(ix) glosso- sve: only 1 muscle stylopharyngeusteammotivation.in/onlinetest/backend/source/cns -...
TRANSCRIPT

Cranial Nerve Supply
(IX) Glosso- Pharyngeal
SVE: only 1 muscle – stylopharyngeus GVE: to parotid gland GVA: touch, pain & temperature from postr 1/3rd of the tongue, pharynx, carotid bodies & carotid sinus to the ganglion SVA: taste sensation from the postr 1/3rd and the circumvallate papillae of the tongue.
(X) Vagus SVE: (arise from nucleus ambiguous) supply muscles of pharynx & larynx : GVE: (pre-ganglionic parasympathetic fibers) to heart, lungs, GIT upto transverse colon GVA: carry sensations from pharynx, larynx, trachea, esophagus & from thoracic & abdominal viscera. SVA: taste sensations from posterior most part of the tongue & epiglottis GSA: skin of the external ear

Nuclei of cranial nerves
Cranial nerve
Cranial nerve Nuclei
I Olfactory Ant olfactory nucleus
II Optic Lateral geniculate nucleus
III Occulomotor Occulomotor nucleus, Edinger Westphal Nucleus
IV Trochlear Trochlear nucleus
V Trigeminal Chief, spinal & mesencephalic nucleus of trigeminal Trigeminal motor nucleus
VI Abducens Abducens nucleus
VII Facial SSN, NTS, spinal nucleus of V cn & motor nucleus
VIII Vestibulo-cochlear
Vestibular & cochlear nuclei
IX NA, ISN, NTS

Limbic System
(AN INTRO)
• The entire neuronal circuit that controls emotional behaviour & motivational drives
• Primarily concerned with emotional part of our life & is extensively concerned with memory.
• It is a system of cortical & sub cortical structures • One of the oldest part of our brain
(phylogenetically) • Limbic system & forebrain communicate by—
1. Medial forebrain bundle 2. Short pathways among reticular formation
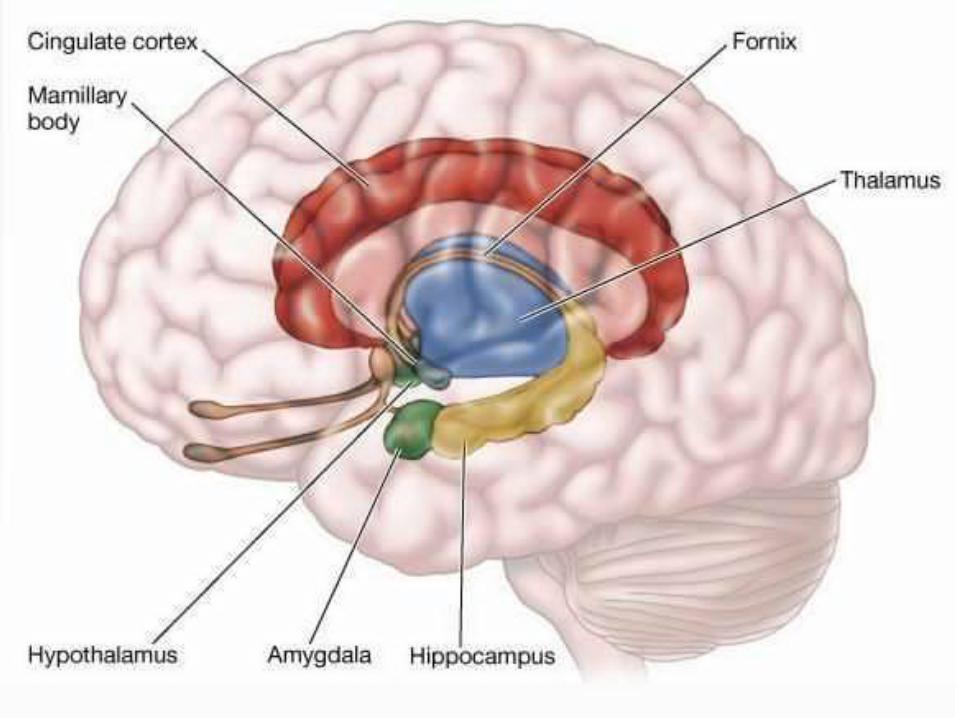




COMPONENTS OF THE LIMBIC SYSTEM
• Hypothalamus—located in the middle of the limbic system is considered as the key (central element) of the limbic system
• Sub-cortical limbic structures are : Amygdala
Septum area
Anterior nuclei of thalamus
Para- olfactory area
Portions of basal ganglia
Hippocampus

Limbic cortex
• Surrounds subcortical limbic areas. It is a ring of cerebral cortex composed of:
1. Cingulate gyrus
2. Orbitofrontal cortex
3. Parahippocampal gyrus
4. Uncus
5. Subcallosal gyrus
• Window through which limbic system sees the place of person in the world
• B/l ablation of amygdala leads to Kluver Bucy Syndrome, features are: 1. Loss of fear
2. Extreme curiosity
3. Forgets rapidly
4. Tendency to place every thing in mouth
5. Strong sex drive (tends to do sexual activity even with inanimate objects & animals )

• Almost all sensory experience activates some part of hippocampus.
• It then distributes signals to other part of the limbic system • It is channel through which incoming sensory signal can
initiate behavioural reactions for different purposes • It determines importance of incoming sensory signals • Plays a critical decision making role that the information is
likely to be committed to memory • Consolidation of memory—makes the mind to rehearse the
new information until it gets permanently stored (long term potentiation)
• Lesions l/t bilateral damage of hippocampus causes—anterograde amnesia
• Most anterior & most posterior area of hypothalamus: stimulate sexual drive
• Fear: produced by stimulation of hypothalamus & amygdaloid nuclei
• Anxiety: anterior end of temporal lobes
• Violent rage: destruction of ventromedial nuclei & septal nuclei
• Reward/satisfaction/approach centres: located along the course of MFB especially in lateral & ventromedial nucleus of hypothalamus

Emotions
• There are 2 aspects of emotions—sensory & motor
• Sensory aspects are—cognition, rage & conation • Sensory aspect of emotion develop in limbic
system (part of the brain that consists of rim of cortical tissue around the hilum of cerebral hemisphere + deep structures)
• Expressive side are—somatic (act of beating) & autonomic (via sympathetic & parasympathetic)
• Expressive aspect develops only in hypothalamus & amygdala

• Concerned with expressive side of emotions
• It links limbic system with hypothalamus & thalamus
• Hippocampus (Fornix)Mamillary body (hypothalamus)anterior thalamic nucleus cingulate gyrus hippocampus

FUNCTIONS OF THE LIMBIC SYSTEM
1. Olfaction
2. Regulation of endocrine glands
3. Regulation of autonomic activities
4. Regulation of food intake
5. Regulation of sexual functions
6. Role in emotional state
7. Role in memory
8. Role in motivation

Memory
• Defined as
1. ability to recall past experiences & information
2. Retention of learned material.
• Classified as :
1. Short term
2. Long term

• Short term memory:
1. Recalling the events that happened very recently (hours or days)
2. Its one form is called working memory (concerned with recollection of past experience for a very short period to execute a task)
• Long term memory: recalling the events for months/years/lifetime

HYPOTHALAMUS
TEMPERATURE REGULATION
FOOD INTAKE
THIRST
HORMONE REGULATION
SEXUAL BEHAVIOUR
DEFENSE
CIRCADIAN RHYTHM


FUNCTIONS ACTION/CENTER NUCLEI/PARTS INVOLVED
Secretion of posterior pituitary hormones
Oxytocin ADH
PV SO
Control of Adrenal Cortex CRH PV
Control of Adrenal Medulla Catecholamines during emotion
Post & DM
ANS regulation Sympathetic Parasympathetic
Post & lat Ant
Heart rate regulation Acceleration Inhibition
Post & lat Preop & Ant
BP regulation Pressor effect Depressor effect
Post & lat Preop
Body temperature regulation Heat gain centre Heat loss centre
Posterior hypothalamus Pre Op of Anterior hypothalamus
Hunger & food intake regulation Feeding centre Satiety centre
Lat VM
Sleep & wakefulness regulation Sleep Wakefulness
Ant hypothalamus Mamillary body
Behaviour & emotion regulation Reward Punishment
VM Post & lat

Regulation of Hunger
• Hunger, satiety & appetite are regulated by feeding & satiety centre.
1. Glucostatic mechanism
2. Lipostatic mechanism
3. Peptide mechanism
4. Hormonal mechanism
5. Thermostatic mechanism

• Following peptides stimulate food intake:
1. Ghrelin secreted by stomach during fasting.
2. Neuropeptide Y
• Following peptides decrease food intake:
1. Leptin (secreted from adipocytes)
2. Peptide YY

Role of Leptin
• Leptin is a peptide secreted by fat cells. It inhibits feeding centre after passing through BBB.
• It inhibits secretion of Neuropeptide-Y (secreted by the SI, medulla & hypothalamus stimulates food intake).
• It stimulates the secretion of POMC (Pre-opio melanocortin-secreted by hypothalamus, lungs, GI tract & placenta). POMC inhibits food intake.
• Leptin acts via “LepRb”- only active receptor present in nuclei of hypothalamus.

Hormones inhibiting food intake
• Glucagon
• Oxytocin
• Cholecystokinin
• PP
• Somatostatin

REGULATION OF WATER BALANCE Thirst Mechanism
Water loss decreases ECF
volume & increases osmolality
Osmoreceptors in thirst centre of
lateral hypothalamus
stimulated
Thirst centre stimulated, person
feels thirsty & drinks water

REGULATION OF WATER BALANCE ADH Mechanism
Water loss decreases ECF
volume & increases osmolality
SO nucleus stimulated & ADH
released
Facilitated reabsorption of water in renal
tubules

Role in behaviour & emotional change
• Reward centre : medial forebrain bundle & VM nucleus of hypothalamus.
• Punishment centre : posterior & lateral centre of hypothalamus
• If a person, while doing something, feels rewarded he or she continues to do so & vice-versa.
• Rage: Violent & aggressive emotional expression with anger • Sham rage: means false rage, occurs in certain pathological
conditions. An extreme emotional condition that resembles rage. It is due to release of hypothalamus from the inhibitory influences of cerebral cortex

• Role in response to smell
1. Posterior hypothalamus + hippocampus + brain stem nuclei are autonomic responses of the body to smell.
2. Responses include---feeding activities, fear, excitement, pleasure.
• Role in circadian rhythm Suprachiasmatic nucleus of hypothalamus is connected to retina by
retino-hypothalamic fibers. Through efferent fibers it send signals to different parts and maintain the circadian rhythm of sleep, hormonal secretion, thirst, hunger, appetite.
When the body is exposed to a new pattern of daylight, the biological clock is reset, provided the new pattern is regular. Accordingly the circadian rhythm also changes.

NREM Sleep/Orthodox sleep/Slow wave sleep
REM Sleep/Paradoxical sleep
70 to 80 % sleep (regular respiration, low BP, low HR)
20 to 30 % of sleep (irregular respiration, variable BP & HR, arrythmia +nt)
•Stage I (dozing) First & lightest stage of sleep (θ wave) •Stage II (unequivocal) SLEEP DEEPENS Characterised by sleep spindle & K-complexes (easily evoked) •Stage III (deep sleep transition) δ-wave first appear & K-complexes (evoked with strong stimuli) •Stage IV (cerebral sleep) Predominantly δ-wave
•Light phase of sleep but arousal is difficult •QMixed frequency, low amplitude waves on EEG (predominantly β-like activity ) •Also called desynchronised sleep / active sleep •Called as PARADOXICAL SLEEP as EEG similar to awake state BUT difficult to awaken the patient
Called dreamless sleep BUT dreams occur but not registered to memory
•Dreaming (seen 80% can be recalled) & associated with more muscular activity

Sleep disorders during NREM IV Sleep disorders of REM
Sleep walking (Somnambulance) Night mares
Sleep talking (Somnaloquy) Narcolepsy
Night terror (Pavor nocturnus) Nocturnal penile tumescence
Bruxism (tooth grinding)
Nocturnal eneuresis

• An EEG waveform (HIGH VOLTAGE SPIKES) that appear during stage 2 of NREM sleep
• Considered as largest event in healthy human EEG
• Occur roughly every 1 to 1.7 minutes • Often followed by burst of sleep spindles • Has 2 proposed functions:
1. Known to protect sleep (suppressing cortical arousal in response to stimuli)
2. Engage in information processing (consolidation of sleep)

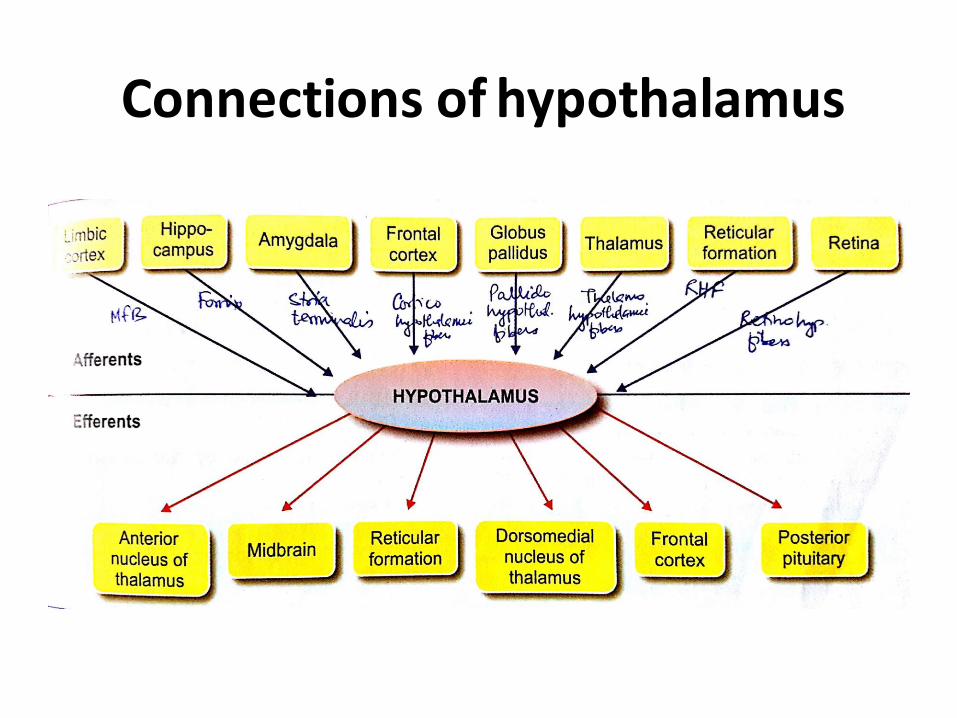
Connections of hypothalamus

Effects of lesions in hypothalamus
Features after the lesion Site of the lesion
Disturbance in carbohydrate & fat metabolisms
Lateral, arcuate & ventromedial nuclei
Disturbance in sleep Mamillary body & ant hypothalamus
Disturbance in sympathetic & parasympathetic functions
Posterior, lateral & anterior nuclei
Emotional manifestations leading to sham rage
Ventromedial & posterolateral parts
Disturbance in sexual functions Mid-hypothalamus

Clinical manifestations
• Diabetes insipidus • Dystrophia adiposogenitalis (Frohlich’s syndrome) obesity + sexual infantilism + dwarfism • Kallmann syndrome Anosmia/hyposmia + hypogonatrophic-hypogonadism • Laurence-moon-biedl syndrome moon face + obesity + polydactylism + mental retardation • Narcolepsy sudden attack of uncontrollable desire for sleep & person falls
asleep. Duration of sleep may be few seconds to 20 mins • Cataplexy After sudden uncontrollable outburst of emotions (anger, fear,
excitement) person becomes completely exhausted with muscular weakness & falls asleep

Brain stem (Medulla + pons + midbrain)
• MEDULLA OBLONGATA
1. Forms the main pathway for the ascending & descending tracts of spinal cord.
2. Has many important centres:
• Respiratory centre (DRG & VRG)
• Vasomotor centre (for BP & HR regulation)
• Deglutition centre (regulates pharyngeal & esophageal stage)
• Vomiting centre
• Superior & inferior salivatory nucleus (control saliva secretion)
• Cranial nerve nuclei (XII, XI, X & few nuclei of VIII & V

PONS • Bridge between medulla & midbrain.
• It forms the pathway that connects cerebral cortex & cerebellum.
• Pyramidal tracts pass through it.
• Fibers of X, IX, VII & V cranial nerves join the medial leminiscus in pons.
• Nuclei of VIII, VII, VI & V cranial nerves are located in pons
• It contains the pneumotaxic & apneustic centre for regulation of respiration.
• Contain vestibular nuclei
NOTE: There are 4 vestibular nuclei (Superior, inferior, lateral & medial). Medial & inferior vestibular nuclei

MIDBRAIN
• Consists of --- (A) Tectum (B) Cerebral Peduncles • Tectum has 2 structures --- superior colliculus &
inferior colliculus • Superior colliculus 1. Small & important centre for reflexes. 2. Through tectospinal tract controls the
movement of eyes, head, trunk & limbs in response to visual impulses.
3. Centre for light reflex: efferent fibers from superior colliculus reach III c.n. nuclei & cause constriction of pupil
4. Receives afferent from optic tract (helps in the integration of optical & postural reflexes).

• Inferior colliculus:
1. Centre for auditory reflexes. Consists of single layer of neurons to which the lateral leminiscus (auditory fibers) synapse.
2. Stimulation of this produces reflex vocalisation.

T.S. Of midbrain

TS of midbrain at the level of Inferior colliculus

TS of midbrain at the level of Superior colliculus

CEREBRAL PEDUNCLES
• Include: Basis pedunculi, Substantia nigra & tegmentum.
• Basis pedunculi contain:
1. Temporopontine, parietopontine & occipitopontine fibers in lateral 1/6th.
2. Corticonuclear and corticospinal fibers (of pyramidal tract) in lateral 2/3rd.
3. Frontopontine fibers in medial 1/3rd.

CEREBRAL PEDUNCLES
• Substantia nigra: situated below the red nucleus & considered as one of the parts of BG.
• Tegmentum 1. Considered as the upward continuation of reticular
formation in pons. 2. Comprises of 3 decussations & red nucleus • Decussations in tegmentum i. Superior cerebellar decussation: formed by fibers
from cerebellum & other parts of the CNS (mainly from dentate n.)
ii. Dorsal tegmental decussation (of Myenert): crossing of medial longitudinal bundle formed by efferent fibers from III, IV & VI c.n.
iii. Ventral tegmental decussation (of Forel): due to crossing of rubrospinal tracts from either side.

RED NUCLEUS
• Large oval or round mass of gray matter extend between superior colliculus & hypothalamus.
• Has 2 parts:
1. Nucleus magnocellularis: formed of large cells. Fibers from this form rubrospinal & rubrobulbar tracts. It receives fibers from motor cortex (area 6) – corticorubral fibers & from Globus pallidus – pallidorubral fibers.
2. Nucleus parvocellularis: formed of small cells. Fibers from this form rubroreticular tract. It receives fibers from dentate nucleus of opposite side (dentatorubral/cerebellorubral fibers)
Functions of RED NUCLEUS
1. Control of muscle tone: due to its connections with cerebellum, VA & skeletal muscles.
2. Control of complex muscle movements: integrates various impulses received from many important areas of brain.
3. Control of movements of eyeball: through its efferent connections with nuclei of c.n. controlling eye movements
4. Control of skilled movements: by its connections with spinal cord & cerebral

Thalamus A large ovoid mass of gray matter situated bilaterally in
diencephalon Both thalami form 80% of diencephalon FUNCTIONS 1. Relay centre 2. Center for processing of sensory information 3. Center for determining quality of senses 4. Center for sexual sensations 5. Role in arousal & alertness reactions (due to connections with nuclei of reticular
formation) 6. Center for reflex activity 7. Center for integration of motor activity (due to connections with cerebellum & basal ganglia)

• Thalamus forms the relay center for the sensations.
• Almost all the sensations reach thalamic nuclei† (especially VPL n.) get processed in the thalamus reach cerebral cortex through thalamocortical fibers
• † Due to this thalamus is also called “functional gateway to cerebral cortex”.
• Thalamus determines the quality of sensations. It determines the type, location & other details of the sensation (discriminative nature).
• Capacity to determine whether sensation is

NUCLEI OF THALAMUS

CONNECTIONS OF THALAMUS

MAIN THALAMIC CONNECTIONS
AFFERENT FIBERS ON LEFT & EFFERENT ON RIGHT (NEXT SLIDE)




THALAMI & III VENTRICLE (AFTER REMOVING OVERLYING TELA CHOROIDEA)

RELATION OF THALAMUS (IN CORONAL SECTION)

Thalamic syndrome 1. Loss of sensations
2. Astereognosis
3. Ataxia (sensory ataxia: due to loss of kinesthetic sensations)
4. Thalamic phantom limb (pt unable to locate the position of limb with closed eyes)
5. Anosognosia (lack of awareness & denial of existence of any neurological disease)
6. Spontaneous pain & thalamic over reaction
7. Involuntary movements (athetosis, chorea & intention tremor)
8. Thalamic hand or athetoid hand (abnormal attitude of hand in thalamic lesions – moderate flexion at wrist &

Reticular formation

Reticular formation
• Located in central portion/core of the brain stem extends down into spinal cord (cervical region) & upwards upto thalamus & sub-thalamus.
• It is diffused ill-defined mass of neurons forming an ill-defined network or reticulum.
• Has 5 groups of nuclei: raphe, paramedian, lateral, medial & intermediate group
• Based on functions it is divided into 2 systems:
1. Ascending reticular activating system (ARAS)
2. Descending reticular system

ARAS-functioning
• Impulses of all the sensations reach cerebral cortex through 2 channels:
1. Classical sensory pathway
2. ARAS
Classical/Specific sensory pathway:
o Pathways which transmit the sensory impulses from receptors to cerebral cortex VIA thalamus
o E.g. Sound impulses reach auditory cortex via thalamus

ARAS/non-specific sensory pathway:
• All sensory pathways send collaterals to ARAS. These collaterals project in diffused areas of ARAS.
• Also receives impulses from spinal cord directly (by spinoreticular tract).
• ARAS sends the impulses to almost all the areas of cerebral cortex & other parts of the brain, hence called non-specific.
• This non-specific projections of ARAS into the cortex is responsible for arousal, alertness & wakefulness.
• The classical/specific sensory pathways carry sensations of only particular sensation whereas the impulses transmitted via ARAS cause generalised activation of almost all areas of

Descending reticular system Descending facilitatory
RS
(in upper & lateral ret formation)
Facilitation of somatomotor
activities
Facilitation of vegetative functions
Descending inhibitory RS
(in lower & medial ret formation)
Control of somatomotor
activities
Control of vegetative functions

Descending facilitatory RS
• Facilitation of somatomotor activities:
1. maintains muscle tone by exciting gamma motor neurons in spinal cord.
2. Facilitates the movement of the body.
3. Wakefulness and alertness by activating the ARAS
• Facilitation of vegetative functions:
1. Center for facilitation of autonomic functions – cardiac function, BP, respiration, GI function & body temperature

Descending inhibitory RS
• Control of somatomotor activities:
1. Receive signals from the BG inhibits gamma motor neurons in spinal cord & decrease muscle tone.
2. Smoothness & accuracy of movements.
3. Controls reflex movements
• Control of vegetative functions:
1. Center for inhibition of autonomic functions – cardiac function, BP, respiration, GI function & body temperature

SPINAL CORD • Cylindrical shaped, 45 cm long, loosely lying
in the vertebral canal & is covered by all meninges
• Has 2 spindle shaped enlargements – cervical & lumbar (innervate upper & lower extremities)
• Has 31 segments (C8T12L5S5Co1)
• Terminal part is called Conus medullaris
• Lumbar & sacral nerves form Cauda equina


• Carry various sensations to the brain.
• The pathways of these sensations involve following neurons:
1. First order neurons: receive sensory information from receptors sensory neuron in posterior gray horn
2. Second order neurons: present in posterior gray horn & fibers from these form the ascending tracts of spinal cord
3. Third order neurons: are in the sub-cortical area. Fibers from these carry impulses from sub-

SITUATION TRACT FUNCTION
Anterior white column
Ant spinothalamic t. Crude touch
Lateral white column
Lateral spinothalamic t. Pain & temperature
Ventral spinocerebellar t. Sub-conscious kinesthetic sensations
Dorsal spinocerebellar t.
Spinotectal tract Spinovisual reflex
Fasciculus dorso-lateralis Pain & temperature
Spinoreticular tract Consciousness & awareness
Spino-olivary tract Proprioception
Spinovestibular tract Proprioception
Posterior white column
Fasciculus gracilis (Tract of Goll) Fine touch, Vibratory sensation
Tactile localisation, Tactile discrimination, Conscious kinesthetic sensation Stereognosis
Fasciculus cuneatus (Tract of Burdach)

Descending tracts of spinal cord
• These contain motor fibers arising from brain & descend down in spinal cord.
• These are of 2 types:
1. Pyramidal (ant & lat corticospinal tracts)
2. Extra-pyramidal i. Medial longitudinal fasciculus
ii. Ant & lat vestibulospinal
iii. Reticulospinal
iv. Tectospinal
v. Olivospinal
vi. Rubrospinal

BROWN SEQUARD SYNDROME
Tract Clinical effect
Ipsilateral pyramidal tract involvement
Ipsilateral loss of 1. motor power 2. Plantar extensor reflex (+ve Babinski) 3. Brisk tendon reflex
Dorsal/posterior column involvement
Ipsilateral loss of 1. Vibration sense 2. Joint position (proprioception) 3. Fine touch
Spinothalamic tract involvement
Contralateral loss of 1. Crude touch 2. Pain 3. Temperature

Extra-pyramidal tracts Tract Origin Function
Medial longitudinal fasciculus
Vestibular nucleus Reticular formation Superior colliculus & cells of cajal
Coordination of reflex ocular movements Integration of movements of eye & neck
Ant vestibulospinal tract
Medial Vestibular nucleus Maintenance muscle tone & posture
Maintenance of position of head & body during acceleration Lat vestibulospinal
tract
Lateral Vestibular nucleus
Reticulospinal tract Reticular formation of pons & medulla
Coordination of voluntary & reflex movements Control of muscle tone Control of respiration & diameter of blood vessels
Tectospinal Superior colliculus Control of movement of head in response to visual

FEATURES UMN LESION LMN LESION
Neurons Pyramidal cells & their axons
Anterior horn cells & further
Muscle atrophy No marked
Fasciculations No Common
Tone Increased (spasticity) Lost (flaccidity)
Clonus Present Absent
Tendon jerks Exaggerated Lost
Babinski sign Present Absent
Superficial abdominal reflex
Lost Lost only when particular neuron supplying the muscle is lost
Babinski reflex/Plantar response
• Infants are not neurologically mature & show babinski response
• With time as the infant grows it disappears & should never return under normal circumstances
• Babinsky reflex present after the age of infancy is abnormal and is a sign of trouble to pyramidal tract of the person
• METHOD: elicited by stroking the external portion of the sole starting from back of the heel to the root of toes. If big toe goes up,

Pyramidal lesion Extra-pyramidal lesion
Involuntary movements

Motor neuron disease
• Characterised by degeneration of motor neuron either upper motor, lower motor or both
• It can be classified as : – Chronic
• UMN+LMN : Amyotrophic lateral sclerosis
• UMN alone: Primary lateral sclerosis
• LMN alone: Progressive muscle atrophy
– Acute • Poliomyelitis
• Herpes zoster
• Cox sackie virus

DISEASES OF THE SPINAL CORD
SYRINGOMYELIA
• Due to (1)overgrowth of neuroglial cells accompanied by (2)cavity formation. The cavity is first formed near the central canal of gray matter which then expands and involves the surrounding white matter to variable degree.
• Lower cervical & upper thoracic regions are affected the most.
• Loss of pain - temperature sensations & muscular weakness

Tabes Dorsalis
• Slow degeneration of neural tracts primarily in dorsal column of the spinal cord affecting both sensory & motor functions of spinal cord
• Cause: demyelination due to advanced syphilis infection
• A late manifestation of untreated syphilis (tertiary syphilis)
• Characterised by triad of gait unsteadiness, lightning pains & urinary incontinence
• Features 1. Initially there is exaggeration
of pain sensation 2. Later on impairment & loss
of all sensations 3. Due to loss of sensations
movements of joints become uncontrolled – Charcot’s Joints
4. Osteoarthritis 5. Both superficial & deep
reflexes are lost 6. Ataxia, stamping gait 7. Atonic bladder (micturition
reflex is lost) - incontinence
Multiple sclerosis
• A chronic progressive inflammatory disease characterised by demyelination in brain & spinal cord
• Immune system attacks the myelin sheath
• Features :
1. Tremor, fatigue & muscle spasms
2. Speech difficulty
3. Bladder bowel dysfuntion
4. Emotional outburst
5. Short term memory loss
6. Complete blindness

Hemisection of spinal cord (Brown Sequard Syndrome)
• Ipsilateral involvement of corticospinal tract: ipsilateral loss of motor power
• Ipsilateral involvement of posterior column:
ipsilateral loss of joint position & vibratory sensations
• Contralateral involvement of spinothalamic tract: contralateral loss of crude touch, crude pressure, pain & temperature sense.
Fibers of the spinothalamic tract may ascend 1 or 2 segments & then cross to opposite side.

Proprioceptors
• Detect movement & change in position of different parts of the body
• Also termed kinesthetic receptors
• Situated in – labyrinth, muscles, tendons, joints, ligaments & fascia
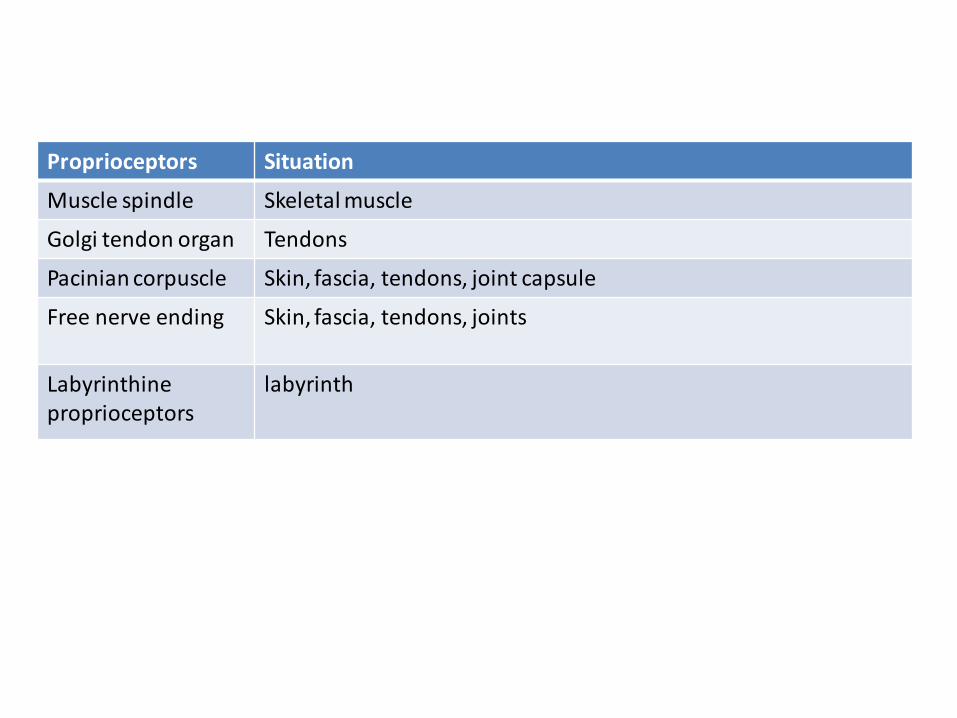
Proprioceptors Situation
Muscle spindle Skeletal muscle
Golgi tendon organ Tendons
Pacinian corpuscle Skin, fascia, tendons, joint capsule
Free nerve ending Skin, fascia, tendons, joints
Labyrinthine proprioceptors
labyrinth

Muscle spindle
• A central bulged portion with 2 tapering ends
• Each muscle spindle has 5 to 12 intrafusal muscle fibers enclosed by a connective tissue capsule
• Central portion of intrafusal fibers acts only as receptor & does not contract
• There are 2 types of intrafusal fibers: nuclear bag & nuclear chain fibers
• Forms receptor organ for stretch reflex & plays an important role in maintaining muscle tone

• Present in the tendon at the attachment of extrafusal fibers
• Formed by group of nerve endings covered by a CT capsule
• During powerful contractions tension in the muscle increases & GTO is stimulated to discharge impulse carried by Ib sensory neuron inhibitory interneuron contraction of muscle is inhibited
• Inverse stretch reflex

Pacinian corpuscle
• Situated in deeper layers of the skin, fascia, tendon & joint capsule
• They determine the joint position
• It is rapidly adapting receptor – phasic receptor

Free nerve endings
• Receptor for pain sensation
• Situated in skin, muscle, tendon, fascia & joints
• It also sends information about joint position to the CNS
• It is slowly adapting receptor – tonic receptor


Visual pathway
