jacobs journal of physiotherapy and...
TRANSCRIPT
OPEN ACCESS
Jacobs Journal of Physiotherapy and Exercise
The Effects of Massage Therapy: Validation by Clinical, Laboratorial and Single Photon Emission Cerebral Tomography in Randomized Patients with Cancer PainGabriela R Lauretti MD MSc PhD FIPP1*, Adriana S M Ferreira2, José R W Almeida MD 3, Euclides T Rocha MD 4,
Rogério F Costa MD 5, Davi Reial MD 5
1Associate Professor of Anesthesia and Pain Management, Brazil2Physioterapist, Postgraduate student, School of Medicine of Ribeirão Preto, University of São Paulo, Brazil3Consultant in Neurooncology, Barretos Cancer Hospital, Brazil4Consultant in Nuclear Medicine, Barretos Cancer Hospital, Brazil5Postgraduate student, School of Medicine of Ribeirão Preto, University of São Paulo, Brazil
*Corresponding author: Dr. Gabriela R Lauretti, Gabriela Rocha Lauretti, Rua-Maestro, Joaquim Rangel, 644, Ribeirão Preto- São Paulo;
Brazil, ZIP-14025 610, Phone: 010 55 16 602 22 11; Fax: 010 55 16 633 11 44; Email: [email protected]
Received: 08-30-2016
Accepted: 09-13-2016
Published: 10-19-2016
Copyright: © 2016 Gabriela R Lauretti
Research Article
Cite this article: Gabriela R Lauretti . The Effects of Massage Therapy: Validation by Clinical, Laboratorial and Single Photon Emission Cerebral Tomography in Randomized Patients with Cancer Pain. J J Physiother Exercise. 2016, 2(3): 021.
Abstract
Background
A randomized controlled trial was conducted to investigate the efficacy of massotherapy in reducing cancer-related bony-type pain and mood disturbances.
Methods
Trial design included men randomized into intervention or control groups. For 10-day, apart from routine physical and respira-tory therapies, the intervention group received daily standard massage. Treatment efficacy was evaluated prior (T1) and after 10-day massage (T2) by: 1) pain VAS, anxiety, depression, fatigue, comfort; 2) plasmatic noradrenaline; 3) daily opioid consump-tion, and 4) cerebral tomography single photon emission.
Results
Besides decreased VAS pain for the intervention group (p<0.05), there was lower noradrenaline plasmatic levels at T2 (p<0.001). Anxiety and depression were similar (p>0.05), while fatigue and comfort improved after massage (p<0.05). The intervention group displayed hyperfusion at the left post-central gyrus only, while the control group displayed hyperfusion at the left medium frontal gyrus; the right medium frontal gyrus; the right superior frontal gyrus and the right post central gyrus. Massotherapy decreased pain VAS, resulted in comfort, less fatigue; lesser noradrenaline plasmatic levels at T2, and hyperfusion in the left post-central gyrus, which corresponds to the somatosensory functions such as location of touch, temperature, vibration and pain, while in the control group.
JACOBSPUBLISHERS

Conclusions
Massotherapy resulted in decreased Pain VAS, lower noradren-aline plasmatic level which was corroborated by hyperfusion in four areas of the brain that correspond to the anticipation of pain, worry, motor control and response to painful stimuli.
Keywords: Cancer Pain; Cerebral Tomography Single Photon Emission; Plasmatic Noradrenaline; Massotherapy
Introduction
Recent meta-analysis indicates that massage is effective sup-portive therapy to relieve symptoms in patients with cancer pain [1]. Symptoms scores for pain, fatigue, stress, anxiety, nausea and depression were substantially improved, with per-sisted benefits after massage therapy [2-4]. Nevertheless, its efficacy and effectiveness for cancer patients lacks more de-tailed scientific evaluation [1,5,6].
Apart from clinical evaluation, functional brain imaging techniques allow to noninvasively visualize neuronal activi-ty during pain processing [7]. In previous data concerning 5 patients with severe chronic cancer pain the authors demon-strated significantly less blood flow in 3 out of 4 of the individ-ual quadrants of the hemithalamus contralateral to the side of pain [8], suggesting blood flow alteration in chronic pain state. In combination with elegant experimental paradigms in both volunteers and, increasingly, in patients, it has led to a vast ac-cumulation of knowledge concerning the central nervous sys-tem mechanisms involved in pain perception and pain modu-lation in humans [9].
This randomized controlled trial was conducted to investigate the efficacy of standard massage in reducing cancer-related symptoms and in improving mood disturbances. Treatment efficacy was evaluated: 1) clinically (pain VAS, Beck Invento-ry, opioid consumption); 2) by determination of the plasmatic noradrenaline concentration and by 3) single photon emission cerebral tomography (SPECT).
Methods
After ethics committee approval (Brazilian Plataform) and written informed consent, 16 male patients (30-70 year-old), capable of understanding the protocol, right handing, with intact body skin, with bone-type cancer pain with either ma-lignant tumor of the prostate, kidney, colon and rectum with widespread bone metastases and pain VAS> 4-cm were in-cluded. The study was prospective, computer randomized and conducted in a double-blind fashion way. The professional was the same for conducting the massage therapy, physical and respiratory therapies, and plasmatic noradrenaline material collection. Clinical data collection was performed by a second professional. The exclusion criteria included epilepsy, neuro-logical disorders, brain metastasis, amputees, bone fractures, neuropathic pain or refusal of the patient. All patients were in
Cite this article: Gabriela R Lauretti . The Effects of Massage Therapy: Validation by Clinical, Laboratorial and Single Photon Emission Cerebral Tomography in Randomized Patients with Cancer Pain. J J Physiother Exercise. 2016, 2(3): 021.
Jacobs Publishers 2use of daily oral morphine as part of the protocol for pain con-trol. All patients were also prescribed anticonvulsant carba-mazepine (400 mg at might time) and or amitriptilyne 25 mg before bedtime, as part of local protocol of the Cancer Hospital.
The interventional group received 20 minutes of massage ther-apy in a standardized technique during 10 consecutive days, in addition to daily physical and respiratory motor therapies, per-formed always by the same author. The massage consisted of 4 min at the back and 4 min at each extremity. It was performed in the morning, 4 hours after the last morphine oral dose ad-ministration, and consisted of subsequent sliding movements with the hands, applying superficial [10] and deeper pressure [11]. The massotherapy was always performed by the same au-thor in all patients, and who applied the same pressure charac-teristics on the patients´ skin. The control group received only physical and respiratory motor therapies.
Both groups underwent SPECT intervention, for the assess-ment of cerebral blood flow; and plasma noradrenaline eval-uation before (T1) and after the 10-day therapy (T2). For the SPECT, each participant was injected through the intravenous cannula (IV) with 7 mCi (99m)Tc and scanned using SPECT at T1 (i.e., before the massage technique sessions), and then was injected with 25 mCi (99m)Tc through the IV and scanned using SPECT at T2, i.e., after the massotherapy sessions. Plas-ma measurements of noradrenaline were done through High Performance Liquid Chromatography (HPLC) at the Faculty of Pharmaceutical Sciences of Ribeirão Preto, University of São Paulo. After withdraw of 10-ml blood in order to avoid any di-lution at the site of collection, 5-ml of venous blood was col-lected at the times T1 and T2. The samples were transposed in heparinized tubes and plasma separated by centrifugation. The plasma samples were stored at –70oC until drug assay by HPLC. Detection was operated under selected ion monitoring mode. The analyte was stable during all sample storage, prepa-ration and analysis procedures, described elsewhere [12].
Pain (VAS) was clinically evaluated daily, before and after the therapies, i.e., massage, physical and respiratory for the inter-ventional group and physical and respiratory therapies for the control group. The concept of visual analog scale (VAS), which consisted of a 10 cm line with 0 equaling “no pain at all” and 10 equaling “the worst possible pain” was previously introduced. The opioid consumption representative of the last 24-h was evaluated at T1 and in the morning during all the study period. Anxiety and depression were evaluated at T1 and T2 with the Beck Inventary [13] for the categories depression, anxiety, fa-tigue and comfort. P<0.05 was considered significant.
Statistical Analysis
The definition of the number of patients was based on prelim-inary study of the same authors using the same methodology for massage therapy [14]. We hypothesised that 20-min mas-sage therapy would decrease the pain VAS by 100%, compared
Cite this article: Gabriela R Lauretti . The Effects of Massage Therapy: Validation by Clinical, Laboratorial and Single Photon Emission Cerebral Tomography in Randomized Patients with Cancer Pain. J J Physiother Exercise. 2016, 2(3): 021.
Jacobs Publishers 3to the control group. If a standard deviation was estimated, an 80% and an alpha value of 0.05, these assumptions would re-quire at least 6 patients per group. This population was fur-ther analized regarding mood, noradrenaline plasmatic level, SPECT, morphine consumption and fatigue. The normality of the data was first evaluated by the Shapiro Wilkings test. De-mographic data, degree of depression and anxiety were ana-lyzed by the Fisher exact test. Quantitative data was compared using Mann-Whitney test, ANOVA, Kruskal Walis or Friedman, followed by Tukey Honest test, when indicated. P<0.05 was considered significant. The SPECT analysis was automatically done by the Statistical Parametric Mapping (SPM), versions Matlab 6.5 and SPM2. SPM is a mathematical model of for processing functional images with the finality to build spatial tridimensional maps. This program created by Friston K can be obtained at the site http:/www.fil.ion.ucl.ac.uk/spm/. The images were converted to the Analyse format, with both ante-rior and posterior commissures aligned (Talairach System). It was considered only images with at least 20 voxels after cor-rections for multiple comparisons. The deformations parame-ters were generated within Bayzeano statistic context, where the images are placed over a probabilistic model by Friston. P<0.05 was considered significant.
Results
The demographic data are described in Tables 1- 3. Three pa-tients from the Intervention group and four from the Control group were withdrawn from the final analysis. Two of them died in each group, one in each group refused to collect blood for plasmatic noradrenaline measurement and the last patient in the Control group refused to submit to SPECT at T2.
NSAID-Non Steroidal Antiinflamatory Drug
The groups were demographically similar with regard to age, body weight, initial morphine consumption, adjuvant anticon-vulsant intake, antidepressive intake, and initial pain VAS val-ues at T1 (Tables 1-3, p>0.05). In addition, body weight index was also similar between groups (24±3.4; 25±2.1; Interven-tional and Control groups, respectively, p>0.05). The groups were also similar in respect to religion (Presbyterian or Cath-olic), schooling, smoking and previous alcohol consumption, (data not shown, p>0.05), initial level of anxiety, depression,
fatigue, comfort and complain of pain for more than 4 months (Table 2, p>0.05). All patients were right handed (p>0.05, data not shown).
The oral dose of morphine consumption (mg) at T1 was sim-ilar between groups (60±38; 60±27, interventional and con-trol group, respectively, p>0.05, Table 1), as were the adju-vant drugs consumption prior to the study inclusion (Table 3, p>0.05). Although there was a trend not statistically significant towards decreased oral morphine consumption during the 10-day study for the Intervention group (Table 4, p>0.05), during the study period, the Intervention group showed lower per-ception of pain evaluated by decreased daily pain VAS (Table 5, p<0.05).
Table 4. Descriptive analysis of the morphine consumption (mg) during the 10-day evaluation after daily physical and respiratory motor therapies for the control group and daily physical, respiratory motor and massage therapies for the in-tervention group.
Related to levels of anxiety and depression, the two groups were similar at T1 and at T2, showing no improvement (p>0.05). However, patients from the massotherapy group referred less fatigue and more comfort at T2 (p<0.05). All pa-tients from both groups referred classified fatigue as “moder-ate” at T1, while at T2, only patients from the interventional group improved and classified fatigue as “none” (p>0.05).
Related to the noradrenaline plasmatic levels, their concentra-tion at T1 was similar between groups (p>0.05, Table5).
However, patients who received massage as part of the proto-col had lower noradrenaline plasma levels when compared to the control group at T2 (Table 6).
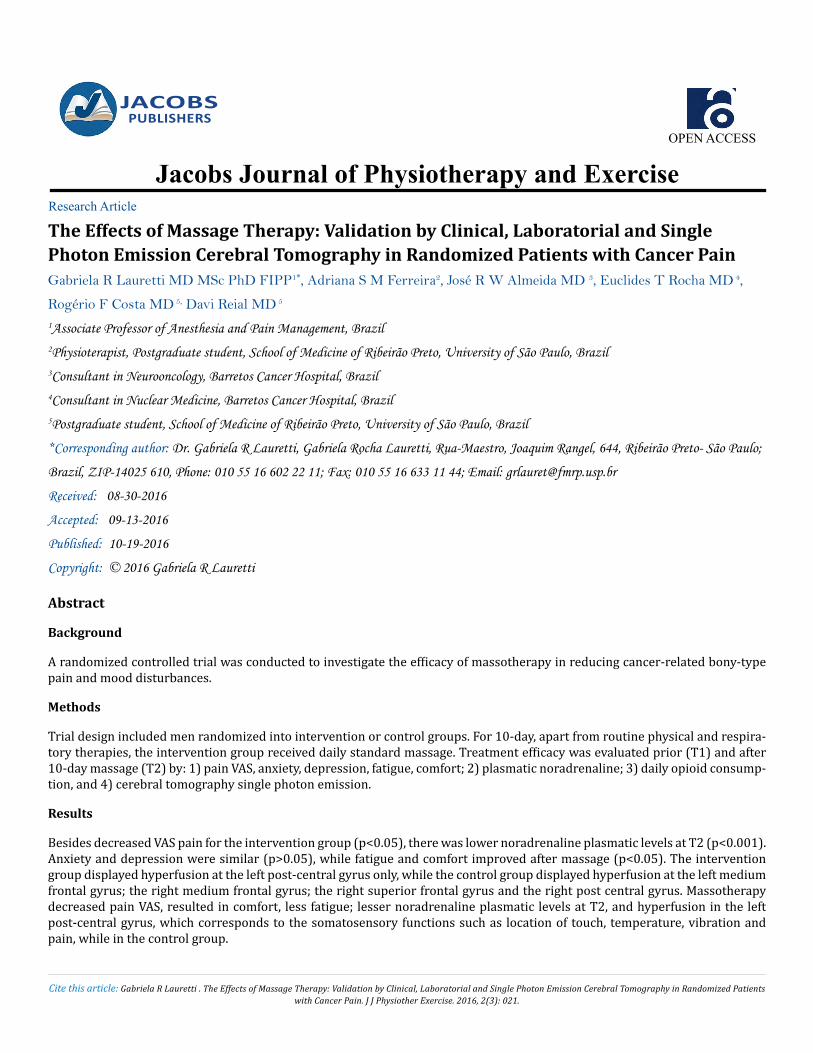
Related to the SPECT evaluation, neither the control nor the massotherapy groups showed any brain hypoperfusion areas during the study evaluation (Figures 1-5). However, all pa-tients submitted to massotherapy displayed hyperfusion at only one site: a) the left post-central gyrus only, which cor
Intervention Group Control Group p
mean(SD) median min-max mean (SD) median min-max (M-W)
Age (years) 60.1(7.6) 63 50.0-68.0 65.3(3.9) 66.5 60.0-69.0 0.197 Corporal body weight (kg) 24.2(3.4) 23.3 20.4-31.2 24.8(2.1) 25.2 21.7-27.2 0.475
Morphine (T1) 60(38.4) 60 20.0-100.0 60(26.8) 60 30.0-90.0 0.46 Pain VAS (T1) 6.1(1.3) 6 5.0-9.0 5.7(1.2) 5 5.0-8.0 0.278 M-W- Mann-Whitney Test. T1- time before the 10-day massage therapy. VAS- visual analog scale.
Table 1. Demographic data
Cite this article: Gabriela R Lauretti . The Effects of Massage Therapy: Validation by Clinical, Laboratorial and Single Photon Emission Cerebral Tomography in Randomized Patients with Cancer Pain. J J Physiother Exercise. 2016, 2(3): 021.
Jacobs Publishers 4
* Fisher Test. T1- Time before the 10-day massage therapy Table 2. Symptoms, no. and percentage of patients in the study groups (T1).
*Fisher exact test, comparison between the control group and the in-terventional group at T1 (time before the 10-day massage therapy).Table 3. Number (n), percentage, diagnostic, and drug consumption in the study groups at T1.
(M-W) - Mann-Whitney Test
Table 4. Descriptive analysis of the morphine consumption (mg) during the 10-day evaluation after daily physical and respiratory motor therapies for the control group and daily physical, respiratory motor and massage therapies for the intervention group.
(M-W) - Mann-Whitney Test
Table 5. Descriptive analysis of the pain VAS after the treat-ment therapy during the 10-day evaluation.
Variável Interventional group Control group p*
n (%) n (%) Chronic Pain (≥ 4 months)*
No 4 57.1 1 16.7 0.266 Yes 3 42.9 5 83.3
Anxiety
None 2 28.6 2 33.3 0.629 Little 4 57.1 2 33.3 Moderate 1 14.3 2 33.3
Depression
None 1 14.3 1 16.7 0.672 Little 4 57.1 2 33.3 Moderate 2 28.6 3 50
Fatigue
None 0 0 0 0 Little 0 0 0 0 Moderade 7 100 6 100
Comfort
None 3 42.9 1 16.7 0.266 Little 4 57.1 5 83.3 Moderate 0 0
Intervention Group Control Group
P* (n=7) (n=6) n (%) n (%)
Diagnostic
Colon 0 0 1 16.7 0.255 Prostate 5 71.4 4 66,7 Rectum 0 0 1 16.7 Kidney 2 28.6 0 0
Anticonvulsant*
No 6 85.7 4 66.7 0.559 Yes 1 14.3 2 33.3
Antidepressant*
No 4 57.1 5 83.3 0.192 Yes 3 42.9 1 16.7
NSAID*
No 7 100 5 83.3 0.462 Yes 0 0 1 16.7 Total 7 6
Intervention Group Control Group p
mean (SD) median min-
max mean (SD) median min-max (M-W)
Morphine
1º day 57.1(50.6) 30 20.0-140.0 60.0(26.8) 60 30.0-90.0 0.467
2º day 54.3(45.4) 30 20.0-120.0 60.8(25.8) 60 30.0-90.0 0.386
3º day 62.8(42.3) 60 20.0-120.0 61.7(24.8) 60 30.0-90.0 0.827
4º day 60.0(43.2) 40 20.0-120.0 61.7(24.8) 60 30.0-90.0 0.663
5º day 60.0(43.2) 40 20.0-120.0 66.7(33.3) 60 30.0-120.0 0.561
6º day 58.6(44.1) 40 20.0-120.0 66.7(33.3) 60 30.0-120.0 0.468
7º day 58.6(44.1) 40 20.0-120.0 70.0(33.5) 70 30.0-120.0 0.427
8º day 58.6(44.1) 40 20.0-120.0 70.0(33.5) 70 30.0-120.0 0.427
9º day 58.6(44.1) 40 20.0-120.0 70.0(33.5) 70 30.0=120.0 0.427
10º day 58.6(44.1) 40 20.0-120.0 70.0(33.5) 70 30.0-120.0 0.427
Variável Interventional Group Control Group p
mean (SD) median min-
max mean (SD) median min-
max (M-W)
Pain 1º day 1.8 (2.1) 1 0.0 – 6.0 6.0 (1.3) 5.5 5.0 – 8.0 0.012 2º day 2.0 (1.7) 2 0.0 – 4.0 5.0 (1.1) 5 4.0 – 7.0 0.006 3º day 0.8 (1.2) 0 0.0 – 3.0 4.7 (1.9) 5 2.0 – 7.0 0.006 4º day 0.6 (1.0) 0 0.0 – 2.0 5.0 (1.4) 5 3.0 – 7.0 0.002 5º day 0.3 (0.7) 0 0.0 – 2.0 5.0 (1.8) 4.5 3.0 – 8.0 0.002 6º day 0.1 (0.4) 0 0.0 – 1.0 5.0 (1.8) 4.5 3.0 – 8.0 0.002 7º day 0.6 (1.1) 0 0.0 – 3.0 5.0 (1.8) 5 3.0 – 7.0 0.003 8º day 0.1 (0.4) 0 0.0 – 1.0 4.3 (2.1) 3 3.0 – 7.0 0.001 9º day 0.1 (0.4) 0 0.0 – 1.0 4.3 (2.5) 3 2.0 – 8.0 0.001 10º day 0.1 (0.4) 0 0.0 – 1.0 4.8 (2.8) 3 3.0 – 9.0 0.001
Cite this article: Gabriela R Lauretti . The Effects of Massage Therapy: Validation by Clinical, Laboratorial and Single Photon Emission Cerebral Tomography in Randomized Patients with Cancer Pain. J J Physiother Exercise. 2016, 2(3): 021.
Jacobs Publishers 5
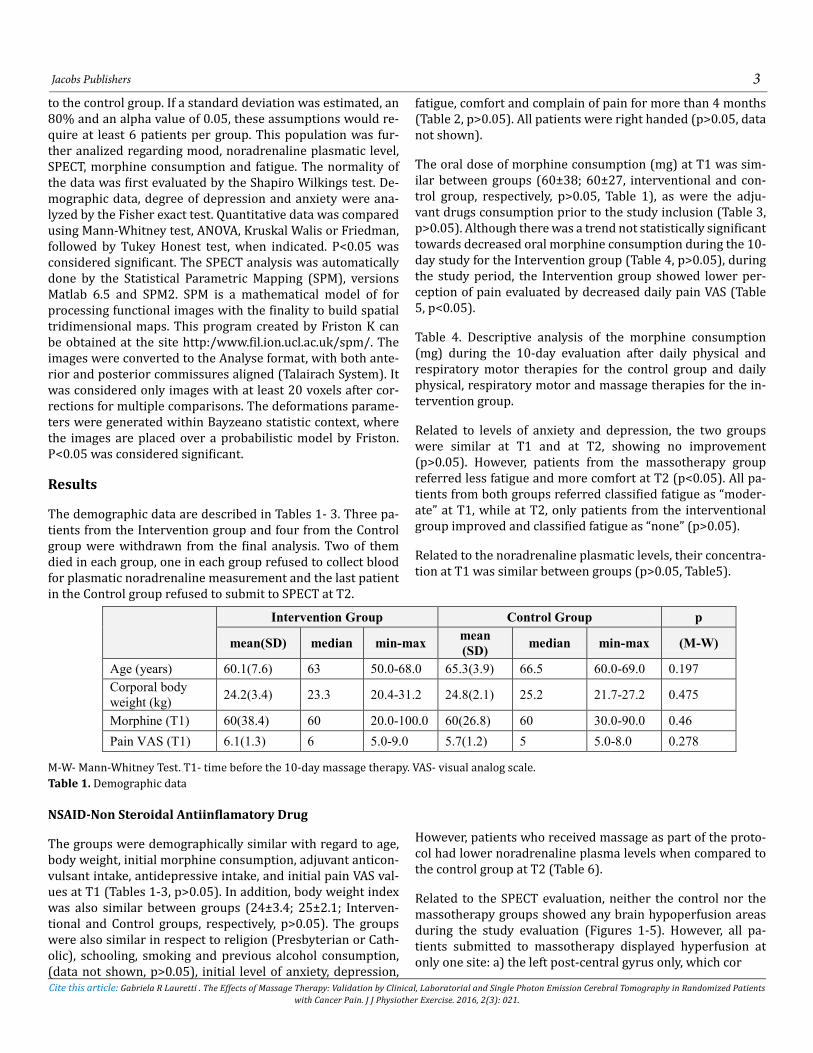
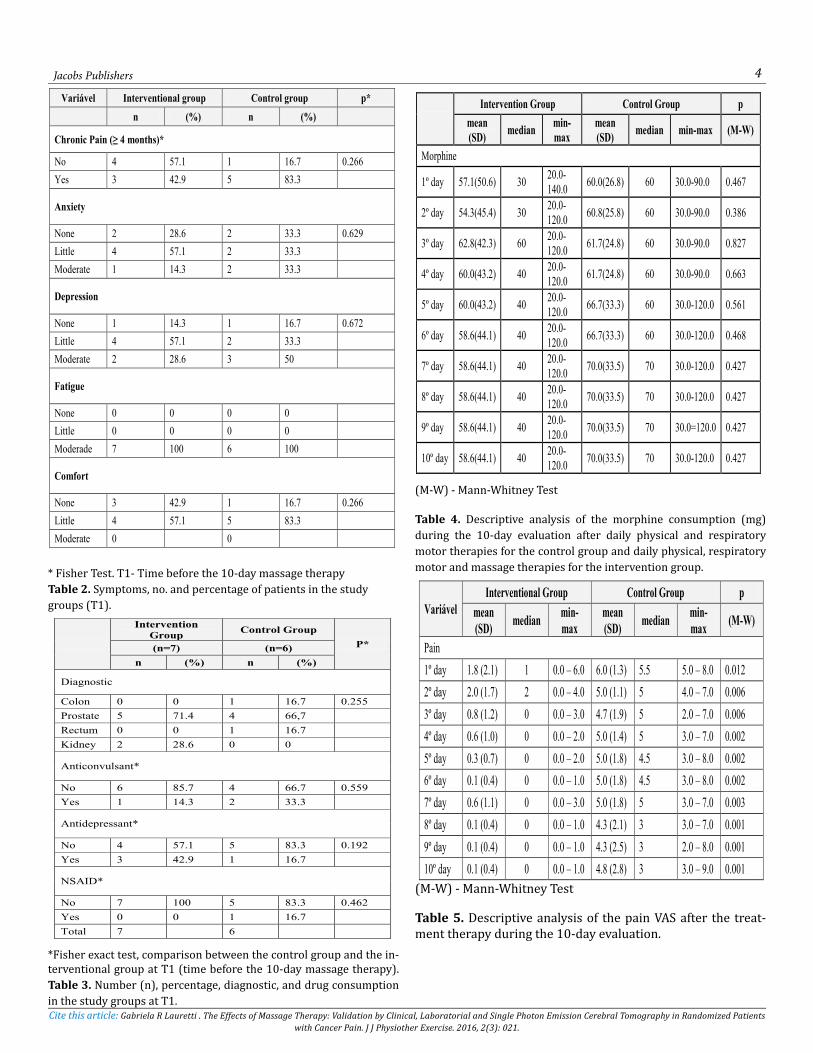
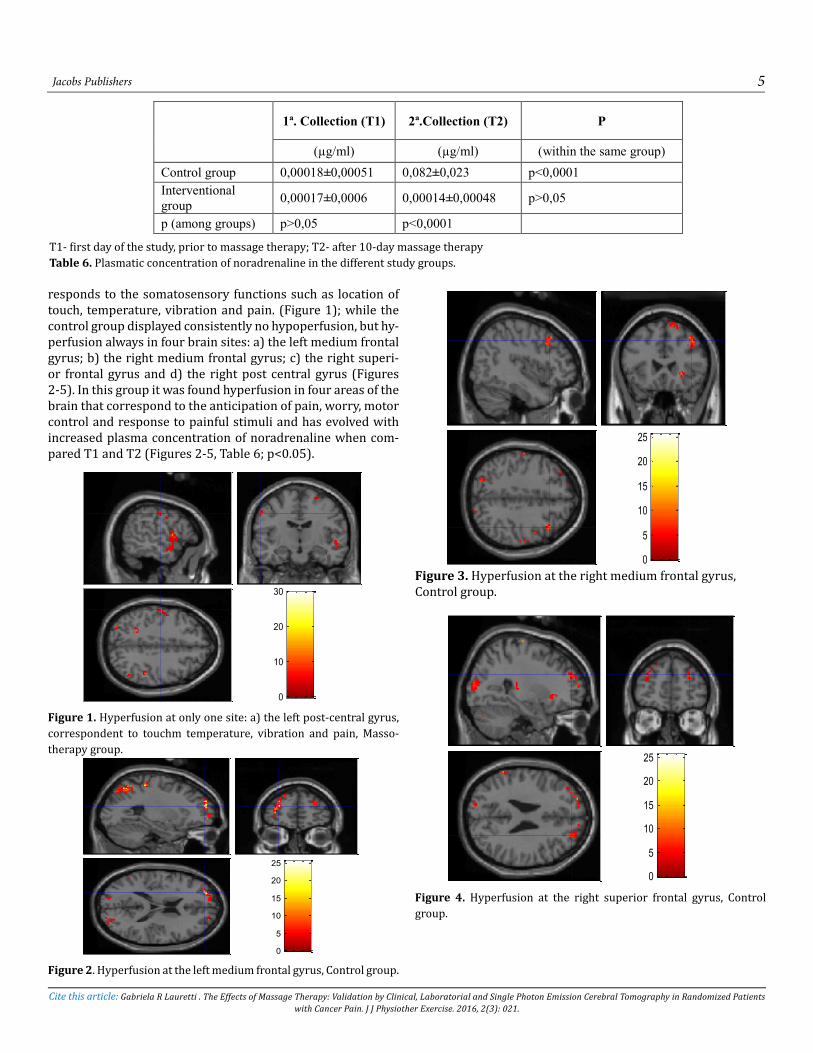
responds to the somatosensory functions such as location of touch, temperature, vibration and pain. (Figure 1); while the control group displayed consistently no hypoperfusion, but hy-perfusion always in four brain sites: a) the left medium frontal gyrus; b) the right medium frontal gyrus; c) the right superi-or frontal gyrus and d) the right post central gyrus (Figures 2-5). In this group it was found hyperfusion in four areas of the brain that correspond to the anticipation of pain, worry, motor control and response to painful stimuli and has evolved with increased plasma concentration of noradrenaline when com-pared T1 and T2 (Figures 2-5, Table 6; p<0.05).
Figure 1. Hyperfusion at only one site: a) the left post-central gyrus, correspondent to touchm temperature, vibration and pain, Masso-therapy group.
Figure 2. Hyperfusion at the left medium frontal gyrus, Control group.
Figure 3. Hyperfusion at the right medium frontal gyrus, Control group.
Figure 4. Hyperfusion at the right superior frontal gyrus, Control group.
1ª. Collection (T1) 2ª.Collection (T2) P
(µg/ml) (µg/ml) (within the same group) Control group 0,00018±0,00051 0,082±0,023 p<0,0001 Interventional group 0,00017±0,0006 0,00014±0,00048 p>0,05
p (among groups) p>0,05 p<0,0001 T1- first day of the study, prior to massage therapy; T2- after 10-day massage therapy
Table 6. Plasmatic concentration of noradrenaline in the different study groups.
SPM
mip
[-56,
-12,
42]
<
< <
SPM{T4}
hiperperfusão pós central esquerda. Massoterapia
SPMresults: .\matHeight threshold T = 3.75Extent threshold k = 20 voxels
Design matrix2 4 6
2
4
6
8
10
3
0
10
20
30
SPM
mip
[-26,
54, 1
8]
<
< <
SPM{T4}
hiper giro frontal médio esquerdo
SPMresults: .\paired t test Controles\matHeight threshold T = 3.75Extent threshold k = 20 voxels
Design matrix2 4 6
2
4
6
8
10
contrast(s)
5
0
5
10
15
20
25
SPM
mip
[42,
24,
42]
<
< <
SPM{T4}
hiper giro frontal médio direito
SPMresults: .\paired t test Controles\matHeight threshold T = 3.75Extent threshold k = 20 voxels
Design matrix2 4 6
2
4
6
8
10
5
0
5
10
15
20
25
SPM
mip
[28,
50,
26]
<
< <
SPM{T4}
giro frontal superior direito RM
SPMresults: .\paired t test Controles\matHeight threshold T = 3.75Extent threshold k = 20 voxels
Design matrix2 4 6
2
4
6
8
10
5
0
5
10
15
20
25
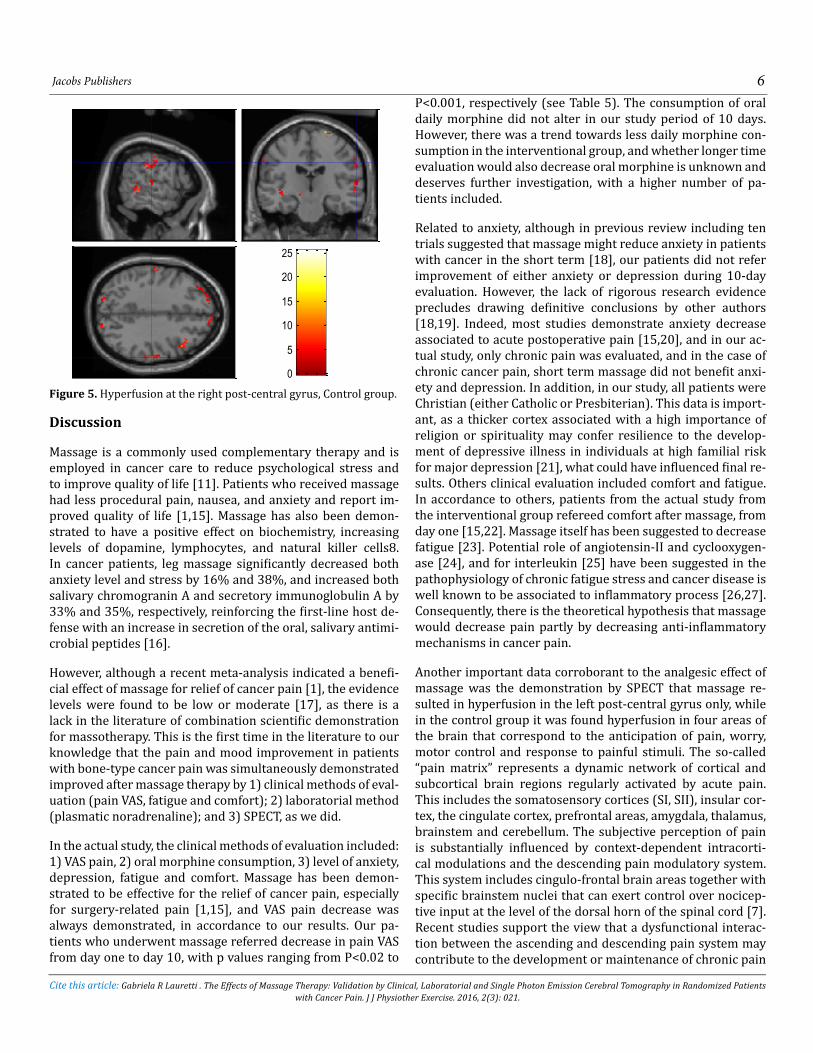
Figure 5. Hyperfusion at the right post-central gyrus, Control group.
Discussion
Massage is a commonly used complementary therapy and is employed in cancer care to reduce psychological stress and to improve quality of life [11]. Patients who received massage had less procedural pain, nausea, and anxiety and report im-proved quality of life [1,15]. Massage has also been demon-strated to have a positive effect on biochemistry, increasing levels of dopamine, lymphocytes, and natural killer cells8. In cancer patients, leg massage significantly decreased both anxiety level and stress by 16% and 38%, and increased both salivary chromogranin A and secretory immunoglobulin A by 33% and 35%, respectively, reinforcing the first-line host de-fense with an increase in secretion of the oral, salivary antimi-crobial peptides [16].
However, although a recent meta-analysis indicated a benefi-cial effect of massage for relief of cancer pain [1], the evidence levels were found to be low or moderate [17], as there is a lack in the literature of combination scientific demonstration for massotherapy. This is the first time in the literature to our knowledge that the pain and mood improvement in patients with bone-type cancer pain was simultaneously demonstrated improved after massage therapy by 1) clinical methods of eval-uation (pain VAS, fatigue and comfort); 2) laboratorial method (plasmatic noradrenaline); and 3) SPECT, as we did.
In the actual study, the clinical methods of evaluation included: 1) VAS pain, 2) oral morphine consumption, 3) level of anxiety, depression, fatigue and comfort. Massage has been demon-strated to be effective for the relief of cancer pain, especially for surgery-related pain [1,15], and VAS pain decrease was always demonstrated, in accordance to our results. Our pa-tients who underwent massage referred decrease in pain VAS from day one to day 10, with p values ranging from P<0.02 to
P<0.001, respectively (see Table 5). The consumption of oral daily morphine did not alter in our study period of 10 days. However, there was a trend towards less daily morphine con-sumption in the interventional group, and whether longer time evaluation would also decrease oral morphine is unknown and deserves further investigation, with a higher number of pa-tients included.
Related to anxiety, although in previous review including ten trials suggested that massage might reduce anxiety in patients with cancer in the short term [18], our patients did not refer improvement of either anxiety or depression during 10-day evaluation. However, the lack of rigorous research evidence precludes drawing definitive conclusions by other authors [18,19]. Indeed, most studies demonstrate anxiety decrease associated to acute postoperative pain [15,20], and in our ac-tual study, only chronic pain was evaluated, and in the case of chronic cancer pain, short term massage did not benefit anxi-ety and depression. In addition, in our study, all patients were Christian (either Catholic or Presbiterian). This data is import-ant, as a thicker cortex associated with a high importance of religion or spirituality may confer resilience to the develop-ment of depressive illness in individuals at high familial risk for major depression [21], what could have influenced final re-sults. Others clinical evaluation included comfort and fatigue. In accordance to others, patients from the actual study from the interventional group refereed comfort after massage, from day one [15,22]. Massage itself has been suggested to decrease fatigue [23]. Potential role of angiotensin-II and cyclooxygen-ase [24], and for interleukin [25] have been suggested in the pathophysiology of chronic fatigue stress and cancer disease is well known to be associated to inflammatory process [26,27]. Consequently, there is the theoretical hypothesis that massage would decrease pain partly by decreasing anti-inflammatory mechanisms in cancer pain.
Another important data corroborant to the analgesic effect of massage was the demonstration by SPECT that massage re-sulted in hyperfusion in the left post-central gyrus only, while in the control group it was found hyperfusion in four areas of the brain that correspond to the anticipation of pain, worry, motor control and response to painful stimuli. The so-called “pain matrix” represents a dynamic network of cortical and subcortical brain regions regularly activated by acute pain. This includes the somatosensory cortices (SI, SII), insular cor-tex, the cingulate cortex, prefrontal areas, amygdala, thalamus, brainstem and cerebellum. The subjective perception of pain is substantially influenced by context-dependent intracorti-cal modulations and the descending pain modulatory system. This system includes cingulo-frontal brain areas together with specific brainstem nuclei that can exert control over nocicep-tive input at the level of the dorsal horn of the spinal cord [7]. Recent studies support the view that a dysfunctional interac-tion between the ascending and descending pain system may contribute to the development or maintenance of chronic pain
Jacobs Publishers 6
Cite this article: Gabriela R Lauretti . The Effects of Massage Therapy: Validation by Clinical, Laboratorial and Single Photon Emission Cerebral Tomography in Randomized Patients with Cancer Pain. J J Physiother Exercise. 2016, 2(3): 021.
SPM
mip
[62,
-20,
36]
<
< <
SPM{T4}
giro pós central direito RM
SPMresults: .\paired t test Controles\matHeight threshold T = 3.75Extent threshold k = 20 voxels
Design matrix2 4 6
2
4
6
8
10
5
0
5
10
15
20
25

states. Here we demonstrated that patients who received dai-ly massotherapy during ten consecutive days, the only change observed by SPECT was the hyperfusion of the left post-central gyrus, related to somatosensory functions (vibration, touch and temperature); while the control group showed hyperfu-sion in four areas (correspondent to pain anticipation, motor control and response to painful stimuli. Nevertheless, there were no significant changes in the prefrontal or primary so-matosensory cortex in chronic pain. It resulted in a decrease of synaptic activity at thalamic level either from decreased ac-tivity in neurons projecting to that region and/or attenuated local neuronal firing. The authors demonstrated no secondary remote effects in cortex, indicating the importance of subcorti-cal mechanisms in central responses to chronic pain [28].
Finally, apart from clinical and image data, we also evaluated laboratorial data such as plasmatic noradrenaline levels. The biochemical and clinical response to massage in preterm in-fants was assessed, and blood samples were obtained for the determination of adrenaline, noradrenaline, and cortisol 45 minutes before the start of massage and approximately one hour after completion of massage. Cortisol, but not catechol-amine, concentrations decreased consistently after massage [29]. These data is in accordance to ours, where we have demonstrated that the noradrenaline level remained constant in the interventional group, while increasing in the control group. It could imply that the analgesic action of massother-apy would not be secondary to activation of descending pain pathways, but it would suggest be secondary to the decreased action of the sympathetic system, also in accordance to others [30], demonstrated indirectly by the absence of hyperfusion in brain areas related to anticipation of pain, motor control, anxi-ety and motor response to painful stimuli.
In conclusion, 10-daily massage was an effective adjuvant treatment for reducing pain VAS pain scores, decrease fatigue, increase comfort in men with bone-type cancer, data consis-tently reenforced by the maintenance of noradrenaline plas-matic level and absence of brain hyperfusion in areas correlat-ed to pain.
Acknowledgments
None of the authors has personal interest/involvement or po-tential/actual conflict of interest with, or the benefit of finan-cial support from any organization with financial interest in the subject matter.
References
1. Lee SH, Kim JY, Yeo S, Kim SH, Lim S. Meta-Analysis of Mas-sage Therapy on Cancer Pain. Integr Cancer Ther. 2015, 14(4): 297-304.
2. Cassileth BR, Vickers AJ. Massage therapy for symptom con-trol: outcome study at a major cancer center. J Pain Symptom
Manage. 2004, 28(3): 244-249.
3. Myers CD, Walton T, Small BJ. The value of massage thera-py in cancer care. Hematol Oncol Clin North Am. 2008, 22(4): 649-660.
4. Falkensteiner M, Mantovan F, Müller I, Them C: The use of massage therapy for reducing pain, anxiety, and depression in oncological palliative care patients: a narrative review of the literature. SRN Nurs. 2011:929868.
5. Wilkinson S, Barnes K, Storey L. Massage for symptom relief in patients with cancer: systematic review. J Adv Nurs. 2008, 63(5): 430-439.
6. MacDonald G. Massage therapy in cancer care: an overview of the past, present, and future. Altern Ther Health Med. 2014, 2: 12-5.
7. Somborski K, Bingel U. Functional imaging in pain research. Schmerz. 2010, 24(4): 385-400.
8. Di Piero V, Jones AK, Iannotti F, Powell M, Perani D et al. Chronic pain: a PET study of the central effects of percutane-ous high cervical cordotomy. Pain. 1991, 46(1): 9-12.
9. Peyron R, Laurent B, García-Larrea L. Functional imaging of brain responses to pain. A review and meta-analysis. Neuro-physiol Clin. 2000, 30(5): 263-288.
10. Wilkie DJ, Kampbell J, Cutshall S, Halabisky H, Harmon H et al. Effects of massage on pain intensity, analgesics and quality of life in patients with cancer pain: a pilot study of a random-ized clinical trial conducted within hospice care delivery. Hosp. 2000, 15(3):31-53.
11. Gecsedi RA. Massage therapy for patients with cancer. Clin J Oncol Nurs. 2002,6: 52-54.
12. Lauretti GR, Mattos AL. The clinical and laboratorial eval-uation of transdermal ketamine, fentanyl, clonidine or their combination in chronic low back pain. Coluna/Columna. 2009, 8(4): 434-440.
13. Bourgeois M, Louette B. Alcoholism and depression (Note apropos of a survey using Beck’s inventory. Ann Med Psychol. 1975, 1(15): 706-711.
14. Ferreira ASM, Lauretti GR. Study of the effects of masso-therapy on pain relief and improvement of quality of life in câncer pain under palliative care. Rev Dor. 2007, 8: 983-993.
15. Dion LJ, Engen DJ, Lemaine V, Lawson DK, Brock CG et al. Massage therapy alone and in combination with meditation for breast cancer patients undergoing autologous tissue recon-struction: A randomized pilot study. Ther Clin Pract Comple-ment. 2016, 23: 82-87.
Jacobs Publishers 7
Cite this article: Gabriela R Lauretti . The Effects of Massage Therapy: Validation by Clinical, Laboratorial and Single Photon Emission Cerebral Tomography in Randomized Patients with Cancer Pain. J J Physiother Exercise. 2016, 2(3): 021.
16. Noto Y, Kitajima M, Kudo M, Okudera K, Hirota K. Leg mas-sage therapy promotes psychological relaxation and reinforces the first-line host defense in cancer patients. J Anesth. 2010, 24:827-831.
17. Bao Y, Kong X, Yang L, Liu R, Shi Z et al. Complementary and alternative medicine for cancer pain: an overview of sys-tematic reviews. Evid Based Complement Alternat Med. 2014, 170396.
18. Wilkinson S, Barnes K, Storey L . Massage for symptom relief in patients with cancer: systematic review. J Adv Nurs. 2008, 63(5): 430-439.
19. Newby TA, Graff JN, Ganzini LK, McDonagh MS. Interven-tions that may reduce depressive symptoms among prostate cancer patients: a systematic review and meta-analysis. Psy-chooncology. 2015, 24(12): 1686-1693.
20. Çelebioğlu A, Gürol A, Yildirim ZK, Büyükavci M. Effects of massage therapy on pain and anxiety arising from intrathecal therapy or bone marrow aspiration in children with cancer. Int J Nurs Pract. 2015, 21(6): 797-804.
21. Miller L, Bansal R, Wickramaratne P, Hao X, Tenke CE et al. Neuroanatomical correlates of religiosity and spirituality: a study in adults at high and low familial risk for depression. JAMA Psychiatry. 2014, 71(2): 128-135.
22. Townsend CS, Bonham E, Chase L, Dunscomb J, McAlister S. A comparison of still point induction to massage therapy in reducing pain and increasing comfort in chronic pain. Holist Nurs Pract. 2014, 28: 78-84.
23. Yoopat P, Maes C, Poriau S, Vanwonterghem K. Thai tra-ditional massage: efficiency-assessment of three traditional massage methods on office workers: an explorative study. J Bodyw Mov The. 2014, 19(2): 246-252.
24. Kumar A, Singh B, Mishra J, Sah SP, Pottabathini R. Neu-roprotective mechanism of losartan and its interaction with nimesulide against chronic fatigue stress. Inflammopharma-cology. 2015, 23(6): 291-305.
25. Johnstone CN, Chand A, Putoczki TL, Ernst M. Emerging roles for IL-11 signaling in cancer development and progres-sion: Focus on breast cancer. Cytokine Growth Factor Rev. 2015, 26(5): 489-498.
26. Sarkar FH, Adsule S, Li Y, Padhye S. Back to the future: COX-2 inhibitors for chemoprevention and cancer therapy. Mini Rev Med Chem. 2007,7(6): 599-608.
27. Hugo HJ, Saunders C, Ramsay RG, Thompson EW. New In-sights on COX-2 in Chronic Inflammation Driving Breast Can-cer Growth and Metastasis. J Mammary Gland Biol Neoplasia. 2015, 20(3-4): 109-119.
28. Calenda E. Massage therapy for cancer pain. Curr Pain Headache Rep. 2006, 10: 270-274.
29. Acolet D, Modi N, Giannakoulopoulos X, Bond C, Weg W et al. Changes in plasma cortisol and catecholamine concen-trations in response to massage in preterm infants. Arch Dis Child. 1993, 68(1): 29-31.
30. Lee YH, Park BN, Kim SH. The effects of heat and massage application on autonomic nervous system. Yonsei Med J. 2011, 52(6): 982-989.
Jacobs Publishers 8
Cite this article: Gabriela R Lauretti . The Effects of Massage Therapy: Validation by Clinical, Laboratorial and Single Photon Emission Cerebral Tomography in Randomized Patients with Cancer Pain. J J Physiother Exercise. 2016, 2(3): 021.