jcia clinical laboratory survey process guide 2nd edition-final
DESCRIPTION
medical documentTRANSCRIPT

i
TT AA BB LL EE OO FF CC OO NN TT EE NN TT SS
Contact Directory ...........................................................................................................................1
Introduction ....................................................................................................................................2
The Value of Joint Commission International Accreditation .................................................2
Joint Commission International—Who Are We?.....................................................................3
Who Is Eligible for an International Clinical Laboratory Accreditation Survey? ................5
How to Request an International Clinical Laboratory Accreditation Survey .......................5
Survey Scheduling, Postponements, and Cancellations ...........................................................6
The Standards Manual ...................................................................................................................7
International Patient Safety Goals for Clinical Laboratories ..........................................................9
Scoring Guidelines for Survey Consistency ............................................................................ 11
Accreditation Decision Rules – Effective 1 April 2010 ........................................................ 14
Accreditation Preparation .......................................................................................................... 17
Preparation Timeline .................................................................................................................... 18
Accreditation Process Timeline ..................................................................................................... 22
The On-Site Survey ................................................................................................................... 23
Sample Survey Agenda ............................................................................................................... 24
Tracer Methodology ................................................................................................................... 27
The Accreditation Decision ....................................................................................................... 30
Survey Agenda: Detailed Descriptions

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
Opening Conference ................................................................................................................. 32
Orientation to the Clinical Laboratory’s
Services and the Quality Improvement Process .................................................................... 34
Surveyor Planning Session ......................................................................................................... 36
Document Review ....................................................................................................................... 38
Documents Available in English .................................................................................................. 39
Evaluation of the Policies and Procedures by the Survey Team ...................................................... 41
Daily Briefing ............................................................................................................................... 43
Clinical Laboratory Environment Tour................................................................................... 45
Individual Patient Tracer Activity............................................................................................. 47
System Tracer: Infection Control ............................................................................................. 50
System Tracer: Quality Management and Improvement Process ....................................... 53
Visits to Laboratory Sections and/or
Off-Site Laboratories and Collection Stations ....................................................................... 56
Inpatient Unit/Setting Visits ..................................................................................................... 58
Undetermined Survey Activities ............................................................................................... 60
Education Session: Clinical Laboratory Decision Rules,
Scoring Guidelines, and Strategic Improvement Plan .......................................................... 61
Joint Commission International Accreditation Strategic Improvement Plan (SIP) Form ............... 62
Staff Qualifications and Education Session ............................................................................ 69
Competency Assessment Process Review Form .............................................................................. 71
Leadership Conference ............................................................................................................. 72

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
Surveyor Team Meeting ............................................................................................................. 74
Surveyor Report Preparation ..................................................................................................... 75
Leadership Exit Conference ...................................................................................................... 76
Survey Planning: Reference Lists
Required Quality Monitors ........................................................................................................ 79
Required Clinical Laboratory Plans .......................................................................................... 80
Required Policies and Procedures, Written Documents,
Clinical Laboratory Plans, and Bylaws ..................................................................................... 81
Standards that Reference Laws and Regulations and Standards of Practice ................... 106
Law and Regulation Worksheet ............................................................................................... .107
External Auditing Body Recommendation Worksheet ............................................................. .110

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
1
Contact Directory
Joint Commission International Accreditation Central Office
1515 West 22nd Street, Suite 1300W
Oak Brook, IL 60523 U.S.A
Phone: +1.630.268.4800
Fax: +1.630.268.2996
E-mail: [email protected]
Joint Commission International Joint Commission International Joint Commission International
European Office Middle East Office Asia Pacific Office
Dr. Carlo Ramponi, Managing Director Dr. Ashraf Ismail, Managing Director Dr. Paul Chang, Managing Director
13, Chemin du Levant P.O. Box 505018 37th Floor
Immeuble JB Say Dubai Healthcare City Singapore Land Tower
F-01210 Ferney-Voltaire Dubai, United Arab Emirates 50 Raffles Place
France Phone: +971. 4369.4930 Singapore 048623
Phone: +33.4.50.42.60.82 Fax: +971.4362.4951 Phone: +6. 6829.7208
Fax: +33.4.50.2.48.82 E-mail: [email protected] Fax: +65.6829.7070
E-mail: [email protected] E-mail: [email protected]
Contact Joint Commission International for any of the following:
To inquire about a completed application for survey, survey date, or schedule or for
assistance with specific problems or information related to accreditation
To register for or receive information about education programs and to purchase or to
inquire about publications
Joint Commission International Web Site: http://www.jointcommissioninternational.org
Visit the Web site to obtain any of the following:
General information about accreditation
Joint Commission International news
Information about accreditation status for specific clinical laboratories
Application for survey
Frequently asked questions (FAQs)
JCInsight, JCI’s newsletter

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
2
Revisions to standards
Standards
To submit a complaint about an accredited clinical laboratory
Joint Commission Resources Web Site: http://www.jcrinc.com
Visit the Web site to obtain any of the following:
Information about upcoming education programs
Catalog of publications
Access to official JCI publications and e-books
Video streaming presentations

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
3
Introduction
The Joint Commission International Accreditation Clinical Laboratory Survey Process Guide is designed to help
clinical laboratories learn about Joint Commission International (JCI) standards and the survey
process. This guide will provide clinical laboratories with important information about JCI, the
clinical laboratory standards manual, eligibility for accreditation, how to request accreditation, survey
preparation, the on-site survey, and the accreditation decision.
Clinical laboratories should not hesitate to contact any of the JCI Accreditation Offices by telephone
or e-mail using the contact directory above for any other information they may need.
The Value of Joint Commission International Accreditation
Accreditation may benefit clinical laboratories by accomplishing the following:
Giving clinical laboratories a competitive advantage
Accreditation provides evidence of high-quality patient care that helps level the playing field for
clinical laboratories performing the same types of procedures.
Strengthening community confidence
Achieving accreditation is a visible demonstration to patients and the community that a
clinical laboratory is committed to providing the highest-quality services.
Obtaining recognition from insurers, associations, employers, and other stakeholders
Increasingly, accreditation is becoming eligibility prerequisite for reimbursement, association
membership, community awareness, and contracts or grants.
Validating high-quality care to patients
JCI standards are focused on achieving one goal: raising the safety and quality of care to the
highest possible level. Achieving accreditation is a strong validation that a clinical laboratory has
taken the extra steps to meet a high level of safety and quality.
Helping clinical laboratories organize and strengthen their improvement efforts
Accreditation encompasses state-of-the-art performance improvement concepts that help clinical
laboratories continuously improve quality.
Enhancing staff education
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
4
The survey process is designed to be educational, not punitive. JCI surveyors are trained to help
clinical laboratories improve their internal procedures and day-to-day operations.
Improving risk management
By enhancing risk management efforts, accreditation may improve access to or reduce the cost
of liability coverage. It can also assist in lowering adverse events or outcomes for the clinical
laboratory, and, more importantly, for the patient.
Facilitating staff recruitment
As staff recruitment becomes more difficult, achieving accreditation as a demonstration of a
clinical laboratory’s commitment to quality and patient safety will enhance recruitment efforts
and retention of staff.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
5
Promoting team-building skills for staff
The process of obtaining and maintaining accreditation demands a team approach to good
patient care. Establishing processes and systems that support good patient care is achieved
through strong team activities.
Joint Commission International—Who Are We?
JCI is a division of Joint Commission Resources (JCR), the subsidiary of The Joint Commission. For
more than 75 years, The Joint Commission (U.S.A.) and its predecessor organization have been
dedicated to improving the quality and safety of health care services. Today, The Joint Commission
is the largest accreditor of health care organizations in the United States—it surveys nearly 18,000
health care programs through a voluntary accreditation process. The Joint Commission and JCI are
both nongovernmental, not-for-profit U.S. corporations.
The mission of The Joint Commission is to continuously improve health care for the public, in
collaboration with other stakeholders, by evaluating health care organizations and inspiring them to
excel in providing safe and effective care of the highest quality and value.
The Joint Commission was founded in 1951 under the auspices of the American Hospital
Association, the American Medical Association, the American College of Physicians, and the
American College of Surgeons, with the later addition of the American Dental Association, to act as
an independent accrediting body for organizations nationwide. As such, The Joint Commission
currently accredits nearly 80% of U.S. health care organizations. Because of the changing nature of
health care in America, beginning in 1975, The Joint Commission broadened its scope to include
accreditation of many non-hospital settings.
JCI extends The Joint Commission’s mission worldwide. Through international consultation,
accreditation, publications, and education, JCI helps to improve the quality of patient care in many
nations. JCI has extensive international experience working with public and private health care
organizations and local governments in more than 90 countries.
JCI established the Clinical Laboratory Accreditation Program to encourage quality testing in all
types of clinical laboratory facilities. Today’s health care environment is changing rapidly, and clinical
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
6
laboratory providers are experiencing new competitive pressures in the health care marketplace.
Providing safe, high-quality testing and continually improving clinical laboratory performance are
benchmarks of success. JCI clinical laboratory accreditation is a widely recognized standard for high-
quality services.
Why Choose Joint Commission International over Other Options?
JCI is the leader in international accreditation, with more than 10 years of experience across the full
spectrum of health care organizations. JCI accreditation represents the ―Gold Seal of Approval™‖ in
health care and provides the most comprehensive evaluation process.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
7
The Joint Commission International Patient-Centered Accreditation Process
Significant changes were made to the JCI accreditation process in 2006 to make the process
more focused on the patient’s care experience. To help clarify the changes to this process,
tracer methodology was introduced as a new term. The new patient-centered process also shifts
accreditation away from survey preparation to continuous standards compliance. The survey
becomes merely the on-site evaluation piece of a continuous quality improvement process. See page
27 for more information on tracer methodology.
Joint Commission International Standards Represent an International Consensus
In October 2009, a revised set of standards was published for implementation on 1 April 2010. The
standards in the second edition of the Joint Commission International Accreditation Standards for Clinical
Laboratories were created through the following processes:
JCI Standards Committee, Accreditation Committee, and Board of Directors
The standards undergo extensive field review prior to being published. An International Standards
Committee, composed of experts in the health care quality and patient safety fields, was established.
This committee provides advice and assistance in developing new and revised standards and
recommends improvements to the accreditation process. These changes are reviewed by the
Accreditation Committee and are approved by the Board of Directors. This committee also oversees
the revision of the standards and their introduction to the health care community.
Regional International Advisory Groups
Regional International Advisory Groups, representing ministries of health, professional health care
associations, and national accrediting organizations, meet on a regular basis to discuss ongoing issues
and potential future improvements to the JCI accreditation process.
Field Review Process
When periodic revisions or changes to the standards are made, health care organizations, whether
accredited or not, are given an opportunity to comment on those changes. Field review
announcements are posted on the JCI Web site and are sent to the JCI list serve to elicit
individual/organization comments. To join the JCI list serve, please contact the JCI Accreditation
Central Office or sign up on the JCI Web site. (See the Contact Directory on page 1).

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
8
Standards Interpretation
JCI will answer specific questions about JCI standards and how they are interpreted. This is a no-
cost service that can be accessed by telephone, by e-mail, or through the JCI Web site. Please direct
standards-related inquiries to Standards Interpretation at
http://www.jointcommissioninternational.org/interpretation-question/.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
9
Who Is Eligible for an International Clinical Laboratory
Accreditation Survey?
Any clinical laboratory may apply for JCI clinical laboratory accreditation if it meets the following
requirements:
The clinical laboratory is currently in operation as a health care provider in the country and
is licensed (if required).
The clinical laboratory assumes, or is willing to assume, responsibility for improving the
quality of its care and services.
The clinical laboratory provides services addressed by JCI standards.
How to Request an International Clinical Laboratory
Accreditation Survey
Clinical laboratories that wish to be accredited by JCI can obtain an application for survey by downloading the
application from the JCI Web site at http://www.jointcommissioninternational.org/Clinical-
laboratory/.
The application for survey should be submitted to JCI at least six months prior to the clinical
laboratory’s preferred on-site accreditation survey dates. Applications should be submitted, in
electronic format, by e-mail attachment to [email protected] or by fax to +1.630.268.2996.
The application for survey is valid for six months from the date it is submitted; this means a clinical
laboratory can submit its application and still have time to finish preparations before the on-site
survey takes place. It is best to submit the application when the clinical laboratory is confident it will
be able to demonstrate a four-month track record of compliance with the standards at the time of
the on-site survey (see ―Preparation Timeline‖ on page 18).
On the application for survey, clinical laboratories must indicate three months when they would like
the survey to take place and five additional weeks during the year when they would not like the
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
10
survey to take place. JCI will make every effort to accommodate these time requests. The earlier the
request is submitted, the more likely the specific requests can be accommodated.
After the application for survey is received, the manager for JCI Accreditation Services will contact
the clinical laboratory. The manager will do the following:
Answer the clinical laboratory’s questions about survey preparation and help guide
individuals through each step of the accreditation process
Analyze the application for survey and contact the clinical laboratory if there are any
questions or items requiring clarification
Update changes to the clinical laboratory’s demographic information, including the address,
contact name(s), and so forth
Assist in locating other resources or JCI contacts to answer questions
Schedule the on-site survey and assign the survey team and survey team leader
Forward the contract agreement for the on-site survey for a signature
JCI schedules on-site surveys based on information provided in the application for survey. Based on
this information, JCI determines the number of days required for a survey, the composition of the
survey team, and the services to be reviewed.
Four to six months before the survey, the accreditation survey contract agreement will be sent to the
clinical laboratory. Until the signed contract agreement and the down payment of at least 50% of the
survey fees are received, the scheduled survey cannot be confirmed. The clinical laboratory will also
receive notification of the surveyor’s(s’) name(s) before its survey. The survey team leader will
contact the person responsible for the clinical laboratory’s survey approximately four to eight weeks
before the survey to finalize the agenda and to coordinate the availability of certain staff for key
survey activities, as well as to provide information regarding the surveyor’s(s’) travel arrangements
and logistics.
Handling Changes During the Application Process
If a clinical laboratory undergoes a change that modifies the information reported in the application
for survey after it submits its application, the clinical laboratory must notify JCI immediately of the
change. Changes that must be reported to JCI include the following:
A change in clinical laboratory name, ownership, and/or leadership
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
11
A significant increase or decrease in the volume of services
The addition of a new type of health service
The deletion of an existing health service
A significantly altered building/physical plant
A required closure of a department or service by a regulatory or other legal authority
It may be necessary for JCI to schedule an additional survey for a later date if its survey team arrives
at the clinical laboratory and discovers that a change was not reported. JCI may also review any
unreported services addressed by its standards. In either case, additional fees may be assessed. JCI
will make the final accreditation decision for the clinical laboratory only after reviewing all services
provided by the clinical laboratory for which JCI has standards.
Survey Scheduling, Postponements, and Cancellations
Initial Schedules for Surveys
JCI schedules surveys systematically and efficiently to keep accreditation fees to a minimum.
Therefore, clinical laboratories are encouraged to accept scheduled survey dates. Initial surveys (a
clinical laboratory’s first full accreditation survey) should be scheduled within six months from the
time JCI receives the clinical laboratory’s application for survey.
JCI tries to honor specific requests for times during which a clinical laboratory prefers not to be
surveyed. The clinical laboratory should include these specific dates in the completed application for
survey, when possible. There may, however, be circumstances that prevent JCI from accommodating
these dates.
Definition of Postponement
JCI also allows the postponement of initial surveys or re-surveys. A postponement is a clinical
laboratory’s request to alter an already scheduled survey date or to push back the survey date before
it is actually scheduled. A clinical laboratory should direct a request for a postponement to the
manager for JCI Accreditation Services. A new survey application may be required when a new date
is established if the original application is older than six months.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
12
Acceptable Reasons for Postponement
A clinical laboratory may postpone scheduled surveys when one or more of the following events
occur:
A natural disaster or another major unforeseen event that totally or substantially
disrupts operations
A major strike that causes a clinical laboratory to cease performing tests
Patients and/or the clinical laboratory are being moved to another building during
the scheduled survey
JCI reserves the right to conduct an on-site survey if the clinical laboratory continues to perform
testing under such circumstances. Prior to postponing a scheduled survey, it is recommended that
clinical laboratories contact the manager for JCI Accreditation Services.
JCI understands that clinical laboratory operations may need to be modified to accommodate
construction and temporary disruptions in service. These situations are expected as part of managing
clinical laboratories and do not require postponement of a scheduled survey.
Cancellation
The survey may be canceled by JCI or the clinical laboratory without penalty or damages in the event
that acts of God, wars, terrorism, government regulations, disasters, strikes, civil disorders, or other
emergencies of a similar nature make it impossible, illegal, or unreasonable to go forward, provided
notice of the event requiring cancellation is communicated in writing as soon as practically possible.
Further, JCI may follow the advice of relevant ministries concerned with evaluating political and
military circumstances with regard to scheduling surveys.
If the clinical laboratory cancels the survey 60 days or less prior to the first day of the survey for any
reason(s) other than those previously stated, JCI Accreditation Services may require payment of one
half of the survey fees to recover costs JCI Accreditation Services has incurred.
The Standards Manual
The Joint Commission International Accreditation Standards for Clinical Laboratories, Second Edition is the
place to begin preparing for accreditation. The introduction to the manual contains the applicable

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
13
JCI accreditation policies and procedures (see pages 1–5). Clinical laboratories considering
accreditation can review these policies and procedures to better understand the expectations before
beginning the accreditation journey. Even if clinical laboratories do not pursue accreditation
immediately, the manual is an excellent tool to help them evaluate current practices and structures.
The manual is designed to be used in self-assessment activities and forms the basis for an
accreditation survey. The manual contains functional standards that are organized around
management and leadership, resource management, management of the environment, and quality
control processes. The standards address clinical laboratory functions and processes, including
organization, management, and development and control of policies and procedures.
The JCI publication Joint Commission International Accreditation: Getting Started, Second Edition, provides
detailed information to assist clinical laboratories plan the approach, structure, and process for
beginning the accreditation journey.
Standards Chapters Several changes were made to the clinical laboratory standards chapters from the first to the second editions. The original five chapters were reduced to four, and the International Patient Safety Goals were added. Although the requirements of the standards have not changed significantly, the new revision has reduced repetition of requirements in more than one chapter and makes it easier to find the requirements. The chapters are as follows: International Patient Safety Goals (IPSG)
The purpose of the International Patient Safety Goals (IPSG) is to promote specific improvements
in patient safety. The goals highlight problematic areas in health care and describe evidence- and
expert-based consensus solutions to problems related to patient safety. Recognizing that sound
system design is intrinsic to the delivery of safe, high-quality health care, the goals generally focus on
systemwide solutions whenever possible. A summary of the IPSGs for clinical laboratories is
provided on page 9.
Effective in 2010, the IPSGs were introduced into the laboratory standards and accreditation process. Surveyors will evaluate compliance with these goals during 2010 surveys, but the findings will not affect the accreditation decision. Effective 1 January 2011, laboratories are required to demonstrate compliance with the IPSGs to achieve and maintain accreditation.
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
14
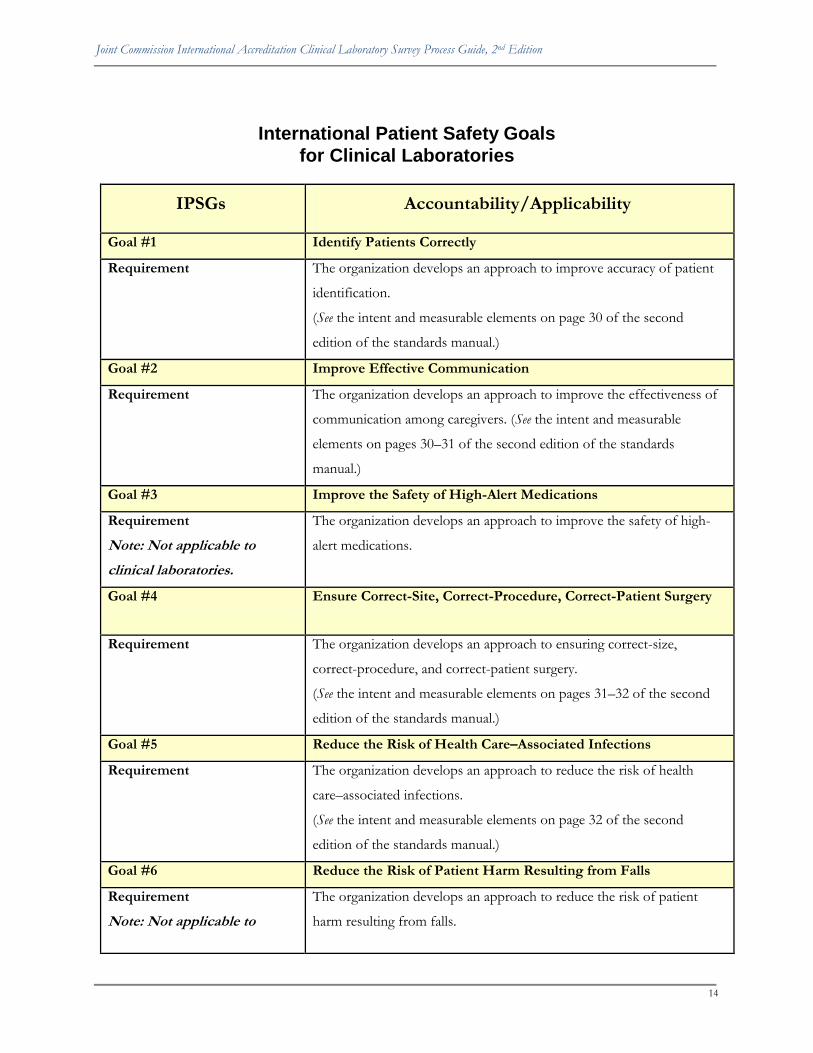
International Patient Safety Goals
for Clinical Laboratories
IPSGs Accountability/Applicability
Goal #1 Identify Patients Correctly
Requirement The organization develops an approach to improve accuracy of patient
identification.
(See the intent and measurable elements on page 30 of the second
edition of the standards manual.)
Goal #2 Improve Effective Communication
Requirement The organization develops an approach to improve the effectiveness of
communication among caregivers. (See the intent and measurable
elements on pages 30–31 of the second edition of the standards
manual.)
Goal #3 Improve the Safety of High-Alert Medications
Requirement
Note: Not applicable to
clinical laboratories.
The organization develops an approach to improve the safety of high-
alert medications.
Goal #4 Ensure Correct-Site, Correct-Procedure, Correct-Patient Surgery
Requirement The organization develops an approach to ensuring correct-size,
correct-procedure, and correct-patient surgery.
(See the intent and measurable elements on pages 31–32 of the second
edition of the standards manual.)
Goal #5 Reduce the Risk of Health Care–Associated Infections
Requirement The organization develops an approach to reduce the risk of health
care–associated infections.
(See the intent and measurable elements on page 32 of the second
edition of the standards manual.)
Goal #6 Reduce the Risk of Patient Harm Resulting from Falls
Requirement
Note: Not applicable to
The organization develops an approach to reduce the risk of patient
harm resulting from falls.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
15
clinical laboratories
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
16
Management and Leadership (MGT)
These standards address the requirements for leadership planning and oversight of the functions of
the clinical laboratory. Effective leadership depends on successfully performing the following
processes:
Planning and designing services—defining a clear mission, including a vision of the future
and the values which underlie day-to-day activities
Directing services—developing and maintaining policies, providing an adequate number of
staff, and determining their qualifications and competence
Integrating and coordinating services to meet the needs of the laboratory’s clients.
Improving performance—including leaders’ critical roles in initiating performance and
maintaining a clinical laboratory’s performance improvement activities
Development and Control of Policies and Procedures (DCP) This chapter delineates the requirements for policies and procedures, including the following:
General requirements
Procedures to order laboratory tests
Step-by step instructions for collecting and handling specimens
Step-by-step instructions for performing tests and other procedures
Reporting of results
Record and specimen retention Resource Management and Laboratory Environment (RSM)
These standards address the requirements for providing and managing the resources necessary for proper functioning of the clinical laboratory. The standards specifically address the following:
Human resources, including providing leaders and personnel with the necessary qualifications for the testing provided by the clinical laboratory
Infrastructure, including provision of necessary space, utilities, and equipment
Providing processes and equipment to assure a safe and secure environment Quality Control Processes (QCP) This chapter has the most standards and addresses the following:
General quality control requirements for all areas of the clinical laboratory
Specific quality control requirements for each laboratory specialty

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
17
SCORING GUIDELINES FOR SURVEY CONSISTENCY
PURPOSE OF THIS DOCUMENT
Each measurable element (ME) of a standard is scored either ―fully met,‖ ―partially met,‖ ―not met,‖
or ―not applicable.‖ The purpose of this document is to bring consistency to the assignment of these
scores, recognizing that many types of evidence will be examined prior to the survey team arriving at
a final score for each ME.
DETERMING THE APPROPRIATE SCORE
1. “Fully Met” Score
A. An ME is scored ―fully met‖ if the answer is ―yes‖ or ―always‖ to the specific
requirements of the ME. Also considered are the following:
i. A single negative observation may not prevent a score of ―fully met.‖ (Also
see ―Consideration of Impact and Criticality‖ on page 13.)
ii. If 90% or more of observations or records (for example, 9 out of 10) are
met
B. The track record related to a score of ―fully met‖ is as follows:
i. A 12-month look-back period of compliance for triennial surveys
ii. A 4-month look-back period of compliance for initial surveys
2. “Partially Met” Score
A. An ME is scored ―partially met‖ if the answer is ―usually‖ or ―sometimes‖ to the
specific requirements of the ME. Also considered are the following:
i. If 50% to 89% (for example, 5 through 8 out of 10) records or
observations demonstrate compliance
ii. Evidence of compliance cannot be found in all areas/departments in which
the requirement is applicable When there are multiple requirements in one
ME, at least half (50%) are present.
iii. A policy/process is developed, implemented, and sustainable but does not
have the track record required for ―fully met.‖

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
18
iv. A policy/process is developed and implemented but does not seem to be
sustainable.
B. The track record related to a score of ―partially met‖ is as follows:
The requirements of the ME are ―fully met‖; however, there is only
i. a 5- to 11-month look-back period of compliance for triennial surveys; or
ii. a 1- to 3-month look-back period of compliance for initial surveys.
3. “Not Met” Score
A. An ME is scored ―not met‖ if the answer is ―rarely‖ or ―never‖ to the specific
requirements of the ME. Also considered are the following:
i. If 49% or fewer (for example, 4 or less out of 10) records or observations
demonstrate compliance
ii. There was a finding of ―not met‖ for the ME during the last full survey and
now the finding is 67% or fewer observations of compliance.
iii. When there are multiple requirements in one ME, 49% or fewer are
present.
iv. A policy/process is developed but is not implemented.
B. The track record related to a score of ―not met‖ is as follows:
The requirements of the ME are ―fully met‖; however, there is only
i. a less than 5-month look-back period of compliance for triennial surveys;
or
ii. a less than 1-month look-back period of compliance for initial surveys.
C. If an ME of a standard was scored ―not met‖ and some or all of the other MEs are
dependent on the one scored ―not met,‖ then the remaining MEs that are tied to
the prior ME are scored as ―not met.‖ See the figure below for RSM.5 as an
example:
RSM.5 There is a plan to ensure that laboratory services and

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
19
facilities are secure.
❒ 1. A written plan that describes security measures for laboratory
services and facilities is implemented.
Not
Met
❒ 2. The plan addresses security issues for people, property, and
equipment, as required in elements c) and d) in the intent.
Not
Met
❒ 3. The plan provides safeguards for specimens, resources, and
laboratory spaces against unauthorized access.
Not
Met
4. “Not Applicable” Score
An ME is scored ―not applicable‖ if the requirements of the ME do not apply based on the
clinical laboratory’s services, patient population, and so forth (for example, the clinical laboratory
does not have blood donor services).

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
20
OTHER CONSIDERATIONS
1. The Look-Back Period for New Standards
The effective date of new standards is published with the standards. Clinical laboratories are
expected to be in compliance with the standards on the published effective date. The look-back
period for new standards can go back only to the effective date of the standard. Thus, for a new
standard effective 1 January, the look-back period on a 1 April triennial survey is 3 months back to
the 1 January effective date, not the 12 months for existing standards. Similarly, for a 1 April initial
survey, the look-back period is 3 months rather than 4 months.
If a clinical laboratory does not meet the shorter look-back period for a new standard, the score on
the ME will be influenced in the same manner in which a full 12-month (triennial) or 4-month
(initial) look-back period would be influenced. For example, if on a triennial survey, the possible
look-back period for a new standard is 6 months, and the clinical laboratory is in full compliance
(―fully met‖) with the ME, but the clinical laboratory can demonstrate compliance going back only
4 months, the ME will be scored ―partially met,‖ as 67% of the required look-back period was met.
The ME would be scored ―not met‖ if compliance could be demonstrated for only 2 months, or
33% of the possible look-back period.
2. The Look-Back Period on Follow-Up Focused Surveys
If, following a full survey—initial or triennial—a follow-up focused survey is required within 90
days per the accreditation decision rules, the look-back period at the time of the follow-up focused
survey is from the date of the follow-up focused survey, not from the date of the full survey. This
will permit clinical laboratories with good compliance for an ME on full survey, but inadequate
look-back periods, to obtain 3 months of additional look-back and thus possibly obtain full credit
for compliance with the ME.
3. Consideration of Impact and Criticality
Scores may be influenced by other factors, such as the impact or criticality of noncompliance for a
standard or an ME. Impact refers to the effect or outcome of the finding. Criticality refers to the
level or measure of importance of the finding. It is important to note that impact and criticality
determinations are not rule based, nor are they individual based; rather, they are determinations

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
21
made by the entire survey team, usually at the time each surveyor’s findings are integrated to
determine the final score of an ME.
Impact and criticality influence scoring in the following two ways:
1. The impact of a particular compliance percentage or the actual number of noncompliant
observations is an important consideration. For example, 1 sharps container that is full and
unavailable for use out of 6 sharps containers has a more limited impact than when all 6
sharps containers are full and unavailable for use. The criticality of the finding, rather than the
actual number of noncompliant observations, is also important. For example, failing to
provide, inspect, and identify the use of 1fire extinguisher out of 12 is a critical finding if this
fire extinguisher is the incorrect type or the only one available for a particular area of the
laboratory.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
22
Accreditation Decision Rules (Effective 1 April 2010)
I. ACCREDITATION DECISIONS
INTRODUCTION
The Accreditation Committee considers all information from the initial or triennial full survey and
any required follow-up focused survey in making its decision regarding accreditation. The outcome
is that the clinical laboratory meets the criteria for accreditation or does not meet the criteria and is
denied accreditation. The criteria for these two potential outcomes are as follows:
A. ACCREDITED
This decision results when a clinical laboratory meets all the following conditions.
1. The clinical laboratory demonstrates acceptable compliance at the measurable element
level.
Acceptable compliance is:
No more than one measurable element is scored a ―0‖ for any standard.
No more than one measurable element is scored a ―0‖ for any International Patient
Safety Goal.
2. The clinical laboratory demonstrates acceptable compliance with each standard.
Acceptable compliance is:
A score of at least ―5‖ on each standard.
3. The clinical laboratory demonstrates acceptable compliance with each International
Patient Safety Goal.
Acceptable compliance is:
A score of at least ―5‖ on each International Patient Safety Goal.
4. The clinical laboratory demonstrates overall acceptable compliance.
Acceptable compliance is:
An aggregate score of at least ―9‖ on all standards.
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
23
B. ACCREDITATION DENIED
This decision results when a clinical laboratory meets one or more of the following conditions
at the end of any required focus survey subsequent to an initial or triennial full survey, or during
the period of accreditation as a result of a focus survey for the evaluation of one or more policy
related conditions that may place the clinical laboratory At Risk for Denial of Accreditation.*
1. Two or more measurable elements in a standard or International Patient Safety Goal are
scored a ―0‖.
2. One or more standard is scored less than a ―5‖.
3. One or more International Patient Safety Goal is scored less than a ―5‖.
4. The aggregate score for all standards is less than ―9‖.
5. A required Focused Survey subsequent to an initial or triennial full survey has not resulted
in acceptable compliance with applicable standards. .
6. One or more of the conditions that place the clinical laboratory At Risk for Denial of
Accreditation* have not been resolved at the time of the focused survey to evaluate the
condition.
7. The clinical laboratory voluntarily withdraws from the accreditation process.
8. The clinical laboratory does not permit the performance of any survey by Joint Commission
International
* Conditions that place a clinical laboratory At Risk for Denial of Accreditation
1. An immediate threat to patient/public health or staff safety exists within the clinical laboratory.
2. An individual who does not possess a license, registration, or certification is providing or has provided health care
services in the organization that would, under applicable law or regulation, require such a license, registration, or
certification and which placed the organization’s patients at risk for a serious adverse outcome.
3. Joint Commission International is reasonably persuaded that the clinical laboratory submitted falsified documents
or misrepresented information in seeking to achieve or retain accreditation, as required by the Information
Accuracy and Truthfulness Policy.
4. The clinical laboratory does not possess a license, certificate, and/or permit, as, or when, required by applicable law
and regulation, to provide the health care services for which the clinical laboratory is seeking accreditation.
5. The clinical laboratory has not met the accreditation policy for ―Reporting Requirements between Surveys‖.
6. The clinical laboratory fails to submit an acceptable Strategic Improvement Plan (SIP) within 120 days of the
clinical laboratory’s survey.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
24
II. ASSIGNMENT OF FOLLOW-UP REQUIREMENTS AS A RESULT OF A FULL
SURVEY
INTRODUCTION
Full surveys are conducted at the time of initial accreditation and at the time of
reaccreditation, every three years. At the conclusion of the survey, the findings are evaluated
against the required conditions for accreditation. When the survey results meet all the
conditions for accreditation, the clinical laboratory receives an Accredited status. The clinical
laboratory will then be requested to develop a Strategic Improvement Plan (SIP) that defines
the improvement strategy(ies) and/or approach to bring any noncompliant standards
and/or International Patient Safety Goals into acceptable compliance. However, when the
results of a full survey do not meet one or more of the conditions for accreditation, the
clinical laboratory will have a period of time to come into acceptable compliance. Acceptable
compliance can then be demonstrated by a visit from one or more surveyors to the clinical
laboratory. The visit is named a follow-up focused survey, as only the standards and/or
International Patient Safety Goals in noncompliance are the ―focus‖ of the survey.
A. PROCESS
An Official Survey Findings Report is sent to the clinical laboratory by the Accreditation
Office within 10 to 15 days following the survey. An SIP will be requested for any ―not
met‖ standard(s)/measurable element(s) and/or International Patient Safety Goal(s) cited
in the survey report when the clinical laboratory meets the conditions for accreditation.
The SIP explains the clinical laboratory’s process in defining the improvement strategy(s)
and/or approach, including specific actions to bring the cited findings into acceptable
compliance. The plan also identifies the methodology to prevent reoccurrence and
sustain improvements over time. The SIP is due to the Accreditation Office for review
and acceptance within 45 days after receiving the final report.
B. A Preliminary Survey Findings Report is sent to the clinical laboratory by the
Accreditation Office when the documented findings of the accreditation survey team do
not meet one or more of the conditions for accreditation. The preliminary report is sent
to the clinical laboratory within 10 to 15 days after the survey; the report includes all
standard(s)/measurable element(s) and/or International Patient Safety Goal(s) that were

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
25
found to be not compliant at the time of the survey. Each of the noncompliant (―partially
met‖ and/or ―not met‖) findings will be reviewed for compliance by the surveyors
during the follow-up focused survey.
C. FOLLOW-UP FOCUSED SURVEY
A follow-up focused survey is required within 90 days from the date when the clinical
laboratory received the Preliminary Survey Findings Report. During the on-site visit, the
surveyor(s) will determine the clinical laboratory’s compliance with the standards and
International Patient Safety Goals through various survey activities and methods, such as
direct observation, staff or patient interviews, review of documents, review of medical
records and/or personnel files, or the inspection of the physical facility.
When the results of the follow-up focused survey meet all the conditions for
accreditation, the clinical laboratory receives an Accredited status. The clinical laboratory
will then be requested to develop an SIP.
When the results of the follow-up focused survey do not meet one or more of the
conditions for accreditation, the clinical laboratory will receive a Denied Accreditation
status by the Accreditation Committee.
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
26
Accreditation Preparation
After JCI accepts the clinical laboratory’s application for survey, both parties make preparations for
the on-site survey. To help clinical laboratories prepare for accreditation, JCI offers seminars,
custom education, numerous publications (such as Joint Commission International Accreditation: Getting
Started, Second Edition), online education and training (such as webinars or live video streaming), a
new electronic self-assessment tool, and this Clinical Laboratory Survey Process Guide. These resources
provide specific information on JCI standards and teach concepts related to performing tests in
clinical laboratories. Go to the JCI Web site at
http://www.jointcommissioninternational.org/Products-and-Services/ for up-to-date information
on available educational resources.
JCI organizes a team of surveyors to match the clinical laboratory’s needs and unique characteristics.
JCI will make every effort to provide a surveyor(s) who is fluent in the language(s) used at the clinical
laboratory. If a JCI surveyor(s) with the appropriate language capabilities is not available, it is the
clinical laboratory’s responsibility to provide interpreter services throughout the survey. The
interpreter(s) must be fluent in English and the language(s) used at the clinical laboratory, be
experienced in verbal and written translation, be able to follow recognized Medical Interpreting
Standards of Practice, and abide by the confidentiality policies and regulations set up by the clinical
laboratory.
On-site clinical laboratory accreditation surveys are typically conducted one or two surveyors,
depending on the size and complexity of the clinical laboratory. The survey follows laboratory testing
throughout the facility and includes interviews with key personnel, observation of the clinical
laboratory’s administrative and testing activities, assessment of the physical facilities and laboratory
equipment, and review of documentation. A sample survey agenda appears on pages 24–26. The
actual agenda will be customized by the survey team to fit the needs and services of the clinical
laboratory. The survey activities may vary depending on whether the clinical laboratory is an
inpatient or outpatient laboratory.
The survey team leader will contact the clinical laboratory approximately four to eight weeks prior to
the survey to discuss and coordinate a workable and mutually agreeable agenda. The survey team
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
27
leader identifies those services/areas that need to be included in the review and suggests staff who
should be involved in each survey activity.
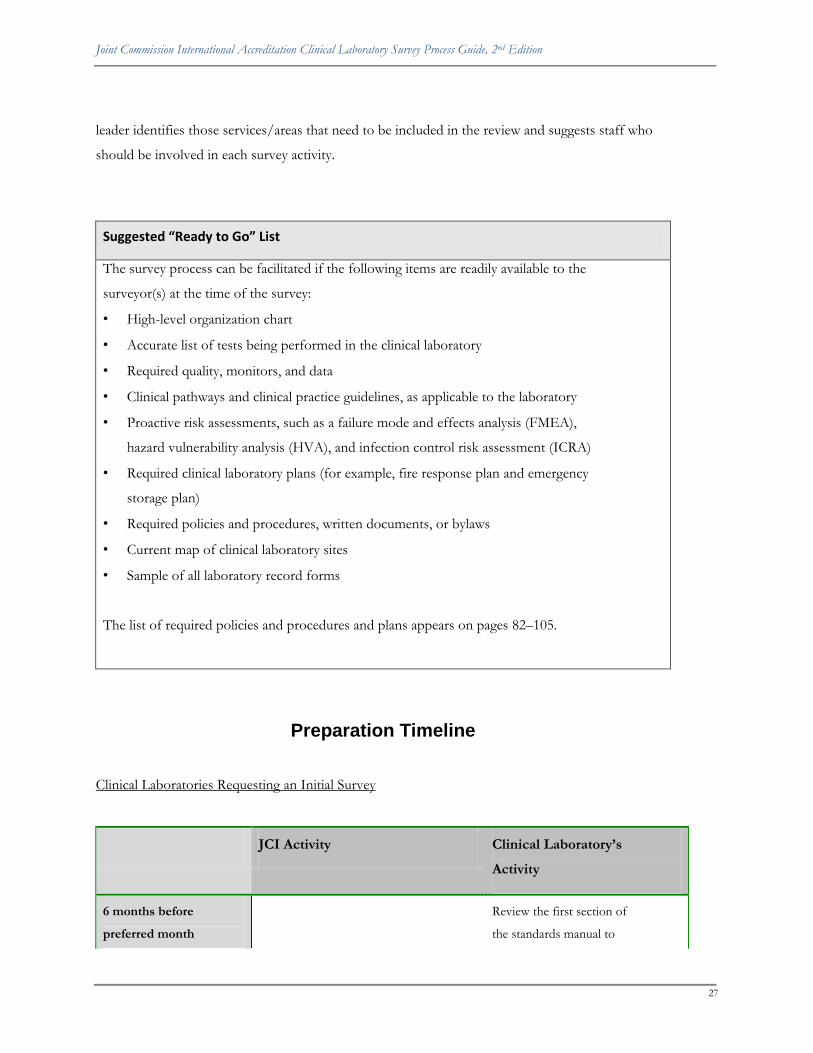
Suggested “Ready to Go” List
The survey process can be facilitated if the following items are readily available to the
surveyor(s) at the time of the survey:
• High-level organization chart
• Accurate list of tests being performed in the clinical laboratory
• Required quality, monitors, and data
• Clinical pathways and clinical practice guidelines, as applicable to the laboratory
• Proactive risk assessments, such as a failure mode and effects analysis (FMEA),
hazard vulnerability analysis (HVA), and infection control risk assessment (ICRA)
• Required clinical laboratory plans (for example, fire response plan and emergency
storage plan)
• Required policies and procedures, written documents, or bylaws
• Current map of clinical laboratory sites
• Sample of all laboratory record forms
The list of required policies and procedures and plans appears on pages 82–105.
Preparation Timeline
Clinical Laboratories Requesting an Initial Survey
JCI Activity Clinical Laboratory’s
Activity
6 months before
preferred month
Review the first section of
the standards manual to

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
28
of survey better understand the
expectations related to JCI
accreditation policies and
procedures.
Submit the application for
survey to the JCI
Accreditation Central
Office (electronically or by
fax).
Upon receipt of
the application
for survey
JCI manager for Accreditation
Services will review the
application.
The clinical laboratory will be e-
mailed a complimentary copy of
this Clinical Laboratory Survey
Process Guide.
Clinical Laboratories Requesting Reaccreditation
JCI Activity Clinical Laboratory’s
Activity
6 to 9 months
before the due
date of the next
triennial survey
An application for survey is e-
mailed to prepare for the next
on-site survey.
Complete
application at
least 4 to 6
months before
the accreditation
expires
Staff member(s) with
knowledge of the clinical
laboratory’s services, sites,
and testing volume will
need to complete and
submit the application for

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
29
survey (electronically or by
fax). The application
should be received by JCI
no later than 4 to 6 months
before the preferred survey
dates.
All Clinical Laboratories Requesting Accreditation
JCI Activity Clinical Laboratory’s
Activity
4 to 5 months
before survey
A contract agreement is e-mailed to
the clinical laboratory.
An invoice for down payment of at
least 50% of the survey fees is e-
mailed by the Finance Department
when the signed contract is
received. The clinical laboratory
can elect to pay 100% based on the
preference of the clinical laboratory
E-mail or fax the signed
contract to JCI no later
than 90 days prior to the
survey date. Notify
accounts payable staff to
expect an invoice and to
remit payment with a wire-
transfer form (found in the
application) no later than
60 days prior to survey
date.
8 weeks
before survey
Verification of survey date(s) and
name of surveyor(s) are e-mailed to
the clinical laboratory.
4 to 8 weeks
before survey
The survey team leader contacts
the clinical laboratory’s contact
person to finalize the survey
agenda and to request presurvey
information.
Appropriate staff
member(s) will need to
discuss the proposed
survey agenda and
determine whether times
are feasible for the clinical
laboratory given patient

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
30
JCI Activity Clinical Laboratory’s
Activity
needs and availability of
staff.
Clinical laboratories must
follow the guidelines in
requesting observers
during a survey (refer to
the survey agreement and
policies in the manual).
Survey Surveyor(s) arrives for the on-site
survey. At the conclusion of the
survey, the clinical laboratory
receives a copy of the Exit Report,
which details partial or
noncompliant areas that need to be
addressed. This report is not final
until the JCI Accreditation Central
Office has reviewed the report.
As outlined on the survey
agenda, staff should be
available during the survey.
An approved observer may
not answer questions or
contribute to discussions
unless requested by the
surveyor(s).
Within 15
days after
survey
JCI reviews, approves, and sends
the Official Survey Findings
Report. A follow-up focused
survey may be required prior to an
accreditation decision
determination. If the accreditation
is granted, the award letter, report,
and accreditation certificate are
mailed after all the survey fees have
been paid. The Gold Seal
guidelines and publicity kit will also
be posted to the Accredited
Clinical Laboratory Resource
Center on the JCI Web site at
http://www.jointcommissionintern
After the JCI Accreditation
Central Office sends the
Official Survey Findings
Report, the clinical
laboratory should begin
either of the two follow-up
processes as requested:
Develop the SIP if
accredited.
Prepare for the follow-
up focused survey if the
conditions for
accreditation were not

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
31
JCI Activity Clinical Laboratory’s
Activity
ational.org/accredited.
The chief executive officer (CEO)
of the surveyed clinical laboratory
will be sent a JCI Accreditation
Satisfaction Survey to assist JCI in
performance improvement
activities.
met.
The CEO of the surveyed
clinical laboratory should
encourage members of the
leadership team to provide
input for the JCI
Accreditation Satisfaction
Survey.
Within 3 days
after the
certificate is
mailed
The clinical laboratory’s name,
location, and date of accreditation
are added or updated for public
viewing on the JCI Web site at
http://www.jointcommissionintern
ational.org.
The clinical laboratory may
request JCI Accreditation
Services to place a link on
the JCI Web site to the
accredited clinical
laboratory’s Web site.
Ongoing Each accredited clinical laboratory
will have access to the Accredited
Clinical Laboratory Resource
Center via the JCI Web site, which
contains the JCI newsletter
(JCInsight), as well as many other
resources, publications, and
services that will assist in achieving
continuous compliance with the
standards.
Staff should review all
changes featured in the
newsletter to keep abreast
of official changes and
developments in the
standards and survey
process. Compliance is
required with new
standards and survey
processes for accredited
clinical laboratories.
Periodic submission of
evidence of compliance is
required as part of the
accreditation process; for
example, IPSG monitoring
data, SIP compliance data,

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
32
JCI Activity Clinical Laboratory’s
Activity
and self-assessments of
standards compliance.
6 months after
publication of
a new JCI
Clinical
Laboratory
standards
edition
JCI publishes a new edition of the
clinical laboratory standards
approximately every 3 years. The
manual becomes effective for all
accredited clinical laboratories and
all surveys 6 months after
publication.
Staff should review the
new accreditation manual
or supplement to
implement and act on any
new and modified
standards, scoring
guidelines, policies, and
procedures. If JCI needs to
visit the clinical laboratory,
the current, effective
standards will be used.
Within 30 days of
any significant
organizational
changes
The clinical laboratory
must notify JCI (via letter,
fax, or e-mail) of any
significant change in the
clinical laboratory (as
defined in the ―Joint
Commission International
Accreditation Policies and
Procedures‖ chapter of the
standards manual).
6 to 9 months
before the due
date of the
next triennial
survey
An application for survey is mailed
to the clinical laboratory to prepare
for the next on-site survey.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, Second Edition
33
Accreditation Process Timeline
12 to 24
Months Prior
to Survey
6 to 9
Months
Prior to
Survey
4 to 6
Months
Prior to
Survey
4 to 8 Weeks
Prior to
Survey
Survey
Dates
Within 15
Days After
Survey
6 to 9 Months
Prior to Triennial
Due Date
Obtain JCI standards
manual and begin
preparing for JCI
accreditation.
Submit
application for
survey to JCI, and
schedule survey
dates with JCI.
JCI survey team
leader contacts the
clinical laboratory
to determine
survey agenda and
logistics.
Receive accreditation
decision and Official
Survey Findings Report
from JCI.
Receive and complete
JCI survey contract and
invoices for survey fees.
JCI
accreditation
survey occurs.
Submit revised
application and
schedule triennial
JCI accreditation re-
survey.
Continuous
Quality
Improvement
Journey
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
34

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, Second Edition
35
The On-Site Survey
The purpose of a JCI accreditation survey is to assess the extent of a clinical laboratory’s compliance
with applicable JCI standards. Clinical laboratories undergoing their first survey need to demonstrate a
track record of 4 months of compliance with the standards. Clinical laboratories being re-surveyed
need to demonstrate 12 months of compliance with the standards. Understanding the clinical
laboratory and assessing compliance is accomplished through a number of methods, including the
following:
Receipt of verbal information concerning implementation of standards or examples of their
implementation
On-site observation by a JCI surveyor(s)
Review of documents that demonstrate compliance and assistance in orienting the
surveyor(s) to the clinical laboratory’s operations
The on-site survey uses tracer methodology to follow a sample of clinical tests and potentially active
patients, if appropriate, through the laboratory processes, and if appropriate, patients, through their
experiences of care in the clinical laboratory to evaluate individual components and systems of care.
An important characteristic of the JCI survey process is on-site education conducted by the
surveyor(s). This support occurs throughout the survey as the surveyor(s) offers suggestions and
strategies that may help the clinical laboratory better meet the intent of the standards and, more
importantly, improve performance.
The on-site review consists of the following steps:
1. Opening conference and orientation to the organization
2. Survey planning meeting
3. Document review
4. Individual patient tracer activities
5. Quality control process review
6. Visits to clinical laboratory areas
7. Visits to collection stations
8. Visits to off-site laboratory services
9. Competence assessment and credentials evaluation

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
36
10. Resource management, including tours of the building, facility space, and equipment
11. Leadership conference
12. Leadership exit conference
Frontline Staff Ownership of the Process
Involving staff in the initial accreditation process and continuing to involve them in ongoing
assessments and process and system reviews enhance ownership, which results in continued safe,
high-quality care for patients and their families. During the tracer activities, the surveyor(s) will focus
his or her discussions on the clinical and support staff and will request manager and leadership staff
only to provide clarification, if needed.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
37
JOINT COMMISSION INTERNATIONAL
CLINICAL LABORATORY
SAMPLE SURVEY AGENDA
3 DAY – 1 SURVEYOR
DAY ONE
Time Survey Activity
07:30 – 08:00 Opening Conference
08:00 – 10:00 Document Review
10:00 – 11:00 Leadership Conference
11:00 – 12:00 Walk-through Orientation to the Laboratory(ies)
12:00 – 12:45 Lunch
12:45 – 13:45 Visit to Blood Collection and Processing Areas
13:45 – 15:15 Quality Management and Improvement Process Systems
Tracer

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
38
15:15 – 16:30 Visit to Patient Care Units
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
39
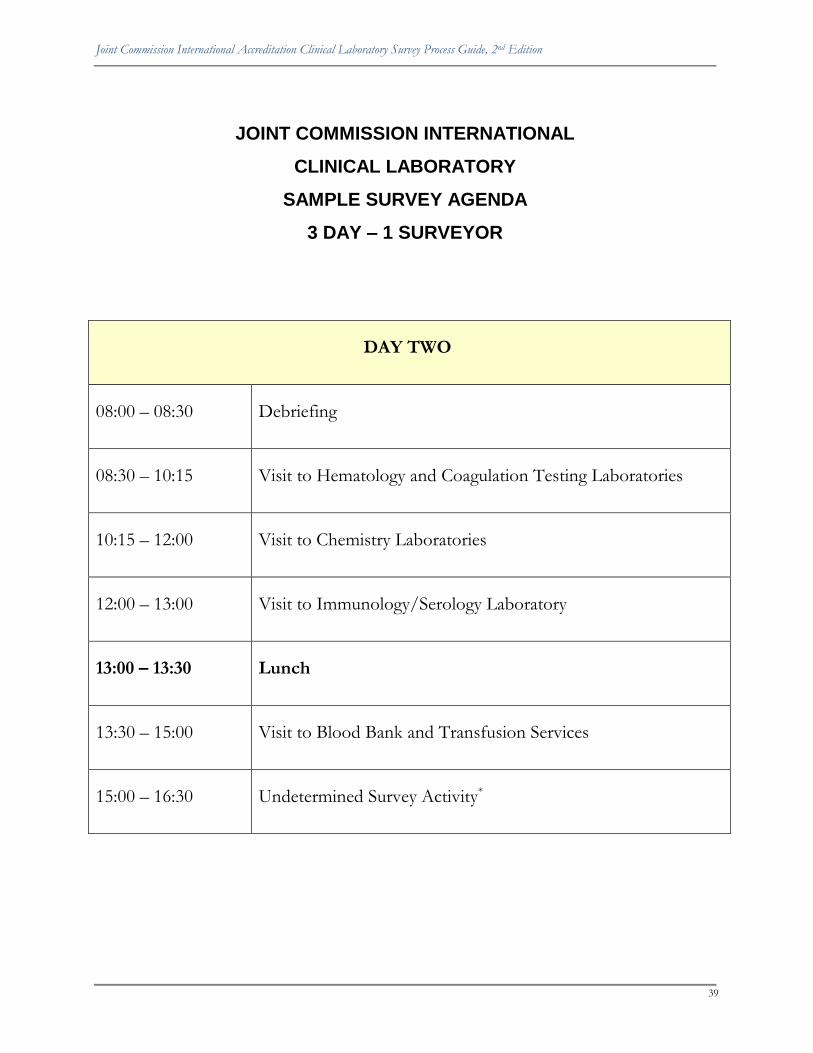
JOINT COMMISSION INTERNATIONAL
CLINICAL LABORATORY
SAMPLE SURVEY AGENDA
3 DAY – 1 SURVEYOR
DAY TWO
08:00 – 08:30 Debriefing
08:30 – 10:15 Visit to Hematology and Coagulation Testing Laboratories
10:15 – 12:00 Visit to Chemistry Laboratories
12:00 – 13:00 Visit to Immunology/Serology Laboratory
13:00 – 13:30 Lunch
13:30 – 15:00 Visit to Blood Bank and Transfusion Services
15:00 – 16:30 Undetermined Survey Activity*

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
40
* See page 60 for more information on ―Undetermined Survey Activities.‖

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
41
JOINT COMMISSION INTERNATIONAL
CLINICAL LABORATORY
SAMPLE SURVEY AGENDA
3 DAY – 1 SURVEYOR
DAY THREE
08:00 – 08:30 Debriefing
08:30 – 10:30 Visit to Microbiology Laboratories
10:30 – 12:00 Visit to Surgical Pathology and Autopsy Laboratories
12:00 – 12:30 Lunch
12:30 – 14:00 Visit to Histopathology and Cytology Laboratory
14:00 – 16:00 Surveyor time to organize findings
16:00 – 16:30 Leadership Exit Interview and Closing Conference

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
42
Tracer Methodology
Tracer methodology is the foundation of the JCI on-site survey and accomplishes the following:
Incorporates the use of information provided in the accreditation survey application and
previous survey and monitoring reports
Follows the experience of testing for a number of patients through the organization’s entire
health care process
Allows the surveyor(s) to identify issues in one or more steps of the patient testing process
or the interfaces between processes
Individual Patient Tracer Activity
The individual patient tracer activity is an evaluation method that is conducted during the on-site
survey and is designed to ―trace‖ the testing experiences that a patient had during his or her stay in
or visit to the organization. Tracer methodology is used to analyze a clinical laboratory’s system of
providing services using actual patients as the framework for assessing international standards
compliance. During an individual tracer, the surveyor(s) will perform the following:
Follow the course of testing services provided to the patient by and within the organization
and the clinical laboratory using current records whenever possible
Assess the interrelationships between and among disciplines and departments, programs,
services, or units, and the important functions in the services being provided
Evaluate the performance of relevant processes, with particular focus on the integration and
coordination of distinct but related processes
Identify potential concerns in the relevant processes
Using the information from the application, the surveyor(s) will select patients from an active patient
list to ―trace‖ their experiences throughout the organization. Patients typically selected are those who
have received multiple or complex services and therefore have experienced more contact with
various parts of the organization. This interaction will provide the opportunity to assess continuity of
care issues (also see the Glossary in the Joint Commission International Accreditation Standards for Clinical
Laboratories, Second Edition). To the extent possible, the surveyor(s) will make every effort to avoid
selecting tracers that occur at the same time and may overlap in terms of sites within the
organization.
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
43
Individual Patient Tracer Selection Criteria
Patient tracer selection may be based on, but not limited to, the following criteria:
Patients in the top five diagnoses groups for that organization, as applicable to the
laboratory setting
Patients who have testing done in more than one laboratory area, such as hematology, blood
bank, and microbiology
Patients who cross programs (such as patients who require laboratory results before dosing
and administration of certain medications)
Patients receiving specific tests on a specified date
The surveyor(s) will follow the patient’s experiences, looking at services provided by various
individuals and departments within the organization as well as ―handoffs‖ between them.
This type of review is designed to uncover systems issues, to look at the individual components of an
organization, and to examine how the components interact to provide safe, high-quality patient care.
The number of patients followed under tracer methodology will depend on the size and complexity
of the organization that the clinical laboratory serves and the number and types of the tests
performed. As appropriate to the provision of care being reviewed, the tracer will include the
following elements:
Review of the patient record with the staff person responsible for the patient’s care,
treatment, or services provided. If the responsible staff person is not available, the
surveyor(s) may speak with other staff members. Supervisor participation in this part of the
tracer should be limited. Additional staff involved in the patient’s care will meet with the
surveyor(s) as the tracer proceeds.
Observation of infection prevention and control issues
Discussion of data use in the clinical laboratory. This includes quality improvement
measures being used, information that has been learned, improvements made using data,
and data dissemination (also see the Glossary in the Joint Commission International Accreditation
Standards for Clinical Laboratories, Second Edition).
Observation of the impact of the environment on safety and staff roles in minimizing
environmental risk
Observation of maintenance of equipment (also see the Glossary in the Joint Commission
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
44
International Accreditation Standards for Clinical Laboratories, Second Edition) and review of
qualified personnel responsible for the maintenance of the equipment
Linkages to Other Survey Activities
Issues identified from the individual patient tracer activities may lead to further exploration in the
system tracers or other survey activities, such as the facilities tour and the leadership conference.
Findings from tracer visits provide focus for other tracers and may influence the selection of other
tracers. They may also identify issues related to the coordination and communication of information
relevant to the safety and quality of care services.
Individual-Based System Tracer Activity
Individual-based system tracers look at a specific system or process across the organization. When
possible, this activity will focus on the experiences of specific patients or on activities relevant to
specific patients. This differs from the individual tracers in that during individual tracers, the
surveyor(s) follows a patient or test through his or her course of care or through the test process,
evaluating all aspects of care rather than a system of care. During an individual-based system tracer,
the surveyor(s) will perform the following:
Evaluate the performance of relevant processes, with particular focus on the integration and
coordination of distinct but related processes
Evaluate communication among disciplines and departments
Identify potential concerns in relevant processes
An individual-based system tracer includes unit/department visits to evaluate the implementation of
the system process and to review the impact on patient care services, treatments, and tests. The
tracer also includes an interactive session that involves a surveyor(s) and relevant staff members and
that will utilize information from unit/department visits and individual tracers. Points of discussion
in the interactive session include the following:
Strengths in the process, weaknesses in the process, and possible actions to take in areas
needing improvement
Issues requiring further exploration in other survey activities
A baseline assessment of international standards and IPSG compliance
Education by the surveyor(s), as appropriate

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
45
Prevention and Control of Infections System Tracer
The infection prevention and control individual-based system tracer explores a clinical laboratory’s
infection prevention and control processes. The goals of this session are to assess a clinical
laboratory’s compliance with IPSG.5 and RSM.6.1 to identify infection prevention and control issues
that require further exploration, to determine actions that may be necessary to address any identified
risks, and to improve patient and staff safety.
Quality Management and Improvement Process Systems Tracer
The focus of this system tracer is the processes a clinical laboratory uses to collect, analyze, interpret,
and use data to improve patient safety, care, and processes. The surveyor(s) will also evaluate the
effectiveness of the clinical laboratory’s implementation of quality and safety action plans, processes,
and programs.
The Role of Staff in Tracer Methodology
Staff will be asked to provide the surveyor(s) with a list of patients presently in the organization,
including the patients’ names, current locations in the organization, and diagnoses, as appropriate.
The surveyor(s) may request assistance from organization staff for selection of appropriate tracer
patients. As the surveyor(s) moves around the organization, he or she will converse with a wide
variety of staff involved in the traced patient’s care, treatment, services, and tests. This staff could
include nurses, physicians, therapists, case managers, aides, pharmacy staff, lab personnel (as
appropriate), and support staff. If those staff members are not available, the surveyor(s) will ask to
speak to another staff member who would perform the same function(s) as the member who has
cared for or is caring for the tracer patient.
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
46
The Accreditation Decision
The final accreditation decision is based on the clinical laboratory’s compliance with JCI standards.
Clinical laboratories do not receive a numeric score as part of the final accreditation decision. When
a clinical laboratory successfully meets JCI accreditation requirements, it will receive an award of
Accredited. This decision indicates that a clinical laboratory is in compliance with all applicable
standards at the time of the on-site survey. The JCI Accreditation Central Office may request an SIP,
which must be accepted by the JCI Accreditation Central Office, or the status of Accredited could be
removed.
Promoting Accreditation
After a clinical laboratory receives official notification of the accreditation decision, it can publicize
its international accreditation achievement by notifying patients, the public, the local media, third-
party payers, and resident referral sources. JCI provides a free publicity kit to accredited clinical
laboratories that includes the following:
Suggestions for celebrating accreditation
Guidelines for publicizing JCI accreditation
Frequently asked questions
Sample news release
Fact sheet
Information about a clinical laboratory’s accreditation status will be posted on the JCI Web site at
http://www.jointcommissioninternational.org. The Web site allows anyone to locate JCI–accredited
clinical laboratories within a country and region of the world.
The Continuing Accreditation Cycle
The accreditation process does not end when the on-site survey is completed. In the three
years between on-site surveys, JCI requests ongoing evidence of compliance and corrective
actions, such as a self-assessment, periodic submission of compliance data, root cause
analyses, and/or response to complaints. For this reason, it is very important for the clinical
laboratory to maintain compliance with standards between on-site surveys as well as new
standards published in new editions of the manual.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
47
Continuous survey compliance means clinical laboratories can focus less on ―ramping up‖ for
survey every three years and, instead, can (and should) focus on continually improving their systems
and operations, thereby eliminating the need for intense survey preparation. Continuous compliance
with JCI standards directly contributes to the maintenance of safe, high-quality care and improved
clinical laboratory performance.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
48

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
49

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
50
Opening Conference
PURPOSE
During the opening conference, the surveyor(s) describes the structure and content of the
survey to the clinical laboratory.
LOCATION
At the discretion of the clinical laboratory
CLINICAL LABORATORY PARTICIPANTS
Laboratory director and/or chief executive officer
Individual responsible for coordinating the clinical laboratory’s survey agenda, such as a
survey coordinator
Representatives of the organization’s leadership if the clinical laboratory is part of a health
care organization, such as a hospital or ambulatory care center
Others, at the discretion of the clinical laboratory
SURVEYOR(S)
All surveyors
STANDARDS/ISSUES TO BE ADDRESSED
Introduction and coordination of the survey
DOCUMENTS/MATERIALS NEEDED
Final survey agenda
WHAT WILL OCCUR
Surveyor(s) will be introduced.
Leadership will be introduced.
Agenda will be reviewed and modified.
Surveyor(s) will answer questions about the survey agenda.
Surveyor(s) will explain the use of tracer methodology during the survey process activities.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
51
Surveyor(s) will explain the concept of ―drilling down‖ as an interviewing
technique/approach that aims to gather specific information about a process or outcome.
Staff members involved in drilling down inquiries should not perceive this approach as
personal or necessarily an indication of noncompliance. It is an indication that the
surveyor(s) is evaluating the establishment of systems to support a process.
Surveyor(s) will explain staff involvement in the documentation review process.
Surveyor(s) will explain staff involvement in the staff qualifications and education interview.
Surveyor(s) will explain the purpose of and the leaders’ involvement in the daily briefing
sessions.
Clinical laboratory staff will be encouraged to ask questions and seek clarification from the
surveyor(s) throughout the survey process.
Clinical laboratory staff will notify the surveyor(s) where lunch will be served or where he or
she can purchase lunch.
Clinical laboratory staff will identify country-specific information to ensure that the survey
team observes significant customs and values of the clinical laboratory during the survey
process, particularly if observance of customs impacts the survey agenda. For example, how
would the clinical laboratory prefer that the surveyor(s) conduct survey sessions during
times that staff members participate in prayer activities? In addition, clinical laboratory staff
should indicate how staff members would prefer to be addressed and should discuss the use
of interpreters, when needed.
Clinical laboratory staff will show the surveyors where the surveyors can meet as a group.
This location should be the same room where documents are gathered for surveyor review.
Clinical laboratory staff will introduce the surveyor(s) to the staff member who will provide
assistance throughout the day. This staff person will help the surveyor(s) to move quickly
between clinical laboratory locations and to maintain the planned schedule. This staff person
is usually a leader of the clinical laboratory or the survey coordinator.
HOW TO PREPARE
Set up a meeting or conference room large enough for the surveyor(s) to meet with key
organization and clinical laboratory leaders and with survey coordinators.
Notify clinical laboratory receptionists, so they can direct the surveyor(s) to the room when
he or she arrives.
Have copies of the survey agenda available for all participants in the opening conference.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
52
Prior to the survey, decide which clinical laboratory leader or staff member will accompany
each surveyor throughout the survey day.
Arrange for surveyor(s) to be served or to purchase lunch.
Notify clinical laboratory staff of the survey agenda.
The surveyor(s) will wear a name badge that will identify him or her as a JCI surveyor(s). If
the clinical laboratory requires additional clinical laboratory–specific identification, prepare
and make it available to the surveyor(s) in the opening conference.
Note: The survey team leader will conduct a brief meeting prior to the opening conference with the
CEO, survey coordinator, and translators to discuss the logistics and expectations for the on-site
survey and use of translators. If there will be any approved observers, clinical laboratories must
provide a list of their names, titles, and organization affiliations to the survey team leader.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
53
Orientation to the Clinical Laboratory’s Services and the Quality
Improvement Process
PURPOSE
The clinical laboratory orients the surveyor(s) to the services, programs, and strategic
activities the clinical laboratory provides and its quality improvement process. This
information provides the surveyor(s) with baseline information about the clinical laboratory
and the quality and patient safety program that can help focus subsequent survey activities.
LOCATION
At the discretion of the clinical laboratory
CLINICAL LABORATORY PARTICIPANTS
Chief executive officer
Individual responsible for coordinating the clinical laboratory’s survey agenda, such as a
survey coordinator
Medical staff leadership
Nursing leadership
Staff responsible for the quality improvement and patient safety program, if applicable
Others, at the discretion of the clinical laboratory
SURVEYOR(S)
All surveyors
STANDARDS/ISSUES TO BE ADDRESSED
Overview of the clinical laboratory’s services
Overview of the quality improvement and patient safety program and process
DOCUMENTS/MATERIALS NEEDED
Organization chart
Quality improvement example

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
54
WHAT WILL OCCUR
The clinical laboratory will give an overview of its structure, services, and strategic activities.
The clinical laboratory may include a brief presentation about the structure and methods of
the quality improvement and patient safety program.
The presentation should show how quality and safety information flows through the clinical
laboratory committee structure.
The presentation should describe the following:
o How quality and safety measures were chosen
o How the measures were prioritized for data collection
o How data are collected, aggregated, and analyzed
o How findings from data analysis are communicated and used for planning
improvements
The clinical laboratory may choose to present a quality improvement example to
demonstrate the clinical laboratory’s methodology and sustained improvement.
The surveyor(s) will ask questions, as needed, to clarify information or to request additional
information for use at a later time.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, Second Edition
55
Surveyor Planning Session
PURPOSE
During this session, the surveyor(s) reviews data and information about the clinical laboratory and
the organization (if appropriate) and plans the survey agenda. The surveyor(s) also selects initial
tracer patients/tests.
LOCATION
The clinical laboratory should provide space for this activity, usually the room designated as the
―surveyor headquarters.‖ This space should have the following items:
Conference table
Power outlets
Telephone
High-speed Internet connection/access for each surveyor
Printer
CLINICAL LABORATORY PARTICIPANTS
Clinical laboratory survey coordinator (as needed by team)
Translators (as needed by team)
SURVEYOR(S)
All surveyors
WHAT WILL OCCUR
This time is set aside for the surveyor(s) to review and discuss pertinent data and plan the survey
agenda. The surveyor(s) reviews the following items (as applicable to the setting), and these materials
should remain available to the surveyor(s) for the entire duration of the survey:
Performance improvement data, including committee meeting minutes for 12 months
prior to the survey
Infection prevention and control surveillance data, including committee meeting minutes
for 12 months prior to the survey
An organization chart and map

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
56
A current list of inpatients, including their names, diagnoses, ages, admission dates,
physicians, and units/services
Name of key contact person (such as a supervisor or scheduler) who can assist the
surveyor(s) in planning tracer selection
A list of contact telephone numbers in case the surveyor(s) needs to reach key staff
SELECTION OF INDIVIDUAL TRACERS
Surveyor(s) reviews the information from the survey application and the list of patients
currently receiving care in the organization to guide his or her selection of patients to
trace.
Surveyor(s) identifies a clinical/service group and some general information about the
patient population receiving care and services.
Surveyor(s) describes to the survey coordinator the type of patient that he or she is
seeking to trace and requests staff’s assistance in identifying an individual.
In surveys longer than one day, the surveyor(s) informs the clinical laboratory during the
morning daily briefing about the types of tracers he or she wants to perform that day to
facilitate activity planning. This does not mean that the surveyor(s) will identify a specific
patient from the list supplied by the clinical laboratory. For example, the surveyor(s) may
choose to trace the following types of patients:
o An ambulatory patient who visited the internal medicine clinic and had
laboratory services
o An intensive care patient who is receiving blood gas testing
o An inpatient receiving point-of-care testing
o A critical patient receiving multiple tests
o A patient whose medication dosage is dependent on results of a laboratory test
(for example, a patient on heparin)
In team surveys, tracer selection should be coordinated when possible to avoid overlap of
visits to various units.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
57
In clinical laboratories with multiple sites, individual tracers will include patients who
move between locations and services addressed by the represented accreditation
programs.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
58
Document Review
PURPOSE
The objective of the document review session is to survey standards that require some written
evidence of compliance, such as the plan for the Quality Management and Improvement Process or
Proficiency Testing documentation. Additionally, this session orients the survey team to the structure
of the organization, clinical laboratory, and management.
LOCATION
A meeting room or office that will be used throughout the duration of the survey as a meeting place
and work area for the survey team
CLINICAL LABORATORY PARTICIPANTS
Participants should include clinical laboratory staff members who are familiar with the documents
that will be reviewed, can translate these, and are able to respond to questions the surveyor(s) may
have during the session. At the discretion of the team, the surveyor(s) may designate a limited
number of staff members to attend and participate in the document review session. The session may
be conducted as an interview of staff about the documents. This approach has been very effective
when language barriers exist and the survey activities necessitate the use of professional interpreters.
SURVEYOR(S)
All surveyors
STANDARDS/ISSUES TO BE ADDRESSED
Almost all standards chapters make reference to plans, policies, and procedures that are to be
written. The following section and the ―Survey Planning: Reference Lists‖ section on pages 79–110
will assist staff members in understanding the particular documents that are a part of the
accreditation survey.
DOCUMENTS/MATERIALS NEEDED
The documents that should be available to the survey team for their review or reference during the
survey process are listed in the ―Survey Planning: Reference Lists‖ section on pages 79–110. The list
of documents includes the following:

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
59
Required quality monitors with data from the past 4 months (initial surveys) and/or 12
months for triennial surveys
Required clinical laboratory plans
Required policies and procedures, written documents, or bylaws
Minutes of the key committees for the past year, such as Performance Improvement,
Infection Prevention and Control, Safety, Leadership/Management Team Meetings, and
Medication Systems
If the laboratory is part of a larger organization, the following documents are required:
o An accurate list of the patients currently receiving care in the organization
o A list of the operative and other invasive procedures scheduled for the day,
including surgeries in the operating theatre, day surgeries, cardiac catheterizations,
endoscopies/colonoscopies, and in vitro fertilizations
o A sample action plan for a root cause analysis for a sentinel event or a near miss
o A sample FMEA action plan
o A current map of the hospital campus
o A sample of all medical record forms
In addition, the clinical laboratory should complete and have available for the survey teams the
worksheet related to relevant national or local health care–related laws and regulations. (See the Law
and Regulation Worksheet on pages 107–109.)
DOCUMENTS AVAILABLE IN ENGLISH
Documents showing evidence of compliance with the following standards must be provided to the
surveyor(s) in English:
Required Clinical Laboratory Plans
The quality management and improvement program is defined in a written plan. (MGT.4,
ME2)
Definition of the laboratory’s mission, vales, and goals. (MGT.1, intent)
The leaders identify, in writing, the type and scope of services provided by the laboratory.
(MGT.1.1, ME 4)

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
60
The organizational structure of the laboratory is defined in writing and/or by diagram, and
responsibilities and authorities of leadership positions are clearly communicated. (MGT.2,
ME 3, ME 4)
Required Policies and Procedures, Written Documents, or Bylaws
A collaborative process is used to develop policies and/or procedures that address the
accuracy of patient identification. (IPSG.1)
A collaborative process is used to develop policies and/or procedures that will establish
uniform processes to ensure the correct site, correct procedure, and correct patient,
including procedures done in settings other than the operating theatre. (IPSG.4, ME1)
The organization uses a checklist and time-out procedure just before starting a surgical
procedure. (IPSG.4, ME4)
The mission, values, and goals are delineated in a written document. (MGT.1, ME 2)
Laboratory leaders are involved in defining the program in writing. (MGT.4, ME 2)
The plan defines the structure, goals, and components of the program. (MGT.4.1, ME 2)
The plan describes the methodology used to measure and improve processes and services.
(MGT.4.1, ME 3)
The laboratory has a plan for inventory, handling, storage, and use of hazardous materials
and the control and disposal of hazardous waste. (RSM.6)
WHAT WILL OCCUR
The documents should be made available to the survey team in the meeting room that has
been designated for their use throughout the duration of the survey.
At the beginning of the session, one staff person should briefly orient the survey team to the
organization of the documents.
During the remainder of the session, a staff member who can respond to any questions the
surveyor(s) may have should be readily available (in person or by telephone).
The materials should remain available to the survey team throughout the survey for
reference purposes. However, if documents are required for use by clinical laboratory staff,
they may of course be removed. The surveyor(s) may schedule a second document review
session during the course of the survey. The survey team may also request additional
documents throughout the survey to clarify or become knowledgeable about the clinical

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
61
laboratory’s policies and procedures or performance. Clinical laboratory staff should be as
proactive as possible in complying with requests for documents.
Some of the documents may need to be translated into English, whereas other documents
may require an interpreter to be made available.
HOW TO PREPARE
It is highly probable that many of the required documents will be part of larger documents. Clinical
laboratories do not need to remove or photocopy pertinent sections of these documents. Instead,
clinical laboratories can identify these sections using bookmarks or tabs. Guidelines for cross-
referencing this information are provided in the next section.
Other documents, such as minutes and reports, may be freestanding or individual documents.
Clinical laboratories should decide whether to provide the original document or a photocopy. It is
always beneficial to have several examples of these documents, such as committee minutes from the
last few meetings.
If the clinical laboratory has a large quantity of examples or a large volume of materials on a given
topic, it should select the most representative or the most pertinent examples. There will not be time
for the surveyor(s) to review large amounts of material on any given topic.
ORGANIZATION OF THE MATERIALS
Because the issues identified in the document review list may be addressed in different documents
depending on the clinical laboratory, the following guidelines for organizing the documents to be
used by the surveyor(s) are provided.
Group the freestanding or individual documents according to the following lists provided in this
guide:
Required quality monitors (See page 79.)
Required clinical laboratory plans (See page 80.)
Required policies and procedures, written documents, clinical laboratory plans, or bylaws
(See page 81.)
Required personnel information, such as job descriptions, orientation documents, in-service
education documentation, and competence assessment information
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
62
Quality control documents, including quality control procedures, quality control results for
each laboratory area, and proficiency testing results
Note: When possible, please indicate the standards that the document addresses. The documents
may be grouped in binders or folders or other means may be used to separate major topical areas.
Gather the documents in one place. Identify the location in the document where the specific
information that is required by the standard may be found. The clinical laboratory may use methods
such as the following to identify the information:
A guide
An index
Bookmarks
Tabs
Note: When information is provided using computer monitors rather than paper, the following
conditions should be met:
Each member of the survey team should be provided with a monitor.
A printer should be available in case a member of the survey team wishes to print a
paper copy of a given document.
Staff may be needed to assist the surveyor(s) in locating the documents in the
computer.
Printed copies of bylaws and longer documents that may require extensive reading or
scanning by the surveyor(s) should be available.
EVALUATION OF THE POLICIES AND PROCEDURES BY THE SURVEY TEAM
The documents reviewed by the survey team provide an overview of what they expect to see in
actual practice during the survey process. For example, they would expect to find the following when
a new procedure on the disposal of infectious waste is developed:
That appropriate staff have been educated about the new procedure
That any special skills or other needed training has taken place
That waste is actually being disposed of according to the new procedure

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
63
That any documentation required by the procedure is available for review
The presence of a policy or procedure alone usually does not determine the score of the standard.
Rather, the score is determined by the daily practice (implementation) of the policy or procedure.
The survey team will look for evidence that the practice related to the policy or procedure is well
implemented, as appropriate, throughout the clinical laboratory and thus is sustainable. In the event
the implementation appears incomplete to the survey team or the implementation occurred in a
manner that is not sustainable, the survey team will make a recommendation that more time be
allowed for better evidence of sustainable implementation and for incorporating the
recommendation into the survey follow-up requirements.
In general, the length of time a policy has been implemented is referred to as a ―track record.‖ The
survey team will look for a 4-month track record for policy-related standards during an initial survey
and for a 12-month track record during a triennial survey. For policy-related standards to be scored
―fully met,‖ the track record requirement must be met. When the track record period has not been
met, but the survey team finds that the policy has been implemented in a sustainable manner, the
team has the prerogative to score the standard as ―fully met.‖
The track record for new standards will be from the ―effective date‖ to the date of survey. For
example, if a new standard/ME is effective on 1 April and the survey takes place on 1 September of
the same year, the required track record for the new standard/ME is 5 months for ―fully met.‖

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
64
Daily Briefing
PURPOSE
To facilitate understanding of the survey process and the findings that contribute to the
accreditation decision
LOCATION
At the discretion of the clinical laboratory
CLINICAL LABORATORY PARTICIPANTS
Clinical laboratory survey coordinator (as needed by team)
Chief executive officer and/or clinical laboratory director
Designated leaders (as determined by the clinical laboratory)
SURVEYOR(S)
All surveyors
WHAT WILL OCCUR
The daily briefing occurs every morning of a multiday survey with the exception of the first
day. The session is intended to be brief; 30 to 60 minutes is suggested depending on the
number of surveyors on the team.
When multiple surveyors are on site, the briefing is conducted jointly, with the survey team
leader serving as the facilitator.
During the daily briefing with the clinical laboratory, the surveyor(s) will perform the
following actions:
Offer a concise summary of the survey process activities completed on the previous
day
Make general comments regarding significant issues resulting from the previous day’s
activities
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
65
Note any specific positive findings
Emphasize patterns or trends of significant concern that could lead to
noncompliance determinations. The surveyor(s) does not report minor, one-time, or
single observations that do not impact scoring.
Inform the clinical laboratory that final findings for any given standard will be
possible only when all activities are complete and results are aggregated
Allow the clinical laboratory to provide information that may have been missed
during the previous survey day
Address clinical laboratory requests for discussion on findings and indicate when
such discussions can take place
Schedule time for more extensive discussion or review of additional evidence of
compliance on issues that arise
Review the agenda for the survey day ahead (including the identification of
individual patient tracers) and make any necessary adjustments based on clinical
laboratory needs or the need for more intensive assessment of an issue during the
―undetermined survey activity‖ time
Conclude the briefing and transition to the next activity(s) according to the agenda
Do not expect the surveyor(s) to perform the following actions:
Repeat observations made at a previous daily briefing unless it is in the context of
identifying a systemic issue
Discuss, in detail, each survey activity, specific records, and conversations held with
individuals during tracers
Delay scheduled activities for the current day to have an in-depth discussion of
issues from the previous day
SPECIAL SITUATIONS
There may be instances when a surveyor(s) will be scheduled to survey an activity that is not
taking place at the same location where a daily briefing would normally occur; this may take
place particularly when surveying with a team. There may also be situations in which a

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
66
surveyor(s) is brought in for a day or two and departs earlier than the rest of the team. If a
surveyor(s) cannot be physically present for the daily briefing, the surveyor(s) will do the
following:
Try to make arrangements to join via conference call
Share details of the previous day’s activities and findings with another surveyor for
the daily briefing presentation, even if a conference call is anticipated

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
67
Clinical Laboratory Environment Tour
PURPOSE
The purpose of the environment tour is to address issues related to the following:
The physical environment
Medical and other equipment
Patient, visitor, and staff safety and security
Infection prevention and control
Emergency preparedness
Hazardous materials and waste
Staff education
LOCATION
Depending on the size and location of the clinical laboratory services, selected areas of the clinical
laboratory will be visited. The surveyor(s) will be looking to see if the corridors and exit paths of
travel are free for the safe exit of the facility in an emergency. The tour is designed to cover high-risk
areas for safety and security.
CLINICAL LABORATORY PARTICIPANTS
Laboratory manager
Safety officer and/or facility manager (if applicable)
Laboratory director(s)
Infection control practitioner (if applicable)
Others, as identified by the clinical laboratory
SURVEYOR(S)
All surveyors
STANDARDS/ISSUES TO BE ADDRESSED
Laboratory environment safety (RSM.5, RSM.7)
DOCUMENTS/MATERIALS NEEDED

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
68
Documents, such as plans (for example the risk assessment plan identified in RSM.7, intent),
policies and procedures, test and maintenance reports (as identified in (a) through (g) of
RSM.4.1.1, intent), that describe the plans for the following:
(a) Safety and security (RSM.5, RSM.7.2)
(b) Hazardous materials (RSM.6, RSM.6.2, RSM.6.3)
(c) Biohazardous materials and waste (RSM.6.1)
(d) Fire safety (RSM.7.1)
(e) Laboratory equipment and other materials (RSM.4 through RSM.4.5)
(f) Utilities Management (RSM.3.2 through RMS.3.2.1)
(g) Infrastructure–Basic Facilities (RSM.3 through RSM.3.1.1)
WHAT WILL OCCUR
The surveyor(s) may request to review the risk management report identified in RSM.7, intent, and will then
visit different areas of the clinical laboratory to observe adequacy of space and other necessary resources,
such as equipment and supplies. The surveyor(s) will examine the design of the clinical laboratory and
whether areas that require mental concentration are separated from areas with constant disruptions and
whether high-risk areas, such as bacteriology, are away from main traffic areas. If specimens are collected
from outpatients in the laboratory, the surveyor(s) will observe the area to determine that it is protected and
provides adequate privacy.
The surveyor(s) will visit testing and patient care areas as well as non-testing and non–patient care
areas of the clinical laboratory. In all areas, the surveyor(s) will observe the facility and interview staff
to learn how the clinical laboratory manages the facility to accomplish the following:
Reduce and control hazards and risks
Prevent accidents and injuries
Maintain safe conditions
Maintain secure conditions
Implement emergency response plans
Note: In some survey agendas, two surveyors will visit separate sections of the clinical
laboratory at the same time. The clinical laboratory should be prepared to have staff
available to guide and assist each surveyor on the tour of the facility.
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
69
The non-patient care areas visited by the surveyor(s) include the following:
The emergency power generator
Storage areas such as:
o Hazardous materials storerooms
o Hazardous materials disposal area
o Equipment storage area
Decontamination areas
HOW TO PREPARE
Prior to survey, the clinical laboratory leaders and facility manager(s) should carefully
read the relevant standards.
The facility manager(s) should tour the facility, conduct an inspection according to
the standards, and attempt to address any deficiencies prior to survey.
The clinical laboratory should be aware of relevant laws, regulations, and facility
inspections and should be able to share this information with the surveyor(s).
Complete the relevant sections of the Law and Regulation Worksheet on pages 107–
109.)
Representatives of the clinical laboratory should be prepared to show the surveyor(s)
how their facility management plans are implemented. For example, they should
demonstrate how hazardous materials are stored and disposed of.
Prior to survey, the clinical laboratory should ensure that all laboratory equipment
has been maintained, tested, and inspected and that these activities are documented
(RSM.4.1).
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
70
Individual Patient Tracer Activity
PURPOSE
A tracer follows the experiences of an individual patient’s testing process to evaluate the
laboratory’s and organization’s performance against international standards. One approach
to conducting a tracer is to sequentially follow the testing processes from ordering the test
through reporting the results. During an individual tracer, the surveyor(s) will do the
following:
Follow the course of the test using current records or patients who were tested in the
past
Assess the interrelationships between and among disciplines and departments,
programs, services, or units and the important functions in the care, treatment, and
services being provided
Evaluate the performance of relevant processes, with particular focus on the
integration and coordination of distinct, but related, processes
Identify potential concerns in the relevant processes
LABORATORY PARTICIPANTS
During a tracer, the surveyor(s) will converse with a wide variety of staff involved in the patient’s
care, treatment, and services. Staff could include nurses, physicians, therapists, case managers, aides,
pharmacy and lab personnel (as appropriate), and support staff. When an individual who actually
performed the function is available, the surveyor(s) prefers to interview that staff member. This
would include staff members who transcribe orders, collect specimens, transport specimens, receive
specimens in the laboratory, process specimens, perform patient testing, and review and report
results.
SURVEYOR(S)
All surveyor(s)
STANDARDS/ISSUES TO BE ADDRESSED
All standards chapters may be addressed during this visit.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
71
DOCUMENTS/MATERIALS NEEDED
All documentation of the clinical laboratory’s activities related to the quality control program may be
reviewed. This will include the documentation of the orders and test results in the clinical records of
patients.
WHAT WILL OCCUR
During the visits to the laboratory and patient care areas, the surveyor(s) may conduct a tracer. A laboratory
tracer follows the pre-analytic, analytic, and post-analytic testing practices through the entire process. A
complete tracer will include a review of the following:
Order for the test or blood component
Requesting process
Specimen collection procedures and processes
Specimen transport to the laboratory
Specimen accessioning and processing in the laboratory
Specimen testing
Review of test results and quality control reporting of results
The surveyor(s) selects patients for tracers using various methods, including the most treated diagnosis or
least treated diagnosis in a clinical laboratory, or he/she may select specific dates and ask the clinical
laboratory to give them a list of patients who had specific tests ordered on those dates. They will typically
select patients who have had testing performed in more than one laboratory area, for example, hematology,
blood bank, and microbiology. The surveyor(s) will then ―trace‖ the course of the patient and specimen
experience through the processes listed above.
The surveyor(s) will follow the patient’s experience, looking at services provided by various
individuals and departments within the organization as well as at ―handoffs‖ between them. This
type of review is designed to uncover systems issues, looking at both the individual components of
the clinical laboratory, and how the components interact to provide safe, high-quality patient care.
The tracer starts in the patient care setting or unit where the patient and the clinical record are
currently located. This is where the surveyor(s) begins to trace the entire care or service
process from preadmission through postdischarge. The surveyor(s) has approximately two
hours to conduct a tracer, although it may be shorter or longer depending on its complexity

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
72
and other circumstances. Multiple patient records may be reviewed during a single
designated tracer activity.
As appropriate to the provision of care being reviewed, the tracer will include the following
elements:
Review of records and documents in each step of the care process
Observation of specimen collection, processing, and testing, including the patient and specimen
identification processes
Observation of the movement of blood for transfusion out of the laboratory and to
the patient care unit where the identification process is observed and observation of
the initiation of the transfusion
Observation of infection prevention and control issues
Discussion of data use in the laboratory, including review and interpretation of
quality control data and other quality improvement measures
Observation of the impact of the environment on safety
Staff roles in minimizing environmental risk
If the surveyor(s) finds problems with the documents, such as quality control
documentation, he or she may select and review additional records to verify issues
that may have been identified. The surveyor(s) may ask staff to assist with the review
of the additional records.
Interview with staff
LINKAGES TO OTHER SURVEY ACTIVITIES
Issues identified from the tracer activities may lead to further exploration in the system tracers or
other survey activities, such as the facilities tour and leadership conference. The surveyor(s) will use
time scheduled as ―undetermined survey activity‖ on the agenda to conduct additional activities to
clarify issues, to gather additional information, and to evaluate standards compliance that is not
directly related to a patient tracer.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
73
Findings from tracer visits provide focus for other tracers and may influence the selection of
other tracers. They may also identify issues related to the coordination and communication
of information relevant to the safety and quality of care services.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
74
System Tracer: Infection Control
PURPOSE
During the discussion of the infection prevention and control program, the surveyor(s) and clinical
laboratory will be able to accomplish the following:
Identify strengths and potential areas of concern in the infection prevention and control
program
Begin determining actions necessary to address any identified risks in infection prevention
and control processes
Begin assessing or determining the degree of compliance with relevant standards
Identify infection prevention and control issues requiring further exploration
Note: When a separate Infection Control System Tracer is not noted on the agenda (for example, on
shorter surveys), the surveyor(s) will address infection prevention and control throughout individual
patient tracers and during the Quality Management and Improvement Process tracer.
CLINICAL LABORATORY PARTICIPANTS
Individuals from the clinical laboratory selected for participation should be able to address issues
related to the infection prevention and control program in all major areas within the clinical
laboratory. This group should include, but not be limited to, representatives from the following
departments, as applicable:
Clinical staff, including physicians, technicians, and laboratory personnel
Clinicians from the laboratory who are knowledgeable about microbiology
Staff responsible for the physical plant
Clinical laboratory leadership
Note: To facilitate a beneficial exchange between the surveyor(s) and the clinical laboratory, the
clinical laboratory should identify a relatively small group of active participants for discussions and
interviews. Other staff may attend as observers.
SURVEYOR(S)
All surveyors available to participate
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
75
WHAT WILL OCCUR
The session will open with introductions and a review of the goals for the Infection Control System
Tracer, which include the following:
Exploration, critical thinking, and potential problem solving about how the infection
prevention and control program incorporates laboratory services
Identification of potential areas of concern in the laboratory setting that relate to the
infection prevention and control program and areas for improvement and actions that could
be taken to address these
Process
The tracer may begin with a short group meeting with individuals responsible for the clinical
laboratory’s infection prevention and control program or in a patient care area identified by
the surveyor(s) for the focused-tracer activity.
During the group meeting, the surveyor(s) will gain a better understanding of the infection
prevention and control system and will identify potential areas that could be explored during
the patient care area visit and potential areas of concern that require further discussion with
staff knowledgeable about the clinical laboratory’s infection prevention and control
program. Examples of these areas include the following:
o How are infections, such as methicillin-resistant staphylococcus aureus (MRSA) and
Clostridium difficile (C diff), identified?
o Who is notified that these infections are present?
o How does the microbiology department communicate the various results to relevant
infection control personnel?
The surveyor(s) may move to other settings as appropriate and applicable to tracing
infection prevention and control processes across the clinical laboratory. Surveyors may ask
questions, such as the following:
o What are the infection control requirements for the different areas in the laboratory?
o Are there certain requirements related to eye protection, respiratory protection,
gloves, gowns and other protective equipment that should be worn in a laboratory?
The surveyor(s) will observe staff and engage them in discussions focused on infection
prevention and control practices in any setting that is visited during this system tracer
activity.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
76
Discussion
The surveyor(s) will draw from his or her tracer activity experience, clinical laboratory infection
prevention and control surveillance data, and other infection prevention and control–related data to
inspire scenarios for discussion with the clinical laboratory. Participants will be asked to discuss the
following aspects of the clinical laboratory’s infection prevention and control program as they relate
to the scenarios:
How patients with infections are identified by the clinical laboratory
Interactions with other departments, such as pharmacy, related to antibiotic selection
How patients with infections are considered within the context of the infection prevention
and control program
Current and past surveillance activities that took place in the previous 12 months or more
for re-surveys and 4 months or more for initial surveys
Type of analysis being conducted on the infection prevention and control data, including
comparisons
Reporting of infection prevention and control data, including frequency and audience
Prevention and control activities (for example, staff training, education of
patient/resident/client population, and housekeeping procedures)
Physical facility changes, either completed or in progress, that have an impact on infection
prevention and control
Actions taken as a result of surveillance and the outcomes of those actions
Effectiveness of implementation of IPSG.5 and the hand-hygiene guidelines
Clinical laboratories may use infection prevention and control data during this part of the activity if
the data are relevant to the discussion.
Conclusion
The surveyor(s) and clinical laboratory will summarize identified strengths and potential areas of
concern in the infection prevention and control program. The surveyor(s) will provide education as
applicable.
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
77
System Tracer: Quality Management and Improvement Process
PURPOSE
This session focuses on the clinical laboratory’s activities to improve quality and patient safety
through the use of data to manage risk. The goals of this session include the following:
Review the laboratory’s quality management and improvement plans and current activities
Provide feedback on those quality management and improvement activities observed during the unit
visits and interviews
Provide education and technical assistance on the establishment of a coordinated program for
managing quality in the laboratory
LABORATORY PARTICIPANTS
Chief executive officer and/or chief operating officer (if applicable)
Medical director
Laboratory supervisors
Staff responsible for the quality management and improvement process activities (if applicable)
Others, at the discretion of the laboratory leaders.
Note: To facilitate a beneficial exchange between the surveyor(s) and the clinical laboratory, the
clinical laboratory should identify a relatively small group of active participants for discussions and
interviews. Other staff may attend as observers.
SURVEYOR(S)
All surveyors available to participate
STANDARDS/ISSUES TO BE ADDRESSED
Standards in the Management and Leadership (MGT) chapter
DOCUMENTS/MATERIALS NEEDED
Clinical laboratories should have all of the following documents available for review during
this session or for the document review session on day one (see pages 38 to 39).

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
78
Leadership reports as identified in MGT.1.2.1 for contracted laboratory services and
reference laboratory services identified in MGT.1.2.2
Root cause analysis for any sentinel events and/or near misses, including definitions of
sentinel event and near miss and the methods and processes for performing a root cause
analysis. If possible, include a real-world example of a near miss event for which a root
cause analysis was performed.
Proactive risk assessments, such as failure mode and effects analysis (FMEA), hazard
vulnerability analysis (HVA), and infection control risk assessment (ICRA), including a
proactive risk analysis and redesign of at least one process per year. During this session,
the laboratory will show at least one example of a process that was analyzed and
redesigned to prevent possible problems.
Committee manuals, including committee minutes (for example, minutes from the
Quality Improvement and Patient Safety, Infection Prevention and Control, Risk
Management, and Complaint Management committees).
WHAT WILL OCCUR
The session is organized to better understand the processes related to quality monitoring and
improvement. Some of the activities for this session will be discussions and document
review for measures that are being used for improvement. Other activities can include the
surveyor(s) conducting focused tracers in the departments/services to evaluate the
effectiveness of the laboratory’s and organization’s implementation of the overall quality
plan; quality standards; and patient safety action plans, processes, and programs. The
surveyor(s) will perform the following activities and use the following methods:
The basics of data gathering and preparation, including the following:
o Selecting measures
o Data collection and aggregation
o Data analysis and interpretation
o Disseminating/transmitting findings
o Taking action
o Monitoring performance/improvement

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
79
Identify how the decision for the measures was made; how the data were collected; how
the findings were used; and how data, findings, and problems are communicated
throughout the clinical laboratory.
Determine the effectiveness in implementing the laboratory’s and organization’s action plans
developed as improvements following root cause analyses for sentinel events or near misses,
proactive risk assessments (such as FMEA and HVA), and managing quality and safety
complaints.
The surveyor(s) may incorporate examples from observations obtained from previous
individual patient tracers. During this session, the surveyor(s) will review only the monitoring
measures that have not been reviewed previously during the survey as part of the individual
or system tracers.
Infection Prevention and Control Data Issues (also see ―System Tracer: Infection
Control‖ on pages 50–52)
This system tracer is applicable in smaller surveys in which only one system tracer (Quality
Management and Improvement Process) is scheduled. Discussion explores the following
topics:
Types of monitoring measures and data collected:
o Whether infection-related data are collected
o Whether the laboratory and/or organization has developed and implemented a
system for measuring improvements
Using standardized definitions
Control methods (includes data dissemination to physicians, staff, leaders, and
external entities)
Prevention based on data findings
The laboratory’s and organization’s plans to collect data relevant to the JCI
Prevention and Control of Infections (PCI) standards
Conclusion

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
80
As a result of this session, the surveyor(s) and the laboratory leaders will be able to do the
following:
Identify strengths and weaknesses in the laboratory’s implementation of the quality plan,
including monitoring of performance measures, data use, areas identified for
improvement, and actions that could be taken
Identify specific data-use issues requiring further exploration as part of subsequent survey
activities
Provide appropriate education, as applicable

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
81
Visits to Laboratory Sections and/or Off-Site Laboratories and
Collection Stations
PURPOSE
The purpose of the visits to the laboratory sections and/or off-site laboratories and collection stations is to
address the following topics:
Section-specific policies and technical procedures
Preventive-maintenance and quality control documentation
Infection prevention and control and safety practices
Specimen collection and processing practices
Staff competence and whether the number of staff is adequate
Proficiency testing
LOCATION
The surveyor(s) will visit each section of the clinical laboratory listed on the final survey agenda. If clinical
laboratories have locations other than the main site where laboratory testing is performed, the surveyor(s)
will also visit these areas. If clinical laboratories have remote specimen collection sites, the surveyor(s) will
visit a sampling of these sites as well.
LABORATORY PARTICIPANTS
The participants will be determined by the clinical laboratory but should include at least the supervisory staff
in each clinical laboratory area. The clinical laboratory director and/or manager may participate, as
appropriate.
SURVEYOR(S)
If there is more than one surveyor, this activity will be divided among them, and the locations each will visit
will be determined while preparing the survey agenda.
STANDARD/ISSUES TO BE ADDRESSED
Resource Management and Laboratory Environment (RSM)
Development and Control of Policies and Procedures (DCP)
Quality Control Processes (QCP)

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
82
DOCUMENTS/MATERIALS NEEDED
Written technical procedures for performing tests
Laboratory records and applicable logs and registers documenting the accession of specimens,
documenting patient results, and including examples of laboratory reports
Quality control records and evidence of quality control evaluations
Equipment maintenance, performance testing, calibration, and linearity testing records and
documentation of review of these records
Records of method validation for newly implemented test methods
Records of correlation of test methods performed according to different methodologies, at different
sites, or on different instruments
Records of remedial actions taken when quality control or equipment performance testing is not
acceptable
Evidence of implementing infection prevention and control and other safety policies and
procedures in the clinical laboratory
Adequacy of space and resources for services provided by the clinical laboratory
Discussion about and evidence of how STAT tests or critical values are reported
Documents that show this particular area of the clinical laboratory’s involvement in the quality
management and improvement process
WHAT WILL OCCUR
The surveyor(s) will review the documentation listed in the previous section and discuss the quality control
policies and documentation of remedial action with supervisory staff. The process used to label specimens
and access them into the clinical laboratory will be reviewed. The methods used to document test results will
be evaluated, along with the method of reporting these results. There will also be a discussion of the
knowledge each area of the clinical laboratory has concerning the laboratory’s quality management and
improvement process program as well as their involvement.
HOW TO PREPARE
Educate staff about applicable standards. Prepare staff by conducting mock interviews based on these
standards. Some sample questions include the following:

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
83
QCP.1.1 and QCP.1.1.1: Who performs the tests on proficiency samples? Do these personnel also test
patient samples? How many times do you analyze proficiency specimens, and is it consistent with how you
analyze patient samples?
QCP.1.1.2: Are there tests that are not included in a proficiency testing program? If so, what means do you
have of verifying their accuracy and reliability?
QCP.1.6: What is your process for reviewing quality control and patient results, and where is this review
process documented? Who performs the review?
QCP.1 (along with specific quality control standards found under each laboratory section): What are your
quality control processes for each test and how are results documented?
QCP.1.7: What are your policies regarding unacceptable quality control results, and how do you document
remedial action when this occurs?
Carefully observe the area to look for other standards compliance issues that the surveyor(s) is likely to
notice on the tour. These issues include infection prevention and control, fire safety, area cleanliness, and
equipment maintenance and performance testing.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
84
Inpatient Unit/Setting Visits (where applicable)
PURPOSE
The purpose of conducting visits to inpatient units/settings is to evaluate the interface between the
laboratory and the rest of the organization, to review any point-of-care testing performed on patient units,
and to review blood transfusion practices.
LOCATION
Patient unit or clinical department
CLINICAL LABORATORY PARTICIPANTS
Laboratory leader(s)
Clinic manager(s)
Others engaged in providing patient care in the unit/setting
SURVEYOR(S)
If there is more than one surveyor, each will visit separate patient units.
STANDARDS/ISSUES TO BE ADDRESSED
All standards chapters may be addressed during this visit.
DOCUMENTS/MATERIALS NEEDED
A sample of clinical records of patients currently receiving care in the unit/setting
Laboratory specimen collection procedures
Procedures for blood transfusions and for identifying and reporting a suspected transfusion
reaction
WHAT WILL OCCUR
Visits to inpatient units/settings include the following elements:
A review of patient records to determine how laboratory results are reported
A review of laboratory specimen collection procedures provided to the unit
A review of blood transfusion procedures

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
85
An observation of a clinician starting a blood transfusion (if possible)
A review of any point-of-care laboratory testing that is being performed on the unit/setting,
including laboratory testing performed outside formal laboratory areas
An interview with unit managers to determine how the laboratory works with units/settings and
how emergency test results and critical values are reported
The surveyor(s) begins the inpatient visit by explaining the purpose of the survey visit, then asks for a brief
general orientation to the unit/service from the manager or director. The surveyor(s) will then review a list
of the patients in the unit/setting and begin selecting patient clinical records to be reviewed with staff during
the visit.
The inpatient visit may include an observation of the start of a blood transfusion to verify adequate
procedures are being used to identify the patient and the unit(s) of blood and to ensure patient monitoring
for any signs of a transfusion reaction is initiated. (QCP)
The surveyor(s) may interview staff to better understand how the laboratory communicates with the
unit/setting. (MGT)
The standards require that anyone who prepares patients for specimen collection or who collects specimens
does so using written procedures for these activities. The surveyor(s) will verify that such procedures are
current, complete, and that staff are familiar with them. (DCP)
As in any unit/setting, the surveyor(s) will also observe the condition of the facility (RSM) and infection
prevention and control practices (RSM).
HOW TO PREPARE
Laboratory leaders should help managers and directors of each unit/setting become familiar with applicable
standards. Laboratory leaders should closely evaluate any point-of-care testing being performed on the unit
or in the setting to ensure applicable standards in the QCP chapter are being met. Necessary changes should
be made before the survey, and staff should be educated in care practices required by the standards.
Staff should be told what to expect when the surveyor(s) visits the unit/setting. It may be helpful to conduct
mock interviews with staff, so they are comfortable with the types of questions the surveyor(s) may ask.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
86
Staff should also be made aware of the location in the unit/setting of the laboratory’s specimen collection
procedures and quality control, maintenance, and competency records for the testing performed outside the
main laboratory. These records should be assembled and be readily available when the surveyor(s) visits the
area.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
87
Undetermined Survey Activities
PURPOSE
Tracer methodology is used as the primary tool to assess standards compliance. However, other
tools or a focused approach can be used to gather additional information to evaluate standards
compliance that is not directly related to a specific patient tracer. Each of these focused activities is
listed on the survey agenda as an ―Undetermined Survey Activity.‖
Undetermined survey activities are broadly defined and encompass a variety of activities customized
to the particular needs of each clinical laboratory. Undetermined survey activities are selected by the
survey team to allow for a more intensified assessment of a targeted area when information from any
survey activity, such as tracers or discussions, identifies a need to focus on a specific concern or to
increase the sample size of a review item.
LABORATORY PARTICIPANTS
Participants will be identified by the surveyor(s) depending on the activity being evaluated.
STANDARDS/ISSUES TO BE ADDRESSED
Standards/issues that will be addressed are those that relate to the specific activity that is being
surveyed. For example, if the survey activity is focused on hazardous materials, one of the standards
that would be addressed is RSM.6.
WHAT WILL OCCUR
Examples of undetermined survey activities include, but are not limited to, the following:
Focused tracers that are not patient tracers:
o Access to medical information
o Disinfection processes
o Blood product infusion processes
Focused process tracer:
o Hazardous materials management
o Laboratory specimen handling
Specific patient safety and quality activities:

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
88
o Failure mode and effects analysis
o Root cause analysis review
o Sentinel event review
Focused document/policy review to close gaps in the usual document review exercise
Other items as appropriate to the needs of the team

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
89
Education Session: Clinical Laboratory Decision Rules, Scoring
Guidelines, and Strategic Improvement Plan
PURPOSE
The purpose of this session is to provide education to clinical laboratory leadership to help them
understand the decision rules, the surveyor scoring guidelines, and the SIP.
LOCATION
At the discretion of the clinical laboratory leaders
CLINICAL LABORATORY PARTICIPANTS
Chief executive officer
Chief operating officer
Chairman, governing body, or similar representative
Medical staff leadership
Survey coordinator and core quality leadership group
Others, at the discretion of the clinical laboratory leaders
STANDARDS/ISSUES TO BE ADDRESSED
Clinical laboratory decision rules
Surveyor’s(s’) scoring guidelines
SIP tool
DOCUMENTS/MATERIALS NEEDED
None
WHAT WILL OCCUR
The surveyor(s) will cover the following topics:
Explanation of each of the decision rules for clinical laboratories
Scoring criteria for ―fully met,‖ ―partially met,‖ ―not met,‖ and ―not applicable‖ logic based
on the surveyor’s(s’) scoring guidelines

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
90
The survey team leader or designee will select one or two of the surveyor’s(s’) observations
that were reported at the daily debriefing to use as examples to illustrate how the findings
would be scored based on the scoring guidelines.
The survey team leader or designee will provide education on developing a postsurvey SIP
to address compliance issues identified in the ―not met‖ findings in the survey report.
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
91
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
92

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
93

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
94

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
95

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
96

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
97
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
98
Staff Qualifications and Education Session
PURPOSE
The objective of this interview is to address the clinical laboratory’s processes to recruit,
orient, educate, and evaluate all clinical laboratory staff. In addition, the interview addresses
the clinical laboratory’s process to evaluate the credentials of the medical and other health
care professional staff and their ability to provide clinical services consistent with their
qualifications.
LOCATION
Small meeting rooms at the discretion of the clinical laboratory’s leaders
CLINICAL LABORATORY PARTICIPANTS FOR EACH INTERVIEW WHEN HELD
SEPARATELY
The survey team may elect to conduct separate interviews, depending on the number of health care
professional staff present in the laboratory and the number of surveyors. Staff who may be
interviewed are as follows:
Medical staff:
o Elected or appointed senior leader of the medical staff and/or the medical director (if
applicable)
o Representatives of the medical staff involved in credential collection and review
Other health professional staff
o Manager of the human resources/personnel department
o Representatives of the group(s) involved in the orientation, education, and training of
health professional staff
Other clinical laboratory and/or organization staff
o Manager of the human resources/personnel department
o Representatives of the group(s) involved in the orientation, education, and training of
clinical laboratory staff
SURVEYOR(S)
All surveyors

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
99
STANDARDS/ISSUES TO BE ADDRESSED
RSM.1: Provision of resources
RSM.1.1: Personnel policies and procedures
RSM.1.2 : Qualified professionals who direct pathology and clinical laboratory services
RSM.1.3: Training and qualifications of supervisory staff and other leaders
RSM.1.4: Number of qualified staff
RSM.1.5: Orientation to organization of the laboratory and specific job responsibilities
RSM.1.6: In-service or other education and training required to maintain and improve competence
RSM.1.7: Competence assessments
RSM.2: Documented personnel information

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
100
DOCUMENTS/MATERIALS NEEDED
Policies and procedures related to human resources/personnel management, staff
credentials, and staff orientation and education
A sample of laboratory personnel files and health care practitioner staff credential files
A sample of medical staff files
The surveyor(s) will provide instructions on the first day of the survey, generally during the
document review session, regarding this interview and the preparation of the files for review. The
survey team will provide the director of human resources with a list that identifies the type and
number of personnel and medical staff files selected for review later in the survey during the staff
qualifications and education interview. Sample request and review forms are shown on the next few
pages. The survey team will provide copies of the current survey tool on the first day of the survey.
It is important to know that the tools used by the surveyor(s) throughout the survey may change at
any time to continually improve the survey team’s abilities to score the laboratory’s compliance with
standards fairly and accurately. The tool merely reflects current JCI standards.
HOW TO PREPARE
The laboratory should include a list of all current personnel and medical staff in the document
review session on the first day. The list should identify each staff member’s specific discipline, hire
date, and department or service assigned (for example: Medical Director; Hired 20 July 2001;
Pathology). These documents should be in English, when possible.
The laboratory should closely review all personnel and credential files using the Competency
Assessment Process Review Form on page 71. Laboratories should ensure that all required elements
are in the files.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
101
Health Care Professional Staff
Competency Assessment Process Review Form

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
102
Name or
Category of
Staff
Date
of
Hire
Job qualifications
applicable to
services provided
and in accordance
with law and
regulations
RSM.1.4
QCP.2.2
All new employees
are oriented to the
area where they are
assigned and to
specific job
responsibilities
RSM.1.5
In-service education
and training are
provided, specifically
for occasions identified
in a) through e) of the
intent statement
RSM.1.6
Verification
of
education,
training, and
experience
RSM.2
QCP.2.2
Record of
appropriate personnel
information required
by standard, including
license and
certification, when
applicable.
RSM.2
Ongoing
competence
assessment
RSM.1.7
QCP.2.3

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
103
Leadership Conference
PURPOSE
The purpose of the leadership conference is to assess communication among senior leaders of the
laboratory and the organization and how they address organizational performance issues.
LOCATION
At the discretion of the clinical laboratory’s leaders
CLINICAL LABORATORY PARTICIPANTS
Chief executive officer
Chief operating officer, when applicable
Chairman, governing body, or similar representative
Medical director, when applicable
Quality improvement coordinator
Other senior leaders, at the discretion of the clinical laboratory
To foster an interactive process, a large group is not recommended for this conference.
SURVEYOR(S)
All surveyor(s)
STANDARDS/ISSUES TO BE ADDRESSED
Collaborative involvement of the senior leaders of the clinical laboratory and the organization in
governing, managing, and directing the laboratory will be evaluated. The following standards will be
addressed:
Laboratory planning, laboratory services, and resource planning (MGT.1 through MGT.1.3)
Responsibility and authority (MGT.2 through MGT.2.2)
Communication and coordination (MGT.3 through MGT.3.2)
Quality management and improvement processes (MGT.4 through MGT.4.1.4)
DOCUMENTS/MATERIALS NEEDED
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
104
No documents are required to be made available during the leadership conference. However, during
the document review session, the surveyor(s) may have reviewed the following documents in
preparation for the leadership conference:
Organizational chart
Mission statement
Budget and resource allocation
Strategic planning documents
Staffing plans
Information management plan
Quality management plan
Worksheet of applicable laws and regulations
WHAT WILL OCCUR
The surveyor(s) will ask questions related to leadership activities and the decisions that have been
made as well as clarify any leadership issues identified during the survey. Everyone present should
participate in answering the questions. This is designed to be an interactive session.
The surveyor(s) will assess compliance with certain standards identified in the Management and
Leadership (MGT) chapter and with the Standards/Issues To Be Addressed in this section on page
72. During the leadership conference, the surveyor(s) will also identify issues that he or she will
pursue in later survey activities.
HOW TO PREPARE
Clinical laboratories should identify the participants in the leadership conference. Although leaders
should be familiar with all the standards, the clinical laboratory’s leaders should read closely the
standards identified in the Management and Leadership (MGT) chapter and the Standards/Issues To
Be Addressed in this section on page 72 prior to survey. In preparation for this session, it would be
useful to turn the standards into questions. Mock discussions could then be conducted with
participants, so they feel more comfortable with possible questions.
The following are a few sample questions:

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
105
RSM.1: Please explain the process you, as leaders, use to determine the resources needed to
support the operation of the laboratory.
MGT.2: How do you evaluate the effectiveness of the laboratory leadership?
MGT.4: What is a recent example of how laboratory leaders have supported and promoted the
quality management and patient safety improvement program?
MGT.1.2.1: How do you monitor the services offered by an outside organization with which you
have a contract to provide services?

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
106
Surveyor Team Meeting
PURPOSE
For surveys being conducted by more than one surveyor, scheduled team meetings provide an
opportunity for surveyors to share information and observations, plan for upcoming survey
activities, and plan for communication and coordination with the laboratory and/or organization.
When only one surveyor is present, this time is an opportunity to plan upcoming survey activities,
including the selection of additional tracers.
LOCATION
Surveyor headquarters
CLINICAL LABORATORY PARTICIPANTS
None
SURVEYOR(S)
All surveyors
WHAT WILL OCCUR
For surveys lasting more than one day, a 30-minute session is scheduled at the end of each day to
allow the surveyor(s) an opportunity to debrief and to plan for subsequent survey days and activities.
Surveys lasting longer than two days will include an additional 30-minute session before or after
lunch to allow for midday activity planning and observation sharing. During these sessions the
surveyor(s) will do the following:
Identify areas that have been visited during tracer activity
Coordinate locations, services, and other areas that will be visited during continuing
tracer activities
Share observations on the laboratory’s performance
Identify key findings that have surfaced
Ask other surveyors to follow up on potential issues
Identify issues/areas that all surveyors should be exploring during individual patient
and system tracers

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
107
When surveyors are in different locations at the times scheduled for team meetings, they may request
assistance from the laboratory and/or organization to facilitate communication among the members
of the team (such as ensuring availability of a speaker phone or a phone with conference call
capability).

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
108
Surveyor Report Preparation
PURPOSE
The surveyor(s) will use this time to compile, analyze, and organize the data he or she has collected
throughout the survey into a report reflecting the clinical laboratory’s compliance with standards.
LOCATION
Designated surveyor conference room with a computer that has an Internet connection and a printer
provided for the use of the surveyor(s) on each day of the survey
CLINICAL LABORATORY PARTICIPANTS
None
SURVEYOR(S)
All surveyors
WHAT WILL OCCUR
This time is reserved on the agenda for the surveyor(s) to review his or her observations and to
determine if there are any findings that reflect issues of standards compliance. The surveyor(s) will
be using his or her laptop computer to prepare the report and to plan for the leadership exit
conference.
The surveyor(s) may ask laboratory and/or organization representatives for additional information
during this session to confirm or disprove a finding. In addition, the surveyor(s) may request that the
laboratory and/or organization photocopy the report, as needed.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
109
Leadership Exit Conference
PURPOSE
The purpose of this conference is to report the findings of the survey to clinical laboratory
leadership and to resolve any issues of interpretation that may have been identified during the survey.
LOCATION
At the discretion of the laboratory’s and/or organization’s leaders
CLINICAL LABORATORY PARTICIPANTS
Chief executive officer
Chief operating officer
Chairman, governing body, or similar representative
Medical staff leadership
Others, at the discretion of the clinical laboratory’s leaders
SURVEYOR(S)
All surveyor(s)
STANDARDS/ISSUES TO BE ADDRESSED
Survey findings
DOCUMENTS/MATERIALS NEEDED
None
WHAT WILL OCCUR
This session includes the following two components:
1. Discussion with key leaders of the laboratory and/or organization about the survey report and
follow-up process, including review of the SIP. The discussion will cover the following topics:
Purpose of the conference
Summary of compliance findings related to standards
Discussion of any compliance findings for which there are questions or differences of
perspective

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
110
The content of the formal report of findings
The expected follow-up to the survey findings, for example, an SIP or a follow-up focused
survey
2. Formal presentations of an overview of the report to clinical laboratory staff selected at the
discretion of the CEO
The surveyor(s) will provide education to assist the laboratory in developing an SIP based on the
―not met‖ findings from the survey report. The surveyor(s) will explain the survey follow-up process
regarding communication of the accreditation decision by the JCI Accreditation Central Office.
At the discretion of the CEO, a brief conference will be held with other selected staff in the clinical
laboratory to provide an overview of the report and to complete the survey activities.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
111

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
112
Required Quality Monitors
The clinical laboratory chooses clinical and managerial structures, processes, and outcomes that are
most important to monitor based on its mission, patient needs, and services provided. The
laboratory’s leaders identify key measures (indicators) to monitor the clinical laboratory’s clinical and
managerial structures, processes, and outcomes.
Required monitoring includes structure, process, or outcomes data on the following:
MGT.4.2.1 Quality measurement processes selected by the leaders, including aspects of:
a) The laboratory’s safety and infection control programs
b) The laboratory’s quality control programs
c) Pre-analytic processes, including:
Patient preparation
Specimen quality processes (collection, labeling, preservation, transportation, and
rejection)
Completeness of requisitions
d) Post-analytic processes, including:
Efficient transfer of information
Timeliness of reporting test results
Adequacy of documentation
Accuracy of reports
MGT.4.2.2 Managerial measurement includes aspects of the following selected by leaders:
a) The needs, expectations, and satisfaction of individuals and organizations served by the
laboratory
b) The appropriateness of tests offered

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
113
c) Key aspects of the procurement of routinely required supplies and equipment essential to
providing laboratory services
d) Those aspects of laboratory employee expectations and satisfaction selected by the
leaders
e) Those aspects of financial management selected by the leaders
f) Those aspects of the prevention and control of events that jeopardize the safety of
patients, families, and staff selected by the leaders, including the International Patient
Safety Goals
MGT.4.6 Data are analyzed when undesirable trends and variation are evident from the data.
MGT.4.6, ME 2 All confirmed transfusion reactions, if applicable to the laboratory, are analyzed.
MGT.4.9 An ongoing program of identifying and reducing unanticipated adverse events and safety risks
to patients and staff is defined and implemented.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
114
Required Clinical Laboratory Plans
The following standards identify requirements that relate to a written plan. A plan is usually more
comprehensive in content than a policy or procedure. A plan can also be more long-range or strategic in
content. Frequently, a plan also sets priorities for the entire clinical laboratory. For example, the quality
management and improvement plan may address the clinical laboratory’s commitment to quality and
methods for organizing quality improvement efforts. It will also identify short- and long-range priorities and
methods to achieve those priorities.
A select few of these documents need to be in English. Please refer to the list of the documents that
need to be in English on page 39 or the tables on pages 82–105 of this guide. Other documents do
not need to be translated. For non-English documents, the survey team will have one member able
to read the documents, or alternatively, the survey team may request that one or more individuals be
available to describe the contents of the document and answer questions concerning the document.
QUALITY MANAGEMENT AND IMPROVEMENT
Laboratory leaders are responsible for planning, documenting, implementing, and monitoring a
quality management and improvement program. (MGT.4)
Laboratory leaders are involved in defining the program in writing. (MGT.4, ME 2)
MANAGEMENT AND LEADERSHIP
The laboratory’s mission, values, and goals are defined by laboratory leaders. There is a written
document that delineates the mission, values, and goals. (MGT.1, ME 1 and ME 2)
The type and scope of laboratory services provided are defined in a written policy. (MGT.1.1, ME 4)
DEVELOPMENT AND CONTROL OF POLICIES AND PROCEDURES
The requirements for developing and maintaining the laboratory’s policies and procedures are defined in a
written protocol. (DCP.1)
RESOURCE MANAGEMENT
The leaders determine and provide adequate resources to support laboratory services and implement
maintain and improve the quality management and improvement system. (RSM)

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
115
Planning should include the following areas, when appropriate to the facility and the activities of the clinical
laboratory:
1. An adequate number of qualified staff (RSM.1.4)
2. Adequate space, utilities, and equipment (RSM.3)
3. Adequate and reliable utilities and environmental conditions (RSM.3.2)
4. Hazardous materials and waste (RSM.6)
5. Reagents, equipment, and other materials (RSM.4.4)
6. Security of property and occupants (RSM.5)
7. Safety and security (RSM.5.)

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
116
Required Policies and Procedures, Written Documents, Clinical
Laboratory Plans, and Bylaws
The standards in the tables on pages 82–105 identify a requirement for a written document. In some cases,
that document is in the form of a policy and procedure. In other cases, the document is less formal but
addresses the issue identified in the standard. The document that is required is specified in the ―Type of
Documentation‖ column in the tables. In many cases, a number of standards requirements or MEs can be
combined into one policy and procedure. Organizations may find it useful to group all related policies and
procedures. For example, many of the quality control requirements are interconnected and can be contained
in one policy.
The standards in the tables on pages 82–105 also identify a requirement for a written plan. A plan is usually
more comprehensive, has more of a long-range focus, and is more strategic in content than a policy or
procedure. Frequently, a written plan also sets priorities for the entire clinical laboratory. For example, the
quality management and improvement plan may address the clinical laboratory’s commitment to quality and
methods for organizing quality improvement efforts. It will also identify short- and long-range priorities and
methods to achieve those priorities.
The surveyor(s) may not need to review all these documents in detail. It is, however, best to gather all these
documents into one book, or, alternatively, to identify the document by standard number in the traditional
location of the document for easy location.
Note: The specific requirements are addressed in the MEs for each standard; however, additional
details of what should be included in the documents is often found in the intent statement.
Note: Clinical laboratories should refer to the guidelines for document review for detailed suggestions on
the presentation of documents for the surveyor(s).
A select few of these documents need to be in English, and these are indicated in the ―English‖ column in
the tables Please refer to the list of the documents that need to be in English on pages 82–105 of this guide.
Other documents do not need to be translated. For non-English documents, the survey team will have one
member able to read the documents, or alternatively, the survey team may request that one or more

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
117
individuals be available to describe the contents of the document and answer questions concerning the
document.
The ―Page Number‖ column in the tables refers users to the page in the Joint Commission International
Accreditation Standards for Clinical Laboratories, Second Edition, where the standard is discussed.
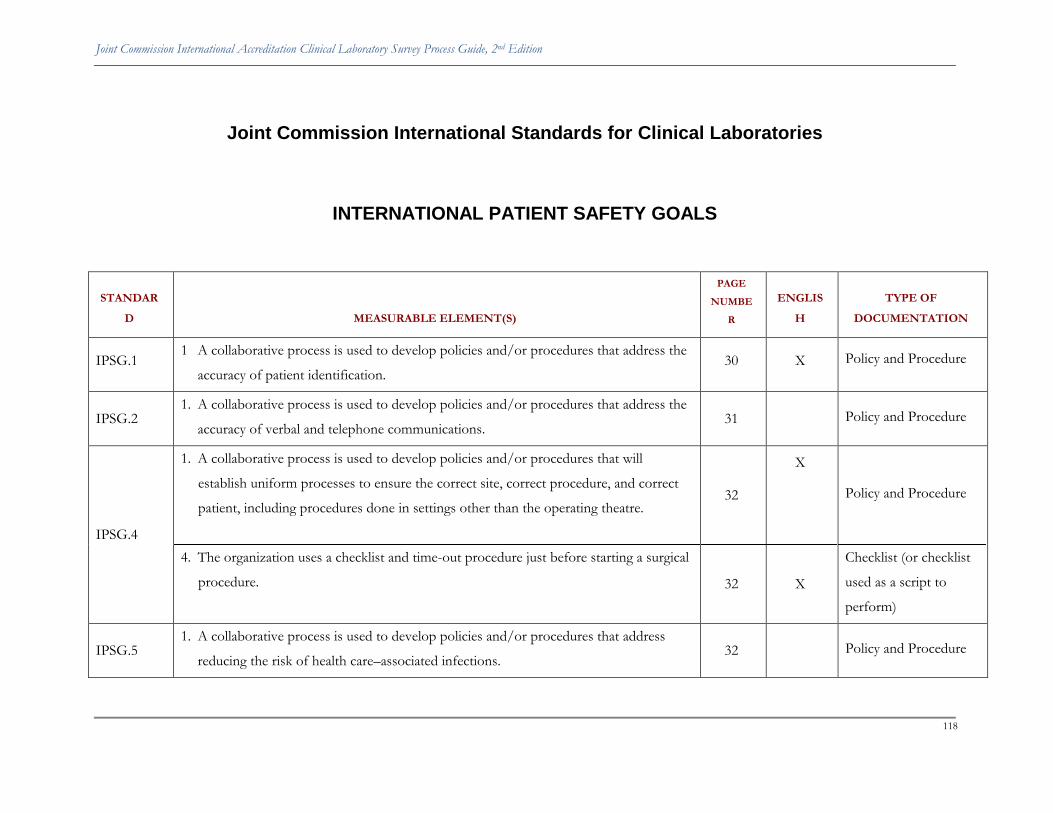
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
118
Joint Commission International Standards for Clinical Laboratories
INTERNATIONAL PATIENT SAFETY GOALS
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
IPSG.1 1 A collaborative process is used to develop policies and/or procedures that address the
accuracy of patient identification. 30 X Policy and Procedure
IPSG.2 1. A collaborative process is used to develop policies and/or procedures that address the
accuracy of verbal and telephone communications. 31 Policy and Procedure
IPSG.4
1. A collaborative process is used to develop policies and/or procedures that will
establish uniform processes to ensure the correct site, correct procedure, and correct
patient, including procedures done in settings other than the operating theatre. 32
X
Policy and Procedure
4. The organization uses a checklist and time-out procedure just before starting a surgical
procedure. 32 X
Checklist (or checklist
used as a script to
perform)
IPSG.5 1. A collaborative process is used to develop policies and/or procedures that address
reducing the risk of health care–associated infections. 32
Policy and Procedure

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
119

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
120
MANAGEMENT AND LEADERSHIP
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
MGT.1 2. The mission, values, and goals are delineated in a written document. 37 X Mission Statement
MGT.1.1 4. The type and scope of laboratory services provided are defined in a written policy. 38 Policy
MGT.1.2
The laboratory director and other leaders define the process for selecting and approving
contract and reference laboratory services, including services that provide blood and
blood products.
38
Document
1. The laboratory director defines in writing the criteria used to select and approve
contract laboratory services. 38
Policy
2. The laboratory director defines in writing the criteria used to select and approve
reference laboratory services. 38
Policy
MGT.1.2.1 1. The laboratory director defines in writing the means used to monitor the accuracy,
availability, appropriateness, and effectiveness of contracted laboratory services. 39
Procedure
MGT.1.2.2 1. The laboratory director defines in writing the means used to monitor the accuracy,
availability, appropriateness, and effectiveness of reference laboratory services. 40
Procedure
MGT.2
Responsibilities for administrative direction and clinical direction of the laboratory are
defined in writing. In addition, other leadership roles are also defined. 41
Document
1. Laboratory directors’ responsibilities are clearly defined in writing. 41 Policy

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
121
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
2. Other leaders’ responsibilities are clearly defined in writing. 41 Policy
4. The organizational structure of the laboratory is defined in writing and/or by diagram. 41 Document
MGT.2.2
The laboratory director is responsible for requiring practices that respect the needs of
patients and other customers. This includes defining and implementing policies that
support patients’ rights to:
a) privacy;
b) security;
c) confidentiality;
d) ask questions or express complaints about their care or services; and
e) effective communication.
42
Policy and Procedure
1. Patients’ privacy and security are provided and supported by policies and practice. 42 Policy
2. The patient’s right to voice complaints about care or services and to have these
complaints reviewed—and, when possible, resolved—is respected and supported by a
written policy, and the policy is implemented.
42
Policy
3. The patient’s right to effective communication is supported by a written policy, and
the policy is implemented. 42
Policy
4. Confidentiality regarding patients and their information is required of all employees in
a written policy, and the policy is implemented. 42
Policy

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
122
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
MGT.3.1 1. Leaders require procedures to address complaints from clinicians who order tests, to
address complaints or questions from patients, and to respect patient rights. 43
Procedure
MGT.3.2
Necessary policies are developed for communicating with clinicians who order tests. The
laboratory has defined policies and implemented practices for these communication
practices, which include the following:
a) There is a protocol for critical test results that indicate an immediate threat to the
patient’s condition.
b) Providing guidelines to practitioners for requesting and receiving test results on an
emergency or STAT basis.
c) A process for notifying clinicians and others responsible for the patient’s care when
incorrect test results have been reported and for correcting the results.
43–44
Policy and Procedure
Protocol
Guidelines
Process
1. There are policies addressing communications with clinicians that include the
following elements:
a) There is a protocol for critical test results that indicate an immediate threat to the
patient’s condition
b) Providing guidelines to practitioners for requesting and receiving test results on
an emergency or STAT basis
c) A process for notifying clinicians and others responsible for the patient’s care
when incorrect test results have been reported and for correcting the results
44
Policy and Procedure
Protocol
Policy and Procedure

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
123
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
MGT.4 2. Laboratory leaders are involved in defining the program in writing. 46 X Policy
MGT.4.1
2. The plan defines the structure, goals, and components of the program. 46 X Policy and Plan
3. The plan describes the methodology used to measure and improve processes and
services. 46
Policy and Plan
MGT.4.1.4
The leaders define performance and quality control activities used to monitor the
laboratory’s processes and the systems used to ensure proper operation and control of
these processes.
47
Document
1. The laboratory director requires and approves written quality criteria for test method
and equipment performance. 48
Criteria
2. The laboratory director requires and approves written criteria for internal quality
control and external quality control (proficiency testing) performance. 48
Criteria
3. The laboratory director requires and approves written quality criteria for specimen
quality. 48
Criteria
4. The laboratory director requires and approves written quality criteria for reporting
results and documenting all verbal reporting of results. 48
Criteria
MGT.4.2 The laboratory’s leaders identify key measures (indicators) to monitor clinical and
managerial structures, processes, and outcomes. 49
Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
124
DEVELOPMENT AND CONTROL OF POLICIES AND PROCEDURES
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
DCP.1
The requirements for developing and maintaining the laboratory’s policies and
procedures are defined in a written protocol. 58
Document
1. There is a defined protocol for policies and procedures that includes the requirements
of the following elements:
a) Initial review and approval of all policies and procedures is performed and
documented by the clinical director of the laboratory. Policies and procedures are
not distributed for use until the approval process is completed.
b) Periodic review of all policies and procedures is performed and documented at a
frequency defined in the protocol, but at least every two years. This review is
performed by the director, an appropriate supervisor, or another knowledgeable
individual.
c) The director or supervisor approves, in writing, all changes in policies and
procedures.
d) All policies and procedures are clearly and legibly written.
e) If manufacturers’ manuals or package inserts are used for technical procedures,
they are enhanced to include specific operational policies (for example, detailed
quality control protocols, calibration procedures, and other laboratory-specific
58
Detailed policy

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
125
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
procedures).
DCP.2
Procedures for ordering tests are defined in writing. 59 Document
1. Policies and procedures describe processes that comply with the following elements:
a) the use of correct request forms
b) the process for identifying patients
c) information required on orders or request forms, to include at least the following:
• Patient’s name
• Patient’s gender
• Patient’s age or date of birth
• Authorized requesting individual, including, as applicable, a contact person to
enable the reporting of imminently life-threatening laboratory results
• The specimen source, when appropriate
• Test(s) or examination(s) requested
• Date and, when relevant, time of specimen collection
• Additional information required to select appropriate tests and to ensure accurate
test interpretation and reporting of results (for example, race/ethnicity, family
history, pedigree)
59
Policy and Procedure
2. The process for confirming oral and telephone requests is defined in writing. 59 Process
3. There is a written description of the process for ordering tests on an emergency basis. 59 Description

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
126
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
DCP.2.1
Policies and procedures are developed to provide step-by-step specimen collection
protocols for each type of specimen submitted to the laboratory. (Also included on
written document list)
59–60
Detailed procedures
and instructions/
Document
DCP.2.2
Policies and procedures are developed to guide how specimens are accessioned and
processed in the laboratory. 60–61
Document
1. Policies and procedures describe how specimens are received by the laboratory, logged
in to the laboratory’s systems, and processed. 61
Detailed procedures
2. The policies describe the specimen accessioning process and how records are
maintained, including the system for maintaining the identity of specimens, aliquots,
and records throughout the time they are in the laboratory.
61
Detailed procedures
DCP.3
The laboratory has current written descriptions and instructions for performing test
methods and procedures. 61–62
Document
1. The laboratory has a current written procedure for each analytic method performed. 62 Detailed procedures

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
127
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
2. The procedure includes the requirements in the following elements:
a) A complete description of reagents and equipment used
b) Any equipment function verification required before testing is performed
c) Specific instructions for verifying method validity through controls or calibrators,
including a definition of acceptable control values and actions to take when control
results are not acceptable
d) The reportable range for patient test results
e) Limitations in methodologies, including interfering substances
f ) A step-by-step description of each phase of patient testing
g) Reference ranges, when applicable
h) Instructions for reporting results
i) Literature references
62
Detailed procedures
DCP.4
The laboratory develops policies, procedures, and controls for the postexamination
processes. 62
Document
2. The defined requirements for the laboratory’s reports, including those from reference
or contract laboratories, include the following elements and are implemented:
b) The report includes the following:
• The name and other identifiers of the patient and the specimen
• The name of the ordering clinician
62
Policy and Procedure

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
128
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
• The tests performed, test results, and units of measurement
• Date and, when relevant, time of specimen collection
• The condition of any unsatisfactory specimen
• Reference values for the tests performed
• Date and time the result is reported
• The identity of the laboratory that performed the test
c) The above elements are also included in reports from reference or contract
laboratories.
d) Reports from reference or contract laboratories are not modified in any way that
would change their meaning.
DCP.4.1
The laboratory has defined a process for immediate notification of the responsible
clinician when specific critical results indicate that the patient’s situation is life-
threatening.
63
Document
1. The laboratory has a written policy defining the laboratory’s critical values and the
process to follow when a test result is critical. 63
Policy
DCP.4.2
The laboratory has defined the process for measuring turnaround times. 63 Document
Intent. The laboratory follows a written process to measure turnaround times for tests.
The process includes a means of ensuring that turnaround times are acceptable. 63
Defined procedure
DCP.4.3 The laboratory has a defined process for correcting reported results. (Also in written 64 Procedure/ Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
129
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
document list)
DCP.5 A written protocol defines the storage and maintenance requirements for records,
including retained specimens, slides, tissues, and blocks. 64
Detailed policy/
Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
130
RESOURCE MANAGEMENT AND LABORATORY ENVIRONMENT
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
RSM.1.1
Personnel policies and procedures are described in writing and are followed. 70 Document
Intent.
a) The desired education, skills, knowledge and other requirements of all staff
members have been described.
b) Each staff member’s responsibilities are defined in a current job description.
c) A policy describes how all staff members are oriented to the organization and the
laboratory.
d) There is a description of the laboratory’s process for staff education and training.
e) The processes for ongoing competence assessment and performance evaluation
are described.
70
Document
1. The following elements are described in written policies and other documents:
a) The desired education, skills, knowledge, and other requirements of all staff
members have been described.
b) Each staff member’s responsibilities are defined in a current job description.
c) A policy describes how all staff members are oriented to the organization and the
laboratory.
d) There is a description of the laboratory’s process for staff education and training.
71
Policy and Procedure
Description
Job descriptions
Policy
Description

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
131
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
e) The processes for ongoing competence assessment and performance evaluation
are described. Process
RSM.1.2 2. The professional education, training, experience, and expertise of the director(s) are
documented. (Also included on written document list) 71
Personnel
record/Document
RSM.1.3 2. Supervisor and management staff qualifications are documented. (Also included on
written document list) 71
Personnel
record/Document
RSM.1.5
2. Participation and successful completion of the orientation is documented, including
approval by the laboratory director or appropriate supervisor that the individual is
competent to perform assigned tasks.
72
Personnel
record/Document
RSM.1.6 2. In-service education and on-the-job training are documented for each staff member.
(Also included on written document list) 73
Personnel
record/Document
RSM.1.7 1. The organization has a laboratory policy that defines the process and criteria for
assessing staff competence. 74
Personnel record

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
132
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
2. Staff members’ performance and competence are assessed annually. 74 Document
RSM.2
Documented personnel information is maintained for each staff member. 74 Document
1. There is documented personnel information for each staff member. 74 Personnel record
2. Documented personnel information includes the following elements:
a) A summary of education and training relevant to duties when hired
b) History of related work experience, including references from previous employers,
if available
c) Primary source verification of certification or licensure, if required by applicable
law and regulation
d) Evidence of certification or licensure, if not required by law and regulation, but if
required by organization policy
e) Current job description
f ) Records of initial orientation and any retraining required
g) Records of any additional training for new job responsibilities
h) Records of continuing education and achievement
i) Records of performance evaluations and periodic assessments of competence
j) Records of health status (as related to work), such as immunization status and
health status after work-related accidents
k) Records of radiation exposure and any monitoring for radiation exposure, when
74
Personnel record

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
133
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
relevant
l) Records of monitoring for exposure to hazardous chemicals, when indicated
m)Records of untoward incident or accident reports, such as accidental needlesticks
RSM.3.2 A plan for providing and maintaining necessary utilities is defined and implemented. 77 Document
RSM.3.2.1
There is a system to inspect, test, and maintain critical operating components for utility
systems and to investigate and correct utility system problems. 77
Document
1. There is a written plan defining the inspection, testing, and maintenance of critical
components for utility systems. 78
Plan
2. The plan includes at least the following elements:
a) periodically testing the emergency generator
b) at least annually checking for polarity and ground integrity on electrical outlet
circuits
c) periodically checking (at least annually) and maintaining for the biological safety
hood
d) periodically checking (at least annually) on the chemical fume hood
e) daily monitoring of temperature-controlled spaces
f ) monitoring of humidity, where indicated.
78
Plan
RSM.4 1. There are defined processes for selecting and using equipment, reagents, and other
supplies. 78
Policy

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
134
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
3. The director has defined performance criteria for test methodologies, equipment, and
quality control. 78
Policy
RSM.4.1
1. There is a defined program for regular monitoring of equipment to demonstrate
proper calibration and function. 79
Procedures /Document
4. All performed verification checks and preventive maintenance are documented. 79 Document
RSM.4.1.1
An historical record is maintained for each analytical instrument and piece of equipment
used by the laboratory. 79
Document
1. There is an historical record for each analytic instrument and piece of equipment. 80 Equipment records
RSM.4.3
There are defined processes in place for validating and maintaining computer software
and information when they are used by the laboratory. 80
Document
1. There is validation of computer software for computers or electronic testing
equipment, prior to use. 81
Procedures
3. Written procedures meet the requirements of the following elements:
c) Procedures are developed for the use of computers and routine maintenance.
d) There are defined procedures to protect data and information against loss,
destruction, tampering, and unauthorized access or use.
e) There is a defined backup procedure to follow a computer is not functioning, so
that laboratory results continue to be reported in a timely manner and data during
81
Procedures

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
135
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
this time are not lost.
RSM.4.4
The laboratory follows written guidelines for the periodic evaluation of all reagents,
including water, to provide for accuracy and precision of results. 81
Document
1. Written guidelines address the requirements that the laboratory has and follows written
guidelines for the periodic evaluation of all reagents, including water, to provide for
accuracy and precision of results.
81
Procedures
2. Reagents, including water, are evaluated according to the requirements of the written
guidelines and the following elements:
b) Reagent performance and adequacy are verified before use.
c) Kits that contain all essential reagents, standards, diluents, and any other reagent
water are evaluated according to an established protocol.
d) Water used in laboratory testing is appropriate for such use.
81
Procedures
RSM.4.5
Laboratory records include documentation of required information for reagents, and
reagents are completely and accurately labeled. 81
Document
1. Records for reagents, controls, kits, and solutions include the identity of the reagent,
the date of receipt or preparation, and the lot number, if available. 82
Records

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
136
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
2. All reagents are labeled with the information required in the following elements:
a) identity;
b) strength;
c) storage requirements;
d) cautionary and accessory information;
e) date prepared or received; and
f ) expiration date
82
Records
RSM.5
There is a plan to ensure that laboratory services and facilities are secure. 82 Document
1. A written plan that describes security measures for laboratory services and facilities is
implemented. 82
Plan
2. The plan addresses security issues for people, property, and equipment, as required in
the following elements:
c) addresses security issues for patients, visitors and other customers, laboratory staff,
and property
d) provides safeguards for equipment (software and hardware), reference materials,
consumables, reagents, and analytic systems
82
Plan
3. The plan provides safeguards for specimens, resources, and laboratory spaces against
unauthorized access. 82
Plan
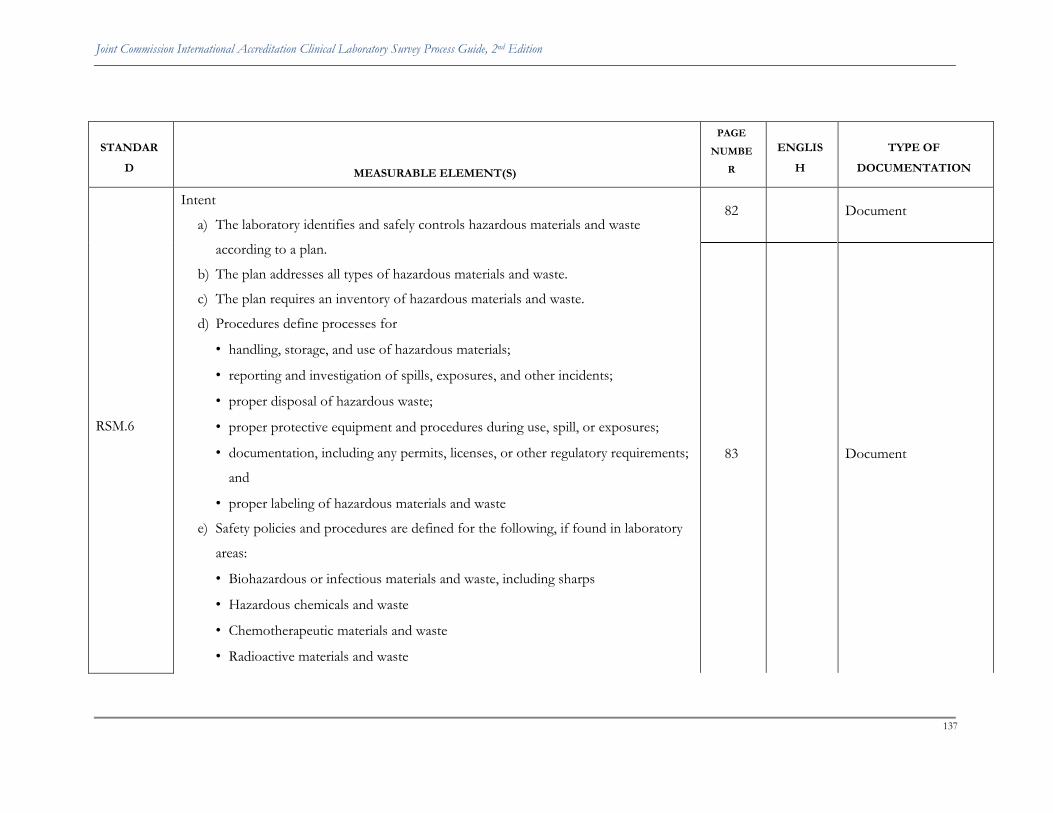
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
137
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
RSM.6
Intent
a) The laboratory identifies and safely controls hazardous materials and waste
according to a plan.
b) The plan addresses all types of hazardous materials and waste.
c) The plan requires an inventory of hazardous materials and waste.
d) Procedures define processes for
• handling, storage, and use of hazardous materials;
• reporting and investigation of spills, exposures, and other incidents;
• proper disposal of hazardous waste;
• proper protective equipment and procedures during use, spill, or exposures;
• documentation, including any permits, licenses, or other regulatory requirements;
and
• proper labeling of hazardous materials and waste
e) Safety policies and procedures are defined for the following, if found in laboratory
areas:
• Biohazardous or infectious materials and waste, including sharps
• Hazardous chemicals and waste
• Chemotherapeutic materials and waste
• Radioactive materials and waste
82
Document
83
Document
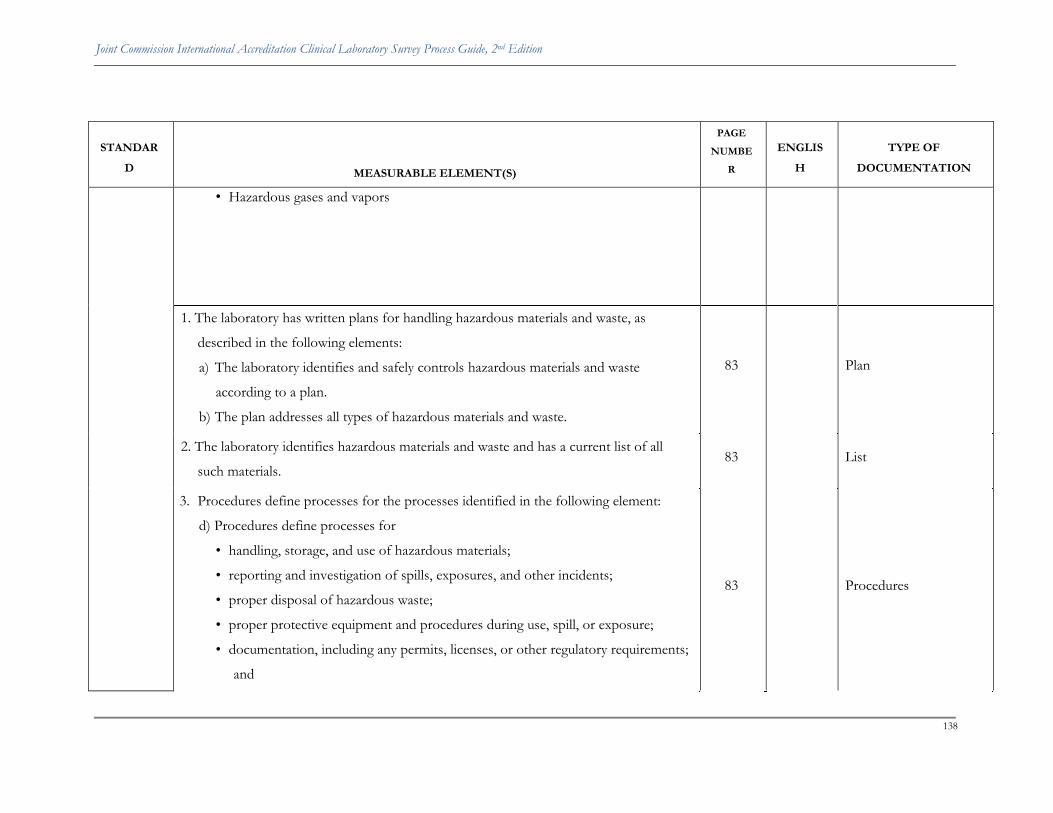
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
138
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
• Hazardous gases and vapors
1. The laboratory has written plans for handling hazardous materials and waste, as
described in the following elements:
a) The laboratory identifies and safely controls hazardous materials and waste
according to a plan.
b) The plan addresses all types of hazardous materials and waste.
83
Plan
2. The laboratory identifies hazardous materials and waste and has a current list of all
such materials. 83
List
3. Procedures define processes for the processes identified in the following element:
d) Procedures define processes for
• handling, storage, and use of hazardous materials;
• reporting and investigation of spills, exposures, and other incidents;
• proper disposal of hazardous waste;
• proper protective equipment and procedures during use, spill, or exposure;
• documentation, including any permits, licenses, or other regulatory requirements;
and
83
Procedures

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
139
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
• proper labeling of hazardous materials and waste.
4. Safety policies and procedures are defined for the types of hazardous materials
identified in the following element:
e) Safety policies and procedures are defined for the following, if found in laboratory
areas:
• Biohazardous or infectious materials and waste, including sharps
• Hazardous chemicals and waste
• Chemotherapeutic materials and waste
• Radioactive materials and waste
• Hazardous gases and vapors
83
Policy and Procedure
RSM.6.1
The laboratory uses a coordinated process to reduce the risks of infection as a result of
exposure to biohazardous materials and waste. 83
Document
1. The laboratory has a defined process for reducing the risks of infection. 84 Process
3. The laboratory follows biosafety rules for relevant practices addressed in the following
elements:
a) Exposures to aerosols and droplets are controlled (for example, when mixing,
sonicating, centrifuging, and flaming inoculating loops).
b) Exposure to needlestick and puncture by other sharps is controlled.
c) Laboratory coats, gowns, or uniforms are worn to protect street clothes and
84
Rules

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
140
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
prevent contamination.
d) Gloves are worn by all personnel who handle potentially infectious specimens,
cultures, or tissues.
e) Personnel are given training on the proper use of personal protective equipment
(for example, gloves, gowns, masks, eye protectors).
f ) Biosafety cabinets are used, when required.
g) Rules govern how to handle laboratory exposure to infectious agents, accidental
cuts, needlestick injuries, accidental ingestion, and contact of potentially infectious
agents with mucus membranes. These rules include decontamination procedures,
whom to contact for emergency treatment, and the location and use of safety
equipment.
h) Rules govern handling, decontamination, and disposal of infectious waste.
i) Appropriate immunizations are defined, as required.
j) There are written procedures defining safe collection, transport, and handling of all
specimens.
k) As part of the plan, there is a safety procedure prohibiting anyone in laboratory
technical areas from eating, drinking, smoking, applying cosmetics, manipulating
contact lenses, and mouth pipetting.
l) When relevant to their jobs, personnel have received training about precautionary
measures, modes of transmission, and prevention of bloodborne pathogens.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
141
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
m) The laboratory has a plan to control exposure to tuberculosis.
RSM.6.2
The laboratory follows defined guidelines for handling and disposing of hazardous
chemicals and waste (including chemotherapeutic materials and waste). 84
Document
1. The program for hazardous chemicals and waste includes the requirements of the
following elements:
a) Guidelines describe the processes for selecting, handling, storing, using, and
disposing of hazardous chemicals and waste from receipt or generation through
use or final disposal.
b) The program includes evaluating each chemical in the laboratory for carcinogenic
potential, reproductive toxicity, and acute toxicity.
84
Program
2. Procedures and containers for handling chemicals meet the requirements described in
the following elements:
c) Handling criteria are defined for each category of hazardous chemical.
d) Containers of hazardous chemicals are labeled with precautionary information
identifying the type and severity of hazard. Examples of types of hazards include
flammable liquids, asphyxiants, corrosives, irritants, and potential carcinogens.
85
Procedures

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
142
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
RSM.6.3
1. When the laboratory stores, uses, or generates radioactive materials and waste, safety
measures and procedures for decontamination are defined and followed, according to
the following elements:
a) There are safety measures for handling radionuclides and radioactive waste.
b) There are procedures for decontamination.
85
Procedures
3. There are procedures for monitoring the amount of radiation in the area. 85 Procedures
RSM.7
1. Laboratory leaders implement a process to evaluate safety issues required in the
following element:
a) Laboratory leaders conduct a risk assessment that proactively evaluates the impact
of buildings, grounds, equipment, occupants, and internal physical systems on
patient and personnel safety.
86
Process/Document
3. Laboratory leaders implement a process for reporting and investigating incidents as
described in the following element:
c) Laboratory leaders report and investigate all incidents of property damage,
occupational illness, and patient, personnel, or visitor injury.
86
Process/Document
4. Laboratory leaders implement safety processes to ensure a safe physical environment. 86 Process/Document
RSM.7.1 Intent. The laboratory’s safety processes provide adequate fire detection and prevention
policies and equipment. 86
Processes

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
143
STANDAR
D MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATION
a) protecting patients, personnel, visitors, and property from fire, smoke, and other
products of combustion;
b) inspecting, testing, and maintaining all required fire alarm systems;
c) inspecting, testing, and maintaining all required automatic fire-extinguishing systems;
d) managing portable fire extinguishers, including monthly inspection, regular
maintenance, and guidelines for their identification, placement, and use; and
e) establishing evacuation routes in case of a fire in the laboratory.
RSM.7.1.1
1. A written policy describes how fire drills are conducted, along with employee roles in
drills and how they will be monitored. 86
Policy/Document
3. Results of drills are reviewed, and actions are taken to improve the laboratory’s
performance, when appropriate. 86
Document
RSM.7.3
Intent. The laboratory’s policies and practices for electron microscopy address the
following elements:
a) precautions related to radiation and the electrical hazards of electron microscopes;
b) pathologist review of embedded tissue sections to effectively select areas for
examination; and
c) reporting of all electron microscopic studies performed for diagnostic purposes in
the clinical record.
87
Policy

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
144
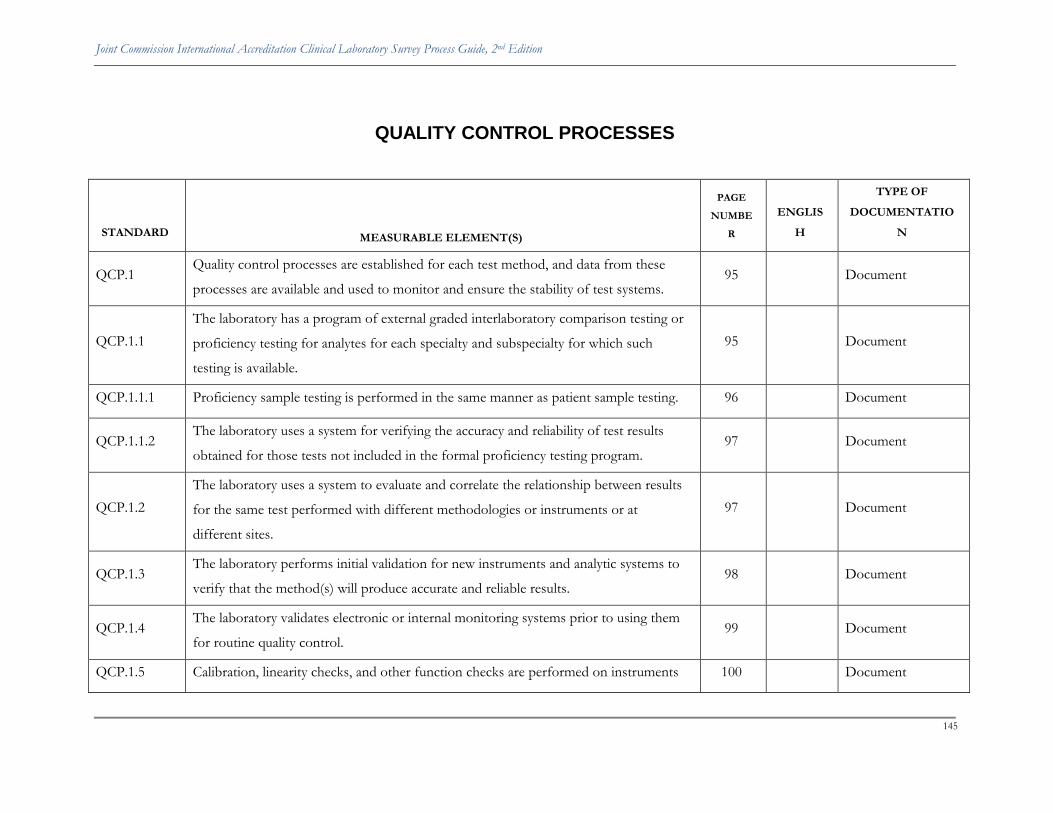
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
145
QUALITY CONTROL PROCESSES
STANDARD MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATIO
N
QCP.1 Quality control processes are established for each test method, and data from these
processes are available and used to monitor and ensure the stability of test systems. 95
Document
QCP.1.1
The laboratory has a program of external graded interlaboratory comparison testing or
proficiency testing for analytes for each specialty and subspecialty for which such
testing is available.
95
Document
QCP.1.1.1 Proficiency sample testing is performed in the same manner as patient sample testing. 96 Document
QCP.1.1.2 The laboratory uses a system for verifying the accuracy and reliability of test results
obtained for those tests not included in the formal proficiency testing program. 97
Document
QCP.1.2
The laboratory uses a system to evaluate and correlate the relationship between results
for the same test performed with different methodologies or instruments or at
different sites.
97
Document
QCP.1.3 The laboratory performs initial validation for new instruments and analytic systems to
verify that the method(s) will produce accurate and reliable results. 98
Document
QCP.1.4 The laboratory validates electronic or internal monitoring systems prior to using them
for routine quality control. 99
Document
QCP.1.5 Calibration, linearity checks, and other function checks are performed on instruments 100 Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
146
STANDARD MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATIO
N
and analytic systems used for patient testing.
QCP.1.6 The quality control processes of the laboratory include a coordinated review of patient
results, quality control results, and instrument function checks. 101
Document
QCP.1.7 The laboratory takes remedial action for deficiencies identified through quality control
measures or authorized inspections and documents such actions. 101
Document
QCP.2 There are quality control processes in place for surgical pathology and autopsy services. 102 Document
QCP.2.1 The laboratory has implemented processes for ensuring the proper identification,
preservation, and documentation of receipt of surgical specimens sent for analysis. 103
Document
QCP.2.1.2 When immunohistochemistry is performed, the laboratory has appropriate quality
control processes. 103
Document
QCP.2.2
The laboratory implements quality control and assurance processes for evaluating the
ongoing qualifications of individuals who perform gross analysis of tissue and
microscopic analysis of tissue.
103
Document
QCP.2.3 There are defined processes to document the ongoing proficiency of individuals who
perform microscopic analysis of tissue. 104
Document
QCP.2.4
The laboratory has implemented processes to ensure access to required patient
information and to crossreference such information to assist in providing a complete
and proper diagnosis.
105
Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
147
STANDARD MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATIO
N
QCP.3 A pathologist or physician qualified in cytology maintains the quality of the
cytopathology service through direct supervision. 105
Document
QCP.3.1 The cytology laboratory has a process to measure, assess, and improve quality. 106 Document
QCP.4 The laboratory leaders have defined quality control processes for all clinical chemistry,
hematology, and coagulation tests. 107
Document
QCP.4.1
For tests that produce quantitative results (such as many clinical chemistry,
hematology, and coagulation analyses), laboratory quality meets certain requirements.
The laboratory defines and follows certain quality control guidelines.
107
Document
QCP.4.2 The laboratory has quality control processes in place for blood film evaluation and
differential counts. 108
Document
QCP.5 The laboratory has quality control processes when performing bacteriology,
mycobacteriology, and mycology. 109
Document
QCP.5.1 Antimicrobial, antimycobacterial, and antifungal susceptibility testing systems are
verified with approved reference organisms. 110
Document
QCP.5.2 All stains are tested with appropriate controls. 110 Document
QCP.5.3 There are adequate quality control procedures when molecular microbiology testing is
performed. 111
Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
148
STANDARD MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATIO
N
QCP.6 If the laboratory is performing parasitology, appropriate reference materials,
equipment, and methods are used. 111
Document
QCP.7 If the laboratory performs tests for identifying viruses, records detailing the systems
used and the reactions observed are maintained. 112
Document
QCP.7.1 The laboratory uses controls that will identify erroneous results in tests for identifying
viruses. 112
Document
QCP.8 The laboratory ensures the quality of tests performed in urinalysis and clinical
microscopy. 113
Document
QCP.9
The laboratory runs serologic tests on unknown specimens, including those for
syphilis, concurrently with a positive control serum of known titer and a negative
control, or controls of graded reactivity, to ensure specificity of antigen reactivity.
113
Document
QCP.9.1 Equipment, glassware, reagents, controls, and techniques for syphilis tests conform to
manufacturers’ specifications. 114
Document
QCP.10 The laboratory uses written quality control procedures that provide diagnostic
reliability and patient and staff safety when it uses in vitro radioisotopes. 114
Document
QCP.10.1 Any laboratory performing in vivo testing uses an appropriate quality control system
for such testing and equipment performance checks. 115
Document
QCP.11 The director of the blood bank or transfusion services is responsible for developing 115 Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
149
STANDARD MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATIO
N
policies and procedures and implementing practices that ensure the safety of patients
being transfused.
QCP.11.1 There are defined procedures and practices for blood donor selection and blood
collection. Staff are trained and assessed as competent to perform these procedures. 116
Document
QCP.11.1.1 A detailed history of a donor is performed prior to selection for blood donation. 116 Document
QCP.11.1.2 An adequate physical examination is performed prior to approving the individual as a
blood donor. 117
Document
QCP.11.1.3 Donor blood is collected safely and aseptically according to a defined protocol. 118 Document
QCP.11.1.4 Written guidelines are implemented when autologous blood is collected. 118 Document
QCP.11.2 Blood and related donor records are properly identified, and the identification is
maintained from collection through the time the unit is transfused. 119
Document
QCP.11.3
Donor blood undergoes routine testing before being used for transfusion. In addition,
process controls are used to ensure appropriate tracking and prevent blood from being
released prematurely.
119
Document
QCP.11.4
When components are prepared or modified by the organization, there are defined
procedures for their processing and storage, and appropriate quality control measures
are taken.
120
Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
150
STANDARD MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATIO
N
QCP.11.4.1 Tests and processes are used to maintain the quality of whole blood. This includes
whole blood from which components and products are to be processed. 121
Document
QCP.11.4.2 Defined processes are implemented to maintain the quality of red blood cells. 121 Document
QCP.11.4.3 Defined processes are used to ensure the quality of platelets. 122 Document
QCP.11.4.4 Defined processes are used to ensure the quality of plasma. 123 Document
QCP.11.4.5 Defined processes are used to ensure the quality of cryoprecipitated AHF. 125 Document
QCP.11.5 The blood bank director ensures that blood and components are stored in a secure and
appropriate fashion in order to prevent damage or deterioration. 126
Document
QCP.11.5.1 Storage areas used for blood and components are appropriate for the volume and
variety of components stored. 126
Document
QCP.11.5.2 Storage areas for blood and components are monitored to ensure that appropriate
temperatures are maintained. 127
Document
QCP.11.6 The laboratory maintains identification and traceability of specimens; reagents; test
results; and blood, blood components, and products. 127
Document
QCP.11.7
The laboratory tests donor blood and recipient blood with potent typing sera and
adequately reactive cells of a known type to determine the correct ABO blood group
and Rh type.
128
Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
151
STANDARD MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATIO
N
QCP.11.7.1 The potency and reliability of reagents used for ABO grouping, Rh typing, antibody
detection, and compatibility determinations are tested for reactivity. 129
Document
QCP.11.8
Before blood is administered, appropriate compatibility testing and antibody testing
(except in an emergency) are performed. In addition, other procedural controls are
implemented.
129
Document
QCP.11.9 Specific procedures are followed when selecting blood and components for
transfusion. 130
Document
QCP.11.10 The director of the blood transfusion services provides policies and procedures to
guide acceptable practices for blood and component transfusion. 131
Document
QCP.11.10.1 There are defined processes for checking blood out of the blood bank before
transfusion. 131
Document
QCP.11.10.2 Specific policies and practices are required before and during blood administration. 132 Document
QCP.11.10.3 The director has defined criteria for recognition of transfusion reactions, as well as
steps to take when symptoms occur. 133
Document
QCP.11.11
When the laboratory draws donor blood, prepares blood components, stores blood
and/or components, and/or issues blood for transfusion, there are specific records
that must be maintained.
134
Document
QCP.12 When performing histocompatibility testing, the laboratory uses appropriate screening 135 Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
152
STANDARD MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATIO
N
techniques for donors and recipients.
QCP.12.1 The laboratory performs mixed lymphocyte cultures or other recognized methods to
detect cellular-defined antigens according to defined methods. 135
Document
QCP.12.2 The laboratory performs HLA serologic typing of both donor and recipient as
appropriate to the study or individual procedure performed. 136
Document
QCP.12.3
Before transplantation is performed, the laboratory crossmatches potential recipients
and donors using the most reactive and recent sera, as appropriate to the study or
individual procedure performed.
137
Document
QCP.12.4 The laboratory uses reagents and antisera that are specific and verified with appropriate
controls when available. 137
Document
QCP.12.5
The laboratory participates in at least one national or regional cell-exchange program, if
available, or develops an exchange system with another laboratory to validate
interlaboratory reproducibility.
138
Document
QCP.12.6 Storage of records and specimens is addressed. 138 Document
QCP.13 Laboratory procedures and practices in cytogenetics provide for accurate results. 139 Document
QCP.13.1 Laboratory records identify the media used, the reactions observed, and the details of
each step of the identification procedure. 139
Document
QCP.13.2 The laboratory obtains and includes in the interpretative report all required clinical 140 Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
153
STANDARD MEASURABLE ELEMENT(S)
PAGE
NUMBE
R
ENGLIS
H
TYPE OF
DOCUMENTATIO
N
information.
QCP.13.3 The laboratory maintains individual sample identification during all phases of testing
and reporting. 140
Document
QCP.14 The laboratory follows written policies and procedures for molecular testing. 141 Document
QCP.14.1 Validation studies include representatives from each specimen type expected to be
tested in the assay and specimens representing the scope of reportable results. 141
Document
QCP.14.2 The laboratory establishes quality control limits, reference ranges, and reportable
ranges. 142
Document
QCP.14.3 The laboratory verifies each test run of patient samples in molecular pathology, using
quality controls. 142
Document
QCP.14.4 Molecular testing reports include specific testing information. 142 Document
QCP.14.5 The laboratory follows written policies and procedures for molecular genetic testing. 143 Document
QCP.14.6 Molecular genetic testing reports include specific testing information. 143 Document

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
154
Standards that Reference Laws and Regulations and Standards of
Practice
The Joint Commission International Accreditation Standards for Clinical Laboratories were designed to be surveyed
in the context of relevant, country-specific local and national laws and regulations. The survey process
takes into account laws and regulations under which a clinical laboratory operates and provides patient
care in one of the following two ways:
1. If a relevant law and/or regulation sets a less stringent expectation than the accreditation standard,
then the expectation of the accreditation standard is surveyed and scored.
2. If, on the other hand, the law and/or regulation sets a more stringent expectation than the
accreditation standard, then the survey team will expect to find that the laboratory is in compliance
with the relevant law and/or regulation.
In addition, it is possible that current standards of practice in a country or region are not identical to those
required by JCI standards but provide equivalent assurance of the quality of the laboratory’s services. The
Law and Regulation Worksheet on pages 107–109 is designed to allow the clinical laboratory to document
when laws and regulations or standards of practice differ with the JCI laboratory standards and to estimate
whether equivalency with each standard has been achieved. Clinical laboratories can use this worksheet to
indicate when there are laws and/or regulations that are in conflict with each other and with a JCI standard.
Clinical laboratory staff should complete this worksheet and provide it to the survey team at the
document review session. The worksheet contains additional space to include other laws and regulations
that may be applicable to the accreditation survey process but that may not be referenced in the JCI
standards.
Clinical laboratories can use the External Auditing Body Recommendation Worksheet on page 110 to
provide information regarding the results of on-site evaluations conducted by a government-authorized
department, a regulatory agency, or an invited evaluator within the past 12 months. An executive
summary (in English) of the outcome of on-site evaluations should be provided to the survey team at the
document review session.

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
155
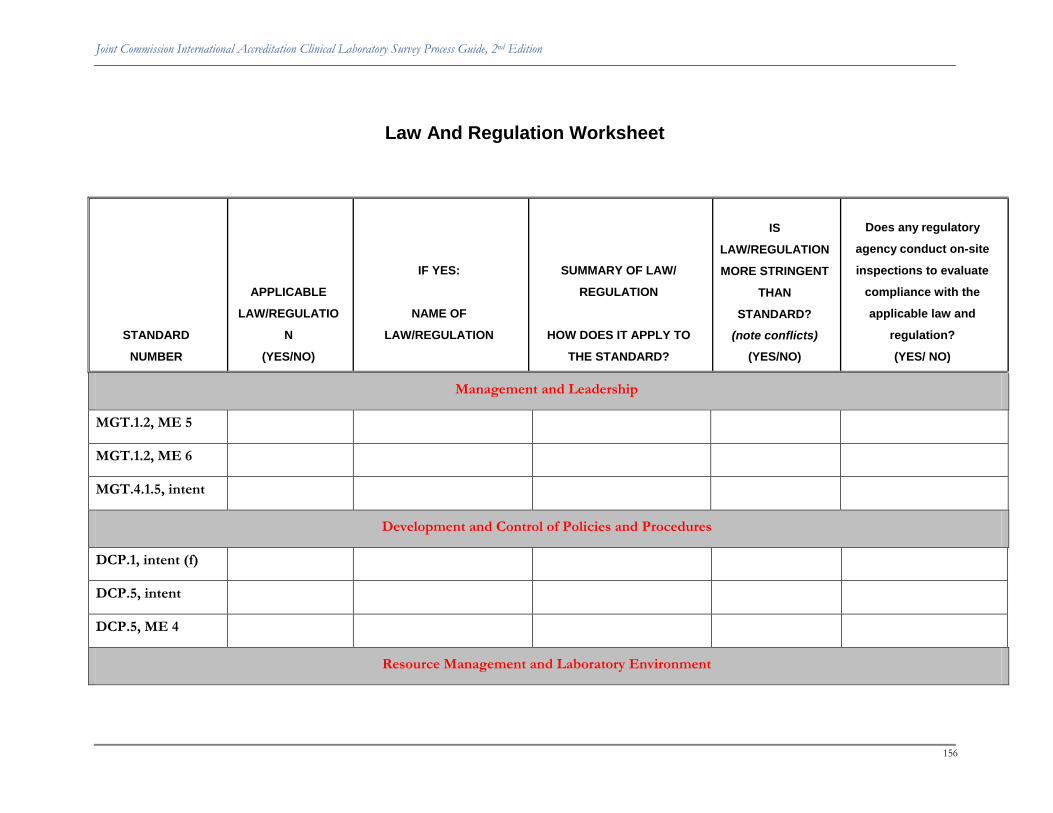
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
156
Law And Regulation Worksheet
STANDARD
NUMBER
APPLICABLE
LAW/REGULATIO
N
(YES/NO)
IF YES:
NAME OF
LAW/REGULATION
SUMMARY OF LAW/
REGULATION
HOW DOES IT APPLY TO
THE STANDARD?
IS
LAW/REGULATION
MORE STRINGENT
THAN
STANDARD?
(note conflicts)
(YES/NO)
Does any regulatory
agency conduct on-site
inspections to evaluate
compliance with the
applicable law and
regulation?
(YES/ NO)
Management and Leadership
MGT.1.2, ME 5
MGT.1.2, ME 6
MGT.4.1.5, intent
Development and Control of Policies and Procedures
DCP.1, intent (f)
DCP.5, intent
DCP.5, ME 4
Resource Management and Laboratory Environment

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
157
RSM.1.2, intent
RSM.1.2, ME 4
RSM.1.3, ME 3
RSM.1.4, intent
RSM.1.4, ME 2
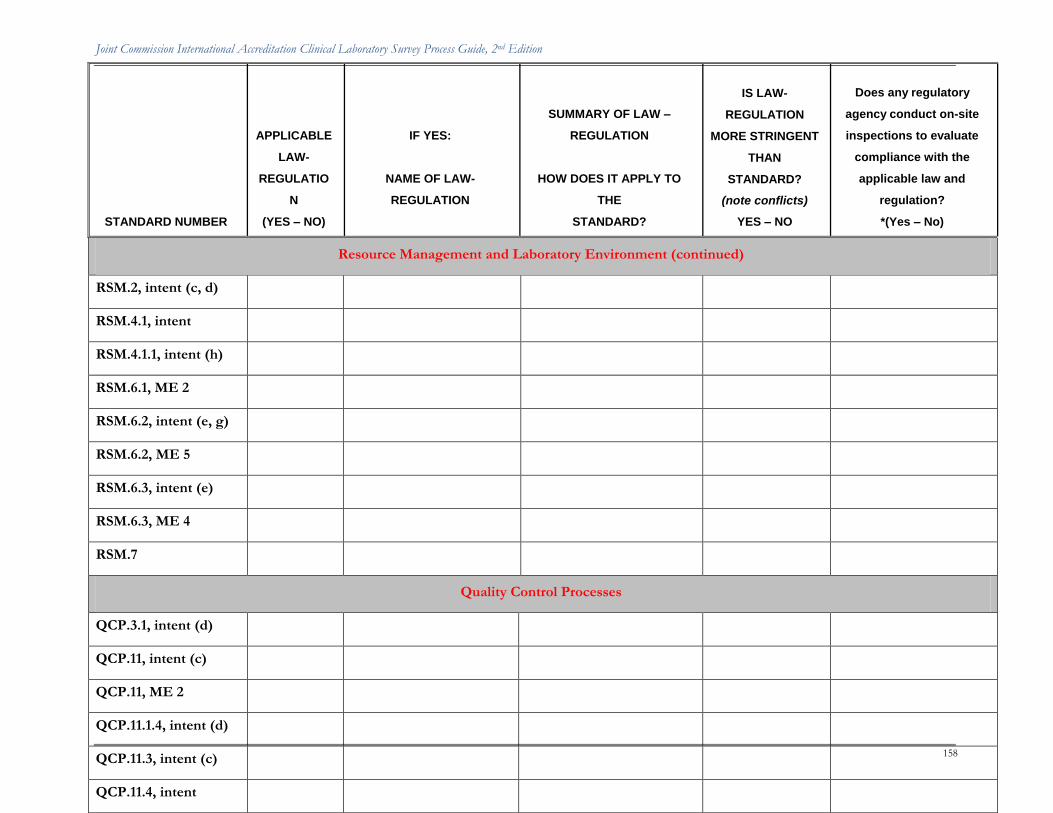
Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
158
STANDARD NUMBER
APPLICABLE
LAW-
REGULATIO
N
(YES – NO)
IF YES:
NAME OF LAW-
REGULATION
SUMMARY OF LAW –
REGULATION
HOW DOES IT APPLY TO
THE
STANDARD?
IS LAW-
REGULATION
MORE STRINGENT
THAN
STANDARD?
(note conflicts)
YES – NO
Does any regulatory
agency conduct on-site
inspections to evaluate
compliance with the
applicable law and
regulation?
*(Yes – No)
Resource Management and Laboratory Environment (continued)
RSM.2, intent (c, d)
RSM.4.1, intent
RSM.4.1.1, intent (h)
RSM.6.1, ME 2
RSM.6.2, intent (e, g)
RSM.6.2, ME 5
RSM.6.3, intent (e)
RSM.6.3, ME 4
RSM.7
Quality Control Processes
QCP.3.1, intent (d)
QCP.11, intent (c)
QCP.11, ME 2
QCP.11.1.4, intent (d)
QCP.11.3, intent (c)
QCP.11.4, intent

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
159
STANDARD NUMBER
APPLICABLE
LAW-
REGULATIO
N
(YES – NO)
IF YES:
NAME OF LAW-
REGULATION
SUMMARY OF LAW –
REGULATION
HOW DOES IT APPLY TO
THE
STANDARD?
IS LAW-
REGULATION
MORE STRINGENT
THAN
STANDARD?
(note conflicts)
YES – NO
Does any regulatory
agency conduct on-site
inspections to evaluate
compliance with the
applicable law and
regulation?
*(Yes – No)
Quality Control Processes (continued)
QCP.11.4, ME 5
QCP.11.4.1, intent (h)
QCP.11.6, intent (h)
QCP.11.6, ME 4
QCP.11.10.3, intent (j)
QCP.11.11, intent
QCP.11.11, ME 4

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
160
External Auditing Body Recommendation Worksheet
If an on-site evaluation was conducted by a government authorized department, regulatory agency, or any other invited evaluator within the past 12
months, please complete and provide this form with an executive summary (in English) of the outcome of each on-site evaluation to the survey team
at the document review session.
Name of the governmental
department, regulatory agency,
or invited evaluator that
conducted the on-site
audit/inspection
Date of the
on-site
audit
Were any
recommend
ations or
citations
noted?
(Yes/No)
If Yes, what
department(s) or
service(s) was identified
in the report (for
example, laboratory,
operating theater,
kitchen, and pharmacy.)
How much time
was allotted to
achieve
compliance (for
example, 90 days,
6 months)
On what
date was full
compliance
was
achieved by
the clinical
laboratory?
Has the
auditor
returned to
validate
compliance?
(Yes/No)

Joint Commission International Accreditation Clinical Laboratory Survey Process Guide, 2nd Edition
161
Name of the governmental
department, regulatory agency,
or invited evaluator that
conducted the on-site
audit/inspection
Date of the
on-site
audit
Were any
recommend
ations or
citations
noted?
(Yes/No)
If Yes, what
department(s) or
service(s) was identified
in the report (for
example, laboratory,
operating theater,
kitchen, and pharmacy.)
How much time
was allotted to
achieve
compliance (for
example, 90 days,
6 months)
On what
date was full
compliance
was
achieved by
the clinical
laboratory?
Has the
auditor
returned to
validate
compliance?
(Yes/No)