arnold, Norvell, Ecker, and Fehlings, (2011) summarized the safety and effectiveness of these drug classifications in the management of LBP.
A secondary objective of this study was to evaluate whether certain subpopulations respond more favorably to pharmacological management (White et al., 2011). The conclusions drawn were consistent with other researchers (Chou et al., 2007) whose findings support NSAIDs as being effective for managing chronic LBP, the strength of evidence is strong. Opioids were also found to be effective but based on the significant rate of side effects including aberrant drug-related behaviors and the lack of convincing superiority over NSAID’s,
conclusions included that opioids are not recommended as a treatment for CLBP (White et al., 2011). Antidepressants had no meaningful clinical benefit and thus based on these reviews should not be routinely used for managing CLBP (Chou et al., 2007; White et al., 2011). Additional conclusions drawn suggest that categorization of certain patient specific subgroups may be helpful in guiding future treatment decisions because LBP is a heterogeneous condition and as such, all patients will not respond in the same fashion (White et al., 2011).
Interestingly, the physical therapy literature consistently reports the need to manage LBP as a heterogeneous condition. The cause of a person’s LBP is not the same in every case thus managing LBP symptoms will be considerably different based on the heterogeneous nature this condition (Delitto et al., 2012; Fritz, Cleland, & Childs, 2007). Common to physical therapy practice, the primary purpose for categorizing LBP is to identify features at baseline that predict responsiveness to different treatment strategies thus reducing the likelihood of bouts of LBP recurrences while increasing the probability of a successful outcome (Delitto et al., 2012; Fritz et al., 2007; Herbert, Koppenhaver, & Walker, 2011).
Myth #2: Exercise is Bad for My Back. While this belief is slowly fading, there are still portions of the population that believe exercising is harmful to their backs and thus serves no benefit. According to the U.S. Bureau of Labor Statistics, only an estimated 13% to 20% of people over the age of 15 participate in regular lifestyle physical activity, with variations based on regional habitat (Dreisinger, 2014). Individuals with CLBP are even less likely to participate in exercises. Therefore the lack of physical activity then perpetuates their symptoms.
Anatomy Review and Rationale for Exercise in LBP ManagementThe spine is comprised of 33 vertebrae.
Each vertebral body has two bony projections extending from the sides. These projections articulate with the vertebrae above thus forming an articular joint, the facet joints. The facet joints are weight bearing joints that allow for trunk movement in all directions: rotation, bending forward and backward, and side bending right and left. These weight bearing joints can become stiff secondary to a lack of movement in the trunk. This process is similar to a knee that loses joint range of motion when individuals become more sedentary and less active.
Pain is a likely consequence associated with joint stiffness. As joint movement continues to decline and lifestyles become more sedentary, muscles don’t contract. Over time they too become weak and thus are no longer able to support the spine which can lead to different degrees of spinal instability. Yanik, Keyik, and Conkbayir (2013) showed that individuals with CLBP have greater fatty infiltration and less muscle mass in the segmental lumbar extensor muscles, the lumbar multifidus. These muscles are important in providing segmental stabilization of the trunk. This muscle composition is relevant because multifidus fibers show a natural degree of atrophy even in individuals with no history of back pain as well as in patients with CLBP (Hides et al., 1996; Mattila et al., 1986).
Considerable work in the past several years has theorized a correlation between lumbar multifidus atrophy persisting even after spontaneous resolution of symptoms in those patients who did not exercise following recovery from LBP. This led Dreisinger (2014) to conclude that “exercise is an important strategy in the management of back pain regardless of whether the pain is acute or chronic” (p. 105).
The weakness of the transversus abdominus (TrA) has also been implied as a possible leading cause for the persistence of LBP. The TrA is another very important core stabilizer of the spine because of its attachment on the thoracodorsal fascia of the spine. When working to increase abdominal
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 7
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
strength and endurance this muscle has often been overlooked as the focus has been on strengthening the rectus abdominis and the internal and external oblique musculature. O’Sullivan et al. (1997) demonstrated decreased pain and disability in patients with chronic LBP by targeting specific exercise for the TrA. The participants in the study had a radiologically confirmed diagnosis of spondylolysis or spondylolisthesis, which oftentimes results in spinal instability (O’Sullivan et al., 1997). It is believed that when there is a simultaneous contraction of the multifidus muscles and the TrA there is maximum stabilization of the spine resulting in less chronic pain severity (Delitto et al., 2012).
In summary, although general exercises for the whole body and encouraging the individual to stay active have been shown to be beneficial for chronic LBP sufferers, in recent years increasing emphasis has placed more attention directed at exercises to improve endurance of the core spinal muscles, namely multifidus and TrA, in addition to a more generalized exercise program (Chou et al., 2007; Ladeira, 2011; Wong et al., 2017; Maher, Latimer, & Refshauge, 1999). These more specific exercises were developed to target the muscles that are associated with
lumbar–pelvic stability with the aim of developing more effective and efficient exercise for low back control (Hodges & Richardson, 1996).
Myth #3: X-rays and MRI Scans are Needed to Show the True Source of LBP. One might expect that improvement in the resolution of imaging technology has increased the likelihood of detecting a link between pathology and pain in the lumbar spine. However, the determination of a pathoanatomic origin of low back pain is made difficult by the rate of false-positive findings on imaging studies, that is, individuals without low back pain showing abnormal findings (Chou, Qaseem, Owens, & Shekelle, 2011). Research has shown that as many as 36% of asymptomatic persons aged 60 years or older had a herniated disc, and more than 90% had a degenerative or bulging disc (Chou et al., 2011). Current recommendations are that “clinicians should not routinely obtain imaging or other diagnostic tests in patients with nonspecific low back pain” (Chou, et al., 2007, p.478). Further, clinicians should perform diagnostic imaging and testing for patients with low back pain when severe or progressive neurologic
deficits are present or when serious underlying conditions are suspected by history and physical examination (Chou et al., 2007). These findings are further supported by the American College of Physicians (Chou et al., 2011).
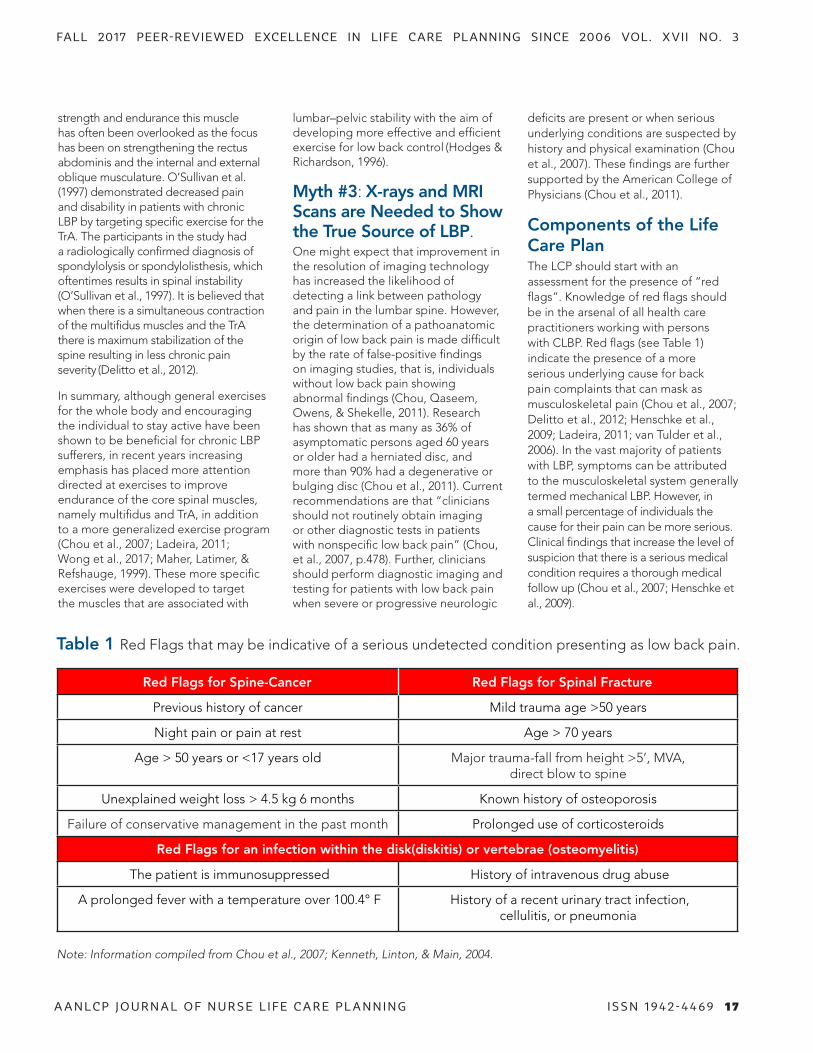
Components of the Life Care PlanThe LCP should start with an assessment for the presence of “red flags”. Knowledge of red flags should be in the arsenal of all health care practitioners working with persons with CLBP. Red flags (see Table 1) indicate the presence of a more serious underlying cause for back pain complaints that can mask as musculoskeletal pain (Chou et al., 2007; Delitto et al., 2012; Henschke et al., 2009; Ladeira, 2011; van Tulder et al., 2006). In the vast majority of patients with LBP, symptoms can be attributed to the musculoskeletal system generally termed mechanical LBP. However, in a small percentage of individuals the cause for their pain can be more serious. Clinical findings that increase the level of suspicion that there is a serious medical condition requires a thorough medical follow up (Chou et al., 2007; Henschke et al., 2009).
Red Flags for Spine-Cancer Red Flags for Spinal Fracture
Previous history of cancer Mild trauma age >50 years
Night pain or pain at rest Age > 70 years
Age > 50 years or <17 years old Major trauma-fall from height >5’, MVA, direct blow to spine
Unexplained weight loss > 4.5 kg 6 months Known history of osteoporosis
Failure of conservative management in the past month Prolonged use of corticosteroids
Red Flags for an infection within the disk(diskitis) or vertebrae (osteomyelitis)
The patient is immunosuppressed History of intravenous drug abuse
A prolonged fever with a temperature over 100.4° F History of a recent urinary tract infection, cellulitis, or pneumonia
Table 1 Red Flags that may be indicative of a serious undetected condition presenting as low back pain.
Note: Information compiled from Chou et al., 2007; Kenneth, Linton, & Main, 2004.

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 8
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Recent evidence has also advised that “yellow flags” be taken into account. Yellow flags (see Table 2) describe a person’s personal mistaken attitudes and beliefs about pain and injury and are believed to represent psychological barriers that risk delayed recovery. Many researchers have begun to establish a link between fear-avoidance beliefs (FABs) in those with LBP and the transition from acute to chronic symptoms (Cleland, Fritz, & Brennan, 2008; Fritz & George, 2002; Fritz, George, & Delitto, 2001). It is important to identify clients who are at risk of developing long-term pain and disability by assessing a person’s FAB’s, hypervigilance (preoccupation with pain), and pain catastrophizing (over estimating the negative effects of the pain).
A well-researched questionnaire commonly used in clinical practice to assess FAB is the fear-avoidance beliefs questionnaire (FABQ). The FABQ measures a patients’ fear of pain and subsequent avoidance of physical activity (Rainville et al., 2011). This self-report measure consists of two subscales: 1) work (maximum value 42 points, >34 indicate high fear-avoidance beliefs that may affect the outcome) and 2) physical activity (maximum value 24 points). See resource list for how to access the FABQ.
The presence of yellow flags may indicate the need to alter the management approach using cognitive behavioral therapy (CBT) and/or referral to a mental health professional (Fritz & George, 2002; George, Fritz, & Childs, 2008). Cognitive behavioral therapy is a type of psychotherapy that takes a practical approach to problem-solving. Its goal is to change patterns of thinking or behavior by focusing on the thoughts, images, beliefs and attitudes that are held and how these processes relate to the way a person behaves (Cherkin et al., 2016; Hanscom, Brox, & Bunnage, 2015).
Once red and yellow flags have been accounted, the life care planner should relay reassurance, let the client know LBP has a favorable outcome and that symptoms can be resolved with vigilance. Long periods of bed rest should not be encouraged, but rather advise clients to return to their normal activity levels soon after symptom onset. Educate individuals that moving stiff joints and stretching tight muscles can cause some discomfort in the beginning but that ultimately the movement will improve their symptoms. Low-level activity such as walking can also be encouraged. Walking is a fundamental human activity that is easy to perform, has a low risk of injury, and is associated
with many health benefits (Dreisinger, 2014; Hendrick et al., 2010; Hurley et al., 2015). Something as simple as a daily walk keeps individuals out of a wheelchair and in many instances allows them to continue to participate in activities at home as well as in their communities ultimately enhancing functional levels.
Types of Exercise for LBPExercise can come in many forms from flexibility and range of motion, strengthening, endurance, stretching, aerobic, aquatic, and many more. Selecting
Yellow Flags Explanation/Description
Fear-avoidance beliefsInappropriate beliefs that back pain is harmful or
potentially severely disabling
HypervigilanceExcessive pre-occupation with pain, preoccupied with
constant scanning of the environment for possible threats to their LBP
Pain catastrophizing
An overestimation of the impact pain has on physical activity, conceptualized as a negative cognitive–
affective response to anticipated or actual pain or a tendency to magnify the threat value of a pain stimulus
Low self- efficacyFeelings of having little control over the pain, have
very little confidence in self
Emotional problems Depression, anxiety, withdrawal from social interaction
Misunderstanding about effective treatment strategiesThe expectation of passive treatments rather than the
belief that active participation will help
Table 2 Examples of Yellow Flags
Note: Information compiled from Beattie, 2011; Delitto, 2012; van Tulder, 2006.
1) Impaired physical mobility (Domain 4, Activity/Rest, Class 2, Activity/Exercise)
2) Activity intolerance (Domain 4, Activity/Rest, Class 4, Cardiovascular/Pulmonary Responses)
3) Impaired resilience (Domain 9, Coping/Stress Tolerance, Class 2, Coping Responses)
4) Chronic pain (Domain 12, Comfort, Class 1, Physical Comfort)
Nursing Diagnoses To Consider

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 1 9
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
the correct type of exercise can be tricky when first engaging clients. If an exercise is too difficult individuals may become discouraged and if too easy there may not be a direct benefit. The nurse life care planner (NLCP) should determine the individual’s current physical activity level: deconditioned, sedentary, or active. Additionally, the NLCP needs to get an idea of the percent of the day the client spends in a reclined state, the person’s tolerance for activities of daily living (ADL); and if assistance is needed, how much is required. Ultimately the NLCP acquires a sense of the demands required of each client and the client’s current ability to meet those demands.
The NLCP should consider a consultation with a physical therapist particularly for those clients who have not been active for a long time. Physical therapists may be better equipped to more objectively evaluate and design exercise programs tailored to the specific needs of the client especially given the heterogeneous nature of LBP and the physical therapist’s education and background rich in assessment and management of musculoskeletal conditions
such as LBP. Invariably persons suffering from CLBP may need specific exercise targeting the TrA and lumbar multifidus muscles. See resources list for information on how to target these muscles.
Other exercise programs that have shown some promise in managing CLBP are yoga and Tai chi. Although the evidence to date has not been robust, it is however, improving (Chou et al., 2017; Hall, Maher, Lam, Ferreira, & Latimer, 2011; Holtzman & Beggs, 2013). These types of programs can be found at local health clubs or YMCA facilities.
Conclusion Life care planning for individuals with CLBP should adequately address the areas covered in this manuscript while dispelling myths that negatively impact individual’s perceptions and preconceived notions about low back pain management. CLBP can result in devastating impairments if left poorly managed both from a physical and psychological perspective. The NLCP should speak encouragingly with optimism, encourage exercise and walking programs such as yoga and Tai chi. In
those individuals who may have high fear-avoidance behaviors or yellow flags don’t hesitate to recommend a CBT approach. Some activities may require modifications but rarely are they eliminated. Individuals who suffer CLBP can live productive and happy lives.
Resources:Link to gain better understanding of the abdominal musculature and role of transverse abdominus muscle:http://www.physio-pedia.com/Abdominal_Muscle_Anatomy
Link to gain better understanding of the lumbar multifidus muscles:https://www.coreconcepts.com.sg/article/multifidus-smallest-yet-most-powerful-muscle/
Link to FABQ:https://www.tac.vic.gov.au/files-to-move/media/upload/fear_avoidance.pdf.
Link that discusses how to activate the transverse abdominus muscle:
https://www.youtube.com/watch?v=aqwx6uCwhUQ
Yellow Flags Explanation/Description
Fear-avoidance beliefsInappropriate beliefs that back pain is harmful or
potentially severely disabling
HypervigilanceExcessive pre-occupation with pain, preoccupied with
constant scanning of the environment for possible threats to their LBP
Pain catastrophizing
An overestimation of the impact pain has on physical activity, conceptualized as a negative cognitive–
affective response to anticipated or actual pain or a tendency to magnify the threat value of a pain stimulus
Low self- efficacyFeelings of having little control over the pain, have
very little confidence in self
Emotional problems Depression, anxiety, withdrawal from social interaction
Misunderstanding about effective treatment strategiesThe expectation of passive treatments rather than the
belief that active participation will help
REFERENCESBeattie, P. F. (2011). Current Concepts for Orthopaedic Physical Therapy, 3rd Edition: the lumbar spine: physical therapy patient management utilizing current evidence. LaCrosse, Wis.: Orthopaedic Section, APTA, © 2011
Belavý, D .L., Armbrecht, G., Richardson, C. A., Felsenberg, D., & Hides, J. A. (2011) Muscle atrophy and changes in spinal morphology: Is the lumbar spine vulnerable after prolonged bed-rest? Spine, 36(2), 137-145. doi: 10.1097/BRS.0b013e3181cc93e8.
Bortz II, W. M. (1984). The disuse syndrome. Western Journal of Medicine, 141, 691-694.
Cherkin, D. C., Sherman, K .J., Balderson, B. H., Cook, A .J., Anderson, M. L., Hawkes, R. J.,… Turner, J. A. (2016). Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: A randomized clinical trial. Journal of the American Medical Association, 315(12), 1240-1249.
Chou, R., Deyo, R., Friedly, J., Skelly, A., Hashimoto, R., Weimer, M.,…Brodt, E. D. (2017). Nonpharmacologic therapies for low back pain: A systematic review from the American college of physicians clinical practice guidelines. Annals of Internal Medicine, 166(7), 493-505.
Chou, R., Qaseem, A., Snow, V., Casey, D., Cross, J. T., Shekelle, P., & Owens, D.K. (2007). Diagnosis and treatment of low back pain: A joint clinical practice guideline from the American college of physicians and the American pain society. Annals of Internal Medicine, 147, 478-491.
Chou, R., Qaseem, A., Owens, D.K., & Shekelle, P. (2011). Diagnostic imaging for low back pain: Advice for high-value health care from the American college of physicians. Annals of Internal Medicine, 154(3), 181-189.
Cleland, J.A., Fritz, J.M., & Brennan, G.P. (2008). Predictive validity of initial fear avoidance beliefs in patients with low back pain receiving physical therapy: Is the FABQ a useful screening took for identifying patients at risk for a poor recovery? European Spine Journal, 17, 70-79. doi:10.1007/s00586-007-0511-y
Dahm, K. T., Brurberg, K. G., Jamtvedt, G., & Hagen, K. B. (2010). Advice to rest in bed versus advice to stay active for acute low-back pain and sciatica. Cochrane Database of Systematic Reviews, 16(6). doi:0.1002/14651858.CD007612.pub2
Delitto, A., George, S. Z., Van Dillen, L., Whitman, J. M., Sowa, G., Shekelle, P.,… Godges, J. J. (2012). Low back pain clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American physical therapy association. Journal of Orthopaedic & Sports Physical Therapy, 42(4), A1-A57.
Dreisinger, T. E. (2014). Exercise in the management of chronic back pain. Ochsner Journal, 14(1), 101-107.
Fritz, J. M., Cleland, J. A., & Childs, J. D. (2007). Subgrouping patients with low back pain: evolution of a classification approach to physical therapy. Journal of Orthopaedic & Sports Physical Therapy, 37(6), 290-302.
Fritz, J.M., & George, S.Z. (2002). Identifying psychological variables in patients with acute work-related low back pain: The importance of fear-avoidance beliefs. Physical Therapy, 82, 973-983.

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 0
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Fritz, J. M., George, S. Z., Delitto, A. (2001). The role of fear-avoidance beliefs in acute low back pain: relationships with current and future disability and work status. Pain, 94, 7-15.
George, S. Z., Fritz, J. M., & Childs, C. D. (2008). Investigation of elevated fear-avoidance beliefs for patients with low back pain: A secondary analysis involving patients enrolled in physical therapy clinical trials. Journal of Orthopaedic & Sports Physical Therapy, 38(2), 50-58.
Hall, A. M., Maher, C .G., Lam, P., Ferreira, M., & Latimer, J. (2011). Tai chi exercise for treatment of pain and disability in people with persistent low back pain: A randomized controlled trial. Arthritis Care & Research, 63(11), 1576-1583. doi:10.1002/acr.20594
Hanscom, D.A., Brox, J. I., & Bunnage, R. (2015). Defining the role of cognitive behavioral therapy in treating chronic low back pain: an overview. Global Spine Journal, 5, 496-504.
Hebert, J. J., Koppenhaver, S. L., & Walker, B.F. (2001). Subgrouping patients with low back pain: a treatment-based approach to classification. Sports Health, 3(6), 534-542.
Hendrick, P., Te Wake, A M., Tikkisetty, A. S., Wulff, L., Yap, C., & Milosavljevic, S. (2010). The effectiveness of walking as an intervention for low back pain: A systematic review. European Spine Journal, 19, 1613–1620. doi:10.1007/s00586-010-1412-z
Henschke, N., Maher, C. G., Refshauge, K. M., Herbert, R. D., Cumming, R. G., Bleasel, J.,…McAuley, J. H. (2009). Prevalence of and screening for serious spinal pathology in patients presenting to primary care settings with acute low back pain. Arthritis & Rheumatism, 60(10), 3072-3080.
Hides, J.A., Richardson, C.A., & Jull, G.A. (1996). Multifidus muscle recovery is not automatic after resolution of acute, first-episode low back pain. Spine, 21(23), 2763-2769.
Hides, J.A., Stokes, M. J., Saide, M., Jull, G.A., & Cooper, D.H. (1994). Evidence of lumbar multifidus muscle wasting ipsilateral to symptoms in patients with acute/subacute low back pain. Spine, 19(2), 165-172.
Hodges, P., & Richardson, C. (1996). Inefficient muscular stabilization of the lumbar spine associated with low back pain: a motor control evaluation of transversus abdominis. Spine, 21, 2640-2650.
Holtzman, S., & Beggs, R. T. (2013). Yoga for chronic low back pain: A meta-analysis of randomized controlled trials. Pain Research & Management, 18(5), 267-272.
Hurley, D. A., Tully, M. A., Lonsdale, C., Boreham, C. A., van Mechelen, W., Daly, L.,…McDonough, S. M. (2015). Supervised walking in comparison with fitness training for chronic back pain in physiotherapy: Results of the SWIFT single-blinded randomized controlled trial. Pain, 156(1), 131-147.
Koes, B. W., van Tulder, M. W., Ostelo, R., Burton, A. K., & Waddell, G. (2001). Clinical guidelines for the management of low back pain in primary care: An international comparison. Spine, 26(22), 2504-2513.
Kuritzky, L., & Samraj, G.E. (2012). Nonsteroidal anti-inflammatory drugs in the treatment of low back pain. Journal of Pain Research, 5, 579-590. doi:10.2147/JPR.S6775
Ladeira, C. E. (2011). Evidence based practice guidelines for management of low back pain: Physical therapy implications. Brazilian Journal of Physical Therapy, 15(3), 190-199.
Maher, C., Latimer, J., & Refshauge, K. (1999). Prescription of activity for low back pain: What works? Australian Journal of Physiotherapy, 45, 121–132.
Mattila, M., Hurme , M., Alaranta, H., Palijavi, L., Kalimo, H., Falck, B.,..Jarvinen, M. (1986). The multifidus muscle in patients with lumbar disc herniation: A histochemical and morphometric analysis of intraoperative biopsies. Spine, 11(7), 732-738.
Nguyen, T. H., Randolph, D .C. (2007). Nonspecific low back pain and return to work. American Family Physician, 76(10), 1497-1502.
Nordqvist, C. (2015). Inflammation: causes, symptoms and treatment. Medical News Today. Retrieved from http://www.medicalnewstoday.com/articles/248423.php.
O’Sullivan, P. B., Twomey, L.T., & Allison, G.T. (1997). Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine, 22(24), 2959-67.
Philadelphia Panel. (2001). Philadelphia Panel Evidence-based clinical practice guidelines on selected rehabilitation interventions for low back pain. Physical Therapy, 81(10), 1641–1674.
Rainville, J., Smeets, R. J., Bendix, T., Tveilto, T. H., Poiraudeau, S., & Indahl, A. J. (2011). Fear-avoidance beliefs and pain avoidance in low back pain-translating research into clinical practice. Spine Journal, 11(9), 895-903. doi: 10.1016/j.spinee.2011.08.006
van Tulder, M., Becker, A., Bekkering, T., Breen, A., Gil del Real, M.T., Hutchinson A.,…Rozenberg, S. (2006). European guidelines for the management of acute nonspecific low back pain in primary care. European Spine Journal, 15 (Suppl. 2), S169–S191.
White, A. P., Arnold, P. M., Norvell, D. C., Ecker, E., & Fehlings, M. G. (2011). Pharmacologic management of chronic low back pain: synthesis of the evidence. Spine, 36(21), S131-143. doi: 10.1097/BRS.0b013e31822f178f.
Wong, J. J, Cote, P., Dutton, D.A., Randhawa, K., Yu, H., Varatharajan, S.,… Taylor-Vaisey, A. (2017). Clinical practice guidelines for the noninvasive management of low back pain: a systematic review by the Ontario protocol for traffic injury management (OPYIMA) collaboration. European Journal of Pain, 21, 201-216. doi: 10.1002/ejp.931
Yanik, B., Keyik, B., & Conkbayir, I. (2013). Fatty degeneration of multifidus muscle in patients with chronic low back pain and in asymptomatic volunteers: Quantification with chemical shift magnetic resonance imaging. Skeletal Radiology, 42, 771-778. doi: 10.1007/s00256-012-1545-8
EMMA W. WHITE, PT, DPT, OCS Dr. Emma White is a Clinical Assistant Professor, Department of Physical Therapy, Winston Salem State University. Dr. White received her PT degree from the Medical College of Virginia in 1978. Dr. White brings 30 years of clinical experience with 16 of those years owning an orthopedic private practice in Thomasville, NC (1991-2007) working extensively in the management of patients presenting with musculoskeletal spine and extremity conditions, both surgical and non-surgical. Dr. White received her clinical doctorate in physical therapy from the University of North Carolina at Chapel Hill in 2008, and her ABPTS certification in Orthopedics in 2014. Dr. White joined the WSSU DPT faculty in 2011. Dr. White is very active and a passionate member of the North Carolina Physical Therapy Association serving as the Director at Large for Reimbursement. Dr. White’s research interest: conservative management of LBP, quantifying forward head postural dysfunction and exploring its relationship to fall risk in older adults, and injury prevention in athletes and sports enhancement.

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 1
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 4 6
S P R I N G 2017 P E E R - R E V I E W E D E XC E L L E N C E I N L I F E C A R E P L A N N I N G S I N C E 20 0 6 V O L . X V I I N O. 1
CRASHCART - Is your practice experiencing a Code Blue? Revive it with AANLCP’s resource cart. Forms, templates, contracts and resources all at your fingertips.
PMIC’S MEDICAL FEES BOOK - Need the most recent medical cost? Yep, that’s right, we’ve got it!
EBSCO: REHAB REFERENCE / CINAHL - Bump up your plans with research, journals and industry insights.
FIND-A-CODE - Save time and get access to an expansive medical coding and billing resource, now with Anesthesia crosswalk.
DISCOUNTS, DISCOUNTS, DISCOUNTS... We’ve got member only discounts you won’t want to miss, check out #thriftythursdays
MARKETING MATERIAL - Tired of explaining what a life care planner does? Present your practice with high quality and professionally designed marketing materials that get you hired.
OFFICIAL DISABILITY GUIDELINES - Need a comprehensive tool to assess treatment options? Members have access to the most comprehensive and up to date medical treatment guidelines worldwide. Yep it’s included.
Don’t forget our webinars, journals, Lifeline (mentorship), and much, much more.
*Resource access is dependent upon your individual membership type and tier.
A M E R I C A N A S S O C I A T I O N O F N U R S E L I F E C A R E P L A N N E R S

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 2
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Genetics, trauma, vascular complications, infectious disease, and environmental factors cause disorders of the central and peripheral nervous system leading to spinal cord injuries (SCI). The most common causes of mechanical SCIs are motor vehicle accidents (MVA) (40.4%), falls (27.9%), and acts of violence (15%) (Li & Lepski, 2013). The average age at highest risk for a SCI is 40.7 years (Li & Lepski, 2013).
This article discusses current and potential alternative therapies available for persons with SCI to minimize disease progression and provide maximum independence. The areas of focus are cell transplantation, alternative spinal surgery, neuroplasticity, upper/lower extremity functional electrical stimulation (FES), and exoskeleton.
Cell TransplantationThere are four sections of cell transplantation: human embryonic cells, mesenchymal stromal cells, differentiation and growth hormone
of stem cells, and allogeneic cell transplantation. These sections discuss the history and use of stem cells, and the function, mechanism, and drawbacks of cell transplantation.
History and UseAccording to Harrison (2016), clinics around the world are offering cell transplantation treatments for SCI, but it is still in the beginning stages. Until December 2016, the United States clinics operated under the assumption that the Food and Drug Administration (FDA) would permit treating patients with stem cells from their bodies. Recently, the FDA issued guidance that these products are for homologous purposes (bone cells for bone treatments and skin cells for skin treatment). According to Dr. Jeffrey C. Wang, chief of the Orthopaedic Spine Service at the University of Southern California in Los Angeles, proper studies are needed to acquire much-needed evidence to support the use of stem cells in the United States (Harrison, 2016). Barriers currently
hinder studies that are desired to establish standards for treatment and insurance reimbursement.
In countries other than the United States, alternatives to current spinal surgery techniques are led by stem cell science and provide promise in improving and expanding current spinal surgery techniques (Goldschlager et al., 2013). Cell transplantation may promote nerve regeneration and potentially reverse impaired nerve function after a SCI. Cell-based treatments aimed at intervention and attenuation of intervertebral disc degeneration and radiculopathies early in the SCI may provide regenerative and anti-inflammatory treatments (Goldschlager et al., 2013).
The primary goal of stem cell-based therapy for SCI is to promote axonal regrowth above and below the injury site with regeneration and replacement of nerve cells. Mesenchymal cells are considered an ideal cell source for cell therapy of neurological lesions
ERIN T. OCONNELL, MSN, MBA, RN-BC, CNL, CNLCP®
Alternative Treatments for
Individuals with a Spinal
Cord Injury

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 3
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
to facilitate their recovery through immunomodulatory and anti-inflammatory mechanisms. Persons with SCI who received mesenchymal stromal cell transplantation have reported improvement in motor and somatosensory functioning (Li & Lepski, 2013).
Human Embryonic Stem Cells (ESC)Human embryonic stem cells (ESC) have the capacity for rapid reproduction and self-renewal. They are capable of giving rise to several different cell types and have the ability to differentiate into all three germ layer lineages: mesoderm (middle layer of an embryo during the early development of the embryo), endoderm (innermost layer of cells of an embryo during the early development of the embryo or lining of the gut), and ectoderm (outermost layers of cells during the early development of the embryo). The mesoderm layer is most relevant to spine surgery (Goldschlager et al., 2013). On the downside, since ESCs are unlimited, self-renewing, and differentiated, they tend to develop undesired teratomas, a tumor with tissue or organ components (Goldschlager et al., 2013).
Mesenchymal Stromal Cells (MSC)Mesenchymal stromal cells derived from almost all tissue in the body. The cells most significant to spinal cord surgery are mesenchymal in origin (Goldschlager et al., 2013). The cells are derived from post-natal tissues and do not evoke the same ethical dilemmas as the ESCs (Goldschlager et al., 2013). Harvested from bone marrow, adipose tissue, muscle, and dental pulp, the MSC have less differentiation than ESCs, but can predominately differentiate into bone, cartilage, muscle, and fat (Goldschlager, et al., 2013).
Since inflammation is a causative factor for back pain, the MSC’s anti-inflammatory properties may directly reduce pain in addition to or as an
alternative to a surgical procedure (Goldschlager et al., 2013). Anti-inflammatory mechanisms of MSCs include immune modulation, inhibition of T-cell activation, and proliferation and reduction of pro-inflammatory cytokines (Buzhor et al., 2014). Mesenchymal progenitor cells (MPC) are a type of stromal cells isolated from the bone marrow and adipose tissue (Goldschlager et al., 2013). According to DiazQuiroz, and Echeverri (2013), MPCs are currently the closest of all stem cells for clinical enhancement for spinal surgery.
Differentiation and Growth Hormone of Stem CellsThe cell populations harvested from different sources and methods grow at different rates (Goldschlager et al., 2013). As a result, cell differentiation must be identified and then controlled, so that, the transplanted cells develop into the desired end product. For example, progenitor cells tend to differentiate into a cell type with greater specificity than a stem cell. Similarly, the growth factors required for mesenchymal stromal cells (MSC) derived from bone marrow to differentiate into cartilage is different from growth factor needed to differentiate MSC from adipose tissue into cartilage.
Allogeneic Cell TransplantationAllogeneic cell transplantation (ALT) refers to stem cells collected from a matching donor. The ALT is produced in batches with batch-to-batch consistency (Goldschlager et al., 2013). Although ACT promotes donor site morbidity, this form of transplantation has increased the risk of infection and rejection. Extensive screening, such as blood transfusion screening, is used to minimize these risks (Goldschlager et al., 2013). There are no reported allogeneic transplant reactions, and they do not elicit delayed or immediate hypersensitivity reactions (Li & Lepski, 2013).
Alternative Spinal SurgerySpinal cord surgery indications occur
when conservation measures are exhausted, and pain and disability persist. In general, spinal surgery is indicated to accomplish the following goals: neural decompression, stabilization or restoration of the deformity, and removal of a pain generator (Goldschlager et al., 2013).
In Australia, cell transplantation is used as part of spinal discectomy surgery (Goldschlager et al., 2013). Stem cells replace the spinal disc with a new tissue engineered disc to facilitate regeneration of the excised tissue. This method of interbody replacement is thought to provide the best option to fill the void following a discectomy (Goldschlager et al., 2013).
Allograft and autograft options are
1) Impaired physical mobility (Domain 4, Activity/Rest, Class 2, Activity/Exercise)
2) Impaired transfer ability (Domain 4, Activity/Rest, Class 2, Activity/Exercise)
3) Risk for disuse syndrome (Domain 4, Activity/Rest; Class 2, Activity/Exercise)
4) Activity intolerance (Domain 4, Activity/Rest, Class 4, Cardiovascular/Pulmonary Responses)
5) Bathing self-care deficit (Domain 4, Activity/Rest, Class 5, Self-Care)
6) Dressing self-care deficit (Domain 4, Activity/Rest, Class 5, Self-Care)
7) Feeding self-care deficit (Domain 4, Activity/Rest, Class 5, Self-care)
8) Toileting self-care deficit (Domain 4, Activity/Rest, Class 5, Self-care
9) Impaired resilience (Domain 9, Coping/stress Tolerance, Class 2, Coping Responses)
10) Chronic pain (Domain 12, Comfort, Class 1, Physical Comfort
Nursing Diagnoses To Consider

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 4
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
currently available for cervical and lumbar fusion surgery. Allograft is tissue or bone from a donor of the same species, and they reduce the complications related to donor site morbidity. The drawbacks to allografts are they produce an inferior fusion rate when compared to the autograft. Allografts have a greater potential for rejection reabsorption, infection, and logistical issues (Goldschlager et al., 2013). Possible complications of the autograft include donor site residual pain, infection, or cosmetic problems.
NeuroplasticityNeuroplasticity is the brain’s ability to form new nerve cell connections throughout our lives. It provides us the opportunity to compensate for injury or disease that affects the neurons of the brain. Neuroplasticity also allows the brain to change and adjust to activities and environmental changes. Brain reorganization occurs when “axonal sprouting” occurs, the healthy axons grow, and the nerve endings connect with other healthy nerves. When they reconnect, the new neural pathways achieve a needed function (Medical Definition of Neuroplasticity, 2017).
The brain can compensate for a damaged area by reorganizing the neurons and forming new connections to bypass the damaged area. For axonal sprouting to occur, activity stimulates the neurons. The nervous system may change when exposed to a stimulus (Martin, Sadowsky, Obst, Meyer, & McDonald, 2012). Since permanent changes are possible with long-term, repeated exposure, the quantity, and type of activity are crucial in development and plasticity within the nervous system. Developments can include gene expression, modification of synaptic strength, synapse elimination, myelination, maintenance of myelination, and axonal growth (Martin et al., 2012). Neuroplasticity is also known as brain plasticity or brain malleability.
Functional Electrical Stimulation (FES)Persons with upper and lower limb paralysis may be limited in their
capacity to walk, perform activities of daily living (ADLs), or their ability to perform the physical exercise to the extent needed to improve health and fitness. The application of electrical stimulus to a paralyzed muscle or nerve to achieve or restore function is called FES (Martin et al., 2012). Functional electrical stimulation (FES) provides exercise to improve blood circulation, aerobic conditioning, heart health, bone density, overall fitness, and reduction of muscles spasms of persons with SCI. Functional electrical stimulation (FES) therapy emits low-level electrical impulses to activate specific muscles in the hands, arms, legs, and other areas. The designated muscles receive electrical impulses via surface electrodes or implanted electrodes.
Up and coming research has indicated positive outcomes related to neural restoration due to neural plasticity and recovering function following a SCI (Martin et al., 2012). Martin et al. (2012) noted the nervous system is capable of permanent changes when exposed to long-term, repetitive stimulation. “Clinically, a significant number of individuals with ‘so-called’ complete SCI retain some connectivity across injury sites that could potentially provide a connection over the injured site” (Martin et al., 2012). Martin et al. (2012) noted, that SCI patients with complete or incomplete injury show proof of FES-induced muscle activation by performing a stepping response. Martin et al. (2012), noted patients with SCI treated with FES on a regular schedule experiences improved lower limb ASIA motor and sensory scores. They also experienced a decrease in spasticity of the lower extremities in response to stimulation.
“Because of cardiovascular conditioning with the FES following a SCI the study participants noted a 2-fold increase in the oxygen uptake, 5-beats per minute increase in heart rate, a 3-fold increase in ventilation rate, and peak oxygen uptake increased by 103%,” (Martin et al., 2012). Functional electrical stimulation studies show metabolic benefits including increased lean muscle mass, capillary
numbers, and a decrease in adipose tissue (Martin et al., 2012). According to Ho et al. (2014), improved muscle tone and bone density may prevent fewer life threatening complications (e.g., pressure injuries, infections, and bone fractures).
Unfortunately, studies related to FES use for SCI is limited to small, sample-size studies, leaving questions related to clinical indications and necessity (Martin et al., 2012). For example, a 2012 feasibility of home base FES lower extremity cycling consisted of one male subject 64 years old (Dolbow, Gorgey, Cifu, Moore, & Gater, 2012). The case report noted after nine weeks there were positive changes in the study related to body composition, quality of life and seat pressure provided support for the feasibility of home-based FES of lower extremity cycling. Mr. Martin (personal communication, July 5, 2017), from Restorative Therapies, noted that inpatient rehabilitation centers are using the FES systems to treat persons with SCI.
Upper Extremity Functional Restoration with FESIndividuals with a cervical (C5-C6) level SCI use neuroprosthesis, a device that supplements the input and output of the nervous system, in combination with FES to increase the function of the hands and arms. The primary purpose of the neuroprosthesis is to decrease the need for assistance by others, lessen the dependence on adaptive equipment, the possibility of eliminating braces or orthotic equipment, and time needed to perform tasks. Functional electrical stimulation provides coordination of grasp; thumb opening and closing, flexion and extension of the wrist, pronation of the forearm, and extension of the elbow. Implanted FES systems are utilized for long-term functional independence for individuals with cervical SCI (Ho et al., 2014).
Lower Extremity Restoration with FESThe ability to stand or step helps individuals perform ADLs and provides

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 5
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
them with mobility and independence. Conversely, the inability to stand or step limits an individual’s performance in many areas of their life including mobility, ADLs, and independence. When using the FES system, individuals with complete SCI at the thoracic level can experience stimulated contractions of the muscle in the lower extremity, promoting stepping and walking. The SCI patient has variable channels of continuous stimulation of the knee, hip, and trunk extensors that can power the sit-to-stand transition and support the body vertically to prevent against collapse (Ho et al., 2014 ).
Life Care Planning Implications for in-home FESThe two primary companies that supply the FES in-home systems: Restorative Therapies, located in Baltimore Maryland, and MotoMed, located in Germany. According to the Restorative Therapies representative, the company works with the discharging facility to maintain consistency when transitioning between inpatient and home therapies (B. Martin, personal communication, July 5, 2017). Mr. Martin reported (personal communication, July 5, 2017) that select insurance companies, including worker’s compensation, victims of violent crimes might pay for all or part of the cost. MotoMed was unavailable for information related to their pricing and products. Mr. Martin reported that there are various costs and replacement frequencies of the parts of the FES systems. Table 1 depicts such costs for the RT300 arm and leg systems.
Lower Extremity ExoskeletonLower extremity robotic exoskeleton technology developed for the lower extremities with the intention to provide people with SCI the ability to stand and walk. The increased physical demand of walking stimulates the cardiorespiratory system. Evidence suggests greater participation in exercise and physical activity may lessen the effects of SCI on long-term secondary health problems (Evans, Hartigan, Kandilakis, Pharo, & Clesson, 2015). Initially, SCI rehabilitation used body weight-supported treadmill exercise with lower extremity robotic exoskeleton technology to stimulate neuroplasticity using task specific, motor-patterned activities. Now robotic devices designed for over ground walking offer persons with SCI the opportunity to stand and walk at home or in the community. According to Evans et al. (2015), preliminary data suggests cardiorespiratory and metabolic demands of exoskeleton-assisted walking may deliver a stimulus to increase cardiorespiratory fitness. Louie, Eng, & Spinal Cord Injury Research Evidence (SCIRE), (2015) noted an unexpected relationship between age and gait speed. They noted the older participants achieved a faster gait speed versus the younger participants. Louie et al. (2015), wrote the possible reasons were the younger person with a SCI was due to trauma and the older person with a SCI was because of non-traumatic injuries. Currently, there is limited data on the long-term benefits of the lower extremity exoskeleton. Participants with SCI learn to use the lower
extremity exoskeleton in a minimum of 24 learning sessions (Kozlowski, Bryce, & Dijkers, 2015). Persons with SCI needed less ambulation assistance when they moved at higher exoskeleton speeds. (Yang, Asselin, Knezevic, Kornfeld, & Spungen, 2015).
Persons with SCI may have a permanent impairment, which makes walking, with or without conventional assistive devices challenging. Alternatives for an individual with SCI who does not have the needed strength in the muscles associated with the hips and knees to permit over ground walking including knee-ankle-foot orthoses (KAFOs), isocentric reciprocating gait orthoses, and other similar devices, classically used in combination with forearm crutches. Users of these devices face high-energy burdens and substantial stressors of the upper extremities. According to Kozlowski, Bryce, & Dijkers (2015), most abandon the use or decrease the frequency of the orthoses shortly after learning. Overall, the less support a participant needed, the quicker he or she accomplished exoskeleton achieved walking (Yang et al., 2015).
ConclusionSpinal cord injuries have diverse etiologies, which include trauma, vascular, infections, and environmental causes. They have an enormous cost to the individual and society with a poor response to current therapies. Current medical and surgical treatments focus on the alleviation of symptoms. Further constraints are the minimal endogenous ability of the brain and spinal cord for repair (Ess, 2013).
The primary goal of stem cell-based therapy for individuals with SCI is to
Table 1: Cost for the Restorative Therapies RT300 Arm and Leg System
Machine Machine CostMachine
ReplacementAxel Gaard brand replacement pads
Replacement cables
RT300 Arm and Leg
$15,000-$30,0000
Every 10-15 years $400-$600 per year$300 each replace as needed dependent on wear and tear

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 6
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
promote axonal regrowth above and below the injury site with regeneration and replacement of nerve cells. Mesenchymal cells are considered an ideal cell source for cell therapy of neurological lesions to facilitate lesion recovery through immunomodulatory and anti-inflammatory mechanisms. Clinics around the world are offering cell transplantation treatments for SCI, but
it is still in the beginning stages in the United States. Limited studies show the efficacy of stem cell transplantation on a large scale. Currently, the United States FDA restricts research related to the use of stem cell treatment for persons with spinal cord injuries, which adds to the challenge in establishing standards for treatment and reimbursement in the US.
Functional electrical stimulation is a method to aid in brain stimulation and repetition may increase neuroplasticity to “re-wire” the neuron pathways. Functional electrical stimulation is available for in-home use. There are few studies available related to the effectiveness of FES for persons with brain injuries.
REFERENCESArazpour, M. S. (2016). The influence of orthosis options on walking parameters in spinal cord-injured patients a literature review. Spinal Cord, 54, 412-422. doi: 10.1038/sc.2015.238
Buzhor, E., Leshansky, L., Barash, H., Warshawsky, D., Mazor, Y., & Shtrichman, R. (2014). Cell-based therapy approaches: the hope for incurable diseases. Regenerative medicine, 9(5), 649-672. doi:10.2217/rme.14.35
Diaz Quiroz, J. F., & Echeverri, K. (2013). Spinal cord regeneration: where fish, frogs and salamanders lead the way, can we follow? Biochemisty Journal, 415, 353-364. doi:10.1042/BJ20121807
Dolbow, D., Gorgey, A., Cifu, D., Moore, J., & Gater, D. (2012, February). Feasibility of home-based functional electrical stimulation cycling: Case report. Spinal Cord-Nature, 50(2), 170-171. doi:10.1038/sc.2011.115
Ess, K. C. (2013). Patient heal thyself: modeling and treating neurological disorders using patient-derived stem cells. Experimental Biology and Medicine (Maywood), 238(3): 308-314. doi:10.1177/1535370213480713
Evans, N., Hartigan, C., Kandilakis, C., Pharo, E., & Clesson, I. (2015). Acute cardiorespiratory and metabolic responses during exoskeleton-assisted walking overground among persons with chronic spinal cord injury. Top Spinal Cord Injury Rehabilation, 21(2), 122-132. doi:10.1310/sci2102-122
Goldschlager, T., Oehme, D., Ghosh, P., Zannettino, A., Rosenfeld, J. V., & Jenkin, G. (2013). Current and future applications for stem cell therapies in spin surgery. Current Stem Cell Research & Therapy, 8, 381-393.
Harrison, L. (2016, May 6). Stem Cell Therapy for Spinal Cord Injury: A Status Report. Retrieved July 5, 2017, from Medscape: http://www.medscape.com/viewarticle/862775
Ho, C. H., Triolo, R. J., Elias, L. A., Kilgore, K. L., DiMarco, A. F., Bogie, K., . . . Mushahwar, V. K. (2014 August). Functional electrical stimulation and spinal cord injury. Physical Medical & Rehabilitation Clinic of North America, 25(3), 631-661. doi:10.1016/j.pmr.2014.05.001
Kozlowski, A. J., Bryce, T. N., & Dijkers, M. P. (2015). Time and effort required by persons with spinal cord injury to learn to use a powered exoskeleton for assisted walking. Top Spinal Cord Injury Rehabilitation, 21(2), 110-121. doi:10.1310/sci2102-110
Li, J., & Lepski, G. (2013). Cell transplantation for spinal cord injury: A systemic review. BioMed Research International, 1-32. doi:10.1155/2013/786475
Louie, D. R., Eng, J. J., Lam, T., & Spinal Cord Injury Research Evidence (SCIRE) (2015). Gait speed using powered robotic exoskeletons after spinal cord injury: A systemic review and correlational study. Journal of NeuroEngineering and Rehabilitation, 12, 82. doi:10.1186/s12984-015-0074-9
Martin, R., Sadowsky, C., Obst, K., Meyer, B., & McDonald, J. (2012). Functional electrical stimulation in spinal cord injury: from theory to practice. Top Spinal Cord Injury Rehabilitation, 18(1), 28-33. doi: 10.1310/sci1801-28
Medical Definition of Neuroplasticity (1997-2017). MedicineNet.com. Retrieved from: http://www.medicinenet.com/script/main/art.asp?articlekey=40362
Yang, A., Asselin, P., Knezevic, S., Kornfeld, S., & Spungen, A. (2015). Assessment of in-hospital walking velocity and levels of assistance in a powered exoskeleton in persons with spinal cord injury. Top Spinal Cord Injury Rehabilitation, 21(2),
100-109. doi:10.1310/sci2102-100
ERIN T. OCONNELL, MSN, MBA, RN-BC, CNL, CNLCP® Erin OConnell has had over a decade of clinical nursing experience in a multitude of nursing areas including the ICU, telemetry, emergency, long-term care, rehabilitation, and same day/PACU. Her career has afforded her a diverse set of experiences. It has also deepened her appreciation for the field as a whole. She currently works as the Clinical Nurse Leader in the long-term care setting. She is compelled to continuously learn and stay involved. She currently serves on the AANLCP’s research committee, whose goal is to enrich resources for Nurse Life Care Planners. She is also Webinar Committee Chair of the AALNC West Virginia Upper Ohio Valley Chapter. In her free time, she enjoys hiking, backpacking, biking, kayaking, downhill skiing and cross country skiing. She recently moved to Seattle and is loving every minute.

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 7
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 8
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
IntroductionLong-term pain management is a growing patient need. Because the extent and duration of pain management can often span a patient’s person’s lifetime, it is important for life care planners to understand the impact of treatment expense for inclusion in case evaluation. Many pain specialists rely on traditional methods of treatment, such as medication, injections, and therapies, but the use of new or emerging options are becoming more common. Platelet-rich plasma (PRP) therapy is a procedure that is gaining popularity. As the use of PRP grows, so does the need to better understand the treatment and its place in the work of life care planners.
Although platelet-rich plasma therapy may be growing in popularity, controversy plagues its use. Platelet-rich-plasma is considered by many to be an emerging pain management
therapy without widely accepted indicators of effectiveness. This has led to access and payment complications for patients, health care providers, and billing professionals. Understanding the fundamentals of PRP, application techniques, patient benefits, and treatment billing is important for nurse life care planners evaluating cases involving PRP.
What is PRP? For more than three decades, medical professionals have used PRP as a recovery agent following dental, orthopedic, and surgical procedures. Recently, it has expanded into many other fields of medicine in the quest for improved healing. Studies have shown PRP therapy to be effective for the treatment of tendinopathy, chronic tendon and muscle injury, and joint degeneration (Filardo et al., 2015; Fitzpatrick, Bulsara, & Zheng, 2016; Mishra, Woodall & Vieira, 2009). However,
the efficacy of its application continues to be a subject of debate.
Proponents of the treatment maintain PRP capitalizes on the body’s innate ability to cure itself. These advocates claim that employing a patient’s organic matter – with the added benefit of low rejection risk – to stimulate natural, restorative healing should not be considered unconventional. Critics of the treatment attribute patient success stories to a placebo effect and view PRP as a marketing ploy and a means to influence unwitting patients. Although ongoing research studies evaluating PRP therapy may settle the efficacy debate in the future, the therapy has garnered enough support to make it a viable option for patients.
Medical professionals derive PRP from a predetermined measure of the patient’s blood, which is then put through a process of centrifugation to generate a natural concentrate of autologous
PLATELET-RICH-PLASMA: LIFE CARE PLANNING CONSIDERATIONS
DAWN COOK, RN, LNCP-C, CLCP, CLNC

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 2 9
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
growth factors. From the platelet’s alpha granules, bioactive cytokines and proteins stimulate chemotaxis, cellular migration, proliferation, differentiation, and extracellular matrix production (Lyras et al., 2011). Additionally, these proteins promote the release of angiogenic growth factors contributing to tissue regeneration and healing (Alsousou, Thompson, Hulley, Noble, & Willett, 2009; Anitua et al., 2007). The main growth factors present in PRP are platelet-derived growth factor (PDGF), transforming growth factor β (TGF β), insulin-like growth factor (IGF-1), and fibroblast growth factor (FGF) (Wu et al., 2011). Clinically, PRP is an autologous blood product that can be non-invasively injected into an affected area of the body to activate healing through the delivery of PDGF.
Types of patients who benefit A number of professional athletes have undergone PRP therapy to treat sports injuries, raising the profile of the procedure. Los Angeles Dodgers’ pitcher Takashi Saito received PRP injections to heal an elbow injury prior to the 2008 major league baseball playoffs (Storrs, 2009). In the following year, professional national football league players Hines Ward and Troy Polamalu used PRP therapy for different ailments before their SuperBowl XLIII win (Storrs, 2009). Tiger Woods underwent post-surgery PRP injection therapy for his knee before participating in the 2009 PGA season (Storrs, 2009). Although the therapy had been around long before as part of regimens to treat various problems such as sprains and chronic tendon injuries, these professional athletes increased publicity for PRP as an effective treatment for sports-related injuries. Many athletes reported claims of a quick recovery and return to competition shortly after PRP therapy.
The results for athletes and non-athletes alike can vary due to factors such as overall patient health, the area of the body impacted, and whether the injury is chronic (long-term) or acute (short-term, yet severe) (Kelly, 2011).
Individuals with conditions affected by hypoxia – poor blood supply or low oxygen content – such as tendon and ligament tears, cartilage injuries, bone injuries, and even arthritis, often benefit the most from PRP treatment. This is because PRP helps create and improve blood flow in these hypoxic areas, subsequently prompting the body to improve stem cell supply – the body’s natural repair cells – to the injury (Institute of Regenerative Medicine, n.d., para. 2).
In some cases, PRP therapy has reduced or negated the need for medication or surgery. Specifically, recent studies report compelling evidence of PRP therapy demonstrating more effective results than hyaluronic acid for knee osteoarthritis and hip osteoarthritis (Laudy, Bakker, Rekers, & Moen, 2015; Dallari et al., 2016). Also, for tennis elbow sufferers, studies have shown PRP to outperform local steroids for lasting pain relief (Mundla, Venkataramana, Koduru, & Ravindran, 2017).
ProcedurePreparation and Injection As an outpatient procedure, PRP is administered by injection at the site of pain. As with the administration of any therapy, evaluation and diagnostic workup should occur. Since PRP originates from the patient’s blood, there is a low risk of reaction. However, patients must still be made aware of potential complications, such as infection, bleeding, nerve damage, pain, or lack of desired result (International Cellular Medicine Society, 2011). As part of a surgical procedure, PRP injection may be integrated at the conclusion of an operation, or be a part of the follow-up regimen as prescribed by the physician. Whether performed as an inpatient or outpatient therapy for pain management, PRP is generally considered an elective treatment. Nevertheless, medical personnel are expected to follow standard practices and procedures when administering the treatment.
A dose of PRP originates from a small amount of the patient’s blood, usually
60 ml.. The drawn blood is placed in a specialized processing unit and spun at high speed to separate platelets from other blood cells. The extracted concentrate of platelets is then injected around or near the area of injury being treated. A physician or technician may use x-ray or ultrasound to guide placement of the injection.
Once injected, growth factors are released, triggering an inflammatory response lasting around three days (Kumar, 2005). The proliferative phase of healing may last several weeks, followed by a remodeling phase that leads to the formation and stabilization of mature tissue in approximately six months’ time (Tate & Crane, 2010). The patient may experience mild pain or irritation at the application site for few days after the injection. Use of NSAIDs is discouraged until the patient heals, becomes pain-free, has achieved full function, or shows evidence of a plateau (International Cellular Medicine Society, 2011).
In some cases, a physician may request a patient limit weight-bearing activity or motion immediately after receiving the injection. Commonly, health care providers recommend the use of a cast, boot, or brace during the early, post-injection period. Patients may gradually return to regular physical activities up to one week after the injection. Return to full activity depends on how the body responds to the therapy and the recommendation of the physician.
1) Impaired physical mobility (Domain 4, Activity/Rest, Class 2, Activity/Exercise)
2) Dressing self-care deficit (Domain 4, Activity/Rest, Class 5, Self-Care)
3) Impaired comfort (Domain 12, Comfort, Class 1, physical comfort)
4) Chronic pain (Domain 12, Comfort, Class 1, Physical Comfort
Nursing Diagnoses To Consider

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 3 0
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Frequency of treatmentBased on the type of injury and a patient’s documented initial response to the treatment, the physician may recommend additional injections. For treatments administered in a series, the number of injections typically ranges from three to five. The progress of the affected area typically determines the number of injections. However, if no improvement in symptoms is observed after the first or second treatment, multiple injections are often not recommended.
Case study: PRP Treatment for CRPSJohn Doe is a patient that suffers from Complex Regional Pain Syndrome (CRPS). Often called Reflex Sympathetic Dystrophy (RSD), CRPS describes a condition of chronic pain often affecting a post-injury extremity. Prolonged or excessive pain characterizes the condition along with any combination of the following: changes in skin color, temperature, and swelling in the affected area (National Institute of Neurological Disorders and Stroke, n.d., para. 1).
Clinical management can be challenging in CRPS cases. In instances involving a lower extremity, allodynia frequently minimizes the patient’s ability bear weight. Adaptive aids to ambulate may inadvertently reduce mobility and further contribute to worsening symptoms (Schwartz, 2015). Many patients manage the pain associated with CRPS with oral medications, sympathetic block intervention, restorative therapy, and other supportive methods (Lee & Cohen, 2008).
Mr. Doe was diagnosed with CRPS following surgery and therapy after an accident. Despite his post-operative pain, he was able to function normally with his symptoms controlled by various medical treatments. However, as time went on, the suffering became much more difficult to control. Over time, a progressive worsening of symptoms led to a perpetual cycle of medical provider
visits and traditional treatments for chronic pain.
When visiting his pain management specialist, Mr. Doe presented with severe pain in his lower back with lower extremity radiation of symptoms accompanied by equally severe ankle pain. A prior intra-articular injection in the ankle had given him immediate relief, but that recovery was short-lived, and the symptoms returned. His pain management specialist listed impressions of traumatic arthropathy in the ankle, lumbar radiculopathy, and low back pain consistent with degenerative disc disease (DDD) and prescribed Voltaren gel for temporary treatment.
Eventually, results of an MRI of the lumbar spine with flexion and extension led to a series of selective nerve root blocks (SNRBs) to his lowest spinal segments with transforaminal placement of epidural corticosteroid. The SNRBs initially provided significant relief of his lower back and lower extremity symptoms. He underwent a course of physical therapy followed by adjustments to the low back, thoracic spine, and foot with a chiropractor. The chiropractic adjustments helped somewhat but the pain reoccurred.
Following a series of lumbar sympathetic plexus blocks added to SNRBs, Mr. Doe’s doctor presented the option of platelet-rich plasma injections. Mr. Doe’s condition had deteriorated considerably, necessitating the use of a cane or walker to stay mobile and minimize the pain caused by bearing weight or pressure on his hypersensitive areas. With some skepticism, Mr. Doe decided to undergo PRP injection treatment.
Upon receiving his first PRP treatment, Mr. Doe was astounded by the results. He was able to walk without his walker or cane and reported no back or leg pain and very little ankle pain. Several weeks later, he received another series of PRP injections as well as platelet rich plasma inhalation therapy. Mr. Doe reported that, with regular intervals of PRP injection treatment, he was able
to walk, stop taking pain medications temporarily, and even saw improvement in lesion flare-ups from CRPS. Historical use of opioids in his treatment was mostly ineffective, and the PRP injections were the only therapy that brought him relief lasting anywhere from four to six months. Most of his healthcare providers recommended that he continue PRP injection therapy with his pain management specialist for lifetime treatment in mitigating his pain, necessitating the inclusion of the treatment in the regimen outlined in his future medical costs report.
Navigating Billing Codes In addition to the controversy surrounding the use of PRP in medical field, there are also PRP-related billing debates. Understanding applicable standards and their variations can be particularly useful in code and cost research when creating a life care plan for a patient who has undergone or is a potential candidate for PRP treatment.
Compliance and medical coding experts outline multiple scenarios that observe different PRP coding approaches (TCI Supercoder, 2009). The first example involves orthopedic surgery followed by blood draw, centrifuge to prepare the PRP, and then site injection. Because the procedure involves multiple steps, it is logical to assume that the injection would be coded separately. However, most resources instruct otherwise and dictate that the platelet injection should be considered part of the surgery.
A second example handles the billing of PRP differently. It involves a case of epicondylitis treated with a PRP injection. In this instance, the blood draw and processing of platelets are coded as a separate procedure (86999, Unlisted transfusion medicine procedure) in addition to the injection code. While these particular examples illustrate references that may be considered acceptable alternatives, it is important to consult insurance or payer standards and guidelines (TCI Super Coder, 2009).

A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 3 1
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Examples of commonly misused codes used in billing for PRP therapy: n 36513 (Therapeutic apheresis; for
platelets)
n 86985 (Splitting of blood or blood products, each unit)
n 20926 (Tissue grafts, other [e.g., paratenon, fat, dermis])
n 20552 (Injection[s]; single or multiple trigger points[s], 1 or 2 muscle[s])
n 20610 (Arthrocentesis, aspiration and/or injection; major joint or bursa [e.g., shoulder, hip, knee joint, subacromial bursa])
n 36514 (Therapeutic apheresis; for plasma pheresis)
n 38230 (Bone marrow harvesting for transplantation).
Navigating billing codes related to PRP is getting easier. In July of 2010, the American Medical Association (AMA) introduced the code 0232T for Platelet-rich Plasma Injection in its Current Procedural Terminology (CPT®) catalog (Twetten, 2010). The code is listed as Category III in the CPT® catalog because it “represent[s] services considered to be emerging technologies within healthcare” (AMA, 2010). The code is used for PRP injection treatment administered in-office. The code bundles together all aspects of the procedure, including
image guidance (such as x-ray or ultrasound), blood draw, harvest and preparation of platelet rich plasma, and the injection itself. Whether the patient is sponsored by insurance or paying directly out of pocket, the AMA recommends using code 0232T (AMA, 2010). Although there are individual codes for the procedural components of the treatment, those separate codes should not be used for PRP treatments administered in-office.
Although the AMA standardized a code for PRP injection, its use is not always consistent. Life care planners must still be cautious when evaluating or determining medical costs associated with PRP. Category III code classifications may be rejected by certain payer policies because they do not support experimental or investigational procedures. As a result, component CPT and Healthcare Common Procedure Coding System (HCPCS) codes might be used to convey PRP treatment. A novice biller without knowledge or experience in the PRP coding procedure might also use component CPT and HCPCS codes in error. Life care planners should seek the expertise of practiced coders using credible, standardized resources to determine the proper codes and their usage. The use of excess codes
or promoting the use of codes that infer associations to PRP may lead to problems such as payment denial or even the discredit of cost research in reports such as a life care plan or reasonableness of medical bills assessment.
ConclusionAs platelet-rich plasma therapy becomes more prevalent for the treatment of pain management, life care planners need to be aware of the complexities surrounding the treatment, and the coding for billing associated with the treatment. Because PRP is considered to be a controversial treatment, understanding the debate surrounding the procedure can provide important insight and context. The ability to defend its value may be necessary when establishing a life care plan for a client. Life care planners educated on the benefits and the value the treatment are at an advantage when reviewing cases involving PRP. Just as important is the need to understand the billing codes associated with the treatment, which can aid in defending cost analysis and projection. The quality-of-life benefit to the patient receiving PRP is an important consideration when supporting the inclusion of this pain treatment in a life care plan.
REFERENCESAlsousou, J., Thompson, M., Hulley, P., Noble, A., & Willett, K. (2009). The biology of platelet-rich plasma and its application in trauma and orthopaedic surgery. The Journal of Bone and Joint Surgery, 8, 987–996. doi: 10.1302/0301-620X.91B8.22546.
American Medical Association. (2010). CPT® Category III Codes: The First Ten Years. https://www.ama-assn.org/practice-management/cpt-category-iii-codes.
Anitua, E., Sanchez, M., Nurden, A.T., Zalduendo, M. M., de la Fuente, M., Azofra, J., & Andia, I. (2007). Platelet-released growth factors enhance the secretion of hyaluronic acid and induce hepatocyte growth factor production by synovial fibroblasts from arthritic patients. Rheumatology, 46, 1769–1772. doi: 10.1093/rheumatology/kem234.
Dallari, D., Stagni, C., Rani, N., Sabbioni, G., Pelotti, P. Torricelli, P….Giavaresi, G. (2016). . Ultrasound-guided injection of platelet-rich plasma and hyaluronic acid, separately and in combination, for hip osteoarthritis a randomized controlled study. American Journal of Sports Medicine, 44(3), 664-671. doi: 10.1177/0363546515620383.
Filardo, G., Kon, E., Roffi, A.,Di Matteo, B., Merli, M. L., & Maracacci, M. (2015). Platelet-rich plasma: Why intra-articular? A systematic review of preclinical studies and clinical evidence on PRP for joint degeneration. Knee Surgery, Sports Traumatology, Arthroscopy, 23(9), 2459-2474. doi:10.1007/s00167-013-2743-1
Fitzpatrick, J., Bulsara, M., & Zheng, M. H. (2016). The effectiveness of platelet-rich plasma in the treatment of tendinopathy a meta-analysis of randomized controlled clinical trials. American Journal of Sports Medicine, 45 (1), 226-23. doi:10.1177/0363546516643716
Institute of Regenerative Medicine. (n.d.). Stem Cell Therapy. Retrieved from http://stemcellorthopedic.com/treatments/
International Cellular Medicine Society. (2011). Section 10: Guidelines for the use of platelet rich plasma. . Retrieved from http://www.cellmedicinesociety.org/icms-guidelines/guidelines
Kelly, F. B. (2011). Platelet-rich plasma. Retrieved from http://orthoinfo.aaos.org/topic.cfm?topic=A00648
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 3 2
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Kumar, V. (2005). Inflammation and repair. In V. Kumar, A. K. Abbas, & A. Fausto (Eds.) Robbins and Cotran pathologic basis of disease (7th ed. pp.75-94). Philadelphia, Pennsylvania: Elsevier Saunders Publisher.
Laudy, A. B, Bakker, E. W., Rekers, M., & Moen, M.N. (2015). Efficacy of platelet-rich plasma injections in osteoarthritis of the knee: a systematic review and meta-analysis. British Journal of Sports Medicine, 49(10), 657-672. doi: 10.1136/bjsports-2014-094036
Lee, M., & Cohen, J. (Eds). (2008). Rehabilitation medicine and thermography. Wilsonville, Oregon: Impress Publications.
Lyras, D. N., Kazako, K., Georgiadis, G., Mazis, G., Middleton R., Richards, S., … Agrogiannis, G. (2011). Does a single application of PRP alter the expression of IGF-I in the early phase of tendon healing? Journal of Foot Ankle Surgery, 50,276–282. doi: 10.1053/j.jfas.2011.02.010.
Mishra, A., Woodall, J., & Vieira, A. (2009). Treatment of tendon and muscle using platelet-rich plasma. Clinics in Sports Medicine, 28(1), 113-125. https:doi.org/10.1016/j.csm.2008.08.007
Mundla, G., Venkataramana, P., Koduru, M., & Ravindran, B. (2017). Study comparing the efficacy of platelet rich plasma versus steroid versus placebo in lateral epicondylitis. Retrieved from http://www.ijoro.org/index.php/ijoro/article/view/276
National Institute of Neurological Disorders and Stroke. (n.d.). Complex regional pain syndrome fact sheet. Retrieved from https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Complex-Regional-Pain-Syndrome-Fact-Sheet
Schwartz, R.G. (2015). Stem cells for the treatment of complex regional pain syndrome (CRPS)/reflex sympathetic dystrophy (RSD): A case study. Pan American Journal of Medical Thermology, 1(2), 89-92. doi.org/10.18073/2358-4696/pajmt.v1n2p89-92
Storrs, C. (2009). Is platelet-rich plasma an effective healing therapy. Scientific American. Retrieved from https://www.scientificamerican.com/article/platelet-rich-plasma-therapy-dennis-cardone-sports-medicine-injury/
Tate, K.S., & Crane, D. (2010). Platelet rich plasma grafts in musculoskeletal medicine. Journal of Prolotherapy, 2(2),371-376. Retrieved from http://journalofprolotherapy.com/table-of-contents-of-volume-2-issue-2-may-2010/
TCI Super Coder (2009). On the cutting edge: Pull the plug on PRP denials by limiting when you pick 86999 for PRP injections [blog]. Retrieved from https://www.supercoder.com/my-ask-an-expert/topic/platelet-rich-plasma-prp-injections
Twetten, M. (2010). PRP gets CPT category III code. Retrieved from http://www.aaos.org/AAOSNow/2010/Aug/managing/managing9/?ssopc=1
Wu, C. C., Chen, W. H., Zao, B., Lai, P. L., Lin, T. C., Lo, H. Y., ... Deng, W. P. (2011). Regenerative potentials of platelet-rich plasma enhanced by collagen in retrieving pro-inflammatory cytokine-inhibited chondrogenesis. Biomaterials,
32(25), 5847-5854. doi:10.1016/j.biomaterials.2011.05.002
DAWN COOK, RN, LNCP-C, CLCP, CLNCDawn Cook has been a life care planner since 2012 and has completed over 250 expert reports, and has qualified to testify in Nevada, California, New Mexico and at Federal Court. Dawn has been a Registered Nurse since 1979 when she graduated as the Valedictorian of her Nursing class in Victoria, British Columbia. She has worked in Home Care and Acute Hospital facilities for over 30 years. Dawn is certified as a Lifetime Nurse Care Planner, Certified Nurse Life Care Planner and Certified Life Care Planner. Dawn developed a special interest in platelet rich plasma (PRP) therapy because she has seen the benefits for pain reduction and healing for injured knees when she worked at a hospital at a California ski resort and as a life care planner with patients receiving PRP for pain. Dawn has been a speaker at the American Association of Legal Nurse Consultants, the Executive Forum of Nurse Life Care Planners, the Society of Pain Management Nursing, the American Association of Nurse Life Care Planners, the International Symposium of Life Care Planners and the International Transplant Nurse Society.
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 3 3
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
Candidates must meet the following eligibility criteria per the application deadline as indicated in the CNLCP®
Handbook for Candidates and on the Website: http://cnlcp.org/certification-by-examination/
NURSE LIFE CARE PLANNING CERTIFICATION
Sed justo.
Value of CNLCP® Certification
As healthcare has become more complex, it is increasingly vital to assure the public that healthcare professionals are competent. Individual State Registered Nurse (RN) licensure measures entry-level competence only; and, in so doing, provides the legal authority for an individual to practice nursing. It is the minimum professional practice standard.
Certification, on the other hand, is a formal recognition that validates knowledge, experience, skills and clinical judgment within a specific nursing specialty; and, as such, is reflective of a more stringent professional practice standard. It affirms achievement of proficiency beyond basic licensure.
The Certified Nurse Life Care Planner (CNLCP®) Certification Board is a separately incorporated entity that facilitates consumer health and safety through credentialing/certification of nurse life care planners. It ensures that their practice is consistent with established standards of excellence in the development and defense of the life care planning document.
Similar to consumers knowing to seek out certification status within other professions (e.g., dentists, pharmacists), certification within the field of nurse life care planning has become an important indicator that a certified nurse not only holds state licensure to practice nursing, but is qualified, competent and has met rigorous requirements in the achievement of the CNLCP®
credential.
The policies and procedures used by the CNLCP® Certification Board to construct and review items and examination forms for the CNLCP® examination are consistent with guidelines recommended by the American Educational Research Association, the American Psychological Association, and the National Council on Measurement in Education (AERA, APA, NCME; 2014) as well as other industry standards such as: Standards for the Accreditation of Certification Programs (National Commission for Certifying Agencies, 2014) and Conformity assessment — General requirements for bodies operating certification of persons (ISO/IEC 17024).
AANLCP® supports certification through the CNLCP® Certification Board.
CNLCP® is a registered trademark of the CNLCP® Certification Board.
CNLCP® HANDBOOK FOR CANDIDATES & APPLICATION CANDIDATES
CERTIFICATION BY EXAM
Application: http://ptcny.com/pdf/cnlcp.pdf
CNLCP® Handbook for Candidates: http://www.ptcny.com/PDF/CNLCP.pdf
_________________________
AANLCP® Member Discounts _________________________
FOR MORE INFORMATION PLEASE VISIT
WWW.CNLCP.ORG
OR CONTACT:
Jan Roughan, Chairperson
Phone: 626-303-6333 Ext. 216
A A N L C P J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G I S S N 1 9 4 2 - 4 4 6 9 3 4
FALL 2017 PEER-REVIEWED EXCELLENCE IN L IFE CARE PL ANNING SINCE 2006 VOL. XVI I NO. 3
2012XII.1 Coding and CostingXII.2 Electrical Stimulation TechnologyXII.3 Preconference / Brain InjuryXII.4 Veterans Administration
2013XIII.1 LCP for Motor and Developmental
DisordersXIII.2 Ethical Topics in LCPXIII.3 Preconference / Exemplars in NLCPXIII.4 Home Modifications
2014XIV.1 Technology UpdatesXIV.2 LCP Across All AgesXIV.3 Psych topics in LCPXIV.4 LCP and the ACA
2015 XV.1 Topics in TransplantationXV.2 Updates in Spinal Cord InjuryXV.3 BurnsXV.4 Perinatal / Childhood
2016XVI.1 PainXVI.2 GI issuesXVI.3 International LCPXVI.4 Home Care
2017XVII.1 Brain InjuryXVII.2 The Business of Life Care Planning XVII.3 Back and Spine
ISSUE INDEX
J O U R N A L O F N U R S E L I F E C A R E P L A N N I N G
P E E R - R E V I E W E D E X C E L L E N C E I N L I F E C A R E P L A N N I N G S I N C E 1 9 9 8
LCP and
the
ACA
Winter 2014 vol. XIV, no. 4
Spring 2015 vol. XV, no.1
Topics in Transplantation
P E E R - R E V I E W E D E X C E L L E N C E I N L I F E C A R E P L A N N I N G S I N C E 1 9 9 8
Spring 2014 vol. XIV, no.2
Life care
Summer 2015 vol. XV, no.2
Updates in Spinal Cord Injury
®