joim 2553 13
TRANSCRIPT

doi: 10.1111/j.1365-2796.2012.02553.x
Dietary fats and coronary heart diseaseW. C. Willett
FromtheDepartmentofNutrition,HarvardSchoolofPublicHealth,Boston,MA,USA
Abstract. Willett WC (Harvard School of Public Health,Boston, MA, USA). Dietary fats and coronary heartdisease (Review). J Intern Med 2012; 272: 13–24.
The relation of dietary fat to risk of coronary heartdisease (CHD) has been studied extensively usingmany approaches, including controlled feedingstudies with surrogate end-points such as plasmalipids, limited randomized trials and large cohortstudies. All lines of evidence indicate that specificdietary fatty acids play important roles in thecause and the prevention of CHD, but total fat as apercent of energy is unimportant. Trans fatty acidsfrom partially hydrogenated vegetable oils haveclear adverse effects and should be eliminated.Modest reductions in CHD rates by further de-creases in saturated fat are possible if saturatedfat is replaced by a combination of poly- andmono-
unsaturated fat, and the benefits of polyunsatu-rated fat appear strongest. However, little or nobenefit is likely if saturated fat is replaced by car-bohydrate, but this will in part depend on the formof carbohydrate. Because both N-6 and N-3 poly-unsaturated fatty acids are essential and reducerisk of heart disease, the ratio of N-6 to N-3 is notuseful and can be misleading. In practice, reduc-ing red meat and dairy products in a food supplyand increasing intakes of nuts, fish, soy productsand nonhydrogenated vegetable oils will improvethe mix of fatty acids and have a markedly benefi-cial effect on rates of CHD.
Keywords: coronary heart disease, trans fat, saturatedfat, polyunsaturated fat,monounsaturated fat, bloodcholesterol.
Early interest in the relation between dietary fatsand cardiovascular disease emerged from animalstudies conducted during the 1930s, showing thatdietary cholesterol causes arterial lesions and thatthis is mediated largely through elevation in bloodcholesterol levels [1–5]. Subsequent studies of heartdisease rates in different populations, controlledfeeding studies on the effects of dietary fats on serumcholesterol and epidemiologic studies relating serumcholesterol to risk of coronary heart disease (CHD)risk led to the conclusion that high intake of satu-rated fat is a major cause of heart disease. This con-cept has been widely incorporated in dietary recom-mendations and policies to reduce intake ofsaturated fats. In the 1970s, these recommenda-tions emphasized replacement of saturated fat withpolyunsaturated fat, but in the 1980s and 1990s,the emphasis shifted to replacement of all fats bycarbohydrates. Recently, studies have cast doubt onthe relation of saturated fat to risk of CHD andencouraged the promotion of low-carbohydrate dietsthat are often high in red meat and dairy products,and thus high in saturated fat. This review willexamine the development of the classical diet-hearthypothesis, an expanded mechanistic perspective,and the implications of current evidence for dietaryrecommendations.
The classical diet-heart hypothesis and beyond
According to the classic ‘diet-heart’ hypothesis, highintake of saturated fats and cholesterol and low in-take of polyunsaturated fats increase the level of ser-um cholesterol, which leads to the development ofatheromatous plaques. Accumulation of these pla-ques narrows the coronary arteries, reduces bloodflow to the heart muscle and finally leads to myocar-dial infarction. However, the common clinical pre-sentation of sudden, catastrophic chest pain is notadequately accounted for by a slowly progressiveprocess that develops over decades, and in the lastseveral decades, many additional mechanistic path-ways potentially leading from diet to CHD have beenidentified (see Fig. 1). These include importantmedi-ating roles of thrombosis, hypertension, insulinresistance, inflammation, endothelial function andarrhythmia. Thus, we cannot assume that an effectof a dietary fat can be predicted by its effect on onepathway, such as blood total cholesterol level. Forthis reason, evidence directly relating a dietary factorto risk of CHD,which incorporates all competing andsynergistic effects, is essential, and this review willfocus on this evidence. Understanding the potentialpathways by which an effect of diet is mediated canstill be valuable; the vast literature on this topic will
ª 2012 The Association for the Publication of the Journal of Internal Medicine 13
Review |

be mentioned only briefly but is discussed in detailelsewhere [6].
Descriptive studies of diet and CHD
Studies comparing rates of CHDacross different geo-graphical areas have documented that age-adjustedincidenceandmortality ratesvaryby10-foldormore.Coupled with studies showing that migrants fromlow- tohigh-riskareas adopt the rates of thenewarea[7, 8], this evidence indicated powerfully that thelarge differences in rates are not owing to genetic fac-tors and are thus potentiallymodifiable. As shown inFig. 2, intake of saturated fat as a percentage of calo-rieswasstronglycorrelatedwithcoronarydeathrates(r = 0.84) [9]. However, the countries with low satu-rated fat intake and low incidence of CHD were lessindustrialized and differed in many other ways fromthewealthiercountries,particularly inphysicalactiv-ity,obesityand,at that time, smokinghabits.
Studies of blood cholesterol as an intermediary factor
Studies of dietary fats and blood cholesterol level,and those relating cholesterol levels to risk of CHD,have played a central role in the classical diet-hearthypothesis. Studies of dietary factors and blood lipidlevels have mainly been randomized controlled feed-ing trials in 10–50 humans, and hundreds of suchstudies have been conducted. Although details of theshape of the dose–response relationships have been
debated by Keys andHegsted [10, 11], compared iso-calorically with carbohydrate, higher intakes of die-tary cholesterol and saturated fats and lower intakeof polyunsaturated fats clearly increase blood totalcholesterol levels. Monounsaturated fat does notinfluence total serumcholesterol.
A frequent underlying assumption has been that ser-um cholesterol represents a surrogate end-point andthat a dietary factor that changes serum cholesterolwill also change riskofCHD ina similarmanner. Thislogic, however, has been weakened by recognitionthat total serumcholesterol representsmultiple sub-components, including the deleterious LDL andVLDL fractions, and the beneficial HDL component.Thus, the effect of a specific dietary change on totalserum cholesterol might increase, decrease or notinfluence risk of CHD, depending on which choles-terol components were changed. More recent meta-bolic feeding studies havemeasured a variety of lipidfractions and have consistently observed the effectsdemonstrated in Fig. 3. As expected, substitution ofcarbohydrate for saturated fat reduces total choles-terol levels (and LDL cholesterol), but also reducesHDL cholesterol and increases fasting triglyceridelevels. Substitution of monounsaturated fat (or poly-unsaturated fat) for saturated fat similarly reducesLDL cholesterol but does not reduceHDL or increasetriglycerides [12]. Thus, the ratio of total cholesteroltoHDL cholesterol, which appears to summarizewellthe relation between serum lipids and CHD, is notappreciably influenced by saturated fat intake. How-ever, when unsaturated fat replaces carbohydrate,
Hyperglycemia/hyperinsulinemia
Intermediary biological mechanisms
Lipid LevelsLow-density lipoprotein cholesterol
High-density lipoprotein cholesterol
Lipoprotein(a)
Blood pressure
Thrombotic tendency
Cardiac rhythm
Diet Risk ofcoronary heart disease
Endothelial function
Systemic inflammation
Oxidative stress
Homocysteine level
Triglycerides
Fig. 1 Potential pathways mediating the effects of diet onriskof coronaryheartdisease (fromthereference [93]).
10-year coronary incidence per 10 000 men
Keys, 1980
Inci
denc
e
0
1000
2000
3000
0 5 10 15 20 25
DalmatiaVelika Krsna
Zrenjanin
BelgradeRome railro
ad
MontegiorgioCrevalcore
Corfu
Crete
Slavonia
Zutphen
West Finland
East Finland
Ushibuka
Tanushimaru
y = 77 + 78xr = 0.73
% Diet calories from saturated fat
Fig. 2 Ten-year coronary death rates of the cohorts plottedagainst the percentage of dietary calories supplied by satu-rated fattyacids (modifiedfromthe reference [9]).
W. C. Willett | Review: Fats and CHD
14 ª 2012 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2012, 272; 13–24

HDL increases and LDL changes little, suggestingbenefit.
A monotonic relation between blood total cholesterollevel and risk of CHD is firmly established by manystudies inmany countries. However, the ratio of LDLtoHDLcholesterol (or total cholesterol toHDLcholes-terol) provides a stronger prediction of risk becausethese fractions of cholesterol are related to risk inopposite directions. Ongoing work attempts tostrengthen the prediction of CHDby further fraction-ating both the LDLandHDL components, but the va-lueof thissimpleratio remains [13].
The causal relation betweenLDL cholesterol and riskof CHDwas firmly established by randomized trial ofLDL-lowering drugs that reduced CHD incidence[14–16]. Some have argued that the reductions inHDL resulting from a high carbohydrate diet do nothave the same adverse effect as similar reductionscaused by other factors. However, other factors thatinfluence HDL levels including alcohol, estrogens,obesity, smoking, exercise and medications affect
CHD risk in the predicted direction [17, 18]. Never-theless, uncertainties regarding the relevance ofdietary effects on various lipid fractions should beresolved by evaluating the effects of diet on risk ofmyocardial infarction itself, either in carefully con-ductedcohortstudiesor inrandomized trials.
Prospective cohort studies of diet and CHD
Biases related to the selection of control subjects andthe recall of past diet in case–control studies are diffi-cult to avoidordetect; thus, these studies arenot dis-cussed here. Because these biases are eliminated inprospective cohort studies, they shouldprovidemoreconsistent findings on diet and CHD. Many of theearly studies, however, were not primarily designedas investigations into diet andheart disease and thushad numerous limitations. In these studies, the find-ings for specific dietary lipids were weak and incon-sistent, and no relation between saturated fat intakeandriskofCHDwasseen in themostdetailed investi-gation [19].
Although the early prospective studies did not pro-vide consistent findings for any specific dietary lipid,they should not be interpreted as providing strongnegativeevidence.Serious limitationsofmost studiesincluded small size, use of a single 24-h recall for die-tary assessment, lack of updated dietary data duringfollow-up and no adjustment for total energy intakeor other dietary factors. Many of these limitationshave been addressed inmore recent cohort studies ofdiet and CHD. For example, in the Nurses’ HealthStudy, diet was assessed first in 1980with a 61-itemsemi-quantitative food frequency questionnaire, andrepeated assessments have collected since then at4-year intervals using an expanded questionnaire. Adetailedanalysiswasconductedamongst80 082wo-men free of diagnosed CHD in 1980 [20], and during14 years of follow-up, 939 incident cases of acutemyocardial infarction or CHD death were docu-mented. The percentage of energy fromdifferent fats,mutually adjusted for each other, was compared tothe same percentage of energy from carbohydrate(see Fig. 4). By far, the strongest associationwaswithintake of trans fatty acids; saturated fat was onlyweakly and nonsignificantly associated with risk ofCHD, which is consistent with its lack of effect on thetotal cholesterol to HDL ratio. In contrast, monoun-saturated fat was associated with a modestly lowerrisk of CHD, and polyunsaturated fat (specifically li-noleic acid)was associatedwith a substantially lowerrisk.Thestronger inverse relationofpolyunsaturatedfat than with monounsaturated fat may be due to
5.1
mmol L–1 mg dL–1
195
185
175
60
50
100
75
10
western olive oilcomplex carb.diets
20 30 40 50 days
total cholesterol
4.9
4.7
4.51.6
1.4
1.21.2
1.0
0.8
HDL- cholesterol
triglycerides
Fig. 3 Mean serum total andHDL cholesterol and serum tri-glyceride concentrations throughout the experiment. All 48subjects first received a Western-type diet high in saturatedfat for 17 days. For the next 36 days, half of the subjects re-ceived an olive-oil-rich diet (symbol) and the other half a dietlow in fat and high in complex carbohydrates andfibre (sym-bol) (fromthereference [95]; reproducedwithpermission).
W. C. Willett | Review: Fats and CHD
ª 2012 The Association for the Publication of the Journal of Internal Medicine 15
Journal of Internal Medicine, 2012, 272; 13–24

beneficial effects onmultiple pathways in addition toeffects on blood lipids. The percentage of energy fromtotal fat was not associated with risk of CHD. Com-paring one type of fat with another isocalorically, thegreatest reduction in risk would be expected fromreplacing transorsaturated fatwithpolyunsaturatedfat (seeFig.5).
Cohort studies of dietary fats and CHD have beensummarized inapooledanalysis of original data [21].
As in theNurses’HealthStudy, intakeofsaturated fatwas not associated with higher risk of CHD whencompared to the same percentage of energy from car-bohydrates (for a 5% increase in saturated fat,RR = 0.97, 95%CI 0.81–1.16), but saturated fat wasassociatedwithhigher risk if compared to polyunsat-urated fat (for 5% of energy replacement, RR = 1.25,95% CI 1.01–1.56). Total fat intake was not associ-ated with risk of CHD. A limitation of this and mostother pooled analyses is that it usedonly the baselinedata because in most studies, only this informationwas available; as a result, the association with poly-unsaturated fat intake is almost certainly a majorunderestimate of the true relationship. In a recentmeta-analysis of cohort studies using only publisheddata [22], saturated fat was also not associated withrisk of CHD. In this analysis, the unstated compari-son was with other calories in the diet because moststudies did not specifically compare saturated fatwith another source of energy; in most countries,these other calories would be predominately derivedfromrefinedgrainsandsugar.
Studies using biomarkers of fatty acid intake
One alternative to measuring dietary intake is to usebiochemical analyses of fatty acids in plasma lipidfractions, platelet or red cellmembranes, or subcuta-neous adipose as biomarkers of fatty acid intake.These analyses can provide information about dietthat may be difficult to obtain from questionnaires,such as the type of fat used in prepared foods and thedegree to which it has been modified by processing.Althoughattractive inprinciple, fatty acid concentra-tions in blood or tissue need to be interpreted cau-tiouslybecausesaturatedandmonounsaturated fatscan be synthesized endogenously; thus, these mea-surements may not reflect intake. Also, the levels ofessential fatty acids in membranes or lipoproteinsare often strongly regulated so their relation to dietmay be weak and nonlinear. In case–control studies,thevalidity ofplasmaandplatelet fatty acidmeasure-mentswill usuallybequestionable because the levelsmay be affected by the acute infarction itself, or beinfluenced by changes in diet after the diagnosis ofthedisease.
The use of blood specimens collected before theoccurrenceofCHD,most frequentlyasanestedcase–controlanalysis inwhichsamplesarestoredandlateronly incident cases and selected controls are analy-sed, avoids the possible effects of disease or changesin diet after diagnosis on fatty acid levels. Sur-prisingly, few such studies have been conducted to
1%E 2%E 3%E 4%E 5%E
100
80
60
40
20
0–20
–40
Trans
Sat
Mono
Poly
% C
hang
e in
CH
D
Type of Dietary Fat and Risk of Coronary Heart DiseaseThe Nurses' Health Study
14-Year Follow-up
Fig. 4 Multivariate relative risks of coronary heart diseasewith increasing intakesof specific typesof fat, comparedwiththe same energy intake from carbohydrate. Data are basedon14 yearsof follow-up in theNurses’HealthStudy (fromthereference [20]; usedwithpermission).
Nurses’ health studydietary fats and risk of CHD
–80 –60 –40 –20 0 20 40 60 80
Sat -->Carbo (5%E)
Mono -->Carbo (5%E)
Poly --> Carbo (5%E)
Sat--> Mono (5%E)
Sat--> Poly (5%E)
Sat-->Unsat (5%E)
Trans--> Mono (2%E)
Trans --> Poly (2%E)
Trans --> Unsat (2%E)
Change in CHD Risk (%)
Fig. 5 Estimated changes in risk of CHD for isocaloric sub-stitution one type of fat for another. Data are based on14 years of follow-upof 80 082women in theNurse’sHealthStudy (fromthereference [20]).
W. C. Willett | Review: Fats and CHD
16 ª 2012 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2012, 272; 13–24

examine the relation of fatty acids in stored biologicalsamples to risk of CHD. As described later in thischapter, whole blood omega-3 fatty acids in relationto risk of suddencardiacdeathwere studiedamongstmen participating in the Physicians’ Health Study[23], and red cell trans fatty acids were examined inrelation to risk of CHD in the Nurses’ Health Study[24].
Trials of dietary fat modification for prevention of CHD
The most direct test of a diet-heart hypothesis is toconduct a randomized trial amongst healthy personsto determine whether changes in diet can reduce theriskofCHD.Twogeneral strategieshavebeenused totest the classical diet-heart hypothesis: replacementof saturated fat by polyunsaturated fat or replace-mentofsaturated fatbycarbohydrate.Mostof therel-evant trials were conducted several decades ago, butthese remain important despite major limitations,includingthesmall sizeofmost.
Two early trials were conducted amongst institution-alized men, specifically residents of the Los AngelesVeterans Administration Hospital [25] and two Finn-ish mental hospitals [26]. In both studies, patientspassively received modified diets; cholesterol intakewas reduced largely by decreasing egg consumption,and polyunsaturated fats were increased to approxi-mately 20% of calories by substitution for saturatedfats in many foods. In the Veterans study, 846 menwererandomized toeitherof thecontrolorspecialdietand followed for up to 8 years. Seventy-one controlmen and 54 men on the special diets developed defi-nite myocardial infarction or sudden death; this dif-ference was not statistically significant. When cere-bral infarction and other secondary end-points wereincluded, however, the difference was significant(P = 0.02). In the Finnish study, approximately 250men in one hospital received the modified diet and asimilar number in the other served as a control; after6 years, the diets were reversed. CHD rates were re-ducedonthemodifieddiet:51%lower forCHDdeathsalone(P = 0.10)and67%lower forCHDdeathsorma-jor electrocardiogram change (P = 0.001). In a laterUSstudyofsimilardesign, little evidencewasseen fora reduction inCHDamongst the groupwithmodifiedfat intake [27]; however, themean follow-up of 1 yearwas likely tooshort toobserveaneffect.
Because the sample size required for a randomizedtrial of CHD prevention in noninstitutionalized per-sons involving only change in dietary fats was esti-mated to be very large, twomajor trials were initiated
to evaluate the effect on CHD rates of dietary modifi-cationwith simultaneous reduction in other risk fac-tors includingsmoking. Sucha studydesign canpro-vide useful information, but may be difficult tointerpret because the interventions are completelyconfounded, and any effect could be due to any com-bination of the interventions. In the Multiple RiskFactor Intervention Trial (MRFIT), over 12 000 USmen at high risk of CHD were randomly assignedeither to an intensive programme of dietarymodifica-tion, smoking cessation and blood pressure controlor to a control group involving an annual check-up[28]. The dietary intervention was relatively unsuc-cessful, in part because the control group also chan-ged its diet (serum cholesterol was reduced by only5–7% in both groups). No significant reduction inCHDmortality was foundbetween the groups duringthe10-year follow-upperiod. In the16-year follow-upof the MRFIT cohort, long after intervention hasstopped, amarginally significant reduction in deathsowing to acute MI, but not all CHD deaths, was seen[29], but no inference regarding diet is possible forreasonsnoted [29].
TheOsloHeartStudy [30,31]providedmoreconvinc-ing support for thediet-heart hypothesis. In this trial,1232 normotensivemenwith high serum cholesterollevels, 80%of whomalso smoked,were randomly as-signed either to a programme of dietary interventionand smoking cessation or to a control group. Menwho were already following a lipid-lowering diet,based on responses to a simple eight-item question-naire, were excluded before randomization. Dietaryintervention involved primarily a reduction in satu-rated fat and cholesterol; polyunsaturated fat intakeincreased only slightly. During the intervention peri-od, serum cholesterol fell by 17% compared with thecontrol group after 1 year, and after 5 years, it was13% lower in the intervention group. The smokingintervention was less successful; only 25% of thesmokers in the intervention group stoppedcomparedwith 17% in the control group. After 5 years, the inci-dence of nonfatal myocardial infarction and fatalCHD was 47% lower in the intervention group com-paredwithcontrols (P = 0.03). Inaseriesofmultivari-ate analyses to assess the relative effects of dietaryintervention,most of the reduction in CHD incidencecould be attributable to reduction in serum choles-terol. Although active intervention stopped in thispopulationafter 5 years, a similar reduction (approx-imately 45%) was observed after 102 months, andthe difference in total mortality had become margin-ally significant (19 deaths in the intervention groupcomparedwith31in thecontrol group).
W. C. Willett | Review: Fats and CHD
ª 2012 The Association for the Publication of the Journal of Internal Medicine 17
Journal of Internal Medicine, 2012, 272; 13–24
The most recent and largest randomized trial of dietand heart disease was theWomen’sHealth Initiative,in which over 48 000 women were randomized to adiet low in total fat or their usual diet [32]. The majortypes of fatty acids decreased proportionally, so thetype of fat in the diet, as a percentage of total fat, wasnot appreciably changed. Although the main focuswas reduction in breast cancer, CHD and total car-diovascular disease were also primary end-points.After a mean follow-up of 8.1 years, the interventiondiet had no effect on risk of CHD (RR = 0.97; 95% CI0.90–1.06) or total cardiovascular disease. However,this study is largely uninformative because the die-tary interventionhadnoeffectonplasmaHDLcholes-terol or triglycerides, which should have changed ifthere were truly differences in fat intake betweengroups [33].
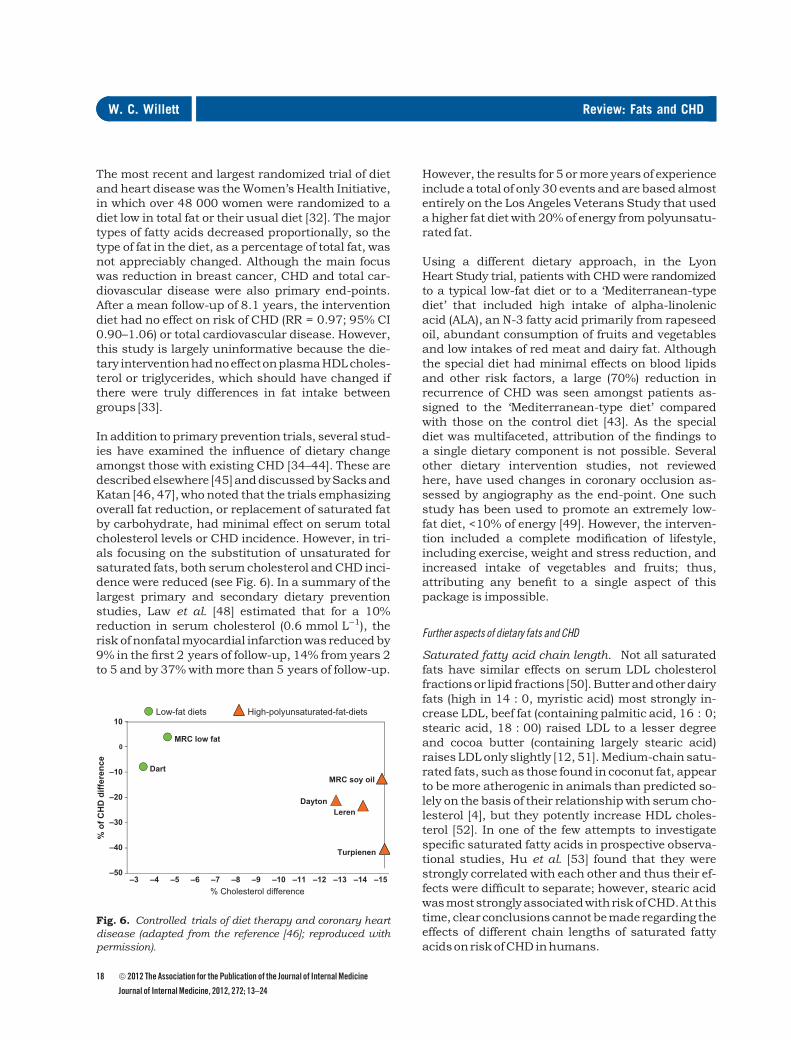
In addition toprimary prevention trials, several stud-ies have examined the influence of dietary changeamongst those with existing CHD [34–44]. These aredescribedelsewhere [45]anddiscussedbySacksandKatan [46, 47],whonoted that the trials emphasizingoverall fat reduction, or replacement of saturated fatby carbohydrate, had minimal effect on serum totalcholesterol levels or CHD incidence. However, in tri-als focusing on the substitution of unsaturated forsaturated fats, both serumcholesterol andCHD inci-dence were reduced (see Fig. 6). In a summary of thelargest primary and secondary dietary preventionstudies, Law et al. [48] estimated that for a 10%reduction in serum cholesterol (0.6 mmol L)1), therisk ofnonfatalmyocardial infarctionwas reducedby9% in the first 2 years of follow-up, 14% from years 2to 5 and by 37%withmore than 5 years of follow-up.
However, the results for 5 ormore years of experienceincludea total of only 30events andarebasedalmostentirely on the Los Angeles Veterans Study that useda higher fat diet with 20%of energy frompolyunsatu-rated fat.
Using a different dietary approach, in the LyonHeart Study trial, patients with CHDwere randomizedto a typical low-fat diet or to a ‘Mediterranean-typediet’ that included high intake of alpha-linolenicacid (ALA), an N-3 fatty acid primarily from rapeseedoil, abundant consumption of fruits and vegetablesand low intakes of red meat and dairy fat. Althoughthe special diet had minimal effects on blood lipidsand other risk factors, a large (70%) reduction inrecurrence of CHD was seen amongst patients as-signed to the ‘Mediterranean-type diet’ comparedwith those on the control diet [43]. As the specialdiet was multifaceted, attribution of the findings toa single dietary component is not possible. Severalother dietary intervention studies, not reviewedhere, have used changes in coronary occlusion as-sessed by angiography as the end-point. One suchstudy has been used to promote an extremely low-fat diet, <10% of energy [49]. However, the interven-tion included a complete modification of lifestyle,including exercise, weight and stress reduction, andincreased intake of vegetables and fruits; thus,attributing any benefit to a single aspect of thispackage is impossible.
Further aspects of dietary fats and CHD
Saturated fatty acid chain length. Not all saturatedfats have similar effects on serum LDL cholesterolfractionsor lipid fractions [50].Butterandotherdairyfats (high in 14 : 0, myristic acid) most strongly in-crease LDL, beef fat (containing palmitic acid, 16 : 0;stearic acid, 18 : 00) raised LDL to a lesser degreeand cocoa butter (containing largely stearic acid)raisesLDLonly slightly [12, 51].Medium-chain satu-rated fats, such as those found in coconut fat, appearto bemore atherogenic in animals than predicted so-lely on the basis of their relationshipwith serumcho-lesterol [4], but they potently increase HDL choles-terol [52]. In one of the few attempts to investigatespecific saturated fatty acids in prospective observa-tional studies, Hu et al. [53] found that they werestrongly correlated with each other and thus their ef-fects were difficult to separate; however, stearic acidwasmoststronglyassociatedwithriskofCHD.At thistime, clearconclusionscannotbemade regarding theeffects of different chain lengths of saturated fattyacidsonriskofCHDinhumans.
–50
–40
–30
–20
–10
0
10
Turpienen
Low-fat diets
MRC low fat
DartMRC soy oil
DaytonLeren
% o
f CH
D d
iffer
ence
–15–14–9–8–7–6–5–4–3 –12–11–10 –13% Cholesterol difference
High-polyunsaturated-fat-diets
Fig. 6. Controlled trials of diet therapy and coronary heartdisease (adapted from the reference [46]; reproduced withpermission).
W. C. Willett | Review: Fats and CHD
18 ª 2012 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2012, 272; 13–24

N-6 polyunsaturated fatty acids. As noted earlier, li-noleic acid (the largemajority ofN-6 polyunsaturatedfat) reduces total and LDL cholesterol, and this evi-dence formed the basis for policies that approxi-matelydoubled intake in theUnitedStatesduring the1960s and 1970s, which corresponded to a largereduction in CHD mortality. More recently, a strongbenefit has been supported by prospective cohortstudies. Interestingly, the strength of the inverseassociation has been stronger than anticipated onlyon the basis of cholesterol lowering, suggesting thatother pathwaysmight be involved, such as reductionin insulin resistance and inflammation that is sup-ported by considerable mechanistic evidence [54,55]. Further, some evidence suggests that higher in-take of N-6 polyunsaturated fat may reduce suddendeath by raising the threshold for ventricular ar-rhythmias [56]. Based simply on the relationshipwith total serumcholesterol, one could conclude thatmaximizing the intake of polyunsaturated fat wouldbedesirable, andsomeguidelinessuggest that intakebe increased to 10% of energy (compared with USaverages of about 3% in the 1950s and 6 or 7% atpresent) with a P ⁄S ratio of 1.0 [57]. Using platelet ag-gregability rather than serum cholesterol to evaluatethe effect of diet, Renaud and colleagues [58] havesuggested that a dietary P ⁄S ratio of 0.6 to 0.8maybesuperior to a ratio of 1.0. Within the Nurses’ HealthStudy, intakes up to about 8% of energy could bestudied and the dose–response relation appeared tobe linearly inverse with no evidence of a plateau [59].Muchhigher intakes are feasible; for example, in Tai-wan, the average intake is about 12% of energy [60].Also, as noted previously, the early intervention trialsthat showed marked reductions in cardiovasculardisease used very high intakes of polyunsaturatedfatty acids, primarily linoleic acid, up to about 20%ofenergy.
Others have suggested that high intakes of linoleicacid, even at current levels, are harmful and shouldbe reduced [61]. This theoretical argument is basedon the possibility that N-6 and N-3 polyunsatu-rated fatty acids in the diet compete with eachother in elongation and desaturation pathways andthat longer-chain N-6 polyunsaturated fatty acidsare precursors to pro-inflammatory eicosanoids.This ignores that the elongation of linoleic acid tolonger-chain fatty acids is highly regulated and thatlinoleic acid can influence CHD risk favourablythrough many other pathways. There is no actualevidence that linoleic acid is pro-inflammatory inthe range of current diets, and the opposite may betrue [54].
N-3 fatty polyunsaturated fatty acids. Low rates ofCHD in Japan andGreenland led to speculation thatthe high consumption of fish in these areas might beprotective [62, 63]. The initial hypothesized mecha-nism was that the high concentrations of N-3 fattyacids in fish reduce thrombus formation in coronaryarteries by inhibiting platelet function. A benefit wassupported by the finding that Dutchmen consumingmore than30 g of fishper dayhad only about half therisk of fatal CHD comparedwithmenwho consumednone [64]. Lower rates ofCHDmortality amongstper-sonswho consumedhigher amounts of fishwere alsoobserved in other early prospective studies [65–68],but not in large prospective studies of CHD incidencethat included nonfatal end-points [69–71]. More re-cently, omega-3 fatty acids have been hypothesizedto act primarily by increasing the threshold for ven-tricular fibrillation [72]; if so, there may be little rela-tion with nonfatal CHD and the benefit may be onlyfor fatal CHD and sudden cardiac death. In a meta-analysis of prospective studies and randomized tri-als, Mozaffarian [73] estimated that consuming250 mg day)1 of EPA + DHA (equivalent to approxi-mately 1–2 servings per week of oily fish), comparedto no intake, was associated with a 36% lower risk ofCHD death, but little additional benefit was gainedwith higher intakes. Even stronger inverse associa-tions were seen in nested case–control studies usingfatty acid levels in blood; for example, in the Physi-cians’ Health Study, the adjusted relative risk ofsudden cardiac death for men in the highest versuslowestquintilewas0.19 (95%CI0.05–0.71) [23].
In a recent, large randomized trial in theNetherlands[74], neither supplementation with long-chain fishoils nor ALA, the major plant N-3 fatty acid, reducedoverall incidence of CHD. Nonsignificant effects werealso seen for ventricular arrhythmias, but the num-berofeventswasmodestandtheconfidence intervalsincluded important reductions in risk (for fish oilsRR = 0.90, 95% CI 0.65–1.26), and for ALARR = 0.79, 95% CI 0.57–1.10). The observationaldata based on fatty acid analyses should show stron-ger associations than would be seen in randomizedtrials with fish oil supplements because in the obser-vational data, levels representing intakes above thethreshold for maximal benefit are compared to verylow levels. In a randomized trial, the control grouphas the distribution of levels in a population; manypersons may be above the threshold for benefit andnot experience any benefit from supplementation.Because fish consumption differs greatly amongstvarious populations, this means that the results ofsupplementation trials are likely to vary; if the
W. C. Willett | Review: Fats and CHD
ª 2012 The Association for the Publication of the Journal of Internal Medicine 19
Journal of Internal Medicine, 2012, 272; 13–24

population intake of fish is relatively high, the find-ings could be null but in a population with low fishintake, an important benefit might be seen. Notably,N-3 fatty acid intake from both fish and plant formsis high in the Netherlands, where the recent lack ofbenefitwasseen [75].
Although benefits of long-chain omega-3 fatty acidsin reducing cardiac death are well supported, andthis has been translated into advice to consume atleast two servings of fish per week [76], additional is-sues remain unresolved. Most important is whetherALA has similar benefits in reducing cardiovasculardisease [77]. This is a major issue globally becausefish consumption is very low in vast regions of theworld [75], and the catch of wild fish cannot be in-creased further.
Trans fatty acids. Trans fatty acids are producedwhen liquid vegetable oils, which normally have alldouble-bonds in the cis position, are heated in thepresenceofmetalcatalysts to formvegetableshorten-ingandmargarine.Thisprocess,calledpartialhydro-genation, was developed around 1900 and produc-tion increased steadily until about the 1960s asprocessed vegetable fats displaced animal fats inmanydiets, first becauseof costsand thenbecauseofpurported health benefits. This increase has oc-curred worldwide; for example, in parts of India, apartially hydrogenated fat containing approximately60% of fat as trans isomers is widely used as areplacement for ghee (butter fat) [78]. Fat from cattleand other ruminants (for example, in red meat andbutter) also has small amounts (typically 4 or 5%) oftrans fatty acids due biohydrogenation in the rumenof theseanimals.
Concern that trans fatty acidsmight have adverse ef-fects on CHD risk was greatly heightened by a con-trolled feeding study by Mensink and Katan [79] inwhich 10% of energy as trans fatty acids raised LDLcholesterol to a similar degree as did saturated fatand also reduced HDL when both were compared tomonounsaturated fat. Thus, the increase in the ratioof total cholesterol to HDL cholesterol owing to transisomerswas about twice that seenwith saturated fat.These findings have been reproduced consistently,and trans fatty acids have also been shown to reducethe particle size of LDL cholesterol, increase bloodlevels of Lp(a), increase inflammatory factors and ad-verselyaffect endothelial function [80].
Positive associations between intake of trans fattyacids and risk of CHD were observed in the Nurses’
HealthStudycohort [81] andconfirmed inother largeprospectivestudies [80]. Inameta-analysis, thesum-mary relative risk for an increment of 2% of energyfrom trans fat was 1.23 (95% CI 1.11–1.37;P < 0.001). More recently, the relation between transfatty acids in red cell membranes and risk of CHDwas examined in the Nurses’ Health Study using anested case–control design [24]; the relative risk forthe highest versus lowest quartile was 3.3 (1.5–7.2,P for trend<0.01).
The combination of many metabolic studies demon-stratingadverseeffectsof trans fatty acidsonblood li-pid fractions and prospective epidemiologic studieshas provided strong support for an adverse effect onCHD risk. Thus, actions to reduce intake have in-cludedbanning theuseofpartially hydrogenated fatsin Denmark, Brazil and Chile and in many cities intheUnited States. Althoughmuch progress has beenmade inreducing the intakeofsomecountries, intakeremains high in other parts of the world. Also, even ifthe average intake has been greatly reduced in acountry, amodest percent of the populationmay stillconsume largeamountsof trans fats.
The number of different trans isomers in partiallyhydrogenated vegetable oils is very large because thetrans double-bonds can vary in number (usually 0, 1or2)andposition in thecarbonchain,andthenumberof carbonsatomscandiffer. In twostudiesusinganal-yses of red cells or adipose tissue [24, 82], 18 : 2 transisomers were substantially more strongly associatedwith risk of CHD than were 18 : 1 trans isomers. Thiscan have practical implications because if the degreeof partial hydrogenation is reduced but not elimi-nated, the amounts of 18 : 2 trans isomers can be in-creased. This light degree of hydrogenation has oftenbeen usedwhen the goal was to destroy ALA (which issusceptible to oxidation, thus producing rancidityand shortened shelf life) rather than to create a hardfat.Althoughourunderstandingof theeffectsofdiffer-ent trans isomers is incomplete, the goal should be toeliminatepartialhydrogenation,not just reduce it.
Trans isomers fromruminant fatswill usually not ex-ceedonepercentof fatty acids, evenwithhigh intakesof red meat and butter fat, but this has become ofgreater interest as other sources of trans fatty acidshave been reduced. The relation between the intakeof trans fatty acids from ruminants and the risk ofCHD has been examined in four prospective studies;none identified a significant positive association andin three a nonsignificant inverse trend was observed[81,83–85].
W. C. Willett | Review: Fats and CHD
20 ª 2012 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2012, 272; 13–24

Although major progress has been made in under-standing the consequences of partial hydrogenationof vegetable oils, not all issues regarding cooking fatsare resolved. The sustainedheating of fats, asused inthe deep frying processes of the fast food industry,can lead to the oxidation of polyunsaturated fattyacids [86], but intake is usually low because oxida-tion creates undesirable flavours. Virtually, no epi-demiologicdataexistontheconsequencesofoxidizedcooking fats.
Fatty acids, dietary fats and dietary patterns. Moststudies have focused on specific fatty acids ratherthan ondietary fats, even though fats arewhatwe se-lect and eat, and these contain a combination of dif-ferent fatty acids in the triglyceride molecule. Fur-ther, plant oils contain many other componentsbesides fatty acids, usually a variety of antioxidantssuchasvitaminEandpolyphenols,whichprotect theembryonic plant in the seeds from which the oils areextracted. Also, fatty acids from animal sources arenot consumed in isolation; other components includecholesterol and other sterols. Many of these fats areconsumed as part of foodswithmany other constitu-ents such as in cheese and redmeat, which containsproteins, abundant heme iron andmany other nutri-entandnon-nutrientcomponents [87].
Amongst the fewstudies tospecificallycompare typesof dietary fats in relation to risk of CHD was a largeCosta Rican case–control study of CHD designed tocompare soybean oil with palm oil, which washypothesized to be less adverse than predicted owingto itshighcontent of tocotrienols [88]. In this compar-ison, consumptionof soybeanoilwasassociatedwiththe lowest risk, consistentwith its fatty acid composi-tion that includes bothN-6 andN-3 polyunsaturatedfatty acids. In an example explicitly comparing foodsources, red meat, a major source of saturated fat,was associated with higher risk of CHD when com-paredwith othermajor protein sources [89].Whetherthesubstantial differencesweredueonly to thediffer-ences in fatty acid composition is not clear, but com-ponentsof these foodsmaycontribute.Suchcompar-isons can provide more direct evidence for dietaryguidance thandatabasedsolelyon fattyacid intakes.
Dietary fatty acids and other diseases
Decisions about diet should be made considering allimportant outcomes. Although dietary total fat andsaturated fat have been hypothesized to increaserisks of many cancers, no clear relationships havebeen documented despite intense investigation.
Some evidence suggests that risks of prostate cancer[90] and macular degeneration [91] might be in-creased by high intakes of ALA, the main plant N-3fatty acid, but these relationshipsneed further inves-tigation. In the most detailed dietary study of type 2diabetes, theratioofpolyunsaturated tosaturated fatwas associatedwith reduced risk and trans fat intakewas associated with elevated risk [92]. Thus, at pres-ent, the relation between fatty acids and risk of CHDcan serve as the basis for dietary guidance abouttypesof fat.
Additional diet-heart hypotheses
Althoughsubstantial evidence supports amajor role ofdietary fatty acids and fats in the aetiology of CHD,many other aspects of diet are also likely to influencerisk of this disease, possiblymediatedby changes in li-pid fractions, platelet aggregability, fibrinogen levels,arrhythmia, blood pressure, glucose levels, insulinresistance, endothelial damage, obesity and othermechanisms that have yet to be discovered. These arediscussedelsewhere [93,94]andincludealcoholicbev-erages, sugar-sweetened beverages, glycaemic load,dietaryfibre, fruitandvegetables,andsodiumintake.
Summary
Excess body fat, the result of the imbalance betweenenergy intake and expenditure, is a powerful risk fac-tor for CHD but in many randomized trials has notbeen related to the percentage of energy from dietaryfat. Abundant evidence from controlled feeding stud-ies of blood lipids, prospective observational studiesand limited randomized trials have shown that spe-cific dietary fatty acids play important roles in thecause and prevention of CHD. Trans fatty acids frompartially hydrogenated vegetable oils have clear ad-verseeffectsandshouldbeeliminated.Modestreduc-tions in CHD rates by further decreases in saturatedfat arepossible if saturated fat is replacedbyacombi-nation of poly- and mono-unsaturated fat, and thebenefits of polyunsaturated fat appear strongest.However, little or no benefit is likely if saturated fat isreplacedbycarbohydrate,but thiswill inpartdependon the form of carbohydrate. Because both N-6 andN-3 polyunsaturated fatty acids are essential and re-duce riskofheartdisease, the ratioofN-6 toN-3 isnotuseful and can be misleading. The optimal amountsofbothneedtobebetterdefined.
Also, much evidence indicates that replacement ofred meat with alternative protein sources includingfish and nuts will reduce risk of CHD. Additional
W. C. Willett | Review: Fats and CHD
ª 2012 The Association for the Publication of the Journal of Internal Medicine 21
Journal of Internal Medicine, 2012, 272; 13–24

reduction in risk will be achieved by a diet generousin fruits, vegetables and whole grains and low in re-fined starches, sugar-sweetened beverages, potatoesandsalt.
Conflict of interest
Noconflictof interest todeclare.
References
1 GordonT. Thediet-heart idea.Outlineofahistory.AmJEpidemiol
1988;127:220–5.
2 AnitschkowN.Ahistoryofexperimentationonarterioatheroscle-
rosis in animals. In: Blumenthal HT, ed. Cowdry’s Arteriosclero-
sis,2ndedn.Springfield, IL,USA:Macmillan,1967;21–44.
3 Katz LN, Stamler JS. Experimental Atherosclerosis. Springfield:
CharlesC.ThomasPublishing,1953.
4 Wissler RW, Vesselinovitch D. The effects of feeding various die-
tary fats on the development and regression of hypercholesterol-
emiaandatherosclerosis.AdvExpMedBiol1975;60:65–76.
5 GrundySM,BilheimerD,BlackburnHetal.Rationaleof thediet-
heart statement of the American Heart Association. Report of
NutritionCommittee.Circulation1982;65:839A–54A.
6 Institute ofMedicine.Dietary reference intakes for energy, carbo-
hydrate, fiber, fat, fatty acids, cholesterol, protein, and amino
acids (macronutrients). A Report of the Panel on Macronutrients,
Subcommittees on Upper Reference Levels of Nutrients and Inter-
pretationandUsesofDietaryReference Intakes,andtheStanding
Committee on the Scientific Evaluation of Dietary Reference
Intakes. http://www.nap.edu/catalog/10490.html.Washing-
ton,DC,USA:NationalAcademyofSciences,2002.
7 KatoH,TillotsonJ,NichamanMZ,RhoadsGG,HamiltonHB.Ep-
idemiologic studiesof coronaryheart disease and stroke inJapa-
nesemen living in Japan, Hawaii and California.AmJEpidemiol
1973;97:372–85.
8 Robertson TL, KatoH, RhoadsGG et al.Epidemiologic studies of
coronary heart disease and stroke in Japanese men living in
Japan,Hawaii andCalifornia: incidence ofmyocardial infarction
and death from coronary heart disease. Am J Cardiol 1977; 39:
239–43.
9 Keys A. Seven Countries: A Multivariate Analysis of Death and
Coronary Heart Disease. Cambridge, MA: Harvard University
Press,1980.
10 Keys A. Serum-cholesterol response to dietary cholesterol. Am J
ClinNutr1984;40:351–9.
11 Hegsted DM. Serum-cholesterol response to dietary cholesterol:
a re-evaluation.AmJClinNutr1986;44:299–305.
12 Mensink RP, Katan MB. Effect of dietary fatty acids on serum
lipids and lipoproteins: a meta-analysis of 27 trials. Arterioscler
Thromb1992;12:911–9.
13 Sacks FM. Lipid and lipoproteinmetabolism, and risk for cardio-
vascular disease. In: Eckel RH, ed.Metabolic Risk for Cardiovas-
cular Disease: The AHA Clinical Series. West Sussex, UK: Wiley-
Blackwell, 2011;18–40.
14 LipidResearchClinicsProgram.TheLipidResearchClinicscoro-
naryprimaryprevention trial results. I. Reduction in incidence of
coronaryheartdisease.JAMA1984;251:351–64.
15 Shepherd J, Cobbe SM, Ford I et al. Prevention of coronary heart
disease with pravastatin in men with hypercholesterolemia –
West of Scotland Coronary Prevention Study Group. N Engl J
Med1995;333:1301–7.
16 Sacks FM, Pfeffer MA, Moye LA et al. The effect of pravastatin on
coronaryevents aftermyocardial infarction inpatientswithaver-
age cholesterol levels – cholesterol and recurrent events trial
investigators.NEnglJMed1996;335:1001–9.
17 Sacks FM,WillettWC.More on chewing the fat – the good fat and
thegoodcholesterol.NEnglJMed1991;325:1740–2.
18 KatanMB, GrundySM,WillettWC. Should a low-fat, high-carbo
hydrate diet be recommended for everyone?Beyond low-fat diets
NEnglJMed1997;337:563–7.
19 Shekelle RB, Shryock AM, Paul O et al. Diet, serum cholesterol,
and death from coronary heart disease: the Western Electric
Study.NEnglJMed1981;304:65–70.
20 Hu F, Stampfer MJ, Manson JE et al. Dietary fat intake and the
riskof coronaryheartdisease inwomen.NEngl JMed1997;337:
1491–9.
21 Jakobsen MU, O’Reilly EJ, Heitmann BL et al. Major types
of dietary fat and risk of coronary heart disease: a pooled
analysis of 11 cohort studies. Am J Clin Nutr 2009; 89:
1425–32.
22 Siri-Tarino PW, Sun Q, Hu FB, Krauss RM. Meta-analysis of
prospective cohort studies evaluating the association of satu-
rated fat with cardiovascular disease. Am J Clin Nutr 2010; 91:
535–46.
23 Albert CM, Campos H, Stampfer MJ et al. Blood levels of long-
chain n-3 fatty acids and the risk of sudden death. N Engl J Med
2002;346:1113–8.
24 Sun Q, Ma J, Campos H et al. A prospective study of trans fatty
acids in erythrocytes and risk of coronary heart disease.Circula-
tion2007;115:1858–65.
25 Dayton S, Pearce ML, Hashimoto S, Dixon WJ, Tomiyasu U. A
controlledclinical trialofadiethighinunsaturatedfat inprevent-
ing complications of atherosclerosis.Circulation 1969; 40(Suppl
II):1–63.
26 Turpeinen O, Karvonen MJ, Pekkarinen M, Miettinen M, Elosuo
R, Paavilainen E. Dietary prevention of coronary heart disease:
the Finnish Mental Hospital Study. Int J Epidemiol 1979; 8: 99–
118.
27 Frantz IDJ, Dawson EA, Ashman PL et al. Test of effect of lipid
lowering by diet on cardiovascular risk: theMinnesota Coronary
Survey.Arteriosclerosis1989;9:129–35.
28 MultipleRiskFactor InterventionTrial ResearchGroup.Multiple
risk factor intervention trial: risk factor changes and mortality
results.JAMA1982;248:1465–77.
29 Multiple RFITRG. Mortality after 16 years for participants ran-
domized to the multiple risk factor intervention trial. Circulation
1996;94:946–51.
30 Hjermann I, Velve Byre K, Holme I, Leren P. Effect of diet and
smoking intervention on the incidence of coronaryheart disease.
Report from the Oslo Study Group of a randomised trial in
healthymen.Lancet1981;2:1303–10.
31 Hjermann I, Holme I, Leren P. Oslo study diet and antismoking
trial; resultsafter102 months.AmJMed1986;80:7–11.
32 HowardBV, VanHornL,Hsia J et al. Low-fat dietarypattern and
risk of cardiovascular disease: the Women’s Health Initiative
Randomized Controlled Dietary Modification Trial. JAMA 2006;
295:655–66.
33 Willett WC. The WHI joins MRFIT: a revealing look beneath
thecovers.AmJClinNutr2010;91:829–30.
34 Morrison LM.Diet in coronary atherosclerosis.JAMA1960;173:
884–8.
W. C. Willett | Review: Fats and CHD
22 ª 2012 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2012, 272; 13–24

35 Koranyi A. Prophylaxis and treatment of the coronary syndrome.
TherHung1963;12:17–20.
36 Rose GA, Thomson WB, Williams RT. Corn oil in treatment of
ischaemicheartdisease.BrMedJ1965; I:1531–3.
37 Morris JN, Ball KP, Antonis A et al. Controlled trial of soya-bean
oil inmyocardial infarction.Lancet1968;2:693–9.
38 Leren P. The Oslo diet-heart study. Eleven-year report. Circula-
tion1970;42:935–42.
39 Woodhill JM, Palmer AJ, Leelarthaepin B, McGilchrist C,
Blacket RB. Low fat, low cholesterol diet in secondary
prevention of coronary heart disease. Adv Exp Med Biol 1978;
109:317–30.
40 BurrML,FehilyAM,GilbertJFetal.Effectsofchanges in fat,fish,
and fibre intakes on death andmyocardial reinfarction: diet and
reinfarction trial (DART).Lancet1989;2:757–61.
41 Watts GF, Lewis B, Brunt JNH et al. Effects of coronary artery
disease of lipid-lowering diet, or diet plus cholestyramine, in the
St. Thomas’ Atherosclerosis Regression Study (STARS). Lancet
1992;339:563–9.
42 Singh RB, Rastogi SS, Verman R et al. Randomised controlled
trialof cardioprotectivediet inpatientswith recentacutemyocar-
dial infarction: results of one year follow up.BrMed J1992;304:
1015–9.
43 de Lorgeril M, Renaud S, Mamelle N et al.Mediterranean alpha-
linolenic acid-rich diet in secondary prevention of coronaryheart
disease [Erratum in: Lancet 1995; 345: 738]. Lancet 1994;
343:1454–9.
44 Ball KP, Hanington E, McAllen PM et al. Low-fat diet in myocar-
dial infarction–acontrolled trial.Lancet1965;2:501–4.
45 Willett WC, Lenart EB. Dietary factors. In: Manson JE, Ridker
PM, Gaziano JM, Hennekens CH, eds. Prevention of Myocardial
Infarction. New York, NY, USA: Oxford University Press, 1996;
351–83.
46 Sacks F. Dietary fats and coronary heart disease. Overview.
JCardiovascRisk1994;1:3–8.
47 Sacks FM, Katan MB. Randomized clinical trials on the ef-
fects of dietary fat and carbohydrate on plasma lipoproteins and
cardiovascular disease. Am J Med 2002; 113(Suppl 9B): 13S–
24S.
48 LawMR,WaldNJ, ThompsonSG.Byhowmuchandhowquickly
does reduction in serum cholesterol concentration lower risk of
ischaemicheartdisease?BrMedJ1994;308:367–72.
49 Ornish D. Dr. Dean Ornish’s Program for Reversing Heart
Disease.NewYork:BalantineBooks,1990.
50 Hunter JE, Zhang J, Kris-Etherton PM. Cardiovascular disease
risk of dietary stearic acid comparedwith trans, other saturated,
and unsaturated fatty acids: a systematic review. Am J Clin Nutr
2010;91:46–63.
51 DenkeMA,GrundySM.Effects of fatshigh in stearic acidon lipid
and lipoprotein concentrations inmen.AmJ Clin Nutr 1991; 54:
1036–40.
52 KatanMB,ZockPL,MensinkRP.Effectsof fats and fatty acidson
blood lipids in humans: an overview. Am J Clin Nutr 1994;
60(Suppl6):1017S–22S.
53 HuFB,StampferMJ,MansonJEetal.Dietary saturated fats and
their food sources in relation to the risk of coronary heart disease
inwomen.AmJClinNutr1999;70:1001–8.
54 WillettWC. The role of dietary n-6 fatty acids in the prevention of
cardiovascular disease. J Cardiovasc Med (Hagerstown) 2007;
8(Suppl1):S42–5.
55 RiserusU,WillettWC,HuFB.Dietary fats andprevention of type
2diabetes.ProgLipidRes2009;48:44–51.
56 Charnock JS,McLennan PL, AbeywardenaMY. Dietarymodula-
tion of lipid metabolism and mechanical performance of the
heart.MolCellBiochem1992;116:19–25.
57 Anonymous.ConsensusConference. Loweringblood cholesterol
topreventheartdisease.JAMA1985;253:2080–6.
58 RenaudS,GodseyF,DumontE,ThevenonC,OrtchanianE,Mar-
tin JL. Influence of long-term diet modification on platelet func-
tion and composition in Moselle farmers. Am J Clin Nutr 1986;
43:136–50.
59 Oh K, Hu FB, Manson JE, Stampfer MJ, Willett WC. Dietary fat
intake and risk of coronary heart disease in women: 20 years of
follow-upof theNurses’HealthStudy.AmJEpidemiol2005;161:
672–9.
60 Lyu LC, YehCY, LichtensteinAH, Li Z,Ordovas JM,Schaefer EJ.
Association of sex, adiposity, and diet with HDL subclasses in
middle-agedChinese.AmJClinNutr2001;74:64–71.
61 Simopoulos AP. The importance of the omega-6 ⁄ omega-3 fatty
acid ratio in cardiovascular disease and other chronic diseases.
ExpBiolMed (Maywood)2008;233:674–88.
62 Bang HO, Dyerberg J, Sinclair HM. The composition of the Eski-
mo food in North Western Greenland. Am J Clin Nutr 1980; 33:
2657–61.
63 KagawaY,NishizawaM,SuzukiM et al.Eicosapolyenoic acids of
serum lipids of Japanese islanders with low incidence of cardio-
vasculardiseases.JNutrSciVitaminol1982;28:441–53.
64 Kromhout D, Bosscheiter EB, de Lezenne Coulander C. The in-
verse relation between fish consumption and 20-year mortality
fromcoronaryheartdisease.NEnglJMed1985;312:1205–9.
65 Shekelle RB,Missell L, PaulO, ShryockAM, Stamler J. Fish con-
sumption and mortality from coronary heart disease (letter).
NEnglJMed1985;313:820–4.
66 Norell SE, Ahlbom A, Feychting M, Pedersen NL. Fish consump-
tion and mortality from coronary heart disease. Br Med J 1986;
293:426.
67 Dolecek TA. Epidemiological evidence of relationships between
dietary polyunsaturated fatty acids andmortality in themultiple
risk factor intervention trial. Proc Soc Exp Biol Med 1992; 200:
177–82.
68 Kromhout D, Feskens EJM, Bowles CH. The protective effect of
a small amount of fish on coronary heart disease mortality in an
elderlypopulation. IntJEpidemiol1995;24:340–5.
69 Curb JD, Reed DM. Fish consumption and mortality from coro-
naryheartdisease (letter).NEnglJMed1985;313:820–4.
70 Ascherio A, RimmEB, Stampfer MJ, Giovannucci E, Willett WC.
Dietary intake of marine n-3 fatty acids, fish intake and the risk
of coronary disease among men. N Engl J Med 1995; 332:
977–82.
71 MorrisMC,MansonJE,RosnerB,BuringJE,WillettWC,Henne-
kens CH. Fish consumption and cardiovascular disease in the
Physicians’ Health Study: a prospective study. Am J Epidemiol
1995;142:166–75.
72 Leaf A. Omega-3 fatty acids and prevention of ventricular
fibrillation. Prostaglandins Leukot Essent Fatty Acids 1995; 52:
197–8.
73 MozaffarianD. Fish and n-3 fatty acids for the prevention of fatal
coronaryheart disease and sudden cardiacdeath.AmJClinNutr
2008;87:1991S–6S.
74 KromhoutD,GiltayEJ, Geleijnse JM.n-3 fatty acids and cardio-
vascular events after myocardial infarction. N Engl J Med 2010;
363:2015–26.
75 Petrova S, Dimitrov P, Willett WC, Campos H. The global avail-
abilityofn-3 fattyacids.PublicHealthNutr2011;14:1–8.
W. C. Willett | Review: Fats and CHD
ª 2012 The Association for the Publication of the Journal of Internal Medicine 23
Journal of Internal Medicine, 2012, 272; 13–24

76 U.S. Department of Agriculture. Dietary Guidelines for Ameri-
cans.Washington,DC,USA:U.S.Gov’tPrintingOffices,2010.
77 CamposH, Baylin A,WillettWC. Alpha-linolenic acid and risk of
nonfatal acute myocardial infarction. Circulation 2008; 118:
339–45.
78 Achaya KT. Fat status of Indians – a review. J Sci Ind Res 1987;
46:112–26.
79 MensinkRP, ZockPL,KatanMB,HornstraG.Effect of dietary cis
and trans fatty acids on serum lipoprotein [a] levels in humans.
JLipidRes1992;33:1493–501.
80 Mozaffarian D, KatanMB, Ascherio A, Stampfer MJ, Willett WC.
Trans fatty acidsandcardiovasculardisease.NEngl JMed2006;
354:1601–13.
81 Willett WC, Stampfer MJ, Manson JE et al. Intake of trans fatty
acids and risk of coronary heart disease among women. Lancet
1993;341:581–5.
82 Baylin A, KabagambeEK, Ascherio A, SpiegelmanD, CamposH.
High 18:2 trans-fatty acids in adipose tissue are associated with
increased risk of nonfatal acute myocardial infarction in costa
ricanadults.JNutr2003;133:1186–91.
83 Pietinen P, Ascherio A, Korhonen P et al. Intake of fatty acids and
risk of coronary heart disease in a cohort of Finnish men: the
ATBCStudy.AmJEpidemiol1997;145:876–87.
84 Oomen C, OckeM, Feskens E, van Erp-Baart M, Kok F, Kromh-
out D. Association between trans fatty acid intake and 10-year
risk of coronary heart disease in the Zutphen Elderly Study: a
prospectivepopulation-basedstudy.Lancet2001;357:746–51.
85 Jakobsen MU, Overvad K, Dyerberg J, Heitmann BL. Intake of
ruminant trans fatty acids and risk of coronary heart disease.
IntJEpidemiol2008;37:173–82.
86 KrannerJ.Dietaryadvanced lipidoxidationendproductsare risk
factors tohumanhealth.MolNutrFoodRes2007;51:1094–101.
87 AstrupA,Dyerberg J,ElwoodP et al.The role of reducing intakes
of saturated fat in the prevention of cardiovascular disease:
wheredoes the evidence stand in2010?AmJClinNutr2011;93:
684–8.
88 Kabagambe EK, Baylin A, Ascherio A, Campos H. The type of oil
used for cooking is associated with the risk of nonfatal acute
myocardial infarction incosta rica.JNutr2005;135:2674–9.
89 Bernstein AM, Sun Q, Hu FB, Stampfer MJ, Manson JE, Willett
WC. Major dietary protein sources and risk of coronary heart
disease inwomen.Circulation2010;122:876–83.
90 Giovannucci E, Liu Y, Platz EA, Stampfer MJ, Willett WC. Risk
factors for prostate cancer incidence and progression in the
health professionals follow-up study. Int J Cancer 2007; 121:
1571–8.
91 Cho E, Hung S, Willett WC et al. Prospective study of dietary fat
and the risk of age-relatedmacular degeneration. AmJ Clin Nutr
2001;73:209–18.
92 HuFB,MansonJE,StampferMJetal.Diet, lifestyle, and the risk
of type 2 diabetes mellitus in women. N Engl J Med 2001; 345:
790–7.
93 HuFB,WillettWC.Optimal diets for preventionof coronaryheart
disease.JAMA2002;288:2569–78.
94 Mente A, de Koning L, Shannon HS, Anand SS. A systematic re-
viewof theevidence supportinga causal linkbetweendietary fac-
tors and coronary heart disease. Arch Intern Med 2009; 169:
659–69.
95 Mensink RP, Katan MB. Effect of monounsaturated fatty acids
versus complex carbohydrates on high-density lipoprotein in
healthymenandwomen.Lancet1987;1:122–5.
Correspondence: Walter C. Willett MD, DrPH, Department of
Nutrition,Harvard School of PublicHealth, 665HuntingtonAvenue,
Boston,MA02115,USA.
(fax: (617) 432 0464; e-mail: [email protected])
W. C. Willett | Review: Fats and CHD
24 ª 2012 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine, 2012, 272; 13–24