jack perry strong, md boyd professor department of pathology
TRANSCRIPT

Atherosclesosis in Youth:The PDAY Study
Jack Perry Strong, MDBoyd Professor Department of Pathology

The Natural History of Atherosclerosis
The Early Aortic Lesions as seen in New Orleans
in the middle of the 20th Century*Russell L. Holman, Henry C. McGill, Jr., MD,
Jack P. Strong, MD and Jack C. Geer, MD
From the Department of Pathology, Louisiana State University School of Medicine and Charity Hospital of
Louisiana, New Orleans, LA
Reprinted from The American Journal of Pathology, 1958, XXXIV, No. 2, pp. 209-235

The Natural History of Coronary Atherosclerosis
Jack P. Strong, MD and Henry C. McGill, Jr., MD
From the Department of Pathology, Louisiana State University School of Medicine
New Orleans, LA
Reprinted from Vol. 40, No. 1, January 1962The American Journal of Pathology

Myocardial infarct
Cerebral infarct
Gangreneof extremities
AbdominalAortic
aneurysm
Natural History of Atherosclerosis
Clinical horizon
CalcificationComplication lesion – hemorrhage, ulceration, thrombosis
Fibrous plaque
Fatty streak
Age
in Y
ears
Pathology







The Value of Autopsy Studies of Atherosclerosis in
Human Subjects as We Approach the 21st Century
Study of Soldiers Killed in the Korean War Middle ofEarly Studies of Natural History in New Orleans 20th Century
International Atherosclerosis Project 1960’s
Community Pathology of Atherosclerosis in New Orleans 1970’s
Studies of Atherosclerosis and Risk Factors in Hisayama 1970’s-1980’sThe Akita Pathology Study
Comparison of Atherosclerosis in Tokyo, New Orleans and Oslo Nationwide Study of Atherosclerosis in Infants and Children and Young Adults in Japan 1980’s
Bogalusa Hearty Study- Atherosclerosis in Children and Youth Histological Classification of Coronary Atherosclerosis in Young Subjects 1980’s-1990’s
Pathobiological Determinants of Atherosclerosis in Youth 1980’s 1990’s

Coronary and Aortic Atherosclerosis in
Young Men from Tokyo and New Orleans
Toshiharu Ishii, William P. Newman III, Miguel A. Guzman, Yahuhiro Hosoda , Jack P. Strong
Laboratory Investigation 1986; 54:561-565

Coronary Atherosclerosis in New Orleans and Japan,
Men 25-44 Years of AgePercent Intimal Surface Involvement
with Atherosclerotic Lesions
NO Black NO White Japan0
10
20
Right Coronary Artery
Fatty StreaksRaised Lesions
NO Black NO White Japan0
10
20
Circumflex Left Coronary Artery
NO Black NO White Japan05
101520
Left Anterior Descending Coronary
NO Black NO White Japan05
101520
Combined Coronary Arteries

PDAYPathobiological Determinants of
Atherosclerosis in Youth
Nationwide study of atherosclerosis in autopsied persons,
15-34 years old, conducted by 14 cooperating centers.

PDAY Study Subjects
Males and females aged 15-34
Death due to external causes (accidents, homicides, suicides)
2876 cases collected

Institutions Participating in the Multicenter Cooperative Study, Pathobiological Determinants of
Atherosclerosis in YouthUniversity of Alabama
Birmingham
Albany Medical CollegeAlbany
Baylor College of MedicineHouston
University of ChicagoChicago
The University of IllinoisChicago
Louisiana State University Medical CenterNew Orleans
University of Maryland Baltimore
Medical College of Georgia Augusta
University of Nebraska Medical Center Omaha
The Ohio State University Columbus
Southwest Foundation for Biomedical Research
San Antonio
The University of Texas Health Science Center
San Antonio
Vanderbilt UniversityNashville
West Virginia State UniversityMorgantown

PDAY Methods of Evaluating Atherosclerosis
Visual estimate of surface involved by fatty streaks and raised lesions in Sudan-IV-stained arteries by three pathologists (LSU)
Computerized image analysis of lesions in photographs of arteries (OSU)
Computerized image analysis of histologic sections (OSU)

Risk Factors Measured in Autopsied Persons
Risk Factor Marker
• Serum lipoprotein cholesterol and apolipoprotein concentrations
• Smoking
• Blood pressure
• Diabetes mellitus
• Obesity
• DNA Polymorphisms
• Total cholesterol, HDL cholesterol, and apolipoproteins in post mortem serum
• Thiocyanate in post mortem serum
• Wall thickness of renal arteries
• Glycosylated hemoglobin in post mortem red blood cells
• Body mass index and panniculus adiposus
• RFLP’s in liver DNA


F8502532 Year
Old Black Male

F8851331 Year Old White Male

15-19
20-24
25-29
30-34
15-19
20-24
25-29
30-34
15-19
20-24
25-29
30-34
15-19
20-24
25-29
30-34
010203040
Thoracic Aorta
Raised LegionsFatty Streaks
15-19
20-24
25-29
30-34
15-19
20-24
25-29
30-34
15-19
20-24
25-29
30-34
15-19
20-24
25-29
30-34
0
20
40
60Abdominal Aorta
Raised LegionsFatty Streaks
15-19
20-24
25-29
30-34
15-19
20-24
25-29
30-34
15-19
20-24
25-29
30-34
15-19
20-24
25-29
30-34
0
10
20
30
Right Coronary
Raised LegionsFatty Streaks
Perc
en
t In
tim
al S
urf
ace
MalesWhite Black
FemalesWhite Black


Intimal Surface of Right Coronary Artery involved by Athersclerosis in 351 Males at
Two Risk Levels

Effects* on Percentage Total Surface Involvement of Abdominal Aorta, Adjusted
for other VariablesVariable Unit Effect
Age 5 years 5.0
Race Black-White 6.6
VLDL+LDL-C 45 mg/dl 5.4
HDL-C 20 mg/dl -3.1
Smoking Smoker-Nonsmoker 6.9
Apo B 40 mg/dl 3.9
Apo A-I 35 mg/dl -3.6
* Estimated from multiple regression analysis of 533 cases (except for Apo B and A-I 255 cases) all males – PDAY, 1990

Raised Lesions and Fatty Streaks in Three Arterial Segment for
Normal (N) Borderline (B) and Definite Hypertensive (H)
0
5
10
15
20
25
30
35
40
45
50
N B H N B H N B H
Fatty Streaks
Raised Lesions
Perc
en
t In
tim
al S
urf
ace
P ValuesTotal Lesions 0.9421 0.3116 0.0159Raised Lesions 0.0001 0.0001 0.0001
Aorta Right CoronaryThoracic Abdominal

Raised Lesions in Right Coronary Artery of 30-Year-Old White Males by Risk Factor Status
0
2
4
6
8
10
12
14
16
18
20
Perc
en
t S
urf
ace I
nvolv
ed PDAY, 1994
SmokingBlood Pressure
Cholesterol
No YesNormal
No YesHigh
No YesNormal
No YesHigh________________________
Normal
________________________
High

F3860430 Year Old Black Female

F716623 Year Old Black Male

Human Template – Half Aorta







PDAY Abdominal Aorta Sudan Probability
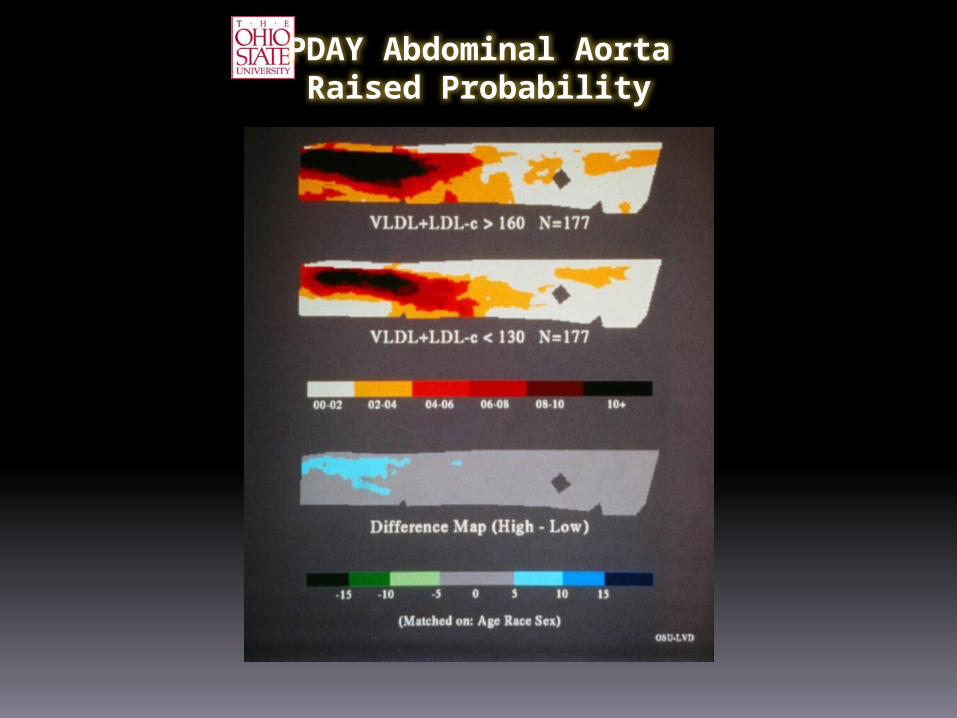
PDAY Abdominal AortaRaised Probability

PDAY Right CoronarySudan Probability

PDAY Right CoronaryRaised Probability

PDAY Abdominal Aorta Sudan Probability

PDAY Abdominal Aorta Raised Probability

PDAY Coronary ArterySudan Probability

PDAY Coronary ArteryRaised Probability

PDAY Abdominal AortaSudan Probability

PDAY Abdominal Aorta Raised Probability

PDAY Abdominal AortaSudan Probability

PDAY Abdominal Aorta Raised Probability

PDAY Right CoronarySudan Probability

PDAY Right CoronaryRaised Probability

PDAY Abdominal AortaSudan Probability

PDAY Abdominal AortaRaised Probability

PDAY Right CoronarySudan Probability

PDAY Right CoronaryRaised Probability

Atherosclerosis of Abdominal Aortaby Age and GlycohemoglobenAdjusted for Race and Sex
0
10
20
30
40
50
60
70
Fatty Streaks P = 0.752
Raised Lesions P = 0.025
Perc
en
t S
urf
ace I
nvolv
ed
Glycoemoglobin:
NormalHigh
15-19Age:
PDAY, 1994
Normal
High20-24
NormalHigh
25-29
NormalHigh
30-34
N = 1,309

Atherosclerosis of Right Coronary Artery by Age and GlycohemoglobenAdjusted for Race and Sex
0
5
10
15
20
25
30
35
40
45
50
Fatty Streaks P = 0.010
Raised Lesions P = 0.0003
Perc
en
t S
urf
ace I
nvolv
ed N = 1,275
Glycohemoglobin: NormalHigh
15-19
Age:
PDAY, 1994
Normal
High20-24
NormalHigh
25-29
NormalHigh
30-34

Atherosclerosis of Right Coronary Artery by Body Mass Index and Sex Adjusted for Race and Age
<25 25-30 >30 <25 25-30 >300
2
4
6
8
10
12
14
Fatty Streaks P = 0.0001
Raised Lesions P = 0.0045
Perc
en
t S
urf
ace I
nvolv
ed N = 1,455
BMI: _________________________Male
___________________________FemaleSex:
PDAY, 1994

APO E Isoforms
E2 Least common receptor binding domain: 112 CYS 158 CYS
E3 MOST COMMON 112 CYS 158 ARG
E4 112 ARG 158 ARG

0
50
100
150
200
147.3(107.6-201.7)
166.4(153.4-180.5)155.3
(132.4-185.8)
179.0(172.4-185.8)
188.2(78.4-198.5)
160.2(133.5-192.3)
APO E Genotype
Total Serum Cholesterol by APO E GenotypeAdjusted for Age and Race
Tota
l S
eru
m C
hole
ste
rol m
g/d
l) P = 0.03
N=3
N=45 N=1
2N=107 N=
9
N=223
E2 E2
E2 E3E2 E4
E3 E3E3 E4
E4 E4

Lesions in Abdominal Aorta by Apo E Genotype adjusted for age and Race
0
5
10
15
20
25
30
35
40
45
50
8.7(5.5-13.6)
20.517.4-24.0
21.516.2-28.5
30.127.8-32.5
33.529.8-37.6
27.019.5-37.3
APO E Genotype
Perc
en
t S
urf
ace
Involv
ed
P = 0.0001
E2 E2
E2 E3E2 E4
E3 E3E3 E4
E4 E4


Summary and Conclusions
Atherosclerosis begins in childhood with the appearance of aortic fatty streaks.
Coronary fatty steaks begin to form in adolescence
Most persons have coronary fatty streaks by the age 20-29 years.

In the PDAY study, the association of serum lipoprotein levels with atherosclerotic lesions in young persons 15-34 years of age supports the view that control the hyperlipoproteinemia will retard the progression of atherosclerosis in the young.

There is strong evidence for the effects of smoking on atherosclerosis in this young age group.
The association of a hypertensive index to clinically significant raised arterial lesions is also well established in this young age group, 15-34 years of age.
Elevated glycohemoglobin levels and obesity are associated with accelerated atherosclerosis in the third and fourth decades of life.

Control Programs to prevent coronary heart disease should be directed toward individuals in the twenties and thirties for maximum benefits
Early detection and control of hypercholesterolemia hypertension, hyperglycemia and obesity in young persons should reduce the risk of atherosclerotic disease later in life.
Dietary and other habits that retard atherosclerosis should be established in childhood.

The LSU PDAY Team Richard S. Vander Heide, MD,
PhD
Jack P. Strong, MD
Gray T. Malcom, PhD
Arthur W. Zieske, MD
Dana A. Troxclair, MD
Grace B. Athas, PhD
Cynthia J. Sprow, BS
Penelope H. Strenge, MS, MT
(ASCP)