joseph ongrÁdi institute of medical microbiology
TRANSCRIPT

JOSEPH ONGRÁDIINSTITUTE OF MEDICAL MICROBIOLOGY
SEMMELWEIS UNIVERSITYBudapest 2013
GRAM POSITIVE SPORE-FORMING
RODS
NON-SPORE FORMING OBLIGATE
ANAEROBIC BACTERIA AND
ASSOCIATED INFECTIONS
ALLOCATED IN SEVERAL TAXONOMIC UNITSHERE: FUNCTIONAL GROUPINGS
GRAM POSITIVE SPORE-FORMING RODS
CLOSTRIDIUM GENUSONLY!!!
NON-SPORE FORMINGANAEROBIC BACTERIAGram + cocci and
rodsGram – cocci and
rods
COMMON CHARASTERISTICS
CATABOLISM: ANAEROBIC (fermentation)lack of the cytochrom system, superoxide dismutase,catalase and peroxidase enzymes
TOXIC END PRODUCTS OF OXYGEN METABOLISM
OBLIGATE ANAEROBIC --------- AEROTOLERANT
SPECIMEN COLLECTION: transport media without O2
CULTIVATION: removal of O2 (GasPack, etc.)

DISTINCT CHARACTERISTICS
GRAM POSITIVESPORE-FORMING RODS
Exogenous infections1 species = 1 diseaseSmall number of species ���� more clinical entitiesVaried pathomechanisms,
but molecularly wellcharacterized
Diagnosis: unambigousTreatment: unambigousPrevention: unambigous
NON-SPORE FORMING ANAEROBIC BACTERIA
Endogenous infectionsMany species Mixed infections: (polymicrobial)
more aerobic + anaerobic species
����
similar clinical entities
Diagnosis: complicatedTreatment: difficultPrevention: difficult
3
ENDOSPORE: ENSURES SURVIVALPRODUCED IN THE ENVIRONMENT (SOIL, WATER, AIR)EXTREME RESISTANCE(PARAMETERS AND BIOLOGICAL MONITORING OF STERILIZATION PROCEDURES)
Bacillus genus
AerobicSpore Ø < bacterium ØB. anthracis (flagella-, capsule+) B. cereus (flagella+, capsule-) enterotoxins: (food poisoning) heat stabile: emeticheat labile: diarrhoeaeye, wound infections, IVDA
B. subtilis: contaminant ,bioterrorism model
B. megaterium: contaminantB. mesentericus: contaminantB. stearothermophilus, B. pumilis:
monitoring sterilization proceduresB. globigii: modelling bioterrorismsOther Bacilii: insecticides
Clostridium genus
Obligate anaerobicSpore Ø > bacterium ØPeritrichous flagella(capsule: C. perfringens)Exogenous infectionsEndogenous: C. perfringens
C. difficile Intensive metabolism,
gas production +/-Neurotoxic (exotoxin): C. tetani (non- invasive) C. botulinum (toxicosis) Histotoxic (invasive):C. perfringens + C. septicum +C. novyi + otherEnteral (nosocomial): C. difficile (dysbacteriosis) 4

MORPHOLOGY: 5-10 μm x 1 μmSquare endsCapsule (in host), central spore(in nature)
CULTIVATION:agar/bloodagar: medusa headlecithinase (weak)
PATHOGENIESIS: cattle, sheep> feces/carcasses>soil>saprophytic > spores persist for decades in dry earth> human infection
Capsule+exotoxin (protective antigen, edema factor, lethal factor)
CLINICAL FINDINGS:
Skin anthrax:animal products , scratch,wound, > 12-24 h latency> gelation edema>
malignant pustule>necrotic ulcer>bacteremia>sepsis
Inhalation anthrax: hemorrhagic lobular pneumonia,edema>meningitis, sepsis, shock „woolsorter's disease”biological warfare (bioterrorism)
Intestinal anthrax: abdominal pain, bloody diarrhea, vomiting, ascites

Cutaneous anthrax
Respitarory anthrax
Intestinalanthrax

7
DIAGNOSIS:Specimens: fluid or pus from pustules
blood, sputum, fecesstaining, immunofluorescent stainingcultivation on blood agar(no hemolysis, no swarming)
Serology: precipitation, hemagglutinationto detect animal or human antibodiesAscoli test: immune serum + tissue extractAnimal infection: guinea pig andmouse – sensitive, rat – resistant
PREVENTION: public health control measuresdeep burial in lime-pitsautoclaving animal productsprotective clothing
Vaccination: live attenuated vaccine for animalshumans (occupational risk): cell-free vaccine
TREATMENT: as early as possible!penicillin (except in inhalation anthrax)tetracyclin, erythromycin, clindamycin

8
WHAT IS BIOTERRORISM?A BIOTERRORIST ATTACK IS
THE DELIBERATE RELEASE OF BACTERIA, VIRUSES, OTHER GERMSOR TOXINS TO CAUSE ILLNESS, DEATH, DISRUPTION OR FEARIN HUMANS, LIVESTOCK, FOOD CROPS AND ENVIRONMENTAL RESOURCES
39 MAJOR MICROORGANISMS AND BIOLOGICALS TO BE USED (NATO categorization)
RECENT DEVELOPMENT:corrosive microbes to destroy electric appliances, health care products,
gaskets
THE MOST LIKELY, PREDICTED METHOD OF NEXT BIOLOGICAL ATTACKS: AEROSOLIZED AGENTS

9
CHARACTERISTICS OF BIOTERRORIST ATTACKS
SUDDEN AND UNEXPECTED ONSETLARGE NUMBER OF CASESTYPICAL, ATYPICAL OR UNKNOWN CLINICAL ENTITIESTHE EFFECT: DEADLY (SMALLPOX)
INCAPACITIVE, TEMPORARY (Q-FEVER)SPREAD: CONTAGIOUS (PLAGUE)
NON-CONTAGIOUS (TOXINS)THE FATE OF AFFECTED PERSONS: CURABLE (ANTHRAX)
INCURABLE (EBOLA)SPREAD OF THE AGENT: aerosol (<5 micrometer droplets)
ventillation systems, water supply, food, public transportinfected humans, animals, vectors, contaminated objects
THE TERRORIST: strongly motivated, fanatic, well educated,good financial support minority groups, governmental support: global terrorism
(BIOLOGICAL CRIMES: THREATENING USE OF MICROBES FOR COMMON CRIMES)

10
BIOTERRORISM AGENT CATEGORIZATION
CATEGORIZATION
HOW EASILY THEY ARE TO OBTAIN, WEAPONIZE,
DISSEMINATE
HOW MUCH DEATH, THE SEVERITY OF ILLNESS
HOW MUCH DAMAGE, DISRUPTION OR FEAR THEY
MIGHT CAUSE

11
CATEGORY AHigh priority agents (organisms, toxins) that pose the highest risk to the public security:easy spread or transmitted from person to personhigh death rate, major public health impactcause public panic, social disruptionrequire special action for public health preparedness
Variola majorBacillus anthracisClostridium botulinum (toxin)Yersinia pestisFrancisella tularensisFILOVIRUSES (Ebola, Marburg viruses)ARENAVIRUSES (Lassa, Junin, Machupo)BUNYAVIRUSES (Crimean-fever, Rift-valley fever)

2010 SU Dept. Public Health 12
THE MOST IMPORTANT MICROORGANISMS FOR BIOTERRORISM (II)
CATEGORY BTHE SECOND HIGHEST PRIORITYMODERATELY EASY TO SPREADMODERATE ILLNESS RATES, LOW DEATH RATESREQUIRE SPECIFIC ENHANCEMENTS OF LABORATORY CAPACITY
Brucella spp.Burkholderia malleiBurkholderia pseudomalleiRickettsia prowazekiiCoxiella burnettiChlamydia psittaciAlphaviruses (Venezuelan horse encephalitis)Staphylococcus aureus (enterotoxin B)Salmonella spp.Escherichia coli O57:H7Vibrio cholerae Shigella spp.Cryptosporidium parvum

2010 SU Dept. Public Health 13
THE MOST IMPORTANT MICROORGANISMS FOR BIOTERRORISM (III)
CATEGORY C EMERGING PATHOGENS THAT COULD BE ENGINEERED FOR THE FUTURE
EASILY AVAILABLEEASILY PRODUCED AND SPREADATYPICAL OR NEW DISEASESPOTENTIAL HIGH MORBIDITY AND MORTALITY RATESMAJOR HEALTH IMPACT
NIPAH VIRUS, HANTA VIRUSRECOMBINANT MICROBES (bacteria, viruses, fungi)THE FUTUREADAPTING ANIMAL VIRUSES TO HUMANS (Iraq: camel smallpox virus)ENHANCED PATHOGENICITY OF KNOWN MICROBES
insertion of IL-4 gene into mouse pox virus to inhibit immune functions(Australia)Clostridium botulinum: to spread from person to person (Soviet Union)Bacillus anthracis: insertion of more virulence genes to circumvent vaccination(Soviet Union)recombination of Ebola and HIV (Soviet Union)insertion of antibiotic resistance genes to produce polyresistant bacteria (SU)

RISK OF ANTHRAX INFECTION
U.S. Postal Service distribution clerk Sheila Dickson-Ongrady uses gloves as shesorts mail in Hamilton Township, N.J., facility Tuesday. An employee of thefacility is believed to have contracted inhalation anthrax (Laredo MorningTimes).

Saprophyte in the soil
MORPHOLOGY: flagella +, capsule –
CULTIVATION: swarming, hemolysis on blood agar
PATHOGENESIS:1. Enterotoxin>food poisoning, intoxication
Emetic type (spores: soiI>rice, pasta) Diarrheal type (meat)2. Other: eye infections (trauma, foreign body>
keratitis, end-, panophthalmitis) endocarditis, meningitis, osteomyelitis, pneumonia, IVDA
OTHER BACILLIParasites of insects < commercial insecticidesFood poisoning?
DIFFERENTIAL DIAGNOSIS: biochemistry, phage typization
15

Tetanus (1888)
MORPHOLOGY: 2-5 μm x 1-2 μm, flagella (specific antigen), terminal spore
CULTIVATION: obligate anaerobic ββββ-hemolysis on blood agar
PATHOGENESIS: 1884EXOTOXIN=tetanospasmin (151 kD, A-B-C chains)Released by bacteriolysis. Minimal wound>necroparasite>non invasivegermination and toxin production is aided by associated pyogenic infection, calcium salts reducing oxidation-reduction potentialToxin absorption in neurons>retrograde axonal transport to CNS >circulation>fixed to gangliosides> postsynaptic inhibition of acetylcholineinhibitory factor>generalized muscular spasms, hyperreflexia, seizures =TOXEMIA (tetanolysin=exotoxin, non pathogenic)
16

Opisthotonus
Trismus
Risus sardonicus Neonatal tetanus
TETANUS

CLINICAL FINDINGS:
5-7 days of latency>spasms> convulsive tonic contraction of voluntary muscles> lockjaw, hydrophobia, opisthotonus, interference with
mechanics of respiration>death. Fully conscious!
INFECTION: soil, horse stool (occupational disease),spores in air
wounds, uterus, umbilical stump (90% in developing countries), abortion, burns
iatrogenic: surgery, ointments, catgut, injections mortality: 50-60%, 1 M cases/year worldwide
DIFFERENTIAL DIAGNOSIS: rabies, strychnin poisoning

TREATMENT:1.Symptomatic: proper care of wounds, surgical debridement (no hyperbaric oxygen) muscle relactants, sedation (external stimuli precipitate tetanic seizures), assisted ventilation2.Toxoid recall injectiontoxoid + antitoxin iv. (earlier horse serum,recently human serum: tetanus immunoglobulin, HTIG) 3. Antitoxin: before toxin becomes fixed onto nerves4.Antibiotics (penicillin, tetracyclin to stop toxin production)
treatment of associated pyogenic infection
PREVENTION: toxoid - active immunizationDPT combination (childhood)recall injections in every 10 years (toxoid 0.5 ml)totally preventable, immunization is mandatory
Booster shot in the elderly population would be ideal!

SAPROPHYTE BACTERIA (SOIL, INTESTINAL TRACT, DUNG)
MORPHOLOGY: 7-8 μm x 1-2 μm, Gram+spore Ø > bacterium ØGermination into bacterium > sporulationC. perfringens: capsulePeritrichous flagella: C. novyi, C. septicum,
C. histiolyticum, C. sporogenes, C. tertium, C. bifermentans, C. fallax, C. sordelli, etc.(90 species/20 human pathogens)
CULTIVATION: anaerobic, gas production(aerotolerants: milk stormy fermentation, clot torn)
ANTIGENS: 12 types
BIOCHEMISTRY: 1. Toxins: α, β, …,τ(αααα=lecithinase, LD50=50 ng, hemolysing, cell lysing, cardiotoxicinhibition by antitoxin: Nagler-reaction)toxinogenic strains: A-E 2. Enzymes: collagenase, hyaluronidase, proteinase, DNase, etc.
20

PATHOGENESIS: normal habitat in the gut (skin, vagina) flora
Pathogenical local effects = tissue necrosis:1. >endogenous infections: Colon surgery, colon-carcinoma,appendicitis>perforation,uterus <instrumental abortus, puerperal infections,abscess in pelvis (female),brain abscess +/- meningitis, empyema, pneumonia, biliary tract inflammations (male, diabetes)
2. Exogenous infection: soil, feces> war, trauma, iatrogenicfoul-smelling discharge, edema malignum,gas-phlegmone.myositis: edema,myonecrosis,exsudate,rapid progression, crepitation (acetylene, H2, etc), cellulitis
General effects = toxic: malaise, hypotonia, fever, vomiting, nervousity, toxemia, shock, death.
21

GAS GANGRENE

3. Bacteremia (10-15%): death
4. C. perfr. "A" (C,D): food poisoning, meat dishes high protein content protects bacteria form strong acidic pHincubation: 9-15 hsymptomps: abdominal cramps, diarrhea<enterotoxin (through sporulation, spore coat) ileum, jejunum
(w/o adenylyl/guanylyl cyclase) self limited, no treatment is needed (but: infusion application)
5. C. perfringens "C": enteritis necrotisans (pigbel) contaminated pork,New Guinea
<ββββ toxinhighly fatal in childrenprevention: immunization with type C toxoid
6. C. septicum: enterocolitis + neutropenianatural: leukemia, congenital neutropeniaiatrogenic: cytotoxic drugs
23
DIAGNOSIS: microscopy, cultivation (chopped meat-glucose medium, egg yolk medium), biochemistry, gas chromatography, toxin-neutralization (VERO-cells) phage typization, DNA-probes
TREATMENT:1. ANTITOXIN
(polyvalent: C. perfringens, C. septicum, C. novyi)to detoxity patients rapidly
2. Antibiotics (penicillin, chloramphenicol, erythromycin, tetracyclin). Metronidazol
3. Symptomatic carepromt and extensive surgical debridement, hyperbaric oxygen early amputation
PREVENTION: Cleansing of contaminated wounds
24


Pseudomembranous colitisIatrogenic: antibiotic-associated diarrhea MORPHOLOGY: spores CULTIVATION: obligate anaerobic. Resistant. PATHOGENESIS: in normal flora (3% of adults)colonization: in newbornsin adults during hospitalization from the hand ofpersonnel, endoscopes, devices NON INVASIVE (yes: newborns, neutropenia) TOXEMIA (plasmid, phage, regulation?)toxin A: 440-500 kD enterotoxin (watery diarrhea)toxin B: 360-470 kD cytotoxic (colon wall destruction)Binding to gut wall: gradual > microabscesses >contraction > bleeding>necrosis>inflammation>protein loss>watery/bloody diarrhea PROLONGED TREATMENT WITH ANTIBIOTICS(aminoglycosid, clindamycin) > dysbacteriosis > selectionof resistant mutants > 4-9 days of incubation, abdominalpain > diarrhea, fever, elevated number of WBC(rarely: perforation, peritonitis, acute arthritis)
26

CLINICAL DIAGNOSIS: endoscopy MICROBIOLOGICAL DIAGNOSIS:1. Cultivation
(cycloserin, cefoxitin, fructose-agar, CCFA)2. Phage typization3. Toxin detection
toxin B on VERO cells (24h CPE) and neutralisationtoxin A detection: latex agglutination toxin A+B: ELISAPCR
TREATMENT:1. Discontinuing administration of offending antibiotic2. Antibiotics: vancomycin, metronidazol, bacitracin3. Symptomatic: cholestyramin
(=toxin B binding, but: binds vancomycin) 4. Surgical (in case of perforation)PREVENTION: vancomycin in case of carriers and hospitalized patientsmedical personneldisinfection of medical devices, endoscopes:glutaraldehyde, Na-hypochlorite, iodine (sporocidal)wearing gloves during physical examinations by health care personnel
27
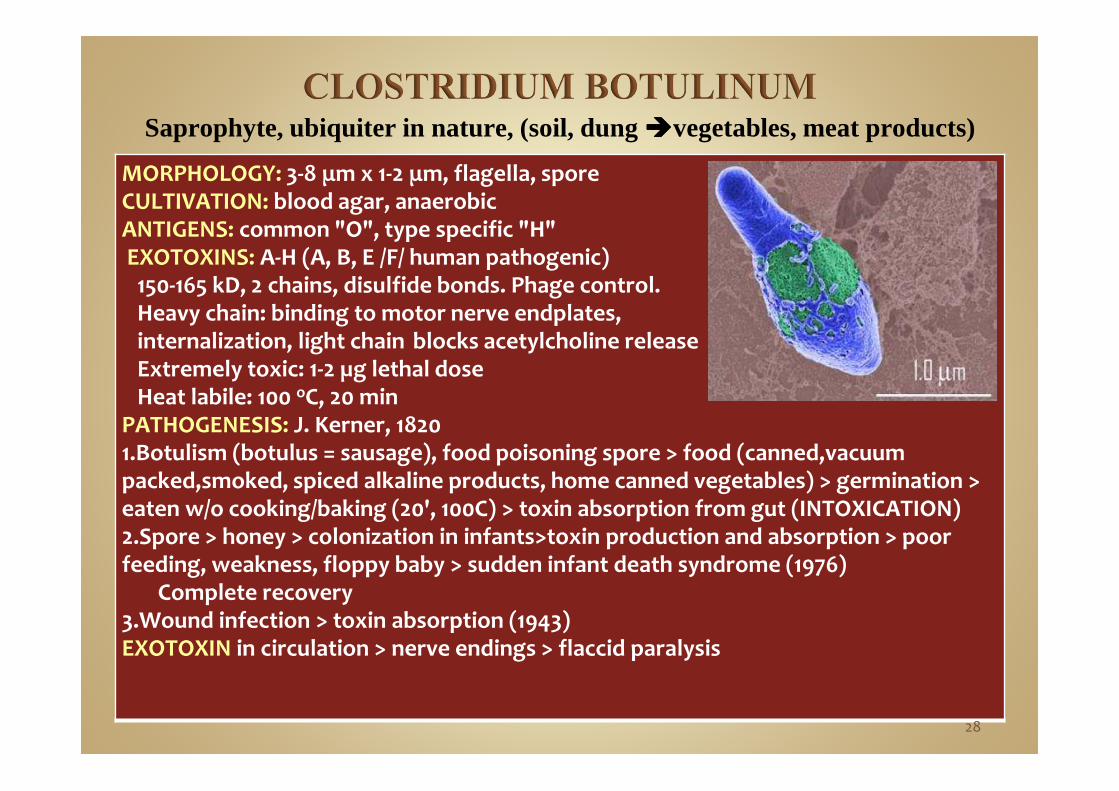
MORPHOLOGY: 3-8 μm x 1-2 μm, flagella, sporeCULTIVATION: blood agar, anaerobicANTIGENS: common "O", type specific "H" EXOTOXINS: A-H (A, B, E /F/ human pathogenic) 150-165 kD, 2 chains, disulfide bonds. Phage control. Heavy chain: binding to motor nerve endplates, internalization, light chain blocks acetylcholine releaseExtremely toxic: 1-2 µg lethal doseHeat labile: 100 oC, 20 min
PATHOGENESIS: J. Kerner, 18201.Botulism (botulus = sausage), food poisoning spore > food (canned,vacuum packed,smoked, spiced alkaline products, home canned vegetables) > germination >eaten w/o cooking/baking (20', 100C) > toxin absorption from gut (INTOXICATION)2.Spore > honey > colonization in infants>toxin production and absorption > poor feeding, weakness, floppy baby > sudden infant death syndrome (1976)
Complete recovery3.Wound infection > toxin absorption (1943)EXOTOXIN in circulation > nerve endings > flaccid paralysis
Saprophyte, ubiquiter in nature, (soil, dung ����vegetables, meat products)
28

CLINICAL FINDINGS: 1-2h—1-2 days of latency, speech difficulty, double vision, inability to swallow, muscular weakness, +/- gastroenteritis, respiratory paralysis, cardiac arrest>no fever>deathFully conscious. High mortality (65>25%)Recovery without antitoxins in serum
DIAGNOSIS: toxin detection: leftover food, vomiting, stool (infants), approx. for 1 month toxin-neutralization: mouse injection, ELISA from sera: passive HA, RIA
TREATMENT: 1. Polyvalent (A,B,E) antitoxin80.000 U horse serum: promtly administered
2.Symptomatic: adequate ventilation (for 100 days!)3.Infants, wound infections: antibiotics (penicillin 10-20 MU/day)
Contraindicated: tetracyclin, aminoglycosid (due to nerve toxicity)PREVENTION:1. strict regulation of commercial canning food hygiene2. home canning: boiling food for >20 min before consumption
toxic food (beans, corn, peas, fish, vacuum-packed fish in plastic bags)spoiled, rancid, cans „swell”, innocuous appearance
29

GENUS Species Biochemistry Residence
Gram positive cocci
Peptostreptococci 13 Protein hydrolysis/utilization
Mouth, vaginaPeptococci 1 Mouth, respiratory tract,
vagina, skinAnaerob streptococci 3
Gram positive rodsAcids
Propionibacteria 4 Propionic Skin, mouth, vaginaBifidobacteria 8 Acetic/lactic Gut, mouth, vaginaLactobacilli 56 Lactic Gut, mouth, vaginaActinomyces 20 +/- fermentation Gut, mouth, vaginaEubacteria 45 Butyric Gut, mouth, vaginaMobiluncus 2 Hydrolysis Vagina, rectum
30

GENUS Species Biochemistry/characteristc
Residence
Gram negative cocci
Veilonella 3 Lactic acid Mouth, vagina
Acidaminococci 1 Acetic/lactic acid Gut
Megasphera 1 Capronic acid Gut
Gram negative rods
Bacteriodes 18 Capsule Mouth, gut, vagina
Prevotella 16 Pigment Mouth, vagina
Porphyromonas 8 Pigment Mouth
Fusobacterium 4 Polymorph Mouth, gut, vagina
Leptotrichia 2 Elongated Mouth
CONTINOUSLY CHANGING TAXONOMY: genera, number of species, new characteristics 31
>40 species pathogenic in human
MICROBIOLOGYObligate anaerobic ---------- microaerophilModerate biochemical activityProtein hydrolisisStarch and carbohydrate fermentation:
CO2, foul-smelling gases
32

Anaerobic streptococci:S. hanseniiS. pleomorphusS. parvulus
Residence:mainly respiratory tract (particularly the pharynx)
Cultivation:non-hemolytic or alpha-hemolytic
33
Peptostreptococcus microsresident in the normal mouth flora
Produced diseases: periodontitis,abscesses around tooth implants(24%)hematogenic spread ���� brain abscesschronic sinusitis in children, nasopharyngitis, otitis mediaretropharyngeal abscess, pulmonary abscess, erythema
Peptostreptococcus anaerobiusresident in normal mouth flora
Produced diseases: as P. microsperitonitis appendicitis, diverticulitis, after abdominal surgery
postpartum endometritis, septic abortion
34

Peptococcus nigerProduced diseases: postpartum endometritis,
tuboovarial abscessseptic abortion
CoprococcusRuminococcus
Residents in the normal flora of human and animal
Sarcina ventriculiMostly in the gut flora of vegetarian peopleUnusual high number in the stomach: cancer
GaffkyaResident in the normal gut flora
35

Pathomechanism:~ 15%- of normal floraPredominantly in dental plaques and periodontal pocketsContinously changing resident flora in the mouth and gutDepending on age and nutrition (food habits)
Polymicrobial (mixed) aerobic +anaerobic infection
1. aerobic bacteria growth ����
2. lack of normal oxygenization in tissues����3. tissue destruction/necrosis, anaerobic conditions����4. vast proliferation of anaerobic bacteria����5. abscess formation, suppuration, gangrene, gas production
36
Specimen collection:aspiration, punction
Laboratory process:smears, staining
Cultivation:usually small, grey colonies or other dark pigmentsno ideal selective media are availableother microbes overgrow gram positive anaerobic cocci
Identification at species level:no concensus protocol or scheme, uncertaincarbohydrate fermentation, gas productionenzyme reaction (urease, phosphatase, etc.)gas- liquid chromatography (GLC)
Common end products: acetate, butyrate, capronic acid
37
Penicillin resistance(due to the mutations of penicllin binding proteins)
Resistance to metronidazole(mainly the microaerophilic species)
Effective antibiotics:clindamycin (depending on geographical location)amoxicillin + clavulic acid4th generation quinolones (e.g. trova- and clinafloxacin)
38

BACTEROIDES GENUSintensive sugar fermentationstrictly anaerobic, very pleomorphic, non-motilepolysaccharide capsule: B. fragilisno lipopolysaccharide endotoxincolonization: fimbriae
Normal inhabitants of the upper respiratory tract, intestinaland female genital tract1011 organism/g stool(B. caccae, B. merdae, etc.)
Produced anaerobic infections:abdominal, brain, lung abcesses, empyema, PIDsurgical infections, peritonitis (pus: foul smelling)bacteremia ���� endocarditis
Taxonomical changes: Bacteroides melaninogenicus ����Porphyromonas gingivalis, Prevotella melaninogenica
39

PORPHYROMONAS GENUSPorphyromonas gingivalisOxygen tolerant, small black colonies
on chocolate agarno carbohydrate fermentation,
but proteolytic
Porphyromonas endodontalis, P. asaccharolytica
Residents of the normal mouth floraProduced diseases: soft tissue infection followinghuman bites
40

PREVOTELLA GENUSmoderate carbohydrate fermentationglucose fermentation ���� acid productionsaccharose fermentation!proteolysispigment production
P. intermedia, P. melaninogenica (B. melaninogenicus), P. denticola, P. loeschii
residents in the normal mouth floraendogenous infections, inflammationsperiodontitis, surgical wound infection
and abscesses
41

FUSOBACTERIUM GENUSPleomorphic rods, produce butyric acidConvert threonine to propionic acidCystein, methionin: H2S productionF. nucleatum**, F. alocis, F. sulci, F. necrophorum, F. periodonticum*
** and * in the normal mouth flora, others in the gut** Prevotella/Porphyromonas coinfection
Fusospirochetosis: nomaOccassionally: Fusobacterium the only species
in an infection (e.g. osteomyelitis)LEPTOTRICHIA GENUS
Pleomorphic rodsFirst isolation: anaerobic,subcultures: elevate CO2 level requirementL. buccalis: resident in the normal mouth florain immunocompromised individuals: ulcerative gingivitisFrequent coinfection with Treponema, Porphyromonas,
Fusobacterium species 42

Metronidazole (Klion)
Amoxicillin + clavulic acid (Augmentin)
Imipenem
Chloramphenicol(severe side effects)
43

Acne (carbunculus,phegmone,sepsis): Propionibacterium
Skin (carbunculus): Eubacterium
Chronic sinusitis: Peptostreptococcus, Eubacterium
Post-maxillo-facial or periodontal surgery: Bacteroides, Fusobacterium, Porphyromonas, Prevotella, Actinomyces, Peptostreptococcus, Veilonella, Propionibacterium
Gingivitis ulcerans: Leptotrichia, Porphyromonas, Fusobacterium (+Treponema)
Peritonsillar abscess: Fusobacterium
44

Brain abscess: Peptostreptococcus
Pulmonary abscess, empyema: Bacteroides, Porphyromonas, Prevotella, Peptostreptococcus
Thoracal infection: Actinomyces
Hepatic- and perihepatic abscesses : Bacteroides
Peritoneal infections, peritonitis, bowel rupture, post-surgicalinfection, war injury: Bacteroides fragilis, Gram+ anaerobic cocci,
Actinomyces
IUD in women, abscess, criminal (instrumental) abortus, salpyngitis, uterus abscess: Bacteroides, Fusobacterium,
Peptostreptococcus, Mobiluncus
Bacterial vaginosis: Mobiluncus, Porphyromonas, Prevotella, Gram+ anaerobic cocci (G.vaginalis)
Perirectal abscess, fistule: Bacteroides, Fusobacterium45

Necrotising cellulitis in the limbs: gas gangrene clostridia
Joint infections: Gram+ anaerobic cocci
Leg ulcers: mixed infection (but: Clostridium)
Bacteremia, septicemia, endocarditis:Bacteroides fragilis, Propionibacterium, Clostridium, Mobiluncus
Infections in immunocompromised: Bifidobacterium, Lactobacillus
46

LOCAL FACTORS
ENDOGENOUS INFECTIONSdermal and mucosal woundsdiminished tissue oxygenization(diabetes mellitus, angiopathy)surgery (oral, abdominal, gynecological)
EXOGENOUS INFECTIONShuman or animal bites
SYMPTOMSfoul-smelling pus, exsudate < fatty acids(diagnosis: gas chromatography)abscess formation, necrosis, gas production(differential diagnosis!)
47

NEWBORN: sterile, colonization in few days
SMALL CHILDREN: mixed flora (cocci, bacilli)FROM PUBERTY:1. Aerobic and anaerobic Lactobacilli (Döderlein)
estrogen > glycogen fermentation of epithelial cells > lactic acid production > pH 4-4.5
(~ treatment: 0.5% lactic acid)
2. Resident flora: Bacteroides, Mobiluncus, Gram+ cocci, αααα-hemolysing streptococci, enterococci, Gardnerella , Mycoplasma, Ureaplasma, staphylococci, Mobiluncus, Candida species etc.
3. Transient flora: Enterobacter, staphylococci, streptococci, clostridia
Critical pH (preventing harmful microbes): 6.0-6.5Anaerobic : aerobic ratio: 2-5:1Sexual activity: individual and continously changing flora
MODEL: VAGINA
48

BACTERIAL VAGINOSISAlterations in the ratio of the normal flora = dysbacteriosis >
inflammation
1. Decreased ratio of Lactobacilli in the flora2. Activation of endogenous bacteria = endogenous infection >
increasing ratio > massive infection3. Promoting factors
hormonal changes (age, menses, gravidity, oral contraception)chemical effects: antibiotics, chemotherapymechanical effects: contraceptive barriers, IUD
4. Consequences: pH increase (alkaline) > increasing ratio of all anaerobic bacteria (1000:1)>genital discharge> „amin vaginosis”>recurrent vaginal and urinary tract infections(109/ml Mobiluncus, Prevotella, Porphyromonas, Gram+anaerob cocci, Myco-, Ureaplasma, Gardnerella, etc.)infection of the sexual partners (non-gonorrhoic urethritis)or the newborn at time of delivery
DIAGNOSIS: clue cells, presence of PMNL, amin-test49

In the majority of cases: mixed (aerobic + anaerobic) infection
Surgical debridement, excision of all devitalized tissues
50

THERAPY ANAEROBESGram positive Gram negative
Recommendedwithout sensitivity test
ββββ-lactam + ββββ-lactamase inhibitors:e.g. Augmentin
imipenemchloramphenicol
clindamycin metronidazole
Recommended as determined
by sensitivity tests
tetracyclineserythromycins
clindamycincefoxitin
moxalactamother β-lactams
penicillinesclindamycin metronidazole
Notrecommended
(resistant)
aminoglycosidesfluoroquinolones
51

www.bact.wisc.edu/Bact330/lectureanthrax
www.cdc.gov
52