journal of alzheimer’s disease 59 (2017) 815–849 doi 10 ... · panza, md, phd, geriatric unit...
TRANSCRIPT
Journal of Alzheimer’s Disease 59 (2017) 815–849DOI 10.3233/JAD-170248IOS Press
815
Relationships of Dietary Patterns,Foods, and Micro- and Macronutrientswith Alzheimer’s Disease and Late-LifeCognitive Disorders: A Systematic Review
Vincenzo Solfrizzia,1,∗, Carlo Custoderoa, Madia Lozuponeb, Bruno P. Imbimboc,Vincenzo Valiania, Pasquale Agostia, Andrea Schilardia, Alessia D’Intronoa,Maddalena La Montagnad, Mariapaola Calvanib, Vito Guerrae, Rodolfo Sardonee,Daniela I. Abbresciae, Antonello Bellomod, Antonio Grecof , Antonio Danieleg,Davide Seripaf , Giancarlo Logroscinob,h, Carlo Sabbaa
and Francesco Panzab,f,h,1,∗aGeriatric Medicine-Memory Unit and Rare Disease Centre, University of Bari Aldo Moro, Bari, ItalybNeurodegenerative Disease Unit, Department of Basic Medicine, Neuroscience, and Sense Organs,University of Bari Aldo Moro, Bari, ItalycDepartment of Research and Development, Chiesi Farmaceutici, Parma, ItalydDepartment of Clinical and Experimental Medicine, Psychiatric Unit, University of Foggia, Foggia, ItalyeNational Institute for Digestive Diseases, IRCCS “Saverio de Bellis”, Castellana, Bari, Italyf Geriatric Unit and Laboratory of Gerontology and Geriatrics, Department of Medical Sciences,IRCCS “Casa Sollievo della Sofferenza”, San Giovanni Rotondo, Foggia, ItalygInstitute of Neurology, Catholic University of Sacred Heart, Rome, ItalyhDepartment of Clinical Research in Neurology, University of Bari Aldo Moro, “Pia FondazioneCardinale G. Panico”, Tricase, Lecce, Italy
Accepted 23 May 2017
Abstract. In the last decade, the association between diet and cognitive function or dementia has been largely investigated. Inthe present article, we systematically reviewed observational studies published in the last three years (2014–2016) on the rela-tionship among dietary factors and late-life cognitive disorders at different levels of investigation (i.e., dietary patterns, foodsand food-groups, and dietary micro- and macronutrients), and possible underlying mechanisms of the proposed associations.From the reviewed evidence, the National Institute on Aging–Alzheimer’s Association guidelines for Alzheimer’s disease(AD) and cognitive decline due to AD pathology introduced some evidence suggesting a direct relation between diet andchanges in the brain structure and activity. There was also accumulating evidence that combinations of foods and nutrientsinto certain patterns may act synergistically to provide stronger health effects than those conferred by their individual dietarycomponents. In particular, higher adherence to a Mediterranean-type diet was associated with decreased cognitive decline.
1These authors contributed equally to this work.∗Correspondence to: Vincenzo Solfrizzi, MD, PhD, Depart-
ment of Geriatric Medicine, Memory Unit and Rare DiseaseCenter, University of Bari Aldo Moro - Policlinico, Piazza GiulioCesare, 11, 70124 Bari, Italy. Tel.: +39 080 5473685; Fax: +39080 5478633; E-mails: [email protected] and FrancescoPanza, MD, PhD, Geriatric Unit and Laboratory of Gerontology
and Geriatrics, Department of Medical Sciences, IRCCS “CasaSollievo della Sofferenza”, San Giovanni Rotondo, Foggia,Italy, and Neurodegenerative Disease Unit, Department of BasicMedicine, Neuroscience, and Sense Organs, University of Bari“Aldo Moro”, Bari, Italy. Tel./Fax: +39 0882 410271; E-mails:[email protected], f [email protected]
ISSN 1387-2877/17/$35.00 © 2017 – IOS Press and the authors. All rights reserved

816 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
Moreover, also other emerging healthy dietary patterns such as the Dietary Approach to Stop Hypertension (DASH) andthe Mediterranean-DASH diet Intervention for Neurodegenerative Delay (MIND) diets were associated with slower ratesof cognitive decline and significant reduction of AD rate. Furthermore, some foods or food groups traditionally consideredharmful such as eggs and red meat have been partially rehabilitated, while there is still a negative correlation of cognitivefunctions with saturated fatty acids and a protective effect against cognitive decline of elevated fish consumption, high intakeof monounsaturated fatty acids and polyunsaturated fatty acids (PUFA), particularly n-3 PUFA.
Keywords: Alzheimer’s disease, dementia, dietary pattern, food groups, foods, healthy diet, Mediterranean diet, macronutri-ents, micronutrients, mild cognitive impairment
INTRODUCTION
Alzheimer’s disease (AD) is the most commonform of dementia. Over 5.4 million people are esti-mated to be affected in the Unites States [1]. In thelast 20 years, most of the therapeutic approaches weredirected against the production and accumulation ofamyloid-� (A�), one of the neuropathological hall-marks of AD, and, up to now, have failed to showclinical efficacy [2].
Currently, available drugs for the treatment ofAD have only symptomatic effects [2], and thereis an unmet need of preventing AD onset anddelaying or slowing disease progression from mildcognitive impairment (MCI) in the absence ofdisease-modifying therapies. Therefore, at present,the management of potential risk factors is believedto be the most effective way of preventing dementia,AD, and MCI. In the last decade, one of the mostintriguing and appealing links hypothesized was theassociation between lifestyle factors such as diet anddietary habits and the occurrence of AD and dementia[3–7]. Dietary factors may affect the risk of cardio-vascular disease (CVD), also influencing the risk ofAD and dementia [8–10]. A growing body of evi-dence suggests that certain diets are associated witha lower incidence of AD, so maintaining a healthydiet may have an impact on many of these possiblerisk factors for cognitive decline, and the model tofollow seems to be the Mediterranean diet (MeDi)[4, 9]. Therefore, elevated dietary monounsaturatedfatty acids (MUFA) and n-3 polyunsaturated fattyacids (n-3 PUFA) and high fish consumption [10, 11],alongside high levels of antioxidants from fruit andvegetables [12, 13], and moderate alcohol and coffeeconsumption [14–16] may have a beneficial effecton the risk of dementia. Nonetheless, diet should beconsidered as a “whole”, consisting of a complexof nutritional principles, foods, micronutrients andmacronutrients interacting with each other. In fact,the combinations of foods and nutrients into certain
patterns may act synergistically to provide strongerhealth effects than those conferred by their individualdietary components. This hypothesis has addressedthe interest in the role of dietary patterns rather thanof the individual components of the diet against CVD,neurodegenerative diseases, and all-cause mortality[17, 18]. Some recent systematic reviews and meta-analyses of pooled studies on this issue found that ahigher adherence to the MeDi was associated with areduced risk of cognitive impairment, MCI and AD,as well as the transition from MCI to AD [19–22].However, in the last few years, some changes haveemerged in approaching the relationship between dietand cognitive impairment. In fact, the National Insti-tute on Aging–Alzheimer’s Association (NIA-AA)guidelines for AD and cognitive decline due to ADpathology [23] introduced some evidence suggest-ing a direct relation between diet and changes in thebrain structure and activity, opening the era of brainimaging biomarkers in nutritional epidemiology. Theaim of the present systematic review article was toshed light on the relationship among dietary patterns,foods, food groups, micro-, and macronutrients andlate-life cognitive disorders considering the resultsof observational studies published in the last threeyears (2014–2016), as well as possible underlyingmechanisms of the proposed associations.
METHODS
In the present systematic review article, we fol-lowed the Preferred Reporting Items for Systematicreviews and Meta-Analyses (PRISMA) guidelines,adhering to the PRISMA 27-item checklist [24].This systematic review was based upon searches ofUS National Library of Medicine (PubMed), OvidMEDLINE, EMBASE, Google Scholar, Web of Sci-ence, and Scopus databases, picking the followingterms to identify the risk exposure (dietary patternsOR foods OR food groups OR micronutrients ORmacronutrients) combined with terms to determine

V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 817
the outcomes of interest [cognitive AND (impair-ment OR decline OR disorders) OR cognition ORAlzheimer’s disease OR dementia OR mild cognitiveimpairment OR vascular dementia]. There were nolanguage restrictions on the search. To be includedin this systematic review, studies were limited toobservational studies (including both cross-sectionaland longitudinal population-based studies) publishedbetween January 1, 2014 and December 31, 2016. Wechoose these time limits on the basis of a pre-searchwithout time limits that included a very high num-ber of identified articles to review (36104 articles).Studies were further required to meet the followinginclusion criteria: (1) studies conducted in humansaged 45 years or older; (2) studies that provideda description of the tools used for collecting theadherence to the different dietary patterns and theintake of foods, food groups, micro- and macronutri-ents (e.g., validated semi-quantitative food frequencyquestionnaires, 7-day dietary records, or 24-h dietaryrecall) or that evaluated nutrient consumption fromthe values of biochemical markers (e.g., serum con-centration or red blood cells levels); (3) studiesassessing cognitive functions according to the diag-nostic criteria for the diagnoses of MCI [Petersencriteria and their revision/modifications, Interna-tional Working Group on Mild Cognitive Impairmentcriteria, European Alzheimer’s Disease Consortium(EADC) criteria, NIA-AA criteria for MCI due toAD, and DSM-5 criteria for Mild NeurocognitiveDisorder), AD [National Institute of Neurologicaland Communicative Disorders and Stroke and theAlzheimer’s Disease and Related Disorders Associ-ation (NINCDS-ADRDA) criteria, NIA-AA criteriafor dementia due to AD, International Working Group(IWG)-1 criteria for AD, and IWG-2 criteria forAD], vascular dementia (VaD) (NINCDS-AIREN),unspecified dementia [Diagnostic and StatisticalManual for Mental Disorders (DSM)-III-R criteria,DSM-IV criteria, DSM-IV-TR criteria, DSM-5 crite-ria for Major Neurocognitive Disorder, InternationalClassification of Diseases (ICD), 9th Revision, Clin-ical Modification (CM), and ICD-10-CM] or thatprovided the neuropsychological tools used for defin-ing late-life cognitive impairment/decline also innon-demented older subjects. The studies includedhad to present original data.
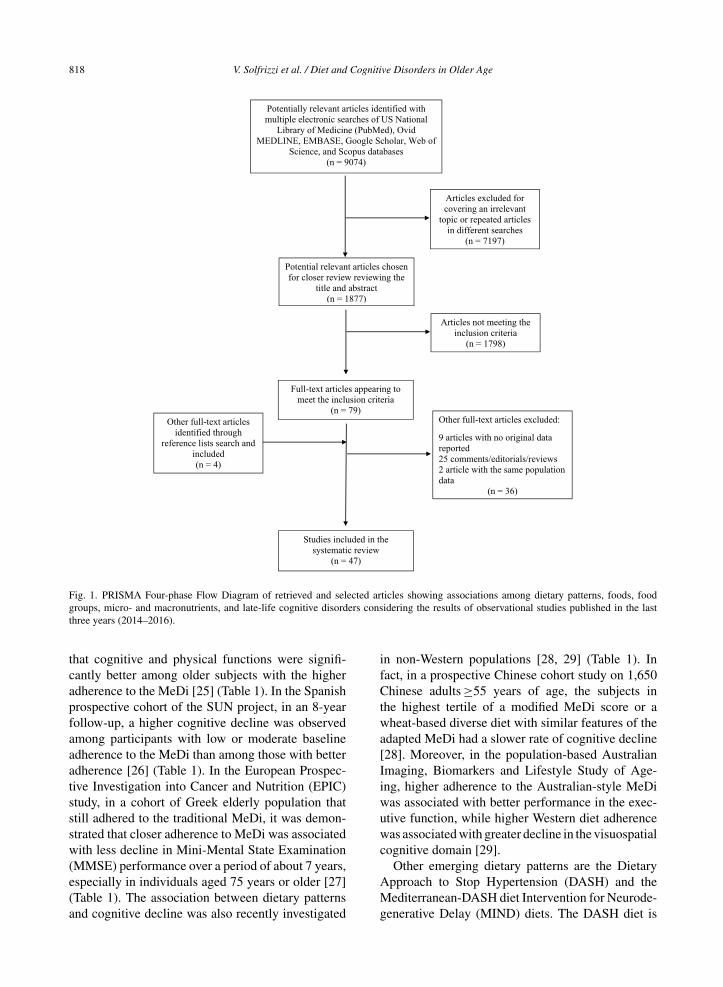
Figure 1 shows the stages in obtaining studiesfor inclusion in the present report (PRISMA Four-phase Flow Diagram). From 9,074 articles identifiedwith multiple electronic searches, we screened titlesand abstracts of the citations downloaded from the
searches and identified 1,877 potential relevant arti-cles chosen for a closer review. We excluded 1,798articles not meeting inclusion criteria and obtainedfull copies of the 79 potentially suitable reports forfurther assessment. After inclusion of 4 articles ofinterest from the reference lists of the selected arti-cles and exclusion of another 36 articles, 47 studiesmet study eligibility criteria and were finally includedin the overall systematic review (Tables 1–3) [25–71].We did not use formal methods of assessment of thequality of the studies included in the present sys-tematic review, given the lack of randomized clinicaltrials, but we described in depth study design andsample together with dietary and cognitive assess-ment and principal results of the included studiesin Tables 1–3 [25–71]. Finally, we used a narrativesynthesis to summarize the findings of the includedstudies, subdividing the articles for the four prin-cipal diet-based approaches (dietary patterns, foodsand food groups, micronutrients, and macronutri-ents), specifying sample size and study design andthe cognitive outcomes of the included studies (late-life cognitive impairment/decline or dementia, AD,and non-AD dementias), when possible.
RESULTS
Dietary patterns and late-life cognition
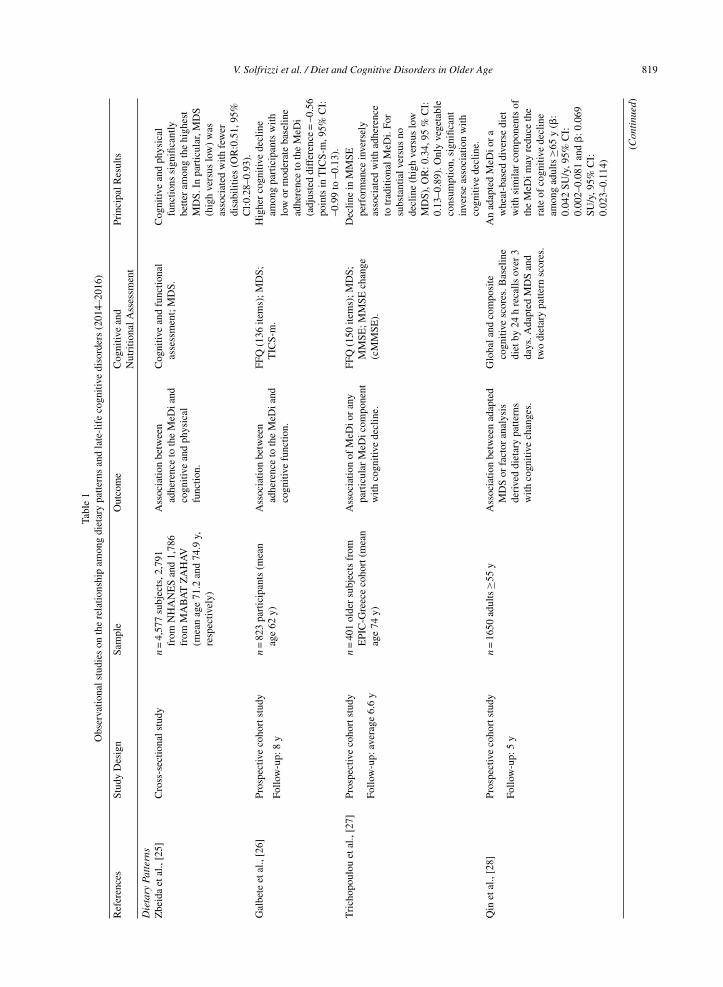
Table 1 shows selected observational studies pub-lished in the last three years that evaluate theassociation of dietary patterns with late-life cogni-tive disorders [25–41]. Among these diets, MeDi isa typical dietary pattern of Mediterranean countries,characterized by high consumption of fruits, vegeta-bles, legumes and cereals, olive oil as the main addedlipid, moderate consumption of alcohol (mainly wineand during meals) and low consumption of red meatand dairy products. It is doubtless the most analyzeddietary pattern, and accumulating evidence supporta potential protective role against cognitive declineand dementia, although there are still inconsisten-cies in the reported data. In particular, the findingsfrom prospective studies and very recent systematicreviews and meta-analyses suggested that adherenceto the MeDi fulfilling the whole-diet approach mayaffect not only the risk of AD, but also of predemen-tia syndromes and their progression to overt dementia[19]. A cross-sectional analysis from the US NationalHealth and Nutrition Survey (NHANES) 1999–2002and from the Israeli National Health and NutritionSurvey (MABAT ZAHAV) 2005–2006 suggested
818 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
Fig. 1. PRISMA Four-phase Flow Diagram of retrieved and selected articles showing associations among dietary patterns, foods, foodgroups, micro- and macronutrients, and late-life cognitive disorders considering the results of observational studies published in the lastthree years (2014–2016).
that cognitive and physical functions were signifi-cantly better among older subjects with the higheradherence to the MeDi [25] (Table 1). In the Spanishprospective cohort of the SUN project, in an 8-yearfollow-up, a higher cognitive decline was observedamong participants with low or moderate baselineadherence to the MeDi than among those with betteradherence [26] (Table 1). In the European Prospec-tive Investigation into Cancer and Nutrition (EPIC)study, in a cohort of Greek elderly population thatstill adhered to the traditional MeDi, it was demon-strated that closer adherence to MeDi was associatedwith less decline in Mini-Mental State Examination(MMSE) performance over a period of about 7 years,especially in individuals aged 75 years or older [27](Table 1). The association between dietary patternsand cognitive decline was also recently investigated
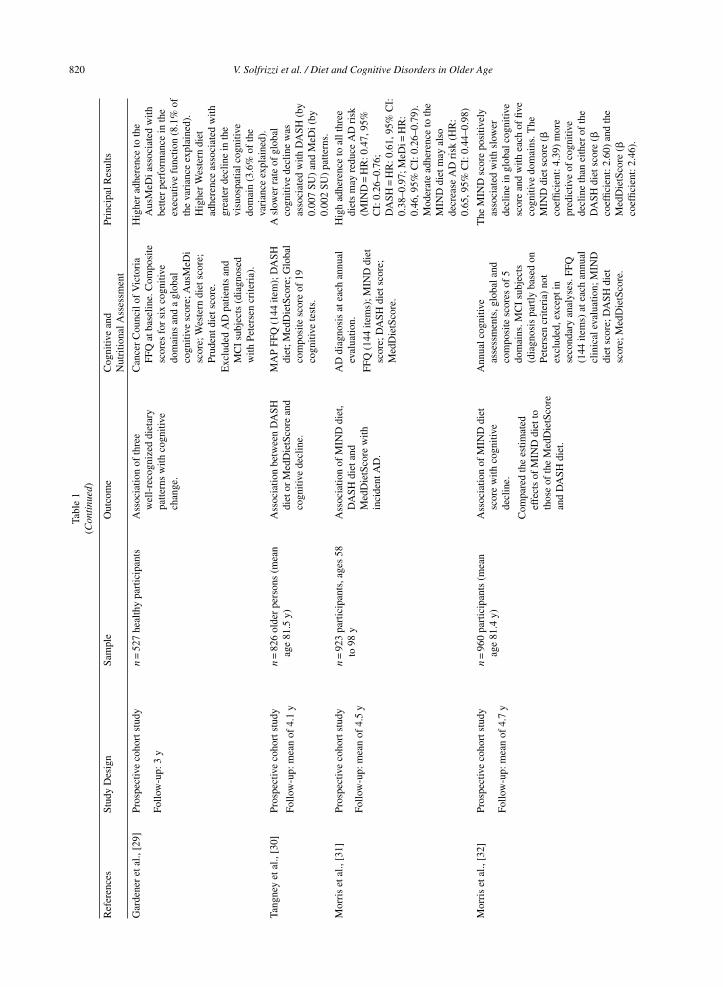
in non-Western populations [28, 29] (Table 1). Infact, in a prospective Chinese cohort study on 1,650Chinese adults ≥55 years of age, the subjects inthe highest tertile of a modified MeDi score or awheat-based diverse diet with similar features of theadapted MeDi had a slower rate of cognitive decline[28]. Moreover, in the population-based AustralianImaging, Biomarkers and Lifestyle Study of Age-ing, higher adherence to the Australian-style MeDiwas associated with better performance in the exec-utive function, while higher Western diet adherencewas associated with greater decline in the visuospatialcognitive domain [29].
Other emerging dietary patterns are the DietaryApproach to Stop Hypertension (DASH) and theMediterranean-DASH diet Intervention for Neurode-generative Delay (MIND) diets. The DASH diet is
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 819Ta
ble
1O
bser
vatio
nals
tudi
eson
the
rela
tions
hip
amon
gdi
etar
ypa
ttern
san
dla
te-l
ife
cogn
itive
diso
rder
s(2
014–
2016
)
Ref
eren
ces
Stud
yD
esig
nSa
mpl
eO
utco
me
Cog
nitiv
ean
dPr
inci
palR
esul
tsN
utri
tiona
lAss
essm
ent
Die
tary
Patt
erns
Zbe
ida
etal
.,[2
5]C
ross
-sec
tiona
lstu
dyn
=4,
577
subj
ects
,2,7
91fr
omN
HA
NE
San
d1,
786
from
MA
BA
TZ
AH
AV
(mea
nag
e71
.2an
d74
.9y,
resp
ectiv
ely)
Ass
ocia
tion
betw
een
adhe
renc
eto
the
MeD
iand
cogn
itive
and
phys
ical
func
tion.
Cog
nitiv
ean
dfu
nctio
nal
asse
ssm
ent;
MD
S.C
ogni
tive
and
phys
ical
func
tions
sign
ifica
ntly
bette
ram
ong
the
high
est
MD
S.In
part
icul
ar,M
DS
(hig
hve
rsus
low
)w
asas
soci
ated
with
few
erdi
sabi
litie
s(O
R:0
.51,
95%
Cl:0
.28–
0.93
).G
albe
teet
al.,
[26]
Pros
pect
ive
coho
rtst
udy
n=
823
part
icip
ants
(mea
nag
e62
y)A
ssoc
iatio
nbe
twee
nad
here
nce
toth
eM
eDia
ndco
gniti
vefu
nctio
n.
FFQ
(136
item
s);M
DS;
TIC
S-m
.H
ighe
rco
gniti
vede
clin
eam
ong
part
icip
ants
with
low
orm
oder
ate
base
line
adhe
renc
eto
the
MeD
i(a
djus
ted
diff
eren
ce=
–0.5
6po
ints
inT
ICS-
m,9
5%C
I:–0
.99
to–0
.13)
.
Follo
w-u
p:8
y
Tri
chop
oulo
uet
al.,
[27]
Pros
pect
ive
coho
rtst
udy
n=
401
olde
rsu
bjec
tsfr
omE
PIC
-Gre
ece
coho
rt(m
ean
age
74y)
Ass
ocia
tion
ofM
eDio
ran
ypa
rtic
ular
MeD
icom
pone
ntw
ithco
gniti
vede
clin
e.
FFQ
(150
item
s);M
DS;
MM
SE;M
MSE
chan
ge(c
MM
SE).
Dec
line
inM
MSE
perf
orm
ance
inve
rsel
yas
soci
ated
with
adhe
renc
eto
trad
ition
alM
eDi.
For
subs
tant
ialv
ersu
sno
decl
ine
(hig
hve
rsus
low
MD
S),O
R:0
.34,
95%
CI:
0.13
–0.8
9).O
nly
vege
tabl
eco
nsum
ptio
n,si
gnifi
cant
inve
rse
asso
ciat
ion
with
cogn
itive
decl
ine.
Follo
w-u
p:av
erag
e6.
6y
Qin
etal
.,[2
8]Pr
ospe
ctiv
eco
hort
stud
yn
=16
50ad
ults
≥55
yA
ssoc
iatio
nbe
twee
nad
apte
dM
DS
orfa
ctor
anal
ysis
deri
ved
diet
ary
patte
rns
with
cogn
itive
chan
ges.
Glo
bala
ndco
mpo
site
cogn
itive
scor
es.B
asel
ine
diet
by24
hre
calls
over
3da
ys.A
dapt
edM
DS
and
two
diet
ary
patte
rnsc
ores
.
An
adap
ted
MeD
ior
aw
heat
-bas
eddi
vers
edi
etw
ithsi
mila
rco
mpo
nent
sof
the
MeD
imay
redu
ceth
era
teof
cogn
itive
decl
ine
amon
gad
ults
≥65
y(�
:0.
042
SU/y
,95%
CI:
0.00
2–0.
081
and
�:0
.069
SU/y
,95%
CI:
0.02
3–0.
114)
Follo
w-u
p:5
y
(Con
tinu
ed)
820 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older AgeTa
ble
1(C
onti
nued
)
Ref
eren
ces
Stud
yD
esig
nSa
mpl
eO
utco
me
Cog
nitiv
ean
dPr
inci
palR
esul
tsN
utri
tiona
lAss
essm
ent
Gar
dene
ret
al.,
[29]
Pros
pect
ive
coho
rtst
udy
n=
527
heal
thy
part
icip
ants
Ass
ocia
tion
ofth
ree
wel
l-re
cogn
ized
diet
ary
patte
rns
with
cogn
itive
chan
ge.
Can
cer
Cou
ncil
ofV
icto
ria
FFQ
atba
selin
e.C
ompo
site
scor
esfo
rsi
xco
gniti
vedo
mai
nsan
da
glob
alco
gniti
vesc
ore;
Aus
MeD
isc
ore;
Wes
tern
diet
scor
e;Pr
uden
tdie
tsco
re.
Hig
her
adhe
renc
eto
the
Aus
MeD
iass
ocia
ted
with
bette
rpe
rfor
man
cein
the
exec
utiv
efu
nctio
n(8
.1%
ofth
eva
rian
ceex
plai
ned)
.H
ighe
rW
este
rndi
etad
here
nce
asso
ciat
edw
ithgr
eate
rde
clin
ein
the
visu
ospa
tialc
ogni
tive
dom
ain
(3.6
%of
the
vari
ance
expl
aine
d).
Follo
w-u
p:3
y
Exc
lude
dA
Dpa
tient
san
dM
CI
subj
ects
(dia
gnos
edw
ithPe
ters
encr
iteri
a).
Tang
ney
etal
.,[3
0]Pr
ospe
ctiv
eco
hort
stud
yn
=82
6ol
der
pers
ons
(mea
nag
e81
.5y)
Ass
ocia
tion
betw
een
DA
SHdi
etor
Med
Die
tSco
rean
dco
gniti
vede
clin
e.
MA
PFF
Q(1
44ite
m);
DA
SHdi
et;M
edD
ietS
core
;Glo
bal
com
posi
tesc
ore
of19
cogn
itive
test
s.
Asl
ower
rate
ofgl
obal
cogn
itive
decl
ine
was
asso
ciat
edw
ithD
ASH
(by
0.00
7SU
)an
dM
eDi(
by0.
002
SU)
patte
rns.
Follo
w-u
p:m
ean
of4.
1y
Mor
ris
etal
.,[3
1]Pr
ospe
ctiv
eco
hort
stud
yn
=92
3pa
rtic
ipan
ts,a
ges
58to
98y
Ass
ocia
tion
ofM
IND
diet
,D
ASH
diet
and
Med
Die
tSco
rew
ithin
cide
ntA
D.
AD
diag
nosi
sat
each
annu
alev
alua
tion.
Hig
had
here
nce
toal
lthr
eedi
ets
may
redu
ceA
Dri
sk(M
IND
=H
R:0
.47,
95%
CI:
0.26
–0.7
6;D
ASH
=H
R:0
.61,
95%
CI:
0.38
–0.9
7;M
eDi=
HR
:0.
46,9
5%C
I:0.
26–0
.79)
.M
oder
ate
adhe
renc
eto
the
MIN
Ddi
etm
ayal
sode
crea
seA
Dri
sk(H
R:
0.65
,95%
CI:
0.44
–0.9
8)
Follo
w-u
p:m
ean
of4.
5y
FFQ
(144
item
s);M
IND
diet
scor
e;D
ASH
diet
scor
e;M
edD
ietS
core
.
Mor
ris
etal
.,[3
2]Pr
ospe
ctiv
eco
hort
stud
yn
=96
0pa
rtic
ipan
ts(m
ean
age
81.4
y)A
ssoc
iatio
nof
MIN
Ddi
etsc
ore
with
cogn
itive
decl
ine.
Ann
ualc
ogni
tive
asse
ssm
ents
,glo
bala
ndco
mpo
site
scor
esof
5do
mai
ns.M
CI
subj
ects
(dia
gnos
ispa
rtly
base
don
Pete
rsen
crite
ria)
not
excl
uded
,exc
epti
nse
cond
ary
anal
yses
.FFQ
(144
item
s)at
each
annu
alcl
inic
alev
alua
tion;
MIN
Ddi
etsc
ore;
DA
SHdi
etsc
ore;
Med
Die
tSco
re.
The
MIN
Dsc
ore
posi
tivel
yas
soci
ated
with
slow
erde
clin
ein
glob
alco
gniti
vesc
ore
and
with
each
offiv
eco
gniti
vedo
mai
ns.T
heM
IND
diet
scor
e(�
coef
ficie
nt:4
.39)
mor
epr
edic
tive
ofco
gniti
vede
clin
eth
anei
ther
ofth
eD
ASH
diet
scor
e(�
coef
ficie
nt:2
.60)
and
the
Med
Die
tSco
re(�
coef
ficie
nt:2
.46)
.
Follo
w-u
p:m
ean
of4.
7y
Com
pare
dth
ees
timat
edef
fect
sof
MIN
Ddi
etto
thos
eof
the
Med
Die
tSco
rean
dD
ASH
diet
.
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 821M
osco
niet
al.,
[33]
Cro
ss-s
ectio
nals
tudy
n=
52cl
inic
ally
and
cogn
itive
lyno
rmal
subj
ects
(mea
nag
e54
y)
Ass
ocia
tions
betw
een
adhe
renc
eto
aM
eDia
ndst
ruct
ural
MR
I-ba
sed
brai
nat
roph
yin
key
regi
ons
for
AD
.
Sem
iqua
ntita
tive
FFQ
(61-
item
);C
DR
=0;
MD
S;M
RI
CT
mea
sure
sfo
r5
RO
Is.
Subj
ects
with
high
erM
eDi
adhe
renc
esh
owed
grea
ter
CT
ofA
D-v
ulne
rabl
eR
OIs
asco
mpa
red
tosu
bjec
tsw
ithlo
wer
MeD
iad
here
nce.
Ber
tiet
al.,
[34]
Cro
ss-s
ectio
nals
tudy
n=
52cl
inic
ally
and
cogn
itive
lyno
rmal
subj
ects
(mea
nag
e54
y)
Ass
ocia
tions
ofnu
trie
ntpa
ttern
s(N
P)w
ithm
ajor
brai
nA
Dbi
omar
kers
.Fiv
eN
PSw
ere
iden
tified
.
Sem
iqua
ntita
tive
FFQ
(116
-ite
m);
CD
R=
0;Pi
B-
and
FD-
PET
scan
sM
RI
mea
sure
s.
NP4
scor
es(v
itam
ins
B12
,D,
and
zinc
)w
ere
posi
tivel
yas
soci
ated
with
ME
Tgl
can
dT
GM
V,a
ndne
gativ
ely
asso
ciat
edw
ithPi
Bre
tent
ion
inA
D-v
ulne
rabl
ere
gion
s.M
ET
glc
and
TG
MV
wer
epo
sitiv
ely
asso
ciat
edw
ithN
P2sc
ores
(vita
min
E.M
UFA
,and
PUFA
),an
dne
gativ
ely
asso
ciat
edw
ithN
P5sc
ores
(SFA
,tra
nsun
satu
rate
dfa
ttyac
ids,
chol
este
rola
ndso
dium
),an
dM
ET
glc
was
posi
tivel
yas
soci
ated
with
high
erN
P3sc
ores
(vita
min
A,v
itam
inC
,car
oten
oids
,an
ddi
etar
yfib
ers)
.St
aubo
etal
.,[3
5]C
ross
-sec
tiona
lstu
dyn
=67
2co
gniti
vely
norm
alpa
rtic
ipan
ts(m
ean
age:
79.8
y)
Ass
ocia
tion
ofM
DS
and
MeD
icom
pone
nts
with
MR
Im
easu
res
ofC
Tfo
rth
efo
urlo
bes
sepa
rate
lyan
dav
erag
ed.
FFQ
(128
item
s);M
DS;
MR
IC
Tm
easu
res.
Exc
lude
dpa
tient
sw
ithde
men
tiaan
dM
CI
subj
ects
(dia
gnos
edw
ithPe
ters
encr
iteri
a).
Hig
her
MD
Sas
soci
ated
with
larg
erC
T.H
ighe
rle
gum
e,fis
h,ve
geta
bles
,who
legr
ains
orce
real
sin
take
sw
ere
asso
ciat
edw
ithla
rger
CT.
Gu
etal
.,[3
6]C
ross
-sec
tiona
lstu
dyn
=67
4el
derl
yad
ults
with
out
dem
entia
(mea
nag
e80
.1y)
Ass
ocia
tion
betw
een
high
erad
here
nce
toM
eDiw
ithla
rger
MR
Im
easu
red
brai
nvo
lum
eor
CT.
FFQ
;MD
S;M
RI
scan
sfo
rT
BV
,TG
MV
,TW
MV
and
mC
T.
Hig
her
MeD
iadh
eren
ceas
soci
ated
with
13.1
1,5.
00,
and
6.41
mm
larg
erT
BV
,T
GM
Van
dT
WM
V,
resp
ectiv
ely.
Hig
her
fish
inta
keas
soci
ated
with
larg
erT
GM
Van
dm
CT.
Low
erm
eati
ntak
eas
soci
ated
with
larg
erT
GM
Van
dT
BV
.
Exc
lude
dpa
tient
sw
ithde
men
tiaan
dM
CI
subj
ects
(dia
gnos
edw
ithPe
ters
encr
iteri
a).
(Con
tinu
ed)
822 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
Tabl
e1
(Con
tinu
ed)
Ref
eren
ces
Stud
yD
esig
nSa
mpl
eO
utco
me
Cog
nitiv
ean
dPr
inci
palR
esul
tsN
utri
tiona
lAss
essm
ent
Jack
aet
al.,
[37]
Pros
pect
ive
coho
rtst
udy
n=
255
olde
rad
ults
(mea
nag
e62
.6y)
Ass
ocia
tion
betw
een
diet
ary
patte
rns
and
hipp
ocam
pal
volu
me.
Ass
ocia
tion
betw
een
diet
and
diff
eren
tialr
ates
ofhi
ppoc
ampa
latr
ophy
over
time.
FFQ
;“Pr
uden
t”(h
ealth
y)di
etan
d“W
este
rn”
(unh
ealth
y)di
et;T
wo
MR
Isc
ans.
Eve
ryon
eSD
incr
ease
ina
“pru
dent
”di
etar
ypa
ttern
was
asso
ciat
edw
itha
45.7
mm
3(S
E22
.9m
m3)
larg
erle
fthi
ppoc
ampa
lvo
lum
e,w
hile
high
erco
nsum
ptio
nof
a“W
este
rn”
diet
ary
patte
rnw
asas
soci
ated
with
a52
.6m
m3
(SE
26.6
mm
3)
smal
ler
left
hipp
ocam
pal
volu
me.
No
evid
ence
that
diet
ary
patte
rns
influ
ence
dhi
ppoc
ampa
lvol
ume
decl
ine.
Follo
w-u
p:4
y
Pelle
tier
etal
.,[3
8]Pr
ospe
ctiv
eco
hort
stud
yn
=14
6no
n-de
men
ted
part
icip
ants
(mea
nag
e73
y)
Ass
ocia
tion
betw
een
high
erad
here
nce
toth
eM
eDia
ndpr
eser
ved
brai
nG
Mvo
lum
ean
dW
Mm
icro
stru
ctur
e.
FFQ
(148
item
s);M
DS;
MR
I;B
rain
GM
and
WM
volu
mes
,and
WM
mic
rost
ruct
ure;
Cog
nitiv
eas
sess
men
t.
Adh
eren
ceto
the
MeD
isi
gnifi
cant
lyas
soci
ated
with
pres
erve
dW
Mm
icro
stru
ctur
ein
exte
nsiv
ear
eas,
aga
inin
stru
ctur
alco
nnec
tivity
rela
ted
tost
rong
cogn
itive
bene
fits.
Follo
w-u
p:M
RI
perf
orm
edm
ean
of8.
9y
afte
rdi
etar
yas
sess
men
t
Exc
lude
dpa
tient
sw
ithde
men
tia.
Shak
ersa
inet
al.,
[39]
Popu
latio
n-ba
sed
long
itudi
nals
tudy
n=
2,22
3de
men
tia-f
ree
olde
rad
ults
(mea
nag
e70
.6y)
Impa
ctof
diet
ary
patte
rns
onco
gniti
vede
clin
e.M
MSE
;Sem
i-qu
antit
ativ
eFF
Q(9
8ite
ms)
;Tw
odi
etar
ypa
ttern
s:1)
the
“Wes
tern
”,2)
the
“pru
dent
”;fa
ctor
scor
esfo
rea
chdi
etar
ypa
ttern
cate
gori
zed
into
quin
tiles
.E
xclu
ded
patie
nts
with
dem
entia
.
Hig
hest
adhe
renc
eto
prud
ent
patte
rnre
late
dto
less
MM
SEde
clin
e(�
:0.1
06),
whe
reas
the
high
est
adhe
renc
eto
Wes
tern
patte
rnw
asas
soci
ated
with
mor
eM
MSE
decl
ine
(�:0
.156
).D
eclin
eas
soci
ated
with
Wes
tern
diet
,atte
nuat
edby
high
adhe
renc
eto
prud
ent
patte
rn.
Follo
w-u
p:6
y
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 823
Smyt
het
al.,
[40]
Pros
pect
ive
coho
rtst
udy
n=
27,8
60pa
tient
s(m
ean
age
66.2
y)A
ssoc
iatio
nof
diet
ary
fact
ors
and
cogn
itive
decl
ine
ina
popu
latio
nat
high
risk
ofca
rdio
vasc
ular
dise
ase.
MM
SE;F
FQ(2
0ite
ms)
;m
AH
EI.
Hig
hest
quin
tile
ofm
AH
EI
(hea
lthie
stdi
et)
asso
ciat
edw
itha
redu
ced
risk
ofco
gniti
vede
clin
e(H
R:
0.76
,95%
CI:
0.66
–0.8
6).
Follo
w-u
p:56
mon
ths
Oza
wa
etal
.,[4
1]Pr
ospe
ctiv
eco
hort
stud
yn
=5,
083
patie
nts
(mea
nag
e56
y)In
vest
igat
edi
etar
ypa
ttern
sas
soci
ated
with
infla
mm
atio
n.
Alic
eH
eim
4-I,
shor
t-te
rmve
rbal
mem
ory,
phon
emic
and
sem
antic
fluen
cy,
MM
SE.F
FQ(1
27ite
m).
Seru
mIL
-6.I
DP.
Die
tary
patte
rnw
ithhi
gher
inta
keof
red
and
proc
esse
dm
eat,
peas
,leg
umes
and
frie
dfo
od,a
ndlo
wer
inta
keof
who
legr
ains
asso
ciat
edw
ithhi
gher
infla
mm
ator
ym
arke
rsan
dac
cele
rate
dco
gniti
vede
clin
e.In
part
icul
ar,t
here
was
agr
eate
rde
clin
ein
reas
onin
gin
part
icip
ants
inth
ehi
ghes
tter
tile
ofad
here
nce
toth
eID
P(–
0.37
SD,9
5%C
I:–0
.40,
–0.3
4)co
mpa
red
toth
ose
inth
elo
wes
tter
tile
(–0.
31SD
;95%
CI:
–0.3
4,–0
.28)
afte
rad
just
men
tfor
cova
riat
es.
Follo
w-u
p:10
y
Ass
ocia
tion
ofsu
chdi
etw
ithco
gniti
vede
clin
e.
NH
AN
ES,
Nat
iona
lHea
lthan
dN
utri
tion
Surv
ey;M
AB
AT
ZA
HA
V,I
srae
liN
atio
nalH
ealth
and
Nut
ritio
nSu
rvey
;MeD
i,M
edite
rran
ean
diet
;MD
S,M
edite
rran
ean
diet
scor
e;O
R,o
dds
ratio
;CI,
confi
denc
ein
terv
al;
FFQ
,Foo
dFr
eque
ncy
Que
stio
nnai
re;
TIC
S-m
,Tel
epho
neIn
terv
iew
ofC
ogni
tive
Stat
us-m
odifi
ed;
MM
SE,M
ini-
Men
tal
Stat
eE
xam
inat
ion;
SU,s
tand
ard
units
;A
usM
eDi,
Aus
tral
ian-
styl
eM
edite
rran
ean
diet
;DA
SH,D
ieta
ryA
ppro
ach
toSt
opH
yper
tens
ion;
MA
P,M
emor
yan
dA
ging
Proj
ect;
AD
,Alz
heim
er’s
dise
ase;
MIN
D,M
edite
rran
ean-
DA
SHdi
etIn
terv
entio
nfo
rN
euro
dege
nera
tive
Del
ay;C
DR
,Clin
ical
Dem
entia
Rat
ing
scal
e;H
R,h
azar
dra
tio;M
RI,
mag
netic
reso
nanc
eim
agin
g;C
T,co
rtic
alth
ickn
ess;
RO
I,re
gion
ofin
tere
st;P
ET,
posi
tron
emis
sion
tom
ogra
phy;
PiB
,11
C-P
ittsb
urgh
com
poun
d-B
;FD
G,
18F-
fluor
odeo
xygl
ucos
e;M
ET
glc,
gluc
ose
met
abol
ism
;T
GM
V,
tota
lgr
aym
atte
rvo
lum
e;M
UFA
,m
onou
nsat
urat
edfa
ttyac
ids;
PUFA
,po
lyun
satu
rate
dfa
ttyac
ids;
SFA
,sat
urat
edfa
ttyac
ids;
TB
V,t
otal
brai
nvo
lum
e;T
WM
V,t
otal
whi
tem
atte
rvo
lum
e;m
CT,
mea
nco
rtic
alth
ickn
ess;
SD,s
tand
ard
devi
atio
n;SE
,sta
ndar
der
ror;
GM
,gra
ym
atte
r;W
M,w
hite
mat
ter;
mA
HE
I,m
odifi
edA
ltern
ativ
eH
ealth
yE
atin
gIn
dex;
IL-6
,int
erle
ukin
-6;I
DP,
infla
mm
ator
ydi
etar
ypa
ttern
.

824 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
characterized by low consumption of saturated fat andcommercial pastries and sweets, and higher intake ofdairy than in the MeDi. In the last three years, in theMemory and Aging Project (MAP) study, a prospec-tive study on older adults with 4 years of follow-up,the DASH pattern was associated with slower ratesof cognitive decline. In particular, a 1-unit-higherDASH score, was equivalent of being at least 4.4years younger [30] (Table 1). These results were inline with those of Morris and colleagues, in the sameMAP study, in which higher adherence to DASH dietwas related with greater reduction of incident ADrather than higher adherence to MeDi (54% and 39%reduction, respectively) [31] (Table 1).
The MIND diet was based on the dietary compo-nents of the MeDi and DASH diet with modificationsthat highlight the foods and nutrients shown to beassociated with dementia prevention. Among theMIND diet components, there are 10 brain healthyfood groups (green leafy vegetables, other vegetables,nuts, berries, beans, whole grains, seafood, poultry,olive oil, and wine) and five unhealthy food groups(red meats, butter and stick margarine, cheese, pas-tries and sweets, and fried/fast food). Hence, MINDdiet uniquely specifies consumption of berries andgreen leafy vegetables and does not specify high fruitconsumption (both DASH and MeDi), high dairy(DASH), high potato consumption, or >1 fish meal perweek (MeDi). Other recent findings from the MAPstudy suggested that higher MIND diet score wasassociated with slower decline in cognitive abilities[32] (Table 1). The rate reduction for persons in thehighest tertile of diet scores compared with the lowesttertile was the equivalent of being 7.5 years younger.MIND diet score was also more predictive of cogni-tive decline than either of the other diet scores (DASHand MeDi) [32]. Furthermore, in a follow-up of 4.5years of the MAP study, participants with higher andmoderate adherence to MIND diet had statisticallysignificant reduction in AD rate compared with thosewith lower adherence (53% and 35% respectively)[31] (Table 1). Instead, only the highest tertiles of theDASH and MeDi scores were significantly associatedwith incident AD reduction [31].
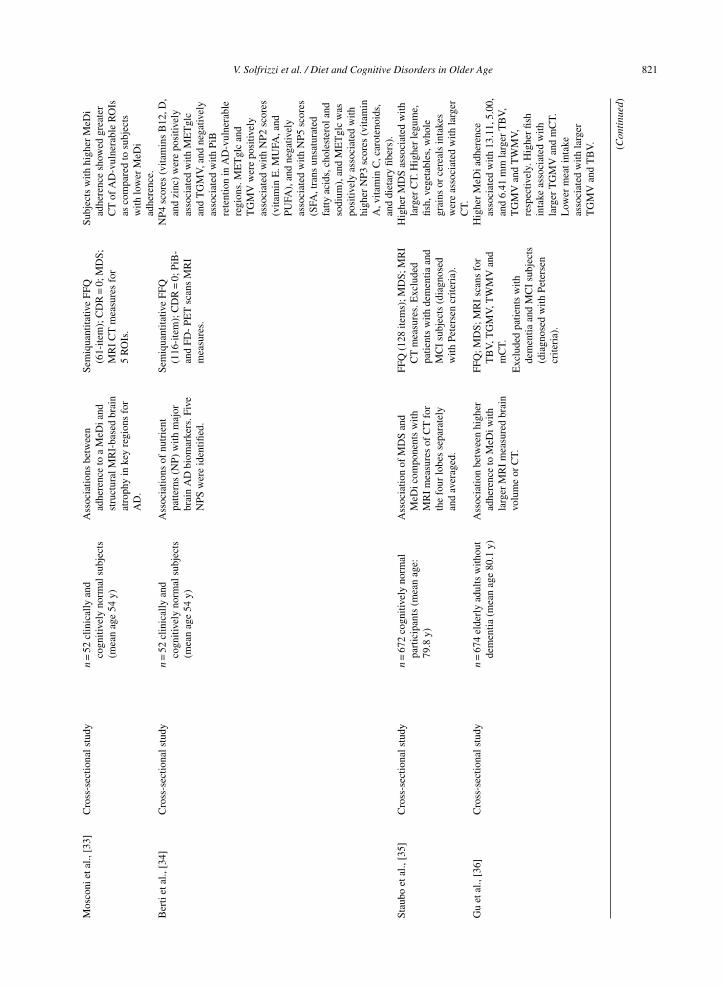
Despite the promising results of these two diets,to date, we have brain imaging data only on thecorrelation with the MeDi (Table 1). The fewcross-sectional studies carried out on cognitively nor-mal people showed that higher adherence to MeDiwas related to greater magnetic resonance imaging(MRI)-based cortical thickness in AD-vulnerableregions and larger brain volumes. MeDi effects on
MRI biomarkers were significant in the left, but notin the right hemisphere, and were most pronouncedin entorhinal cortex, orbito-frontal cortex and pos-terior cingulate cortex [33] (Table 1). In the samesample of cognitively normal people, 5 differentnutrients patterns (NPs) were identified and associ-ated with major brain AD biomarkers. NP4 scores(vitamins B12, D, and zinc) were positively asso-ciated with glucose metabolism investigated with18F-fluorodeoxyglucose positron emission tomog-raphy (PET) scans and MRI-based total graymatter volume, and negatively associated with PET-11CPittsburgh compound-B (PiB) retention in AD-vulnerable regions. Glucose metabolism and totalgray matter volume were also positively associatedwith NP2 scores (vitamin E, MUFA, and PUFA),and negatively associated with NP5 scores [satu-rated fatty acids (SFA), trans unsaturated fatty acids,cholesterol and sodium], and glucose metabolism waspositively associated with higher NP3 scores (vita-min A, vitamin C, carotenoids, and dietary fibers)[34] (Table 1). Higher adherence to a Mediterraneandietary pattern was associated with larger MRI mea-sures of cortical thickness and with several individualregion of interests (ROIs) that undergo age-relatedor AD-related neurodegeneration, was marginallyassociated with temporal and AD signature corticalthickness, and was not associated with hippocampalvolume [35] (Table 1). This finding may be explainedwith the observation from the Alzheimer’s DiseaseNeuroimaging Initiative in which presymptomaticindividuals had significantly reduced cortical thick-ness in AD-vulnerable regions compared to controlsbut did not differ in regard to hippocampal volume[72]. In the Washington Heights–Inwood CommunityAging Project (WHICAP), higher MeDi adherencewas associated with less brain atrophy (larger totalbrain volume, total gray matter volume, total whitematter volume), with an effect similar to 5 years ofaging [36] (Table 1).
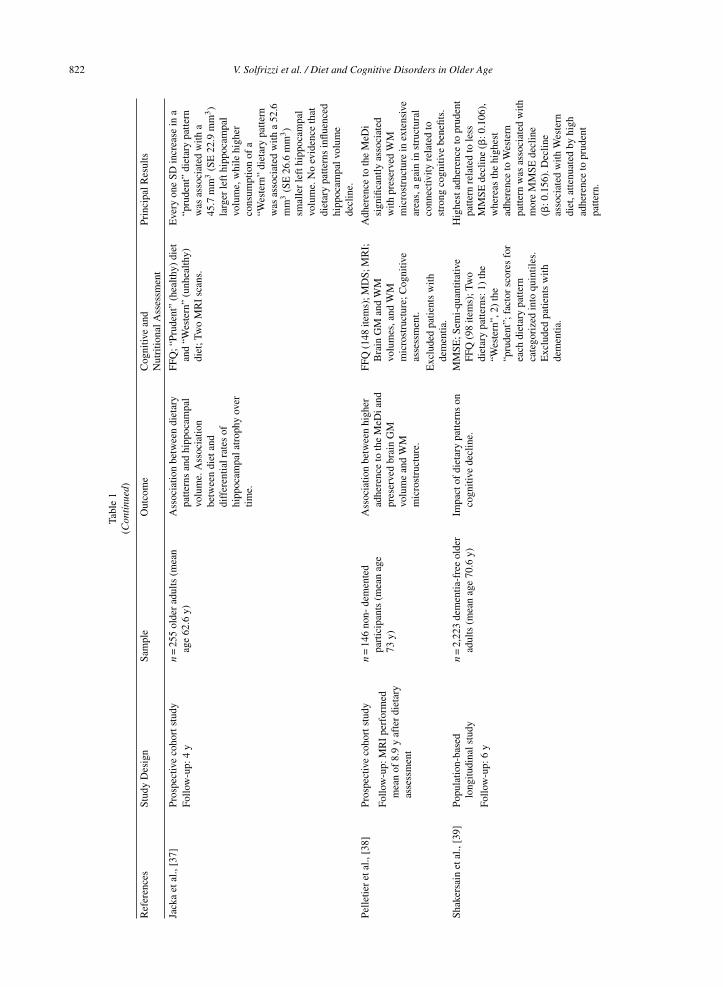
In the last three years, only one prospectiveimaging-diet study on older adults was conducted[37] (Table 1), confirming other results coming fromcross-sectional studies. In fact, Jacka and colleagues,in the Personality and Total Health Through LifeStudy, found that a healthy “prudent” dietary pat-tern characterized by intake of fresh vegetables,salad, fruit and grilled fish was associated with alarger left hippocampal volume on MRI over 4 yearsof follow-up [37] (Table 1). In particular, every onestandard deviation (SD) increase in healthy “pru-dent” dietary pattern was associated with a 45.7 mm3

V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 825
larger left hippocampal volume [37]. While higherconsumption of an unhealthy Western dietary pat-tern characterized by intake roast meat, sausages,hamburgers, steak, chips, crisps, and soft drinks wasindependently associated with a 52.6 mm3 smallerleft hippocampal volume [37]. The difference in hip-pocampal volume between those classified with ahealthy and or unhealthy diet was 203 mm3, a dif-ference which corresponds to 62% of the averagedecline in left hippocampal volume observed overthe 4-year period. It was found no interaction betweenright hippocampus volumes and the two dietary factorscores [37]. Other studies suggested a strong impactof healthy diets on structural connectivity in oldersubjects, rather than gray and white matter volumes.In fact, through diffusion tensor imaging (DTI) atMRI examination was seen that higher adherenceto the MeDi was associated with preserved whitematter microstructure in multiple brain areas andappeared to delay cognitive aging by up to 10 years[38] (Table 1). None of the individual componentswas strongly associated with DTI parameters, sup-porting the hypothesis that overall diet quality maybe more important to preserve brain structure than anysingle food. These results suggested the involvementof vascular pathways rather than neurodegenerativemechanisms in the link between the MeDi and lowerrisks of cognitive decline and related diseases [38].
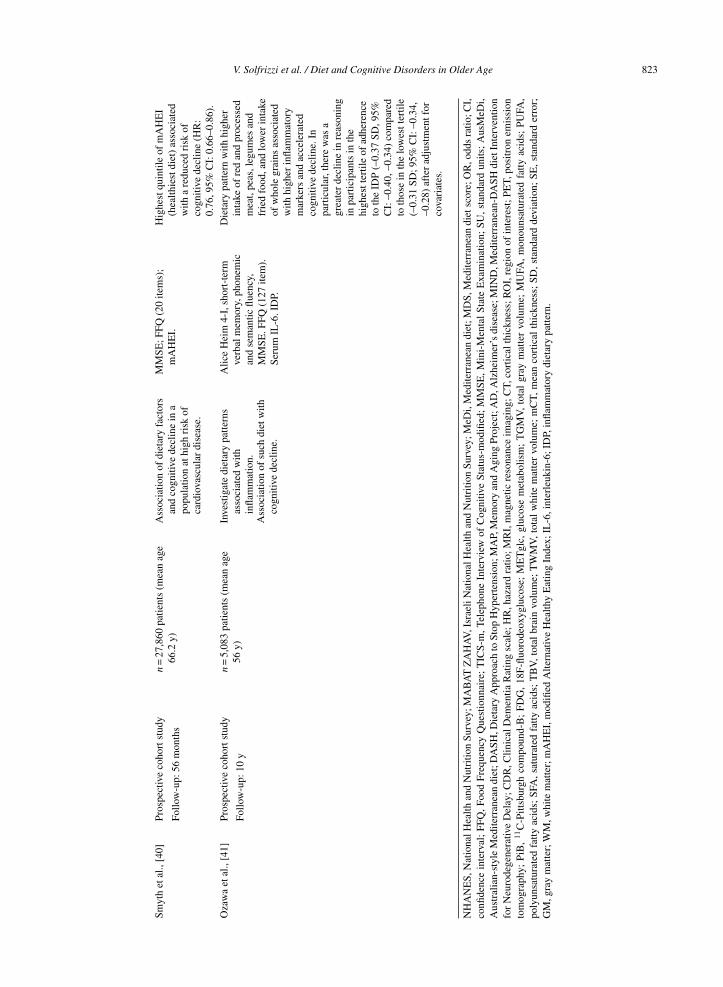
The importance of components of prudent dietarypattern (vegetables, fruit, cooking/dressing oil, cere-als and legumes, whole grains, rice/pasta, fish, low-fatdairy, poultry and water) was confirmed by theobservation that the MMSE decline associated withWestern diet may be attenuated by high adherenceto prudent pattern [39] (Table 1). In fact, the declinebecame less pronounced (53.5%) and non-significantamong people who had a high adherence to both theprudent and Western patterns. Furthermore, West-ern dietary pattern score was significantly associatedwith all-cause mortality in the older age cohorts [39].Instead, people followed healthiest diet was slightlyolder, more active, less likely to smoke, had a lowerbody mass index, normal serum creatinine, and hadhigher MMSE score [40] (Table 1). The healthi-est diet was associated with a reduction of about24% in risk of cognitive decline and in particularwas shown a significant association between higherdiet quality and reduced risk of decline in 4 com-ponents of the MMSE including copying, attentionand calculation, registration, and writing [40]. Thebrain damage related to an unhealthy diet may bebased on a pro-inflammatory mechanism. Ozawa and
colleagues detected an inflammatory dietary patterncharacterized by higher intake of red meat, processedmeat, peas and legumes, and fried food, and lowerintake of whole grains which correlated with elevatedinterleukin (IL)-6 [41] (Table 1). It was related withgreater decline in reasoning and in global cognitionand, in a cross-sectional analysis at baseline, a twotimes greater risk of having a decline of 3 points ormore in MMSE [41].
Foods, food groups, and late-life cognitivedisorders
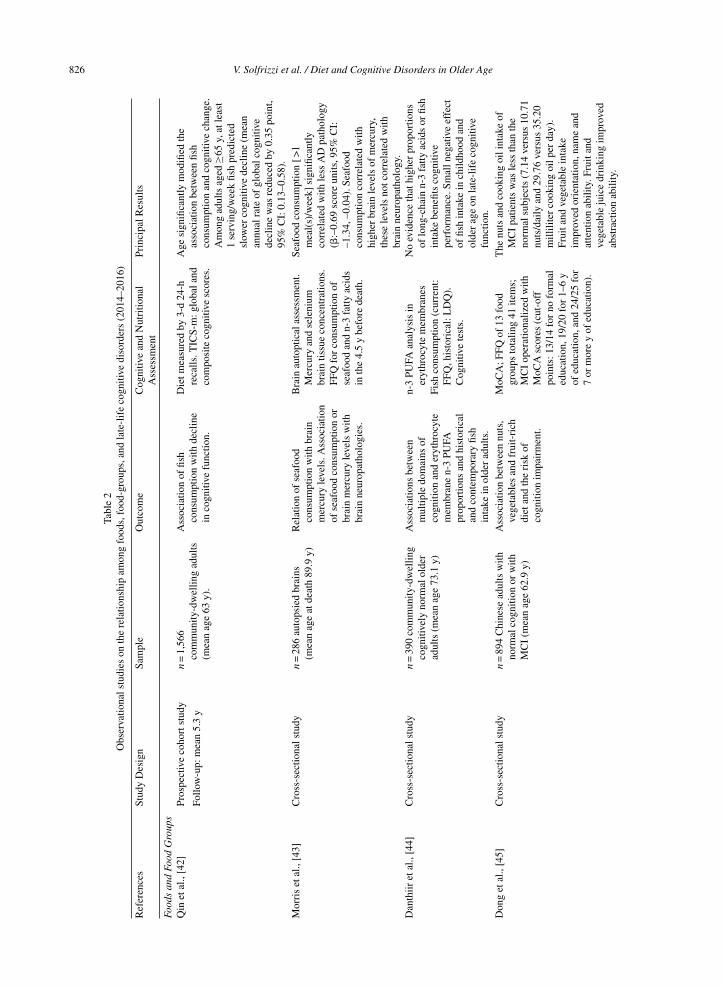
Fish and seafoodTable 2 shows selected observational studies pub-
lished in the last three years and evaluating therelationship among foods, food-groups, and late-lifecognitive disorders [42–54]. In particular, the emerg-ing data from the last studies on the correlationbetween fish and seafood consumption and cogni-tive decline are conflicting. Significant correlationswere found in some particular population subgroups[ ≥65 years and apolipoprotein E (APOE) �4 car-riers]. Age significantly modified the associationbetween fish consumption and cognitive change [42](Table 2). In fact, no association was observed amongadults aged 55–64 years. Conversely, adults aged ≥65years, that consuming ≥1 servings/week fish (i.e.,100 g) had a reduction of cognitive decline rate[42]. Compared with individuals who consumed <1serving/week fish, the mean annual rate of global cog-nitive decline was reduced by 0.35-point equivalent tothe disparity associated with 1.6 years of age. Remov-ing shellfish and/or preserved fish from the total fishdid not appreciably alter the results [42].
Interestingly, Morris and colleagues showed that,in APOE �4 carriers, seafood consumption≥β1meals/week was correlated with lesser burden ofbrain AD neuropathology, including lower densityof neuritic plaques, less severe and widespread neu-rofibrillary tangles, and lower neuropathologicallydefined AD [43] (Table 2). Furthermore, some studiesdemonstrated an association between fish consump-tion and MRI biomarkers [34, 35] (Table 1). Inthe Mayo Clinic Study of Aging, higher fish intakewas associated with larger cortical thickness sum-mary measures for parietal and average lobar corticalthickness and marginally associated with AD signa-ture cortical thickness, temporal and frontal corticalthickness, and also associated with several individ-ual cortical thickness measures: precuneus, superiorparietal, posterior cingulate, supramarginal, middle
826 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
Tabl
e2
Obs
erva
tiona
lstu
dies
onth
ere
latio
nshi
pam
ong
food
s,fo
od-g
roup
s,an
dla
te-l
ife
cogn
itive
diso
rder
s(2
014–
2016
)
Ref
eren
ces
Stud
yD
esig
nSa
mpl
eO
utco
me
Cog
nitiv
ean
dN
utri
tiona
lA
sses
smen
tPr
inci
palR
esul
ts
Food
san
dFo
odG
roup
sQ
inet
al.,
[42]
Pros
pect
ive
coho
rtst
udy
n=
1,56
6co
mm
unity
-dw
ellin
gad
ults
(mea
nag
e63
y).
Ass
ocia
tion
offis
hco
nsum
ptio
nw
ithde
clin
ein
cogn
itive
func
tion.
Die
tmea
sure
dby
3-d
24-h
reca
lls.T
ICS-
m:g
loba
land
com
posi
teco
gniti
vesc
ores
.
Age
sign
ifica
ntly
mod
ified
the
asso
ciat
ion
betw
een
fish
cons
umpt
ion
and
cogn
itive
chan
ge.
Am
ong
adul
tsag
ed≥6
5y,
atle
ast
1se
rvin
g/w
eek
fish
pred
icte
dsl
ower
cogn
itive
decl
ine
(mea
nan
nual
rate
ofgl
obal
cogn
itive
decl
ine
was
redu
ced
by0.
35po
int,
95%
CI:
0.13
–0.5
8).
Follo
w-u
p:m
ean
5.3
y
Mor
ris
etal
.,[4
3]C
ross
-sec
tiona
lstu
dyn
=28
6au
tops
ied
brai
ns(m
ean
age
atde
ath
89.9
y)R
elat
ion
ofse
afoo
dco
nsum
ptio
nw
ithbr
ain
mer
cury
leve
ls.A
ssoc
iatio
nof
seaf
ood
cons
umpt
ion
orbr
ain
mer
cury
leve
lsw
ithbr
ain
neur
opat
holo
gies
.
Bra
inau
topt
ical
asse
ssm
ent.
Mer
cury
and
sele
nium
brai
ntis
sue
conc
entr
atio
ns.
FFQ
for
cons
umpt
ion
ofse
afoo
dan
dn-
3fa
ttyac
ids
inth
e4.
5y
befo
rede
ath.
Seaf
ood
cons
umpt
ion
[>1
mea
l(s)
/wee
k]si
gnifi
cant
lyco
rrel
ated
with
less
AD
path
olog
y(�
:–0.
69sc
ore
units
,95%
CI:
–1.3
4,–0
.04)
.Sea
food
cons
umpt
ion
corr
elat
edw
ithhi
gher
brai
nle
vels
ofm
ercu
ry,
thes
ele
vels
notc
orre
late
dw
ithbr
ain
neur
opat
holo
gy.
Dan
thiir
etal
.,[4
4]C
ross
-sec
tiona
lstu
dyn
=39
0co
mm
unity
-dw
ellin
gco
gniti
vely
norm
alol
der
adul
ts(m
ean
age
73.1
y)
Ass
ocia
tions
betw
een
mul
tiple
dom
ains
ofco
gniti
onan
der
ythr
ocyt
em
embr
ane
n-3
PUFA
prop
ortio
nsan
dhi
stor
ical
and
cont
empo
rary
fish
inta
kein
olde
rad
ults
.
n-3
PUFA
anal
ysis
iner
ythr
ocyt
em
embr
anes
No
evid
ence
that
high
erpr
opor
tions
oflo
ng-c
hain
n-3
fatty
acid
sor
fish
inta
kebe
nefit
sco
gniti
vepe
rfor
man
ce.S
mal
lneg
ativ
eef
fect
offis
hin
take
inch
ildho
odan
dol
der
age
onla
te-l
ife
cogn
itive
func
tion.
Fish
cons
umpt
ion
(cur
rent
:FF
Q,h
isto
rica
l:L
DQ
).C
ogni
tive
test
s.
Don
get
al.,
[45]
Cro
ss-s
ectio
nals
tudy
n=
894
Chi
nese
adul
tsw
ithno
rmal
cogn
ition
orw
ithM
CI
(mea
nag
e62
.9y)
Ass
ocia
tion
betw
een
nuts
,ve
geta
bles
and
frui
t-ri
chdi
etan
dth
eri
skof
cogn
ition
impa
irm
ent.
MoC
A;F
FQof
13fo
odgr
oups
tota
ling
41ite
ms;
MC
Iop
erat
iona
lized
with
MoC
Asc
ores
(cut
-off
poin
ts:1
3/14
for
nofo
rmal
educ
atio
n,19
/20
for
1–6
yof
educ
atio
n,an
d24
/25
for
7or
mor
ey
ofed
ucat
ion)
.
The
nuts
and
cook
ing
oili
ntak
eof
MC
Ipa
tient
sw
asle
ssth
anth
eno
rmal
subj
ects
(7.1
4ve
rsus
10.7
1nu
ts/d
aily
and
29.7
6ve
rsus
35.2
0m
illili
ter
cook
ing
oilp
erda
y).
Frui
tand
vege
tabl
ein
take
impr
oved
orie
ntat
ion,
nam
ean
dat
tent
ion
abili
ty.F
ruit
and
vege
tabl
eju
ice
drin
king
impr
oved
abst
ract
ion
abili
ty.
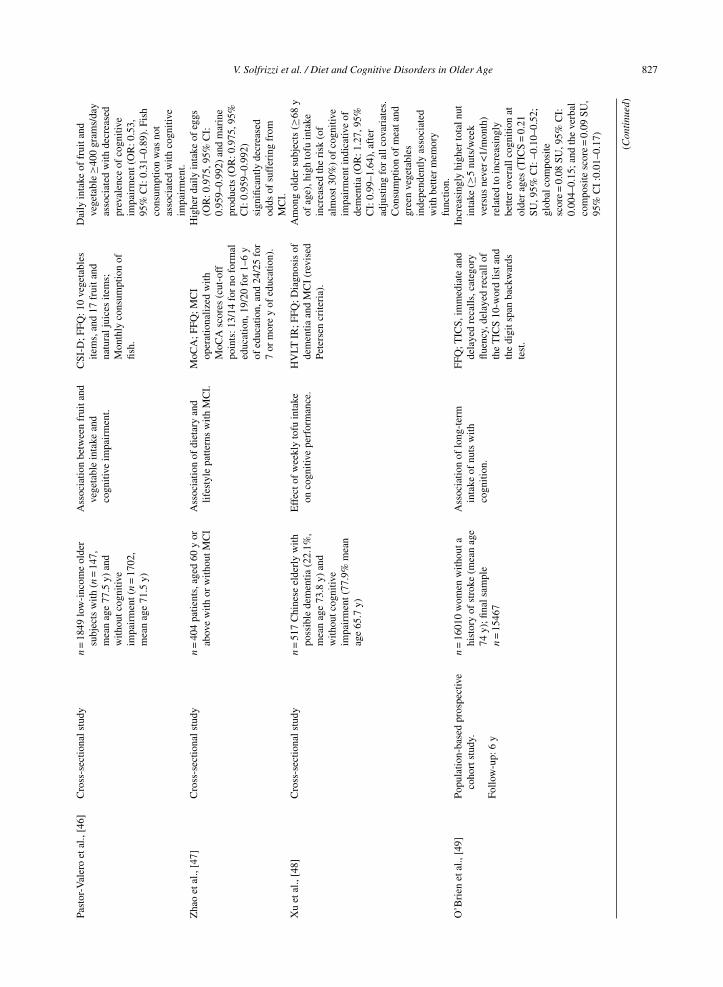
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 827Pa
stor
-Val
ero
etal
.,[4
6]C
ross
-sec
tiona
lstu
dyn
=18
49lo
w-i
ncom
eol
der
subj
ects
with
(n=
147,
mea
nag
e77
.5y)
and
with
outc
ogni
tive
impa
irm
ent(
n=
1702
,m
ean
age
71.5
y)
Ass
ocia
tion
betw
een
frui
tand
vege
tabl
ein
take
and
cogn
itive
impa
irm
ent.
CSI
-D;F
FQ:1
0ve
geta
bles
item
s,an
d17
frui
tand
natu
ralj
uice
site
ms;
Mon
thly
cons
umpt
ion
offis
h.
Dai
lyin
take
offr
uita
ndve
geta
ble≥4
00gr
ams/
day
asso
ciat
edw
ithde
crea
sed
prev
alen
ceof
cogn
itive
impa
irm
ent(
OR
:0.5
3,95
%C
I:0.
31–0
.89)
.Fis
hco
nsum
ptio
nw
asno
tas
soci
ated
with
cogn
itive
impa
irm
ent.
Zha
oet
al.,
[47]
Cro
ss-s
ectio
nals
tudy
n=
404
patie
nts,
aged
60y
orab
ove
with
orw
ithou
tMC
IA
ssoc
iatio
nof
diet
ary
and
lifes
tyle
patte
rns
with
MC
I.M
oCA
;FFQ
;MC
Iop
erat
iona
lized
with
MoC
Asc
ores
(cut
-off
poin
ts:1
3/14
for
nofo
rmal
educ
atio
n,19
/20
for
1–6
yof
educ
atio
n,an
d24
/25
for
7or
mor
ey
ofed
ucat
ion)
.
Hig
her
daily
inta
keof
eggs
(OR
:0.9
75,9
5%C
I:0.
959–
0.99
2)an
dm
arin
epr
oduc
ts(O
R:0
.975
,95%
CI:
0.95
9–0.
992)
sign
ifica
ntly
decr
ease
dod
dsof
suff
erin
gfr
omM
CI.
Xu
etal
.,[4
8]C
ross
-sec
tiona
lstu
dyn
=51
7C
hine
seel
derl
yw
ithpo
ssib
lede
men
tia(2
2.1%
,m
ean
age
73.8
y)an
dw
ithou
tcog
nitiv
eim
pair
men
t(77
.9%
mea
nag
e65
.7y)
Eff
ecto
fw
eekl
yto
fuin
take
onco
gniti
vepe
rfor
man
ce.
HV
LTIR
;FFQ
;Dia
gnos
isof
dem
entia
and
MC
I(r
evis
edPe
ters
encr
iteri
a).
Am
ong
olde
rsu
bjec
ts(≥
68y
ofag
e),h
igh
tofu
inta
kein
crea
sed
the
risk
(of
alm
ost3
0%)
ofco
gniti
veim
pair
men
tind
icat
ive
ofde
men
tia(O
R:1
.27,
95%
CI:
0.99
–1.6
4),a
fter
adju
stin
gfo
ral
lcov
aria
tes.
Con
sum
ptio
nof
mea
tand
gree
nve
geta
bles
inde
pend
ently
asso
ciat
edw
ithbe
tter
mem
ory
func
tion.
O’B
rien
etal
.,[4
9]Po
pula
tion-
base
dpr
ospe
ctiv
eco
hort
stud
y.n
=16
010
wom
enw
ithou
tahi
stor
yof
stro
ke(m
ean
age
74y)
;fina
lsam
ple
n=
1546
7
Ass
ocia
tion
oflo
ng-t
erm
inta
keof
nuts
with
cogn
ition
.
FFQ
;TIC
S,im
med
iate
and
dela
yed
reca
lls,c
ateg
ory
fluen
cy,d
elay
edre
call
ofth
eT
ICS
10-w
ord
lista
ndth
edi
gits
pan
back
war
dste
st.
Incr
easi
ngly
high
erto
taln
utin
take
(≥5
nuts
/wee
kve
rsus
neve
r<1/
mon
th)
rela
ted
toin
crea
sing
lybe
tter
over
allc
ogni
tion
atol
der
ages
(TIC
S=
0.21
SU,9
5%C
I:–0
.10–
0.52
;gl
obal
com
posi
tesc
ore
=0.
08SU
,95%
CI:
0.00
4–0.
15;a
ndth
eve
rbal
com
posi
tesc
ore
=0.
09SU
,95
%C
I:0
.01–
0.17
)
Follo
w-u
p:6
y
(Con
tinu
ed)
828 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
Tabl
e2
(Con
tinu
ed)
Ref
eren
ces
Stud
yD
esig
nSa
mpl
eO
utco
me
Cog
nitiv
ean
dN
utri
tiona
lA
sses
smen
tPr
inci
palR
esul
ts
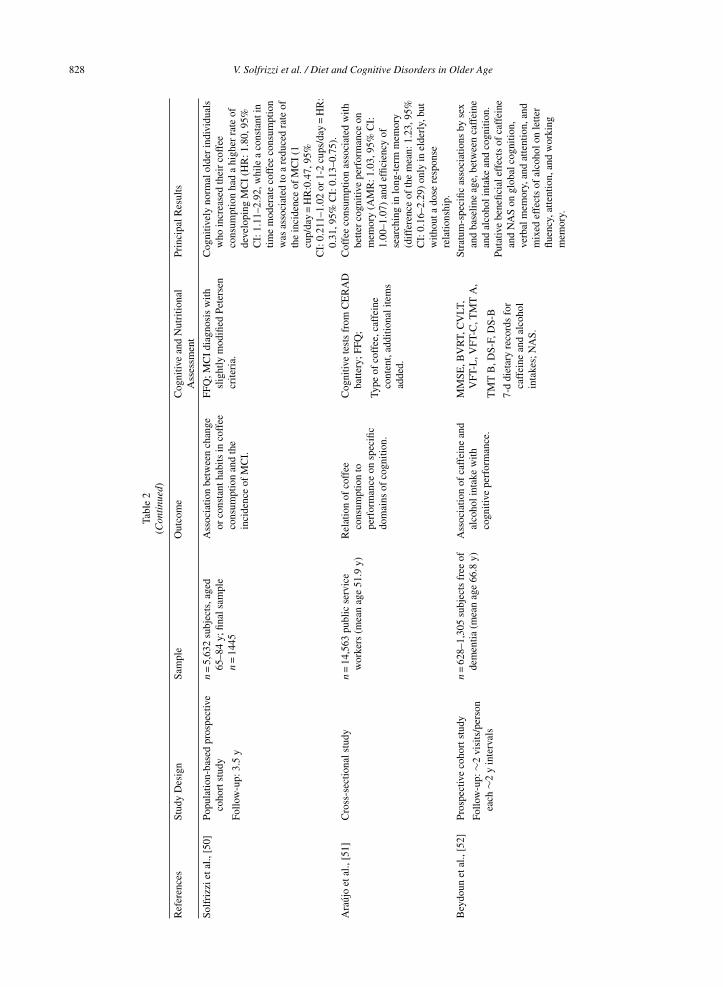
Solf
rizz
ieta
l.,[5
0]Po
pula
tion-
base
dpr
ospe
ctiv
eco
hort
stud
yn
=5,
632
subj
ects
,age
d65
–84
y;fin
alsa
mpl
en
=14
45
Ass
ocia
tion
betw
een
chan
geor
cons
tant
habi
tsin
coff
eeco
nsum
ptio
nan
dth
ein
cide
nce
ofM
CI.
FFQ
;MC
Idi
agno
sis
with
slig
htly
mod
ified
Pete
rsen
crite
ria.
Cog
nitiv
ely
norm
alol
der
indi
vidu
als
who
incr
ease
dth
eir
coff
eeco
nsum
ptio
nha
da
high
erra
teof
deve
lopi
ngM
CI
(HR
:1.8
0,95
%C
I:1.
11–2
.92,
whi
lea
cons
tant
intim
em
oder
ate
coff
eeco
nsum
ptio
nw
asas
soci
ated
toa
redu
ced
rate
ofth
ein
cide
nce
ofM
CI
(1cu
p/da
y=
HR
:0.4
7,95
%
Follo
w-u
p:3.
5y
CI:
0.21
1–1.
02or
1-2
cups
/day
=H
R:
0.31
,95%
CI:
0.13
–0.7
5).
Ara
ujo
etal
.,[5
1]C
ross
-sec
tiona
lstu
dyn
=14
,563
publ
icse
rvic
ew
orke
rs(m
ean
age
51.9
y)R
elat
ion
ofco
ffee
cons
umpt
ion
tope
rfor
man
ceon
spec
ific
dom
ains
ofco
gniti
on.
Cog
nitiv
ete
sts
from
CE
RA
Dba
ttery
;FFQ
;C
offe
eco
nsum
ptio
nas
soci
ated
with
bette
rco
gniti
vepe
rfor
man
ceon
mem
ory
(AM
R:1
.03,
95%
CI:
1.00
–1.0
7)an
def
ficie
ncy
ofse
arch
ing
inlo
ng-t
erm
mem
ory
(dif
fere
nce
ofth
em
ean:
1.23
,95%
CI:
0.16
–2.2
9)on
lyin
elde
rly,
but
with
outa
dose
resp
onse
rela
tions
hip.
Type
ofco
ffee
,caf
fein
eco
nten
t,ad
ditio
nali
tem
sad
ded.
Bey
doun
etal
.,[5
2]Pr
ospe
ctiv
eco
hort
stud
yn
=62
8–1,
305
subj
ects
free
ofde
men
tia(m
ean
age
66.8
y)A
ssoc
iatio
nof
caff
eine
and
alco
holi
ntak
ew
ithco
gniti
vepe
rfor
man
ce.
MM
SE,B
VR
T,C
VLT
,V
FT-L
,VFT
-C,T
MT
A,
Stra
tum
-spe
cific
asso
ciat
ions
byse
xan
dba
selin
eag
e,be
twee
nca
ffei
nean
dal
coho
lint
ake
and
cogn
ition
.Fo
llow
-up:
∼2vi
sits
/per
son
each
∼2y
inte
rval
sT
MT
B,D
S-F,
DS-
BPu
tativ
ebe
nefic
iale
ffec
tsof
caff
eine
and
NA
Son
glob
alco
gniti
on,
verb
alm
emor
y,an
dat
tent
ion,
and
mix
edef
fect
sof
alco
holo
nle
tter
fluen
cy,a
ttent
ion,
and
wor
king
mem
ory.
7-d
diet
ary
reco
rds
for
caff
eine
and
alco
hol
inta
kes;
NA
S.
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 829
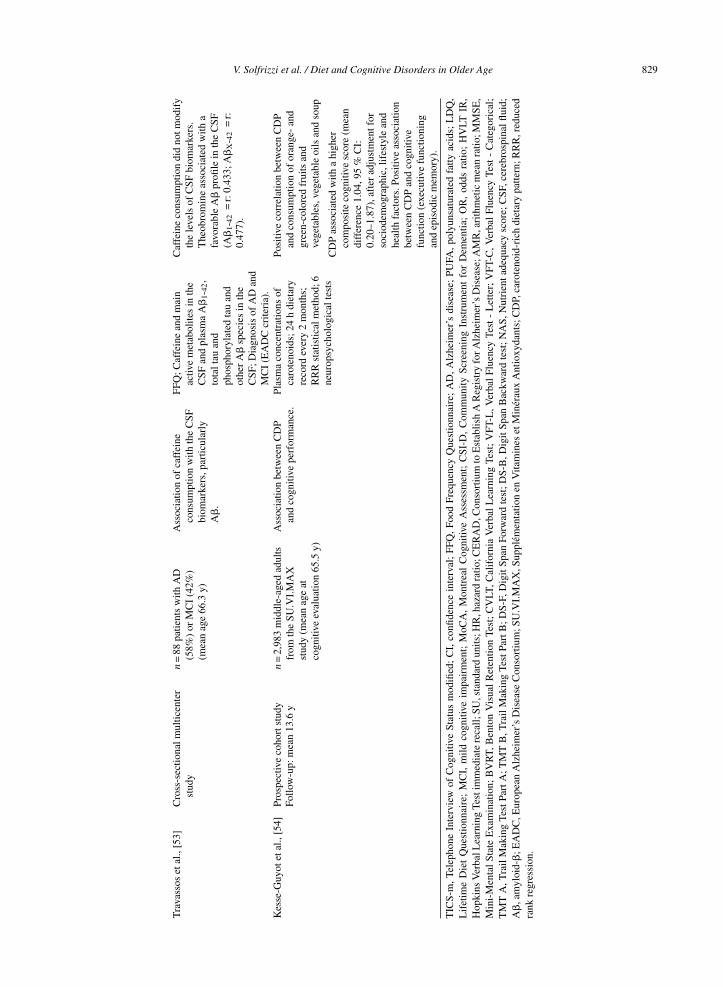
Tra
vass
oset
al.,
[53]
Cro
ss-s
ectio
nalm
ultic
ente
rst
udy
n=
88pa
tient
sw
ithA
D(5
8%)
orM
CI
(42%
)(m
ean
age
66.3
y)
Ass
ocia
tion
ofca
ffei
neco
nsum
ptio
nw
ithth
eC
SFbi
omar
kers
,par
ticul
arly
A�
.
FFQ
;Caf
fein
ean
dm
ain
activ
em
etab
olite
sin
the
CSF
and
plas
ma
A�
1-42
,to
talt
auan
dph
osph
oryl
ated
tau
and
othe
rA
�sp
ecie
sin
the
CSF
;Dia
gnos
isof
AD
and
MC
I(E
AD
Ccr
iteri
a).
Caf
fein
eco
nsum
ptio
ndi
dno
tmod
ify
the
leve
lsof
CSF
biom
arke
rs.
The
obro
min
eas
soci
ated
with
afa
vora
ble
A�
profi
lein
the
CSF
(A�
1-42
=r:
0.43
3;A
�X
-42
=r:
0.47
7).
Kes
se-G
uyot
etal
.,[5
4]Pr
ospe
ctiv
eco
hort
stud
yn
=2,
983
mid
dle-
aged
adul
tsfr
omth
eSU
.VI.
MA
Xst
udy
(mea
nag
eat
cogn
itive
eval
uatio
n65
.5y)
Ass
ocia
tion
betw
een
CD
Pan
dco
gniti
vepe
rfor
man
ce.
Plas
ma
conc
entr
atio
nsof
caro
teno
ids;
24h
diet
ary
reco
rdev
ery
2m
onth
s;R
RR
stat
istic
alm
etho
d;6
neur
opsy
chol
ogic
alte
sts
Posi
tive
corr
elat
ion
betw
een
CD
Pan
dco
nsum
ptio
nof
oran
ge-
and
gree
n-co
lore
dfr
uits
and
vege
tabl
es,v
eget
able
oils
and
soup
Follo
w-u
p:m
ean
13.6
y
CD
Pas
soci
ated
with
ahi
gher
com
posi
teco
gniti
vesc
ore
(mea
ndi
ffer
ence
1.04
,95
%C
I:0.
20–1
.87)
,aft
erad
just
men
tfor
soci
odem
ogra
phic
,lif
esty
lean
dhe
alth
fact
ors.
Posi
tive
asso
ciat
ion
betw
een
CD
Pan
dco
gniti
vefu
nctio
n(e
xecu
tive
func
tioni
ngan
dep
isod
icm
emor
y).
TIC
S-m
,Tel
epho
neIn
terv
iew
ofC
ogni
tive
Stat
usm
odifi
ed;
CI,
confi
denc
ein
terv
al;
FFQ
,Foo
dFr
eque
ncy
Que
stio
nnai
re;
AD
,Alz
heim
er’s
dise
ase;
PUFA
,pol
yuns
atur
ated
fatty
acid
s;L
DQ
,L
ifet
ime
Die
tQ
uest
ionn
aire
;M
CI,
mild
cogn
itive
impa
irm
ent;
MoC
A,
Mon
trea
lC
ogni
tive
Ass
essm
ent;
CSI
-D,
Com
mun
itySc
reen
ing
Inst
rum
ent
for
Dem
entia
;O
R,
odds
ratio
;H
VLT
IR,
Hop
kins
Ver
balL
earn
ing
Test
imm
edia
tere
call;
SU,s
tand
ard
units
;HR
,haz
ard
ratio
;CE
RA
D,C
onso
rtiu
mto
Est
ablis
hA
Reg
istr
yfo
rAlz
heim
er’s
Dis
ease
;AM
R,a
rith
met
icm
ean
ratio
;MM
SE,
Min
i-M
enta
lSt
ate
Exa
min
atio
n;B
VR
T,B
ento
nV
isua
lR
eten
tion
Test
;C
VLT
,Cal
ifor
nia
Ver
bal
Lea
rnin
gTe
st;
VFT
-L,V
erba
lFl
uenc
yTe
st-
Let
ter;
VFT
-C,V
erba
lFl
uenc
yTe
st-
Cat
egor
ical
;T
MT
A,T
rail
Mak
ing
Test
Part
A;T
MT
B,T
rail
Mak
ing
Test
Part
B;D
S-F,
Dig
itSp
anFo
rwar
dte
st;D
S-B
,Dig
itSp
anB
ackw
ard
test
;NA
S,N
utri
enta
dequ
acy
scor
e;C
SF,c
ereb
rosp
inal
fluid
;A
�,a
myl
oid-
�;E
AD
C,E
urop
ean
Alz
heim
er’s
Dis
ease
Con
sort
ium
;SU
.VI.
MA
X,S
uppl
emen
tatio
nen
Vita
min
eset
Min
erau
xA
ntio
xyda
nts;
CD
P,ca
rote
noid
-ric
hdi
etar
ypa
ttern
;RR
R,r
educ
edra
nkre
gres
sion
.

830 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
temporal, and inferior parietal, and marginally associ-ated with fusiform CT [34]. Higher fish consumptionwas also related with larger total gray matter vol-ume [35]. Fish consumption was also associatedwith a slower decline in composite and verbal mem-ory scores [42] (Table 2). Of note, Danthiir andcolleagues demonstrated that more frequent con-sumption of total fish (oily and white) was associatedwith slower cognitive speed for the constructs ofinhibition, simple/choice reaction time, reasoningspeed, and memory scanning [44] (Table 2). Morefrequent consumption of oily fish was significantlyassociated with worse inhibitory processes; similarly,consumption of white fish significantly and nega-tively predicted simple/choice reaction time [44].Danthiir and colleagues hypothesized that the nega-tive trends observed between cognitive performanceand fish consumption were due to neurotoxic contam-inants in fish, such as methylmercury [44]. However,as seen above, Morris and colleagues found thathigher brain levels of mercury were not correlatedwith brain neuropathology [43] (Table 2). Otherstudies did not suggest evidence that higher fishintake may impact positively cognitive performancein older adults with cognitive impairment [45, 46]or in those cognitively normal [46, 47] (Table 2).However, Dong and colleagues found that cognitivelynormal Chinese older subjects consumed more fishthan MCI subjects [45], and Zhao and colleaguessuggested that higher consumption of marine productwas associated with a significantly decreased odd ofsuffering from MCI [47], although in these two Chi-nese studies, MCI was diagnosed only on the basisof a screening cognitive test (the Montreal CognitiveAssessment - MoCA) and not with clinical criteria(Table 2).
Fruits and vegetablesIn Greece, in the EPIC study, among the compo-
nents of MeDi, only vegetable consumption exhibiteda significant inverse association with cognitivedecline [27] (Table 1). The diet low in fruit and veg-etable might increase the risk of cognitive functiondecline in older adults [45] (Table 2). In fact, adher-ence to WHO recommendations for daily intakes offruit and vegetable, that are eating 5 or more por-tions of fruit and/or vegetables a day (≥400 g/day),were significantly associated with a 47% decreasedprevalence of cognitive impairment [45]. In contrastto these findings, Xu and colleagues found that amongolder adults (≥68 y) being vegetarian (not eatingmeat), the risk for cognitive impairment increased
almost 4-fold [48] (Table 2). Imaging data in oldercohort showed that higher intake of total vegeta-bles was associated with larger dorsolateral prefrontaland superior parietal cortical thickness, while veg-etables without legumes were associated with largermiddle temporal, superior parietal, and dorsolateralprefrontal cortical thickness [35] (Table 1). In con-trast, fruit consumption was negatively associatedwith inferior parietal, supramarginal, superior pari-etal, parietal, and precuneus cortical thickness [35].These findings are in keeping with result of anotherstudy in which higher fruit intake was associatedwith lower temporal and hippocampal volumes [36](Table 1). This is probably due to high content ofsimple sugars and a high glycemic index of severalfruits and so the effects of carbohydrate componenton increased risk of MCI [73]. In older adults, fruitintake would benefit name ability and attention level,while vegetables intake would benefit orientationability [45] (Table 2). Finally, consumption of greenvegetables was independently associated with bettermemory function and among older elderly (≥68 y) itreduced the risk for cognitive impairment by almost20% [48] (Table 2).
NutsNuts are rich in PUFA (n-3 and n-6) and MUFA,
and also contain a significant amount of minerals,such as phosphorus, potassium, magnesium, calcium,iron, and sulfur, and vitamins, such as B1, B2, B6,and E. It was found the nut intake of MCI patientswas less than that of cognitively normal subjects[45] (Table 2). In fact, a study performed on olderwomen found that higher total nut intake (i.e.,≥5/week) over the long term was associated withmodestly better cognitive performance [49](Table 2).Increasingly higher total nut intake was related toincreasingly better overall cognition at older age.Considering that one year of age was associated witha mean decline of 0.04 standard units on both theglobal and verbal composite scores, the mean dif-ferences comparing the highest to lowest categoriesof nut intake were equivalent to approximately twoyears of cognitive aging [49]. In the same study, itwas found a suggestion that those who consumedwalnuts 1 to 3 times per month had better cogni-tion than those who consumed walnuts less than onceper month, but there was no overall trend of increas-ingly better cognitive performance with increasingwalnut intake [49]. Dong and colleagues also showedthat nut intake benefited delayed memory [45](Table 2).

V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 831
Coffee and caffeine intakeA recent systematic review suggested that several
cross-sectional and longitudinal population-basedstudies suggested a protective effect of coffee, tea,and caffeine use against late-life cognitive impair-ment/decline, although the association was not foundin all cognitive domains investigated and there wasa lack of a distinct dose-response association, witha stronger effect among women than men [74]. Thefindings on the association of coffee, tea, and caffeineconsumption or plasma caffeine levels with incidentMCI and its progression to dementia were too limitedto draw any conclusion [74]. Furthermore, for demen-tia and AD prevention, some studies with baselineexamination in midlife pointed to a lack of associ-ation, although other case-control and longitudinalpopulation-based studies with briefer follow-up peri-ods supported favorable effects of coffee, tea, andcaffeine consumption against AD [74]. Recent find-ings from the Italian Longitudinal Study on Aging(ILSA) suggested that cognitively normal older indi-viduals who increased their coffee consumption hada higher rate of developing MCI, while a constant intime moderate coffee consumption was associated toa reduced rate of the incidence of MCI [50] (Table 2).Among older adults in Brazil, coffee consumptionwas associated with better cognitive performance onmemory and efficiency of searching in long-termmemory (drinking 2–3 cups of coffee per day wasassociated with about a 3% increase in the mean num-ber of words remembered on the learning, recall, andword recognition tests) [51] (Table 2). Also, drink-ing ≥3 cups/day of coffee was associated with anincrease of about 1.23 words in the mean number ofwords pronounced in the semantic verbal fluency test[51]. However, in this Brazilian study, Araujio andcolleagues did not find indication of a dose responserelationship in these associations [51]. In the Chi-nese study on cognitively normal and MCI adultsof Dong and colleagues, no significant associationwas detected between drinking of coffee and cogni-tive function [45] (Table 2). Another aspect of coffeeassumption is the role of its component such as thecaffeine. Coffee is a rich source of caffeine, whichacts as a psychoactive stimulant. In a cross sectionalanalysis, Beydoun and colleagues found that caffeineintake was associated with better global cognitivefunction (MMSE) at baseline for patients ≥70 years[52] (Table 2). However, in a study that evaluated theassociation of caffeine consumption with the cere-brospinal fluid (CSF) biomarkers, particularly A�,in AD and MCI patients, no significant difference
was found in daily consumption of caffeine betweenMCI and AD patients, with no correlation betweencaffeine consumption and A�1-42 in the CSF [53](Table 2). In the same study, theobromine, xanthineformed upon caffeine metabolism and also directlyingested from chocolate products, was associatedwith a favorable A� profile in the CSF [53]. Inter-estingly, theobromine in the CSF did not correlatewith caffeine consumption, theobromine consump-tion, or the levels of caffeine and other xanthines inthe plasma, but instead it correlated with levels ofcaffeine, theophylline, and paraxanthine in the CSF,suggesting that it may be formed by central metabolicpathways [53].
EggsEggs have a high content of proteins and lipids, in
particular cholesterol. For this reason, they are tra-ditionally considered an unhealthy food. However,eggs have also a significant amount of vitamins A,B6, B12, riboflavin, folic acid, choline, iron, calcium,phosphorus and potassium. In a recent study, higherdaily intake of eggs reduced of about 3% the oddsof suffering from MCI [47] (Table 2). Instead, in theChinese study of Dong and colleagues, no signifi-cant association was detected between intake of eggswith cognitive function in normal and MCI adults[45] (Table 2).
TofuTofu is a common food in most of the Far East. It
is obtained from curdling of the juice extracted fromsoybeans. It has a high protein and PUFA content.Higher weekly intake of tofu was associated withworse memory performance, furthermore amongolder elderly (≥68 y), high tofu intake increases therisk (of almost 30%) of cognitive impairment indica-tive of dementia [48] (Table 2).
MeatRed meat is a classical element of Western diet that,
as mentioned previously, was associated with worsecognitive performance in several imaging studies [37,39, 41] (Table 1). Consistent with these findings, anegative association of red meat with inferior andsuperior parietal cortical thickness was found [35](Table 1). However, this concept should be partiallyreviewed. In fact, in the last years, eating meat (notbeing vegetarian) was independently associated withbetter memory function and in older age (≥68 y)with a four-fold decrease in risk of possible dementia[48] (Table 2). Furthermore, Staubo and colleagues

832 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
also observed that higher red meat intake was asso-ciated with larger entorhinal cortical thickness [35](Table 1). This effect could also be related to somebeneficial components of lean red meat (iron, protein,MUFA, PUFA, cobalamine) and beneficial effects inincreasing satiety and reducing weight gain. In theChinese study of Dong and colleagues, no significantassociation was detected between intake of light orred meat with cognitive function in normal and MCIadults [45] (Table 2).
OilDong and colleagues, in their Chinese cohort,
found that oil intake of MCI patients was lessthan the normal subjects (29.76 versus 35.20 mLcooking oil per day), and, in particular, wouldhave a positive impact on visual-spatial ability [45](Table 2). Vegetable oils are rich in carotenoids, andin the Supplementation en Vitamines et MinerauxAntioxydants (SU.VI.MAX) study carotenoids wereassociated with higher cognitive performance [54](Table 2). Extra-virgin olive oil (EVOO) is one ofthe main elements of MeDi, and clinical trials andpopulation studies indicated that this dietary patternand its main lipid component EVOO could have aprotective role against AD [75].
LegumesDong and colleagues, in their Chinese cohort,
showed that normal subjects consumed more legumesand legume products than MCI subjects, demonstrat-ing that intake of legumes and legume products wouldbenefit overall cognition level [45] (Table 2). Thesedata were confirmed by imaging biomarkers; in fact,Staubo and colleagues also found that higher intakeof legumes was associated with larger parietal andoccipital cortical thickness, and with larger thicknessin ROIs for superior parietal, inferior parietal, pre-cuneus, and lingual cortical thickness [35] (Table 1).
GrainsIn their imaging biomarker study, Staubo and col-
leagues also showed that intake of whole grains orcereals was associated with larger temporal pole andsuperior temporal cortical thickness [35] (Table 1).Conversely, lower intake of whole grains was associ-ated with higher inflammatory markers (IL-6) andaccelerated cognitive decline at older age in theWhitehall II prospective cohort study [41] (Table 1).However, in the Chinese cohort of Dong and col-leagues, no significant association was detected
between intake of whole grains and cognitive func-tion in normal and MCI adults [45] (Table 2).
AlcoholRecent findings from the Baltimore Longitudinal
Study of Aging suggested that alcohol intake wasassociated with slower improvement on letter flu-ency and global cognition among those aged <70years at baseline [52] (Table 2). Conversely, alco-hol intake was associated with better attention andworking memory performance, particularly amongmen and individuals ≥70 years at baseline [52]. Com-pared with moderate consumption (14 to 28 g/d),individuals with higher alcohol intake (>28 g/d) hadfaster decline or slower improvement on the MMSE,particularly among women and in the older group.Overall, among men, and for those aged ≥70 years,lower alcohol intake (<14 g/d) compared with mod-erate consumption (14 to 28 g/d) was associated withpoorer performance in working memory [52]. In theyounger group, consuming <14 g/day was associatedwith slower decline or faster improvement in the let-ter fluency compared with a moderate intake of 14 to28 g/day. Similar pattern was showed also for atten-tion and executive functioning [52].
Relation of micro- and macronutrients withcognition in older age
Vitamin ETable 3 shows selected observational studies pub-
lished in the last three years and evaluating theassociation of micro- and macronutrients with late-life cognitive disorders [55–71]. Vitamin E is a potentantioxidant and seems to slow the effects of aging.It is found mainly in nuts, seeds, and oils. VitaminE is composed by four tocopherols (�-, �, δ, and�-tocopherols) and four corresponding tocotrienols,and it is known that �- and �-tocopherols foundin foods were linked to slower rate of cognitivedecline over a 6-year period [76]. More recently, inthe HANDLS study, Beydoun and colleagues inves-tigated the effects on cognitive domains of only oneof its isoform, �-tocopherol, showing that vitamin Ewas positively associated with performance in verbalmemory and fluency in the total population, partic-ularly among the younger age group (<48 y) andpsychomotor speed among women [55] (Table 3).
Vitamin DVitamin D deficiency is a common condition in
older adults. Furthermore, the detection of hydrox-
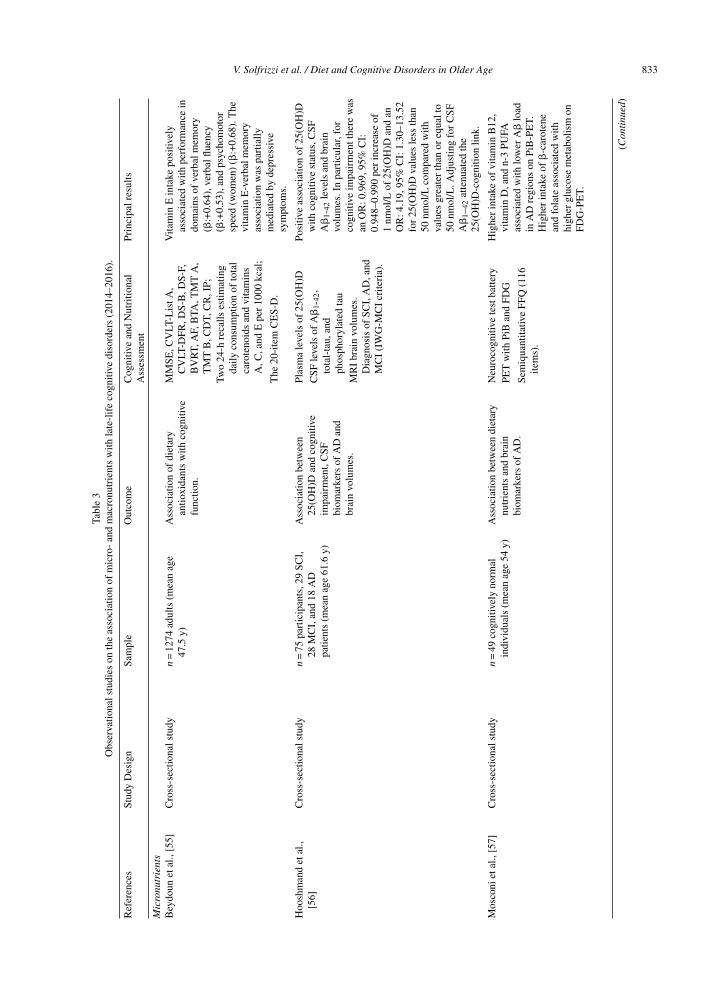
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 833
Tabl
e3
Obs
erva
tiona
lstu
dies
onth
eas
soci
atio
nof
mic
ro-
and
mac
ronu
trie
nts
with
late
-lif
eco
gniti
vedi
sord
ers
(201
4–20
16).
Ref
eren
ces
Stud
yD
esig
nSa
mpl
eO
utco
me
Cog
nitiv
ean
dN
utri
tiona
lPr
inci
palr
esul
tsA
sses
smen
t
Mic
ronu
trie
nts
Bey
doun
etal
.,[5
5]C
ross
-sec
tiona
lstu
dyn
=12
74ad
ults
(mea
nag
e47
.5y)
Ass
ocia
tion
ofdi
etar
yan
tioxi
dant
sw
ithco
gniti
vefu
nctio
n.
MM
SE,C
VLT
-Lis
tA,
CV
LT-D
FR,D
S-B
,DS-
F,B
VR
T,A
F,B
TA,T
MT
A,
TM
TB
,CD
T,C
R,I
P;
Vita
min
Ein
take
posi
tivel
yas
soci
ated
with
perf
orm
ance
indo
mai
nsof
verb
alm
emor
y(�
:+0.
64),
verb
alflu
ency
(�:+
0.53
),an
dps
ycho
mot
orsp
eed
(wom
en)
(�:+
0.68
).T
hevi
tam
inE
-ver
balm
emor
yas
soci
atio
nw
aspa
rtia
llym
edia
ted
byde
pres
sive
sym
ptom
s.
Two
24-h
reca
llses
timat
ing
daily
cons
umpt
ion
ofto
tal
caro
teno
ids
and
vita
min
sA
,C,a
ndE
per
1000
kcal
;
The
20-i
tem
CE
S-D
.
Hoo
shm
and
etal
.,[5
6]C
ross
-sec
tiona
lstu
dyn
=75
part
icip
ants
,29
SCI,
28M
CI,
and
18A
Dpa
tient
s(m
ean
age
61.6
y)
Ass
ocia
tion
betw
een
25(O
H)D
and
cogn
itive
impa
irm
ent,
CSF
biom
arke
rsof
AD
and
brai
nvo
lum
es.
Plas
ma
leve
lsof
25(O
H)D
Posi
tive
asso
ciat
ion
of25
(OH
)Dw
ithco
gniti
vest
atus
,CSF
A�
1-42
leve
lsan
dbr
ain
volu
mes
.In
part
icul
ar,f
orco
gniti
veim
pair
men
tthe
rew
asan
OR
:0.9
69,9
5%C
I:0.
948–
0.99
0pe
rin
crea
seof
1nm
ol/L
of25
(OH
)Dan
dan
OR
:4.1
9,95
%C
I:1.
30–1
3.52
for
25(O
H)D
valu
esle
ssth
an50
nmol
/Lco
mpa
red
with
valu
esgr
eate
rth
anor
equa
lto
50nm
ol/L
.Adj
ustin
gfo
rC
SFA
�1–
42at
tenu
ated
the
25(O
H)D
-cog
nitio
nlin
k.
CSF
leve
lsof
A�
1-42
,to
tal-
tau,
and
phos
phor
ylat
edta
uM
RI
brai
nvo
lum
es.
Dia
gnos
isof
SCI,
AD
,and
MC
I(I
WG
-MC
Icr
iteri
a).
Mos
coni
etal
.,[5
7]C
ross
-sec
tiona
lstu
dyn
=49
cogn
itive
lyno
rmal
indi
vidu
als
(mea
nag
e54
y)A
ssoc
iatio
nbe
twee
ndi
etar
ynu
trie
nts
and
brai
nbi
omar
kers
ofA
D.
Neu
roco
gniti
vete
stba
ttery
Hig
her
inta
keof
vita
min
B12
,vi
tam
inD
,and
n-3
PUFA
asso
ciat
edw
ithlo
wer
A�
load
inA
Dre
gion
son
PiB
-PE
T.H
ighe
rin
take
of�
-car
oten
ean
dfo
late
asso
ciat
edw
ithhi
gher
gluc
ose
met
abol
ism
onFD
G-P
ET.
PET
with
PiB
and
FDG
Sem
iqua
ntita
tive
FFQ
(116
item
s).
(Con
tinu
ed)
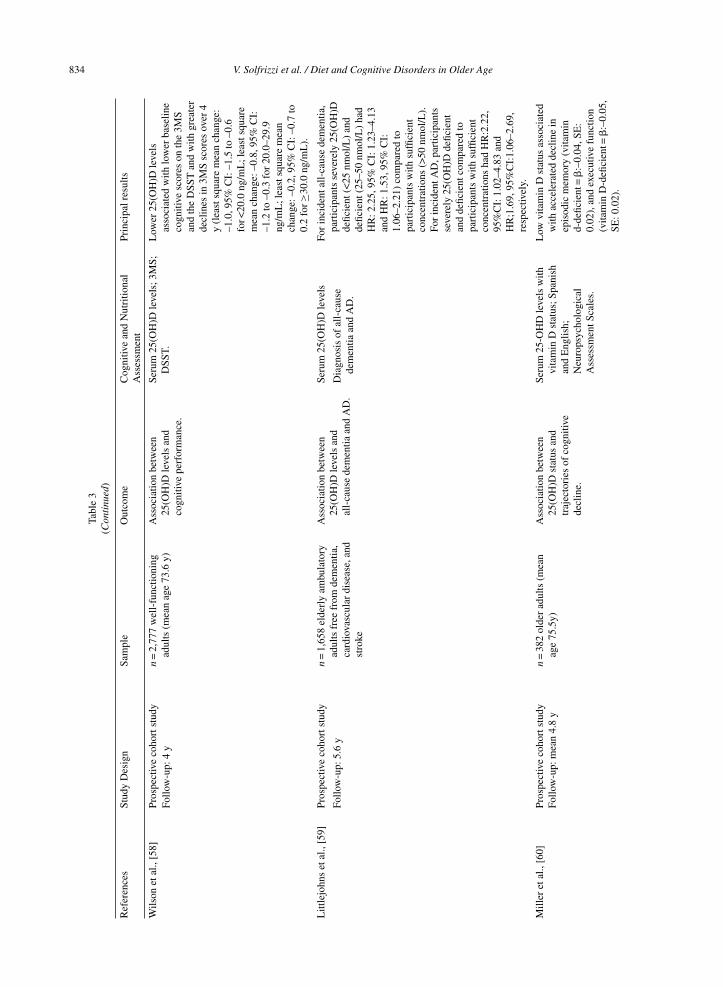
834 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
Tabl
e3
(Con
tinu
ed)
Ref
eren
ces
Stud
yD
esig
nSa
mpl
eO
utco
me
Cog
nitiv
ean
dN
utri
tiona
lPr
inci
palr
esul
tsA
sses
smen
t
Wils
onet
al.,
[58]
Pros
pect
ive
coho
rtst
udy
n=
2,77
7w
ell-
func
tioni
ngad
ults
(mea
nag
e73
.6y)
Ass
ocia
tion
betw
een
25(O
H)D
leve
lsan
dco
gniti
vepe
rfor
man
ce.
Seru
m25
(OH
)Dle
vels
;3M
S;D
SST.
Low
er25
(OH
)Dle
vels
asso
ciat
edw
ithlo
wer
base
line
cogn
itive
scor
eson
the
3MS
and
the
DSS
Tan
dw
ithgr
eate
rde
clin
esin
3MS
scor
esov
er4
y(l
east
squa
rem
ean
chan
ge:
–1.0
,95%
CI:
–1.5
to–0
.6fo
r<20
.0ng
/mL
;lea
stsq
uare
mea
nch
ange
:–0.
8,95
%C
I:–1
.2to
–0.3
for
20.0
–29.
9ng
/mL
;lea
stsq
uare
mea
nch
ange
:–0.
2,95
%C
I:–0
.7to
0.2
for≥
30.0
ng/m
L).
Follo
w-u
p:4
y
Litt
lejo
hns
etal
.,[5
9]Pr
ospe
ctiv
eco
hort
stud
yn
=1,
658
elde
rly
ambu
lato
ryad
ults
free
from
dem
entia
,ca
rdio
vasc
ular
dise
ase,
and
stro
ke
Ass
ocia
tion
betw
een
25(O
H)D
leve
lsan
dal
l-ca
use
dem
entia
and
AD
.
Seru
m25
(OH
)Dle
vels
For
inci
dent
all-
caus
ede
men
tia,
part
icip
ants
seve
rely
25(O
H)D
defic
ient
(<25
nmol
/L)
and
defic
ient
(25–
50nm
ol/L
)ha
dH
R:2
.25,
95%
CI:
1.23
–4.1
3an
dH
R:1
.53,
95%
CI:
1.06
–2.2
1)co
mpa
red
topa
rtic
ipan
tsw
ithsu
ffici
ent
conc
entr
atio
ns(>
50nm
ol/L
).Fo
rin
cide
ntA
D,p
artic
ipan
tsse
vere
ly25
(OH
)Dde
ficie
ntan
dde
ficie
ntco
mpa
red
topa
rtic
ipan
tsw
ithsu
ffici
ent
conc
entr
atio
nsha
dH
R:2
.22,
95%
CI:
1.02
–4.8
3an
dH
R;1
.69,
95%
CI:
1.06
–2.6
9,re
spec
tivel
y.
Follo
w-u
p:5.
6y
Dia
gnos
isof
all-
caus
ede
men
tiaan
dA
D.
Mill
eret
al.,
[60]
Pros
pect
ive
coho
rtst
udy
n=
382
olde
rad
ults
(mea
nag
e75
.5y)
Ass
ocia
tion
betw
een
25(O
H)D
stat
usan
dtr
ajec
tori
esof
cogn
itive
decl
ine.
Seru
m25
-OH
Dle
vels
with
vita
min
Dst
atus
;Spa
nish
and
Eng
lish;
Neu
rops
ycho
logi
cal
Ass
essm
entS
cale
s.
Low
vita
min
Dst
atus
asso
ciat
edw
ithac
cele
rate
dde
clin
ein
epis
odic
mem
ory
(vita
min
d-de
ficie
nt=
�:–
0.04
,SE
:0.
02),
and
exec
utiv
efu
nctio
n(v
itam
inD
-defi
cien
t=�
:–0.
05,
SE:0
.02)
.
Follo
w-u
p:m
ean
4.8
y
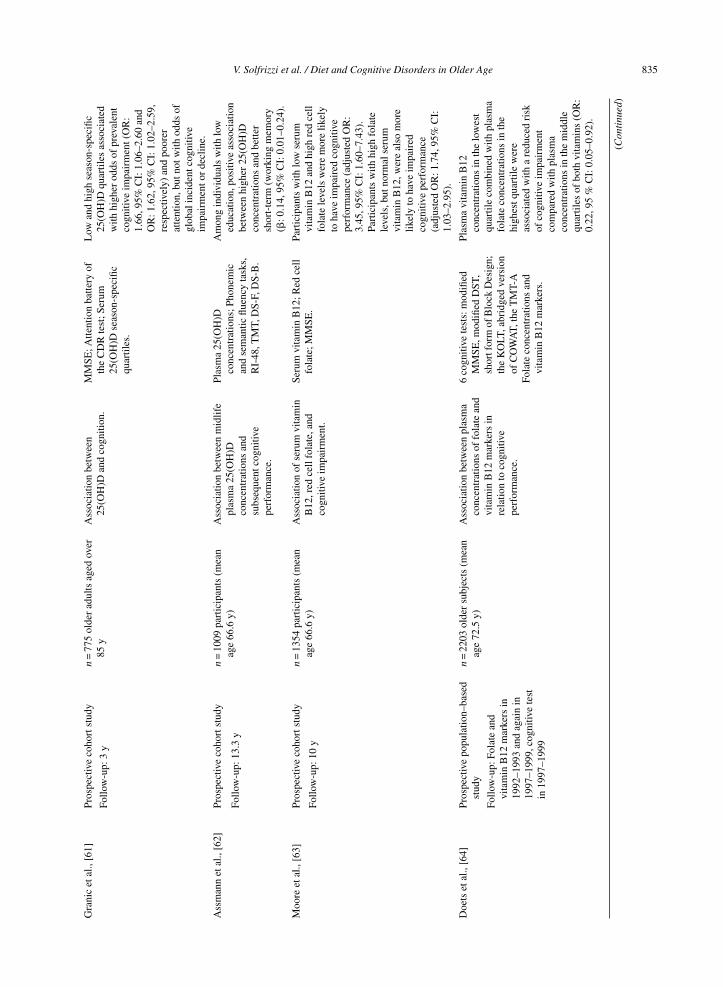
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 835
Gra
nic
etal
.,[6
1]Pr
ospe
ctiv
eco
hort
stud
yn
=77
5ol
der
adul
tsag
edov
er85
yA
ssoc
iatio
nbe
twee
n25
(OH
)Dan
dco
gniti
on.
MM
SE;A
ttent
ion
batte
ryof
the
CD
Rte
st;S
erum
25(O
H)D
seas
on-s
peci
ficqu
artil
es.
Low
and
high
seas
on-s
peci
fic25
(OH
)Dqu
artil
esas
soci
ated
with
high
erod
dsof
prev
alen
tco
gniti
veim
pair
men
t(O
R:
1.66
,95%
CI:
1.06
–2.6
0an
dO
R:1
.62,
95%
CI:
1.02
–2.5
9,re
spec
tivel
y)an
dpo
orer
atte
ntio
n,bu
tnot
with
odds
ofgl
obal
inci
dent
cogn
itive
impa
irm
ento
rde
clin
e.
Follo
w-u
p:3
y
Ass
man
net
al.,
[62]
Pros
pect
ive
coho
rtst
udy
n=
1009
part
icip
ants
(mea
nag
e66
.6y)
Ass
ocia
tion
betw
een
mid
life
plas
ma
25(O
H)D
conc
entr
atio
nsan
dsu
bseq
uent
cogn
itive
perf
orm
ance
.
Plas
ma
25(O
H)D
conc
entr
atio
ns;P
hone
mic
and
sem
antic
fluen
cyta
sks,
RI-
48,T
MT,
DS-
F,D
S-B
.
Am
ong
indi
vidu
als
with
low
educ
atio
n,po
sitiv
eas
soci
atio
nbe
twee
nhi
gher
25(O
H)D
conc
entr
atio
nsan
dbe
tter
shor
t-te
rm(w
orki
ngm
emor
y(�
:0.1
4,95
%C
I:0.
01–0
.24)
.
Follo
w-u
p:13
.3y
Moo
reet
al.,
[63]
Pros
pect
ive
coho
rtst
udy
n=
1354
part
icip
ants
(mea
nag
e66
.6y)
Ass
ocia
tion
ofse
rum
vita
min
B12
,red
cell
fola
te,a
ndco
gniti
veim
pair
men
t.
Seru
mvi
tam
inB
12;R
edce
llfo
late
;MM
SE.
Part
icip
ants
with
low
seru
mvi
tam
inB
12an
dhi
ghre
dce
llfo
late
leve
lsw
ere
mor
elik
ely
toha
veim
pair
edco
gniti
vepe
rfor
man
ce(a
djus
ted
OR
:3.
45,9
5%C
I:1.
60–7
.43)
.Pa
rtic
ipan
tsw
ithhi
ghfo
late
leve
ls,b
utno
rmal
seru
mvi
tam
inB
12,w
ere
also
mor
elik
ely
toha
veim
pair
edco
gniti
vepe
rfor
man
ce(a
djus
ted
OR
:1.7
4,95
%C
I:1.
03–2
.95)
.
Follo
w-u
p:10
y
Doe
tset
al.,
[64]
Pros
pect
ive
popu
latio
n–ba
sed
stud
yn
=22
03ol
der
subj
ects
(mea
nag
e72
.5y)
Ass
ocia
tion
betw
een
plas
ma
conc
entr
atio
nsof
fola
tean
dvi
tam
inB
12m
arke
rsin
rela
tion
toco
gniti
vepe
rfor
man
ce.
6co
gniti
vete
sts:
mod
ified
MM
SE,m
odifi
edD
ST,
shor
tfor
mof
Blo
ckD
esig
n;th
eK
OLT
,abr
idge
dve
rsio
nof
CO
WA
T,th
eT
MT-
A
Plas
ma
vita
min
B12
conc
entr
atio
nsin
the
low
est
quar
tile
com
bine
dw
ithpl
asm
afo
late
conc
entr
atio
nsin
the
high
estq
uart
ilew
ere
asso
ciat
edw
itha
redu
ced
risk
ofco
gniti
veim
pair
men
tco
mpa
red
with
plas
ma
conc
entr
atio
nsin
the
mid
dle
quar
tiles
ofbo
thvi
tam
ins
(OR
:0.
22,9
5%
CI:
0.05
–0.9
2).
Follo
w-u
p:Fo
late
and
vita
min
B12
mar
kers
in19
92–1
993
and
agai
nin
1997
–199
9,co
gniti
vete
stin
1997
–199
9
Fola
teco
ncen
trat
ions
and
vita
min
B12
mar
kers
.
(Con
tinu
ed)
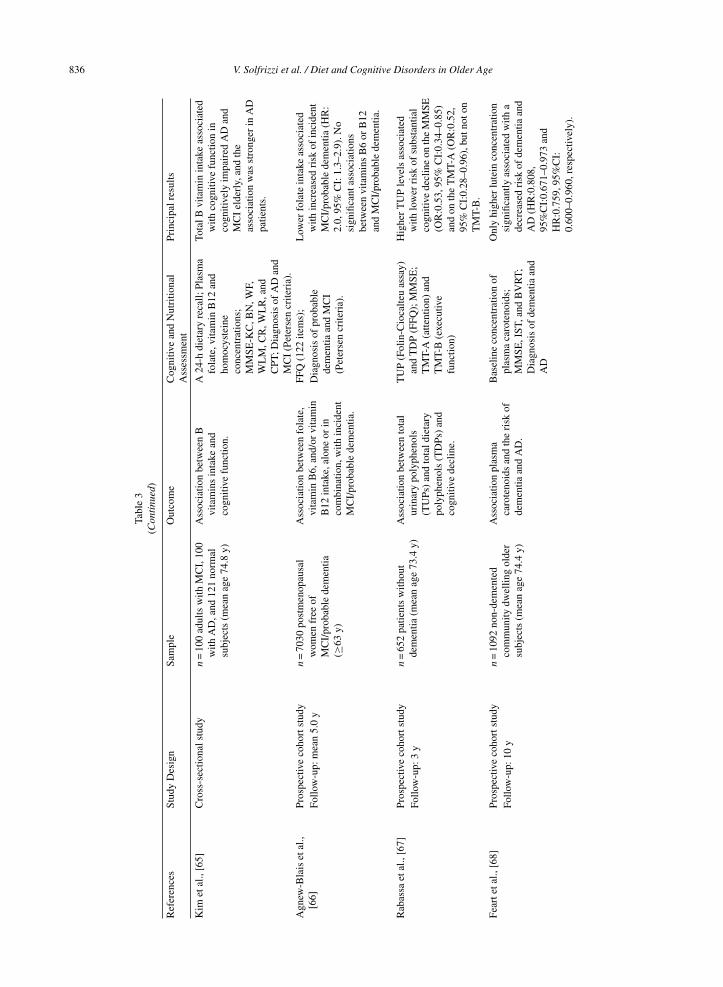
836 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
Tabl
e3
(Con
tinu
ed)
Ref
eren
ces
Stud
yD
esig
nSa
mpl
eO
utco
me
Cog
nitiv
ean
dN
utri
tiona
lPr
inci
palr
esul
tsA
sses
smen
t
Kim
etal
.,[6
5]C
ross
-sec
tiona
lstu
dyn
=10
0ad
ults
with
MC
I,10
0w
ithA
D,a
nd12
1no
rmal
subj
ects
(mea
nag
e74
.8y)
Ass
ocia
tion
betw
een
Bvi
tam
ins
inta
kean
dco
gniti
vefu
nctio
n.
A24
-hdi
etar
yre
call;
Plas
ma
fola
te,v
itam
inB
12an
dho
moc
yste
ine
conc
entr
atio
ns;
MM
SE-K
C,B
N,W
F,W
LM
,CR
,WL
R,a
ndC
PT;D
iagn
osis
ofA
Dan
dM
CI
(Pet
erse
ncr
iteri
a).
Tota
lBvi
tam
inin
take
asso
ciat
edw
ithco
gniti
vefu
nctio
nin
cogn
itive
lyim
pair
edA
Dan
dM
CI
elde
rly,
and
the
asso
ciat
ion
was
stro
nger
inA
Dpa
tient
s.
Agn
ew-B
lais
etal
.,[6
6]Pr
ospe
ctiv
eco
hort
stud
yn
=70
30po
stm
enop
ausa
lw
omen
free
ofM
CI/
prob
able
dem
entia
(≥63
y)
Ass
ocia
tion
betw
een
fola
te,
vita
min
B6,
and/
orvi
tam
inB
12in
take
,alo
neor
inco
mbi
natio
n,w
ithin
cide
ntM
CI/
prob
able
dem
entia
.
FFQ
(122
item
s);
Low
erfo
late
inta
keas
soci
ated
with
incr
ease
dri
skof
inci
dent
MC
I/pr
obab
lede
men
tia(H
R:
2.0,
95%
CI:
1.3–
2.9)
.No
sign
ifica
ntas
soci
atio
nsbe
twee
nvi
tam
ins
B6
orB
12an
dM
CI/
prob
able
dem
entia
.
Follo
w-u
p:m
ean
5.0
yD
iagn
osis
ofpr
obab
lede
men
tiaan
dM
CI
(Pet
erse
ncr
iteri
a).
Rab
assa
etal
.,[6
7]Pr
ospe
ctiv
eco
hort
stud
yn
=65
2pa
tient
sw
ithou
tde
men
tia(m
ean
age
73.4
y)A
ssoc
iatio
nbe
twee
nto
tal
urin
ary
poly
phen
ols
(TU
Ps)
and
tota
ldie
tary
poly
phen
ols
(TD
Ps)
and
cogn
itive
decl
ine.
TU
P(F
olin
-Cio
calte
uas
say)
and
TD
P(F
FQ);
MM
SE;
TM
T-A
(atte
ntio
n)an
dT
MT-
B(e
xecu
tive
func
tion)
Hig
her
TU
Ple
vels
asso
ciat
edw
ithlo
wer
risk
ofsu
bsta
ntia
lco
gniti
vede
clin
eon
the
MM
SE(O
R:0
.53,
95%
CI:
0.34
–0.8
5)an
don
the
TM
T-A
(OR
:0.5
2,95
%C
I:0.
28–0
.96)
,but
noto
nT
MT-
B.
Follo
w-u
p:3
y
Fear
teta
l.,[6
8]Pr
ospe
ctiv
eco
hort
stud
yn
=10
92no
n-de
men
ted
com
mun
itydw
ellin
gol
der
subj
ects
(mea
nag
e74
.4y)
Ass
ocia
tion
plas
ma
caro
teno
ids
and
the
risk
ofde
men
tiaan
dA
D.
Bas
elin
eco
ncen
trat
ion
ofpl
asm
aca
rote
noid
s;M
MSE
,IST
,and
BV
RT;
Dia
gnos
isof
dem
entia
and
AD
Onl
yhi
gher
lute
inco
ncen
trat
ion
sign
ifica
ntly
asso
ciat
edw
itha
decr
ease
dri
skof
dem
entia
and
AD
(HR
:0.8
08,
95%
CI:
0.67
1–0.
973
and
HR
:0.7
59,9
5%C
I:0.
600–
0.96
0,re
spec
tivel
y).
Follo
w-u
p:10
y
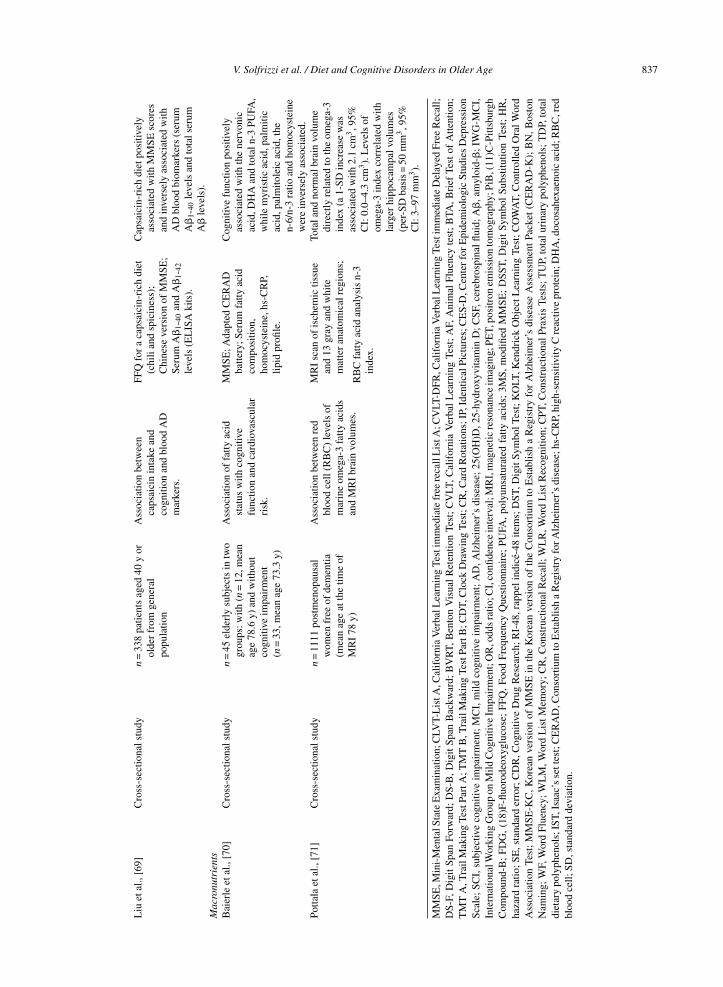
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 837
Liu
etal
.,[6
9]C
ross
-sec
tiona
lstu
dyn
=33
8pa
tient
sag
ed40
yor
olde
rfr
omge
nera
lpo
pula
tion
Ass
ocia
tion
betw
een
caps
aici
nin
take
and
cogn
ition
and
bloo
dA
Dm
arke
rs.
FFQ
for
aca
psai
cin-
rich
diet
(chi
lian
dsp
icin
ess)
;C
hine
seve
rsio
nof
MM
SE;
Seru
mA
�1-
40an
dA
�1-
42le
vels
(EL
ISA
kits
).
Cap
saic
in-r
ich
diet
posi
tivel
yas
soci
ated
with
MM
SEsc
ores
and
inve
rsel
yas
soci
ated
with
AD
bloo
dbi
omar
kers
(ser
umA
�1-
40le
vels
and
tota
lser
umA
�le
vels
).M
acro
nutr
ient
sB
aier
leet
al.,
[70]
Cro
ss-s
ectio
nals
tudy
n=
45el
derl
ysu
bjec
tsin
two
grou
ps:w
ith(n
=12
,mea
nag
e78
.6y)
and
with
out
cogn
itive
impa
irm
ent
(n=
33,m
ean
age
73.3
y)
Ass
ocia
tion
offa
ttyac
idst
atus
with
cogn
itive
func
tion
and
card
iova
scul
arri
sk.
MM
SE;A
dapt
edC
ER
AD
batte
ry;S
erum
fatty
acid
com
posi
tion,
hom
ocys
tein
e,hs
-CR
P,lip
idpr
ofile
.
Cog
nitiv
efu
nctio
npo
sitiv
ely
asso
ciat
edw
ithth
ene
rvon
icac
id,D
HA
and
tota
ln-3
PUFA
,w
hile
myr
istic
acid
,pal
miti
cac
id,p
alm
itole
icac
id,t
hen-
6/n-
3ra
tioan
dho
moc
yste
ine
wer
ein
vers
ely
asso
ciat
ed.
Potta
laet
al.,
[71]
Cro
ss-s
ectio
nals
tudy
n=
1111
post
men
opau
sal
wom
enfr
eeof
dem
entia
(mea
nag
eat
the
time
ofM
RI
78y)
Ass
ocia
tion
betw
een
red
bloo
dce
ll(R
BC
)le
vels
ofm
arin
eom
ega-
3fa
ttyac
ids
and
MR
Ibr
ain
volu
mes
.
MR
Isc
anof
isch
emic
tissu
ean
d13
gray
and
whi
tem
atte
ran
atom
ical
regi
ons;
Tota
land
norm
albr
ain
volu
me
dire
ctly
rela
ted
toth
eom
ega-
3in
dex
(a1-
SDin
crea
sew
asas
soci
ated
with
2.1
cm3,9
5%C
I:0.
0–4.
3cm
3).
Lev
els
ofom
ega-
3in
dex
corr
elat
edw
ithla
rger
hipp
ocam
palv
olum
es(p
er-S
Dba
sis=
50m
m3,9
5%C
I:3–
97m
m3).
RB
Cfa
ttyac
idan
alys
isn-
3in
dex.
MM
SE,M
ini-
Men
talS
tate
Exa
min
atio
n;C
LVT-
Lis
tA,C
alif
orni
aV
erba
lLea
rnin
gTe
stim
med
iate
free
reca
llL
istA
;CV
LT-D
FR,C
alif
orni
aV
erba
lLea
rnin
gTe
stim
med
iate
Del
ayed
Free
Rec
all;
DS-
F,D
igit
Span
Forw
ard;
DS-
B,D
igit
Span
Bac
kwar
d;B
VR
T,B
ento
nV
isua
lR
eten
tion
Test
;C
VLT
,Cal
ifor
nia
Ver
bal
Lea
rnin
gTe
st;
AF,
Ani
mal
Flue
ncy
test
;B
TA,B
rief
Test
ofA
ttent
ion;
TM
TA
,Tra
ilM
akin
gTe
stPa
rtA
;TM
TB
,Tra
ilM
akin
gTe
stPa
rtB
;CD
T,C
lock
Dra
win
gTe
st;C
R,C
ard
Rot
atio
ns;I
P,Id
entic
alPi
ctur
es;C
ES-
D,C
ente
rfo
rE
pide
mio
logi
cSt
udie
sD
epre
ssio
nSc
ale;
SCI,
subj
ectiv
eco
gniti
veim
pair
men
t;M
CI,
mild
cogn
itive
impa
irm
ent;
AD
,Alz
heim
er’s
dise
ase;
25(O
H)D
,25-
hydr
oxyv
itam
inD
;CSF
,cer
ebro
spin
alflu
id;A
�,a
myl
oid-
�;I
WG
-MC
I,In
tern
atio
nalW
orki
ngG
roup
onM
ildC
ogni
tive
Impa
irm
ent;
OR
,odd
sra
tio;C
I,co
nfide
nce
inte
rval
;MR
I,m
agne
ticre
sona
nce
imag
ing;
PET,
posi
tron
emis
sion
tom
ogra
phy;
PiB
,(11
)C-P
ittsb
urgh
Com
poun
d-B
;FD
G,
(18)
F-flu
orod
eoxy
gluc
ose;
FFQ
,Fo
odFr
eque
ncy
Que
stio
nnai
re;
PUFA
,po
lyun
satu
rate
dfa
ttyac
ids;
3MS,
mod
ified
MM
SE;
DSS
T,D
igit
Sym
bol
Subs
titut
ion
Test
;H
R,
haza
rdra
tio;S
E,s
tand
ard
erro
r;C
DR
,Cog
nitiv
eD
rug
Res
earc
h;R
I-48
,rap
peli
ndic
e-48
item
s;D
ST,D
igit
Sym
bolT
est;
KO
LT,K
endr
ick
Obj
ectL
earn
ing
Test
;CO
WA
T,C
ontr
olle
dO
ralW
ord
Ass
ocia
tion
Test
;M
MSE
-KC
,Kor
ean
vers
ion
ofM
MSE
inth
eK
orea
nve
rsio
nof
the
Con
sort
ium
toE
stab
lish
aR
egis
try
for
Alz
heim
er’s
dise
ase
Ass
essm
ent
Pack
et(C
ER
AD
-K);
BN
,Bos
ton
Nam
ing;
WF,
Wor
dFl
uenc
y;W
LM
,Wor
dL
istM
emor
y;C
R,C
onst
ruct
iona
lRec
all;
WL
R,W
ord
Lis
tRec
ogni
tion;
CPT
,Con
stru
ctio
nalP
raxi
sTe
sts;
TU
P,to
talu
rina
rypo
lyph
enol
s;T
DP,
tota
ldi
etar
ypo
lyph
enol
s;IS
T,Is
aac’
sse
ttes
t;C
ER
AD
,Con
sort
ium
toE
stab
lish
aR
egis
try
forA
lzhe
imer
’sdi
seas
e;hs
-CR
P,hi
gh-s
ensi
tivity
Cre
activ
epr
otei
n;D
HA
,doc
osah
exae
noic
acid
;RB
C,r
edbl
ood
cell;
SD,s
tand
ard
devi
atio
n.

838 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
ylases for vitamin D activation and vitamin Dreceptors in neurons and glia suggested that vitaminD might have a role in cognition. In fact, serum 25-hydroxyvitamin D [25(OH)D] was cross-sectionallyassociated with reduced A�1-42 concentrations inCSF [56] (Table 3). These findings were on the sameline of Mosconi and colleagues showing an asso-ciation of higher intake of vitamin D with lowerA� load in AD regions on PET with 11C-PittsburghCompound-B (PiB) [57] (Table 3). Vitamin D defi-ciency was also associated with greater decline inglobal cognitive function over 4 years of follow-up [58] (Table 3) and with a substantially increasedrisk of all-cause dementia and AD over a meanfollow-up of 5.6 years [59] (Table 3). In particular,vitamin D deficiency was related with significantlyfaster declines in both episodic memory and execu-tive function performance, the two cognitive domainsstrongly associated with AD dementia [60] (Table 3).However, Granic and colleagues found a U-shapedrelationship between 25(OH)D and global cognitivefunction and attention in the very old [61] (Table 3).In fact, both low and high season-specific quar-tiles of 25(OH)D were associated with higher oddsof prevalent cognitive impairment, poorer attentionreaction times/processing speed and focused atten-tion/concentration, and greater attention fluctuation[61]. Therefore, it could be hypothesized that theneuroprotective effects of vitamin D may be attainedonly at moderate but not at low or high 25(OH)Dconcentrations. On the other hand, very old sub-jects taking vitamin D supplements could be probablyonly recently advised by their physician to take vita-min D, perhaps due to an underlying vitamin Ddeficiency condition [77]. Finally, findings from theSU.VI.MAX study suggested a positive associationbetween higher 25(OH)D concentrations and bettershort-term and working memory only among individ-uals with low education [62] (Table 3).
Vitamins B and folateVitamin B12 deficiency has been associated with
neurological and psychiatric symptoms includingcognitive impairment [78]. Additionally, vitaminB12, along with folate and vitamin B6, are key actorsin the homocysteine cycle, and the disruption of thiscycle can lead to elevated homocysteine, which hasbeen found among individuals with dementia [79]and has been shown to predict dementia prospec-tively [80]. Despite potential biological mechanismsthrough which B vitamins could play a role in theonset of dementia, results from observational and
intervention studies have been inconsistent. In thelast three years, in imaging studies, higher intake offolate was associated with higher glucose metabolismon (18)F-fludeoxyglucose (FDG)-PET [57] (Table 3)and greater superior temporal cortical thickness [35](Table 1). Positive associations were also foundbetween vitamins B1 and B2 and superior tempo-ral and temporal pole cortical thickness, and vitaminB6 and superior temporal and middle temporal corti-cal thickness [35]. Higher intake of vitamin B12 wasalso associated with lower A� load in AD regionson PiB-PET. The association of vitamin B12 withPiB retention was independent of gender, APOE, andfamily history [57].
Data collected on 1,354 subjects from three Aus-tralian cohorts suggested that participants with lowserum vitamin B12 (<250 pmol/L) and high redcell folate (>1,594 nmol/L) levels were more likelyto have impaired cognitive performance when com-pared to participants with biochemical measurementsthat were within the normal ranges [63] (Table 3). Inthe same cohorts, participants with high folate lev-els, but normal serum vitamin B12, were also morelikely to have impaired cognitive performance [63].Furthermore, in the Hordaland Health Study, plasmavitamin B12 concentrations in the lowest quartile(<274 pmol/l) combined with plasma folate concen-trations in the highest quartile (>18·5 nmol/l) wereassociated with a reduced risk of cognitive impair-ment compared with plasma concentrations in themiddle quartiles of both vitamins [64] (Table 3).
In a cross-sectional study on older Koreans, inthe AD group, positive associations were observedbetween vitamin B2 intake and global cognitivestatus, language, verbal fluency, and verbal andpraxis memory; between vitamin B6 intake andglobal cognitive status, language, verbal fluency, ver-bal and praxis memory, and constructional praxis;between vitamin B12 intake and global cognitivestatus, language, praxis memory, and constructionalpraxis; and between folate intake and praxis mem-ory [65] (Table 3). In the MCI group, vitaminB2 intake was positively associated with globalcognitive status and language, vitamin B6 intakewas positively associated with language, and folateintake was positively associated with global cog-nitive status and verbal memory. No associationswere observed in the normal group [65]. Finally, inthe Women’s Health Initiative Memory Study, folateintake below the recommended daily allowance atstudy baseline was associated with increased riskof incident MCI/probable dementia, after controlling

V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 839
for multiple confounders [66] (Table 3). There wereno significant associations between vitamins B6 orB12 and MCI/probable dementia, nor any evidenceof an interaction between these vitamins and folateintake [66].
PolyphenolsPolyphenols are natural bioactive compounds that
have been identified in foods and beverages. They areassociated with neuroprotective activity probably dueto their antioxidant and anti-inflammatory properties.In the inCHIANTI study, in older adults with-out dementia, high concentrations of total urinarypolyphenols were associated with an approximately47% lower risk of substantial cognitive decline inglobal cognitive function and an approximately 48%lower risk of substantial cognitive decline in attentionover a 3-year period, but not with executive func-tion. No significant association was found betweentotal dietary polyphenols and any cognitive test [67](Table 3).
CarotenoidsCarotenoids are ubiquitous colored pigments,
found mainly in fruits and vegetables such as kiwi,carrots, and tomatoes or in green leafy vegetables.Among carotenoids, positive association was foundbetween higher intake of �-carotene and dorsolat-eral prefrontal and temporal pole cortical thickness[35] (Table 1) and with higher glucose metabolismon FDG-PET [57] (Table 3). However, the �-carotenelevels were related with reduced glucose metabolismfor women, APOE �4-carriers, and participants withpositive AD family history [57].
Among carotenoids, findings from the Three-City-Bordeaux cohort suggested that higher luteinconcentration, considered as a function of plasmalipids, was consistently significantly associated witha decreased risk of all-cause dementia and AD[68] (Table 3). Moreover, in the SU.VI.MAX study,a carotenoid-rich dietary pattern (CDP) stronglycorrelated with the plasma status of �-carotene, �-carotene, �-cryptoxanthin, and lutein, was positivelycorrelated with the consumption of green-coloredfruits and vegetables, vegetable oils, orange-coloredfruits and vegetables and soup, and was negativelycorrelated with that of beer-cider and wine. CDPscore was negatively associated with alcohol andprotein intake and positively associated with carbohy-drate intake [54] (Table 2). Furthermore, CDP scorewas positively associated with the composite cogni-tive performance score assessed 13 years later. More
specifically, higher CDP scores were related to betterepisodic memory, semantic fluency, working mem-ory, and executive functioning [54].
CapsaicinCapsaicin is a micronutrient acting as an active
component of chili peppers. In recent studies, ithas been shown to have favorable effects on vari-ous diseases including atherosclerosis, CVD, cancer,obesity, gastrointestinal diseases, hypertension, andstroke, and also reducing total and cause-specificmortality [81, 82]. Liu and colleagues, in a cross-sectional study collecting the dietary habits ofparticipants in 12 months, found that capsaicin-richdiet was associated with MMSE and serum A�40 lev-els, but not with serum A�42 levels [69] (Table 3).A possible explanation may be that neurons producemore A�40 than A�42 and serum A�42 levels havehigher cerebral tropism with increased capacity ofaggregation in the brain, so it is less prone to effluxfrom the brain to blood.
Macronutrients: Fatty acidsMany epidemiological studies have demonstrated
that dietary fatty acids may play a key role in severalpathological conditions. In particular, an increas-ing body of epidemiological evidence suggested thatelevated SFA could have negative effects on MCI[11], while a clear reduction of risk for cognitivedecline has been found in population samples withelevated fish consumption, high intake of MUFA andPUFA, particularly n-3 PUFA [11]. In fact, it is ofextreme nutritional importance the intake of essen-tial fatty acids from both the n-3 and n-6 series ofPUFA. In the n-3 series, eicosapentaenoic acid (EPA)and docosahexaenoic acid (DHA) are considered themost important. In particular, DHA might affect theneuronal survival. In agreement with this hypoth-esis, Baierle and colleagues showed that cognitivefunction was positively associated with DHA, ner-vonic acid (MUFA), and total n-3 PUFA, while wasinversely related to myristic acid (SFA), palmitic acid(SFA), palmitoleic acid (MUFA), the n-6 PUFA/n-3PUFA ratio, and homocysteine levels [70] (Table 3).In this study, elevated levels of homocysteine werealso inversely associated with total n-3 PUFA whichmay lead to vascular disease and, thus, may beinvolved in the risk of cognitive decline and otherbrain dysfunctions. Therefore, balanced intake ofboth n-3 and n-6 fatty acids may be essential forhealth by avoiding a harmful permanent proinflam-matory state. These data are supported also by recent

840 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
imaging studies. In fact, positive associations (higherintake with larger cortical thickness) were observedfor n-3 PUFA and linolenic acid (n-3 PUFA) withsuperior temporal cortical thickness and for linoleicacid (n-6 PUFA) with superior temporal, precuneus,middle temporal, and parietal cortical thickness [35](Table 1). Furthermore, in postmenopausal womenstudy, n-3 index [red blood cell (RBC) EPA+ DHAlevels] was directly associated with the total brainand hippocampal volumes. In particular, a 2 stan-dard deviation (SD) (3.2% absolute) higher n-3 indexwas associated with a 0.48% (4.2 cm3) larger totalbrain volume measured 8 years later [71] (Table 3).A marginally significant association between a 1-SDincrease in DHA with total and normal brain vol-ume has also been found, instead no association wasfound for EPA [71]. Furthermore, Pottala and col-leagues showed that higher levels of RBC EPA+ DHAwere associated with 50 mm3 larger hippocampal vol-umes [71]. Furthermore, higher intake of n-3 PUFAwas associated with lower A� load in AD regionson PiB-PET, independently of gender, APOE, andfamily history [57] (Table 3). On the contrary, inanother study, in normal older adults, higher propor-tions of long-chain n-3 PUFA did not give benefitson cognitive performances [44] (Table 2). Higherconcentrations of EPA were associated with poorerperceptual and reasoning speed in females, but notin males, before controlling for current fish intake[44]. Therefore, it is plausible that a physiologicallydifferent effect of long-chain n-3 PUFA in relationto gender may lead to differential associations withcognition [44].
Mechanisms underlying the relationship amongdietary factors and late-life cognitive disorders
Dietary patterns and late-life cognitivedisorders: Possible mechanism models
We need to pursue studies which will improve theknowledge of the biochemical mechanisms under-lying the pathophysiological processes and, in apublic health perspective, will examine dietary pat-terns. These mechanisms could be searched at thedifferent levels of investigation of dietary factorslinked to late-life cognitive disorders used in thepresent review article (i.e., dietary patterns, foodsand food-groups, and dietary micro- and macronu-trients). Consumption of the western diet contributesto the development of chronic conditions, such asatherosclerosis, diabetes, obesity, hypertension, andhyperlipidemia, which in turn results in metabolic,
inflammatory, and microvascular changes that induceinjury to the white matter of the brain [83, 84].Subsequently, white matter disease promotes thedevelopment and progression of cognitive declineand dementia [85].
There is converging evidence that compositedietary patterns, such as the MeDi, are relatedto lower risk for CVD, dyslipidemia, hyperten-sion and coronary artery disease, several formsof cancer, cognitive decline, and overall mortality[86, 87]. Several mechanisms have been proposedunderlying the suggested protective role of theMeDi against age-related changes in cognitive func-tion, predementia syndromes and dementia: vascularvariables and non-vascular biological mechanismssuch as metabolic, oxidative, and inflammatory pro-cesses [88]. Therefore, MeDi may act on cognitionthrough cerebrovascular mechanisms. Alternatively,AD almost certainly has its pathological origins inmidlife, and it is possible that components of theMeDi could affect the metabolism of A� or tauprotein [89]. Moreover, the model of “gene environ-ment interaction” may be also considered, in light ofthe recently proposed Latent Early Life AssociatedRegulation model, in which environmental agents,such as heavy metals and toxins, and dietary factors,could perturb gene regulation in a long-term fashion,beginning at early developmental stages, but theseperturbations do not have pathological results untilsignificantly later in life [90].
The DASH is a diet that has been shown by ran-domized clinical trials in the US to protect againstmany cardiovascular risk factors of dementia [91].Some of the protective effects of DASH includedlower blood pressure [92] and blood low-densitylipoprotein (LDL) cholesterol levels [93], weightreduction [94], reduced oxidative stress and inflam-mation [95], improved insulin sensitivity and reducedincidence of diabetes mellitus [96]. DASH diet andthe MeDi have many similar components, such asemphasis on natural plant-based foods and limitedconsumption of red meat, but there are differences.The MeDi is a cultural diet that uniquely empha-sizes daily intake of olive oil (MUFA), fish, andpotatoes, and moderate wine consumption, whereasDASH uniquely emphasizes dairy consumption andrestricted intake of sodium, commercial sweets, andsaturated fat.
The MIND diet is a refinement of the exten-sively studied cardiovascular diets, the MeDi andDASH diets, with modifications based on exist-ing studies relevant to nutrition and associated with

V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 841
dementia prevention. MIND diet is not specific tothe underlying AD pathology, but perhaps betteroverall functioning and protection of the brain. Anumber of prospective cohort studies found thathigher consumption of vegetables was associatedwith slower cognitive decline with the strongest rela-tions observed for green leafy vegetables [12]. Greenleafy vegetables of MIND diet are sources of folate,vitamin E, carotenoids, and flavonoids, micronutri-ents that have been related to lower risk of dementiaand cognitive decline [31, 32].
Foods, food groups, and late-life cognitivedisorders: Possible mechanism models
Fish consumption has been associated with lowerrisk of AD because it could have a preventive effectagainst dementia through its anti-thrombotic andanti-inflammatory properties in addition to its spe-cific effect on neural functions, an effect thought tobe mediated through altering gene expression [97].Furthermore, the favorable effects of fish oil on cere-brovascular function are known, in particular for theimpact of DHA on endothelial nitric oxide synthase(eNOS) expression and a lower risk for ischemicstroke [98]. It was hypothesized that some nega-tive epidemiological findings observed for the impactof fish consumption on cognitive performance maybe due to neurotoxic contaminants in fish, such asmethylmercury [44]. However, as seen in one ofthe reviewed studies, higher brain levels of mer-cury were not correlated with brain neuropathology[43]. Diet may affect trace metal concentrations inthe brain of subjects with normal cognition [99] orAD [100–102], and transition metals, though cru-cial to many biochemical neuronal processes, wereabnormally aggregated and distributed in AD [103,104]. Dyshomeostasis in aluminum, silicon, lead,mercury, zinc, iron, and copper have been reportedin AD brains, where the abnormal accumulation anddistribution of the latter three may elicit oxidativestress and macromolecular damage, impeding cellu-lar function [104–107]. However, considering recentadvances in neurobiology of metals, the complex cor-relation between biometal metabolism, genetics, andthe environmental and the pathophysiology of manyneurodegenerative diseases [106, 107] warrants fur-ther investigation.
In recent years, numerous preclinical studiesinvolving fruits, nuts, and vegetables have identifiedpotential beneficial effects to brain health and cog-nition resulting from their nutrient and non-nutrientphytochemical content. These phytochemicals have
the ability to alter cellular function by modulat-ing transcription factors and altering the expressionof genes, cellular metabolism, and cellular signal-ing [108]. In vitro and in vivo studies have firmlyestablished the mechanistic effects of these phyto-chemicals on cognitive function, with many studiesdemonstrating their ability to counter oxidative stress[109], inflammation [110], as well as promote neu-ronal signaling and regulate transcription [111]. Inthe past five years, there has been an increasinginterest in the role that gut microbiota may play inthe modulation of the bidirectional signaling under-lying the gut–brain axis [112, 113]. In particular,in an Irish study, there was an association betweenindicators of general health, including frailty andMMSE, and microbiota composition only in long-stay subjects [114]. It has been also suggested thatdiet and specific nutrients can affect the compositionof the gut microbiota [115] that might influence theproduction or aggregation of A� protein in AD patho-genesis [116]. Bacteria populating the microbiomehave been shown to produce amyloids, lipopolysac-charides, and other immunogenic compounds [117,118] that might contribute to the regulation of sig-naling pathways implicated in neuroinflammation,brain A� deposition, and AD pathogenesis [116].Plant-derived nutrients and phytocompounds, byameliorating gut inflammation and dysbiosis, mightstimulate a positive modulation of the gut–brainaxis, reduce neuroinflammation, and retard or regresscognitive impairments associated with AD [119].Additionally, high intake of plant foods and spe-cific plant-derived compounds have been shown toreduce A� aggregation and, for this reason, are cur-rently considered suitable for the prevention of AD,as showed in some selected studies of the presentsystematic review [34, 57].
Caffeine, as an antioxidant substance, was revealedto reduce oxidative stress [120] and also to pro-tect against the disruptions of the blood-brain barrier[121]. Most of the biological effects of caffeine,including those on the brain and the central ner-vous system, are mediated through antagonism ofthe adenosine receptors, specifically the A1 andA2A receptors [122]. Other complementary mech-anisms of caffeine action that could contribute toits cognitive benefits in AD mice are the abil-ity of caffeine to decrease hippocampal levels ofpro-inflammatory cytokines [e.g., tumor necrosisfactor-�, interleukin (IL)-12(p70), and interferon-�)[123], caffeine’s beneficial effects on signal trans-duction factors is involved in neuronal plasticity and

842 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
survival [124], and the ability of caffeine to enhancebrain mitochondrial function [125].
Micronutrients, macronutrients, and late-lifecognitive disorders: Possible mechanism models
Optimal micronutrient status would moderate thedeterioration in brain integrity. Autophagy is proba-bly a crucial and a major process in the preservationof brain integrity. Micronutrients (vitamins, trace-elements, and also antioxidants) most likely affectbrain integrity by normalizing efficient autophagy[126]. Multiple lines of evidence indicate that oxida-tive stress not only strongly participates in an earlystage of AD prior to cytopathology, but it plays animportant role in inducing and activating multiplecell signaling pathways that contribute to the lesionformations of toxic substances and then promote thedevelopment of AD. Exogenous anti-oxidants (suchas vitamin E and C, carotenoids, flavonoids) decreasefree radical mediated damage caused by toxic chainreactions in neuronal cells and reduce the toxicity ofA� in in vitro studies of brains of patients with AD[127].
There is a vast literature demonstrating neuro-protection of the brain by vitamin E, rich sourcesof which are vegetable oils, nuts, and whole grains[128]. In particular, vitamin E might exert a regu-latory effect on cell proliferation and a beneficialeffect in improving glucose transport and insulinsensitivity [129]. Most of the known actions offlavonoids are related to their antioxidant propertiesthat can include suppression and scavenging of reac-tive oxygen species, and upregulation of antioxidantdefenses, the control of neuronal survival, death, anddifferentiation, long-term potentiation, and memoryas well as the effect on gene expression and interac-tions with mitochondria [130]. Therefore, flavonoids,lead to increased NO bioavailability in the vascula-ture of the hippocampus and subsequent angiogenesisand neurogenesis.
It has now been proven that vitamin B6, vita-min B12, and folate deficiency, as co-factors in themethylation of homocysteine, are associated withincreased homocysteine concentrations. Supraphys-iological concentrations of homocysteine or deficitsin folate and vitamin B12 should promote A� andtau protein accumulation and neuronal death, andalso have a direct effect on cognitive decline. Thepotential mechanisms whereby homocysteine mightmediate cognitive decline and dementia include:neurotoxicity induced by activation of N-methl-D-aspartate receptors, promotion of apoptosis, vas-
cular injury from promotion of atherogenesis makingvascular endothelium prothrombotic and prolifera-tion of smooth muscle cells, platelet activation, andincreased burden of ischemic strokes and white mat-ter lesions [131].
Epidemiologic investigations have revealed abeneficial role of vitamin D in muscle function, car-diovascular health, diabetes, and cancer prevention.Low levels of serum 25(OH)D are also associatedwith increased odds of prevalent cognitive dysfunc-tion, AD and all cause dementia in a number ofstudies. Vitamin D contributes to neuroprotectionby modulating the production of nerve growth, neu-rotrophin, glial cell derived neurotrophic factor, nitricoxide synthase and choline acetyl transferase [132],and neuroprotective mechanisms including vasopro-tection and A� phagocytosis and clearance [133,134].
Several mechanisms have been postulated for thepossible protective role of n-3 PUFA in demen-tia [77]. Supplementation with n-3 PUFA mayhave cognitive benefits based on animal studiesshowing neuroprotection through anti-oxidant, anti-inflammatory and anti-amyloid effects. DHA, thepredominant n-3 PUFA in the brain, is a key com-ponent of membrane phospholipids in the brain andadequate n-3 PUFA status, coming from dietaryconsumption, may help maintain integrity and neu-ronal function [135]. Secondly, n-3 PUFAs appearto have effects on dopaminergic and serotonergicsystems [136]. The oxidative products of PUFA actas key cellular mediators of inflammation, allergyand immunity, oxidative stress, bronchial constric-tion, vascular response, and thrombosis, and maythereby influence risk especially for vascular demen-tia. DHA may be directly involved in enhancingneuronal health in the aging brain through a range ofpotential mechanisms. In particular, it increases cellviability via neuroprotective and antiapoptotic mech-anisms, while also promoting dendritic arborizationand synaptogenesis [137]. DHA may modify theexpression of genes that regulate a variety of bio-logical functions potentially important for cognitivehealth, including neurogenesis and neuronal function[138]. Long-chain n-3 PUFA have been shown toreduce A� formation and oxidative damage [139].Higher intakes of saturated and trans fat and lowerintakes of mono- and polyunsaturated fat can con-tribute to insulin resistance and an atherogenic lipidprofile [140]. Moreover, insulin resistance, highinsulin levels, and cholesterol are all implicatedin A� accumulation in the brain, the pathologic

V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 843
hallmark of AD [141]. In a very recent neuropatho-logical metabolomic-based study, in the brains ofpatients with varying degrees of AD pathology(healthy brains, brains with AD pathology but with-out cognitive symptoms, and AD brains), significantdifferences in the abundance of six unsaturated fattyacids were identified in three brain regions bothvulnerable and resistant to classical AD pathology,with gradations in these metabolites being relatedto both severity of neuropathology at death as wellas domain-specific cognitive performance during life[142]. These findings suggested that dysregulation ofunsaturated fatty acid metabolism may play a rolein driving AD pathology, providing with further evi-dence for the metabolic basis of AD pathogenesis.
DISCUSSION
In the last decade, the association between dietand cognitive function or dementia has been largelyinvestigated. In the present article, we systematicallyreviewed observational studies published in the lastthree years (2014–2016) on the relationship amongdietary factors and late-life cognitive disorders usingdifferent levels of investigation (i.e., dietary pat-terns, foods and food-groups, and dietary micro- andmacronutrients). In the present systematic review,considering separately the different cognitive out-comes in older age, we included studies focusing ondementia, AD, MCI, and different models of late-life cognitive impairment/decline, but we did notfind studies focusing in particular on VaD. From thereviewed studies, it appeared to be apparent that theNIA–AA guidelines for AD and cognitive declinedue to AD pathology introduced some evidence sug-gesting a direct relation between diet and changesin the brain structure and activity. Several studiesfocused on the role of the dietary patterns on late-lifecognition, with accumulating evidence that higheradherence to a Mediterranean-type diet was associ-ated with decreased cognitive decline, although theMeDi combines several foods, micronutrients, andmacronutrients already separately proposed as poten-tial protective factors against dementia and MCI.Moreover, also other emerging healthy dietary pat-terns, such as the DASH and the MIND diets, wereassociated with slower rates of cognitive decline andsignificant reduction in AD rate.
Furthermore, some foods or food groups tradi-tionally considered harmful such as eggs and redmeat have been partially rehabilitated, while there
is still a negative correlation of cognitive functionswith saturated fatty acids and a protective effectagainst cognitive decline of elevated fish consump-tion, high intake of MUFA and PUFA, particularlyn-3 PUFA. In fact, while a Western diet was asso-ciated with worse cognitive performance in severalimaging studies selected in the present systematicreview [37, 39, 41]; however, for red meat, a classicalelement of this dietary pattern, the epidemiologicalfindings were controversial [35, 48], also includingstudies outside the time limits of the present sys-tematic reviews [143, 144]. Multi-country ecologicalstudies of dietary meat and increased risk of cancer[145] have been strongly supported by trends in can-cer risk in Asian countries undergoing the nutritiontransition [146, 147], as well as in observational stud-ies in Uruguay [148]. Thus, it would be expected thatthey would also be reliable for AD. In 2014, an eco-logical study linked the nutrition transition in Japan tothe greatly increased risk of AD [149], with increasedmeat consumption as an important factor. Interest-ingly, rates of VaD have been relatively unchangedfor many years [149]. Recent observational and eco-logical findings added support for dietary advancedglycation end products as an important risk factorfor AD [150], with meat cooked at high tempera-tures in a dry environment as an important source.Another recent ecological study compared dietaryfactors with prevalence rates of AD in ten countrieswith recent prevalence determinations, showing thatdietary supply of meat or animal products less milk5 years before AD prevalence had the highest corre-lations with AD rates [151]. The three countries withhighest rates of AD and dietary meat, Brazil, Mongo-lia, and the U.S., are considerably different in manyrespects, adding confidence that the finding was notdue to confounding factors [151]. Noteworthy, MeDifalls in the middle of the regression line for meatand AD prevalence [151]. In these ecological stud-ies, countries with high consumption of rice and lowconsumption of meat had the lowest rates of AD, asdid Japan prior to the nutrition transition [149]. Also,eggs and fish added to meat gave similar results asmeat [151]. Fish that does not have PUFA n-3 andvitamin D may act like meat and eggs in terms of ADrisk.
However, some limitations should be reported forthis systematic review article. Heterogeneity existsin the quantification of individual items as wellamong the different diet backgrounds of the popu-lations investigated, especially in view of differentgeographical areas, setting of dietary patterns, such

844 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
as the Mediterranean countries in which a largesegment of the population still adhered to MeDi.Heterogeneity in time between the two assessments,among studies using paired assessments (or a sin-gle assessment) several years after study populationenrollment. Nevertheless, these data represent a brickin the construction of the building of the causal linkbetween dietary habits and cognitive impairment.
The absence of causal etiological therapies againstAD leads to seek multimodal alternative strategies,increasing the interest in the potential for preventionof dementia by targeting modifiable risk factors. Itis now evident that dietary habits influence diversecardiometabolic risk factors, including not only obe-sity and low-density lipoprotein cholesterol, butalso blood pressure, glucose-insulin homeostasis,lipoprotein concentrations and function, oxidativestress, inflammation, endothelial health, hepatic func-tion, adipocyte metabolism, pathways of weightregulation, visceral adiposity, and the gut micro-biome. Whereas decades of dietary recommendationsfocused on dietary fat and single vascular risk fac-tors (e.g., hypertension, blood cholesterol, etc.) andcurrent dietary discussions are often worried abouttotal calories and obesity, the full health impact ofdiet extends far beyond these pathways. Consideringstrategies of prevention of AD could be complicatedand take to negative results. A second key lesson is theimportance of pointing out specific foods and over-all diet patterns, rather than single isolated nutrients,for cognitive impairment. No single micronutrientor macronutrient, no single antioxidant or vitamin,especially in their synthetic forms, may be able toshow a dramatic effect on dementia prevention, dueto the complexity of biochemistry. Even a mixture offixed beneficial compounds applied to everybody willnot show dramatic effects against late-life cognitivedisorders due to interindividual and intraindividualresponse. Natural nutrition may exert better effectsthan single nutrients due to bioavailability and bio-chemical synergisms. However, also the healthiestnatural nutrition alone, such as MeDi, could not exertdramatic effects against cognitive disorders in olderage if not part of diet intended as lifestyle. A food-based approach also better facilitates public guidanceand minimizes industry manipulation. Nevertheless,the complexity of the stake, the correction of mod-ifiable risk factors to expect “the compression ofcognitive morbidity” still remains a desirable goalof public health. Healthy diets and lifestyles could benot very powerful if applied in fixed amounts regard-less of individualized multidimensional needs and
resources. Larger observational studies with longerfollow-up periods should be encouraged, address-ing other potential bias and confounding sources, sohopefully opening new ways for diet-related preven-tion of dementia and AD.
DISCLOSURE STATEMENT
Authors’ disclosures available online (http://j-alz.com/manuscript-disclosures/17-0248r1).
REFERENCES
[1] Alzheimer’s, Association (2016) 2016 Alzheimer’s dis-ease facts and figures. Alzheimers Dement 12, 459-509.
[2] Panza F, Seripa D, Solfrizzi V, Imbimbo BP, LozuponeM, Leo A, Sardone R, Gagliardi G, Lofano L, Cre-anza BC, Bisceglia P, Daniele A, Bellomo A, Greco A,Logroscino G (2016) Emerging drugs to reduce abnormal�-amyloid protein in Alzheimer’s disease patients. ExpertOpin Emerg Drugs 21, 377-391.
[3] Grant WB (1999) Dietary links to Alzheimer’s disease:1999 Update. J Alzheimers Dis 1, 197-201.
[4] Solfrizzi V, Panza F, Capurso A (2003) The role of diet incognitive decline. J Neural Transm 110, 95-110.
[5] Luchsinger JA, Mayeux R (2004) Dietary factors andAlzheimer’s disease. Lancet Neurol 3, 579-587.
[6] Tangney CC (2014) DASH and Mediterranean-typedietary patterns to maintain cognitive health. Curr NutrRep 3, 51-61.
[7] Xu W, Tan L, Wang HF, Jiang T, Tan MS, Tan L, Zhao QF,Li JQ, Wang J, Yu JT (2015) Meta-analysis of modifiablerisk factors for Alzheimer’s disease. J Neurol NeurosurgPsychiatry 86, 1299-1306.
[8] Luchsinger JA, Noble JM, Scarmeas N (2007) Diet andAlzheimer’s disease. Curr Neurol Neurosci Rep 7, 366-372.
[9] Sofi F, Macchi C, Abbate R, Gensini GF, Casini A (2010)Effectiveness of the Mediterranean diet: Can it help delayor prevent Alzheimer’s disease? J Alzheimers Dis 20, 795-801.
[10] Cunnane SC, Plourde M, Pifferi F, Begin M, Feart C,Barberger-Gateau P (2009) Fish, docosahexaenoic acidand Alzheimer’s disease. Prog Lipid Res 48, 239-256.
[11] Solfrizzi V, Frisardi V, Capurso C, D’Introno A, ColaciccoAM, Vendemiale G, Capurso A, Panza F (2010) Dietaryfatty acids in dementia and predementia syndromes:Epidemiological evidence and possible underlying mech-anisms. Ageing Res Rev 9, 184-199.
[12] Loef M, Walach H (2012) Fruit, vegetables and preventionof cognitive decline or dementia: A systematic review ofcohort studies. J Nutr Health Aging 16, 626-630.
[13] Parrott MD, Greenwood CE (2007) Dietary influenceson cognitive function with aging. From high-fat diets tohealthful eating. Ann N Y Acad Sci 1114, 389-397.
[14] Peters R, Peters J, Warner J, Beckett N, Bulpitt C (2008)Alcohol, dementia and cognitive decline in the elderly. Asystematic review. Age Ageing 37, 505-512.
[15] Panza F, Frisardi V, Seripa D, Logroscino G, SantamatoA, Imbimbo BP, Scafato E, Pilotto A, Solfrizzi V (2012)
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 845
Alcohol consumption in mild cognitive impairment anddementia: Harmful or neuroprotective? Int J Geriatr Psy-chiatry 27, 1218-1238.
[16] Panza F, Solfrizzi V, Barulli MR, Bonfiglio C, Guerra V,Osella A, Seripa D, Sabba C, Pilotto A, Logroscino G(2015) Coffee, tea, and caffeine consumption and pre-vention of late-life cognitive decline and dementia: Asystematic review. J Nutr Health Aging 19, 313-328.
[17] Solfrizzi V, Frisardi V, Capurso C, D’Introno A, Colaci-cco AM, Chiloiro R, Dellegrazie F, Di Palo A, Capurso A,Panza F (2006) Whole-diet approach: Working on a cri-terion validity for age-related cognitive decline and mildcognitive impairment. J Am Geriatr Soc 57, 1944-1946.
[18] Gu Y, Scarmeas N (2011) Dietary patterns in Alzheimer’sdisease and cognitive aging. Curr Alzheimer Res 8, 510-519.
[19] Solfrizzi V, Panza F (2014) Mediterranean diet and cogni-tive decline. A lesson from the whole-diet approach: Whatchallenges lie ahead? J Alzheimers Dis 39, 283-286.
[20] Lourida I, Soni M, Thompson-Coon J, Purandare N, LangIA, Ukoumunne OC, Llewellyn DJ (2013) Mediterraneandiet, cognitive function, and dementia: A systematicreview. Epidemiology 24, 479-489.
[21] Psaltopoulou T, Sergentanis TN, Panagiotakos DB, Ser-gentanis IN, Kosti R, Scarmeas N (2013) Mediterraneandiet and stroke, cognitive impairment, depression: A meta-analysis. Ann Neurol 74, 580-591.
[22] Singh B, Parsaik AK, Mielke MM, Erwin PJ, Knop-man DS, Petersen RC, Roberts RO (2014) Associationof Mediterranean diet with mild cognitive impairmentand Alzheimer’s disease: A systematic review and meta-analysis. J Alzheimers Dis 39, 271-282.
[23] McKhann GM, Knopman DS, Chertkow H, Hyman BT,Jack CR Jr, Kawas CH, Klunk WE, Koroshetz WJ, ManlyJJ, Mayeux R, Mohs RC, Morris JC, Rossor MN, Schel-tens P, Carrillo MC, Thies B, Weintraub S, Phelps CH(2011) The diagnosis of dementia due to Alzheimer’s dis-ease: Recommendations from the National Institute onAging-Alzheimer’s Association workgroups on diagnos-tic guidelines for Alzheimer’s disease. Alzheimers Dement7, 263-269.
[24] Moher D, Liberati A, Tetzlaff J, Altman DG, GroupPRISMA (2009) Preferred reporting items for systematicreviews and meta-analyses: The PRISMA statement. PLoSMed 6, e1000097.
[25] Zbeida M, Goldsmith R, Shimony T, Vardi H, NagganL, Shahar DR (2014) Mediterranean diet and functionalindicators among older adults in non-Mediterranean andMediterranean countries. J Nutr Health Aging 18, 411-418.
[26] Galbete C1, Toledo E, Toledo JB, Bes-Rastrollo M, Buil-Cosiales P, Marti A, Guillen-Grima F, Martınez-GonzalezMA (2015) Mediterranean diet and cognitive function: TheSUN project. J Nutr Health Aging 19, 305-212.
[27] Trichopoulou A, Kyrozis A, Rossi M, Katsoulis M,Trichopoulos D, La Vecchia C, Lagiou P (2015) Mediter-ranean diet and cognitive decline over time in an elderlyMediterranean population. Eur J Nutr 54, 1311-1321.
[28] Qin B, Adair LS, Plassman BL, Batis C, Edwards LJ,Popkin BM, Mendez MA (2015) Dietary patterns and cog-nitive decline among Chinese older adults. Epidemiology26, 758-768.
[29] Gardener SL, Rainey-Smith SR, Barnes MB, Sohrabi HR,Weinborn M, Lim YY, Harrington K, Taddei K, Gu Y,Rembach A, Szoeke C, Ellis KA, Masters CL, Macaulay
SL, Rowe CC, Ames D, Keogh JB, Scarmeas N, MartinsRN (2015) Dietary patterns and cognitive decline in anAustralian study of ageing. Mol Psychiatry 20, 860-866.
[30] Tangney CC, Li H, Wang Y, Barnes L, Schneider JA,Bennett DA, Morris MC (2014) Relation of DASH- andMediterranean-like dietary patterns to cognitive decline inolder persons. Neurology 83, 1410-1416.
[31] Morris MC, Tangney CC, Wang Y, Sacks FM, Bennett DA,Aggarwal NT (2015) MIND diet associated with reducedincidence of Alzheimer’s disease. Alzheimers Dement 11,1007-1014.
[32] Morris MC, Tangney CC, Wang Y, Sacks FM4, BarnesLL5, Bennett DA6, Aggarwal NT (2015) MIND dietslows cognitive decline with aging. Alzheimers Dement11, 1015-1022.
[33] Mosconi L, Murray J, Tsui WH, Li Y, Davies M, WilliamsS, Pirraglia E, Spector N, Osorio RS, Glodzik L, McHughP, de Leon MJ (2014) Mediterranean diet and magneticresonance imaging-assessed brain atrophy in cognitivelynormal individuals at risk for Alzheimer’s disease. J PrevAlzheimers Dis 1, 23-32.
[34] Berti V, Murray J, Davies M, Spector N, Tsui WH, LiY, Williams S, Pirraglia E, Vallabhajosula S, McHugh P,Pupi A, de Leon MJ, Mosconi L (2015) Nutrient patternsand brain biomarkers of Alzheimer’s disease in cognitivelynormal individuals. J Nutr Health Aging 19, 413-423.
[35] Staubo SC, Aakre JA, Vemuri P, Syrjanen JA, Mielke MM,Geda YE, Kremers WK, Machulda MM, Knopman DS,Petersen RC, Jack CR Jr, Roberts RO (2017) Mediter-ranean diet, micronutrients and macronutrients, and MRImeasures of cortical thickness. Alzheimers Dement 13,168-177.
[36] Gu Y, Brickman AM, Stern Y, Habeck CG, Razlighi QR,Luchsinger JA, Manly JJ, Schupf N, Mayeux R, ScarmeasN (2015) Mediterranean diet and brain structure in a mul-tiethnic elderly cohort. Neurology 85, 1744-1751.
[37] Jacka FN, Cherbuin N, Anstey KJ, Sachdev P, ButterworthP (2015) Western diet is associated with a smaller hip-pocampus: A longitudinal investigation. BMC Medicine13, 215.
[38] Pelletier A, Barul C, Feart C, Helmer C, Bernard C, PeriotO, Dilharreguy B, Dartigues JF, Allard M, Barberger-Gateau P, Catheline G, Samieri C (2015) Mediterraneandiet and preserved brain structural connectivity in oldersubjects. Alzheimers Dement 11, 1023-1031.
[39] Shakersain B, Santoni G, Larsson SC, Faxen-Irving G,Fastbom J, Fratiglioni L, Xu W (2016) Prudent diet mayattenuate the adverse effects of Western diet on cognitivedecline. Alzheimers Dement 12, 100-109.
[40] Smyth A, Dehghan M, O’Donnell M, Anderson C, TeoK, Gao P, Sleight P, Dagenais G, Probstfield JL, MenteA, Yusuf S, ONTARGET and TRANSCEND Investiga-tors (2015) Healthy eating and reduced risk of cognitivedecline: A cohort from 40 countries. Neurology 84, 2258-2265.
[41] Ozawa M, Shipley M, Kivimaki M, Singh-Manoux A,Brunner EJ (2017) Dietary pattern, inflammation and cog-nitive decline: The Whitehall II prospective cohort study.Clin Nutr 36, 506-512.
[42] Qin B, Plassman BL, Edwards LJ, Popkin BM, AdairLS, Mendez MA (2014) Fish intake is associated withslower cognitive decline in Chinese older adults. J Nutr144, 1579-1585.
[43] Morris MC, Brockman J, Schneider JA, Wang Y, BennettDA, Tangney CC, van de Rest O (2016) Association of
846 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
seafood consumption, brain mercury level, and APOE�4status with brain neuropathology in older adults. JAMA315, 489-497.
[44] Danthiir V, Hosking D, Burns NR, Wilson C, NettelbeckT, Calvaresi E, Clifton P, Wittert GA (2014) Cognitiveperformance in older adults is inversely associated withfish consumption but not erythrocyte membrane n–3 fattyacids. J Nutr 144, 311-320.
[45] Dong L, Xiao R, Cai C, Xu Z, Wang S, Pan L, Yuan L(2016) Diet, lifestyle and cognitive function in old Chineseadults. Arch Gerontol Geriatr 63, 36-42.
[46] Pastor-Valero M, Furlan-Viebig R, Rossi Menezes P, daSilva SA, Vallada H, Scazufca M (2014) Education andWHO recommendations for fruit and vegetable intake areassociated with better cognitive function in a disadvan-taged Brazilian elderly population: A population-basedcross-sectional study. PLoS One 9, e94042.
[47] Zhao X, Yuan L, Feng L, Xi Y, Yu H, Ma W, Zhang D,Xiao R (2015) Association of dietary intake and lifestylepattern with mild cognitive impairment in the elderly.J Nutr Health Aging 19, 164-168.
[48] Xu X, Xiao S, Rahardjo TB, Hogervorst E (2015)Tofu intake is associated with poor cognitive perfor-mance among community-dwelling elderly in China.J Alzheimers Dis 43, 669-675.
[49] O’Brien J, Okereke O, Devore E, Rosner B, Breteler M,Grodstein F (2014) Long-term intake of nuts in relation tocognitive function in older women. J Nutr Health Aging18, 496-502.
[50] Solfrizzi V, Panza F, Imbimbo BP, D’Introno A, Gal-luzzo L, Gandin C, Misciagna G, Guerra V, Osella A,Baldereschi M, Di Carlo A, Inzitari D, Seripa D, PilottoA, Sabba C, Logroscino G, Scafato E; Italian LongitudinalStudy on Aging Working Group (2015) Coffee consump-tion habits and the risk of mild cognitive impairment: TheItalian Longitudinal Study on Aging. J Alzheimers Dis 47,889-899.
[51] Araujo LF, Giatti L, Padilha dos Reis RC, Goulart AC,Schmidt MI, Duncan BB, Ikram MA, Barreto SM (2015)Inconsistency of association between coffee consumptionand cognitive function in adults and elderly in a cross-sectional study (ELSA-Brasil). Nutrients 7, 9590-9601.
[52] Beydoun MA, Gamaldo AA, Beydoun HA, Tanaka T,Tucker KL, Talegawkar SA, Ferrucci L, Zonderman AB(2014) Caffeine and alcohol intakes and overall nutrientadequacy are associated with longitudinal cognitive per-formance among U.S. adults. J Nutr 144, 890-901.
[53] Travassos M, Santana I, Baldeiras I, Tsolaki M, Gkatz-ima O, Sermin G, Yener GG, Simonsen A, HasselbalchSG, Kapaki E, Mara B, Cunha RA, Agostinho P, BlennowK, Zetterberg H, Mendes VM, Manadas B, de Mendon A(2015) Does caffeine consumption modify cerebrospinalfluid amyloid-� levels in patients with Alzheimer’s dis-ease? J Alzheimers Dis 47, 1069-1078.
[54] Kesse-Guyot E, Andreeva VA, Ducros V, Jeandel C, JuliaC, Hercberg S, Galan P (2014) Carotenoid-rich dietarypatterns during midlife and subsequent cognitive function.Br J Nutr 111, 915-923.
[55] Beydoun MA, Fanelli-Kuczmarski MT, Kitner-TrioloMH, Beydoun HA, Kaufman JS, Mason MA, Evans MK,Zonderman AB (2015) Dietary antioxidant intake and itsassociation with cognitive function in an ethnically diversesample of US adults. Psychosom Med 77, 68-82.
[56] Hooshmand B, Lokk J, Solomon A, Mangialasche F,Miralbell J, Spulber G, Annerbo S, Andreasen N, Winblad
B, Cedazo-Minguez A, Wahlund LO, Kivipelto M (2014)Vitamin D in relation to cognitive impairment, cere-brospinal fluid biomarkers, and brain volumes. J GerontolA Biol Sci Med Sci 69, 1132-1138.
[57] Mosconi L, Murray J, Davies M, Williams S, PirragliaE, Spector N, Tsui WH, Li Y, Butler T, Osorio RS,Glodzik L, Vallabhajosula S, McHugh P, Marmar CR,de Leon MJ (2014) Nutrient intake and brain biomark-ers of Alzheimer’s disease in at-risk cognitively normalindividuals: A cross-sectional neuroimaging pilot study.BMJ Open 4, e004850.
[58] Wilson VK, Houston DK, Kilpatrick L, Lovato J, YaffeK, Cauley JA, Harris TB, Simonsick EM, AyonayonHN, Kritchevsky SB, Sink KM (2014) Health, Agingand Body Composition Study, Relationship between 25-hydroxyvitamin D and cognitive function in older adults:The Health, Aging and Body Composition Study. J AmGeriatr Soc 62, 636-641.
[59] Littlejohns TJ, Henley WE, Lang IA, Annweiler C,Beauchet O, Chaves PH, Fried L, Kestenbaum BR, KullerLH, Langa KM, Lopez OL, Kos K, Soni M, Llewellyn DJ(2014) Vitamin D and the risk of dementia and Alzheimerdisease. Neurology 83, 920-928.
[60] Miller JW, Harvey DJ, Beckett LA, Green R, FariasST, Reed BR, Olichney JM, Mungas DM, DeCarli C(2015) Vitamin D status and rates of cognitive declinein a multi-ethnic cohort of older adults. JAMA Neurol 72,1295-1303.
[61] Granic A, Hill TR, Kirkwood TB, Davies K, CollertonJ, Martin-Ruiz C, von Zglinicki T, Saxby BK, WesnesKA, Collerton D, Mathers JC, Jagger C (2015) Serum 25-hydroxyvitamin D and cognitive decline in the very old:The Newcastle 85+Study. Eur J Neurol 22, 106-115.
[62] Assmann KE, Touvier M, Andreeva VA, Deschasaux M,Constans T, Hercberg S, Galan P, Kesse-Guyot E (2015)Midlife plasma vitamin D concentrations and performancein different cognitive domains assessed 13 years later.Br J Nutr 113, 1628-1637.
[63] Moore EM, Ames D, Mander AG, Carne RP, Brodaty H,Woodward MC, Boundy K, Ellis KA, Bush AI, Faux NG,Martins RN, Masters CL, Rowe CC, Szoeke C, Watters DA(2014) Among vitamin B12 deficient older people, highfolate levels are associated with worse cognitive function:Combined data from three cohorts. J Alzheimers Dis 39,661-668.
[64] Doets EL, Ueland PM, Tell GS, Vollset SE, Nygard OK,Van’t Veer P, de Groot LC, Nurk E, Refsum H, Smith AD,Eussen SJ (2014) Interactions between plasma concentra-tions of folate and markers of vitamin B(12) status withcognitive performance in elderly people not exposed tofolic acid fortification: The Hordaland Health Study. Br JNutr 111, 1085-1095.
[65] Kim H, Kim G, Jang W, Kim SY, Chang N (2014) Associ-ation between intake of B vitamins and cognitive functionin elderly Koreans with cognitive impairment. Nutr J 13,118.
[66] Agnew-Blais JC, Wassertheil-Smoller S, Kang JH, HoganPE, Coker LH, Snetselaar LG, Smoller JW (2015) Folate,vitamin B-6, and vitamin B-12 intake and mild cogni-tive impairment and probable dementia in the Women’sHealth Initiative Memory Study. J Acad Nutr Diet 115,231-241.
[67] Rabassa M, Cherubini A, Zamora-Ros R, Urpi-Sarda M,Bandinelli S, Ferrucci L, Andres-Lacueva C (2015) Lowlevels of a urinary biomarker of dietary polyphenol are
V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 847
associated with substantial cognitive decline over a 3-yearperiod in older adults: The Invecchiare in Chianti Study.J Am Geriatr Soc 63, 938-946.
[68] Feart C, Letenneur L, Helmer C, Samieri C, Schalch W,Etheve S, Delcourt C, Dartigues JF, Barberger-Gateau P(2016) Plasma carotenoids are inversely associated withdementia risk in an elderly French cohort. J Gerontol ABiol Sci Med Sci 71, 683-688.
[69] Liu CH, Bu XL, Wang J, Zhang T, Xiang Y, Shen LL,Wang QH, Deng B, Wang X, Zhu C, Yao XQ, Zhang M,Zhou HD, Wang YJ (2016) The associations between acapsaicin-rich diet and blood amyloid-� levels and cogni-tive function. J Alzheimers Dis 52, 1081-1088.
[70] Baierle M, Vencato PH, Oldenburg L, Bordignon S,Zibetti M, Trentini CM, Duarte MM, Veit JC, SomacalS, Emanuelli T, Grune T, Breusing N, Garcia SC (2014)Fatty acid status and its relationship to cognitive declineand homocysteine levels in the elderly. Nutrients 6,3624-3640.
[71] Pottala JV, Yaffe K, Robinson JG, Espeland MA, WallaceR, Harris WS (2014) Higher RBC EPA+ DHA corre-sponds with larger total brain and hippocampal volumes:WHIMS-MRI study. Neurology 82, 435-442.
[72] Sabuncu MR, Desikan RS, Sepulcre J, Yeo BT, LiuH, Schmansky NJ, Reuter M, Weiner MW, BucknerRL, Sperling RA, Fischl B; Alzheimer’s Disease Neu-roimaging Initiative (2011) The dynamics of cortical andhippocampal atrophy in Alzheimer disease. Arch Neurol68, 1040-1048.
[73] Roberts RO, Roberts LA, Geda YE, Cha RH, PankratzVS, O’Connor HM, Knopman DS, Petersen RC (2012)Relative intake of macronutrients impacts risk of mildcognitive impairment or dementia. J Alzheimers Dis 32,329-339.
[74] Panza F, Solfrizzi V, Barulli MR, Bonfiglio C, Guerra V,Osella A, Seripa D, Sabba C, Pilotto A, Logroscino G(2015) Coffee, tea, and caffeine consumption and pre-vention of late-life cognitive decline and dementia: Asystematic review. J Nutr Health Aging 19, 313-328.
[75] Casamenti F, Stefani M (2017) Olive polyphenols: Newpromising agents to combat aging-associated neurodegen-eration. Expert Rev Neurother 17, 345-358.
[76] Morris MC, Evans DA, Tangney CC, Bienias JL, Wil-son RS, Aggarwal NT, Scherr PA (2005) Relation of thetocopherol forms to incident Alzheimer disease and tocognitive change. Am J Clin Nutr 81, 508-514.
[77] Grant WB, Karras SN, Bischoff-Ferrari HA, AnnweilerC, Boucher BJ, Juzeniene A, Garland CF, Holick MF(2016) Do studies reporting ‘U’-shaped serum 25-hydroxyvitamin D-health outcome relationships reflectadverse effects? Dermatoendocrinol 8, e1187349.
[78] Morris M, Selhub J, Jacques P (2012) Vitamin B-12 andfolate status in relation to decline in scores on the Mini-Mental State Examination in the Framingham CohortStudy. J Am Geriatr Soc 60, 1457-1464.
[79] Clarke R, Jobst KA, Refsum H, Sutton L, Ueland PM(1998) Folate, vitamin B12, and serum total homocysteinelevels in confirmed Alzheimer disease. Arch Neurol 55,1449-1455.
[80] Seshadri S, Beiser A, Selhub J, Jacques PF, Rosen-berg IH, D’Agostino RB, Wilson PW, Wolf PA (2002)Plasma homocysteine as a risk factor for dementia andAlzheimer’s disease. NEJM 289, 2651-2662.
[81] Sharma SK, Vij AS, Sharma M (2013) Mechanisms andclinical uses of capsaicin. Eur J Pharmacol 720, 55-62.
[82] Fattori V, Hohmann MS, Rossaneis AC, Pinho-Ribeiro FA,Verri WA (2016) Capsaicin: Current understanding of itsmechanisms and therapy of pain and other pre-clinical andclinical uses. Molecules 21, pii: E844.
[83] Dearborn JL, Knopman D, Sharrett AR, Schneider AL,Jack CR Jr, Coker LH, Alonso A, Selvin E, MosleyTH, Wagenknecht LE, Windham BG, Gottesman RF(2014) The meta-bolic syndrome and cognitive decline inthe Atherosclerosis Risk in Communities study (ARIC).Dement Geriatr Cogn Disord 38, 337-346.
[84] Wang M, Norman JE, Srinivasan VJ, Rutledge JC (2016)Metabolic, inflammatory, and microvascular determinantsof white matter disease and cognitive decline. Am J Neu-rodegener Dis 5, 171-177.
[85] Smallwood A, Oulhaj A, Joachim C, Christie S, Sloan C,Smith AD, Esiri M (2012) Cerebral subcortical small ves-sel disease and its relation to cognition in elderly subjects:A pathological study in the Oxford Project to InvestigateMemory and Ageing (OPTIMA) cohort. Neuropathol ApplNeurobiol 38, 337-343.
[86] Gu Y, Nieves JW, Stern Y, Luchsinger JA, Scarmeas N(2010) Food combination and Alzheimer disease risk: Aprotective diet. Arch Neurol 67, 699-706.
[87] Frisardi V, Panza F, Seripa D, Imbimbo BP, Vendemiale G,Pilotto A, Solfrizzi V (2010) Nutraceutical properties ofMediterranean diet and cognitive decline: Possible under-lying mechanisms. J Alzheimers Dis 22, 715-740.
[88] Solfrizzi V, Panza F, Frisardi V, Seripa D, LogroscinoG, Imbimbo BP, Pilotto A (2011) Diet and Alzheimer’sdisease risk factors or prevention: The current evidence.Expert Rev Neurother 11, 677-708.
[89] Whitmer RA, Sidney S, Selby J, Johnston SC, Yaffe K(2005) Midlife cardiovascular risk factors and risk ofdementia in late life. Neurology 64, 277-281.
[90] Lahiri DK (2006) Where the actions of environment (nutri-tion), gene and protein meet: Beneficial role of fruitand vegetable juices in potentially delaying the onset ofAlzheimer’s disease. J Alzheimers Dis 10, 359-361.
[91] Smith PJ, Blumenthal JA, Babyak MA, Craighead L,Welsh-Bohmer KA, Browndyke JN, Strauman TA, Sher-wood A (2010) Effects of the dietary approaches to stophypertension diet, exercise, and caloric restriction on neu-rocognition in overweight adults with high blood pressure.Hypertension 55, 1331-1338.
[92] Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, SvetkeyLP, Sacks FM, Bray GA, Vogt TM, Cutler JA, Wind-hauser MM, Lin PH, Karanja N (1997) A clinical trialof the effects of dietary patterns on blood pressure. DASHCollaborative Research Group. N Engl J Med 336, 1117-1124.
[93] Blumenthal JA, Babyak MA, Sherwood A, CraigheadL, Lin PH, Johnson J, Watkins LL, Wang JT, Kuhn C,Feinglos M, Hinderliter A (2010) Effects of the dietaryapproaches to stop hypertension diet alone and in com-bination with exercise and caloric restriction on insulinsensitivity and lipids. Hypertension 55, 1199-1205.
[94] Moore TJ, Alsabeeh N, Apovian CM, Murphy MC, Coff-man GA, Cullum-Dugan D, Jenkins M, Cabral H (2008)Weight, blood pressure, and dietary benefits after 12months of a Web-based Nutrition Education Program(DASH for health): Longitudinal observational study. JMed Internet Res 10, e52.
[95] Azadbakht L, Surkan PJ, Esmaillzadeh A, Willett WC(2011) The Dietary Approaches to Stop Hypertensioneating plan affects C-reactive protein, coagulation abnor-
848 V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age
malities, and hepatic function tests among type 2 diabeticpatients. J Nutr 141, 1083-1088.
[96] Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF,Lachin JM, Walker EA, Nathan DM, Diabetes Preven-tion Program Research, Group (2002) Reduction in theincidence of type 2 diabetes with lifestyle intervention ormetformin. N Engl J Med 346, 393-403.
[97] Weaver KL, Ivester P, Seeds M, Case LD, Arm JP, ChiltonFH (2009) Effect of dietary fatty acids on inflammatorygene expression in healthy humans. J Biol Chem 284,15400-15407.
[98] Fotuhi M, Mohassel P, Yaffe K (2009) Fish consump-tion, long-chain omega-3 fatty acids and risk of cognitivedecline or Alzheimer disease: A complex association. NatClin Pract Neurol 5, 140-152.
[99] Hunt JR (2003) Bioavailability of iron, zinc, and othertrace minerals from vegetarian diets. Am J Clin Nutr 78(3Suppl), 633S-639S.
[100] Okubo H, Sasaki S, Murakami K, Takahashi Y; Freshmenin Dietetic Courses Study II group (2011) The ratio of fishto meat in the diet is positively associated with favorableintake of food groups and nutrients among young Japanesewomen. Nutr Res 31, 169-177.
[101] Loef M, Walach H (2012) Copper and iron in Alzheimer’sdisease: A systematic review and its dietary implications.Br J Nutr 107, 7-19.
[102] Brewer GJ (2015) Copper-2 ingestion, plus increased meateating leading to increased copper absorption, are majorfactors behind the current epidemic of Alzheimer’s dis-ease. Nutrients 7, 10053-10064.
[103] Grant WB (1997) Dietary links to Alzheimer’s disease.Alz Dis Rev 2, 42-55.
[104] Bonda DJ, Lee HG, Blair JA, Zhu X, Perry G, SmithMA (2011) Role of metal dyshomeostasis in Alzheimer’sdisease. Metallomics 3, 267-270.
[105] Wong BX, Hung YH, Bush AI, Duce JA (2014) Met-als and cholesterol: Two sides of the same coin inAlzheimer’s disease pathology. Front Aging Neurosci6, 91.
[106] Xu H, Perreau VM, Dent KA, Bush AI, Finkelstein DI,Adlard PA (2016) Iron regulates apolipoprotein E expres-sion and secretion in neurons and astrocytes. J AlzheimersDis 51, 471-487.
[107] Prakash A, Dhaliwal GK, Kumar P, Majeed AB (2017)Brain biometals and Alzheimer’s disease - boon or bane?Int J Neurosci 127, 99-108.
[108] Tsao R (2010) Chemistry and biochemistry of dietarypolyphenols. Nutrients 2, 1231-1246.
[109] Thangthaeng N, Poulose SM, Miller MG, Shukitt-HaleB (2016) Preserving brain function in aging: The anti-glycative potential of berry fruit. Neuromolecular Med 18,465-473.
[110] Heim KC, Angers P, Leonhart S, Ritz BW (2012) Anti-inflammatory and neuroactive properties of selected fruitextracts. J Med Food 15, 851-854.
[111] Rendeiro C, Rhodes JS, Spencer JP (2015) The mecha-nisms of action of flavonoids in the brain: Direct versusindirect effects. Neurochem Int 89, 126-139.
[112] Collins SM1, Surette M, Bercik P (2012) The interplaybetween the intestinal microbiota and the brain. Nat RevMicrobiol 10, 735-742.
[113] Pistollato F, Sumalla Cano S, Elio I, Masias VergaraM, Giampieri F, Battino (2016) Role of gut microbiotaand nutrients in amyloid formation and pathogenesis ofAlzheimer disease. Nutr Rev 74, 624-634.
[114] Claesson MJ, Jeffery IB, Conde S, Power SE, O’ConnorEM, Cusack S, Harris HM, Coakley M, Lakshmi-narayanan B, O’Sullivan O, Fitzgerald GF, Deane J,O’Connor M, Harnedy N, O’Connor K, O’Mahony D, vanSinderen D, Wallace M, Brennan L, Stanton C, MarchesiJR, Fitzgerald AP, Shanahan F, Hill C, Ross RP, O’ToolePW (2012) Gut microbiota composition correlates withdiet and health in the elderly. Nature 488, 178-184.
[115] Scott KP, Gratz SW, Sheridan PO, Flint HJ, Duncan SH(2013) The influence of diet on the gut microbiota. Phar-macol Res 69, 52-60.
[116] Friedland RP (2015) Mechanisms of molecular mimicryinvolving the microbiota in neurodegeneration. JAlzheimers Dis 45, 349-362.
[117] Bhattacharjee S, Lukiw WJ (2015) Alzheimer’s diseaseand the microbiome. Front Cell Neurosci 7, 153.
[118] Schwartz K, Boles BR (2013) Microbial amyloids–functions and interactions within the host. Curr OpinMicrobiol 16, 93-99.
[119] Daulatzai MA (2014) Chronic functional bowel syndromeenhances gut-brain axis dysfunction, neuroinflammation,cognitive impairment, and vulnerability to dementia. Neu-rochem Res 39, 624-644.
[120] Prasanthi JR, Dasari B, Marwarha G, Larson T, ChenX, Geiger JD, Ghribi O (2010) Caffeine protects againstoxidative stress and Alzheimer’s disease-like pathology inrabbit hippocampus induced by cholesterol-enriched diet.Free Radic Biol Med 49, 1212-1220.
[121] Chen X, Ghribi O, Geiger JD (2010) Caffeine protectsagainst disruptions of the blood-brain barrier in ani-mal models of Alzheimer’s and Parkinson’s diseases. JAlzheimers Dis 20, S127-S141.
[122] Fredholm BB, Battig K, Holmen J, Nehlig A, ZvartauEE (1999) Actions of caffeine in the brain with specialreference to factors that contribute to its widespread use.Pharmacol Rev 51, 83-133.
[123] Cao C, Cirrito JR, Lin X, Verges DK, Dickson A, Mam-carz M, Zhang C, Mori T, Arendash GW, Holtzman DM,Potter H (2009) Caffeine suppresses amyloid-beta levels inplasma and brain of Alzheimer’s disease transgenic mice.J Alzheimers Dis 17, 681-697.
[124] Zeitlin R, Patel S, Burgess S, Arendash GW, EcheverriaV (2011) Caffeine induces beneficial changes in PKA sig-naling and JNK and ERK activities in the striatum andcortex of Alzheimer’s transgenic mice. Brain Res 1417,127-136.
[125] Dragicevic N, Delic V, Cao C, Copes N, Lin X, MamcarzM, Wang L, Arendash GW, Bradshaw PC (2012) Caffeineincreases mitochondrial function and blocks melatoninsignaling to mitochondria in Alzheimer’s mice and cells.Neuropharmacology 63, 1368-1379.
[126] Dror Y, Stern F, Gomori MJ (2014) Vitamins in the preven-tion or delay of cognitive disability of aging. Curr AgingSci 7, 187-213.
[127] Feng Y, Wang X (2012) Antioxidant therapies forAlzheimer’s disease. Oxid Med Cell Longev 2012, 472932.
[128] Yamada K, Tanaka T, Han D, Senzaki K, Kameyama T,Nabeshima T (1999) Protective effects of idebenone andalpha-tocopherol on beta-amyloid-(1–42)-induced learn-ing and memory deficits in rats: Implication of oxidativestress in beta-amyloid-induced neurotoxicity in vivo. EurJ Neurosci 11, 83-90.
[129] Yu BP, Kang CM, Han JS, Kim DS (1998) Can antioxi-dant supplementation slow the aging process? Biofactors7, 93101.

V. Solfrizzi et al. / Diet and Cognitive Disorders in Older Age 849
[130] Spencer JP, Vauzour D, Rendeiro C (2009) Flavonoids andcognition: The molecular mechanisms underlying theirbehavioural effects. Arch Biochem Biophys 492, 19.
[131] Garcia A, Zanibbi K (2004) Homocysteine and cognitivefunction in elderly people. CMAJ 171, 897-904.
[132] Balion C, Griffith LE, Strifler L, Henderson M, PattersonC, Heckman G, Llewellyn DJ, Raina P (2012) Vitamin D,cognition, and dementia: A systematic review and meta-analysis. Neurology 79, 1397-405.
[133] Dickens AP, Lang IA, Langa KM, Kos K, Llewellyn DJ(2011) Vitamin D, cognitive dysfunction and dementia inolder adults. CNS Drugs 25, 629-639.
[134] Lu’o’ng KV, Nguyen LT (2011) The beneficial role ofvitamin D in Alzheimer’s disease. Am J Alzheimers DisOther Demen 26, 511-520.
[135] Schubert R, Kitz R, Beermann C, Rose MA, Baer PC,Zielen S, Boehles H (2007) Influence of low-dose polyun-saturated fatty acids supplementation on the inflammatoryresponse of healthy adults. Nutrition 23, 724-730.
[136] Chalon S (2006) Omega-3 fatty acids and monoamine neu-rotransmission. Prostaglandins Leukot Essent Fatty Acids75, 259-269.
[137] Lukiw WJ, Bazan NG (2008) Docosahexaenoic acid andthe aging brain. J Nutr 138, 2510-2514.
[138] Sydenham E, Dangour AD, Lim W-S (2012) Omega 3 fattyacid for the prevention of cognitive decline and dementia.Cochrane Database Syst Rev 6, CD005379.
[139] Lim GP, Calon F, Morihara T, Yang F, Teter B, Ubeda O,Salem N Jr, Frautschy SA, Cole GM (2005) A diet enrichedwith the omega-3 fatty acid docosahexaenoic acid reducesamyloid burden in an aged Alzheimer mouse model. JNeurosci 25, 3032-3040.
[140] Lichtenstein AH, Schwab US (2000) Relationship ofdietary fat to glucose metabolism. Atherosclerosis 150,227-243.
[141] Luchsinger JA, Tang MX, Shea S, Mayeux R (2004)Hyperinsulinemia and risk of Alzheimer disease. Neurol-ogy 63, 1187-1192.
[142] Snowden SG, Ebshiana AA, Hye A, An Y, Pletnikova O,O’Brien R, Troncoso J, Legido-Quigley C, Thambisetty M(2017) Association between fatty acid metabolism in thebrain and Alzheimer disease neuropathology and cogni-tive performance: A nontargeted metabolomic study. PLoSMed 14, e1002266.
[143] Giem P, Beeson WL, Fraser GE (1993) The incidence ofdementia and intake of animal products: Preliminary find-ings from the Adventist Health Study. Neuroepidemiology12, 28-36.
[144] Barberger-Gateau P, Letenneur L, Deschamps V, Peres K,Dartigues JF, Renaud S (2002) Fish, meat, and risk ofdementia: Cohort study. BMJ 325, 932-933.
[145] Armstrong B, Doll R (1975) Environmental factors andcancer incidence and mortality in different countries, withspecial reference to dietary practices. Int J Cancer 15,617-631.
[146] Kono S (2004) Secular trend of colon cancer incidenceand mortality in relation to fat and meat intake in Japan.Eur J Cancer Prev 13, 127-132.
[147] Zhang J, Dhakal IB, Zhao Z, Li L (2012) Trends in mortal-ity from cancers of the breast, colon, prostate, esophagus,and stomach in East Asia: Role of nutrition transition. EurJ Cancer Prev 21, 480-489.
[148] Aune D, De Stefani E, Ronco A, Boffetta P, Deneo-Pellegrini H, Acosta G, Mendilaharsu M (2009) Meatconsumption and cancer risk: A case-control study inUruguay. Asian Pac J Cancer Prev 10, 429-436.
[149] Grant WB (2014) Trends in diet and Alzheimer’s diseaseduring the nutrition transition in Japan and developingcountries. J Alzheimers Dis 38, 611-620.
[150] Perrone L, Grant WB (2015) Observational and ecolog-ical studies of dietary advanced glycation end productsin national diets and Alzheimer’s disease incidence andprevalence. J Alzheimers Dis 45, 965-979.
[151] Grant WB (2016) Using multicountry ecological andobservational studies to determine dietary risk factors forAlzheimer’s disease. J Am Coll Nutr 35, 476-489.