jnm/diagndbtic nuclear medicinejnm.snmjournals.org/content/17/4/241.full.pdf · ease(ashd)...
TRANSCRIPT

Myocardial studies with 99mTc@labeled phosphate agents were obtained in 20 patients without demonstrable cardiovascular disease, 24patients with unstable arteriosclerotic heart digease (ASHD) without acute infarction, and sixpatients with myocardiopathy. The patientswithout cardiovascular disease showed no localization of tracer; the patients with unstable ASHDand without acute infarction showed nonfocal
ill-defined accumulation of tracer; and the patients with myocardiopathy showed diffuse accumulation of tracer throughout the confinesof an enlarged cardiac outline. Careful evaluation of both the distribution and intensity ofthe activity, in conjunction with the clinical picture, allows differentiation among these diseaseprocesses. Since ischemic areas around infarctedtissue may show increased activity, the value ofthis technique for sizing acute myocardial infarction may be limited.
Bonte reported that eemTc@stannouspyrophosphatelocalizes in dog myocardium after experimentallyproduced myocardial infarction (1 ) . Investigationsin humans showed positive myocardial images in 15patients with acute transmural myocardial infarction(2) . Of these patients 13 gave positive studies 3—7days after the initial episode. Electrocardiograms(ECG) correlated well with the localization of theinfarct. Two patients with arteriosclerotic heart disease (ASHD) showed questionably increased activity in the region of the left ventricle (2) . Acutesubendocardial infarction has also been documentedwith this technique (3). Willerson et al have reported that of 55 patients admitted for chest painwho did not evolve ECG or enzyme evidence ofmyocardial infarction, none showed positive localiza
tion of tracer to the myocardium (4) . In anotherstudy, Willerson et al reported on 202 patients admitted to their coronary care unit with chest painof varying origins (5) . Of these, 101 did not developclinical or electrocardiographic evidence of acutemyocardial infarction and 92 had negative myocardial scintigrams. Seven of the remaining nine patientshad “unstableangina pectoris―and a faint, but definitely positive myocardial scintigram (5) . The present investigation was undertaken to assess the possible cardiac uptake of radiophosphate in patientswith no demonstrable cardiac disease, with arteriosclerotic heart disease, and with myocardiopathy.
MATERIALS AND METHODS
Fifteen millicuries of either eemTc_stannous polyphosphate (New England Nuclear Corp., North Bitlerica, Mass.) or oemTc@pyrophosphate (TechneScanPYP Kit, Mallinckrodt/Nuclear, St. Louis, Mo.)was administered intravenously to each patient. Thetracer was prepared according to the manufacturer's
Received May 24, 1975; revision accepted Oct. 22, 1975.For reprints contact: Louis A. Perez, Dept. of Nuclear
Medicine, Norwalk Hospital, 24 Stevens St., Norwalk, Conn.06856.
FIG. 1. Normalheart(Group1).Radioactivityis notincreasedin vicinity of heart.
241Volume 17, Number 4
jnm/DIAGNDBTIC NUCLEAR MEDICINE
LOCALIZATION OF MYOCARDIAL DISORDERS
OTHER THAN INFARCTION WITH
99mTCLABELED PHOSPHATE AGENTS
LouisA. Perez, David B. Hayt, and Leonard M. Freeman
Misericordia Hospital Medical Centerand the Albert Einstein College of Medicine, Yeshiva University, Bronx, New York
by on August 9, 2019. For personal use only. jnm.snmjournals.org Downloaded from
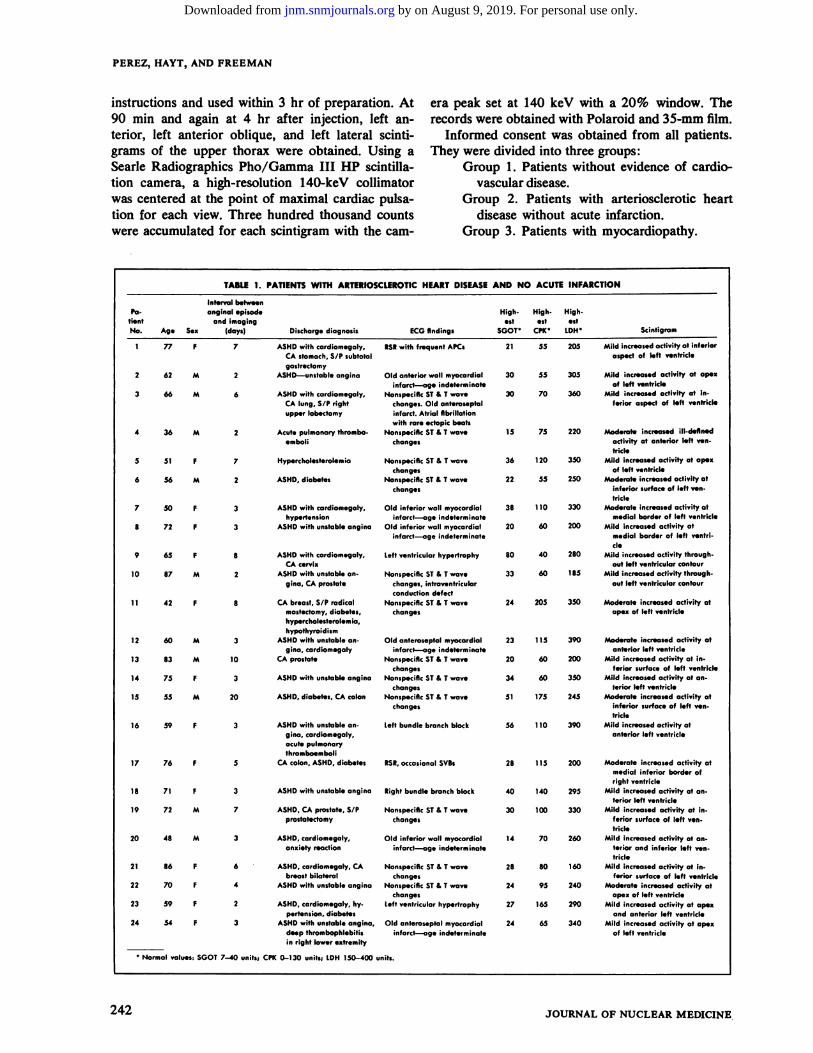
TABLE 1.PATIENTSWITh ARTERIOSCLEROTICHEARTDISEASEANDNOACUTEINFARCTIONPa
tlentNo.AgeSexInterval
betweenanginol episode
and imaging(days)Dischargediagnosis ECG findingsHigh
estSGOTHigh
utCPKHigh
estLDHScintigram177F7tSR
with frequent APCs2155205
PEREZ, HAYT, AND FREEMAN
instructions and used within 3 hr of preparation. At era peak set at 140 keV with a 20% window. The90 mm and again at 4 hr after injection, left an- records were obtained with Polaroid and 35-mm film.tenor, left anterior oblique, and left lateral scinti- Informed consent was obtained from all patients.grams of the upper thorax were obtained. Using a They were divided into three groups:Searle Radiographics Pho/Gamma III HP scintilla- Group 1. Patients without evidence of cardiotion camera, a high-resolution 140-keV collimator vascular disease.was centered at the point of maximal cardiac pulsa- Group 2. Patients with arteriosclerotic hearttion for each view. Three hundred thousand counts disease without acute infarction.were accumulated for each scintigram with the cam- Group 3. Patients with myocardiopathy.
Mild increased activity at inferioraspect of left ventricle
30 55 305 Mild increased activity at apexof left ventricle
30 70 360 Mild increased activity at inferior aspect of left ventricle
15 75 220 Moderate increased ill-definedactivity at anterior left yentricle
36 120 350 Mild increased activity at apexof left ventricle
22 55 250 Moderate increased activity atinferior surface of left ventricle
38 110 330 ModerateIncreasedactivityatmedial border of left ventricle
20 60 200 Mild increasedactivityatmedial border of left ventridc
80 40 280 Mild increased activity through.out left ventricular contour
33 60 185 Mildincreasedactivitythroughout left ventricular contour
24 205 350 Moderate increased activity atapex of left ventricle
23 1t5 390 Moderate increased activity atanterior left ventricle
20 60 200 Mild increased activity at inferior surface of left ventricle
34 60 350 Mildincreasedactivityat antenor left ventricle
51 175 245 Moderate increased activity atinferior surface of left yentricle
56 110 390 Mild increased activity atanterior left ventricle
28 115 200 Moderateincreasedactivityatmedial inferior border ofright ventricle
40 140 295 Mild increasedactivityat antenor left ventricle
30 100 330 Mildincreasedactivityat Inferior surface of left yen.tricle
14 70 260 Mild increased activity at antenor and inferior left ventide
28 80 160 Mild increased activity at Inferior surface of left ventricle
24 95 240 Moderateincreasedactivityatapex of left ventricle
27 165 290 Mild increased activity at apexand anterior left ventricle
24 65 340 Mild increased activity at apexof left ventricle
Old anterior wall myocardiolinfarct-—ag. indeterminate
Nonspecific ST & T wavechanges. Old anteroseptalinfarct. Atrial fibrillationwith rare ectopic beats
NonspecificST & T wavechanges
NonspecifIc ST & T wavechanges
Nonspecific ST& T wavechanges
Old inferior wall myocordialinfarct—ageindeterminate
Old inferior wall myocardial
infarct—age indeterminate
Left ventricular hypertrophy
Nonspecific ST & T wavechanges. intraventricularconduction defect
NonspecificST & I wavechanges
Old anteroseptal myocardial
infarct—ageindeterminateNonspecificST & T wave
changesNonspecific ST & T wave
changesNonspecificST & I wave
changes
Left bundle branch block
tSR, occasional SVBs
Right bundle branch block
Nonspecific ST & T wavechanges
Old inferior wall myocardialinfarct—age indeterminate
Nonspecific ST & T wavechanges
Nonspecific ST & T wavechanges
Left ventricular hypertrophy
Old anteroseptal myocardialinfarct—ageindeterminate
ASHD with cardiomegaly.
CAstomach,S/P subtotalgastredtomy
2 62 M 2 ASHD—unstableangina
3 66 M 6 ASHD with cardiomegaly.CAlung.S/P rightupper lobectomy
4 36 M 2 Acute pulmonary thromboemboli
S 51 F 7 Hypercholesterolemia
6 56 M 2 ASHD, diabetes
7 50 F 3 ASHD with cardiomegaly.hypertension
8 72 F 3 ASHDwithunstableangina
9 65 F 8 ASHD with cardiomegaly.CAcervix
10 87 M 2 ASHD with unstable angina, CA prostate
11 42 F 8 CAbreast,S/P radicalmastectomy.diabetes,hypercholesterolemia,hypothyroidism
12 60 M 3 ASHD with unstable angina, cardiomegaly
13 83 M 10 CA prostate
14 75 F 3 ASHD with unstable angina
15 55 M 20 ASHD. diabetes, CA colon
16 59 F 3 ASHD with unstable angina. cardiomegaly.acute pulmonarythromboemboli
17 76 F 5 CA colon, ASHD. diabetes
18 71 F 3 ASHD with unstable angina
19 72 M 7 ASHD. CA prostate. S/Pprostatectomy
20 48 M 3 ASHD, cardlamegaly,anxiety reaction
21 86 F 6 ASHD. cardiomegaly. CA
breast bilateral22 70 F 4 ASHD with unstable angina
23 59 F 2 ASHD, cardiomegaly. hy.pertension. diabetes
24 54 F 3 ASHD with unstable angina,deep thrombophlebitisin right lower extremity
. Normal valus: SOOT 7—40 units; CPK 0—130 units; LDH 150—400 units.
242 JOURNAL OF NUCLEAR MEDICINE
by on August 9, 2019. For personal use only. jnm.snmjournals.org Downloaded from

Pa High High.HightientestestestNo.
Age Sex Chestpain Condition ECGfindings SGOTCPKLDH Scintigram
1 50 M None 80 120 330
DIAGNOSTICNUCLEARMEDICINE
gina! episode who were not admitted for suspectedacute myocardial infarction. Acute infarction wasexcluded in Group 2 by serial ECGs, serum enzymestudies, and subsequent clinical course.
Group 3. Myocardiopathy. Six patients were studied: all were men, with an age range of 50—70years.A strong history of alcoholic intake was present infour cases. The diagnosis of myocardiopathy wasmade on clinical grounds.
RESULTS
Group 1. No patient had any history of significantcardiac disturbance and physical examination didnot disclose cardiac disease. Electrocardiogramswere all normal, and the highest SGOT, CPK, andLDH values were within normal limits. No myocardial activity was found in 19 of the 20 patientsstudied (Fig. 1) . The exception, a 31-year-oldwoman without confirmable cardiac disease, showedincreased tracer uptake at about the inferior andapical border of the left ventricle. It was not superimposed breast activity, which in this patient waslocalized anterior to the chest wall by a lateral scmtigram. The myocardial activity was confined to thethoracic cavity and did not move with the breast onthe lateral scintigrams. The patient has no knownprimary or metastatic malignant disease. We have
no explanation for this scintigraphic finding.Group 2 (Table 1). All 24 patients had confirma
tory history and physical findings for ASHD. Eachwas studied 2—20 days after an anginal episode. Allshowed ill-defined faint-to-moderate activity in theregion of the anterior or inferior aspect of the leftventricle (Fig. 2). Serial ECG and serum enzymes
-f
——,,@:1k.
FIG.2. Unstablearterioscleroticheartdisease(Group2).Notemoderate ill-defined nonfocal increased radioactivity in vicinity ofleft ventricle.
The Group I patients were studied as part of anexamination for routine bone imaging. They wereall informed that the images of the heart were beingobtained as part of a clinical investigation.
Group 1. No evidence of cardiovascular disease.Twenty patients were studied: 10 men and 10women. The age range was 18—69years. All hadhistory, physical examination, and electrocardiograms. Serum-enzyme determinations included glutamic-oxaloacetic transaminase (SGOT), lactic dehydrogenase (LDH), and creatine phosphokinase(CPK).
Group 2. Arteriosclerotic heart disease withoutacute infarcion. Twenty-four patients were studied:
10 men and 14 women. The age range was 36—87years. These patients all had angina and some hadprevious myocardial infarction as indicated by dcctrocardiograms. This group is actually composedof two subgroups. Approximately one-half were admitted with chest pain and the suspicion of acutemyocardial infarction, and the other half were patients with arteriosclerotic disease and a recent an
TABLE 2. PATiENTS WITH MYOCARDIOPATHY
AlcoholicmyocardiopathyLeft
ventricularhypertrophyFaint
increased activity throughout enlarged cardiac
silhouette252MNoneAlcoholic
myocardiopathyleftbundle
branchblock40140360Faintincreasedactivity through
out enlarged cardiacsilhouette359MNoneAlcoholic
myocardiopathyleftventricular
hypertrophy3524240Moderateincreased activity
throughout enlarged cardiacsilhouette470MNoneAlcoholic
myocardiopathyLeftventricular
hypertrophy6070300Faintincreased activity through
out enlarged cardiacsilhouette577MNoneIdiopathic
myocardiopathyAVblockand
incompleteright bundlebranch block5971270Marked
increased activitythroughout enlarged cardiac
silhouette655MNoneIdiopathic
myocardiopathyLeftventricular
hypertrophy70110300No increasedactivity
Volume 17, Number 4 243
by on August 9, 2019. For personal use only. jnm.snmjournals.org Downloaded from
Clinical diagnosis Distribution of activity Intensity of activity
Normal None None
PEREZ, HAYT, AND FREEMAN
excluded acute myocardial infarction. For those patients who previously had acute myocardial infarction, clinical history and electrocardiogram datingcould not pinpoint the time of the previous infarction. However, it seemed clear that an intervalgreater than 3 weeks had existed between the previous infarction and the subsequent imaging.
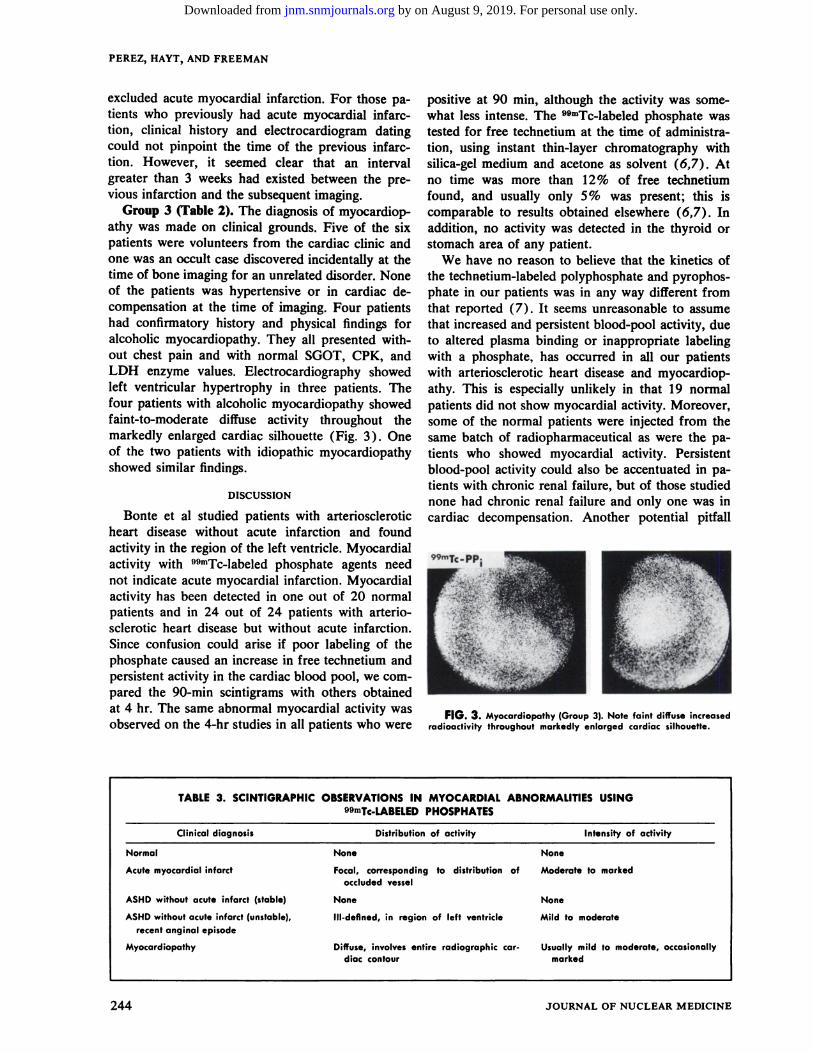
Group 3 (Table 2). The diagnosis of myocardiopathy was made on clinical grounds. Five of the sixpatients were volunteers from the cardiac clinic andone was an occult case discovered incidentally at thetime of bone imaging for an unrelated disorder. Noneof the patients was hypertensive or in cardiac decompensation at the time of imaging. Four patientshad confirmatory history and physical findings foralcoholic myocardiopathy. They all presented without chest pain and with normal SGOT, CPK, andLDH enzyme values. Electrocardiography showedleft ventricular hypertrophy in three patients. Thefour patients with alcoholic myocardiopathy showedfaint-to-moderate diffuse activity throughout themarkedly enlarged cardiac silhouette (Fig. 3) . Oneof the two patients with idiopathic myocardiopathyshowed similar findings.
DISCUSSION
Bonte et al studied patients with arterioscleroticheart disease without acute infarction and foundactivity in the region of the left ventricle. Myocardialactivity with 9OmTc.labeled phosphate agents neednot indicate acute myocardial infarction. Myocardialactivity has been detected in one out of 20 normalpatients and in 24 out of 24 patients with arteriosclerotic heart disease but without acute infarction.Since confusion could arise if poor labeling of thephosphate caused an increase in free technetium andpersistent activity in the cardiac blood pool, we cornpared the 90-mm scintigrams with others obtainedat 4 hr. The same abnormal myocardial activity wasobserved on the 4-hr studies in all patients who were
positive at 90 mm, although the activity was somewhat less intense. The O9mTc4abeled phosphate wastested for free technetium at the time of administration, using instant thin-layer chromatography withsilica-gel medium and acetone as solvent (6,7) . Atno time was more than 12% of free technetiumfound, and usually only 5% was present; this iscomparable to results obtained elsewhere (6,7) . Inaddition, no activity was detected in the thyroid orstomach area of any patient.
We have no reason to believe that the kinetics ofthe technetium-labeled polyphosphate and pyrophosphate in our patients was in any way different fromthat reported (7) . It seems unreasonable to assumethat increased and persistent blood-pool activity, dueto altered plasma binding or inappropriate labelingwith a phosphate, has occurred in all our patientswith arteriosclerotic heart disease and myocardiopathy. This is especially unlikely in that 19 normalpatients did not show myocardial activity. Moreover,some of the normal patients were injected from thesame batch of radiopharmaceutical as were the patients who showed myocardial activity. Persistentblood-pool activity could also be accentuated in patients with chronic renal failure, but of those studiednone had chronic renal failure and only one was incardiac decompensation. Another potential pitfall
FIG.3. Myocardiopathy(Group3).Notefaintdiffuseincreasedradioactivity throughout markedly enlarged cardiac silhouette.
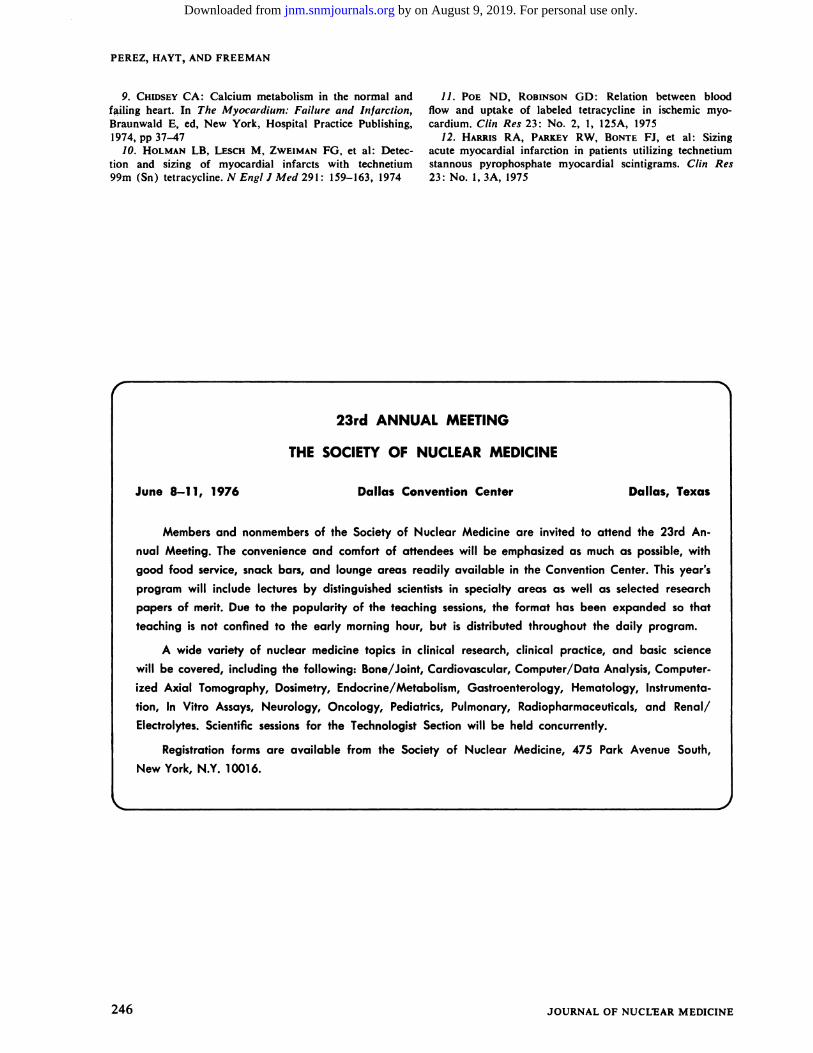
TABLE 3. SCINTIGRAPHIC OBSERVATIONS IN MYOCARDIAL ABNORMALITIES USING99mTc4@BELEDPHOSPHATES
Acute myocardial infarct Focal, corresponding to distribution ofoccluded vessel
Moderate to marked
ASHD without acute infarct (stable) None None
ASHD without acute infarct (unstable),
recent anginal episodeIll-defined, in region of left ventricle Mild to moderate
Myocardiopathy Diffuse, involves entire radiographic cardiac contour
Usually mild to moderate, occasionallymarked
244 JOURNAL OF NUCLEAR MEDICINE
by on August 9, 2019. For personal use only. jnm.snmjournals.org Downloaded from

DIAGNOSTIC NUCLEAR MEDICINE
lated by the difficulties in infarct diagnosis encountered by the standard methods. An extension of thisreasoning suggests the exciting possibility that theabnormal uptake in our patients with arterioscleroticheart disease might conceivably represent areas ofsubclinical infarction, not confirmable by standarddiagnostic tests. Further investigative work shouldhelp to confirm or refute this possibility. As withother radionuclide imaging studies, the specificity ofthe procedure is always enhanced by evaluating theresults in conjunction with other clinical considerations. In addition, careful assessment of the intensityand distribution of the abnormal activity should helpto differentiate the entities of acute infarction, arteriosclerotic heart disease without acute infarction,and myocardiopathy (Table 3, Fig. 4) . We emphasize the relatively unstable status of the Group 2patients. All had recent angina, but no evidence ofacute infarction was present.
Myocardial imaging with oomTc@labeledphosphateis a simple safe noninvasive technique which may beuseful to establish the presence or absence of myocardial infarction. Whether the localization of tracerdetectable by a camera indicates only frank infarctionor may also include areas of simple ischemia stillremains to be determined. This situation may besimilar to that of labeled tetracycline in ischemicmyocardium (1 1 ) . Attempts have been made to sizeacute myocardial infarction in patients using similar methods ( 12) . If it should turn out, however, thatthe scintigram also signals simple ischemia, the estimate of “infarctsize―may be too generous.
REFERENCES
1. BONTE FJ, PARKEY RW, GRAHAM KD, et al: A newmethod for radionuclide imaging of myocardial infarcts.Radiology 110: 473—474,1974
2. PARKEYRW, BONTEFJ, MEYERSL, et al: A newmethod for radionuclide imaging of acute myocardial in.farction in humans. Circulation 50: 540—546,1974
3. WILLERSON JT, PARKEY RW, BONTE FJ, et al: Acutesubendocardial myocardial infarction in patients. Circulation51: 436—441,1975
4. WILLERSONJT, PARKEYRW, BONTEFJ, Ct al: Technetium 99m stannous pyrophosphate myocardial imaging inthe diagnosis of acute myocardial infarction in patients.Circulation 49—50:Suppl No 3, 4, 1974
5. WILLERSONJT, PARKEYRW, BONTEFJ, et al : Technetium stannous pyrophosphate myocardial scintigrams inpatients with chest pain of varying etiology. Circulation 51:1046—1052,1975
6. BILLINGHURSTMW: Chromatographicquality controlof mmTc-Iabeled compounds. I Nucl Med 14: 793—797,1973
7. KRISHNAMURTHYGT, HUEBOrrERRJ, WALSHCF,et al: Kinetics of ‘@mTc-labeled pyrophosphate and poly
phosphate in man. I Nucl Med 16: 109—115, 1975
8. SERAFINIAN, RASKINMM, ZAND LC, et al: Radionuclide breast scanning in carcinoma of the breast. I NuclMed 14:1149—1152,1974
FIG.4. Bycomparisonofscintigraphicpatternsof myocardialactivity, various disease processes can generally be distinguished.
is breast localization of phosphate agents, describedby several investigators (8) . The lateral scintigramis particularly helpful in such situations.
Bonte et al postulated that myocardial infarctioninduces cellular influx of calcium ions with localization in the mitochondria near the hydroxyapatitecrystal (1 ) . Thus, in myocardial ischemia withoutinfarction, the phosphate tracer may be showing thisintracellular flux of calcium ions from the sarcoplasmic reticulum to the mitochondria (9) . Thesechanges may occur early in myocardial ischemia andhave been demonstrated before standard clinicalsigns of overt cardiac failure appeared (9) . Similarly, these intracellular changes associated with thepreclinical stages of cardiac failure may occur inarteriosclerotic heart disease without overt infarction. It is well known that the “diagnosisof acutemyocardial infarction depends on inferential clinicaland laboratory data, including the occurrence ofchest pain, sequential electrocardiographic changes,and altered pattern in serum enzyme activity―(10).Much of the enthusiasm for 99mTc@labeledphosphateor tetracycline in myocardial imaging has been stimu
Volume 17, Number 4 245
by on August 9, 2019. For personal use only. jnm.snmjournals.org Downloaded from
PEREZ, HAYT, AND FREEMAN
9. CHIDSEYCA : Calcium metabolismin the normal andf@i1ing heart. In The Myocardium: Failure and Infarction,Braunwald E, ed, New York, Hospital Practice Publishing,1974,pp 37—47
10. HOLMAN LB, LESCH M, ZWEIMAN FG, et al: Detection and sizing of myocardial infarcts with technetium99m (Sn) tetracycline. N Engi I Med 291 : 159—163,1974
11. POE ND, RoBINsoN GD: Relation between bloodflow and uptake of labeled tetracycline in ischemic myocardium. Clin Res 23: No. 2, 1, 125A, 1975
12. HARRIS RA, PARKEYRW, BONTE FJ, et al: Sizingacute myocardial infarction in patients utilizing technetiumstannous pyrophosphate myocardial scintigrams. Clin Res23: No. 1,3A, 1975
Dallas, TexasJune 8—11,1976
J
246 JOURNAL OF NUCLtAR MEDICINE
23rd ANNUAL MEETING
THE SOCIETY OF NUCLEAR MEDICINE
Dallas ConventionCenter
Members and nonmembers of the Society of Nuclear Medicine are invited to attend the 23rd An
nual Meeting. The convenience and comfort of attendees will be emphasized as much as possible, with
good food service,snackbars, and lounge areas readily available in the ConventionCenter.Thisyear'sprogram will include lectures by distinguished scientists in specialty areas as well as selected research
papers of merit. Due to the popularity of the teaching sessions,the format has been expanded so that
teaching is not confined to the early morning hour, but is distributed throughout the daily program.
A wide variety of nuclear medicine topics in clinical research, clinical practice, and basic science
will be covered,including the following: Bone/Joint,Cardiovascular,Computer/DataAnalysis,Computerized Axial Tomography, Dosimetry, Endocrine/Metabolism, Gastroenterology, Hematology, Instrumenta
tion, In Vitro Assays, Neurology, Oncology, Pediatrics, Pulmonary, Radiopharmaceuticals, and Renal!
Electrolytes. Scientific sessions for the Technologist Section will be held concurrently.
Registration forms are available from the Society of Nuclear Medicine, 475 Park Avenue South,
New York, N.Y. 10016.
by on August 9, 2019. For personal use only. jnm.snmjournals.org Downloaded from

1976;17:241-246.J Nucl Med. Louis A. Perez, David B. Hayt and Leonard M. Freeman Phosphate Agents
Tc-Labeled99mLocalization of Myocardial Disorders other than Infarction with
http://jnm.snmjournals.org/content/17/4/241This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1976 SNMMI; all rights reserved.
by on August 9, 2019. For personal use only. jnm.snmjournals.org Downloaded from