japer 2 master slide deck 11-18 - aamc.org · tradução vai aparecer nesta caixa em um atraso de...
TRANSCRIPT

11/24/2015
1
© 2015 AAMC. May not be reproduced without permission.
Housekeeping If you experience any technical or audio issues
during the webinar, please send a note through the Chat panel to AAMC Meetings.
Se você tiver qualquer problema técnico ou de áudio durante o webinar, por favor, enviar uma nota através do painel de bate-papo para Reuniões AAMC.
Translations will appear in the Chat panel during the presentations. Translations will be on a 2-3 minute delay. Traduções aparece no painel de bate-papo durante as apresentações. Traduções estará em um atraso de 2-3 minutos.
Type your questions in the ‘Q&A’ box at the bottom right of your screen and send to “All Participants.”
Escreva suas perguntas na "Q&A" caixa no canto inferior direito da tela e enviar para "Todos os Participantes."
Translation will appear in this box on a 2-3 minute delay. /Tradução vai aparecer nesta caixa em um atraso de 2-3 minutos.
All Participants
Type your questions here. / Escreva suas perguntas aqui.
© 2015 AAMC. May not be reproduced without permission.
Housekeeping - Audio
• You will hear the audio through your computer speakers. Make sure your computer speakers are on and the sound is turned up.
• If you still have no sound once the webinar starts, click on the audio broadcast icon located in the Participants Panel on the right.
• Você vai ouvir o áudio através dos altifalantes do computador. Certifique-se os alto-falantes do computador estiverem ligados eo som está ligado.
• Se você ainda não tem som uma vez que o webinar é iniciado, clique no ícone de transmissão de áudio localizado no “Painel de Participantes” na direita.

11/24/2015
2
November 18, 2015
October 26, 2015
JAPER Webinar Series
on Racial and Ethnic Disparities in Health (Part II) /
sobre Disparidades Raciais e Étnicas em Saúde (Parte II)
Webinar Agenda
Welcome&IntroductionsBoas‐vindas eIntroduções
MalikaFairJulioDicent‐Taillepierre
English
OpeningRemarksObservações deAbertura
LiaMariaDosSantos Portuguese
Presentation/Apresentação #1 AnnaCoates English
Presentation/Apresentação #2 EdnaMariadeAraujo Portuguese
Presentation/Apresentação #3 MalikaFair English
Presentation/Apresentação #4 RuebenWarren English
Presentation/Apresentação #5 LizaCorso English
ClosingRemarksConsiderações Finais
JoaquinMolina Portuguese

11/24/2015
3
© 2015 AAMC. May not be reproduced without permission.
A Note About Translations• Please note that the webinar will not have simultaneous translation. As
in the first webinar, the presentations made today will alternate between English and Portuguese. Translations of the presentations will be made available, whenever possible, via the Chat box. However, where it has been provided, translations of the slide content have been made available on the slides themselves. A summary of the oral presentations will be viewable during the individual presentations in the Chat box on the right of your monitor screen. Given the limited time available, questions will only be taken in writing, and the responses posted after the webinar recording is released.
• Por favor, note que o webinar não terá tradução simultânea. Como no primeiro webinar, as apresentações feitas hoje irá alternar entre Inglês e Português. Traduções das apresentações serão disponibilizadas, sempre que possível, através da caixa de Chat. No entanto, desde que tenha sido fornecida, as traduções do conteúdo dos slides foram disponibilizados nos próprios slides. Um resumo das apresentações orais serão visíveis durante as apresentações individuais na caixa de bate-papo no lado deixou da tela do seu monitor. Dado o tempo limitado disponível, perguntas só poderão ser tomadas por escrito, e as respostas postadas depois que a gravação do webinar é liberado.
Lia Maria Dos Santos
Gender & Race Policies Specialist, Pan American Health Organization (PAHO)
Brazilian Ministry of Health’s technical team for the Health of the Black Population

11/24/2015
4
© 2015 AAMC. May not be reproduced without permission.
A Note About Translations• Please note that the webinar will not have simultaneous translation. As
in the first webinar, the presentations made today will alternate between English and Portuguese. Translations of the presentations will be made available, whenever possible, via the Chat box. However, where it has been provided, translations of the slide content have been made available on the slides themselves. A summary of the oral presentations will be viewable during the individual presentations in the Chat box on the right of your monitor screen. Given the limited time available, questions will only be taken in writing, and the responses posted after the webinar recording is released.
• Por favor, note que o webinar não terá tradução simultânea. Como no primeiro webinar, as apresentações feitas hoje irá alternar entre Inglês e Português. Traduções das apresentações serão disponibilizadas, sempre que possível, através da caixa de Chat. No entanto, desde que tenha sido fornecida, as traduções do conteúdo dos slides foram disponibilizados nos próprios slides. Um resumo das apresentações orais serão visíveis durante as apresentações individuais na caixa de bate-papo no lado deixou da tela do seu monitor. Dado o tempo limitado disponível, perguntas só poderão ser tomadas por escrito, e as respostas postadas depois que a gravação do webinar é liberado.
PAHO’SAPPROACHTOETHNICITYANDHEALTHINTHEAMERICAS
AnnaCoatesChief,Gender andCulturalDiversity
11/24/2015
5
ABORDAGEMDEOPASPARAETNIAESAÚDENASAMÉRICAS
AnnaCoatesChefe,GeneroeDiversidade Cultural
10
1. Health Disparities in the Americas
2. Ethnicity and Health in PAHO:
o Framework and mandates
o Addressing ethnicity in the Universal Health;
o Towards a strategy: challenges and priority areas foraction
o Examples of interventions
5. Future opportunities
Contents

11/24/2015
6
11
1. Desigualdades étnicas na saúde nas Américas
2. Etnia e Saúde em OPAS:
• Quadro regulamentar e mandatos
• A abordagem de etnia no contexto de saúdeuniversal;
• Rumo a uma estratégia: desafios e linhas de ação
• Exemplos de intervenções
3. Oportunidades de frente
Conteúdo
12
Ethnic Health Disparities in the Americas
• Exclusion/discrimination:o Higher levels of (income and multidimensional) poverty :
o Chile (4.3 times); Ecuador (3.4 times); Paraguay (2.6 times)o Unmet Basic Needs: 70% higher amongst indigenous populations and
30% amongst afrodescent populations
o Lower levels of education:o Brazil and Colombia: school enrollment rates amongsts indigenous
boys and girls lower than amongst non‐indigenous (70% ofindigenous adolescents from 12‐ 17 years of age)
o Affect lifetime opportunities including those related tohealth

11/24/2015
7
13
Desigualdades étnicas na saúdenas Américas
• Exclusão / discriminação:• Níveis mais elevados de pobreza (monetária e
multidimensional):• Chile (4,3 vezes); Equador (3,4 vezes); Paraguai (2,6 vezes)• Necessidades básicas insatisfeitas: 70% mais elevados em
comunidades indígenas e 30% em afrodescendientes
• Níveis mais baixos em educação:• Brasil e Colômbia: percentagem de escolarização de crianças
indígenas menores de não‐indígenas (70% dos adolescentesindígenas de 12 a 17 anos)
• Afetam as oportunidades ao longo da vida, incluindo arelacionada com a saúde
14
Ethnic Health Disparities in the Americas (cont’d.)
• Health disparities:o Higher child mortality rates: Panama: 3 times higher in indigenous
population / Brazil 1.5 times higher in the African descent populationo Disparities in causes of death: assault, infections, parasiteso TB mainly affects indigenous populations, especially meno U.S.:
o 29% higher rates of cardiovascular disease and 40% higher ratesof stroke among African Americans than amongst whites;
o Twice the risk of diabetes mellitus among African Americanso Higher disability prevalence among African Americans and
Native Americans/Alaskan nativeso African Americans and Hispanics more often report poor health

11/24/2015
8
15
Desigualdades étnicas na saúdenas Américas (contd.)
• Iniquidades em saúde:• Níveis mais elevados de mortalidade infantil: No Panamá 3 vezes a
população do resto da população / No Brasil 1,5 vezes a populaçãoafrodescendiente
• As desigualdades na mortalidade provoca: agressões; infecções eparasitas
• TB acomete principalmente a população indígena• UE:
• Mortalidade por doença cardiovascular e 29% maior acidentevascular cerebral 40% maior entre os ascendência Africano do queos brancos;
• Dobrar o risco de diabetes entre os afro‐americanos• Maior prevalência de incapacidade funcional entre Africano‐
americanos e índios americanos / nativos do Alasca• Os afro‐americanos e hispânicos relatados com maior frequência de
problemas de saúde geral
16
Ethnic Health Disparities in the Americas (cont’d.)
• Intersection with other inequalities::• Territorial / rural poverty:• 50.4% of indigenous population and 19% of Afrodescent population live in
rural areas• Poverty rate in rural areas in region only fell from 60% to 53% between
1980 and 2010
• Gender inequalities:• Access to work / schooling: lower for Afrodescendent women (15‐29);• Greater unmet needs for family planning among indigenous women;• Less access to birth control and professional delivery care for
indigenous and Afrodescent women;
• U.S.: increased risk of cervical cancer and breast cancer for African
American women

11/24/2015
9
17
Desigualdades étnicas na saúdenas Américas (contd.)
• Intersecção com outras desigualdades:
• Territorial / pobreza rural:• 50,4% da população indígena e 19% da população afrodescendiente
vive em áreas rurais• A taxa de pobreza em áreas rurais na região caiu por apenas 60 a
53% entre 1980 e 2010
• As desigualdades de gênero:• Trabalho de acesso/escolaridade: menor para a mulher Africana (15‐29);• Maior necessidade não atendida de planejamento familiar entre
as mulheres indígenas;• Menos acesso a controle de natalidade e assistência ao parto
profissional para as mulheres indígenas e africanas;• UE: aumento do risco para as mulheres afrodescendiente de câncer
cervical e de mama
18
PAHO’s normative framework:
‐ The Health of Indigenous Peoples in the Americas (SAPIA)CD37.R5 (1993); CD40.R6 (1997); CD.47.R18 (2006)
‐ Health and Human Rights (2010): CD 50/12 y CD50.R8;
‐ Strategy for Universal Access to Health and UniversalHealth Coverage (CD.53 / 5, CD53.R14) (CD.53/5,CD53.R14)
PAHO’s Normative Framework on Health and Ethnicity

11/24/2015
10
19
Quadro regulamentar da OPAS:
‐ Saúde dos Povos Indígenas das Américas (SAPIA) CD37.R5(1993); CD40.R6 (1997); CD.47.R18 (2006)
‐ Saúde e Direitos Humanos (2010) e CD50.R8 CD 50/12;
‐ Estrategia de Acesso Universal à Saúde e CoberturaUniversal de Saúde (CD.53 / 5, CD53.R14)
Quadro regulamentar de OPAS em etnicidade e saúde
20
Addressing Ethnicity and Health
Ethnicity:
o Social determinant of health: Requires targeted approachto different groups to ensure and monitor universal accessand coverage (equitable inclusion and well being for all);
o Specific cultural barriers to health: Requires interculturalapproaches to ensure access to integral, appropriate, timelyand quality health services

11/24/2015
11
21
Abordagem Etnia e Saúde
Etnia:
o Determinante social da saúde: requer abordagem focadaem diferentes grupos e avaliar a garantir o acesso universale cobertura (inclusão igual e bem‐estar de todos);
o Barreiras culturais específicos para a saúde: Requer umaabordagem intercultural, para que todos ter acessoadequada, cuidados de saúde abrangente oportuna,qualidade.
22
• Gaps in access and coverage amongst and Afro‐descendantsindigenous populations:o Development and implementation of policies and programs
addressing the needs of different groups from rights perspective(people‐centered policies and integral well being);
o Policies and programs that seek to reach groups not traditionallycontemplated
o Intercultural approaches: Promotion of policies and programs thatincorporate ancestral and traditional medicine in national healthsystems
o Social participation and strategic alliances
o Creation and development of capacity at all levels
Towards a PAHO Strategy onEthnicity and Health

11/24/2015
12
23
• Lacunas no acesso e cobertura da saúde dos povos indígenase afro:• Concepção e implementação de políticas e programas que atendam
às necessidades dos diferentes grupos a partir da perspectiva dosdireitos (políticas centradas nas pessoas e bem‐estar global);
• Políticas e programas que visam alcançar grupos nãotradicionalmente coberta
• A abordagem intercultural: Promoção de políticas / programas emedicina tradicional ancestral nos sistemas nacionais
• Participação social e alianças estratégicas
• Criação e desenvolvimento de capacidades a todos os níveis
Rumo a uma Estratégia para a OPAS em Etnia e Saúde
24
Towards a PAHO strategy on Ethnicity and Health (cont’d.)
• Social determinants of health:o Incorporate and unify existing realities in the design of
policies and programs that aim at universal access andcoverage ;
o Intersectoral actions to address determinants in orderto reduce gaps
o Lack of information:o Improved data collection and analysis by countries to
formulate, monitor and evaluate policies

11/24/2015
13
25
Rumo a uma estratégia para a OPAS Em Etnia e Saúde (contd.)
• Determinantes sociais que afetam a saúde:• Incorporar e unificar as realidades existentes na
concepção de políticas e programas que visam acobertura eo acesso universal;
• Ações intersetoriais para abordar os determinantespara reduzir as disparidades
• Falta de informação:• Produção e melhor recolha de dados e análise por
parte dos países para formular, acompanhar eavaliar as políticas
• Tuberculosis: interventions incorporating focus on ethnicity, with indigenous and afro‐descendant populations
• Mental Health and Ethnicity (suicide and indigenous populations)
• Disaster Risk Reduction and Indigenous populations
Selected Example Interventions

11/24/2015
14
• Tuberculose: intervenções com abordagem da população indígenas (tri‐nacional) e população afrodescendiente
• Saúde mental e etnia (suicídio e povos indígenas)
• Redução do risco de desastres e povos indígenas
Algumas intervenções
28
• Universal Access and Coverage: Advances in the countries
• Opportunities of positioning ethnicity in the 2013 Development agenda:
o Health and Well Being for All (Goal 3)
o Reduce inequality within and among countries (Goal 10)
o Data disaggregation: Key to the formulation, implementation and monitoring of policies (Goal 17)
o Three axis: equality, universality, and social inclusion
Reflections and Opportunities
11/24/2015
15
29
• Acesso e Cobertura Universal: Progressos nos países
• Etnia oportunidade para posicionar na implementação da agenda de desenvolvimento pós‐2015:
o Saúde e bem‐estar para todos (Meta 3)
o Reduzir as desigualdades dentro e entre países (Meta 10)
o Desagregação de dados: Chave na política (ODS, Goal 17)
o Os três pilares: igualdade, universalidade e inclusão social
Reflexões e oportunidades
Thank YouAgradecimentos

11/24/2015
16
© 2015 AAMC. May not be reproduced without permission.
A Note About Translations• Please note that the webinar will not have simultaneous translation. As
in the first webinar, the presentations made today will alternate between English and Portuguese. Translations of the presentations will be made available, whenever possible, via the Chat box. However, where it has been provided, translations of the slide content have been made available on the slides themselves. A summary of the oral presentations will be viewable during the individual presentations in the Chat box on the right of your monitor screen. Given the limited time available, questions will only be taken in writing, and the responses posted after the webinar recording is released.
• Por favor, note que o webinar não terá tradução simultânea. Como no primeiro webinar, as apresentações feitas hoje irá alternar entre Inglês e Português. Traduções das apresentações serão disponibilizadas, sempre que possível, através da caixa de Chat. No entanto, desde que tenha sido fornecida, as traduções do conteúdo dos slides foram disponibilizados nos próprios slides. Um resumo das apresentações orais serão visíveis durante as apresentações individuais na caixa de bate-papo no lado deixou da tela do seu monitor. Dado o tempo limitado disponível, perguntas só poderão ser tomadas por escrito, e as respostas postadas depois que a gravação do webinar é liberado.
Edna Maria de Araujo
Professor, Department of HealthState University of Feira de Santana (UEFS)
Member of the Municipal Technical CommitteeState and National Health of the Black Population

11/24/2015
17
© 2015 AAMC. May not be reproduced without permission.
A Note About Translations• Please note that the webinar will not have simultaneous translation. As
in the first webinar, the presentations made today will alternate between English and Portuguese. Translations of the presentations will be made available, whenever possible, via the Chat box. However, where it has been provided, translations of the slide content have been made available on the slides themselves. A summary of the oral presentations will be viewable during the individual presentations in the Chat box on the right of your monitor screen. Given the limited time available, questions will only be taken in writing, and the responses posted after the webinar recording is released.
• Por favor, note que o webinar não terá tradução simultânea. Como no primeiro webinar, as apresentações feitas hoje irá alternar entre Inglês e Português. Traduções das apresentações serão disponibilizadas, sempre que possível, através da caixa de Chat. No entanto, desde que tenha sido fornecida, as traduções do conteúdo dos slides foram disponibilizados nos próprios slides. Um resumo das apresentações orais serão visíveis durante as apresentações individuais na caixa de bate-papo no lado deixou da tela do seu monitor. Dado o tempo limitado disponível, perguntas só poderão ser tomadas por escrito, e as respostas postadas depois que a gravação do webinar é liberado.
The Role of Academic Medicine in Building a Public Health Workforce O papel da medicina acadêmica na construção de uma Força de Trabalho em Saúde Pública
Malika Fair, M.D., M.P.H., FACEPDirector, Public Health Initiatives AAMC

11/24/2015
18
How can we develop a workforce that is poised to improve population health?
PhotoCredit:AAMC,America’sMedicalSchoolsandTeachingHospitals:WeAretheFutureofHealthCareInfographic.
Como podemos desenvolver uma força de trabalho que está pronta para melhorar a saúde da população?
Necessary Collaboration in Medicine & Public HealthA colaboração necessária em Medicina e Saúde Pública
Shifting healthcare landscape
More diverse U.S. population
Healthcare expansion
Increasing healthcare expenditures
New payment models
There are opportunities to:
Support unique career interests of students
Develop the health workforce to address community needs
Mudando o paisagem da assistência médica População EUA mais diversa
expansão da assistência médica Aumento das despesas de
saúde Novos modelos de pagamento
Há oportunidades para: Apoiar os interesses exclusivos
de carreira dos estudantes Desenvolver a força de trabalho
de saúde para atender as necessidades da comunidade

11/24/2015
19
Academic Medical Centers: Areas of Impact Centros médicos acadêmicos: Áreas de Impacto
- Acesso
- Competência
- Oportunidade educacional
Academic medical centers can help increase access to care in underserved communities by graduating more health professionals who will serve in those communities.
Access
Core Areas of Impact: AccessÁreas centrais de Impacto: Acesso
Centros médicos acadêmicos podem ajudar a aumentar o acesso aos cuidados em comunidades carentes por se formar mais profissionais de saúde que atuarão nessas comunidades.

11/24/2015
20
How does diversity impact distribution?Como a distribuição é impactado pela diversidade?
Source:XieraliIM,Castillo‐PageL,ConradS,NivetMA.AnalyzingPhysicianWorkforceRacialandEthnicCompositionAssociations:GeographicDistribution(PartII).AnalysisinBrief2014;14(9).AssociationofAmericanMedicalColleges,Washington,DC.

11/24/2015
21
What influences where clinicians practice?O que influi, onde os médicos praticam?
Source:XieraliIM,MaeshiroR,JohnsonS,ArceneauxT,FairMA.PublicHealthandCommunityMedicineInstructionandPhysicianPracticeLocation.AmJPrev Med 2014;47(5S3):S297‐S300).
18.419.6
20.819.9
20.9 21
27.929
31
0
5
10
15
20
25
30
35
Inadequate Appropriate Excessive
Proportion of Physicians Practicing in HPSAsby Perception of Instruction
Did not plan to practice in underserved areas
Did not know if they would practice in underserved areas
Planned to practice in underserved areas
Academic medical centers can provide more educational opportunities and support for students who are underrepresented in the health professions.
Educational Opportunity
Core Areas of Impact: Educational Opportunity Áreas centrais de Impacto: Oportunidade educacional
Centros médicos acadêmicos pode fornecer mais oportunidades educacionais e de apoio para os estudantes que estão sub-representadas nas profissões de saúde.

11/24/2015
22
Academic Medical Centers as Anchor InstitutionsCentros Médicos Acadêmicos como instituições da âncora
Assessing Community
Needs
Strengthening the Health Workforce
Engaging the
Community
Measuring Institutional
Impact
Avaliar as necessidades Envolver a comunidade Medir o impacto O reforço aos profissionaisda comunidade institucional de saúde
The U.S. Education SystemO sistema educacional dos EUA
Majority low income
Academically lagging
Limited support
Source:SouthernEducationFoundation.ANewMajorityResearchBulletin:LowIncomeStudentsNowaMajorityintheNation’sPublicSchools.http://www.southerneducation.org/Our‐Strategies/Research‐and‐Publications/New‐Majority‐Diverse‐Majority‐Report‐Series/A‐New‐Majority‐2015‐Update‐Low‐Income‐Students‐Now
Maioria de baixa renda
Academicamente atrasada
Suporte limitado

11/24/2015
23
STEM Education in Our SchoolsEducação STEM em nossas escolas
Source:NationalMathandScienceInitiative.STEMEducationStatistics.https://www.nms.org/AboutNMSI/TheSTEMCrisis/STEMEducationStatistics.aspx
High school graduates are not ready academically for STEM careers, particularly minority students
44% are ready for college-level math
36% are ready for college-level science
Diplomados do ensino médio não estão prontos academicamente para carreiras STEM, especialmente estudantes de minorias 44% estão prontos para o de nível
universitário de matemática 36% estão prontos para a ciência de
nível universitário
Competence
Academic medical centers can work to ensure their graduates have the background, qualities, and skills needed to provide effective andequitable care.
Core Areas of Impact: Competence Principais áreas de impacto: Competência
Centros médicos acadêmicos podem trabalhar para garantir que seus graduados têm fundo, qualidades e habilidades necessárias para fornecer assistência eficaz e equitativa.

11/24/2015
24
Core Areas of Impact: CompetencePrincipais áreas de impacto: Competência
Race&Ethnicity
Language
CulturalCompetence
PopulationHealth
Perspectives
Patient‐CenteredCare
Competência
Cuidado Centrado no Paciente
Perspectivas de Saúde da População
CompetênciaCultural
Idioma
Raça e Etnia
Training Shift in Medicine Mudança de formação em medicina
Expert-centered
Monolithic
Individualistic
Basic or clinical science
Tactical
Knowledge-centered
Incremental
Status/titles/income
Patient-centered
Diverse
Teamwork/collaboration
Translational
Strategic
Competence-centered
Breakthrough
Ethical fulfillment
Traditional Future-Oriented

11/24/2015
25
AAMC Strategy Map Mapa estratégico do AAMC
AAMC Public Health Initiatives Iniciativas de saúde pública
• AAMC-CDC Cooperative Agreement
Academic Partnerships to Improve
Health
• Health Equity through Alignment, Leadership, and Transforming the Health Workforce
Urban Universities for
HEALTH

11/24/2015
26
Academic Partnerships to Improve HealthParcerias acadêmicas para melhorar a saúde
Established in 2000 to strengthen the collaboration between academic medicine and public health
Four national academic associations
AAMC
AACN
APTR
ASPPH
Fundada em 2000 para reforçar a colaboração entre a medicina acadêmica e saúde pública
Quatro associações académicas nacionais
AAMC-CDC Cooperative Agreement Acordo de cooperação entre AAMC e CDC
Current Initiatives / iniciativas em curso:
AAMC-CDC Public Health Fellowship Program Programa estágio-médico de Políticas Pública em Saúde
AAMC-CDC Webinar Series Programa estágio-médico de Saúde Pública serie de webinars
MedEdPORTAL® Public/Population Health Collection Colecção de Saúde da População/Pública
Population Health Connect listserv Conectar Saúde da População listserv
Public Health Pathways Caminhos de Saúde Pública
Workforce Improvement Projects Projetos de Melhoria da Força de Trabalho

11/24/2015
27
AAMC-CDC Public Health Policy FellowshipPrograma estágio-médico de Políticas Pública em Saúde
Public health policy experiential learning opportunities for early career physicians
Fellows train with CDC policy experts to understand how policies and legislation impact individual and population health at multiple levels
Oportunidades de aprendizagem da políticas públicas de saúde experiencial para os médicos em início de carreira
Os participantes treinar com especialistas em políticas públicas do CDC para entender como as políticas e legislação impacte saúde individual e da população em vários níveis
AAMC-CDC Webinar SeriesPrograma estágio-médico de Saúde Pública serie de webinars

11/24/2015
28
MedEdPORTAL® Public/Population Health CollectionMedEdPORTAL® Colecção de Saúde da População/Pública
Consider submitting your curricular innovation to be included in the MedEdPORTAL®
Public/Population Health Collection
An online searchable database of domestic and international public health training opportunities for:
Pre-Med Students Medical Students
Residents Early Career Physicians
Scientists Allied Health Professionals
Please visit Public Health Pathways at: www.aamc.org/phpathways
Public Health Pathways Caminhos de Saúde Pública
Um banco de dados pesquisável on-line de oportunidades nacionais e internacionais de formação em saúde pública para:

11/24/2015
29
SummerMedical&DentalEducationProgram
LGBTandDSDHealthCareInitiatives
AAMCHealthEquity:AdvancingthroughDiscovery
(AHEAD)
UrbanUniversitiesfor
HEALTH
FactsandFiguresPublications
AAMCHealthEquityResearchVirtualSiteVisit
AAMCHealthEquityResearch
Snapshot
AcademicPartnershipstoImproveHealth
AAMCHotSpotterMinigrant Project
CulturalCompetenceEducation&Training
MCAT2015
AAMCHolisticReviewProject
- Educação Competência Cultural e Formação
- Iniciativas de Saúde LGBT e DSD
Evaluating Cultural Competence Avaliação da competência cultural
Report released in March 2015 Relatório divulgado mar 2015
Curricular strategies and evaluation tools to improve the assessment of cultural competence education Estratégias curriculares e ferramentas de avaliação para melhorar a avaliação da educação de competência cultural
Download at: www.aamc.org/diversity

11/24/2015
30
Improving LGBT & DSD Health Care / Melhoria dos cuidados das LGBTs & DSD
Report released in November 2014 Relatório divulgado em novembro 2014
Roadmap for improving the care of LGBT and other individuals with differences in gender identity, gender expression, and sex developmentRoteiro para a melhoria dos cuidados de LGBT e outros indivíduos com diferenças na identidade de gênero, expressão de gênero e desenvolvimento sexual
Download at: www.aamc.org/axis
Summer Medical and Dental Education Program (SMDEP) Programa de Educação Médica e Odontológica de Verão 22,293 undergraduate students
have participated since 1989
Of the 14,659 MMEP and SMEP participants, 65% applied to MD granting institutions, of that group, 65.8% were accepted
5,496 have graduated from MD granting institutions
Participants who do not go to medical or dental school still pursue health-related degrees, including public health
Source:SummerMedicalandDentalEducationProgram.http://www.smdep.org. MaterialalsoadaptedfromapresentationgivenbyBridgetteHudson,MPA,NormaPoll‐Hunter,PhD,&MarkLopez,PhDforthe2014NAAHPNationalMeeting.
22,293 alunos de graduação têm participado desde 1989 Dos 14.659 MMEP e SMEP participantes, 65% aplicada a
instituições que concedem MD, desse grupo, 65,8% foram aceitas 5496 se formaram em instituições de concessão de MD Os participantes que não vão à escola médica ou odontológica
ainda perseguir graus relacionadas com a saúde, incluindo a saúde pública

11/24/2015
31
MCAT ® is a program of theAssociation of American Medical Colleges
MCAT2015
Psychological,Social,andBiologicalFoundationsofBehavior
www.aamc.org/mcat2015
GHLO offers 1000+ electives; 98 Collaborators in 39 countries.
Check www.aamc.org/ghlo for most updated list.
Orange: Home Institution only. Purple: Host Institution only. Green: Home and Host Institution.
Global Health Learning Opportunities (GHLO®) CollaborativeA network of institutions facilitating international mobility for final-year medical students in clinical, research and global health electives while promoting faculty engagement and innovation towards building global awareness and understanding.
A rede de instituições facilita a mobilidade internacional para estudantes de medicina do último ano na clínica, pesquisa e eletivas de saúde globais, promovendo o envolvimento do corpo docente e da inovação para a construção de consciência global e compreensão.

11/24/2015
32
Contact InformationInformações de Contato
Malika Fair, M.D., M.P.H., FACEPDirector, Public Health Initiatives / Diretor, Iniciativas de Saúde Pública
Phone: (202) 778-4773E-mail: [email protected]: www.aamc.org/publichealth
© 2015 AAMC. May not be reproduced without permission.
A Note About Translations• Please note that the webinar will not have simultaneous translation. As
in the first webinar, the presentations made today will alternate between English and Portuguese. Translations of the presentations will be made available, whenever possible, via the Chat box. However, where it has been provided, translations of the slide content have been made available on the slides themselves. A summary of the oral presentations will be viewable during the individual presentations in the Chat box on the right of your monitor screen. Given the limited time available, questions will only be taken in writing, and the responses posted after the webinar recording is released.
• Por favor, note que o webinar não terá tradução simultânea. Como no primeiro webinar, as apresentações feitas hoje irá alternar entre Inglês e Português. Traduções das apresentações serão disponibilizadas, sempre que possível, através da caixa de Chat. No entanto, desde que tenha sido fornecida, as traduções do conteúdo dos slides foram disponibilizados nos próprios slides. Um resumo das apresentações orais serão visíveis durante as apresentações individuais na caixa de bate-papo no lado deixou da tela do seu monitor. Dado o tempo limitado disponível, perguntas só poderão ser tomadas por escrito, e as respostas postadas depois que a gravação do webinar é liberado.

11/24/2015
33
" P U B L I C H E A L T H E T H I C S "
N O V E M B E R 1 8 , 2 0 1 5
T I M E : 1 0 : 0 0 A M
J A P E R W E B I N A R
R U E B E N C . W A R R E N , D . D . S . , M . P . H . , D R . P . H . , M . D I V.
P R O F E S S O R O F B I O E T H I C S & D I R E C T O R
T H E N A T I O N A L C E N T E R F O R B I O E T H I C S I N R E S E A R C H &
H E A L T H C A R E A T T U S K E G E E U N I V E R S I T Y SANKOFA BIRD
“At the last session of the Tuskegee Negro Conference, some startling facts were brought out concerning the health of the colored people of the United States. Forty-five percent of all deaths among Negroes were preventable; there are 450,000 Negroes seriously ill all the time; the annual cost of this illness is 75 million dollars; that sickness and death cost Negroes annually 100 million dollars.”
“Na última sessão da Conferência Negro Tuskegee, alguns fatos surpreendentes foram trazidos a respeito da saúde das pessoas de cor dos Estados Unidos. Quarenta e cinco por cento de todas as mortes entre os negros eram evitáveis; existem 450.000 negros gravemente doentes o tempo todo; o custo anual desta doença é de 75 milhões de dólares; que a doença ea morte custo negros anualmente 100 milhões de dólares”
Patterson F. Statement concerning national Negro health week. National Negro Health News. April-June 1939;7:13.
NATIONAL NEGRO HEALTH WEEK 1915

11/24/2015
34
There was a continuing disparity in the burden of death and illness experienced by Blacks and other minority Americans as compared with our nation’s population as a whole. That disparity has existed ever since accurate Federal recordkeeping began more than a generation ago and although our health charts do itemize steady gains in the health status of minority Americans, the stubborn disparity remained ---an affront both to our ideals and to the ongoing genius of American medicine.
Houve uma disparidade contínua da carga de morte e doença experimentada por negros e outras minorias americanos, em comparação com a população da nossa nação como um todo. Essa disparidade tem existido desde que registros Federal precisos começou há mais de uma geração atrás e, embora nossas cartas de saúde fazer relacionar ganhos constantes no estado de saúde dos minoritários americanos, a disparidade teimoso permaneceu --- uma afronta tanto aos nossas ideais e ao gênio em curso de medicina americana.
REPORT OF THE SECRETARY’S TASK FORCE ON BLACK & MINORITY HEALTH
• US Department of Health and Human Services. Report of the Secretary’s Task Force on Black and Minority. Washington, DC: US Government Printing Office; 1985.
In a 2005 article on health disparities published in Health Affairs with a team of scientists, David Satcher, the first author and the 16th U.S. Surgeon General, reported that the 60,000 excess deaths documented in the Heckler Report had, in 2002, risen to 83,000. Clearly, reflecting and eliminating health disparities and promoting health are needed if the challenges that Booker T. Washington identified in 1915, or the health disparities chronicled in 1985 in the Report of the Secretary’s Task Force on Black and Minority Health or the increase in excess deaths Satcher et. al, reported in 2005 are to be addressed.
Em um artigo de 2005 sobre as disparidades de saúde publicada no Health Affairs, com uma equipe de cientistas, David Satcher, o primeiro autor e 16 US Surgeon General, relatou que as 60.000 mortes em excesso documentados no relatório Heckler teve, em 2002, subiu para 83.000. Claramente, é necessário reflectir e eliminar as disparidades de saúde e promoção da saúde, se os desafios que Booker T. Washington identificadas em 1915, ou as disparidades de saúde narrados em 1985 no Relatório da Força-Tarefa do secretário em a Saúde dos pretos e as minorias ou o aumento de mortes em excesso Satcher et. al, relatou em 2005 devem ser abordadas.
EXCESS DEATHS AMONG AFRICAN-AMERICANS
• Satcher, D., Fryer, G. E., McCann, J., Troutman, A., Woolf, S. H., & Rust, G. (2005). What if we were equal? A comparison of the black-white mortality gap in 1960 and 2000. Health Affairs, 24(2), 459-464.

11/24/2015
35
The Salient Language
Recommended
To
Address Ethical Issues
O saliente idioma recomendado para tratar as questões éticas
ETHICS
What is Ethics? Set of rules, principles, values, and ideals of a particular group of people.
The systematic study of morals, concepts, and theories, typically in departments of philosophy.
O que é ética? Conjunto de regras, princípios, valores e ideais de um grupo particular de pessoas. O
estudo sistemático da moral, conceitos e teorias, geralmente em departamentos de filosofia.
Bayer, R., & Beauchamp, D. (2007). Public health ethics: Theory, policy, and practice. New York: Oxford University Press.

11/24/2015
36
BIOETHICS
Applied ethics focusing on doctor-patient relationships and how changes in the health care system affect it.
BioéticaÉtica aplicada com foco na relação médico-paciente e como as mudanças no sistema de saúde afetá-lo.
Daniels, N., Kennedy, B. P., & Kawachi, I. (2007). Why justice is good for our health: The social determinants of health.inequalities. In R. Bayer & D. Beauchamp (Eds.), Public health ethics: Theory, policy, and practice. New York: Oxford University Press
PUBLIC HEALTH ETHICS
Public Health Ethics emphasize the ethical problematic related to interests and health of groups, the social justice of the distribution of social resources, and the positive or social rights of individual. The study of public health ethics requires the practitioner to effectively conceptualize and operate between the tension of individual rights and collective interest.
• Ética de Saúde Pública: enfatizar a ética problemática relacionada com os interesses e saúde dos grupos, a justiça social na distribuição dos recursos sociais e os direitos positivos ou sociais de individual. O estudo da ética da saúde pública exige que o praticante de conceituar e operar entre a tensão de direitos individuais e interesse coletivo de forma eficaz.
Bayer R & Beauchamp, DE. Public Health Ethics: Theory, policy and practice. New York: Oxford University Press.
2007.
Bayer R & Beauchamp, DE. Public Health Ethics: Theory, policy and practice. New York: Oxford University Press.
2007.
Callahan, D & Jennings, B. Ethics and Public Health: Forging a Strong Relationship. American Journal of Public
Health 92: 2002, 169-176

11/24/2015
37
HEALTH DISPARITIES (INEQUALITIES)
Systematic, potentially avoidable differences in health—or in the major socially determined influences on health—between groups of people who have different relative positions in social hierarchies according to wealth, power, or prestige.
Disparidades em saúde (Desigualdades) Sistemáticas, diferenças potencialmente evitáveis na saúde - ou nos
principais influências socialmente determinadas na saúde - entre grupos de pessoas que têm diferentes posições relativas na hierarquia social de acordo com a riqueza, poder ou prestígio.
Braveman, P. (2006). Health disparities and health equity: Concepts and measurement. Annual Review of Public Health, 27, 167-194.
HEALTH EQUITY
Ideally, everyone should have a fair opportunity to attain their full health potential and more pragmatically that no one should be disadvantaged from achieving this full potential if it can be avoided.
Idealmente, todos deveriam ter uma oportunidade justa de atingir o seu potencial de saúde completo e de forma mais pragmática que ninguém deve estar em desvantagem de alcançar esse potencial se puder ser evitado.
Braveman, P. (2006). Health disparities and health equity: Concepts and measurement. Annual Review of Public Health, 27, 167-194.

11/24/2015
38
VENN DIAGRAM
Health Disparities
Public Health Ethics
Health Equity
Bioethics
Bioethics Center
as Disparidades de Daúde
Bioética
Equidade em Saúde
Ética de Saúde Pública
Centro de Bioética

11/24/2015
39
© 2015 AAMC. May not be reproduced without permission.
A Note About Translations• Please note that the webinar will not have simultaneous translation. As
in the first webinar, the presentations made today will alternate between English and Portuguese. Translations of the presentations will be made available, whenever possible, via the Chat box. However, where it has been provided, translations of the slide content have been made available on the slides themselves. A summary of the oral presentations will be viewable during the individual presentations in the Chat box on the right of your monitor screen. Given the limited time available, questions will only be taken in writing, and the responses posted after the webinar recording is released.
• Por favor, note que o webinar não terá tradução simultânea. Como no primeiro webinar, as apresentações feitas hoje irá alternar entre Inglês e Português. Traduções das apresentações serão disponibilizadas, sempre que possível, através da caixa de Chat. No entanto, desde que tenha sido fornecida, as traduções do conteúdo dos slides foram disponibilizados nos próprios slides. Um resumo das apresentações orais serão visíveis durante as apresentações individuais na caixa de bate-papo no lado deixou da tela do seu monitor. Dado o tempo limitado disponível, perguntas só poderão ser tomadas por escrito, e as respostas postadas depois que a gravação do webinar é liberado.
Liza CorsoSenior Advisor for Public Health Practice and Accreditation
Division of Public Health Performance Improvement Office for State, Tribal, Local and Territorial Support
National Voluntary Accreditation for Public Health Departments
Centers for Disease Control and Prevention
Office for State, Tribal, Local and Territorial Support
November 2015

11/24/2015
40
National Voluntary Accreditation Program for Public Health Departments
Public Health Accreditation Board (PHAB) National accrediting body for public health departments
Established in 2007
Program launched in September 2011
www.phaboard.org
Co-funded by CDC and the Robert Wood Johnson Foundation
Field driven – guided by practitioner input and testing
Focus on Quality Improvement
The goal of a voluntary national accreditation program is to improve and protect the public’s health by
advancing the quality and performance of state, tribal, local, and territorial public health departments
11/24/2015
41
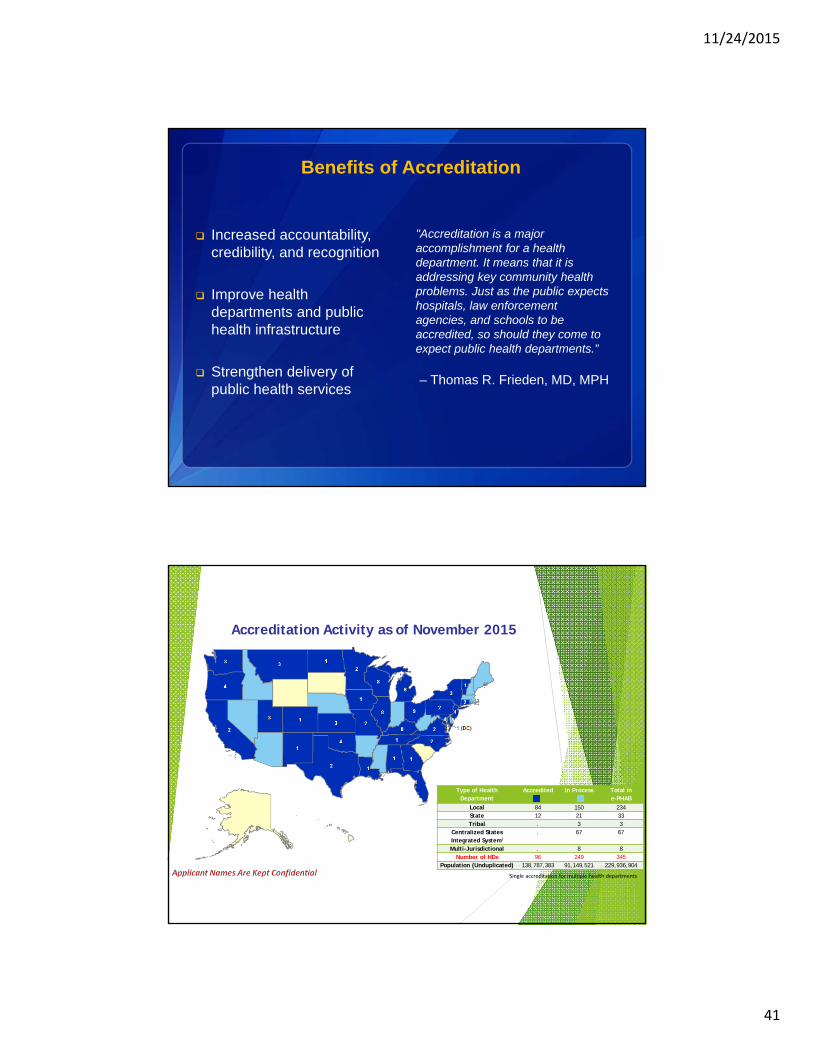
Benefits of Accreditation
Increased accountability, credibility, and recognition
Improve health departments and public health infrastructure
Strengthen delivery of public health services
"Accreditation is a major accomplishment for a health department. It means that it is addressing key community health problems. Just as the public expects hospitals, law enforcement agencies, and schools to be accredited, so should they come to expect public health departments.”
– Thomas R. Frieden, MD, MPH
Type of Health Department
Accredited In Process Total in e-PHAB
Local 84 150 234State 12 21 33Tribal . 3 3
Centralized States Integrated Systemi
. 67 67
Multi-Jurisdictional . 8 8Number of HDs 96 249 345
Population (Unduplicated) 138,787,383 91,149,521 229,936,904
Accreditation Activity as of November 2015
iSingle accreditation for multiple health departments

11/24/2015
42
PHAB Accreditation: Key Elements
Standards and measures across 12 domains: 10 Essential Services, administrative capacity, and
governance
Intended to provide a strong foundation for all public health programs
Accreditation assessment process: External validation through peer reviewers and site visit Annual reporting throughout five-year accreditation status
Technical assistance and support: PHAB CDC and other partners
PHAB Standards - Twelve Domains
1. Assess
2. Investigate
3. Inform and educate
4. Community engagement
5. Policies and plans
6. Public health laws
7. Access to care
8. Workforce
9. Quality Improvement
10. Evidence-based practices
11. Administration and management
12. Governance
11/24/2015
43
Accreditation and Health Equity
Increased focus in Version 1.5 (released 2014)
Numerous standards focus health department attention on health equity and social determinants of health
Examples within standards
Selected Links PHAB
www.phaboard.org
CDC accreditation webpage www.cdc.gov/stltpublichealth/accreditation
Partner accreditation webpages State: http://www.astho.org/Programs/Accreditation-and-Performance/
Local: http://www.naccho.org/topics/infrastructure/accreditation/index.cfm
Tribal: www.nihb.org/public_health/accreditation.php andhttp://redstar1.org/resources/
Journal of Public Health Management and Practice—January/February 2014 Issue on Accreditation (open access) http://journals.lww.com/jphmp/toc/2014/01000

11/24/2015
44
Thank you
Liza Corso
404-498-0313
Office for State, Tribal, Local and Territorial Support
Centers for Disease Control and Prevention
The findings and conclusions in this presentation are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention
© 2015 AAMC. May not be reproduced without permission.
A Note About Translations• Please note that the webinar will not have simultaneous translation. As
in the first webinar, the presentations made today will alternate between English and Portuguese. Translations of the presentations will be made available, whenever possible, via the Chat box. However, where it has been provided, translations of the slide content have been made available on the slides themselves. A summary of the oral presentations will be viewable during the individual presentations in the Chat box on the right of your monitor screen. Given the limited time available, questions will only be taken in writing, and the responses posted after the webinar recording is released.
• Por favor, note que o webinar não terá tradução simultânea. Como no primeiro webinar, as apresentações feitas hoje irá alternar entre Inglês e Português. Traduções das apresentações serão disponibilizadas, sempre que possível, através da caixa de Chat. No entanto, desde que tenha sido fornecida, as traduções do conteúdo dos slides foram disponibilizados nos próprios slides. Um resumo das apresentações orais serão visíveis durante as apresentações individuais na caixa de bate-papo no lado deixou da tela do seu monitor. Dado o tempo limitado disponível, perguntas só poderão ser tomadas por escrito, e as respostas postadas depois que a gravação do webinar é liberado.

11/24/2015
45
Closing Remarks
Joaquin MolinaPAHO Brazil
©