jci-dark pp presentation
TRANSCRIPT

© J
oint
Com
mis
sion
Inte
rnat
iona
l
The Value of Accreditation: the JCI Experience
Claudia Jorgenson, RN, MSNDirector, Standards DevelopmentJoint Commission International

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Presentation Topics
Some facts about Joint Commission International (JCI)
Accreditation and Licensure basics
The JCI accreditation process
The drivers for accreditation
Potential return on the investment
Quality, Safety, and Accreditation

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Organizational Base
Joint Commission International (JCI) is the international arm of The Joint Commission (TJC). Established 1997
TJC and JCI are independent, non-profit, non-governmental agencies

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Mission of Joint Commission International To improve the safety and quality of care in the international community through the provision of education, publications, consultation, evaluation, and accreditation services

© J
oint
Com
mis
sion
Inte
rnat
iona
l
International Accreditation and Certification Programs
Hospitals – 5th Edition effective 2014 Laboratories – 2nd Edition (2009) Medical Transport (2002) Ambulatory Care – 2nd Edition (2009) Primary Care (July 2008) Disease-Condition-Service Certification (2009) Home Care – 1st Edition (2012) Long Term Care – 1st Edition (2012)

© J
oint
Com
mis
sion
Inte
rnat
iona
l
6
Mexico
Chile
Costa Rica
Singapore
China
Hong Kong
Taiwan
S. Korea
Indonesia
Saudi Arabia
QatarUAE
Ireland
JCI HeadquartersChicago, USA
JCI Middle East Office
Dubai, UAE
JCI Asia-Pacific OfficeSingapore
Eastern Europe
Belgium
Current JCIA =
56 Countries as 1 July 2013
541 Accredited IHCOs50 CCPC Certificated Programs
2 Accredited Networks
Countries with JCI Accreditations
Mauritius
Russia
Japan
Kazakhstan
Brazil
Nigeria
Egypt
Ethopia

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Accreditation – A Definition
Usually a voluntary process by which a
government or non-government agency grants
recognition to health care institutions which meet
certain standards that require continuous
improvement in structures, processes,
and outcomes.
VoidVoid
VoidVoid
VoidVoid
Vo
SHANGRI-LA HOSPITALEl Dorado, Republic of Freedonia
ampleSample Sample Sample Sample Sample
VoidVoid
VoidVoid
VoidVoid
Vo
SHANGRI-LA HOSPITALEl Dorado, Republic of Freedonia
ampleSample Sample Sample Sample Sample
© J
oint
Com
mis
sion
Inte
rnat
iona
l
Accreditation – A Definition
Accreditation is often confused with:
– Licensure-governmental activity that sets minimum standards to protect the public
– Certification- evaluates special capability or unique skills/ability

© J
oint
Com
mis
sion
Inte
rnat
iona
l
International Structure
International Board of Directors (of JCR)
International Accreditation Committee
International Standards Committee
Regional Advisory Councils
Four International Offices
International translations of many products

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Hospital Standards
Patient-Centered Standards– Access to Care and Continuity of Care– Patient and Family Rights– Assessment of Patients– Care of Patients– Anesthesia and Surgical Care– Medication Management and Use– Patient and Family Education

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Hospital Standards Health Care Organization and Management
Standards– Quality Improvement and Patient Safety– Prevention and Control of Infections– Governance, Leadership, and Direction– Facility Management and Safety– Staff Qualifications and Education– Management of Communication and Information

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Hospital Standards
4th Edition of the Hospital Standards Contains 320 standards Over 1200 criteria measured during the survey/evaluation process
5th Edition of the Hospital Standards (Due in September) 285 Standards 1160 Measurable Elements
Required compliance with the International Patient Safety
Goals

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Evaluation Methodology Teams of peers gather information on-site
Teams trace patients through the organizations
to evaluate systems of care
The compliance elements and scoring method
is transparent
Decisions on accreditation are rule based

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Patient Tracer
Follows the care and needs of the patient

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Drivers for Accreditation
Aging populations with multiple chronic diseases have
raised costs of care
Emergence of new diseases and HAIs
Movement of patients and health care practitioners
across borders
Globalization of service and manufacturing sectors NA
HA

© J
oint
Com
mis
sion
Inte
rnat
iona
l
How safe is healthcare?
Dangerous(>1/1000)
Risky Safe(<1/100K)
Healthcare
Mountain climbing
Bungee jumping
Driving
Chemical industry
Charter flights
Regular air transport
European railways
Nuclear power
Contacts / 1 death
Dea
ths
/ yea
r
1
100,000
1000
100
10
10,000

© J
oint
Com
mis
sion
Inte
rnat
iona
l
“Medicine used to be simple, ineffective and relatively safe. Now it is complex, effective and potentially dangerous.”
Sir Cyril Chantler, former Dean Guy’s, King and St. Thomas’s Medical and Dental School, Lancet1999

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Potential Returns on Accreditation
Improved care – fewer complications
Better reputation -- increased number of new patients
More satisfied staff – better retention and lower
recruitment and training costs
More efficient, cost effective work processes

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Potential Returns on Accreditation
Better preventive maintenance program – longer life of biomedical equipment
Special recognition from payment sources and insurance companies
Greater clarity to leadership structure and quality oversight
Better safety management, risk reduction, and reduced liability exposure

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Questions to Ask
How does accreditation lead to enhancement of patient and staff safety?
– Is it a result of compliance of standards?– Or is it a function of the survey methodology?
Do you have the data to prove what you aretelling us?

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Medication error rate at Indraprasthra Apollo Hospital, Delhi, India
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
45.00
50.00
Jan Feb Mar Aprl May Jun July Aug Sep Oct Nov Dec
05 06 UCL CR
Decreases in Medication Errors

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Trend on Non Compliance of Allergy Documentation at
11.07
6.404.74
1.900.93 0.5 0.3 0 00
2
4
6
8
10
12
No
v-0
6
Dec-0
6
Jan
-07
Feb
-07
Mar-0
7
Ap
r-07
May-0
7
Ju
n-0
7
Ju
l-07
% N
on
co
mp
lian
ce
Desired Outcome
Improvement in Documentation

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Reduction of Complications at American Hospital, Dubai, UAE
During preparation for re-accreditation:– Emphasis on prevention of hospital associated
infections– New Clinical guidelines introduced
0
2
4
6
8
10
12
VAP UTI BSI Post-C/SInfx (%)
20052006
N/1
00 d
evic
e da
ys

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Reduction of Ventilator-Associated Pneumonia
Moving Average - VAP - Year 2005
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
Jan-05 Feb-05 Mar-05 Apr-05 May-05 Jun-05 Jul-05 Aug-05 Sep-05 Oct-05 Nov-05 Dec-05
Month
Rat
e/10
00 v
enti
lato
r d
ays
QIP
ON
VA
P R
ED
UC
TIO
CO
MP
LE
TE
D

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Reduction of Ventilator-Associated Pneumonia
Month wise Hospital Acquired Infection Survelliance Data (VAP)
47.2
33.71
44.12
7.09
9.435.61
000
10.75
49.2
11.7
43.4
0
10
20
30
40
50
60
Month
VAP (No./1000 days) 43.4 11.7 49.2 47.2 9.43 33.71 44.12 10.75 7.09 0 0 0 5.61
Average 20.17 20.17 20.17 20.17 20.17 20.17 20.17 20.17 20.17 20.17 20.17 20.17 20.17
NNIS 90 percentile 8.9 8.9 8.9 8.9 8.9 8.9 8.9 8.9 8.9 8.9 8.9 8.9 8.9
Dec-05 Jan-06 Feb-06 Mar-06 Apr-06 May-06 Jun-06 Jul-06 Aug-06 Sep-06 Oct-06 Nov-06 Dec-06
*(Number of ventilator-associated pneumonias / Number of ventilator-days) X 1000 ** Source: National Nosocomial Infections Surveillance(NNIS) System Report, October 2004
NNIS

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Incidence of VAP in MSICU - 2000 to Q2 05
25.9
19.617.44
9.129.878.448.82
7.047.62
12.19.669.36
6.13
3.194.81
2.63.864.874.264.58
0
5
10
15
20
25
30
Q3 200
0
Q4 200
0Q1 0
1Q2 0
1Q3 0
1Q4 0
1Q1 0
2Q2 0
2Q3 0
2Q4 0
2Q1 0
3Q2 0
3Q3 0
3Q4 0
3Q1 0
4Q2 0
4Q3 0
4Q4 0
4Q1 0
5Q2 0
5
Per
thou
sand
ven
tilat
or d
ays
Target ________ NNIS ------------
Reduction in VAP Rates –National University Hospital, Singapore

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Reduction of Complications at “Istituto Giannina Gaslini” NI/PICU
27.2
4.92.6
03.6
0.90
5
10
15
20
25
30
2006 2007
******
* Mortality (%) from hosp acq. Infections** Hosp acq. Infections (per 1000 pt days)*** Hosp acq. Pneumonia (per 1000 pt days)
© J
oint
Com
mis
sion
Inte
rnat
iona
l
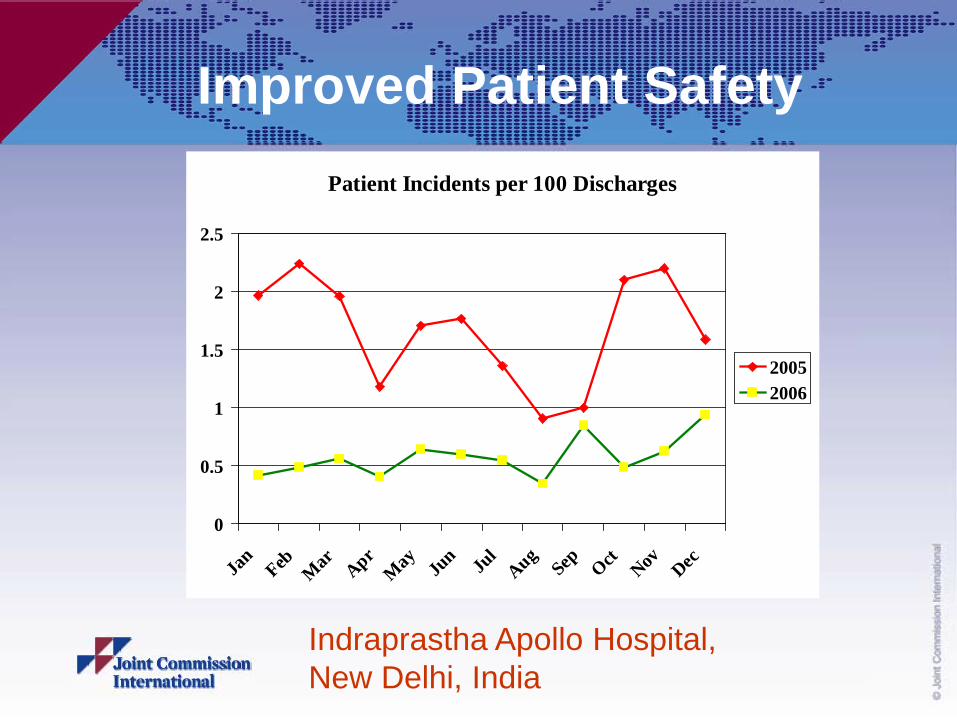
Improved Patient SafetyPatient Incidents per 100 Discharges
0
0.5
1
1.5
2
2.5
Jan
Feb Mar Apr
May Ju
n Jul
AugSep Oct Nov Dec
20052006
Indraprastha Apollo Hospital, New Delhi, India

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Unscheduled Returns to ICU Rates in National University Hospital, Singapore
Comparison With Project-Wide & S'pore Public Hospital Rates
7.956.63
5.67
4.094.63 4.77 4.265.61 5.35
4.684.05 4.54
3.82
3.11
8.09
10.34
7.618.01
4.35
1.47 1.88
3.663.47 3.663.643.50 3.443.39 3.47 3.65 3.57 3.80 3.41
3.99 3.684.23
0.0
2.0
4.0
6.0
8.0
10.0
12.0
Q102 Q202 Q302 Q402 Q103 Q203 Q303 Q403 Q104 Q204 Q304 Q404
NUH S'pore Public Hospitals Project-Wide

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Handwashing Compliance
Trend on Hand Hygiene Compliace Rate in ICUs
77
95 95
68.1
74
40.84
30.26
20.34
45.47
6764.1263.22
95
0
20
40
60
80
100
% Co
mplia
nce R
ate
Compliance 20.34 30.26 45.47 40.84 63.22 64.12 67 74 68.1 77
JCAHO Benchmark 95 95 95 95 95 95 95 95 95 95
38935 38966 38996 39027 39057 39089 39120 39148 39179 39209
JCAHO Benchmark
DesiredOutcome
n=100 n=100 n=250 n=250 n=250 n=250 n=250 n=400 n=400 n=400n = No. of Observations

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Patient Falls (%)
0
5
10
15
20
25
30
35
40
45
2004 2005 2006 2007
Apollo Hospitalstouching lives
INDIA
Indraprastha Apollo Hospital, New Delhi, India

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Laboratory Staff SafetyHospital Clinica Biblica, Costa Rica
171
0 0 0020406080
100120140160180
Q1 Q2 Q3 Q4
Preventable staff accidents 2007

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Needlestick Injuries –Changi General Hospital, Singapore
No. of Needlestick Injury per 1000 CGH Healthcare Workers
0.53
2.80
1.72
0.59
0.001.20
1.17
2.922.88
1.74
2.29
2.85
2.36
5.93
1.192.982.39
2.99
2.36
2.45
3.454.80
2.97
5.96
4.29
6.136.25
2.48
1.871.88
0
2
4
6
8
Jan-0
3
Feb-0
3
Mar-03
Apr-0
3
May-03
Jun-0
3
Jul-0
3Au
g-03
Sep-0
3
Oct-03
Nov-03
Dec-03
Jan-0
4
Feb-0
4
Mar-04
Apr-0
4
May-04
Jun-0
4
Jul-0
4Au
g-04
Sep-0
4
Oct-04
Nov-04
Dec-04
Jan-0
5
Feb-0
5
Mar-05
Apr-0
5
May-05
Jun-0
5
Rate
of Ne
edles
tick I
njury
(CGH) No. of needlestick injury per 1000 CGH healthcare workers
The rate of needlestick injuries per 1000 healthcare workers was reduced from 7.91 in 2003 to 3.48 in 1st 6 months of 2005, an improvement of 127%

© J
oint
Com
mis
sion
Inte
rnat
iona
l
So Far So Good
These are individual reports, dealing with segments of hospital operations – Anecdotal accounts
To study it systematically, – One Middle East hospital embarked on a study of the effect of
the process, not of the outcome, before and after JCI accreditation

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Study Details 400 bed Government Hospital Accredited in 2007 Studied before start of project to comply with JCI standards Repeat study 15 months later (before survey) Perceptions of stakeholders studied by questionnaires 100 point indices
Hassan, DK & Kanji, GK: Measuring Quality Performance in Healthcare 2007. Kingsham Press, Chichester, UK

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Findings of Study All stakeholder groups reported improvement in every dimension measured Overall improvement: 49% over baseline
Main Areas of ImprovementLeadership & managementQuality improvementPatient safetyPt satisfaction & “delight”Ethical performanceDocumentationOrganizational learningOrganizational excellence
Areas of Lesser ImprovementCorporate structureHuman resources managementStaff satisfaction

© J
oint
Com
mis
sion
Inte
rnat
iona
l
37
Value Study in JordanObjective and Study Design
To quantify the value (expressed in monetary terms) and impact (expressed in physical terms) of implementing selected JCI standards
Retrospective
3-year period
Compare two groups of acute general hospitals– Accredited group consisted of 3 private hospitals that received
JCI accreditation in 2007 or 2008
– Non-accredited consisted of 2 similar private hospitals (not obtained nor sought accreditation during that time)

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Results
Net impact of hospital accreditation, 2006-2008
0.6%
27.6%
0.9%
13.0%
1.6%
30.1%
-0.1%-3.0%-0.1%-0.1% -2.5%-0.1%1.1%
-1.8%
-16.0%
0.0%-1.0%-0.5%
-20%
-10%
0%
10%
20%
30%
40%
Readmission to
hospital within 30
days
Return to ICUw
ithin 24 hours^
Return tosurgery w
ithin 24hours
Staff turnoverper year^
Admission of
internationalpatients
Completeness of
medical records^
Accredited hospitals+
Control hospitals (trend)+
Net impact of accreditation+
+ Variable is the change from the before year (2006) to the average of after accreditation years (2007-8). The greatest negative changes are best for hospital readmission, return to surgery, and return to ICU. The greatest positive changes are best for completeness of records and admission of international patients.^Statistically significant (at p<0.05)
© J
oint
Com
mis
sion
Inte
rnat
iona
l
Conclusions
Total saving over two monetary measures US $87,600 per accredited hospital per year
Saving over 2 years follow up equals US $175,200 per hospital
Accreditation demonstrated statistically significant improvement in quality as well as cost saving in key areas
Both accredited and non-accredited hospitals valued study for contribution to staff skills in measuring quality
39

© J
oint
Com
mis
sion
Inte
rnat
iona
l
JCI Standards Address Key IssuesRelevant to Quality, Safety and Satisfaction
Communication Issues (MCI) The organization seeks to reduce physical,
language, cultural, and other barriers to access and delivery of services.
The patient and family are taught in a format and language they understand.

© J
oint
Com
mis
sion
Inte
rnat
iona
l
JCI Standards Address Key IssuesRelevant to Quality, Safety and Satisfaction
Rights as Patients (PFR) Care is considerate and respectful of the patient’s
values and beliefs.
Care is respectful of the patient’s need for privacy.
Patient information is confidential.
Patient informed consent is obtained.

© J
oint
Com
mis
sion
Inte
rnat
iona
l
JCI Standards Address Key IssuesRelevant to Quality, Safety and Satisfaction
Continuity of Care (ACC) Continuity and coordination are evident throughout
all phases of patient care.
Referrals outside the organization are to specific individuals and agencies in the patient’s home community.
A copy of the discharge summary is provided to the practitioner responsible for the patient’s continuing or follow-up care.
© J
oint
Com
mis
sion
Inte
rnat
iona
l
JCI Standards Address Key IssuesRelevant to Quality, Safety and Satisfaction
Truth in admission policies (ACC) Patients are admitted for care only if the
organization can provide the necessary services and settings for care.
At admission patients and families are provided information on the proposed care, expected results of care, and expected costs.
The organization has established and implemented a framework for ethical management.

© J
oint
Com
mis
sion
Inte
rnat
iona
l
JCI Standards Address Key IssuesRelevant to Quality, Safety and Satisfaction
Professional Competence (SQE) The organization has an effective process to
authorize all medical staff members to admit and treat patients and provide other clinical services consistent with their qualifications.
The credentials of medical staff members are reevaluated at least every three years to determine their qualifications to continue to provide patient care services in the organization.

© J
oint
Com
mis
sion
Inte
rnat
iona
l
JCI Standards Address Key IssuesRelevant to Quality, Safety, and Satisfaction
Evidence of quality (QPS) The organization monitors its clinical and
managerial structures, processes, and outcomes including:Laboratory and radiation safety and qualitySurgical proceduresUse of antibiotics and other medicationsUse of blood and blood products’InfectionsAnd 13 other areas including patient safety

© J
oint
Com
mis
sion
Inte
rnat
iona
l
JCI Standards Address Key IssuesRelevant to Quality, Safety and Satisfaction
Complaints (PFR)
The organization informs patients and families about its process to receive and act on complaints, conflicts, and differences of opinion about patient care.

© J
oint
Com
mis
sion
Inte
rnat
iona
l
Conclusions
There are many drivers for quality evaluation however, patient safety is one of the strongest
The accreditation process is an investment in the long-term health of an organization
The accreditation process can provide cost savings in key areas as well as improve the quality and safety in an organization

© J
oint
Com
mis
sion
Inte
rnat
iona
l
48
Questions?