jameel g r 15.01.14
TRANSCRIPT

GRAND ROUND
Dr. Yasir JameelClinical Fellow Orthopedic Trauma

• 25 year old young male H/O fall at work, C/o pain and swelling left elbow.

• History

• Age, sex, occupation• Presenting complain• History of PC• Past medical history• Past surgical history • Drugs, Allergies• Social history

Investigations
• X-Ray• Blood works• CT scan?

X-rays

X-rays

X-rays

Distal Humerus Fracture
• Approx. 2% of all fractures• 15% of all humerus fractures.
• Young patient due to high energy trauma• Older patients due to (low energy)slip and fall
• Male young age • Female elderly >60

Mechanism of injury• The fracture pattern
may be related to the position of elbow flexion when the load is applied
• A elbow bent at 90deg• B elbow loaded
directly on olecranon• C elbow bent >
110deg loaded at olecranon

Distal Humerus Fracture
• Consists of • supracondylar fractures• single column (condyle) fractures• bicolumn fractures• coronal shear fractures
• Most common distal humerus intercondyler fracture

osteology• Constrained hinge joint• 2 columns Medial and
lateral• Trochlea as tie arch• Angulation
– 4-8 deg valgus– 3-8 deg ER– Medial 45deg flexion– Lateral 20 deg flexion
• Articular cartilage – Trochlea 300deg– Capitellum 180 deg

osteology
•Very thin sections of bone at olecranon fossa, radial fossa, coranoid fossa•Provide room for ROM without impingment•Weak area

Evaluation
• Clinical Symptoms – elbow pain and swelling/open wounds.
• Physical exam – gross instability often present – avoid ROM due to risk of neurovascular damage
• neurovascular exam – check function of radial, ulnar, and median nerve
• Distal vascularity:– brachial artery may be injured– if pulse decreased, obtain noninvasive vascular studies;
consult vascular surgery if abnormal– monitor carefully for forearm comparment syndrome

Classification.A0\OTA
• A –Extra Articular• B –Partial Articular• C –Total articular –No
continuity of shaft to articular surface
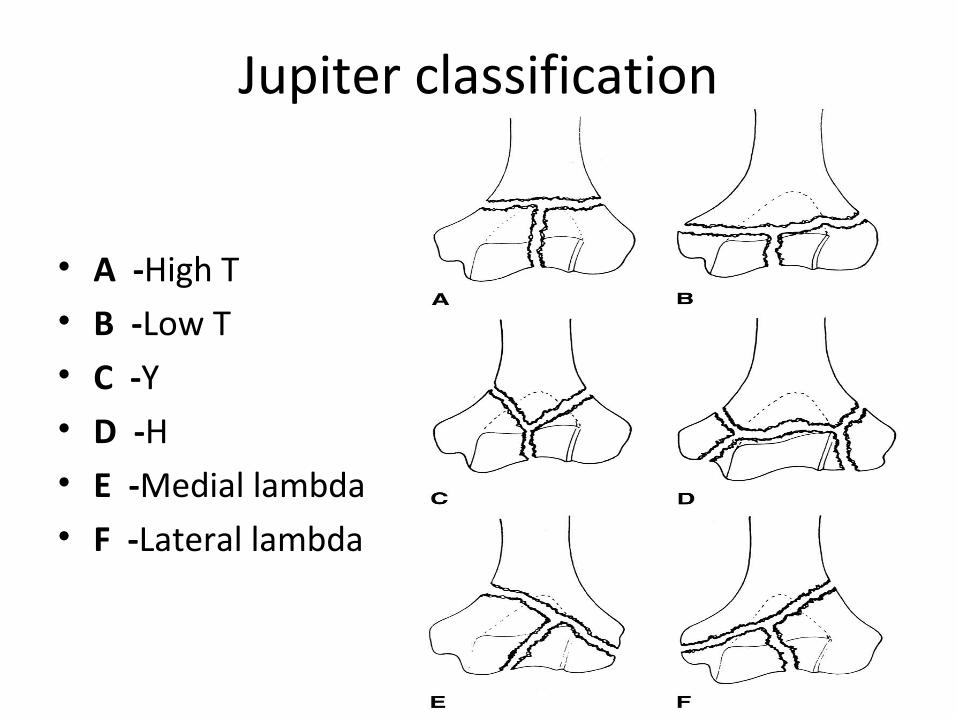
Jupiter classification
• A -High T• B -Low T• C -Y• D -H• E -Medial lambda• F -Lateral lambda

Treatment principles.
1. Anatomic articular reduction
2. Stable internal fixation of the articular surface
3. Restoration of articular axial alignment
4. Stable internal fixation of the articular segment to the metaphysis and diaphysis
5. Early range of motion of the elbow

Historical overview.
• Pionering operative tactics-Lambotte 1913• ”Bag-of- bones” -Eastwood 1937.Brown & Morgan 1971-• Scharphlatz and allgower 1975 articular reduction, articular
diaphyseal continuity and olecranon osteotomy.• Stable fixation- Morrey et al 1981• Jupitar 1985 – reduction techniques 27 of 36 pts with good
to excellent results• Helfet and schmeling 1993- sumrised principal of reduction
and dual platting and anatomical reduction with 75% good to excellent results, first time described early ROM.
• Precontoured plates-Shawn O’Driscol 2002

Treatment options
• Non operative– Elderly not fit for surgery ( cast imobilization)
• Operative – Distal humerus fracture displaced / undisplaced
Extraarticular / intraarticular

Surgical technique

Positioning • Lateral decubitus position
• Prone positioning possible
– Arm hanging over a post
– Sterile tourniquet if
desired
• Exposure dependent on
fracture pattern.• Exposure affects ability to
achieve reduction• Exposure influences
outcome!• Choose the exposure that fits
the fracture pattern.

Approaches• Direct posterior/triceps
split .• Triceps-sparing postero-
medial approach (Bryan-Morrey Approach)
• Needs experience– Midline incision– Ulnar nerve identified and
mobilized– Medial edge of triceps and
distal forearm fascia elevated as single unit off olecranon and reflected laterally
– Resection of extra-articular tip of olecranon

Olecranon osteotomy
• Improves visualisation –distal comminution.• Types-
-transverse-technically easier to do.
-higher incidence of nonunion-Gainor et al 1995
-chevron-apex distal-more stable,technically difficult.

Chevron osteotomy.
• Pre-drill and tap olecranon• –Create chevron apex
distal• –Protect the articular
surface by going through the last milimeterwith an osteotome
• –Aim for the ‘bare patch’at the apex of the trochlear notch

Fixation of the osteotomy.
• Tension band wire• Plate and screw• 6.5 cancellous screw and
tbw

Chevron osteotomy.
• Coles et al (2006) J Orthop Trauma 20:164• 70 chevron osteotomies– All fixed with screw plus tension band or with
plate-and-screw construct– 67 with adequate follow-up: all healed– 2 required revision fixation prior to healing– 18 of 61 with sufficient follow-up required implant
removal

Principle based parallel plate techniqueShawn W. O’Driscoll,jbjs 2007.• Treatment fails b\c of non union at sc level or
stiffness resulting from prolonged immob in an attempt to avoid hardware failure.
• Either way limiting factor is fixation of distal fragment to the shaft.
• To obtain union and mobility.
-maximal fixation in distal fragment.
-stability between distal fragment and shaft.

Controlling fragment rotation.

Plate application,provisional fixation.

Distal fixation.

Supracondylar compression.

In order to do this 7 objectives • Every screw in major distal fragment-
1.should pass thru a plate
2.engage a fragment on the opposite side.
3.be as long as possible.
4.engage as many fragments as possible.
Additional: 1.As many screws as possible should be placed in
the distal fragment.
2.Plates should allow union at sc level.
3.Plates strong enough to resist before union occurs.

Final construct• The screws in the distal
fragments interlock, providing additional stability to the construct.
• “closing the arch.”• Interlocking is best
achieved by contact between the screws.
• The combination of multiple screws criss-crossing in
close proximity with bone between them gives a “rebar” (reinforced concrete)-type structure

Ulnar nerve transposition
• Identification and mobilization of the ulnar nerve is often required
• Ulnar nerve palsy may be related to injury, surgical exposure/mobilization/stripping, compression by implant, or scar formation

Ulnar nerve transposition
• Wang et al (1994) J Trauma 36:770– consecutive series of distal humeral fractures
treated with ORIF and anterior ulnar nerve transposition had no post-operative ulnar nerve compression syndrome.
– overall results: Excellent/Good 75%, Fair 10%, and Poor 15%.
– conclusion: routine anterior transposition indicated.
Ulnar nerve transposition
• Chen et al (2010) J Orthop Trauma 24:391– Retrospective cohort comparison
–89 patients underwent transposition, 48 patients did not
– 4x greater incidence of ulnar neuritis in patients receiving transposition
– Conclusion: routine ulnar nerve transposition not recommended during ORIF of distal humerus fractures

Post op care.
• Measure and document rom obtained • Therapist will blame implants for loss of rom.• Bulky splint applied intra-op• Elbow position– 90 degrees of flexion or extension?– Authors support either and proponents strongly
argue that their position is the best• Extension is harder to recover than flexion• Final arc of motion recovered is more functional
if centered on 90 degrees of flexion• Use what works in your hands and rehab
protocol

complications• Ulnar nerve injury( in type c up to 25%)• Elbow stiffness
– most common flexion contracture mainly loss of terminal extension• Heterotopic ossification
– reported rate of 8%– routine prophylaxis is not warranted
• increased rate of nonunion in patients treated with indomethacin
• Nonunion – low incidence(2-10%) mainly supracondyler then trochlear grove.– avoide excessive soft-tissue stripping
• Malunion – avoided by proper surgical technique
• cubitus valgus (lateral column fxs)• cubitus varus (medial column fxs)
• DJD

Cassebaum 1969
• Described criteria for range of motion of elbow as an outcome meassure post ORIF
• As excellent being 15 deg to 130 deg range of motion arc

Orif of distal humerus fractures.
• Average 75% good to excellent results.
- jupiter et al-jbjs 1985
- sanders et al –orthopaedics 1992
- caja et al-injury 1994
- wang et al-trauma 1994
- papalonnou et al-injury 1995
- mckee et al-jbjs 1996

Non operative vs operative
• Zagorski 1986 : 76% good to excellent result in ORIF, 8% in non-operative
• Robinson 2003 : 2.9% delayed union and 2.9% nonunion in ORIF, 12% delayed union,17% nonunion in non-operative.
• Sirinivasan 2005: 52% mild to no-pain, ROM 22- 100, non-op 25 % mild to no-pain and ROM 36-70. articular step-off 1.2mm in op vs 2.6 in non-op.

Recent studies
• Sanchez and sotelo JBJS 2007 : parallel locked platting, flexion contracture 26 deg, ARC Of motion 99 deg, HTO 38% (69% in open frX)
• Doomberg jbjs 2007: 19 year follow up after ORIF, flexion contracture 23 deg, Arc of motion 106deg, subsequent procedures 40%, arthrosis 80%.

Comparison of different plate constructs
• J Orthop Trauma. 1994 Dec;8(6):468-75.• Biomechanical evaluation of methods of internal fixation of the distal humerus.• Schemitsch EH, Tencer AF, Henley MB.• University of Toronto, St. Michael's Hospital, Ontario, Canada.• Abstract• The best results following fractures of the distal humerus are provided by anatomic
reduction and rigid internal fixation. Plates of two designs placed in five different fixation configurations were used to determine the construct that would maximize rigidity of fixation of the distal humerus. Using a cadaver distal humerus osteotomy, with and then without cortical contact, motion of the distal fragment was measured with respect to the proximal fragment in axial and torsional loading, anterior to posterior and posterior to anterior bending, and lateral to medial and medial to lateral bending. With cortical contact, two plates when placed medial and lateral or at 90 degrees to each other provided equivalent rigidity. However, with a cortical gap, the combination of a specially designed anatomic lateral buttress "J" plate and a medial reconstruction plate gave the greatest rigidity (ANOVA, p < 0.05). Two-plate constructs do not require placement at 90 degrees to obtain sufficient rigidity, but do require placement on separate bony pillars and different surfaces

Summary Distal Humerus
• Preoperative planning CT scans Approach • ORIF successful in the majority of patients• Reestablish joint surface anatomically• Stability between distal fragment and
Humeral shaft• Early Rehabilitation Active and passive ROM• Severe bone loss (low demand seniors)
Consider primary elbow arthroplasty !

THANK YOU