james allen - lead admissions pharmacist - · pdf fileo herbal medicines and homeopathy ......
TRANSCRIPT
Safer Prescribing Workbook SECTION 2
Medication on Admission
James Allen - Lead Admissions Pharmacist
This section will cover the following areas
- Medication History taking o Sources of information o Herbal Medicines and Homeopathy o OTC Medicines
- Managing medicines on admission o Insulins o Anticonvulsants o Renal impairment o Liver impairment o Drug use in pregnancy and breastfeeding o Substance Abuse
a) Opiate abuse b) Alcohol abuse
In a recent audit the average patient is admitted on seven medicines of which two are omitted on admission without a clinical reason. Medication prescribed on admission often continues throughout admission and into primary care. Staffing and bed pressures within NHS trusts mean there is a much faster turnaround of patients. It is therefore conceivable that a chart written on admission could form the basis of a discharge HMR. Minor or major inaccuracies on admission can therefore have a lasting impact on the patient, not only during the inpatient stay but post discharge when the GP records are updated based on the discharge documentation. The overall aim of this section is to provide an understanding of the differing sources of information when undertaking a drug history and their limitations. Prescribing therapy for opiate and alcohol abusers will be covered as will some discussion regarding common areas of error and patients who are at a greater risk of medication errors. Is it important to get the medicines right? (Pirmohamed et al BMJ July 2004)
� 18,820 admissions over 6 month period � 6.5% of admissions related to medicines � 2.3% of those died as a result of the ADR � Accurate medication history required for appropriate management � Accurate data on medicines required at discharge

Medication History Taking The term ‘drug history’ has been adopted to describe the collation of admission medication. In reality the term drug history meant undertaking a lengthy patient centred interview to discuss previous current and previous unsuccessful therapy. This is often not necessary on admission but it is crucial to obtain reliable and robust information regarding current prescribed, herbal and purchased medicines. The aim of this section is to provide an insight into the sources available when documenting an admission medication history. Sources of Information Consider the following information sources: Recent HMR (within 2 weeks) Patient Relative Nursing Home MARS Sheet Patients Own Medication GP Surgery Receptionist GP Printout / Repeat Slip GP Community Pharmacist Specialist Clinic i.e. Clozapine Clinic / Opiate Addiction Treatment Centres Briefly discuss their relative merits and limitations.

As a general rule of thumb an accurate medication history requires at least two sources. It is crucial to ascertain whether the patient is compliant with prescribed medication in order to formulate a safe admission plan. Recent HMR Discharge HMR’s vary greatly in quality and the information provided. They are potentially very helpful if the patient has been readmitted relatively soon after discharge. Discharge medication often takes between one and two weeks to be communicated and updated on the GP records (assuming the patient hasn’t visited their GP with the information). This means recent changes within secondary care can be missed if using GP information as a sole reference source. Remember: A discharge HMR is only going to be 100% accurate if the previous drug history was full and complete. Scepticism should be given to HMR’s not screened by a pharmacist and secretarial typed HMRs often have transcription errors. The patient Within today’s health care system patients are encouraged to become expert patients with detailed knowledge of their disease process and medication. On admission the patient may very well be confused and struggle to recall specific information about medication. Therefore unless the medication regimen is simple and easy for the patient to recall the patient should be considered a useful second line source of information. The majority of patients will recount how they take the medication and whether they were instructed to deviate from the instructions on the repeat or box, however remembering the specifics of dose, name and frequency are often more problematic and as such GP or care home records should be sought as a second source of information. Relative Relatives will often provide a more truthful insight into the way a patient deals with their medication on a daily basis. Frequently they are the first to mention non-compliance with therapy and information the patient believes to be insignificant or embarrassing. It is rare for a relative to be able to offer specifics about dosing regimes unless they deal with the medication on a frequent basis. Nursing Home / MARS Sheet. The Medicine Administration Record Sheet (MARS) used by nursing homes is possibly the most accurate resource available on admission. Assuming it is legible and in its entirety (i.e. not missing pages) this source provides information on dose, route, frequency and crucially compliance. One area of caution is that a number of ‘when required’ medication and some specialist medication may not be documented i.e. analgesia and inhalers. Patients’ Own Medication This is a valuable source of information that can provide clues to previous admissions and how the patient manages their medicines at home. This is also a key area where recently issued medicines from the G.P can be found. These are often not on repeat slips and can often contribute to the admission.

Medication errors issued by community pharmacists are rare but are often spotted when looking through patient’s own medication. Errors of this manner are often the cause of admission or a significant contributory factor. When using patients’ own medication as a source remember to check the labels. Ensure they are labelled for the right patient (not the partner of the patient). Check dates on labels to gather information about compliance and if possible check the patient takes the medication in accordance with the directions, often they deviate due to GP instructions. A range of medicines are often not brought into hospital with the other medicines, these include:
- Eye drops – Often remain in the patient’s fridge - Inhalers - Infrequent medicines i.e. biphosphonates. - Medicines taken at specific times i.e. statins, which are often kept on the
bedside cabinet. Consider specifically asking about these types of medicines when using patient’s own medication as a predominant source of a drug history. A subsection of patients own medication is compliance devices i.e. NOMAD and DOSETTE devices. Identification of patient / relative filled devices is often time consuming and difficult with the number of generic manufacturers. Generally this is a poor source of medication history and further sources should be investigated. Pharmacist filled medication devices come in a range of types. Whilst they do not ensure the patient takes their medication they are a useful resource. Take care with some devices; often they can be poorly labelled and extremely difficult to interpret. Caution should be used if there is evidence of tampering with the future blisters. A number of medication are not stable in compliance devices (i.e. Sodium Valproate) do not assume the trays are the sole source of the patients’ medication. GP Surgery Receptionist GP surgery receptionists are often used as a source of information. They are rarely trained to give this information and pronunciation of medicines can lead to confusion. They often make their own decisions about what is significant and can miss important information. It is generally better to ask for a faxed copy of the recent acute medication and repeat medication. A number of local surgeries prefer this approach and some will only provide information in the form of a fax. GP Printout There has been a recent drive to ensure G.P documentation arrives in hospital with the patient. There are two predominant forms of GP information:
- The repeat printout is simply the form(s) used by the patient to order repeat medication. This often has little information about allergy status, last collection dates or recent acute items.
- The computer records printout. This is often a very useful source detailing allergy status, recent acute items (even records of GP visits) and issue dates for the medication. These systems rely on accurate data entry and require
constant maintenance. Whilst often they are relatively robust many printouts contain very old medications, often ones the patient has stopped taking many years previously.
In the drive towards a more autonomous NHS it is worth mentioning that some patients can get up to 6 months worth of medication on repeat. This system is simply a GP prescription with 6 monthly repeats which the community pharmacist retains and issues every month to the patient. The patient is required to collect on a regular basis or the scheme is suspended, however this may not appear the case on the GP records. This is still relatively rare in Southampton but is becoming more popular with patients and carers. The Patients’ G.P. The patients’ GP is obviously a robust and useful source of medication history. Often the GP will know the patient well and can provide information about compliance and previous failed therapy. Whilst the GP is a robust source it is often not very practical. Usually time constraints force the GP will call back after his / her surgery has finished. This can be very late in the day of admission and postpones the decision regarding therapy to the second day of admission. Community Pharmacist The community pharmacist tends to be a forgotten resource unless a dispensing error has resulted in admission. They can sometimes detail herbal, OTC and repeat medication. Since it is relatively unusual for them to be contacted they are often sceptical and reluctant to provide information that breaches patient confidentiality. The major limitation to the community pharmacist is that the patient can take their prescription to any high street chemist and in such cases the drug history becomes disjointed. They are however useful in confirming information relating to compliance devices especially whether the device contains all the prescribed medicines for an individual patient. Specialist Clinic i.e. Clozapine Clinic / Addiction Treatment Centres There are a number of community treatment services that run independently and supply specialist medicines. The best examples of these include the clozapine clinic run at the Royal South Hants Hospital, anticoagulant clinics and various addiction centres that are discussed in more detail later in the workbook. These centres are run independently and it is often the case that the GP information has no record of these medicines. The medication is often monitored or supplied through other prescribers and as such the GP need not even supply prescriptions and the medication may not be apparent from the repeat slip or GP records. Clozapine is an atypical antipsychotic used for the treatment of refractory schizophrenia. It has a number of side effects and important drug interactions. Clozapine is known to cause pantocytopenia and patients on clozapine require blood tests to monitor blood counts. Initiating and managing clozapine requires specialist dose titration. If therapy is interrupted for more than 48 hours the patient must be re-titrated. It is therefore important to elucidate that the patient takes clozapine early in the patients stay.

These clinics rarely have complete information about the medication a patient may be taking, more commonly they can only supply information about the specialist medication they supply to the patient. Herbal Medicines and Homeopathy The use of herbal medicines has become increasingly popular. The general perception of herbal therapy is that as natural products they have no side effects whilst providing a therapeutic effect similar to conventional therapy. The predominant danger with herbal medicines is that patients rarely consider them medications. It is for this reason they are often missed on admission. Herbal medicines can produce organ dysfunction or interact with prescribed medication. The herbal medicine Kava Kava was banned from the UK market due to reports of serious hepatotoxicity and St Johns Wort has a number of drug interactions most notably oral contraceptives, warfarin, anticonvulsants and other antidepressant therapy. In the context of St Johns Wort sudden withdrawal can often produce a similar withdrawal reaction similar to the withdrawal of an SSRI. This can complicate an admission and prolong the patient stay. Homeopathy is a form of alternative medicine that aims to treat "like with like". Substances that cause symptoms similar to the disease in large quantities are heavily diluted, with shaking at each stage of the dilution. Homeopaths contend that the shaking causes some imprint (or memory) of the diluted substance, despite the fact that at many common homeopathic dilutions, no molecules of the original substance are likely to remain. It is for this reason that it is rare for homeopathic therapy to produce organ dysfunction or interact with conventional therapy unless there has been a mistake in the dilution process. Recent regulations introduced in the UK have tightened the control of herbal medicines. However there can still be variations between the quantities of active substance in the preparations meaning that even if the patient consistently takes the herbal medicine it can have a varied effect, this is most important for herbal medicines that interact with warfarin. The majority of herbal medicines are bought over the counter. This means the patient or is the only viable source of what they are taking. It is worth routinely questioning patients about herbal, homeopathic and other supplements when asking about regular medication. Over the Counter Medicines This term usually encompasses medicines that the patient has access to buy in retail outlets and pharmacies. There is a phenomenal range of medicines that can be bought over the counter often these medicines where originally under the supervision of a community pharmacist but as time progresses they are allowed on the general sale list ensuring they can be bought at almost any high street outlet. High profile examples of medicines that can be bought over the counter include simvastatin, sumatriptan and omeprazole. They are usually in a low dosage form but can still be significant in the context of an admission. Traditional therapy like urinary alkinalisation agents used to treat cystitis can lead to antibiotic therapy failure in patients treated with nitrofurantoin.
It is important to enquire about this form of medication specifically. Patients often consider over the counter medicines as unimportant on admission and will not specifically mention them unless questioned. It is also commonplace for patients who pay prescription charges to buy these medicines over the counter to reduce the overall charge; a good example of this is low dose aspirin.
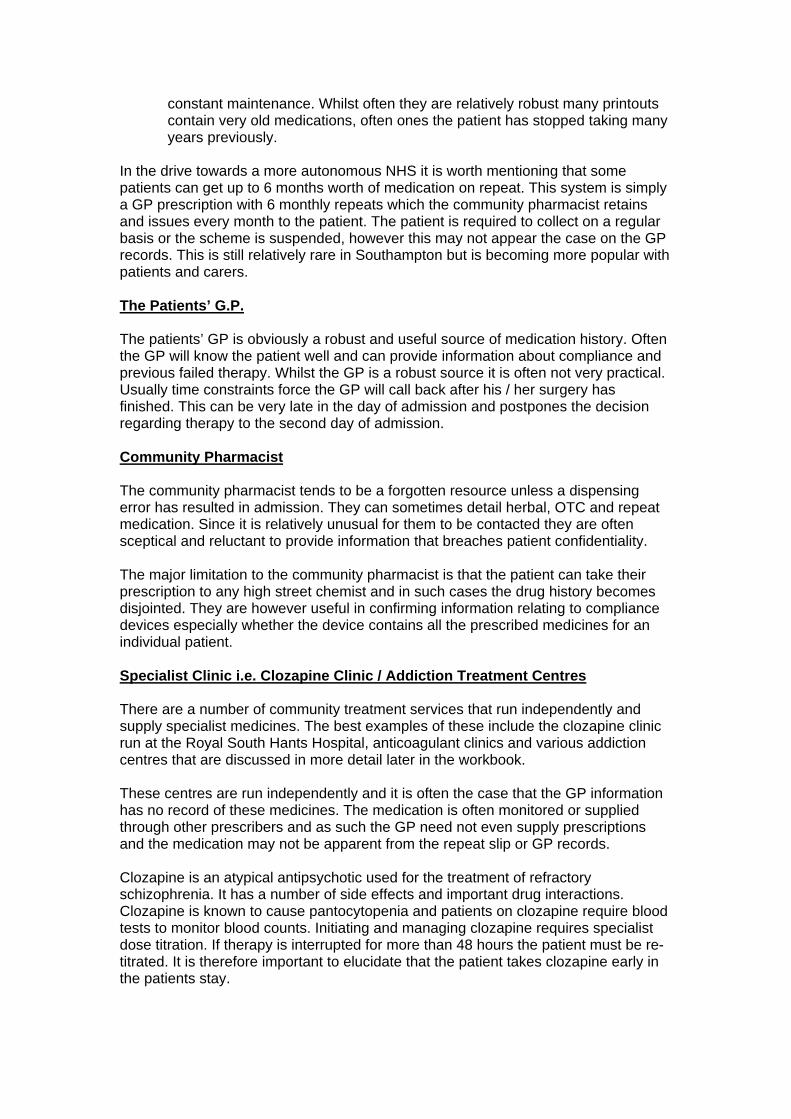
Managing Medicines on Admission The collation of the admission drug history is often only a small part of prescribing on admission. It is also important to identify which medicines could have contributed to the admission and / or require modifying or holding in the acute phase. It is obviously important at this stage to ensure all new medicines prescribed are appropriate taking into account the patients underlying renal and hepatic function. Insulins Consider the following scenario: You are the cover HO and have been called to one of the elderly care wards to assess a patient. It is the patients’ fifth successive hypoglycaemic episode in as many days after his transfer from AMU. The patient states that the problem did not occur on AMU but his own insulin pen has gone missing since the transfer. The nurse is requesting the dose of insulin is amended. The prescription chart is detailed below:
Comment on the possible reasons for this patient’s frequent hypoglycaemic episodes. How would you proceed?
Errors relating to insulins are a large proportion of the serious incidents throughout the hospital. Often these are related to prescribing at inappropriate times and inaccurate prescriptions that don’t detail the type of insulin. Insulins can be categorised as: Short / Rapid Acting Insulins These provide rapid response and short duration of action. There are three predominant types:
o Soluble – Actrapid, Humulin S o Lispro – Humalog o Aspart – Novorapid
The newer aspart and lispro insulins are very rapid acting and their effect can be considered immediate. Soluble insulins like actrapid usually take between 15 – 30min before peak effect is obtained. Intermediate Acting Insulins - Isophanes These provide a 12-hour duration of action with a peak onset of action after approximately 4 hours. The two predominant forms are Insulatard and Humulin I. Long acting Insulins These provide a 24-hour release of insulin with little variation in effect over the 24-hour period. The two available insulins of this nature are glargine and detemir. Biphasic Combination Insulins These are a combination of short / rapid acting insulins with intermediate acting insulins. They are combined in a number of different ratios for example Human Mixtard 30 is equivalent to 30% soluble insulin and 70% isophane insulin. Therefore for example: Human Mixtard 30 = Human Actrapid 30% and Human Insulatard 70% Novorapid 30 = Novorapid 30% and Insulatard 70% Humalog mix 50 = Humalog 50% and Insulatard 50%. It is important to prescribe these preparations denoting the ratio. It is also important to prescribe these bi-phasic insulins at the appropriate times (usually at 9am and 5pm) to ensure peak effect corresponds with meal times. Whilst the majority of patients are currently prescribed human insulin the source of the insulin is extremely important. There are still and number of patients using porcine insulin and to a lesser extent bovine insulin. These patients may still be on these insulins for historical reasons however it is more common for the patients to have been switched to animal derived insulin due to hypoglycaemia with human insulin.

Prescribing Anticonvulsant Therapy on Admission Anticonvulsant therapy often provides complex dosing regimes where the consequences of an error can be very serious. Discussion regarding the regimes and different choices of anticonvulsant is outside the remit of this workbook but consideration should be given on admission to ensure essential therapy is not interrupted. Consider the following scenario Mr KS has been admitted with a CVA. He is a known epileptic but has been well controlled on Phenytoin 100mg MANE and 300mg NOCE Carbamazepine 200mg BD His admission phenytoin and carbamazepine levels are both therapeutic. He has been made nil by mouth pending a swallow assessment tomorrow afternoon. How could you ensure Mr KS receives his medication? Mr KS is not tolerating an NG tube write a prescription for Mr KS to ensure therapy in uninterrupted.
Interruptions in anticonvulsant therapy can have marked effects on seizure control. The anticonvulsant phenytion is extremely susceptible to reductions in plasma levels after missing even a single dose. It is therefore important to understand the different options available to ensure dosing is not missed. Phenytoin is available as a parental formulation and an oral suspension. The parental formulation is considered equal to the oral preparation and a direct conversion from oral to intravenous is possible. It is reasonable to check a baseline phenytoin level and then subsequent phenytoin levels 2 – 3 days into parental therapy. The oral liquid formulation of phenytion is not equivalent to oral tablets / capsules and it is also poorly absorbed if administered at the same time as nastro-gastric feeds. It is worth discussing this conversion with your ward pharmacist or the medicines information department. Sodium valproate can be administered parentally with no dose adjustment from oral to intravenous therapy. Sodium valproate levels do not relate to clinical effect and as such routine levels are not considered useful. Carbamazepine is available in a rectal preparation. There is a standard dose conversion detailed below PO Carbamazepine 100mg = PR Carbamazepine 125mg The maximum dose of rectal carbamazepine is 250mg QDS. Whilst this is less than some patient’s equivalent oral dose it is considered sufficient to maintain plasma levels for 48 – 72 hours until oral therapy can be reinstituted. Phenobarbital (Phenobarbitone) is available as a parental preparation. Baseline levels should be taken and dose conversion discussed with a pharmacist of member of the medicines information department. The newer anticonvulsants like levetiracetam, topiramate and lamotrigine are not available in parental or rectal preparations. In these cases early placement of an NG tube should be considered, as liquid and dispersible preparations are available.
Prescribing in Renal Impairment A large proportion of patients are admitted with a degree of renal impairment. This may be classified as acute, acute on chronic or chronic in nature. Dose adjustments or avoidance of nephrotoxic drugs are often needed in patients with renal impairment. There are several reasons for this:
• Failure to excrete a drug or its metabolites, resulting in accumulation hence toxicity
• Increased sensitivity to some drugs • Lost of effectiveness as renal function diminishes • Side effects are not tolerated by patients with renal impairment.
Consider the following scenario. Scenario 1 Mr AB is an 86 yr old man with known underlying chronic renal impairment (GFR 23mL/min) and type 2 diabetes. He was recently started on rosiglitazone to improve his glycaemic control and in the past few weeks he has had a number of home visits by the GP for symptoms of breathlessness and swollen ankles. His response to furosemide has been insufficient and his GP has arranged admission. On his last visit the GP gave Mr AB a course of erythromycin 500mg QDS for a presumed chest infection, Mr AB has been struggling to take this and keeps vomiting. Mr AB is also complaining of blurred vision and flashes of coloured light in front of his eyes. His medication is Furosemide 120mg OM Bendroflumethiazide 2.5mg OM Ramipril 5mg OM Aspirin 75mg OM Warfarin 4mg OD Last INR 1 week ago Digoxin 187.5mcg OD Metformin 850mg TDS Rosiglitazone 8mg OM Simvastatin 80mg ON He is known to have AF, type 2 diabetes and hypercholesterolaemia His admission Creatinine is 355micromol/L, Potassium is 2.9mmol/L Mr AB is 60kg calculate his GFR using the following Cockcroft-Gault formulae
Y x (140 – Age) x weight (kg) serum creatinine in micromol/L Y = 1.23 in males and 1.04 in females

Comment on any drug interactions
re there any further blood tests you want to order in relation to Mr AB’s medication?
hich medication would you want to hold on admission and why?
Mr AB’s hypokalaemia significant? Why?
hen on cover duty you are asked to review the following prescription for Sando-K in
A W Is WMr AB it is now 5 days after his admission.
What are the risks?
Prescribing in renal impairment requires an element of judgement on a number of
n. A t
s a general rule the following parameters should be considered when prescribing
- Could the patient’s regular or recently prescribed medication be contributing
- l function likely to improve?
mately what are
ny new therapy should be assessed for a dose reduction if the renal impairment is
ometimes in the very ill patient prescribing of essential nephrotoxic drugs cannot be
xample: 62-91% of aciclovir is excreted by the renal tubules. Accumulation causes
r by d
edicines that may be contributing to an acute deterioration in renal function should
is worth remembering that acute changes in renal function can lead to sudden
y
number of sources are available to help guide dosing in renal impairment.
he BNF contains a specific section on renal impairment. Often it does not specify a
pany data sheets often contain information regarding dosing in renal
complex and patient orientated factors. Medicines that are renally toxic are usually either dose reduced or stopped. Often other medicines are dose reduced not because of toxicity to the kidney but because of the side effects of accumulatiogood example of this would be the low molecular weight heparin enoxaparin, whilst iis not in itself toxic to the kidney, accumulation can lead to prolonged bleeding which is difficult to correct. Amedicines for a patient with a deranged renal function on admission.
to the degree of renal impairment? What is the patient’s baseline?
- How quickly (if at all) is the rena- Is the medicine I am prescribing likely to accumulate and ulti
the potential consequences of accumulation?
Agoing to continue for 24 hours post admission. Consider the patients baseline renal function. If the underlying renal function is poor a dose reduction for newly initiated therapy may be reasonable. Finally consider the potential risks to the patient if they receive full dose therapy over a prolonged period for example over a weekend. Savoided. The consequences of the drug accumulation will need to be considered as dose adjustment depends on toxicity of the drug. Ecrystal nephropathy and renal tubular necrosis. In this case, the total daily maintenance dose can be reduced either by reducing the individual doses oincreasing the dosing intervals. If the patient is does not have fluid restrictions anhas good renal output then hydration can prevent renal damage. Mgenerally be held until improvement in renal function is observed. Medication such asACEI or angiotensin 2 receptor antagonists need not be held in the context of chronic renal impairment unless there is another contraindication such as hyperkalaemia or hypotension. Ittoxicity with therapy that the patient has previously tolerated. Common examples include digoxin, beta-blockers and morphine. A number of serious incidents haverelated to continuation of long acting morphine preparations in a patient with acuteldeteriorating renal function. A Tspecific reduction but does allude to whether further consideration should be given to dosing. The comimpairment these can be accessed online via www.emc.medicines.org.uk.

Specialist information sources such as the renal drug handbook are also available
on
o use all these resource calculated GFR must be used not eGFR.
onsider the following scenario
cenario 2
rs JW, 89 year old, woman presented to A&E with a swollen L-leg. She is a Type 2
erum creatinine 550mmol/l
i
te
er drug history consists of the
etformin 850mg tds
on the renal and admissions wards. This text is considered the gold standard resource for prescribing in renal impairment. It contains monographs for most medicines and specific dose reductions including dosing strategies for patientsdialysis. T C S Mdiabetic, with poorly controlled blood glucose, and hypertension. Mrs JW was admitted to the medical ward, and on examination she has a temperature 39oC, sunken eyes, dry lips, painful L-leg, hot, swollen and cellulitic, BP 200/114mmHg, Pulse 90bpm. Her blood results are as follows SSerum urea 36mmol/l Serum potass um 4.3mmol/l Serum calcium 2.4mmol/l Serum phospha 2.20mmol/lCRP 405 Hb 10g/dl BM (random) 11.6mmol/l Weight 56kg Hfollowing MAcarbose 500mg tds Ramipril 2.5mg om Doxazosin 8mg bd Amlodipine 10mg omFrusemide 80mg om
The working diagnosis was severe cellulitis or DVT of the L-leg.
1. The decision was made to initiate benzylpenicillin and flucloxacillin. What dosages of these antibiotics would you prescribe for Mrs JW?
2. How would you manage Mrs JW’s possible DVT?
3. What other drugs / management would you also prescribe or discontinue for Mrs JW at this stage?
4. Mrs JW is complaining of pain. Discuss the choice of analgesic.
Three days later, despite being on antibiotics she is still pyrexial, serum creatinine 602mmol/l, urea 43 mmol/l, despite being on intravenous hydration, serum phosphate 2.77mmol/l, corrected serum calcium 2.0mmol/l, dry weight 76kg, and ankle oedema+++. Microbiology report suggested sensitivity to meropenem. Question: What dose of meropenem you would prescribe?
1 weeks later Mrs JW, cellulitis is resolving, serum creatinine 285mmol/l, serum urea 20mmol/l, serum calcium 2.3mmol/l, BP 175/98mmHg. Microbiology has suggested ciprofloxacin. Question: What dose would you prescribe? Question: A week later it was decided to discharge Mrs JW, what changes would
you make to her medications?
Prescribing in Hepatic Impairment Prescribing in hepatic impairment is often more difficult than prescribing in renal impairment. The dose reductions are often less specific and focus on more subjective parameters or the patient’s response to therapy. In general problems with medication occur in patients with jaundice, ascities or evidence of encephalopathy. In the case of hepatic impairment it can be difficult to identify patients that may have problems metabolising medication. Routine liver function tests are a poor guide to the capacity of the liver to metabolise drugs. It is therefore not possible to accurately predict the extent to which metabolism of a particular drug may be impaired. Markers of synthetic function such as INR and albumin can provide some information as to the metabolising capacity of the liver. Consider the following case: You have been called to see a recently admitted patient on AMU. He is a known liver patient who was started on phenytoin two weeks ago. He has been admitted after a fall with confusion and gait disturbance. His G.P had also treated him with clarithromycin for a presumed chest infection. You have been called to assess his analgesia and his phenytoin level which is 19mg/L (10 – 20) his serum albumin is 16 and his INR is 1.6. Comment on this result is it within normal limits? Comment on the choice of clarithromycin to treat his recent chest infection. It is a Friday. What action would you take and what follow-up would you put in place?

In chronic hepatic impairment the absorption and metabolism of medicines can be profoundly different to that of a normal healthy adult. Metabolism by the liver is the main route of elimination for many medicines. The hepatic reserve appears large and in general liver disease has to be severe before important changes in drug metabolism occur. In established disease hepatically metabolised medicines can accumulate quickly and lead to prolonged effects and toxicity. Hypoproteinaemia as a result of chronic liver disease means protein bound medicines have a greater propensity to produce toxicity. Examples of highly protein bound medicines include phenytoin, diazepam and propanolol. The development of collateral circulation secondary to portal hypertension means that medicines can be absorbed directly from the gut without any filtering by the liver. In this scenario the effect of these medicines can be greatly increased and almost all these medicines require dose reductions in established liver disease. Examples include propanolol, morphine, salbutamol and verapamil. In severe liver disease many medicines can further impair cerebral function and precipitate encephalopathy. These include sedative medication, opioid analgesics, diuretics that produce hypokalaemia and drugs that cause constipation. The effect of all sedative medicines is enhanced in hepatic impairment. Medications such as benzodiazepines and opiates often have a prolonged duration of action and an enhanced central effect. Extreme caution should be used when prescribing these two groups of medicines to end stage liver patients; a rapid and extensive encephalopathy can develop even after only a single dose. The BNF contains a specific appendix on prescribing in liver disease; this should be your first reference when prescribing for patients with hepatic impairment. Prescribing is often patient focused and based on risk vs benefit. In these cases further advice should be sought from medicines information or your ward pharmacist.
General Principles of Drug use in Pregnancy An agent is a teratogen if its administration to the pregnant mother directly or indirectly causes structural or functional abnormalities in the foetus or death of the child. Many pregnant women take medicines inadvertently before they realise they are pregnant. During the pre-embryonic stage an “all or nothing” concept is thought to apply. During this stage, if extensive damage occurs due to toxic insult, failure of implantation and miscarriage can occur. If the medicine is taken after the pre-embryonic phase, or the drug has a long half-life, the effect it will have will depend upon the drug taken. Drug treatment should only be given if it is clearly necessary because the foetus is at risk of developing structural and functional abnormalities. When treatment is deemed necessary, the lowest dose of a single drug should be used, and treatment should be stopped as soon as possible. New drugs are best avoided, because of lack of human data available.
Principles of teratogenesis
Timing of exposure Drugs can cause adverse effects at any stage of pregnancy, not just within the first 3 months. Exposure to a teratogen within the first 3 months is more likely to cause structural malformations and exposure after the first 3 months is more likely to result in growth defects.
Differences in susceptibility
Maternal and foetal susceptibility to a drug can be entirely different; a drug, which is harmless to a mother, can cause severe damage to the embryo foetus. There is no placental barrier to the passage of drugs or chemicals therefore the foetus is inevitably exposed to them.
Teratogenesis in humans
The pharmacokinetic and metabolic differences, between animals and humans, results in differences between teratogenicity.
Dose-response relationships Teratogenic effects are usually dose-dependant, and the dose response is usually steep. In addition, the time of administration after conception is critically important in determining the effects of an agent on the foetus and agents can act synergistically.
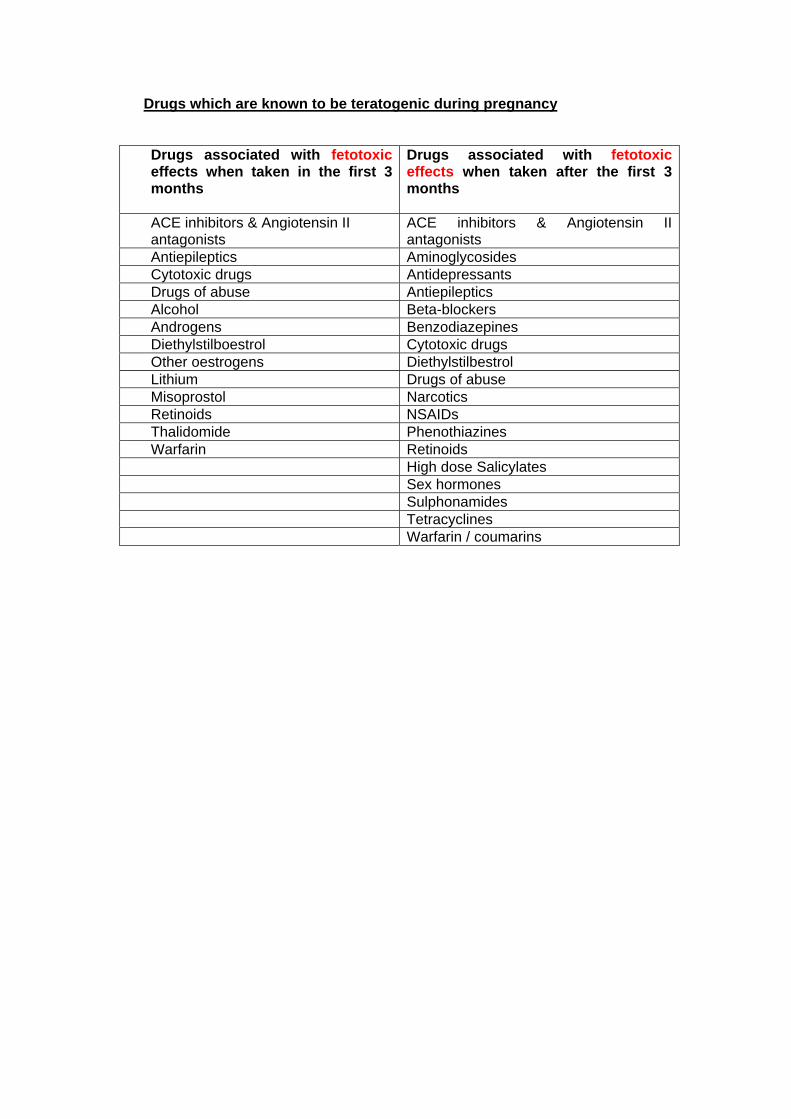
Drugs which are known to be teratogenic during pregnancy Drugs associated with fetotoxic effects when taken in the first 3 months
Drugs associated with fetotoxic effects when taken after the first 3 months
ACE inhibitors & Angiotensin II antagonists
ACE inhibitors & Angiotensin II antagonists
Antiepileptics Aminoglycosides Cytotoxic drugs Antidepressants Drugs of abuse Antiepileptics Alcohol Beta-blockers Androgens Benzodiazepines Diethylstilboestrol Cytotoxic drugs Other oestrogens Diethylstilbestrol Lithium Drugs of abuse Misoprostol Narcotics Retinoids NSAIDs Thalidomide Phenothiazines Warfarin Retinoids High dose Salicylates Sex hormones Sulphonamides Tetracyclines Warfarin / coumarins

Treating Common Conditions during pregnancy
Task 1: Aches and Pains – Use of analgesics
Minor aches and pains often do not require treatment, and analgesia should only be sought if essential A 30-year-old patient of 36 weeks gestation presents with back pain. What would you prescribe as a 1st line analgesic? Would you prescribe NSAIDS and / or opioids to a pregnant patient?
Gastro–oesophageal reflux and heartburn
Gastro–oesophageal reflux and heartburn are common in pregnancy, and are caused by a fall in lower oesophageal sphincter pressure. Conservative measures such as avoiding late meals in the evening, raising the head of the bed, avoiding fatty or spicy food should be encouraged. A 20-year-old patient of 25 weeks gestation presents in A&E with GOR and heartburn. Which antacids are suitable for prescribing for use during pregnancy? If a simple antacid failed to control symptoms, what would you suggest as second line treatment? Would a PPI be suitable for a pregnant patient? If so, which one?
Task 3: Constipation – Use of Laxatives Constipation is caused by reduced bowel movements that occur to allow more fluid to be absorbed during digestion, as more fluid is needed for increased plasma volume and circulation. Increasing fluids, increase dietary fibre and regular exercise may bring about brief relief. Task 6: A patient of 30 weeks gestation presents with constipation. What would you prescribe? What advice would you give?
• She has not been to the toilet for 4 days now • She has been taking Maalox for dyspepsia • She has tried fybogel but it is not working
Task 4: Nausea and Vomiting – Use of antiemetics Anti-emetics may be required in patients with severe vomiting. The drugs must be taken regularly to achieve adequate blood concentrations to control the nausea and vomiting. A 19-year-old patient, of 12 weeks gestation presents with nausea and vomiting. Which 2 anti-emetics are normally considered for 1st line treatment? Which antiemetics are reserved for second line treatment? Which antiemetic would she not be suitable for? If she were unable to tolerate tablets orally, which medicines are available in alternative preparations, what would you prescribe?
Task 5: Infections – Use of antibiotics When considering the treatment of infections with antibacterial agents during pregnancy, the following factors should be considered: The severity of the maternal infection The effects of any fever present on the pregnancy The effects of failing to treat the mother
The potential fetotoxicity of the drugs to be used Where possible, cultures should be sent and sensitivity tests should be available before making a choice on treatment. A patient of 18 weeks gestation is admitted with urinary frequency, pain on urination and a raised temperature. You send off an MSU, cultures and sensitivities will be available in a few days. What questions would you ask the patient in deciding which antibiotic to use?
Blood cultures are positive for e.coli. It is sensitive to trimethoprim, nitrofurantoin, ciprofloxacin, co-amoxiclav and erythromycin. Discuss which would be the most appropriate treatment, and why the others would not be appropriate.
General Principles of Drug use in Breast Feeding Drugs given to a breast-feeding mother may affect her baby. The mechanism of transfer of compounds across the breast differ from the transfer across the placenta therefore drugs safe in pregnancy may not be during breast-feeding and vice-versa. The most important factor is the concentration of the drug that is present in the neonatal blood, and the effect it may have. The factors that affect maternal drug concentrations are:
• Drug dose • Frequency • Route of administration • Patient compliance.
Most drugs will pass into the breast milk in greater or lesser amounts. One of the factors determining how much drug a baby will ingest is the timing of feeds in relation to maternal dose schedule. The frequency, volume and duration of feeds are also important. Infant metabolism is immature compared to adults. Because of this, the half-life of some drugs in the neonatal circulation is longer than in the maternal blood. This may lead to accumulation of drug in the infant.
Drugs which mean that the mother CANNOT breast feed: • Amantadine • Amiodarone • Antithyroid drugs • Antineoplastic drugs:
Amethopterin • Aspirin (in high dose) • Bromocriptine (suppresses
lactation) • Cascara (in large doses) • Carbimazole (can suppress
neonatal thyroid function in high dose)
• Cocaine • Chloramphenicol (can cause
grey syndrome in the baby) • Chlorpropamide • Ciprofloxacin • Cycloposphamide
• Cyclosporin • Doxorubicin • Ergotamine (ergotism can
occur in the infant) • Etretinate for psoriasis • Gold salts • Diamoprhine • Iodine • Isoniazid (GIVE pyridoxine to
the baby to avoid neuropathy) • Lithium • Phenindione • Phencyclidine • Senna (in large doses) • Thiouracil • Radio-isotopes
Breast feeding probably safe but with care • Amitryptiline - may cause sedation
but can be tried. • Barbiturates - avoid if possible
large doses can cause sedation in infant
• Benzodiazepines - same problem • Chlorpromazine • Cimetidine is concentrated in
breast milk but not known to be harmful
• Ethambutol • Flecanide also concentrated but
not known to be harmful • Metoclopramide (dopaminergic
blocker) • Metronidazole (in vitro mutagen.
alters taste of EBM) • Nalidixic acid • Oral Hypoglycaemics • Phenothiazines • Sulphonamides • Tetracycline (short course safe) • Warfarin (safe if mother not above
therapeutic range)

Treating Common Conditions during breastfeeding
Task 6: Antimicrobial agents Which antibiotics are not considered safe for use in breastfeeding, and why?
Task 8: A breast-feeding mother presents with swollen, red and painful area on her breast. She has a raised temperature and flu like feeling. What do you suspect is the problem? How would you tell her to treat it? What analgesia would she be safe to take and continue breastfeeding? After 24 hours she has not improved, and you have decided that an antibiotic is required, which one would you prescribe?

Resources to use when treating a pregnant or breastfeeding patient
• BNF Appendix 4: Pregnancy
Appendix 5: Breastfeeding Each appendix lists the most commonly used drugs and whether they are safe for use in pregnancy or breast-feeding. However, it tends to group drugs together and is sometimes not specific enough.
• Product literature available on line at www.medicines.org.uk
• Toxbase on line at http://www.spib.axl.co.uk/ . A password is required, but there is a password available for use on the acute medical unit and in A&E. Toxbase has monographs for most drugs for use in pregnancy and / or breastfeeding
• The Royal College of Obstetricians and Gynaecologists on line at
http://www.rcog.org.uk No password is required. They have published guidelines for the treatment of specific in pregnancy e.g. Management of chickenpox in pregnancy, management of genital herpes in pregnancy, thromboprophylaxis during pregnancy. • Prodigy guidance at http://www.prodigy.nhs.uk/ No password is required. They have guidance for treatment of pregnancy-associated dyspepsia, hypertension in pregnancy and nausea and vomiting in pregnancy.
• National specialist centres. The numbers are written in the front of the BNF.
The centre in Newcastle specialises in drugs used in pregnancy, and the centre in Sutton Coldfield and Leicester.
• Hospital Medicines information departments
Medicines Information is extension 6908 or 6909
Prescribing for substance misuse
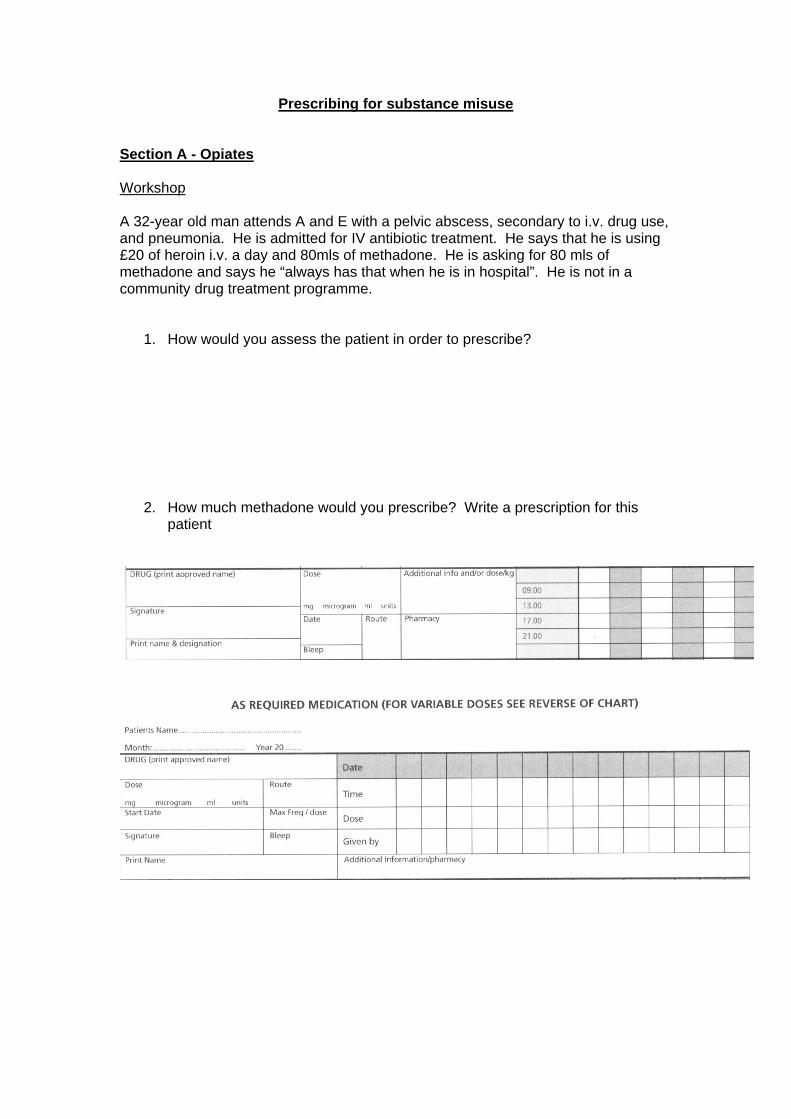
Section A - Opiates Workshop A 32-year old man attends A and E with a pelvic abscess, secondary to i.v. drug use, and pneumonia. He is admitted for IV antibiotic treatment. He says that he is using £20 of heroin i.v. a day and 80mls of methadone. He is asking for 80 mls of methadone and says he “always has that when he is in hospital”. He is not in a community drug treatment programme.
1. How would you assess the patient in order to prescribe?
2. How much methadone would you prescribe? Write a prescription for this patient
SOME KEY PRINCIPLES OF METHADONE PRESCRIBING
WITHDRAWAL SYMPTOMS DON’T KILL, METHADONE CAN.
Identifying withdrawal symptoms:
Objective: • Runny nose and eyes • Tremor • Agitation/fidgeting • Clammy skin or perspiration • Hypertension • Goose pimples • Tachycardia • Dilated pupils • Vomiting • Shivering • Yawning
Subjective:
• Nausea • Feeling hot / cold • Stomach cramps • Muscle tension/spasms/twitching • Aches and pains • Insomnia
These symptoms will generally occur - 6 – 12 hours after last dose of heroin - 18 – 48 hours after last dose of methadone The syndrome is unpleasant, but generally not medically dangerous. HOWEVER, failure to manage it effectively will undoubtedly affect the patient’s compliance with other interventions. N.B. Alcohol and Benzodiazepine withdrawal may mimic some of the above symptoms so beware. Alcohol and other sedatives can increase methadone toxicity so if there is any suggestion of intoxication with alcohol or sedatives methadone should be avoided. Note also that nocturnal sweats are a normal side effect of chronic methadone use. General Rules
• Unless recent opioid use can be confirmed by a RELIABLE source (e.g.
contact with legitimate prescriber/clinic; consumption of methadone under supervision of a pharmacist), treatment of withdrawal should be based on SYMPTOMATIC RELIEF in the first instance. This should be based on objective evidence of withdrawal.
• Only ORAL METHADONE MIXTURE 1mg / ml should be prescribed for this
indication (regardless of any self-reported previous treatment). All doses must be prescribed in milligrams (mg) NOT millilitres (ml)
• Because of the difficulty of verifying both prescribed and non-prescribed opioid use NOTHING should be prescribed to patients without withdrawal signs.
• Remember these patients may become aggressive and become a risk to staff
and other patients, this should always be considered before denying therapy. The patient should be reassured that although immediate prescription is not appropriate, any emerging withdrawal syndrome will be alleviated promptly.
• Opioids required for analgesia should be prescribed as usual, but potential
need for larger doses than usual should be anticipated, especially in acute onset pain, and where degree of dependency is not known.
• No methadone should be prescribed on the HMR UNLESS this has been
discussed with a Community Drugs Team or GP. In exceptional circumstances, a 1-2 day supply might be appropriate, pending contact with the appropriate agency.
DOSES Unless a prescribed methadone or buprenorphine dose can be confirmed with a Community Drugs Team or GP (see below), then proceed as follows when withdrawal symptoms appear:
• Moderate withdrawal syndrome: 20mg methadone at once, followed by 10mg 4 hourly when required. Up to a maximum of 50mg per day.
• Severe withdrawal syndrome : 30mg methadone at once followed by 10mg 4
hourly when required. Up to a maximum of 50mg per day.
• Patients should be observed for at least 4 hours following the administration of the first dose.
• No methadone should be given to a patient who appears drowsy or
intoxicated. Extreme care should be exercised in patients with liver dysfunction as methadone is particularly liable to accumulate and cause toxicity. Lower doses should be used in this situation together with slow dose increases and careful monitoring for sedation.
• Always prescribe IV Naloxone 400mcg ‘when required’ for patients prescribed
methadone.
• After the first 24 hours, the total daily dose given in that period may be written up as a single daily dose. Bear in mind that methadone can accumulate in the body and toxicity might become apparent after several days.
• If a 50mg daily dose does not appear to control withdrawal then care must be
taken in increasing doses beyond this level because of the dangers of toxicity. Preferably seek expert advice from the Community Drugs Team.
Vigilance with regard to drowsiness / intoxication should be ongoing. The signs of intoxication include: • Respiratory depression • Extreme somnolence progressing to stupor or coma • Maximally constricted pupils • Skeletal muscle flaccidity • Cold and clammy skin and sometimes bradycardia and hypotension
PRESCRIBING FOR PATIENTS CURRENTLY ON A TREATMENT PROGRAMME Methadone and buprenorphine are supplied by clinicians registered in the treatment of opiate dependence. The two predominant clinics within the Southampton area are New Road Centre: 02380 717171 – The New Road Centre is a Substance Misuse Service offering a range of treatment options to people who are experiencing problems in their use of drugs or alcohol. The service is offered to anyone who is 18 years or over and who is physically dependent on drugs and/or alcohol. Southampton DIPS: 02380 881409 – This is a combination of the old Bar Gate centre and a number of other detox programs. The DIPS centre provides opioid detox for a range of individuals. A large proportion of the attendees are on a probational program with supervised consumption i.e. they are witnessed taking the methadone or buprenorphine on site. This service is extremely organised and contacting them the day before discharge is usually sufficient to restart the community service for the individual. Opioids Used in the Treatment of Opioid Dependance Methadone and buprenorphine are the two predominant opioids used in the treatment of opioid addiction. Some patients receive treatment as a stepping stone to abstinence; others are on long-term maintenance to prevent a return to injecting. Methadone is a strong opioid with a long duration of action. In stable dependent patients, marked variations in plasma levels have little effect on overall symptoms. Therefore euphoric peak and withdrawal trough effects are not common on appropriate dosing, this is desirable in the treatment of opioid dependence. Buprenophine is a partial opioid agonist classically used for the treatment of opiate addiction. Since buprenorphine is a partial agonist it antagonises other opiates (in a similar way to naloxone) whilst still exerting its own opiate effect. Buprenorphine is often given three times weekly rather than daily. There are two forms of buprenorphine used in the treatment of opiate addiction. Subutex – A sublingual preparation containing Buprenorphine. It comes in 400micrograms, 2mg and 8mg tablets. Suboxone – This is a new sublingual combination preparation containing buprenorphine and naloxone. Problems relating to addicts dissolving and injecting Subutex have lead to the development of this product. If injected the naloxone constituent antagonises the effect of the buprenorphine. Due to poor oral absorption it does not have this effect if taken sublingually. If a patient is currently in a treatment programme then it may not be necessary to re-titrate doses of methadone if all criteria below are met:
1. Dose confirmed by prescriber / clinic / care worker. 2. Last consumption confirmed and is within last 3 days N.B. tolerance can
reduce after as little as 3 days 3. Patient is comfortable on dose (no signs of intoxication/withdrawal) 4. No other contraindications or cautions are present.
Section covered: F1 doctor signature....................................... F2 doctor signature........................................

Section B - Alcohol Workshop A 52-year old man presents with confusion, and visual hallucinations. He smells of alcohol. 1. How would you assess this patient? 2. What medication would you prescribe?

Workshop 2 Mr LS is admitted via his G.P with increasing confusion. On review you elucidate from a relative that he is a known alcoholic who now drinks about a can of strong lager a day. On review of the old notes you discover he is well known to the liver team with end stage chronic liver disease. On the consultant ward round you are asked to prescribe the standard vitamin and chlordiazepoxide regimen. Detail any concerns you have and how you would prescribe this with the charts provided
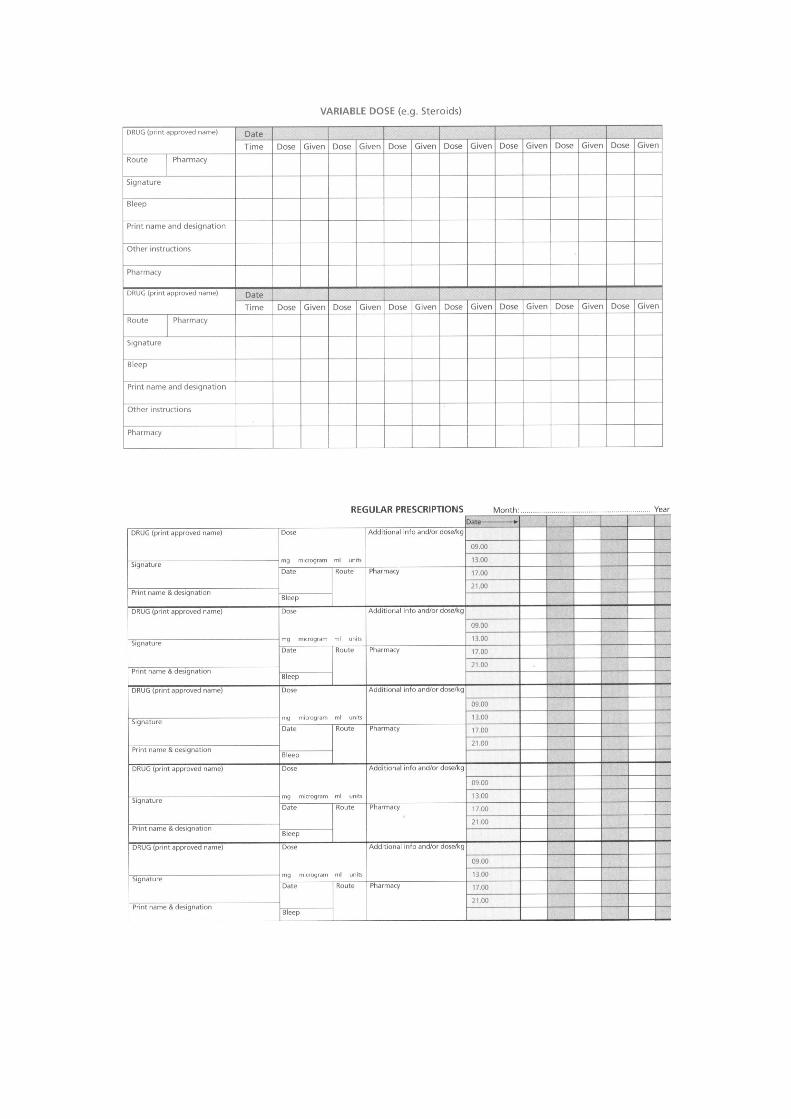
Management of Alcohol Withdrawal All patients requiring admission for alcohol withdrawal should receive parenteral vitamin therapy. ALCOHOL WITHDRAWAL- BASIC PRINCIPLES 1. Assessment of Withdrawal Symptoms
a. History- daily intake, periods of abstinence, morning shakes, previous episodes of withdrawal, history of DTs and fits, time of last drink, other drugs.
b. Severity of withdrawal symptoms-Restlessness, tremor, sweating, anxiety, nausea, vomiting, loss of appetite, insomnia. Tachycardia, systolic hypertension. Generalised seizures. DTs
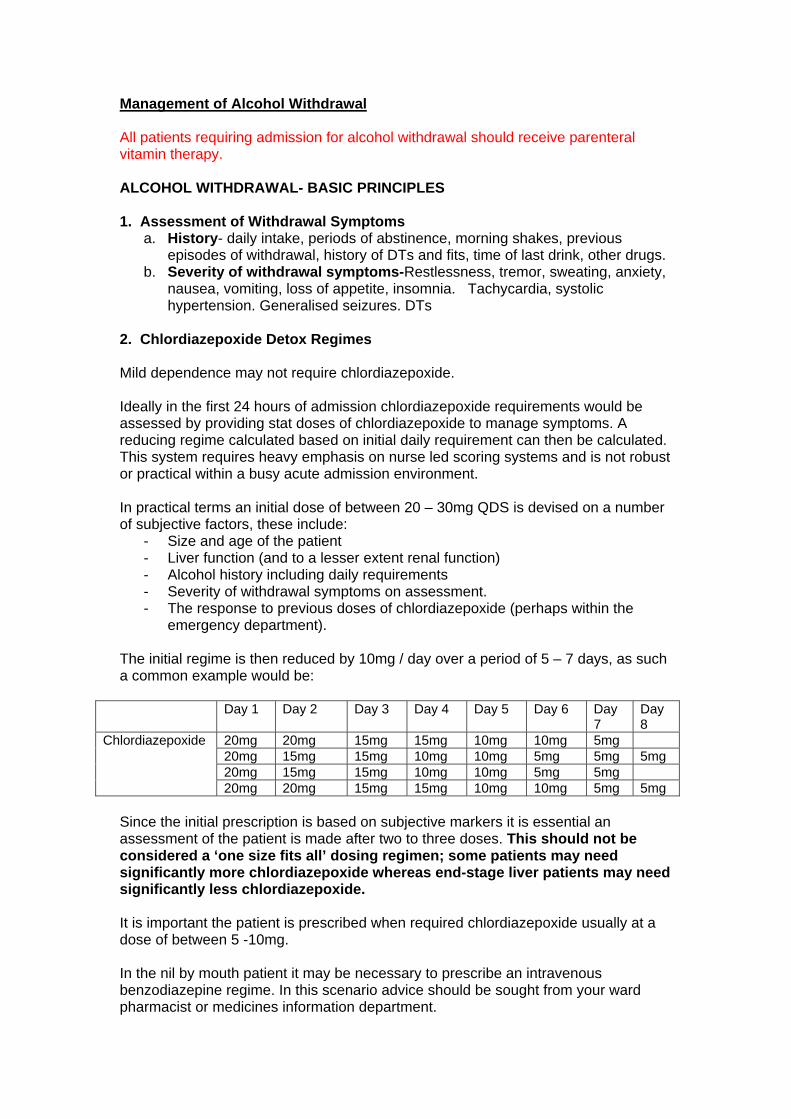
2. Chlordiazepoxide Detox Regimes Mild dependence may not require chlordiazepoxide. Ideally in the first 24 hours of admission chlordiazepoxide requirements would be assessed by providing stat doses of chlordiazepoxide to manage symptoms. A reducing regime calculated based on initial daily requirement can then be calculated. This system requires heavy emphasis on nurse led scoring systems and is not robust or practical within a busy acute admission environment. In practical terms an initial dose of between 20 – 30mg QDS is devised on a number of subjective factors, these include:
- Size and age of the patient - Liver function (and to a lesser extent renal function) - Alcohol history including daily requirements - Severity of withdrawal symptoms on assessment. - The response to previous doses of chlordiazepoxide (perhaps within the
emergency department). The initial regime is then reduced by 10mg / day over a period of 5 – 7 days, as such a common example would be:
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7
Day 8
20mg 20mg 15mg 15mg 10mg 10mg 5mg 20mg 15mg 15mg 10mg 10mg 5mg 5mg 5mg 20mg 15mg 15mg 10mg 10mg 5mg 5mg
Chlordiazepoxide
20mg 20mg 15mg 15mg 10mg 10mg 5mg 5mg Since the initial prescription is based on subjective markers it is essential an assessment of the patient is made after two to three doses. This should not be considered a ‘one size fits all’ dosing regimen; some patients may need significantly more chlordiazepoxide whereas end-stage liver patients may need significantly less chlordiazepoxide. It is important the patient is prescribed when required chlordiazepoxide usually at a dose of between 5 -10mg. In the nil by mouth patient it may be necessary to prescribe an intravenous benzodiazepine regime. In this scenario advice should be sought from your ward pharmacist or medicines information department.
3. Management of Acute Vitamin Deficiency All patients who require hospital admission for acute alcohol withdrawal and patients with evidence of chronic malnutrition, peripheral neuropathy, Wernicke’s encephalopathy, Korsakoff’s psychosis and delirium tremens should receive parenteral vitamins.
There is a risk of serious allergic reactions leading to anaphylaxis with parenteral vitamin therapy. 3.1. Wernicke’s Encephalopathy Classic triad of confusion, ataxia, and nystagmus only present in 10% of pts. 80% of Wernicke’s not diagnosed until post-mortem. Consider Wernicke’s if: Ataxia, Hypothermia and hypotension Confusion Ophthalmoplegia/nystagmus Memory disturbance Coma/unconsciousness 3.2. Thiamine Replacement Prophylactic Treatment (All at-risk patients) - One pair of ampoules of Pabrinex I.V. once daily for 3-5 days Therapeutic Treatment
- One pair of ampoules of Pabrinex, i.v. t.d.s. for 3-5 days or as long as improvement continues.
- Patients with chronic nutritional deficiencies should be given vitamin B compound strong tablets, TWO daily.
o Add extra thiamine, 100mg orally up to three times daily, if necessary. Continue for up to three weeks in severe deficiency.
- Parenteral Vitamins B & C (Pabrinex®) o Give 1 - 2 pairs of ampoules 8 hourly for up to 3 days, then one pair
twice daily for 5-7 days.
The contents of one pair of ampoules should be mixed in a syringe and injected intravenously over 10mins or preferably infused in 50-100mL of 0.9% sodium chloride or 5% glucose over 30mins.
Section covered: F1 doctor signature....................................... F2 doctor signature........................................