it scars': meaning making and psychological impacts of
TRANSCRIPT
University of Calgary
PRISM: University of Calgary's Digital Repository
Graduate Studies The Vault: Electronic Theses and Dissertations
2017
"It Scars": Meaning Making and Psychological
Impacts of Parental Feeding Control
Brun, Isabel
Brun, I. (2017). "It Scars": Meaning Making and Psychological Impacts of Parental Feeding Control
(Unpublished master's thesis). University of Calgary, Calgary, AB. doi:10.11575/PRISM/26687
http://hdl.handle.net/11023/3937
master thesis
University of Calgary graduate students retain copyright ownership and moral rights for their
thesis. You may use this material in any way that is permitted by the Copyright Act or through
licensing that has been assigned to the document. For uses that are not allowable under
copyright legislation or licensing, you are required to seek permission.
Downloaded from PRISM: https://prism.ucalgary.ca

UNIVERSITY OF CALGARY
“It Scars”: Meaning Making and Psychological Impacts of Parental Feeding Control
by
Isabel Brun
A THESIS
SUBMITTED TO THE FACULTY OF GRADUATE STUDIES
IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE
DEGREE OF MASTER OF SCIENCE
GRADUATE PROGRAM IN EDUCATIONAL PSYCHOLOGY
CALGARY, ALBERTA
JULY, 2017
© Isabel Brun 2017

ii
Abstract
Given the negative physiological and psychosocial outcomes associated with childhood obesity,
it is no wonder that parents may want to utilize parental feeding control practices in order to
promote weight loss, or prevent weight gain, in their children. However, regardless of parents’
best intentions, parental feeding control practices have been found to have counterproductive
effects on children’s eating behaviours and weight status. Despite these findings, minimal
research has been conducted to examine how these parental feeding control practices are
subjectively experienced by children. As such, the current study explored perceived meaning
making and psychological impacts of parental feeding control practices through constructivist
grounded theory methods. Results from the preliminary constructivist grounded theory indicate
that individuals face lasting negative meaning making (e.g., viewing self-worth as contingent on
weight), psychological (e.g., fearing weight gain), and behavioural (e.g., engaging in
maladaptive eating behaviours) impacts as a result of experiencing parental feeding control
practices during their childhoods. Findings have implications for counselling and future
research.
Keywords: parental feeding control practices, childhood overweight and obesity,
constructivist grounded theory

iii
Acknowledgements
This thesis would not have been possible without the help, guidance, and support of
several individuals. First and foremost, I would like to thank my advisor, Dr. Shelly Russell-
Mayhew, for her tremendously helpful support and guidance throughout this project. I am
incredibly grateful to have you as my advisor. To my student mentor, Kirsten, thank you for
being my cheerleader. Your enthusiasm for this project, as well as your helpful feedback, has
been invaluable in shaping this project. I would also like to thank my partner, Stephane, for his
unwavering love and support. You have kept me sane throughout this completely insane process
and I could not have done this without you. To my baby dog, Piper, thank you for keeping me
company during the writing process, and for giving me puppy cuddles and kisses when I was
feeling stressed out. Thank you to my fabulous cohort for their encouragement. The supportive
environment we shared made this experience a truly enjoyable one. To my exam committee
members, Dr. Tom Strong and Dr. Janet Groen, thank you for all your helpful feedback. I would
also like to thank the rest of the Counselling Psychology faculty for making my time at
University of Calgary incredibly valuable – thank you. To my long-distance friends and family,
thank you for always supporting and believing in me. I would also like to extend a big thank you
to all of the employees at Sorso for keeping me fed and caffeinated throughout the writing
process. Finally, thank you to the wonderful women who participated in my study. This project
would not have been possible without your candour and vulnerability.

iv
Table of Contents
Abstract ........................................................................................................................................ ii
Acknowledgements ..................................................................................................................... iii
Table of Contents ........................................................................................................................ iv
List of Tables ............................................................................................................................ viii
List of Figures and Illustrations .................................................................................................. ix
Chapter One: Introduction ........................................................................................................1
Parental Feeding Control Practices ...................................................................................1
Personal Relevance ...........................................................................................................2
The Current Study.............................................................................................................4
Overview of Thesis Chapters ............................................................................................4
Chapter Two: Literature Review ..............................................................................................6
Childhood Overweight and Obesity Rates and Consequences .........................................6
Prevalence Rates ...................................................................................................6
Consequences of Obesity ......................................................................................7
Physiological Consequences ........................................................................8
Psychosocial Consequences .........................................................................9
Factors Contributing to Childhood Obesity .......................................................10
The Current Food Environment .................................................................11
Multidimensional Framework....................................................................11
Parenting Factors .......................................................................................12
Parenting and Feeding .....................................................................................................13
Parenting .............................................................................................................13
Parenting Styles .........................................................................................13
Parenting Dimensions ................................................................................14
Parenting Practices .....................................................................................15
Parental Feeding ..................................................................................................15
Feeding Styles ............................................................................................15
Parental Feeding Practices and Control .....................................................16
Covert and Overt Feeding Control Practices ....................................17
Relationships between Feeding Styles and Feeding Practices ...................17

v
Impacts of Parental Feeding Control Practices ...............................................................18
Children’s Self-Regulation of Food Consumption ..............................................18
Children’s Food Preferences and Weight Status .................................................19
Impacts of Covert versus Overt Feeding Control Practices ................................20
Factors that Predict the Use of Parental Feeding Control Practices ...............................21
Parental Factors ...................................................................................................21
Child Factors .......................................................................................................22
Multidirectional Model .......................................................................................23
Summary .........................................................................................................................24
Current Study ..................................................................................................................25
Conclusion ......................................................................................................................26
Chapter Three: Methodology ..................................................................................................27
Grounded Theory ............................................................................................................27
Traditional Grounded Theory Methodology .......................................................28
The Evolution of Grounded Theory ....................................................................29
Constructivist Grounded Theory Methodology ..................................................30
Rationale for Constructivist Grounded Theory Methodology ............................31
Procedures .......................................................................................................................33
Participant Recruitment .......................................................................................33
Data Collection and Analysis ..............................................................................34
Interviews ...................................................................................................35
Grounded Theory Methods and Data Analysis ...................................................36
Questioning ................................................................................................36
Theoretical Sampling .................................................................................37
Constant Comparison Method ...................................................................37
Coding ..............................................................................................38
Memo Writing and Reflexivity ..................................................................39
Theoretical Sensitivity ...............................................................................40
Ethical Considerations .........................................................................................40
Evaluating Grounded Theory ..........................................................................................41
Strategies for Evaluation .....................................................................................42
vi
Thick Descriptions .....................................................................................42
Triangulation ..............................................................................................42
Chapter Summary............................................................................................................43
Chapter Four: Results ..............................................................................................................44
Participants ......................................................................................................................44
Development of Themes and Categories ........................................................................47
Constructivist Grounded Theory Data Analysis Procedures Revisited ..............47
The Constructivist Grounded Theory .............................................................................48
Identified Core Concepts, Themes, and Sub-Themes .........................................48
Identified Dynamic Processes – The Theoretical Model ....................................50
Making Meaning of Parental Feeding Control ....................................................52
Perceiving Parental Motivation for Feeding Control .................................52
Appearance and Child’s Future Success ..........................................53
Weight Stigma and Bullying ............................................................54
Health ...............................................................................................54
Internalizing Parental Messages about Weight ..........................................55
Viewing Self-Worth as Contingent on Weight ..........................................57
Experiencing Psychological Impacts ..................................................................59
Becoming Self-Conscious of Weight ........................................................59
Feeling Guilt about Eating .........................................................................61
Fearing Weight Gain ..................................................................................62
Experiencing Behavioural Impacts .....................................................................64
Engaging in Maladaptive Eating Behaviours ............................................64
Restricting ........................................................................................64
Bingeing and Engaging in Compensatory Eating Behaviours .........65
Developing a Long-Lasting Preoccupation with Weight ....................................68
Seeing Parental Feeding Control Practices as Unhelpful ....................................70
Offering advice ..........................................................................................70
Summary of the Constructivist Grounded Theory ..........................................................72
Chapter Five: Discussion ..........................................................................................................74
Contributions to the Literature ........................................................................................75

vii
Contributions to the Feeding Literature ..............................................................76
Contributions to the Weight Stigma and Weight Bias Literature .......................77
Weight Stigma Literature ...........................................................................77
Internalized Weight Bias Literature ...........................................................79
Consequences of Weight Stigma and Internalized Weight Bias ......80
Consequences of Weight Stigma ............................................80
Consequences of Internalized Weight Bias ............................80
Intergenerational Internalized Weight Bias ............................81
Contributions to the Childhood Obesity Treatment Literature ...........................82
Implications for Counselling Psychology .......................................................................84
Prevention and Treatment Implications ..............................................................85
Strengths and Limitations ...............................................................................................86
Future Research ..............................................................................................................88
Conclusion ......................................................................................................................90
References ..................................................................................................................................93
Appendices ...............................................................................................................................118
Appendix A: Recruitment Poster ..................................................................................118
Appendix B: Recruitment Screening Questions ...........................................................119
Appendix C: Consent Form ..........................................................................................120
Appendix D: Participant Demographic Information Form ...........................................125
Appendix E: Interview Questions .................................................................................128
Appendix F: Sample Memos .......................................................................................130

viii
List of Tables
Table 1: Participant Demographic Information ..........................................................................45
Table 2: Participants’ Parental Demographic Information .........................................................46
Table 3: Meaning Making and Psychological Impact of Parental Feeding Control ...................49

ix
List of Figures and Illustrations
Figure 1: Birch and Ventura’s (2008) Multidirectional Model ..................................................23
Figure 2: Meaning Making and Psychological Impacts of Parental Feeding Control ................51

1
CHAPTER ONE
Introduction
In North America, childhood overweight and obesity continues to be a serious public
health concern (Roberts, Shields, de Groh, Aziz, & Gilbert, 2012). Canadian statistics indicate
that 31.5 % of children (5 to 17 years of age) are classified as overweight or obese (Roberts et
al., 2012). This statistic is concerning as researchers have found that children who are
categorized as obese are at a greater risk for developing a variety of health issues, are more
susceptible to weight-related bullying, stigmatization, and marginalization, and are more likely to
suffer from co-morbid psychological disorders (e.g., depression) than their peers who are
classified as normal weight (Gray, Janicke, Wistedt, & Dumont-Driscoll, 2010; Hayden-Wade et
al., 2005; Roberts et al., 2012). Moreover, it has been found that childhood obesity often persists
into adulthood (Whitaker, Wright, Pepe, Seidel, & Dietz, 1997). Given the potential
implications of childhood obesity, it is no surprise that parents want to protect their children from
becoming, or being classified as, overweight or obese.
Parental Feeding Control Practices
Given the various negative physiological and psychosocial consequences associated with
childhood obesity, it is not shocking that there has been a push towards developing and
implementing strategies that aid in the management of children’s weight (i.e., to help children
lose weight or to prevent children from gaining weight). Furthermore, as the current societal
standard of beauty glorifies thinness and marginalizes fatness, some parents may want to
implement weight management strategies in order to ensure that their children meet societal
beauty standards.

2
While professionally administered child weight management programs aim to maximize
benefits and minimize negative repercussions, not all parents seek professional support while
implementing weight loss, or weight gain prevention, strategies for their children. As a result,
some parents may choose to employ their own tactics to encourage weight loss, or prevent
weight gain, in their children. In fact, some parents may utilize parental feeding control practices
(i.e., restricting and monitoring a child’s diet, as well as pressuring them to eat specific foods like
fruits and vegetables) to limit their children’s consumption of palatable and energy-dense foods
(i.e., foods high in sugar, fat, and calories). Yet, despite their best efforts and intentions, parental
feeding control practices aimed at promoting weight loss or preventing weight gain have been
found to hinder children’s ability to regulate their food consumption which increases their risk
for becoming, or remaining, overweight or obese (Carper, Fisher, & Birch, 2000; Costanzo &
Woody, 1985; Cutting, Fisher, Grimm-Thomas, & Birch, 1999; Shunk & Birch, 2004).
Despite these findings, which indicate that parental feeding control practices aimed at
promoting weight loss or preventing weight gain can negatively impact children’s eating
behaviours and weight status, little research has been conducted to examine how parental feeding
control practices are subjectively experienced by children, and how they impact children’s
psychological well-being. As such, the current study examined remembered childhood
experiences of parental feeding control practices aimed at promoting weight loss or preventing
weight gain. Specifically, the meaning making and psychological impacts of these practices
were investigated.
Personal Relevance
“Nothing tastes as good as skinny feels.” It may not be surprising, in this current thin
obsessed society, that these words were spoken to me by one of my parents during my childhood.
3
As I had dealt with weight-related struggles during my teenage years, I was intensely curious
about the factors that could have contributed to my immense discomfort with living in a body
that did not perfectly fit societal standards. During my undergraduate studies in Psychology, I
began to wonder how my past food-, body-, and weight-related parent-child interactions had
affected my eating behaviours and overall well-being. Consequently, this curiosity sparked my
passion for researching the influence of parenting practices on children’s body image and eating
behaviours.
It was not until I read Dara-Lynn Weiss’ (2013) memoir entitled The Heavy: A Mother, A
Daughter, A Diet that I became interested in examining the effects of parental feeding control
practices on children’s psychological well-being. In her tell-all book, Weiss (2013) chronicled
her experience of putting her seven-year-old daughter on a diet. She described how she put her
daughter on a strict eating regimen that was based on dietary restriction (e.g., calorie counting,
portion control, and withholding the occasional meal). Overall, the book describes Weiss’
experience of getting her daughter’s weight into the “medically-acceptable”, and “socially
desirable”, range.
After reading this book, I felt as though there was a missing voice in the narrative. In
fact, there was little to no mention of Weiss’ daughter’s experience of parental feeding control
practices. How did she feel about being put on a restrictive diet? How did these feeding
methods impact her psychological well-being? How did she make sense of her mother’s
decision to control her eating in that way? I had many questions for Weiss’ daughter, but no
answers. Given these queries, I conducted a preliminary literature review to see if there had been
any research conducted on the subjective experience of parental feeding control practices from
the child’s perspective. To my surprise, most of the research focused on parental experiences of,
4
or motivations for, using these types of feeding methods (e.g., Carnell, Cooke, Cheng, Robbins,
& Wardle, 2011; Gray et al., 2010). Furthermore, when the research was focused on the child, it
explored the behavioural impacts of these practices (e.g., Birch & Fisher, 1995; Johnson &
Birch, 1994; Thompson, 2010; Vos & Welsh, 2010) and did not investigate the effect of these
methods on children’s psychological well-being. Therefore, I made it my mission to give a voice
to individuals who had experienced parental feeding control practices during their childhoods, in
order to gain a deeper understanding of the impacts of, and meanings associated with, these
feeding methods.
The Current Study
The objective of the current study was to examine remembered childhood experiences of
parental feeding control practices from a qualitative perspective. The study investigated the
following two research questions: How do young adults make meaning of their childhood
experiences of parental feeding control practices? and What are the perceived psychological
impacts of parental feeding control practices? A constructivist grounded theory analysis was
used to systematically construct a preliminary conceptualization that was grounded within the
data (i.e., interview transcripts; Charmaz, 2006). Constructivist grounded theory methods were
fitting for the aim of the current study as they enabled me to not only describe experiences of
parental feeding control, but also co-create theoretical hypotheses about the impacts of this
phenomenon (Charmaz, 2006).
Overview of Thesis Chapters
So far, I have provided background information on parental feeding control practices,
explained the personal relevance of this research, and briefly described the current study. In
chapter two, I review the research literature on childhood overweight and obesity, parental

5
feeding control practices, and their associated concepts. Following this, in chapter three, I
describe the study’s methodology, and discuss the ways in which trustworthiness was addressed
according to this method. In chapter four, I describe the results of the data collection and
analysis. Lastly, in chapter five, I discuss the study’s findings in relation to the research
literature. Furthermore, I address the strengths and limitations of the study, implications for
counselling psychology, and recommendations for future research.

6
CHAPTER TWO
Literature Review
This chapter provides a review of the literature on the concepts associated with childhood
obesity and parental feeding control practices. To begin, Canadian statistics on childhood
overweight and obesity will be addressed. This is followed by an overview of the potential
negative physiological and psychosocial consequences of childhood obesity. Factors that may be
contributing to the development of childhood obesity will then be discussed. Next, concepts
associated with parenting and feeding will be described. Parental feeding control practices will
then be defined, and possible consequences of these practices will be outlined. Subsequently,
factors contributing to the use of parental feeding control practices will be provided. Lastly, a
summary of this chapter, as well as an overview of the current study, will be presented.
Childhood Overweight and Obesity Rates & Consequences
In order to understand the context within which parents decide to utilize parental feeding
control practices to promote weight loss or to prevent weight gain in their children, I have
decided to frame my study within the childhood obesity literature. It is important to note that I
am using the language and discourses that are prevalent within this literature (e.g., “childhood
obesity epidemic”) in order to exemplify the messages that parents receive about childhood
overweight and obesity. Altogether, it is necessary to consider the impact of these discourses on
parents’ decision making process related to the use of feeding control practices.
Prevalence Rates
As was previously mentioned, childhood obesity continues to be a serious public health
concern across the globe. According to the World Health Organization (WHO, 2016), the
number of children (0 to 5 years of age) who are classified as overweight or obese worldwide has

7
increased from 32 million in 1990 to 42 million in 2013. The WHO (2014) estimates that, if
current trends persist, the global number of children who are deemed overweight or obese will
climb to 70 million by 2025.
While global statistics on childhood overweight and obesity are unnerving, Canadian
statistics on this topic do not offer much solace. Canadian childhood overweight and obesity
prevalence rates indicate that approximately one third of 5 to 17 year old children (i.e., 1.6
million children) were classified as overweight (19.8%) or obese (11.7%) from 2009 to 2011
(Roberts et al., 2012). Among children ages 5 to 11, approximately 19.7% were categorized as
overweight and 13.1% were classified as obese (Roberts et al., 2012). Prevalence rates among
adolescents (i.e., ages 12 to 17) reveal that approximately 19.9% were deemed overweight, while
10.2% were considered obese (Roberts et al., 2012).
As can be recognized based on the previously mentioned statistics, the obesity epidemic
is no longer an adult issue; children and adolescents are being impacted by obesity in
increasingly large numbers. This is reason for concern as obesity has been associated with a
wide variety of negative physiological and psychosocial consequences.
Consequences of Obesity
In light of these childhood obesity rates, it is crucial to consider its potential negative
impact on children’s physiology and psychosocial well-being. Researchers have found that
children with obesity are more likely to develop a variety of physiological issues (e.g., type II
diabetes; Daniels, 2006), are more vulnerable to social judgement (e.g., weight related
marginalization; Strauss & Pollack, 2003), and are more likely to develop co-morbid
psychological disorders (e.g., depression; Daniels, 2006) than children who are classified as
normal weight (Gray et al., 2010; Hayden-Wade et al., 2005; Roberts et al., 2012). Moreover,

8
researchers suggest that children and adolescents who are classified as overweight or obese are
more likely than their peers who are categorized as normal weight to struggle with adult obesity
(Whitaker et al., 1997).
Physiological consequences. Researchers have established a strong relationship between
childhood obesity and negative physiological conditions, which include: endocrine issues (e.g.,
early onset of puberty in girls), neurological problems (e.g., pseudotumor cerebri),
gastroenterological issues (e.g., gallstones and steatohepatitis), and musculoskeletal conditions
(Dietz, 1998, Must & Strauss, 1999, Philippas & Lo, 2005). Additionally, researchers have
found a relationship between childhood obesity and cardiovascular risk factors such as
dyslipidemia, hypertension, coagulopathy, chronic inflammation, and endothelial dysfunction
(Burke, 2006; Dietz, 1998; Freedman, Dietz, Srinivasan, & Berenson, 1999; Kiess et al., 2001;
Must & Strauss, 1999; Philippas & Lo, 2005; Raitakari, Juonala, & Viikari, 2005; Reilly et al.,
2003; Wabitsch, 2000). In fact, a study conducted by the American Medical Association found
that 70% of the obese children studied had at least one cardiovascular disease risk factor, while
more than 25% of those children possessed two or more risk factors (Bell et al., 2011).
Moreover, childhood obesity has also been associated with certain pulmonary risks which
include: sleep apnea, asthma, and exercise intolerance (Dietz, 1998; Must & Strauss, 1999;
Philippas & Lo, 2005; Reilly et al., 2003).
While early onset cardiovascular and pulmonary risks can significantly impact an
individual’s health, perhaps the most concerning physiological consequence of childhood obesity
is the rising prevalence of insulin resistance and type II diabetes. Type II diabetes is being
diagnosed in children and adolescents much more frequently than in previous years (Vivier &
Tompkins, 2008). While a definitive cause is presently unknown, it is believed that obesity,

9
along with other risk factors (e.g., lack of exercise), can lead to insulin resistance and type II
diabetes (Daniels, 2006; Ludwig & Ebbeling, 2001). The rising prevalence rates of insulin
resistance and type II diabetes in children and adolescents is worrisome as long-term
consequences of these issues include vascular disease leading to heart attacks, strokes, kidney
disease and failure, blindness, and other health problems (Vivier & Tompkins, 2008).
Overall, obesity can significantly affect an individual’s life and health; however,
consequences appear to be more severe when obesity is diagnosed during childhood and
adolescence. Due to the rising prevalence rates of obesity among children, susceptibility to the
development of many chronic diseases has increased and the age of possible onset has decreased
(Flegal, Tabak, & Ogden, 2006; Park, Falconer, Viner, & Kinra, 2012). What is more, childhood
obesity has been linked to negative psychosocial outcomes. As such, the following section will
address the ways in which childhood obesity can affect children’s mental health and social well-
being.
Psychosocial consequences. While greatly understudied in comparison to the potential
physiological consequences, researchers have also investigated the impacts of childhood obesity
on children’s psychological and social well-being. To begin, children who are classified as
obese have been shown to be more susceptible to weight-based stigmatization and
marginalization (Puhl & Latner, 2007; Strauss & Pollack, 2003). In a study conducted by
Strauss and Pollack (2003), the social relationships of adolescents who were classified as
overweight were compared to those of adolescents categorized as normal weight; findings
indicated that adolescents who were deemed overweight were more likely to be socially isolated,
as well as to be peripheral to social groups than their peers who were classified as normal weight.
Furthermore, researchers have found that children who are categorized as overweight or obese
10
are up to two times more likely to fall victim to overt (e.g., hitting) and relational (e.g., teasing
and rumours) bullying than children who are classified as normal weight (Eisenberg, Neumark-
Sztainer, & Story, 2003; Hayden-Wade et al., 2005). Additionally, in a study conducted by
Hayden-Wade and colleagues (2005), it was found that children who were deemed overweight
experienced more prevalent, frequent, and upsetting appearance-related teasing (e.g., derogatory
nicknames) than children who were categorized as normal weight.
Researchers also indicate that children who are classified as overweight and obese are
victims of stigmatization and marginalization not only by their peers, as outlined above, but also
by their teachers (Bauer, Yang, & Austin, 2004; Neumark-Sztainer, Story, & Harris, 1999) and
parents (Crandall, 1995; Davison & Birch, 2004b). This type of treatment is especially
distressing during childhood and adolescence when the development of social relationships is of
utmost importance. As such, it has been found that children who are deemed overweight or
obese may be more susceptible to developing depression, increased suicidal ideation and
attempts, as well as decreased body satisfaction and lower self-esteem as a consequence of
experiencing weight related bias and marginalization (Eisenberg et al., 2003, Hayden-Wade et
al., 2005; Puhl & Latner, 2007; Storch et al., 2007). Lastly, childhood experiences of weight
related stigmatization could encumber children’s psychological, social, and emotional
development, while also exacerbating the negative physiological complications associated with
childhood obesity (Daniels, 2006; Weiss & Caprio, 2005). Given the potential consequences of
childhood obesity stigmatization, it is imperative that researchers and practitioners consider
factors that may be contributing to the development childhood obesity.
Factors Contributing to Childhood Obesity
11
The current food environment. The increasing trend towards higher childhood
overweight and obesity rates has largely been attributed to the ‘obesogenic’ food environment
that is common in developed countries (e.g., the United States of America and Canada), whereby
sedentary lifestyles and the high consumption of palatable, energy dense foods creates an
imbalance in energy intake and energy expenditure; this phenomenon tends to result in excessive
weight gain (Golan & Crow, 2004). In today’s society, parents are held responsible for
promoting the development of healthy dietary habits in their children, and protecting them from
the current obesogenic food environment in which “unhealthy” foods are readily accessible.
Given the current ‘obesogenic’ food environment, it is not shocking that children’s diets
tend to be too high in fat, sugar, and calories, and too low in the intake of fruits and vegetables
(Reedy & Krebs-Smith, 2010). Human predispositions and the current food environment come
together to explain this phenomenon (Savage, Fisher, & Birch, 2007). Children are born with a
preference towards sugar and fat, which are present in energy-dense foods (i.e., high in calories),
and often dislike sour and bitter tastes found in plant-based foods such as fruits and vegetables
(i.e., nutrient-rich foods; Savage et al., 2007). As such, children tend to prefer the “unhealthy”
foods, over “healthier” options. Moreover, marketing strategies that encourage children to
consume energy-dense, nutrient poor foods (e.g., children’s menus) greatly influence children’s
preferences for such foods (Grier, Mensinger, Huang, Kumanyika, & Stettler, 2007; O'Donnell,
Hoerr, Mendoza, & Goh, 2008). Given all of these factors, it is not surprising that some parents
struggle with managing their children’s weight.
Multidimensional framework. As was previously mentioned, the ‘obesogenic’ food
environment has been largely credited for the increasing prevalence rates of childhood
overweight and obesity; however, a growing number of researchers suggest that multiple factors

12
come together to result in childhood obesity. Gable and Lutz (2000) propose that childhood
obesity is a consequence of a multidimensional system with interacting elements (e.g., food
environment, economy, parental factors, child factors, and level of physical activity). With this
being said, they suggest that parental influence is one of the most significant factors contributing
to the development of unhealthy eating habits in children, and their resulting weight status
(Gable & Lutz, 2000). In fact, researchers have shown that a child’s health is more significantly
impacted by their familial microsystems than any other sphere of influence (e.g., media,
community, and school). As such, it is important to take into account parenting factors that may
influence the development of eating habits in children, and their subsequent weight
categorization.
Parenting factors. Researchers suggest that parents can either promote or discourage the
development of particular eating habits through specific feeding practices (Ventura & Birch,
2008). In fact, it has been shown that parental feeding practices can impact children’s food
preferences and consumption which, in turn, may affect children’s weight status (Campbell,
Crawford, & Ball, 2006; Thompson, 2010). Additionally, researchers indicate that eating habits
develop during early childhood and tend to persist into later childhood, adolescence, and
adulthood (Birch & Fisher, 1998). Altogether, the previously mentioned research findings
highlight the importance of considering the influence of parental feeding practices on the
development of children’s eating habits, and their resulting weight status. However, before we
consider the role of parental feeding practices on children’s eating behaviours and weight status,
it is necessary to first understand the concepts surrounding parenting and feeding.
13
Parenting and Feeding
Eating patterns are developed during early childhood, persist into later childhood,
adolescence and beyond, and are significant determinants of weight status (Birch & Davison,
2001a; Robinson et al., 2007). From early childhood, what, when, and how much children
consume is influenced by a multitude of factors including: children’s behaviours and internal
appetitive cues, parents’ recognition of, and responsiveness to, these cues, and the parents’
parenting beliefs and attitudes (Satter, 1986). Researchers suggest that early parent-child
interactions related to food and eating influence children’s development of food preferences,
eating habits, and dietary self-regulation, which subsequently impacts children’s weight status
(Birch, 2006; Hetherington, Cecil, Jackson, & Schwartz, 2011). As such, it is necessary to
consider the role of parenting and feeding in the development of children’s eating behaviours and
habits, as well as their weight status.
Parenting
Parenting refers to child-rearing activities that aim to promote and support development
across a range of domains (Davies, 2000). In the research literature, parenting has been
described in terms of styles, dimensions, and practices.
Parenting styles. Parenting styles refer to the overall emotional environment produced
by parents during interactions with their children (Jansen, Daniels, & Nicholson, 2012).
Traditionally, parenting styles have been characterized using a taxonomical approach based on
combining the two dimensions: parental demandingness (i.e., the extent to which parents have
expectations for, and control over, their children) and parental responsiveness (i.e., the extent to
which parents exhibit warmth and support towards their children; Darling & Steinberg, 1993).
These dimensions come together to form four different parenting styles, these are: (a)

14
authoritative (i.e., high demandingness and high responsiveness); (b) authoritarian (i.e., high
demandingness and low responsiveness); (c) indulgent/permissive (i.e., low demandingness and
high responsiveness); and (d) uninvolved/neglectful parenting (i.e., low demandingness and low
responsiveness; Maccoby & Martin, 1983). Researchers have found that, within a western
context, authoritative parenting has been related to more positive developmental outcomes (e.g.,
children demonstrate better socio-emotional skills and cognitive ability, as well as engage in less
health risk behaviours) than those of authoritarian, indulgent/permissive, and
uninvolved/neglectful parenting styles (Baumrind, 1991; Bornstein & Zlotnik, 2009; Jackson,
Henriksen, & Foshee, 1998; Lytle et al., 2003; Sleddens et al., 2011; Smith, 2011).
Parenting dimensions. Parenting dimensions refer to ways of describing parenting
practices (Lucas, Maguire, & Nicholson, 2010). In addition to the previously mentioned
parenting dimensions, demandingness and responsiveness, other dimensions of parenting
practices have been recognized, including: self-efficacy (i.e., parental beliefs about parenting
ability), irritability or hostility (i.e., displaying feelings of anger or frustration towards their child
or emotional reactivity), consistency (i.e., consistently setting and applying age-appropriate rules
and expectations for their child), autonomy-encouragement (i.e., encouraging self-reliance
through helping the child to make their own decisions, learn rules, and achieve tasks in a
manageable, stepwise manner), and over-protection (i.e., giving too much guidance, protection,
and assistance in relation to the child’s capabilities; Lucas et al., 2010). Commonly, children
demonstrate better developmental outcomes when parents are high in self-efficacy, consistency,
and autonomy-encouragement, as well as low in irritable or hostile affect and over-
protectiveness (Bayer et al., 2011; Wake, Nicholson, Hardy, & Smith, 2007).
15
Parenting practices. Parenting practices refer to situation-specific strategies that parents
use to shape their children’s development; these strategies may change over time, across
situations, and with different children (Bornstein & Zlotnik, 2009; Walker & Kirby, 2010).
Parenting practices are used to operationalize parenting dimensions and styles. In brief,
parenting practices are what parents do (i.e., behaviours they display), while parenting styles
describe how parents do it (i.e., the overall emotional environment characterized by parenting
dimensions).
Parental Feeding
Parenting and feeding are intimately related; in fact, one of the most important
responsibilities associated with early parenting is feeding (Satter, 1986). Given the rising
interest in researching the potential relationships between parenting and the development of
eating habits in children, there has been an attempt to relate conventional parenting concepts to
feeding (e.g., feeding styles and feeding practices).
Feeding styles. The previously mentioned parenting framework (i.e., parenting
taxonomy related to parental responsiveness and demandingness) has also been applied to the
area of feeding (Faith, Scanlon, Birch, Francis, & Sherry, 2004; Hughes, Power, Fisher, Mueller,
& Nicklas, 2005). In feeding, demandingness refers to the extent to which parents have control
over their children’s food intake, while responsiveness refers to how parents encourage their
children to eat (Hughes et al., 2005). For instance, parents who exhibit an authoritative feeding
style (i.e., high responsiveness and high demandingness) may allow their children to choose
among a variety of presented foods, while parents who display an authoritarian feeding style
(i.e., low responsiveness and high demandingness) may disregard the child’s food preferences
and make the dietary decision for the child.
16
Parental feeding practices and control. Parental feeding practices refer to the
situation-specific behavioural strategies that parents use in order to manage when, what, and how
much their children eat (Birch, Fisher, & Davison, 2003; Ventura & Birch, 2008; Vereecken,
Legiest, De Bourdeaudhuij, & Maes, 2009). If parents are concerned about their child’s weight
(i.e., they want their child to lose weight, or are concerned about their child gaining weight), they
may choose to employ an assortment of feeding practices to monitor and control their child’s
eating (Birch et al., 2003). These types of feeding strategies are categorized in the literature as
feeding control practices, and are used to limit children’s access to palatable and energy dense
foods (i.e., foods that are high in fat, sugar, and calories; Fisher & Birch, 1999). For instance,
parents who utilize parental feeding control practices may try to restrict their children’s access
to, and consumption of “unhealthy” foods (Birch et al., 2003). It should be noted that parental
feeding control practices are not always utilized to promote weight loss or to prevent weight gain
in children (e.g., pressuring a child to eat more in order to promote weight gain in a child who is
underweight). However, for the purpose of this study, I have chosen to focus on parental feeding
control practices that are employed to combat the development, or progression, of childhood
overweight and obesity.
Researchers that have investigated feeding control practices have demonstrated that
parents use a myriad of practices to control their children’s consumption of palatable and energy-
dense foods, including: a) restriction, b) pressure to eat, c) monitoring, d) emotional feeding, and
e) using food as a reward (Birch, Fisher, Grimm-Thomas, Markey, Sawyer, & Johnson, 2001;
Davison & Birch, 2001a; Rhee, 2008; Skouteris, McCabe, Swinburn, Newgreen, Sacher, &
Chadwick, 2011; Wardle, Sanderson, Guthrie, Rapoport, & Plomin, 2002). Restriction entails
limiting a child’s total amount of food consumption and/or access to unhealthy foods (Birch et
17
al., 2001). Pressure to eat refers to insisting that a child to eat certain foods (e.g., fruits and
vegetables; Birch et al., 2001). Monitoring involves supervising a child’s consumption of
energy-dense foods (Birch & Fisher, 2000). Emotional feeding has been defined as feeding a
child in an attempt to remedy emotional distress (Wardle et al., 2002). Lastly, using food as a
reward entails giving a child food rewards for good behaviours (Rhee, 2008). While all of the
previously mentioned feeding practices have been recognized as controlling, the use of
restriction, monitoring, and pressure to eat are most commonly described as the three primary
feeding practices associated with parental feeding control aimed at promoting weight loss or
preventing weight gain in children (Birch et al., 2001).
Covert and overt feeding control practices. Parental feeding control practices can also
be described as either covert or overt (Ogden, Reynolds, & Smith, 2006). Parental feeding
control practices are described as covert when they are less perceivable to the child. Such covert
feeding control practices can include: restricting the amount of times children are taken to
restaurants that serve “unhealthy” foods, and not eating unhealthy foods in front of children
(Ogden et al., 2006). Other parental feeding control practices may be categorized as overt (i.e.,
more perceivable to children) and often occur after unhealthy foods are present in the home
(Ogden et al., 2006). Examples of overt parental feeding control practices could include: putting
the “unhealthy” foods out of children’s reach, or getting children to ask permission to eat or
access these foods (Ogden et al., 2006).
Relationships between feeding styles and feeding practices. Researchers that have
investigated the relationship between parental feeding styles and parental feeding practices have
indicated that increased use of parental feeding control practices (e.g., restriction, pressure to eat,
negative monitoring, and using food as a reward) tends to be related to authoritarian feeding

18
styles, while increased levels of parental responsiveness in feeding (e.g., feeding the child in
response to his/her hunger and satiety cues) are associated with authoritative feeding styles
(Hubbs-Tait, Kennedy, Page, Topham, & Harrist, 2008; Hughes et al, 2005).
Impacts of Parental Feeding Control Practices
During early childhood, it is vital that parents help children develop an ability to
appropriately recognize their internal cues for hunger and satiety through their feeding practices
(DiSantis, Hodges, Johnson, & Fisher, 2011; Satter, 1986). Utilizing parental feeding practices
that ignore or override children’s internal satiety cues (e.g., parental feeding control practices)
can have a negative impact on children’s self-regulation of food consumption, food preferences,
and weight status (Birch & Fisher, 1995; Johnson & Birch, 1994; Thompson, 2010; Vos &
Welsh, 2010).
Children’s Self-Regulation of Food Consumption
As was previously discussed, parents are responsible for encouraging the development of
dietary self-regulation in children. In fact, researchers indicate that children’s ability to self-
regulate food consumption can be enhanced through training in which they are taught to respond
to internal sensations of hunger or fullness (Johnson, 2000). For instance, parents can teach their
children to eat more slowly, as well as to stop eating when they feel full. Conversely, if parents
are not able to recognize, or if they actively overrule, their children’s internal cues, children do
not learn to appropriately identify and interpret their hunger and satiety cues and, as a result,
develop poor self-regulation related to food and eating (Satter, 1990).
What is more, parents may utilize inappropriate feeding practices which will further
disrupt children’s ability to regulate their food consumption (Birch et al., 2001; Monasta et al.,
2010). Researchers have shown that children who have parents that employ feeding control

19
practices display diminished ability in self-regulating dietary consumption, and are more likely
to overeat than children with parents who do not exert great control over feeding (Birch &
Fisher, 1995; Johnson & Birch, 1994). For instance, pressuring a child to eat has been found to
result in decreased responsiveness to internal satiety cues for the child, and disinhibited eating
later in life (Carper et al., 2000). Other researchers have suggested that parental, particularly
maternal, use of feeding control practices may encourage eating in the absence of hunger in
young girls (Birch, Fisher, & Davison, 2003; Fisher & Birch, 2002). Furthermore, using food to
reward good behaviour, or as a means to alleviate distress, has also been associated with
children’s reduced ability to recognize internal cues of appetite (Birch, McPheee, Shoba,
Steinberg, & Krehbiel, 1987; Cooke, Chambers, Añez, & Wardle, 2011).
Children’s Food Preferences and Weight Status
Researchers have demonstrated that a variety of parental feeding practices influence a
child’s food intake and weight (Campbell, Crawford, & Ball, 2006). In particular, feeding
control practices have been found to greatly impact a child’s consumption (Campbell et al.,
2006). Researchers propose that parents may inadvertently change their child’s preference for
certain foods through feeding control practices (Thompson, 2010). For example, by restricting a
child’s access to sweets, parents may be unintentionally increasing their child’s desire for the
restricted food (Thompson, 2010). Parents who utilize restrictive feeding practices may
encourage disinhibited eating in their children, which correlates positively with weight status
(Vos & Welsh, 2010).
Moreover, feeding control practices have consistently demonstrated a positive
relationship with childhood overweight and obesity in the literature. In a study conducted by
Gable and Lutz (2000), it was found that as parental control over feeding increases, the child’s

20
ability to self-regulate food consumption decreases. As such, when parents override children’s
ability to regulate their food consumption, it can result in children ignoring their internal
satiation cues and, as result, they continue to eat when they are no longer hungry (Campbell et
al., 2006). In one study that investigated parental feeding pressure and food consumption in four
year old children, it was found that children who are rewarded for finishing their plates
consumed significantly more calories than those who stopped eating when they were full (Birch,
McPhee, Shoba, & Steinberg, 1987).
Impacts of Covert versus Overt Feeding Control Practices
As of yet, most of the research studies on parental feeding control practices have viewed
these methods on a continuum (i.e., from low control to high control). The literature on this
subject matter is unclear on which practices represent high versus low forms of control.
Furthermore, there is no consensus on whether qualitative differences among feeding control
practices impact children’s eating behaviours and weight outcomes in distinctive ways. For
instance, Ogden and colleagues (2006) used a measure of overt and covert feeding control to
evaluate feeding control practices. Findings indicated that covert control was negatively
associated with children’s consumption of unhealthy foods, while no association was found for
overt control; however, overt control was positively linked to children’s consumption of healthy
snacks (Ogden et al., 2006). Similar to Ogden and colleagues’ (2006) conceptualization of
parental feeding control, Grolnick and Pomerantz (2009) presented a model in which the
methods parents employ to structure the home environment (e.g., rules and routines that offer
children occasions to develop self-regulation) differ from the coercive methods that parents may
utilize to control children’s behaviours (e.g., pressure, and forcing children to behave in a certain
manner). Studies examining this type of dichotomy in parental control found that structure-
21
based parenting practices (e.g., setting household rules) were related to positive behavioural
outcomes (e.g., autonomy related to school work; Marbell & Grolnick, 2012) and academic
achievement (Farkas & Grolnick, 2010). While informative, Grolnick and Pomerantz’s (2006)
model does not specifically address parental feeding practices; as such, more research is needed
to qualitatively investigate how different types of parental feeding control practices (e.g., covert
versus overt parental feeding control practices) may affect children’s eating behaviours and
weight status in distinctive ways.
Factors that Predict the Use of Parental Feeding Control Practices
Parents and children bring their own preferences, objectives, and personalities to parent-
child feeding interactions; these factors influence each other to impact parental feeding practices
(Satter, 1990). The following outlines parental and child factors that predict the use of parental
feeding control practices.
Parental Factors
Multiple parental factors come together to predict parents’ use of feeding control
practices. For instance, Costanzo and Woody (1985) theorized that parents are more likely to
engage in controlling feeding practices when they a) are concerned with their own weight and
eating issues, b) observe a tendency towards weight gain in their child, c) believe their child is at
risk for developing eating problems, and d) are worried about their child becoming obese. More
recent literature has provided support for this theory. Researchers have found that mothers are
more likely to use feeding control practices when they struggle with eating and weight issues
(e.g., restrained eating or frequent dieting; Birch & Fisher, 2000), experience body
dissatisfaction (Brown & Ogden, 2004), are worried about their child’s weight status (Francis &
Birch, 2005a; Spruijt-Metz, Li, Cohen, Birch, & Goran, 2006), view their child as overweight
22
(Francis, Hofer, & Birch, 2001), and/or observe excessive weight gain in their child (Rhee et al.,
2009; Rifas-Shiman et al., 2011). Qualitative studies on parental motivations for employing
feeding control practices have corroborated these findings. For example, research investigating
Latino mothers’ feeding beliefs and practices found that mothers employed restrictive feeding
practices when they experienced significant concern over their child becoming overweight in
spite of cultural ideals which favour “chubby” children (Lindsay, Sussner, Greaney, & Peterson,
2011).
Furthermore, researchers have demonstrated that parents are more likely to use feeding
control practices if they are biased towards individuals with larger bodies (Musher-Eizenman,
Holub, Hauser, & Young, 2007). Research conducted by Musher-Eizenman and colleagues
(2007) investigated how parental anti-fat attitudes impact parental feeding practices. They found
that parents’ prejudice towards large individuals predicted the use of restrictive feeding practices
above and beyond the influence of parent and child weight status, as well as parental concern
about the child becoming overweight. These results indicate that parental anti-fat attitudes also
predict the use of parental feeding control practices.
Child Factors
Child temperament may also be associated with parents’ use of feeding control practices.
For example, lower levels of inhibitory control (i.e., ability to plan and suppress inappropriate
responses) have been found to predict weight gain in children as they move from childhood to
adolescence (Anzman & Birch, 2009), and lower self-regulation has been associated with
increased consumption and weight gain in children (Francis & Susman, 2009; Guxens et al.,
2009; Nederkoorn, Smulders, Havermans, Roefs, & Jansen, 2006; Riggs, Spruijt-Metz, Sakuma,
Chou, & Pentz, 2010). Despite a dearth of research in the area, preliminary results have shown
23
that individuals who exhibit increased levels of reward sensitivity (i.e., ability to derive pleasure
from natural reinforcers such as food) are more likely to overeat and be overweight during their
childhoods (Guerrieri, Nederkoorn, & Jansen, 2007; Nederkoorn, Braet, Van Eijs, Tanghe, &
Jansen, 2006). As such, in instances where children have predispositions towards lower levels of
inhibitory control and self-regulation, as well as higher levels of reward sensitivity, it is possible
that parents may choose to exert more control over their feeding in order to manage their
children’s weight.
Multidirectional Model
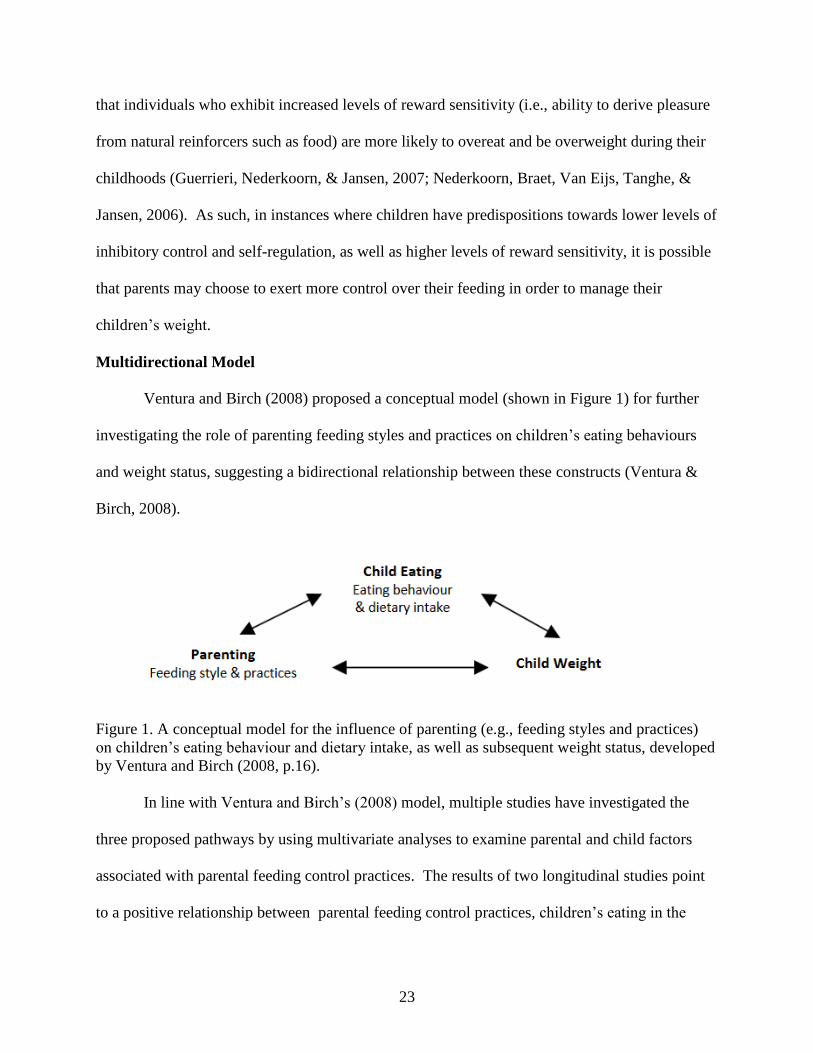
Ventura and Birch (2008) proposed a conceptual model (shown in Figure 1) for further
investigating the role of parenting feeding styles and practices on children’s eating behaviours
and weight status, suggesting a bidirectional relationship between these constructs (Ventura &
Birch, 2008).
Figure 1. A conceptual model for the influence of parenting (e.g., feeding styles and practices)
on children’s eating behaviour and dietary intake, as well as subsequent weight status, developed
by Ventura and Birch (2008, p.16).
In line with Ventura and Birch’s (2008) model, multiple studies have investigated the
three proposed pathways by using multivariate analyses to examine parental and child factors
associated with parental feeding control practices. The results of two longitudinal studies point
to a positive relationship between parental feeding control practices, children’s eating in the
24
absence of hunger, and children’s weight status (Birch et al., 2003; Francis & Birch, 2005).
Furthermore, it was found that the child’s eating in the absence of hunger mediated the
relationship between parental feeding control practices and the child’s weight status (Francis &
Birch, 2005). In addition, researchers who conducted a cross-sectional study found that the use
of parental feeding control practices predicted children’s weight status, and disinhibited eating
behaviour mediated this relationship (Joyce & Zimmer-Gembeck, 2009).
The interactional relationship between parenting, child eating behaviours, and child
weight status echoes the dynamics between parents and their children. It indicates that children’s
eating behaviours impact, and are impacted by, their parents’ use of feeding control practices
(Webber, Cooke, Hill, & Wardle, 2010). In addition, a child’s weight status and eating habits
may both separately influence their parents’ use of feeding control practices (Webber et al.,
2010).
Summary
Despite the growing amount of literature on parental feeding control practices, little is
known about the subjective experience of these feeding methods during childhood. Most of the
literature on this subject matter focuses on the behavioural impacts of, or parental motivations
for, employing feeding control practices. As a result, children’s subjective experience of these
feeding practices has remained largely ignored. By solely investigating the behavioural impacts
of parental feeding control practices, researchers are missing the feeling and thinking aspects of
experiencing parental feeding control practices. Without acknowledgement of these aspects, a
truly rich understanding of how parental feeding control practices impact children cannot be
attained. A qualitative examination of subjective experiences of parental feeding control would
25
allow for a deeper understanding of the psychological impacts of these feeding practices, and
would shed light on how children make meaning of their parents’ decision to control their diet.
Furthermore, the current research literature has not addressed the messages (e.g., beauty
ideals) that are being transmitted by parents, either implicitly or explicitly, about food, weight,
and the body through parental feeding control practices. In a study conducted by Shomaker and
Furman (2009), the impacts of parental messages about thinness on disordered eating in
adolescent girls were examined. Shomaker and Furman (2009) found that both adolescents’
reports of parental pressure to be thin and parents’ reports of pressuring daughters to be thin were
significantly associated with disordered eating. These results emphasize the influence of explicit
messages about food, weight, and the body within the parent-child relationship. Furthermore, in
addition to the communication of direct messages about food, weight, and the body, parents may
also be unintentionally communicating implicit messages regarding these concepts. These
implicit messages may be in agreement with, or completely oppose, the explicit parental
messages that are being communicated to the child. For example, a mother may explicitly
encourage her daughter to love herself the way she is, while implicitly sending her the message
that her body is not good enough through parental feeding control practices. An examination of
the messages, either direct or indirect, communicated through parental feeding control
interactions, has not been conducted as of yet.
Current Study
As most research on this topic has focused on the behavioural consequences of parental
feeding control practices, many psychological aspects of these experiences are unknown. As
such, the objective of the current study is to examine remembered childhood experiences of
parental feeding control practices from a qualitative perspective. The current study investigated
26
the following two research questions: How do young adults make meaning of their childhood
experiences of parental feeding control practices? and What are the perceived psychological
impacts of parental feeding control practices? The use of qualitative research methods was
purposefully chosen as it allowed the researcher to gain access to the intricacies of human
experiences (e.g., underlying meanings, and involved psychological processes). More
specifically, this research study was conducted from the epistemological position of social
constructivism, which suggests that reality is historically and culturally situated, and constructed
through all types of human interactions (Mills, Bonner, & Francis, 2006). Experiences of
parental feeding control practices occur in a culture that glorifies thinness and vilifies fatness;
and acknowledgment of this provided a context for understanding experiences of parental
feeding control practices.
Conclusion
In summary, there has been a considerable amount of research that has focused on the
behavioural impacts of parental feeding control practices on children. Specifically, researchers
have shown that these feeding practices may cause children to exhibit decreased ability in self-
regulating dietary intake (Birch & Fisher, 1995; Birch et al., 1987; Birch et al., 2001; Birch et al.,
2003; Carper et al., 2000; Cooke et al., 2011; Fisher & Birch, 2002; Johnson & Birch, 1994;
Monasta et al., 2010), develop a preference towards restricted foods (Campbell et al., 2006;
Thompson, 2010), as well as increase their risk for becoming overweight or obese (Birch et al.,
1987; Spruijt-Metz, 2011; Vos & Welsh, 2010). However, research examining the impacts of
parental feeding control practices on children’s psychological well-being, as well as research on
how individuals make meaning of these experiences, is particularly absent.

27
CHAPTER THREE
Methodology
This chapter offers an overview and description of the research methods employed to
answer the following two questions: How do young adults make meaning of their childhood
experiences of parental feeding control practices? and What are the perceived psychological
impacts of parental feeding control practices? This chapter begins with a description of
traditional and constructivist grounded theory methodologies, followed by a discussion of
constructivist grounded theory’s suitability for the present study. Then, procedures and ethical
considerations for the present study are described. To conclude, a discussion of the evaluation of
the constructivist grounded theory is provided.
Grounded Theory
Grounded theory (GT) is a qualitative research method used to systematically (i.e.,
through explicit strategies and techniques) develop theories that are ‘grounded’ in qualitative
data (Glaser & Strauss, 1967). GT begins with inductive qualitative data collection, and is
followed by the utilization of strategies and techniques that aid in the constant comparison and
analysis of data (Glaser & Strauss, 1967). GT involves abductive reasoning; as such,
preliminary interpretations of the qualitative data are considered, and further data is collected to
determine whether or not the hypothesized theory accurately explains the process (Charmaz,
2014). This procedure is repeated until the researcher feels that their interpretation correctly
explains the psychological processes involved in the studied experience. Ultimately, through GT
methods, the researcher is able to identify common patterns, processes, and meanings that exist
across a specific experience (e.g., childhood experiences of parental feeding control), and
construct a theory that captures the researched phenomenon (Tweed & Charmaz, 2012).

28
Traditional Grounded Theory Methodology
GT was introduced by two sociologists, Barney G. Glaser and Anselm L. Strauss, in the
mid 1960s with the publication of the book The Discovery of Grounded Theory (Tweed &
Charmaz, 2012). GT offered an innovative and rigorous inductive approach to qualitatively
studying various experiences (Tweed & Charmaz, 2012). This method was distinctively
disparate from the deductive, positivist, quantitative methods that were considered to be the
scientific research standard in the 19th
century (Charmaz, 2014). Glaser and Strauss (1967)
claimed that the quantitative research approach (i.e., testing hypotheses that are pulled from
previously established knowledge) resulted in theories that were disconnected from empirical
reality. Consequently, GT provided a research approach that could help researchers develop
theories directly from the data (Glasser & Strauss, 1967). The main features of traditional GT
are: theoretical sensitivity, theoretical sampling, the constant comparison method, coding, and
theoretical memos (McCann & Clark, 2003).
Theoretical sensitivity refers to the researcher’s ability to develop a theory as it “emerges
from the data” (Glaser & Strauss, 1967, p. 46). As such, grounded theorists do not impose their
preconceived notions or hypotheses onto the data; they discover the theory as it surfaces through
the process of data collection and analysis (Glaser & Strauss, 1967). Glaser and Strauss (1967)
argued that theoretical sensitivity develops and deepens through time and research practice (i.e.,
through gaining theoretical knowledge and personal experience with the research).
In GT, researchers employ two types of sampling, purposive and theoretical. Initially,
grounded theorists utilize purposive samples based on the study’s inclusion and exclusion
criteria. As the research process continues, researchers become more selective in their sampling
in order to advance theory development (McCann & Clark, 2003). Typically, theoretical
29
sampling takes place until saturation is met (i.e., no new data emerges; McCann & Clark, 2003;
Glaser & Strauss, 1967).
Through the constant comparison method, grounded theorists conduct data collection and
analysis simultaneously (McCann & Clark, 2000; Glaser & Strauss, 1967). Glaser and Strauss
(1967) describe four stages of the constant comparison method: comparing incidents related to
each category, exploring relationships between categories, defining the theory, and writing the
theory. Grounded theorists continue this process until a detailed theory is developed (McCann &
Clark, 2000).
Researchers who use traditional GT methods utilize two levels of coding: open and
selective (McCann & Clark, 2000a). Open coding occurs when the researcher breaks down the
data into discrete components and assigns codes (i.e., conceptual labels) to them (McCann &
Clark, 2000a). Grounded theorists use selective coding to define relationships between the
emerging categories (McCann & Clark, 2000a).
Lastly, grounded theorists employ theoretical memos to demonstrate, and make note of,
their analytical process. Throughout the research, memos are written by the researcher to
document ideas and observations, as well as to develop the theory (Glaser & Strauss, 1967;
McCann & Clark, 2000a).
The Evolution of Grounded Theory
Grounded theory has evolved tremendously since its first conceptualization (Charmaz,
2014). Traditional GT (Glaser & Strauss, 1967) adopted an objectivist and realist perspective
(Ghezelije, & Emami, 2009). Glasser and Strauss (1967) described grounded theorists as neutral
observers who witness the emergence of reality (i.e., an objective and observable truth).
However, in 1990, Strauss collaborated with Juliet Corbin to develop a more relativist or

30
subjectivist version of GT (Ghezelije, & Emami, 2009). During this time, many researchers,
including Strauss and Corbin, began embracing constructivist versions of GT. Although they
never explicitly address the constructivist epistemology, Strauss and Corbin adopted a relativist
perspective by recognizing the existence of multiple truths, acknowledging personal biases, and
understanding that theory is constructed through social interactions (Mills, Bonner, & Francis,
2006).
Constructivist Grounded Theory Methodology
Many researchers have tailored GT to suit an array of ontological and epistemological
stances. Kathy Charmaz, a former graduate student of both Glaser and Strauss, developed an
adaptation of GT called constructivist GT founded on the constructivist paradigm (Charmaz,
2006). In Charmaz’s (2006) constructivist version of GT, the researcher is viewed as a filter
through which data is collected and analyzed (Lichtman, 2013). As a result, the researcher’s past
experiences and biases inevitably influence the research process (Charmaz, 2014).
Constructivist grounded theorists recognize that data collection and analysis are impacted by the
researchers’ and their participants’ social locations and perspectives (Ghezelije, & Emami, 2009;
Tweed & Charmaz, 2012). Thus, constructivist grounded theorists argue that theory is not
discovered, but co-created in an interactive process between the researcher, participants, and the
data (Henwood & Pidgeon, 2003).
Constructivist grounded theorists assume a relativist ontological position and a
subjectivist epistemological stance, in which it is believed that multiple realities exist as reality is
understood to be constructed through social interactions between individuals with differing
perspectives (Mills et al., 2006). Contrary to traditional GT’s focus on a discoverable objective
reality, constructivist GT asserts that knowledge is co-created through social interactions

31
between researchers and their participants (Ghezelije & Emami, 2009). Therefore, constructivist
grounded theorists believe that theories are subjectively co-constructed versus objectively
discovered (Charmaz, 2014). As such, theories are personal (i.e., from a particular perspective)
interpretations of data (Mills et al., 2006), rather than exact replications of reality (Andrews,
2012).
Traditional grounded theorists have critiqued other qualitative approaches (including
constructivist GT) by arguing that qualitative researchers frequently mold their data to fit their
preconceived ideas (Glaser, 1992). However, constructivist grounded theorists believe in the co-
construction of knowledge between researchers and their participants, and emphasize that theory
needs to be rooted in the data (Mills et al., 2006). Moreover, constructivist grounded theorists
take a reflexive position towards their analysis of data, experiences, decisions, and
conceptualizations (Charmaz, 2006). In this way, they are reflexive in evaluating how their
interests, social positions, biases, and assumptions impact their research.
Finally, Charmaz (2006) called her approach constructivist GT to state her belief that
theory is developed through social interactions between researchers and their participants.
Charmaz (2014) argues that constructivism is in line with contemporary definitions of social
constructionism. Social constructionism can be described as the belief that reality is constructed
within a historical, social, and cultural context (Charmaz, 2006; Mischler, 1979; Raskin, 2002;
Young & Collin, 2004). As Charmaz (2014) understood constructivism and social
constructionism as encompassing similar notions and meanings, the term constructivism will be
utilized throughout the rest of this paper.
Rationale for Constructivist GT Methodology
In this study, I was interested in exploring the meaning making and psychological

32
impacts of experiencing parental feeding control practices during one’s childhood. Such a
research question seeks to understand subjective meaning, rather than explain or predict
objective phenomena and, therefore, is more aligned with qualitative research methods
(Charmaz, 2006). Qualitative research endeavours to a) reveal how individuals experience a
specific phenomenon, b) gain a better understanding of a phenomenon about which little is
known, and c) provide researchers with the opportunity to gain information about a phenomenon
that would be challenging to obtain via quantitative methods (Strauss & Corbin, 1990). These
three goals are consistent with the aims of the current study and, thus, qualitative methods were
employed.
Of the many qualitative research approaches, constructivist GT was chosen as the most
appropriate methodology for this study as this method allows the researcher to investigate new
areas and over time, develop original theory (Glaser & Strauss, 1967). Little is known about the
child’s subjective experience of parental feeding control practices. As such, GT aligns with this
study as it offers the researcher tools to develop a preliminary theoretical conceptualization of
the processes involved in these experiences (Glaser & Strauss, 1967). Furthermore, GT methods
enable the researcher to not only describe specific experiences, but also create abstract
theoretical hypotheses about the processes involved in the studied phenomenon (Glaser &
Strauss, 1967). Overall, GT methods offer strategies and techniques to identify patterns and
processes that are common within a studied phenomenon (e.g., childhood experiences of parental
feeding control practices; Glaser & Strauss, 1967).
Furthermore, as this study aimed to examine the meaning making and psychological
processes found in descriptions of childhood experiences of parental feeding control, the
constructivist version of GT was found to be most aligned with the current study’s objectives.

33
Past studies on parental feeding control have not adequately considered the numerous social
factors involved in these practices. Social relationships (e.g., family) are central to childhood
experiences of parental feeding control and, according to Charmaz (2006), individuals make
sense of their world through social relationships and interactions. As such, it is important to
consider the social influences involved in childhood experiences of parental feeding control.
With this being said, constructivist GT offers strategies and techniques that help the researcher
explore participants’ social experiences of a specific phenomenon, as well as co-construct the
meanings they attach to it (Tweed & Charmaz, 2012). Altogether, constructivist GT methods
lend themselves well to the aims of the current study.
Finally, it is recognized that the aim of GT is to develop theory that is grounded within
the data; however, GT methods often result in preliminary conceptualizations instead of formal
theories (Charmaz, 2008; Charmaz, 2014; Lichtman, 2013). As this study was conducted for a
Master’s thesis, the current constructivist GT study offers a preliminary conceptualization of the
processes involved in childhood experiences of parental feeding control. Based on the
previously mentioned arguments, constructivist GT was deemed a valuable and appropriate
method for this study as it allows the researcher to identify patterns and processes that are
common to a specific experience through the co-construction of meaning with their participants.
Procedures
Participant Recruitment
Recruitment for this study was conducted through poster advertisements. Posters
promoting the research study (see Appendix A) were displayed around the University of Calgary
campus. Posters included a brief description of the study, participation criteria, and my contact
information in case of interest.
34
Upon contacting me, interested individuals underwent a screening interview (see
Appendix B) to ensure that they met participation criteria for the current study. Inclusion and
exclusion criteria were as follows:
Participants must be between 18-29 years of age. This age group was chosen based on
their ability to reflect upon their childhood experiences of parental feeding control.
Participants must self-identify as individuals who have experienced parental feeding
control practices during their childhood.
Participants must have experienced parental feeding control practices for the purpose of
weight loss promotion or weight gain prevention.
Participants must not have memory impairment as this could interfere with their ability
to recall their childhood experiences.
Participants must not have impaired perceptions (e.g., psychosis), as impaired perceptions
could affect understanding of childhood events.
Participants must not have experienced feeding control practices as a result of abuse or
neglect. The purpose of this study is to examine parental feeding practices that were
purposeful and implemented with good intention (i.e., even though food was available it
was restricted).
Six individuals met the participation criteria, and shared their childhood experiences of parental
feeding control practices during an individual face-to-face interview with me. The interviews
took place in private rooms located in the Taylor Family Digital Library on the University of
Calgary campus. The interviews took 45 minutes on average to conduct.
Data Collection and Analysis
35
I followed constructivist GT data collection and analysis procedures (Charmaz, 2014).
As such, data collection and analysis took place concurrently which allowed me to develop a
deeper understanding of the studied experience (Charmaz, 2006). In order to be transparent
about the research process, strategies and procedures for data collection and analysis are outlined
below.
Data was collected over a period of 3 months (from January to March of 2017).
Informed consent forms (see Appendix C) were sent to participants via e-mail prior to the
interview process for their review. Additionally, I reviewed informed consent with participants
at the beginning of the face-to-face interview, and answered questions, as necessary. Once
informed consent was obtained, participants filled out personal demographic information (see
Appendix D) including gender, age, highest level of education attained, income status, and ethnic
background, as well as participants’ perception of parental demographic information which
included the parental household income, and the mother and father’s ethnic background. Lastly,
participants were asked to report which parent(s) was responsible for controlling their food
intake.
Interviews. This study aimed to explore how young adults describe their childhood
experiences of parental feeding control practices. Thus, it was necessary to implement an open
and exploratory approach to interviewing that allowed for psychological processes to be explored
(Strauss & Corbin, 1990). Consequently, a semi-structured interview approach, outlined by
Charmaz (2014), was used. In line with GT, interview questions were open-ended (see
Appendix E) which allowed participants to comment on the experiences and topics that were
most significant to them.
I transcribed all of the interviews verbatim (this included utterances and non-verbal

36
language) to ensure accuracy of analysis, and to enable increased contact with the data. This
increased contact allowed me to become immersed in the language and meanings of the
participants (Charmaz, 2006), as well as generate further research ideas (Charmaz, 2006). I
utilized these ideas to later develop more direct interview questions to obtain a more
comprehensive understanding of childhood experiences of parental feeding control.
GT Methods and Data Analysis
There are various essential strategies and procedures that constructivist GT studies
employ. These techniques include questioning, theoretical sampling, the constant comparison
method, memo writing and reflexivity, and theoretical sensitivity.
Questioning. In constructivist GT, semi-structured interviews are often utilized to
collect qualitative data for analysis (Charmaz, 2014). During these semi-structured interviews,
constructivist grounded theorists must strike a balance between the use of non-directive
interview strategies (e.g., asking a small number of open-ended questions in order to grasp the
participant’s experience), with directive interview methods (e.g., asking many focused questions
to solidify or dispute conceptualizations; Charmaz, 2014). In order to attain this balance,
researchers can begin the research process by asking general open-ended questions, and adding
more focused questions later on (Charmaz, 2014).
For this study, an interview guide was developed. This guide included broad open-ended
questions, as well as possible follow-up queries. Later in the data collection process, more
purposeful open-ended interview questions were added to the guide in order to help me explore
particular theoretical hunches. Moreover, in order to mitigate the potential risk of influencing
the data to confirm preconceived ideas, I kept questions open-ended, used the interviewees’
language, followed the interviewees’ lead, and asked the interviewees to define their taken-for-
37
granted meanings (Charmaz, 2014). With this being said, the interview guide was not always
followed, and the language used during interviews changed depending on the participant’s
preferred terms.
Theoretical sampling. Theoretical sampling is used to obtain new data in order to
further develop the emerging GT (Charmaz, 2014). This technique is employed after
preliminary categories have been conceptualized (Charmaz, 2008, 2014). In order to carry out
theoretical sampling, the researchers must ask: “Who do I need to interview to further develop
this category?” In general, theoretical sampling takes place until saturation is reached (i.e.,
where no new developments arise; Charmaz, 2008). In this study, theoretical sampling began
after many categories had been developed. During the theoretical sampling portion of data
collection, interview questions were more purposeful and related to the categories that had
previously emerged through data analysis.
Constant comparison method. Through the constant comparison method, GT data
analysis occurs at the same time as data collection (Charmaz, 2008; Tweed & Charmaz, 2012).
By using the constant comparison method, constructivist grounded theorists become more apt to
notice similarities, differences, and relationships that are grounded within the data (Boeije, 2002;
Charmaz, 2006; Hutchinson & Wilson, 2001). Ultimately, this method aids in the development
of conceptual and theoretical categories (Boeije, 2002; Charmaz, 2008).
In this study, I collected most of the data through semi-structured interviews. In addition
to interview transcripts, interesting thoughts and observations that took place during the data
collection process were also noted (i.e., memos) and analyzed (Charmaz, 2014). Interview
transcript and memo data were coded and organized into categories through the use of GT’s
constant comparison method (Charmaz, 2006).
38
Coding. Coding refers to describing or summarizing meaningful segments of the data
(Charmaz, 2006; Miles & Huberman, 1994). Through coding, constructivist grounded theorists
focus on the actions participants describe, and on the meanings they assign to those actions
(Charmaz, 2008). In this study, various coding phases were utilized. The initial coding
techniques used in this study were line-by-line and in-vivo coding (Charmaz, 2006). In the
second coding phase, focused coding took place (Charmaz, 2006). Finally, the third coding
phase consisted of theoretical coding (Charmaz, 2006).
During the initial coding process, I created “active codes” (i.e., reflect the action
described) for each sentence (i.e., line-by-line coding) of the interview transcripts and memos.
Line-by-line coding enabled me to remain immersed in the data, while also taking an analytic
position towards it (Charmaz, 2008). Using gerunds (i.e., the noun form of a verb) to code the
data preserved action by indicating what individuals were doing in the studied data segment
(Tweed & Charmaz, 2012). This technique helped me to make implicit processes and meanings
more explicit (Tweed & Charmaz, 2012). Therefore, line-by-line coding with gerunds allowed
me to remain close to the data (Charmaz, 2014; Tweed & Charmaz, 2012), while staying focused
on developing meaningful categories (Charmaz, 2006).
Furthermore, during the initial coding phase, I engaged in in-vivo coding. In-vivo codes
are direct quotes used by participants during the interview process that convey a taken-for-
granted meaning (Charmaz, 2014). These codes help to give meaning to the data, and inhibit
researchers from imposing their personal ideas on the codes (McCann & Clark, 2000a). In this
study, I made every effort to ask questions about participants’ taken-for granted meanings, and
made sure to include in-vivo data in the report to accurately reflect participants’ experiences.
Once line-by-line and in-vivo coding were complete, I began focused coding, where the
39
codes are more conceptual (Charmaz, 2006). During this coding phase, I used the most
significant initial codes and conceptualized them into focused codes in order to organize the data
from each interview in a meaningful manner (Charmaz, 2006, 2008). Through this method,
preliminary categories were developed. Focused coding further encouraged me to define the
relationships between emerging categories, and prompted additional insight and questions that
led to the refinement and elaboration of the emerging GT (Charmaz, 2006).
Lastly, I engaged in theoretical coding where links between categories were made.
Through theoretical coding, I was able to organize the substantive categories, and make
hypotheses about how they relate to one another (Charmaz, 2014). Altogether, theoretical
coding facilitated the development of an initial conceptualization of how young adults describe
their childhood experiences of parental feeding control practices (Charmaz, 2006, 2014).
Memo writing and reflexivity. Memo writing allows researchers to make note of their
thoughts, hypotheses, conceptualizations, and decision-making during the research process
(Charmaz, 2006). Charmaz (2008) argued that category development is unavoidably impacted
by the researcher’s personal background and biases. Consequently, reflexivity becomes a
necessary practice throughout the progression of research in constructivist GT. Reflexivity
refers to the researcher’s ability to recognize and evaluate how their past experiences influence
their research related decision making process (Charmaz, 2014; Hutchinson & Wilson, 2001). In
constructivist GT, this recognition of personal biases and their impact on the research, as well as
the decision making process, is documented through memo writing (Hutchinson & Wilson,
2001).
In this study, memo writing took place throughout the entire research process (Tweed &
Charmaz, 2012). Memos were written for three main reasons: to aid in my analysis of the data,
40
to keep a research audit trail, and to demonstrate reflexivity (Charmaz, 2014; Miles and
Huberman, 1994). Thus, I developed codes and categories while also conceptualizing their
relationships through the process of memo writing (Hutchinson & Wilson, 2001). Furthermore, I
presented evidence (i.e., quotes) from the raw interview data to support category definitions and
relationships in the memos (Charmaz, 2008). Lastly, in order to demonstrate my process of self-
evaluation, personal biases were recognized and assessed through memo writing (Charmaz,
2008, 2014).
Theoretical sensitivity. Theoretical sensitivity refers to the researcher’s ability to build
a theory as it emerges from the qualitative data (Charmaz, 2014). Theoretical sensitivity
involves going to the root of the studied phenomenon and defining the processes involved
without undue influence from other established theories (Charmaz, 2014). In this study, I aimed
for theoretical sensitivity by conducting a preliminary literature review to become aware of
sensitising concepts, and by being open to unanticipated results throughout the research process
(Charmaz, 2014; Glasser & Strauss, 1967).
Ethical Considerations
The University of Calgary Conjoint Faculties Research Ethics Board approved this study.
Participants received a $20 gift card to Cadillac Fairview malls to thank them for their
participation in the study. Given that the incentive to participate was less than $50, it is believed
that the payment encouraged individuals to engage in the research, but did not cause undue
influence or manipulation. Furthermore, it was recognized that recalling childhood experiences
of parental feeding control could be distressing for some participants. As such, a distress
protocol was developed and outlined in the consent form (see Appendix C).
41
Many steps were taken to guarantee the ethical and confidential storage of data. To
begin, the project supervisor and I had access to the confidential data. The electronic data files
(e.g., audio recordings and transcripts) were stored on password protected computers in
encrypted files that only myself and the project supervisor had access to. Additionally, during
the informed consent process, each participant selected a pseudonym to which their information
(i.e., demographic information and interview transcripts) was ascribed. In this way, any
accessible data provided by this individual was only associated with the pseudonym provided.
Lastly, consent forms were stored in a locked cabinet separate from participant demographic
forms.
Evaluating Grounded Theory
Methods for evaluating qualitative research continue to be highly debated (Corbin &
Strauss, 2008). However, Charmaz (2014) developed four substantive criteria for assessing GT
studies; these include credibility, originality, resonance, and usefulness. These four criteria
require the researcher to engage in self-evaluation throughout the research process (Corbin &
Strauss, 2008). The present study’s emerging GT was evaluated through its ability to answer the
following questions provided by Charmaz (2014, p. 337-338):
1. Credibility: Has your research achieved intimate familiarity with the topic? Are the
data sufficient to merit your claims, considering range, depth, and number of
observations in the data? Do the categories cover a wide range of empirical
observations? Has your research provided enough evidence for your claims to allow
the reader to form an independent assessment and agree with your claims?
2. Originality: Do your categories offer new insights? Does your analysis provide a new
conceptual interpretation of the data? How does your GT challenge, extend, or refine
42
current ideas and concepts?
3. Resonance: Do the categories portray the fullness of the studied experience? Have
you revealed taken-for-granted meanings? Does your GT make sense to your
participants or people who share their circumstances?
4. Usefulness: Does your analysis offer interpretations that people can use in their
everyday worlds? Can the analysis spark further research in other substantive areas?
How does your work contribute to knowledge? How does it contribute to making a
better world?
Strategies for Evaluation
Charmaz’s (2014) criteria and questions guide constructivist grounded theorists to
evaluate their emerging GT during the research process. However, other strategies may also be
useful in evaluating qualitative research. For example, Creswell (2007) outlined eight validation
techniques for evaluating qualitative research, and suggested that qualitative researchers use at
least two of these strategies to assess research credibility. The following two techniques from
Creswell’s (2007) list were employed to attend to trustworthiness.
Thick descriptions. Thick descriptions of research participants allow readers to
determine the transferability of the study’s findings (Charmaz, 2014; Creswell, 2007). As such,
participant demographic information has been thoroughly described in the results section.
Furthermore, a researcher can also gain thick descriptions when they endeavour to make implicit
meanings more explicit (Charmaz, 2008). In this study, I asked participants to elaborate on their
wording and definitions in order to accurately understand their taken-for-granted meanings.
Triangulation. Triangulation involves using different sources (e.g., consultation with an
expert in the field and revisiting the research literature) to provide corroborating evidence for
43
category formation and theory development (Creswell, 2007). By substantiating results through
triangulation, the researcher adds to the trustworthiness of the data analysis (Creswell, 2007;
Hutchinson & Wilson, 2001). In order to enhance the credibility of the current study’s results, I
consulted with my project supervisor and doctoral candidate mentor regarding the process of
category and theory development, as well as conducted a second literature review in order to
explain and find further evidence for my research findings.
Chapter Summary
A constructivist GT methodology was utilized to answer the present study’s research
questions: How do young adults make meaning of their childhood experiences of parental
feeding control practices? and What are the perceived psychological impacts of parental feeding
control practices? Constructivist GT consists of strategies used to construct a theory from
qualitative data (Tweed & Charmaz, 2012). Constructivist grounded theorists assume that
multiple realities exist, and that realities are co-constructed through social interactions between
individuals who embody different perspectives (Mills et al., 2006). Consequently, researchers
who employ this method acknowledge how researchers’ and their participants’ backgrounds and
biases influence the data and its analysis (Ghezelije, & Emami, 2009; Tweed & Charmaz, 2012).
Thus, a constructivist GT emerges from the data, and is co-constructed between researchers and
their participants (Charmaz, 2014). Constructivist GT methods fit the aim of this study, and
guided the process of data collection and analysis.
44
CHAPTER FOUR
Results
This chapter offers a description of the results of data analysis and the generation of a
preliminary constructivist grounded theory (GT). The objective of this study was to describe
meaning making and psychological impacts of experiencing parental feeding control practices,
intended to promote weight loss or to prevent weight gain (i.e., dietary restriction, monitoring,
and pressure), during one’s childhood. As a formal GT is typically developed over many years,
and with numerous research participants, I recognize that the current analysis represents a
preliminary theoretical conceptualization of the meaning making and psychological processes
associated with childhood experiences of parental feeding control. Data collection was achieved
through semi-structured interviews, and the constructivist interpretation of GT methods was used
to code and analyze the transcribed interviews. Results of the data analysis process formed the
preliminary constructivist GT.
Participants
Eighteen individuals contacted me to participate in the study upon viewing the
recruitment poster. I responded to all of the potential participants with an initial e-mail. Twelve
individuals followed up with a phone call to undergo the screening interview (see Appendix B).
Nine individuals met inclusion criteria, based on the recruitment screening questions, and
interviews were scheduled. In GT, data collection and analysis occurs concurrently (Charmaz,
2006); therefore, one or two interviews were booked at a time, and I scheduled them one to two
weeks apart to allow for concurrent data analysis. One participant did not show up for the
interview, and two participants were not included in the analysis as it became apparent, during
the interview, that they did not meet participation criteria (i.e., one participant had not
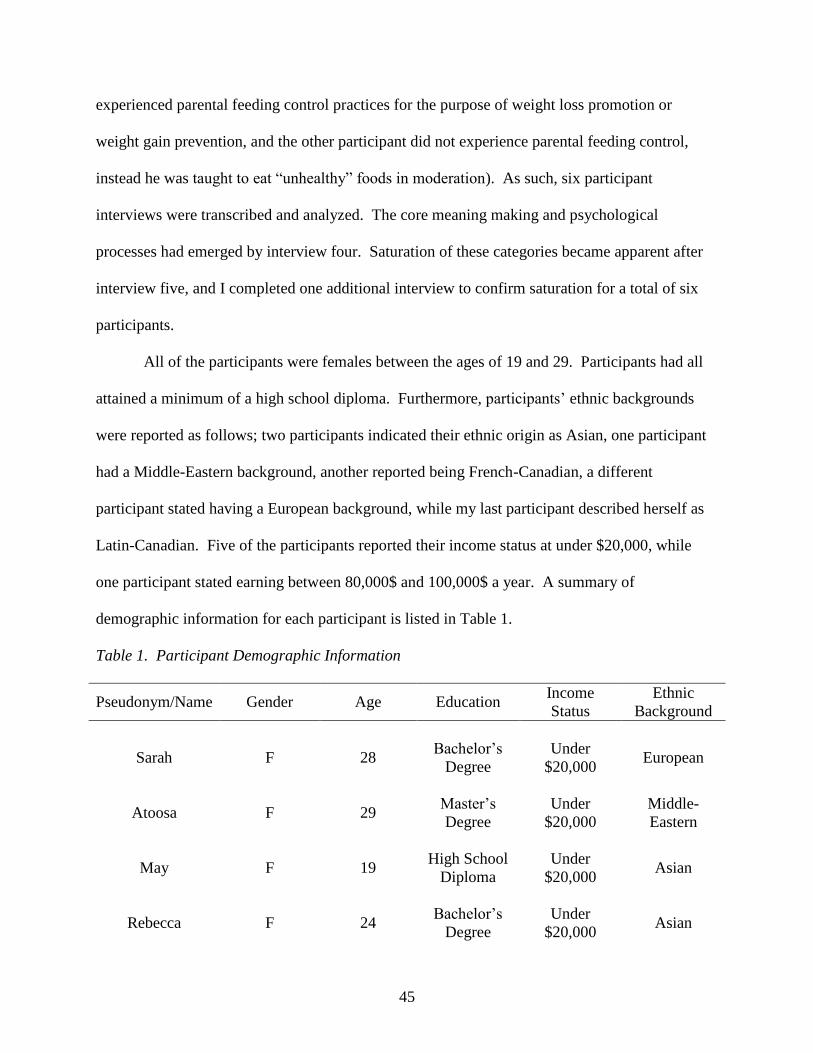
45
experienced parental feeding control practices for the purpose of weight loss promotion or
weight gain prevention, and the other participant did not experience parental feeding control,
instead he was taught to eat “unhealthy” foods in moderation). As such, six participant
interviews were transcribed and analyzed. The core meaning making and psychological
processes had emerged by interview four. Saturation of these categories became apparent after
interview five, and I completed one additional interview to confirm saturation for a total of six
participants.
All of the participants were females between the ages of 19 and 29. Participants had all
attained a minimum of a high school diploma. Furthermore, participants’ ethnic backgrounds
were reported as follows; two participants indicated their ethnic origin as Asian, one participant
had a Middle-Eastern background, another reported being French-Canadian, a different
participant stated having a European background, while my last participant described herself as
Latin-Canadian. Five of the participants reported their income status at under $20,000, while
one participant stated earning between 80,000$ and 100,000$ a year. A summary of
demographic information for each participant is listed in Table 1.
Table 1. Participant Demographic Information
Pseudonym/Name Gender Age Education Income
Status
Ethnic
Background
Sarah F 28 Bachelor’s
Degree
Under
$20,000 European
Atoosa F 29 Master’s
Degree
Under
$20,000
Middle-
Eastern
May F 19 High School
Diploma
Under
$20,000 Asian
Rebecca F 24 Bachelor’s
Degree
Under
$20,000 Asian

46
Jackie F 27 Bachelor’s
Degree
$80,000 to
just under
$100,000
French-
Canadian
Emma F 28 Bachelor’s
Degree
Under
$20,000 Latin
Participants’ perceived parental demographic information was also collected.
Participants’ parents had educational backgrounds raging from high school diplomas to doctoral
degrees. Parental income statuses spanned from $40,000 to $150,000 and above. Moreover, all
of the participants indicated that their mothers were responsible for the dietary control; however,
three participants reported that their fathers also participated in controlling their dietary intake.
A summary of participants’ parental demographic information is listed in Table 2.
Table 2. Participants’ Parental Demographic Information
Pseudonym
/Name
Mother’s
Education
Father’s
Education
Mother’s
Ethnic
Background
Father’s
Ethnic
Background
Parental
Income
Status
Responsible
for Feeding
Sarah Bachelor’s
Degree
Bachelor’s
Degree European European
$100,000 to
just under
$150,000
Mother
Atoosa Diploma Master’s
Degree
Middle
Eastern
Middle
Eastern
$40,000 to
just under
$60,000
Mother
May Doctoral
Degree
Bachelor’s
Degree Asian Asian
$150,000
and above
Mother and
Father
Rebecca College
Degree
College
Degree Asian Asian
$80,000 to
just under
$100,000
Mother and
Father
Jackie Bachelor’s
Degree
High
School
Diploma
French-
Canadian European
$100,000 to
just under
$150,000
Mother and
Father

47
Emma College
Degree
Master’s
Degree Latin Latin
$150,000
and above Mother
Development of Themes and Categories
Theory development in constructivist GT is emergent and constructed (Charmaz, 2006).
It involves abductive reasoning in which the researcher studies the data, develops hypotheses
about the processes that are emerging from the data, and then verifies them empirically by re-
examining the data (Charmaz, 2006).
Constructivist GT Data Analysis Procedures Revisited
Data was collected over a three month period. The interviews were guided by pre-
established semi-structured interview questions (see Appendix E). Throughout the interviews, I
asked follow-up questions and clarifying probes to ensure that I was reasonably interpreting and
understanding participants’ answers. The interview questions were not always asked in the same
order and some probes were omitted in order to reduce redundancy. During the interviews, I
asked broad questions such as, “In what ways, if any, have you been psychologically impacted
by being put on a diet by your parents as a child?” Asking such questions enabled me to gain a
deeper understanding of participants’ experiences of parental feeding control practices and
whether those experiences were consistent with emerging core concepts, themes, and sub-
themes. Furthermore, later in the data collection process, I asked participants more focused
questions in order to develop and refine core concepts, themes, and sub-themes that had emerged
in previous interviews. For example, participants were asked if a previous theme, such as fearing
weight gain, fit within their experience of parental feeding control practices, and if so, how it fit.
Thus, later data collection was impacted by earlier data collection and analysis.
48
Altogether, five preliminary core concepts, and their encompassing themes and sub-
themes, were co-constructed through the process of data collection and analysis. I developed
several different versions of the theoretical model to attempt to conceptualize how the core
concepts, themes, and sub-themes were connected. I engaged in memoing throughout data
collection and analysis (Appendix F provides examples of memos written during the data
collection and analysis). Once it appeared that no new categories were emerging from the data, I
interviewed two more participants to assess whether saturation had been met. When the data fit
within the previously established core concepts, themes, and sub-themes it was deemed that
saturation had been achieved and data collection concluded.
The Constructivist Grounded Theory
The results of this study are presented as a preliminary theoretical model aimed at
capturing the meaning making and psychological processes associated with childhood
experiences of parental feeding control. Core concepts, themes, and sub-themes that form the
constructivist GT emerged through a process of coding, constant comparative analysis, and
theorizing. Participant quotes are used throughout the results section to exemplify the core
concept, themes, and sub-themes, as well as their properties. Participant quotes have been edited
to increase readability (e.g., removing “like”); however, the substantive meanings of the quotes
were not changed. When direct quotes from participants are used, participants’ chosen
pseudonyms are shared. In the general discussion of the constructivist GT, participants are
referred to in the third person as the GT is proposed to represent the participants as a whole.
Identified Core Concepts, Themes, and Sub-Themes
Data analysis resulted in the identification of five core concepts, these included: (a)
making meaning of parental feeding control, (b) experiencing psychological impacts, (c)
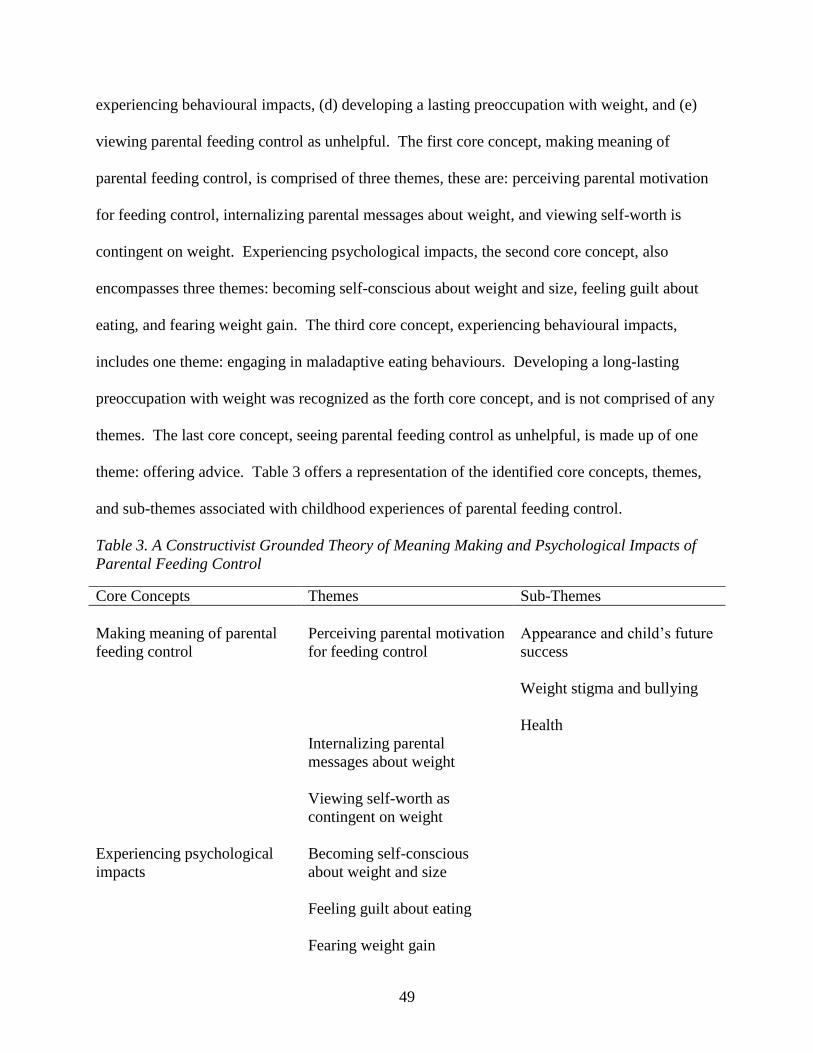
49
experiencing behavioural impacts, (d) developing a lasting preoccupation with weight, and (e)
viewing parental feeding control as unhelpful. The first core concept, making meaning of
parental feeding control, is comprised of three themes, these are: perceiving parental motivation
for feeding control, internalizing parental messages about weight, and viewing self-worth is
contingent on weight. Experiencing psychological impacts, the second core concept, also
encompasses three themes: becoming self-conscious about weight and size, feeling guilt about
eating, and fearing weight gain. The third core concept, experiencing behavioural impacts,
includes one theme: engaging in maladaptive eating behaviours. Developing a long-lasting
preoccupation with weight was recognized as the forth core concept, and is not comprised of any
themes. The last core concept, seeing parental feeding control as unhelpful, is made up of one
theme: offering advice. Table 3 offers a representation of the identified core concepts, themes,
and sub-themes associated with childhood experiences of parental feeding control.
Table 3. A Constructivist Grounded Theory of Meaning Making and Psychological Impacts of
Parental Feeding Control
Core Concepts Themes Sub-Themes
Making meaning of parental
feeding control
Perceiving parental motivation
for feeding control
Appearance and child’s future
success
Weight stigma and bullying
Health
Internalizing parental
messages about weight
Viewing self-worth as
contingent on weight
Experiencing psychological
impacts
Becoming self-conscious
about weight and size
Feeling guilt about eating
Fearing weight gain
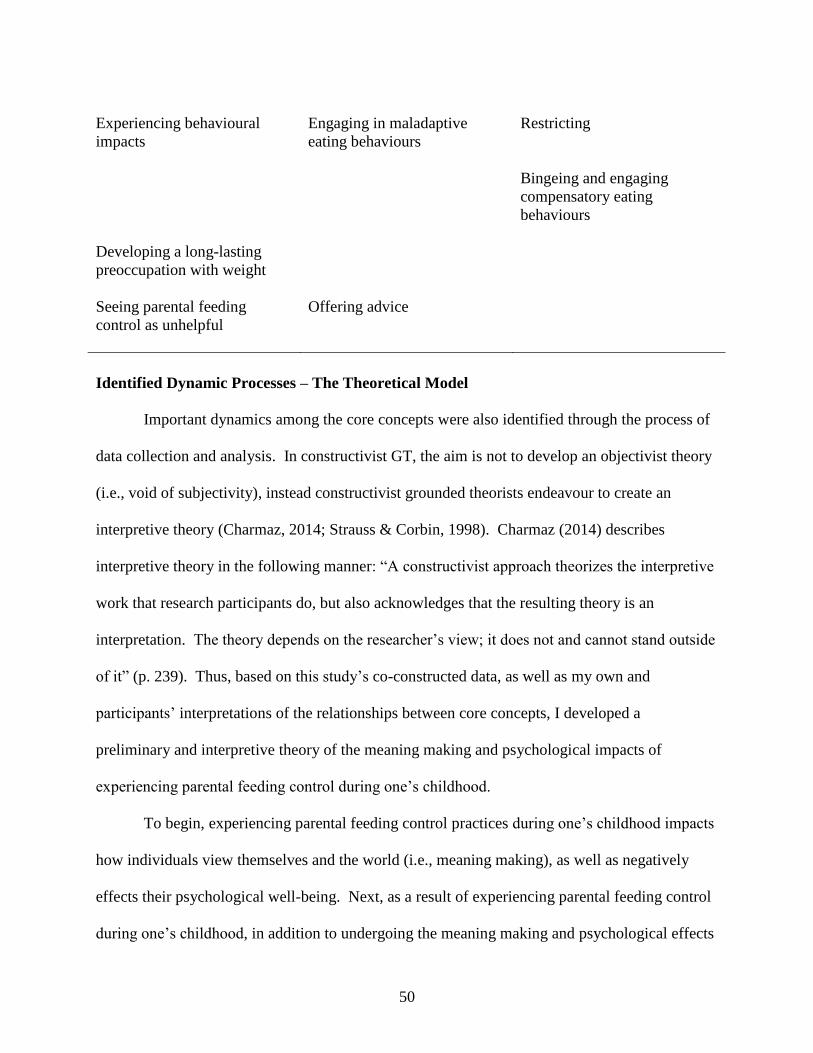
50
Experiencing behavioural
impacts
Engaging in maladaptive
eating behaviours
Restricting
Bingeing and engaging
compensatory eating
behaviours
Developing a long-lasting
preoccupation with weight
Seeing parental feeding
control as unhelpful
Offering advice
Identified Dynamic Processes – The Theoretical Model
Important dynamics among the core concepts were also identified through the process of
data collection and analysis. In constructivist GT, the aim is not to develop an objectivist theory
(i.e., void of subjectivity), instead constructivist grounded theorists endeavour to create an
interpretive theory (Charmaz, 2014; Strauss & Corbin, 1998). Charmaz (2014) describes
interpretive theory in the following manner: “A constructivist approach theorizes the interpretive
work that research participants do, but also acknowledges that the resulting theory is an
interpretation. The theory depends on the researcher’s view; it does not and cannot stand outside
of it” (p. 239). Thus, based on this study’s co-constructed data, as well as my own and
participants’ interpretations of the relationships between core concepts, I developed a
preliminary and interpretive theory of the meaning making and psychological impacts of
experiencing parental feeding control during one’s childhood.
To begin, experiencing parental feeding control practices during one’s childhood impacts
how individuals view themselves and the world (i.e., meaning making), as well as negatively
effects their psychological well-being. Next, as a result of experiencing parental feeding control
during one’s childhood, in addition to undergoing the meaning making and psychological effects

51
of those practices, individuals experience behavioural impacts (i.e., engaging in maladaptive
eating behaviours). Overall, the meaning making, psychological, and behavioural impacts of
experiencing parental feeding control practices during one’s childhood have a lasting effect on
individuals’ psychological well-being and eating behaviours in the form of persistent weight
preoccupation. Altogether, due to its negative meaning making, psychological, and behavioural
impacts, parental feeding control practices were seen as unhelpful. The following figure further
illustrates the dynamics between the recognized core concepts.
Figure 2. The Constructivist Grounded Theory of Meaning Making and Psychological Impacts
of Parental Feeding Control
In order to better understand the core concepts, themes, and sub-themes involved in
childhood experiences of parental feeding control, as well as how they relate to one another, the
following sections describe and exemplify the differing components of the current study’s
preliminary constructivist GT.

52
Making Meaning of Parental Feeding Control
The first identified core concept was making meaning of parental feeding control.
Participants described three themes under this core concept, these were: (a) perceiving parental
motivation for feeding control, (b) internalizing parental messages about weight, and (c) viewing
self-worth as contingent on weight.
To begin, participants reported receiving parental messages, either implicitly or
explicitly, about weight based on their perception of their parents’ motivation for controlling
their dietary intake. For example, if a participant’s parents employed feeding control practices
for appearance reasons, they received the implicit message that being overweight is unattractive.
Moreover, as a result of receiving these implicit or explicit messages about weight, participants
reported internalizing and adopting these messages as their own way of conceptualizing
themselves and the world. In line with this internalization of negative parental messages about
weight, participants began viewing being overweight as less attractive, desirable, as well as less
worthy of love and attention. Subsequently, participants indicated that they started viewing their
own self-worth as being conditionally dependent on their weight. For example, if they gained
weight, they felt less worthy of love. The following sections illustrate in greater detail the
meaning making process associated with experiencing parental feeding control practices during
one’s childhood.
Perceiving parental motivation for feeding control. Participants described perceiving
a variety of parental motivations for utilizing feeding control practices, these sub-themes
included: (a) appearance and child’s future success, (b) weight stigma and bullying, and (c)
health motivations. Whether the parental feeding control practices were utilized for appearance
53
or health reasons, participants received implicit or explicit messages about weight based on their
perceptions of their parents’ motivation for controlling their dietary intake.
Appearance and child’s future success. Many participants indicated perceiving
appearance as the motivating factor for their parents’ use of feeding control practices, and that
appearance was related to future success. For example, Emma recounted her perception of her
mother’s motivation for utilizing feeding control practices:
I think every mom wants their kid to be good looking or successful, right? In Argentina,
it’s a culture thing. Girls are meant to be perfect and have the perfect body and so a lot of
it [using parental feeding control practices] I think was coming from there.
Emma continued to describe the culture in which she was raised, and how it could have impacted
her mother’s motivation for using feeding control practices:
Back there [Argentina], if you are skinny or if you are pretty, you’re going to be
successful. For example, when you apply for a job, you have to send a picture. That’s
how things go. There's a lot of pressure on that front so I think she was trying to kind of
steer me that way. It’s like if you’re skinny, you’re going to be more successful. I think
that was her reasoning behind it.
May described the explicit parental messages about weight that revealed their appearance and
future success motivations for utilizing feeding control practices:
They [my parents] were like, ‘you need to lose weight and you need to be pretty’ and
‘this is for you [and your future success].’
Rebecca recalled perceiving her father’s appearance motivations for utilizing feeding control
practices:
54
He would always emphasize the health part but I think for him it was probably about
appearance as well. He would always talk about being healthy, but he would also add:
‘when you're older and people don't find you attractive or beautiful, don’t blame me.’
By perceiving their parents’ appearance and future success motivations for using feeding control
practices, participants received the following messages: being overweight makes you (a) less
attractive, and (b) less likely to be successful in the future.
Weight stigma and bullying. Some participants viewed their parents’ motivation for
using feeding control practices as related to fears about their child being stigmatized or bullied.
Rebecca exemplified this perception in the following quote:
I think my dad was just worried about how society would perceive me [if I was
overweight] and whether or not I would be able to fit in, and that people would bully me
or pick on me.
Jackie explained her perception of her dad’s bullying related motivation for using feeding control
practices:
My dad was like, ‘maybe she’ll feel better if she doesn’t get teased’ because I was
bullied a little bit for my weight.
In these cases, participants received the message that being overweight will result in weight-
related stigmatization and/or bullying.
Health. Health was also perceived to be a motivator for the use of parental feeding
control practices by a few participants. Participants reported that their parents became concerned
about their weight due to a doctor or health professional’s feedback. Jackie recalled her parents
being motivated to change her diet based on a doctor’s recommendation:
55
Based on my understanding of it [parents’ motivation for using feeding control practices],
the Dr. was concerned about where my weight was, so they [my parents] basically took
that on as needing to do something about it.
Atoosa experienced parental feeding control practices due to feedback her parents received from
a physical education teacher. She recounted her experience in the following quote:
I remember it was part of the exercise course [at school]. We went to a gym and they
weighed all the children in front of each other and it was really embarrassing. They told
me that they needed to talk to my mom and they asked me for her phone number. They
consulted with my mom and told her to put me on a diet.
Perceiving health motivations for using parental feeding control practices indicated to
participants that being overweight is unhealthy.
Altogether, participants described that their parents were implicitly or explicitly
expressing particular messages about weight depending on their motivation for controlling their
dietary intake. These messages included: being overweight (a) is unattractive and will negatively
impact future success, (b) will lead to being stigmatized and bullied, and (c) is unhealthy. In
sum, through parental feeding control practices, parents were reinforcing the message that being
overweight is bad.
Internalizing parental messages about weight. As a consequence of receiving implicit
or explicit parental messages about weight, participants recounted internalizing and adopting
these weight-related messages as their own way of conceptualizing themselves and the world.
Therefore, participants began viewing being overweight as less attractive, desirable, and worthy
of love and attention. Collectively, these internalized parental messages about weight began to
skew how participants’ viewed themselves, others, and the world. For example, Emma

56
described how she internalized her mother’s concern for appearance through her explicit
messages about weight and eating:
I think it all started with the comments [about my weight and eating habits] but
eventually I started internalizing it and making them part of how I see myself and how
much importance I put on appearance because of my mom...I feel like now, in a way,
even my own values are affected by the way I was brought up.
May described internalizing appearance expectations from parental messages about weight:
When I was young I wanted to diet because of their [parents’] expectations, and now, I
want to diet because of my expectations.
May further reported internalizing parental messages about her body, weight, and eating due to
parental feeding control practices:
They [my parents] made me realize that there’s always a problem [with my body, weight,
and eating]. Their constant pressure, for years and years, shaped the way I see things [my
body, weight, and eating] too.”
Emma stated internalizing explicit parental messages about size:
Sometimes, I still hear my mother's voice [in my head] saying, ‘your legs are fat.’
She continued to explain that despite experiencing the negative effects of parental feeding
control practices, she would still be compelled to make comments about her child’s weight. The
following example shows how entrenched the internalization of parental messages about weight
can become:
As much as I wouldn’t like to admit it, and as much as I would like to say that if I had a
kid and they were gaining weight, I would just let them. If I have to be honest with
myself, I probably wouldn’t. I probably would say something, which is bad because I

57
went through that [experiencing parental feeding control practices] and I’m telling you
about all the trouble it caused.
These internalized parental messages about weight came together to form participants’ way of
viewing themselves and the world. Again, through the internalization of negative parental
messages about weight, participants started to adopt the view that being overweight is bad.
Consequently, participants described believing that their self-worth was dependent on their
weight.
Viewing self-worth as contingent on weight. Due to the internalization of negative
parental messages about weight, participants described seeing their worth as contingent on their
weight. They explained that they often felt, and continue to feel, less worthy, less attractive, and
less desirable when they were, or are, overweight. For example, Atoosa described how being
overweight affected, and continues to affect, her self-worth, confidence, and her ability to
socialize:
Whenever I gained weight, I became less confident, shy, and anxious. Even now. This is
my second year in university. In first year, I gained 8 kilos and now, I socialize less.
In this example, Atoosa outlined her experience of lowered self-worth and self-confidence due to
weight gain. She explained that, as a result of gaining weight, she feels less comfortable
socializing for fear of being judged by others. She went on to discuss how her overall self-
concept changes when she gains weight:
Today, I feel ugly again because I didn't exercise for a while and I gained weight. I don't
like to go to the gym and show my body to everybody. Something like that is always
going through my mind.
58
Sarah also described how her self-worth had become contingent on weight, and how she
continues to struggle with untangling the two:
It [feeling worthy when overweight] is something that I still struggle with. Because I
wasn't pretty or small, I was somehow less-than so I had to try harder [in other areas]
which is total societal bullshit and it’s really stupid and it’s not true at all but we’re lead
to believe these things [that being overweight makes you less-than] and so it's very hard
to untangle that as a conscious adult.
Sarah further explained how weight and appearance, over other qualities, had become paramount
in determining her self-worth:
It is almost like your appearance becomes everything and you ignore the fact that you
have other skills or other qualities, and that those also make you a whole person and they
make you worthwhile.
Emma echoed Sarah’s sentiment:
In a way, because I was so self-conscious [about my body] it was almost like my
confidence as a whole wasn't what it should have been. I wasn’t able to see that other
things, like the fact that I was smart and doing well in school, [made me worthy].
She further described how approaching a potential romantic partner was impacted by viewing
herself as less worthy of love because of her weight:
If I liked a guy, I wouldn’t just go for it and think, ‘maybe they like me back.’ I would
think, ‘they would never like me’ or ‘that guy would never go for me.’
Additionally, when participants reported being the only individual in the family that was made to
diet, they further internalized the idea of being less-than as a result of their weight status. For
example, Atoosa reported:

59
I felt, at that time, that she [my mother] didn’t like me because of my weight, because I
felt like she was saying, ‘because you are overweight, you are ugly. You are less likeable
than your other siblings.’ I was comparing myself to my other siblings all the time
because they were girls and I felt like she liked me less and I was ashamed.
In total, participants stated that the meaning making process associated with childhood
experiences of parental feeding control deeply impacted how they view themselves, others, and
the world. Furthermore, participants indicated that experiencing parental feeding control
practices during their childhoods affected their psychological well-being. The following section
describes the reported psychological impacts of experiencing parental feeding control.
Experiencing Psychological Impacts
The second recognized core concept was experiencing psychological impacts.
Participants described three psychological consequences of undergoing parental feeding control
practices during their childhoods, these themes were: (a) becoming more self-conscious about
their weight and size, (b) feeling guilt about eating, and (c) developing a fear of gaining weight.
The following sections illustrate the previously mentioned psychological consequences in more
detail.
Becoming self-conscious of weight. As a result of experiencing parental feeding control
practices, participants described becoming more self-conscious about their weight and size.
They reported feeling uncomfortable or embarrassed when being observed by others due to fears
that they would be judged for their weight and size. To begin, Emma described how she became
more self-conscious about the size of her legs due to explicit parental messages about weight and
size, as well as her perception of appearance motivations for her parents’ use of feeding control
practices:

60
When I was younger, I had a more muscular body type and I remember my mom
mentioning something like, ‘Emma’s legs are so big compared to her friends.’...That’s
when the whole thing with my legs started and me thinking that my legs were fat, and I
didn’t like showing my legs and I didn’t like wearing shorts and all this stuff. I feel like
that’s when I started changing the way I felt about myself. Looking back, I was not
overweight and it makes me a little bit angry now because I just had a different body
shape but it wasn’t a bad thing.
She continued to describe how being self-conscious about her legs persisted into adulthood:
I bought my first pair of skinny jeans when I was in 3rd year of university because I felt
so self-conscious about my legs and my butt and my hips...So it [feeling self-conscious
about my legs] continued on and [because of experiencing parental feeding control
practices] it did take me a very long time to accept my body.
Rebecca described becoming self-conscious about her weight at a very young age as a result of
her experience of parental feeding control practices:
I was a lot more conscious of my weight at a younger age. Like how I was already
noticing my size and my weight in grade one in comparison to my peers. I think I'm a lot
more conscious. Even now, I have to think about what food I’m eating and whether or
not I’m exercising enough.
Atoosa described not only being self-conscious of her body, but of the stretch-marks she
developed as a consequence of gaining weight during her childhood:
Even now, I am so upset about it [how my body looks], it has become an obsession for
me...all those stretch marks...that I am embarrassed of...I can still see the history [of
experiencing parental feeding control practices] on my body.

61
She further outlined how feeling self-conscious about her body made her feel uncomfortable in
social interactions:
It [being overweight] was awful because I felt like I was different from others. I
remember I couldn’t even look people in the eyes [because I was self-conscious about my
body].
In sum, as a consequence of experiencing parental feeding control behaviours, participants
became more focused on their weight and size, as well as became embarrassed of, and
uncomfortable in, their bodies.
Feeling guilt about eating. Participants indicated feeling guilty when they made food
decisions that went against their parents’ dietary wishes. They outlined that the guilt they felt,
and still feel, when eating particular foods was related to internalized parental messages they had
received as a result of experiencing parental feeding control practices. For example, Jackie’s
guilt was associated with consuming carbohydrates because she was put on a “low carb” diet
during her childhood. She described that the guilt she felt when eating carbohydrates carried on
into her adulthood:
I would feel awful, usually because it was carbs. I never threw up in middle school or
high school. In my undergrad, in first year, that was kind of when I struggled with that
[purging].
Rebecca explained how her guilt associated with eating developed. She described feeling as
though she would get in trouble with her father if she engaged in “sneak eating”:
So they [my parents] would just tell me not to snack very often. You know how kids
sneak eat? I’d do that quite a bit. That’s when my dad started being more on guard.
62
Whenever I went to the kitchen, he would watch me and so then I started being like a
little bit more scared and guilty around that aspect.
Furthermore, she indicated that she continues to feel guilty about certain dietary choices, even as
an adult:
I think I still carry guilt. Even nowadays, if I'm eating ice cream, I’ll have that in the
back of my mind, ‘I probably shouldn’t be eating this.’
Overall, through experiencing parental feeding control practices, participants reported
internalizing parental messages about “good” and “bad” foods, which lead to feelings of guilt
when participants consumed “bad” foods. Moreover, most participants outlined that this guilt
stuck with them even into adulthood.
Fearing weight gain. As an outcome of experiencing parental feeding control
behaviours, as well as internalizing associated parental messages about weight (e.g., being
overweight is bad), participants described developing a fear of gaining weight. They indicated
fearing weight gain as they did not want to be seen as less desirable, attractive, or worthy of
other peoples’ love and attention. Atoosa explained that she fears gaining weight as it affects her
confidence and elicits anxiety:
I become anxious and feel less confident and ugly whenever I see myself in the mirror
[and I have gained weight]...So I am really kind of [scared of gaining weight], it became
like a phobia for me of gaining weight.
Atoosa further described how she feels when she gains weight, as well as how she attributes
these feelings to her mother’s use of parental feeding control practices:
63
I feel scared or panic when I gain weight and I don't know why. I can't logically think
about it. I guess it is all because of my mom [and how she handled my weight “issue”]...I
blame her for that.
Rebecca reported the following when asked why she fears gaining weight:
I think that I’m not very attractive at that size and that people will probably think less of
me if I’m that large.
When asked why she feared gaining weight, Jackie offered the description below:
I think it is [due to] other people’s perception of it [being overweight]. As being
unattractive and something to make fun of someone for, or a deficit I guess.
Emma outlined her reasoning for fearing weight gain as being related to her worries of not being
worthy of the opposite sex’s attention:
If they [male peers] talked about girls that they liked, they would never mention the
chubby girl and I didn’t want to be that girl.
Overall, participants outlined developing a fear of gaining weight as a result of experiencing
parental feeding control practices. They described not wanting to gain weight for fear of being
seen as less desirable, attractive, and worthy of other peoples’ love and attention due to their
weight.
In sum, experiencing parental feeding control practices impacted participants’ overall
psychological well-being. Moreover, participants reported that the meaning making process and
the psychological impacts of experiencing parental feeding control practices came together to
affect their eating behaviours. In the following section, I describe how participants reported
engaging in maladaptive eating behaviours in order to remedy their weight-related psychological
distress.
64
Experiencing Behavioural Impacts
The third identified core concept was experiencing behavioural impacts. As a
consequence of undergoing parental feeding control practices during their childhoods, as well as
experiencing the negative meaning making and psychological outcomes of these practices,
participants described engaging in maladaptive eating behaviours, the only theme of this core
concept, in order to lessen their weight-related psychological distress. Furthermore, I interpreted
two sub-themes from participants’ descriptions of engaging in maladaptive eating behaviours,
these were: (a) restricting, and (b) bingeing and engaging in compensatory eating behaviours.
The following sections describe the maladaptive eating behaviours reported by participants in
greater detail. It is important to note that participants did not report engaging in all of the
compensatory behaviours outlined below; however, every participant did describe engaging in at
least one of the following behaviours as a consequence of experiencing parental feeding control
practices.
Engaging in maladaptive eating behaviours. Participants reported engaging in certain
maladaptive eating behaviours in order to manage their weight concerns, reduce their self-
conscious feelings about their weight and size, diminish their guilt associated with eating
particular foods, and lessen their fear of weight gain. Additionally, they reported engaging in
maladaptive eating behaviours to ensure that their worth would not be diminished by weight
gain.
Restricting. In order to promote weight loss, or to guarantee that they would not gain
weight, some participants indicated engaging in self-imposed dietary restriction. Emma
described restricting her own eating due to parental comments about her weight and size:

65
I would ruminate on her comments [about my weight and size] and they would really get
under my skin and eventually would change my [eating] behaviours.
May indicated engaging in calorie restriction in order to lose weight, as well as being motivated
to continue restricting her calories due to weight loss:
I was kind of excited to go on a stricter diet with 1,200 calories a day. After a week, I
saw that it worked... Once you see your weight drop, you’re more motivated to do that
[continue restricting calories].
Sarah described how she internalized her parents’ use of dietary restriction:
Going from really overeating when I was young and being commented on that [my eating
and weight], to eating way less [due to parental feeding control practices], and then I
developed sort of an eating disorder after that point.
In summary, as a result of experiencing parental feeding control practices during their
childhoods, participants described engaging in self-imposed dietary restriction in order to
continue managing their weight concerns.
Bingeing and engaging in compensatory eating behaviours. As a result of prolonged
restriction, some participants reported going through cycles of bingeing and restricting, while
others indicated experiencing phases of bingeing and purging. Participants described growing
tired of dietary restriction, which resulted in bingeing in order to experience dietary freedom.
They stated that the freedom they felt, as a consequence of bingeing, was short-lived as they
were quickly consumed with feelings of guilt, which prompted further dietary restriction or
purging. The sections below describe the binge/restrict and binge/purge cycles reported by
certain participants.
66
Some participants described bingeing as a result of being on a diet for a prolonged period
of time, and trying to remedy the binge through additional dietary restriction. These behaviours
came together to form a binge and restrict cycle. Sarah described her bingeing and restricting as
follows:
It [experiencing parental feeding control practices] set me up for a lifetime of that
restricting, binge, restrict, binge, restrict behaviour. Because it's [restricted food]
forbidden, [I would think,] ‘I’m going to eat all the things [restricted foods] now because
I’m never having it again...I’ll go forward being good: tomorrow and forever.’
Emma described her inhibition and restriction cycles in the following manner:
I remember all of my friends had the thigh gap and I hated the fact that my thighs rubbed
against each other. So I would take care of my eating and then I would realize that I still
didn’t have a thigh gap and I would just be like, ‘screw it [dietary restriction]’ and I’d eat
whatever I wanted. Then, I would kind of go back and start, because my mom would
make a comment like, ‘you shouldn’t be eating so much junk food’, and then I would go
back to taking care of what I ate. So it would go in cycles.
Emma continued to explain how parental messages about her weight and size would push her to
cycle from inhibited to restricted eating:
If she [my mother] would be like, ‘I think your thighs are a little bigger’ or like ‘I think
you’re gaining weight a little. Your butt looks bigger’, then I would go sort of steering
the bus the other way to get on the restricting side of things.
In summary, participants reported being stuck in a cycle of restriction and inhibition, where they
craved freedom from their dietary restriction but once they strayed from their diets, they felt
guilty about their food intake which lead them to, once again, restrict their eating.
67
Other participants reported purging the food they had consumed during a binge in order
to neutralize their feelings of guilt. May outlined her experience of bingeing and purging in the
following quotes:
I know it's super unhealthy but I do have binges sometimes, especially [when I’m] on
diets. When I was younger, after binging, I would throw up but then I googled all of the
symptoms of doing this and they were super bad, but even though I knew it was super
bad I, the more restrictive it is, the more I feel like I need to break free of that [restriction]
and I would binge and then I would feel bad and so then I would throw up.
She went on to explain the thought-process involved in bingeing and purging as it relates to
dietary restriction:
Being on a diet for a long time, you’re just kind of sick of it and you want to eat. But
then there's a lot of pressure from other people to stay on your diet so then that makes you
want to throw up. At the same time, [I’m thinking,] ‘I worked so hard [to lose weight]’
so I just want to have a day of break [from my diet] but then afterwards I feel like, ‘I
worked so hard [to lose weight] and maybe I should not do this [take a break from my
diet and binge eat].’
Sarah explained that she found relief in purging as it meant that she could take a break from
restriction and engage in bingeing without experiencing its negative consequences (e.g., weight
gain):
Between grade 8 and grade 9 it evolved into an eating disorder. And then I was like, ‘I’m
going to super restrict, and restrict’ and then I was like ‘Oh, I can binge and then
compensate’ and like I didn’t know how to do that before. I was like, ‘I can purge! Oh
my god, [this is] amazing!’
68
Altogether, some participants reported finding solace in purging as it allowed them to
momentarily break free from their dietary restriction without experiencing weight gain and the
psychological distress that comes with it. They reported knowing the negative consequences
associated with purging; however, they believed that the benefits of purging outweighed the
costs.
Overall, participants’ reports of engaging in maladaptive eating behaviours demonstrates
how engrained their beliefs about weight (i.e., being overweight is bad) were, and still are, and
how important it was, and continues to be, for them to keep their weight in check.
Developing a Long-Lasting Preoccupation with Weight
The fourth identified theme associated with childhood experiences of parental feeding
control was developing a long-lasting preoccupation with weight. Many participants reported
that they were still struggling with weight-related psychological concerns, as well as engaging in
maladaptive eating behaviours, due to their childhood experiences of parental feeding control
practices. When asked whether or not she had experienced any psychological impacts as a result
of parental feeding control practices, Sarah reported the following:
A lifetime of disordered eating that I’m still not [over]...I’ve tried to manifest that
recovery and affirm that recovery but it’s been fucking challenging. [I’ve experienced] a
lifetime of disordered relationships with my body and food.
May described the following impact of experiencing parental feeding control during her
childhood:
I never thought of myself as not being on a diet or not being restrictive.
69
Rebecca described still feeling the need to monitor her diet and exercise as a result of her
experience of parental feeding control practices and her parents’ emphasis on health and
thinness:
Even now, I have to think about what food I’m eating and whether or not I’m exercising
enough so I guess it's one of my top [concerns]...I guess like health and weight is
something that I'm still pretty concerned about.
Emma described the long-lasting effects of parental feeding control practices:
[It effected] the way I viewed myself and the way I viewed my relationships with others,
and how pervasive their [my parents] comments were...to the point where I still hear my
mother's voice being like, ‘your legs are fat.’ I really have to fight against that [the
thoughts] and be like, ‘No, stop.’ I need to stop that maladaptive thought basically. I feel
like it [experiencing parental feeding control] does affect you and whether you fight it or
not as an adult, it’s [the impact] still there.
Atoosa reported that experiencing parental feeding control practices has had a lasting impact on
her emotional and psychological well-being:
None of those bad feelings about myself or the low confidence due to that childhood
experience, none of them actually went away...I am sure that it’s not going to go away
completely; this problem is stuck with me...It won't go away emotionally, it still exists.
Physically, all the stretch marks remind me of the experiences [of parental feeding
control practices]. So this is a childhood experience that sticks with you, and you carry
[it] for your whole life. It [experiencing parental feeding control practices] scars.
According to participants, the consequences of parental feeding control practices are intense and
long-lasting. Participants indicated that they continue to struggle with the belief that their self-
70
worth is contingent on their weight and still grapple with the psychological consequences of
experiencing parental feeding control practices. Furthermore, participants stated that they
continue to engage in maladaptive eating behaviours in order to lessen their weight-related
psychological distress. Overall, experiencing parental feeding control practices was perceived
by the participants of this research study to cause lasting weight preoccupation.
Seeing Parental Feeding Control Practices as Unhelpful
The last identified core concept was seeing parental feeding control practices as
unhelpful, which included one theme: offering advice. Overall, as a result of living with the
consequences associated with experiences of parental feeding control practices, participants
reported coming to the conclusion that these feeding practices were unhelpful. Atoosa explained
that despite experiencing parental feeding control, her struggle with weight was not resolved:
It's not that it [parental feeding control] happened just once and I became thin. No, I
always dealt with this issue [struggling with weight] after.
Jackie explained how she views parental feeding control practices in the following quote:
I don’t think putting kids on a diet is helpful at all. I think a moderation approach is okay,
but I don’t think you should tell your kid, ‘you can’t have dessert and you can’t have
treats’ regardless of their weight because I don’t think that works.
Emma described that, despite having her dietary intake controlled and restricted, she did not
experience weight loss, which resulted in feelings of frustration:
I wouldn’t eat all these things and my weight would go nowhere. So it was frustrating to
the point that I was like, ‘screw this, I’m going to eat whatever.’
Offering advice. Given that participants disagreed with the use of parental feeding
control practices and believed that they were unhelpful, I asked them to provide advice for
71
parents who are currently raising children that may be struggling with their weight. In response,
Sarah said the following:
Just teach them really explicitly and from day one...reinforce that self-esteem...that
because you are here, you are worthy, [and your worth is] not contingent on anything.
Rebecca suggested that parents not make their children feel guilty about eating certain foods as
that can impact how they view themselves and their relationships:
I think it [my advice] would be not to guilt them [children] because I think that you don’t
often realize how guilty kids can feel and how negatively they can perceive something. I
think at that age, they [children] really want that parental acceptance and so that guilt
[associated with eating certain foods] can isolate them a little bit.
Sarah proposed that parents focus on the fostering a healthy lifestyle. She suggested not
restricting certain foods but instead, adding healthy foods. Furthermore, she recommended that
promoting a healthy lifestyle should become a family bonding activity:
I think it’s really kind of about getting excited about food prepping together, doing things
together to facilitate a healthier lifestyle. So instead of [saying,] ‘we’re not going to do
this [eat particular foods]’, focus on the positives. For example, [saying,] ‘we’re going to
go pick healthy groceries that you like to eat together.’ And you know you can prepare
food as a family. So [saying,] ‘let’s find some recipes’ or ‘let’s go to the market.’
Emma emphasized focusing on health instead of weight loss. She also described working
towards health as a family unit, instead of targeting or alienating a particular family member:
I would focus more on health because I feel like body or weight [change] follows from
health. If you are more health focused, you don’t end up cutting things you shouldn’t. If
you focus more on health and you think about, ‘this as a family, a system, how are we
72
functioning? Are we all eating badly and some of us are gaining more weight than
others?’ But I think working as a family and being like, ‘we’re all going to eat healthier
and try to be more active’ that kind of stuff. So putting a more positive spin on it rather
than [saying,] ‘you’re fat.’
In general, participants agreed that experiencing parental feeding control during their childhoods
was unhelpful and damaging. They believed that parents should focus on encouraging healthy
eating behaviours and family bonding, instead of restricting certain foods and emphasizing
weight loss.
Summary of the Constructivist Grounded Theory
The preliminary constructivist GT consists of five core categories: making meaning of
parental feeding control, experiencing psychological impacts, experiencing behavioural impacts,
developing a long-lasting preoccupation with weight, and viewing parental feeding control
practices as unhelpful. All participants described making meaning of their experience of parental
feeding control practices (i.e., developing the view that being overweight is bad) and
experiencing negative psychological impacts. It was further stated that the two previously
mentioned core concepts came together with experiencing parental feeding control practices to
result in experiencing behavioural impacts (i.e., engaging in maladaptive eating behaviours). All
of the research participants reported developing a long-lasting preoccupation with weight as a
result of their experience of parental feeding control practices and its related meaning-making,
psychological, and behavioural impacts. In total, due to experiencing the negative consequences
of parental feeding control practices, participants viewed these feeding methods as unhelpful and
damaging. Altogether, the categories, themes, and sub-themes of this preliminary and

73
interpretive constructivist GT offer a comprehensive narrative of the meaning making and
psychological impacts of experiencing parental feeding control practices during one’s childhood.

74
CHAPTER FIVE
Discussion
The objective of the current study was to develop a preliminary constructivist grounded
theory (GT) that explains the meaning making and psychological processes associated with
childhood experiences of parental feeding control practices. The constructivist version of GT
methods provided the tools necessary to collect accounts of childhood experiences of parental
feeding control. The preliminary constructivist GT offers insight into how individuals make
meaning of their experience of parental feeding control practices, as well as provides an
understanding of the psychological and behavioural impacts of these feeding methods.
The preliminary constructivist GT details important dynamics between the core concepts
associated with experiencing parental feeding control practices during one’s childhood. To
begin, individuals face meaning making and psychological impacts as a result of experiencing
parental feeding control practices. Furthermore, undergoing parental feeding control practices
during one’s childhood, as well as experiencing the meaning making and psychological impacts
of these practices, combine to support the use of maladaptive eating behaviours. Lastly, the
meaning making, psychological, and behavioural impacts have a lasting effect on individuals’
overall psychological well-being and eating behaviours in the form of persistent weight
preoccupation.
The following chapter attends to the contributions and limitations of the current research
study. In line with constructivist GT methods, a secondary literature review was conducted.
According to constructivist GT methods, a preliminary literature review can be utilized by
novice researchers to clarify research aims, contextualize the research study, and help the
researcher become aware of sensitising concepts (Charmaz, 2006; Heath & Cowley, 2004;
75
Wilson & Barn, 2012). The secondary literature review, based on constructivist GT methods,
allows the researcher to compare and contrast findings with past research studies (Charmaz,
2006). Thus, given the results of the current study, the second literature review, focused on
relevant feeding, weight stigma/bias, and childhood obesity literature, is described. Furthermore,
contributions to the literature and counselling psychology implications of the current study are
also discussed. Finally, the strengths and limitations of this study are addressed, as well as future
directions for research.
Contributions to the Literature
Given the potential negative health and psychosocial consequences associated with
childhood obesity (e.g., type II diabetes, social stigmatization and marginalization, as well as
depression), it is no wonder parents may want to utilize feeding control practices (i.e., dietary
restriction and monitoring, as well as pressuring a child to eat certain foods such as fruits and
vegetables) in order to manage their children’s weight (i.e., promote weight loss or prevent
weight gain). Despite parents’ best intentions, however, researchers have found that parental
feeding control practices can have counterproductive weight-related and eating effects (Birch &
Fisher, 1995; Birch, et al., 2003; Campbell et al., 2006; Carper et al., 2000; Fisher & Birch,
2002; Gable & Lutz, 2000; Johnson & Birch, 1994; Thompson, 2010; Vos & Welsh, 2010).
Furthermore, results of the current study indicate that experiencing parental feeding control
practices during one’s childhood can also contribute to negative and lasting meaning making,
psychological, and behavioural outcomes.
While the results of this study resonate with existing ideas in the literature, they also
provide new insights on how these ideas interact with one another. Altogether, it is my hope that
this study’s preliminary theoretical model will incite discussion about, as well as prompt future

76
research on, the impacts of parental feeding control practices on children’s overall well-being.
The following sections aim to incorporate the findings of this study with the current literature,
while also offering a new way of conceptualizing the impacts of experiencing parental feeding
control practices during one’s childhood.
Contributions to the Feeding Literature
As was noted in chapter two, most of the literature on parental feeding control practices
focuses on the behavioural impacts of employing these feeding methods on children. For
example, parental feeding control practices have been found to be negatively associated with
children’s ability to self-regulate food consumption, positively associated with weight status, as
well as linked to the development of a preference for restricted foods (Birch & Fisher, 1995;
Birch, et al., 2003; Campbell et al., 2006; Carper et al., 2000; Fisher & Birch, 2002; Gable &
Lutz, 2000; Johnson & Birch, 1994; Thompson, 2010; Vos & Welsh, 2010). As the feeding
literature has mostly focused on the behavioural impacts of parental feeding control practices,
children’s subjective experiences of these feeding methods have remained largely ignored.
Moreover, the long-term impacts of parental feeding control practices have not been explored.
For these reasons, the present study aimed to investigate the short- and long-term meaning
making and psychological impacts of experiencing parental feeding control practices during
one’s childhood.
Findings from this study indicate that experiencing parental feeding control practices
during one’s childhood can have a lasting effect on how individuals view themselves and the
world (i.e., adopting the belief that being overweight is bad), as well as impacts their
psychological well-being and eating behaviours. Given the scarcity of research on the meaning
making and psychological impacts of parental feeding control practices, it is necessary to go
77
beyond the feeding literature in order to find an explanation for these results. As such, I have
related findings to the weight stigma and weight bias literature. This literature provides a
framework for comprehending the meaning making, psychological, and behavioural impacts of
experiencing parental feeding control practices during one’s childhood.
Contributions to the Weight Stigma and Weight Bias Literature
Results of this study indicate that individuals who experience parental feeding control
practices during their childhoods engage in a meaning making process which involves: (a)
perceiving parents’ motivation for utilizing feeding control practices, (b) internalizing parental
messages about weight, and (c) viewing self-worth as contingent on weight. During the
interview process, participants’ described receiving and internalizing negative parental messages
about weight through experiencing parental feeding control practices. These parental messages
about weight included that being overweight (a) is unattractive and will negatively impacts
future success, (b) leads to being stigmatized and bullied, as well as (c) is unhealthy. Overall,
through the use of parental feeding control practices, parents reinforce the message that being
overweight is bad. Additionally, the meaning making process was found to be related to lasting
psychological and behavioural impacts. These findings fit within, and add to, the weight stigma
and weight bias literature.
Weight stigma literature. Weight-related stigmatization has been researched largely in
adult populations; in fact, it has been found that adults who are classified as overweight or obese
encounter social disadvantages and stigmatization in various life arenas (e.g., employment,
healthcare, education, and interpersonal relationships) due to their weight status (Brownell, 2005;
Puhl & Brownell, 2001; Russell-Mayhew et al., 2015; Russell-Mayhew et al., 2016). In addition
to the weight stigma literature with adult populations, there is an increasing amount of research

78
showing that children who are categorized as overweight and obese are targets of weight-related
societal stigmatization and marginalization. Researchers have demonstrated that children who
are classified as overweight and/or obese experience weight-related bias and stereotyping by
peers (Brylinsky & Moore, 1994; Kraig & Keel, 2001; Latner & Stunkard, 2003; Neumark-
Sztainer et al., 2002; Neumark-Sztainer, Story, & Faibisch, 1998), teachers (Bauer et al., 2004;
Neumark-Sztainer et al., 1999), and even parents (Adams, Hicken, & Salehi, 1988; Crandall,
1991, 1995; Davison & Birch, 2004).
Despite the limited amount of research on parental weight-related bias, consistent and
disheartening results have emerged (Adams et al., 1988; Crandall, 1991, 1995; Davison & Birch,
2004). To illustrate these findings, I highlight research conducted by Davison and Birch (2004)
in which they investigated weight-related stereotyping among 9-year-old girls and their parents.
They found that parents, and their daughters, attributed significantly more negative
characteristics (e.g., laziness) to individuals who are deemed obese than to thinner individuals.
Additionally, daughters were more likely to endorse negative weight-related stereotypes if their
parents stressed the importance of being thin, as well as emphasized weight loss. Lastly, parents
who were overweight or obese were just as likely to support negative weight-related stereotypes
as thinner parents.
The current study adds to the weight stigma literature by providing evidence that parents
may be expressing weight stigma towards their children through the use of parental feeding
control practices. The current study’s findings endeavour to explain Davison and Birch’s (2004)
results by providing a theory about how negative weight-related stereotypes are transmitted to
children by their parents. Based on this study’s constructivist GT model, children recognize and
adopt negative weight-related stereotypes through perceiving their parents’ motivation for

79
utilizing parental feeding control practices. For example, if parents endorse appearance
motivations for utilizing feeding control practices, they are transmitting the message that
overweight individuals are less attractive than thinner individuals. Through perceiving their
parents’ appearance motivation for using feeding control practices, as well as through receiving
implicit and explicit parental messages about weight, children begin to adopt their parents’
negative weight-related beliefs.
Internalized weight bias literature. The results of the current study suggest that
experiencing parental feeding control practices, as well as receiving negative parental messages
about weight, can lead to the internalization of negative parental weight-related messages (i.e.,
internalized weight bias). Internalized weight bias, defined as having a negative view of oneself
due to weight or size, has been found to develop as a result of experiencing weight stigmatization
and/or marginalization (Latner, Barile, Durso, & O'Brien, 2014). In contrast to other stigmatized
groups (e.g., Jewish and Asian individuals) who do not tend to endorse internalized bias,
researchers have observed internalized weight stigma among individuals who are classified as
obese (Rudman, Feinburg, & Fairchild, 2002; Wang, Brownell, & Wadden, 2004). That is,
despite inclusion in the stigmatized group, researchers have found that individuals who are
categorized as overweight and obese endorse implicit anti-fat attitudes, and some even report an
explicit anti-fat bias (e.g., using unflattering adjectives when describing obese individuals;
Rudman et al., 2002; Wang et al., 2004).
The current study’s findings fit within the internalized weight bias literature. In line with
this study’s preliminary theoretical model, individuals were found to develop internalized weight
bias as a result of experiencing parental feeding control practices and receiving stigmatizing
parental messages about weight. Moreover, despite being part of the stigmatized group (i.e.,

80
individuals who perceive themselves as overweight), participants reported endorsing anti-fat
attitudes (e.g., being overweight makes you less worthy of other people’s love and attention),
which is believed to have impacted their overall psychological well-being and eating behaviours.
Consequences of weight stigma and internalized weight bias. Experiencing weight
stigma and internalized weight bias have been found to be associated with a variety of negative
outcomes. The following sections outline those outcomes in greater detail and relate them back
to the current study’s findings.
Consequences of weight stigma. As was previously mentioned in chapter two,
researchers have found that children who are categorized as overweight or obese may be more
likely to develop depression and suicidal ideation, as well as experience decreased body
satisfaction and lower self-esteem as a result of experiencing weight-related stigmatization and
marginalization (Eisenberg et al., 2003, Hayden-Wade et al., 2005; Puhl & Latner, 2007; Storch
et al., 2007). These findings align with the current study’s results. A number of participants
viewed their childhood experience of parental feeding control as stigmatizing, and they reported
experiencing decreased body satisfaction (i.e., becoming more self-conscious about their weight
and size) as well as lowered self-esteem due to their weight and size (i.e., viewing self-worth as
contingent on weight). However, depression and suicidal ideation were not reported by
participants in this study.
Consequences of internalized weight bias. In samples of individuals who are classified as
overweight and/or obese, internalized weight bias is consistently found to be related to adverse
psychological and behavioural consequences. Various researchers have found a negative
correlation between internalized weight bias and psychological well-being; depression, anxiety,
stress, and lowered self-esteem have all been found to be associated with experiencing
81
internalized weight bias (Carels et al., 2013; Carels et al., 2010; Durso & Latner, 2008; Schvey,
Roberto, & White, 2013; Schvey & White, 2015). Furthermore, internalized weight bias has
been shown to be linked to maladaptive eating and body image-related variables, which include
disordered eating (e.g., bingeing and purging, as well as dietary restraint), body dissatisfaction,
and weight and shape concerns (Carels et al., 2013; Carels et al., 2010; Durso & Latner, 2008;
Pearl, White, & Grilo, 2014; Schvey et al., 2013).
These findings also correspond to the results of the current study. Participants reported
internalizing negative parental messages about weight and size (i.e., internalized weight bias),
and described experiencing weight-related anxiety and stress (i.e., fearing weight gain), as well
as lowered self-esteem in relation to their beliefs about weight-contingent self-worth.
Additionally, participants endorsed engaging in self-imposed dietary restriction, and described
engaging in bingeing and purging. Participants also reported experiencing body dissatisfaction,
as well as overall and lasting weight and shape concerns (i.e., feeling self-conscious about
weight and size, fearing weight gain, viewing self-worth as contingent on weight, and developing
lasting weight preoccupation). These findings suggest that experiencing parental feeding control
practices during one’s childhood can lead to internalized weight bias, and that internalized
weight bias can significantly impact one’s psychological well-being and eating behaviours.
Intergenerational internalized weight bias. Past research conducted by Musher-
Eizenman and colleagues (2007) has demonstrated that parents are more likely to utilize parental
feeding control practices if they endorse anti-fat attitudes. Moreover, findings from the current
study indicate that parents transmit anti-fat attitudes to their children through parental feeding
control practices which results in the internalization of negative parental messages about weight
(i.e., internalized weight bias). In combination, these findings suggest that anti-fat attitudes and

82
internalized weight bias may be passed down intergenerationally through the use of parental
feeding control practices. This intergenerational passing down of stigmatizing weight-related
attitudes creates a damaging cycle in which parents perpetuate anti-fat messages through
utilizing parental feeding control practices, which then leads to internalized weight bias for the
child. This cycle of body hatred is likely to repeat itself if the internalized weight bias, incurred
by the child through experiencing parental feeding control practices, is not addressed (Russell-
Mayhew, in press).
In sum, the weight stigma/bias literature offers insight into why individuals who
experience parental feeding control practices also report psychological and eating disturbances.
Altogether, the current study’s preliminary conceptualization of the meaning making and
psychological impacts of parental feeding control practices provides an explanation of the
mechanism through which individuals internalize anti-fat attitudes, as well as offers a narrative
for its associated psychological and behavioural impacts.
Contributions to the Childhood Obesity Treatment Literature
Overall, the results of the current study indicate that parental feeding control practices are
unhelpful in the treatment of childhood overweight and/or obesity. Furthermore, findings
indicate that utilizing parental feeding control practices in order to remedy childhood overweight
and/or obesity can have a lasting negative impact on children’s overall well-being. These results
fit within the childhood obesity treatment literature. Generally, the literature does not endorse
utilizing parental feeding control practices in order to address childhood overweight or obesity as
these practices have been associated with counterproductive outcomes (e.g., weight gain,
disinhibited eating, and eating in the absence of hunger; Birch & Fisher, 1995; Birch, et al.,
2003; Campbell et al., 2006; Carper et al., 2000; Fisher & Birch, 2002; Gable & Lutz, 2000;

83
Johnson & Birch, 1994; Thompson, 2010; Vos & Welsh, 2010). Additionally, the results of the
current study provide further evidence against the use of parental feeding control practices to
treat childhood overweight and obesity (e.g., negative meaning making, psychological, and
behavioural impacts).
Due to their beliefs about the unhelpful and damaging effects of parental feeding control
practices, participants provided advice for parents of children who may be dealing with weight-
related struggles. Participants’ suggestions included: parental encouragement of healthy eating
behaviours, turning the weight struggle into an opportunity for family bonding (e.g., cooking
healthy meals together), as well as refraining from restricting particular foods and emphasizing
weight loss. These participant recommendations are consistent with the childhood obesity
treatment literature. Current guidelines for childhood obesity treatment recommend
multidisciplinary interventions that highlight change in diet, activity, and behaviour (Barlow,
2007). More specifically, parental/familial involvement is highly recommended, with family-
based behavioural weight loss treatment being the most widely supported method in the literature
for addressing childhood obesity (Altman & Wilfley, 2015; American Dietetic Association,
2006; Ball et al., 2012; Ho et al., 2012; Holt et al., 2008; Snethen, Broome, & Cashin, 2006;
Young, Northern, Lister, Drummond, & O’Brien, 2007).
Family-based behavioural weight loss treatment (FBT) is an evidence-based intervention
which treats the whole family system through comprehensive methods intended to diminish
energy intake, increase physical activity, modify family behavioural patterns, and adjust the
home environment (Holland et al., 2014). FBT endeavours to alter the family environment by
encouraging parents to remove energy-dense foods from the home and make nutrient-dense
foods readily available to all family members (Holland et al., 2014). These alterations to the

84
family home provide an environment that encourages children to make healthy choices, and
removes the need for excessive parental dietary restriction (Holland et al., 2014). As such,
children feel less deprived within their familial environment (Holland et al., 2014). Furthermore,
parents are encouraged to model healthy behaviours (e.g., healthy eating and exercise), and are
taught to create a supportive familial environment in which the child does not feel isolated or
targeted due to their weight struggles (Holland et al., 2014).
Overall, research has demonstrated that FBT is related to a reduction in the use of
parental feeding control practices, which is also related to a reduction in child weight status
(Epstein, Paluch, Beecher, & Roemmich, 2008; Holland et al., 2014). Furthermore, FBT was
found to be more effective than child-only treatments (Brownell, Kelman, & Stunkard, 1983;
Epstein, Valoski, Wing, & McCurley, 1990), as well as control conditions (Epstein et al., 1990;
Graves, Meyers, & Clark, 1988; Israel, Stolmaker, & Andrian, 1985; Kirschenbaum, Harris, &
Tomarken, 1984; Sacher et al., 2010; Savoye et al., 2007) in addressing childhood overweight
and obesity. Generally, FBT methods are line with participants’ previously mentioned
recommendations for dealing with childhood weight concerns, and research supports the use of
these methods as a means for remedying childhood obesity. Although FBT has been associated
with positive weight-related outcomes, the psychological impacts of these weight loss methods
have not been explored. As such, further research is needed to ensure that FBT does not result in
unintended negative consequences.
Implications for Counselling Psychology
The deeper understanding of the impacts of parental feeding control practices, gained as a
result of the current constructivist GT study, offers prevention and treatment implications for
counselling psychologists.
85
Prevention and Treatment Implications
Given the current study’s findings on the potential negative meaning making,
psychological, and behavioural outcomes of parental feeding control practices, as well as the
previously established findings on the counterproductive weight-related and eating impacts of
these feeding tactics, it is important for counselling psychologists to fervently advise against the
use of parental feeding control practices for child weight management. For example, if a parent
presents to counselling with concerns about their child’s weight, it would be imperative to
educate the parent on feeding control practices and their potential negative impacts (i.e.,
explaining how parental dietary restriction, monitoring, or pressure can lead to lasting
maladaptive meaning making, psychological, behavioural outcomes in children), as well as
strongly advise against the use of feeding control practices for addressing their child’s weight. In
fact, Russell-Mayhew (in press) suggests that counselling psychologists should refrain from
discussing weight loss efforts with their clients. She proposes that helping clients in their weight
loss endeavours, or their efforts to promote weight loss in their children, can be described as a
micro-aggression as it perpetuates dominant oppressive discourses about weight, which can be
damaging to all involved parties (Russell-Mayhew, in press). Counselling psychologists can
prevent the potential damage that a child could incur as a result of experiencing parental feeding
control practices by enthusiastically advising against the use of these feeding methods, helping
parents work through their thoughts and emotions related to having a child who is struggling
with their weight, and employing a family-based approach towards health and wellness.
If the parent is still adamant about addressing their child’s weight, it may be best to refer
them to another professional, who has an awareness of the negative impacts of parental feeding
control practices, in order to provide them with the necessary guidance in their endeavour. For
86
example, as it has been found to be the most effective treatment in the childhood obesity
literature, it would be advisable for the counselling psychologist to suggest that the parent, child,
and the family as a whole, seek FBT in order to address the child’s weight concerns through
means that do not involve parental feeding control.
Strengths and Limitations
The current study had many strengths and limitations. To begin, given the scarcity of
research on the meaning making and psychological impacts of experiencing parental feeding
control practices during one’s childhood, the first strength of the current study was filling these
gaps in the literature. Through demonstrating that parental feeding control practices contribute
to negative and lasting meaning making, psychological, as well as behavioural outcomes, the
current study added to the feeding, weight stigma/bias, and childhood obesity treatment
literature. Furthermore, prominent weight bias researchers, Puhl and Latner (2007), outlined a
need for future research studies to determine the ways in which parents communicate
stigmatizing weight-related messages to their children, as well as investigate the impacts of these
messages on children’s well-being. The current research study fulfilled this need, and
contributed to the weight stigma and weight bias literature, by indicating that experiencing the
stigmatizing effects of parental feeding control practices during one’s childhood can lead to
internalized weight bias.
Moreover, Charmaz (2008) argues that a researcher’s active involvement in the process
of data collection and analysis, rather than passively analyzing previously collected and
transcribed data, provides a significant strength or advantage in the process of developing a
constructivist GT. As such, by collecting, transcribing, as well as coding participant interviews
myself, I was able to maintain closeness with the data, and recognize themes and patterns that I

87
may have overlooked if I had not been so involved with data collection and analysis (Charmaz,
2014).
In addition to the strengths, there were several limitations associated with this research
study. Firstly, although Charmaz (2006) argues that semi-structured interviews offer
inexperienced researchers with a format for organized data collection, it is possible that this
interviewing method could have limited the range of collected information (Tweed & Charmaz,
2012). Therefore, future studies should consider adopting a more open interviewing style in
order to collect a broader array of information from participants. Moreover, limiting data
collection to one interview per participant could have resulted in less complete information about
participants’ experience of parental feeding control practices. It is possible that participants
could have felt more comfortable sharing their experiences of the impacts of parental feeding
control, or could have had more time to reflect upon their experiences, if a second or third
interview had been administered.
Secondly, Charmaz (2014) explains that researcher subjectivity and the influence of
previously established research and theories are inevitable in qualitative research. As such,
despite my efforts to remain open to the data, as well as my intent to develop a preliminary
theory that was grounded in participants’ descriptions of the impacts of parental feeding control
practices, it is possible that personal biases and expectations influenced my research findings.
However, memo writing, discussions with my thesis advisor and student mentor, as well as
reflexive interviewing (i.e., asking participants clarifying questions in order to ensure that I am
accurately understanding their experience of parental feeding control instead of imposing my
research agenda onto the data) aided in enhancing the credibility of this study’s research
findings.
88
Thirdly, even though data collection terminated when it was deemed that no new themes
where emerging from the data, it is possible that further interviews could have resulted in the
emergence of additional themes. Therefore, true saturation may not have been achieved.
Hutchinson and Wilson (2001) argue that the premature termination of research can result in an
incomplete theory; thus, I recognize that the results of this study provide a preliminary
theoretical model of the meaning making and psychological impacts of experiencing parental
feeding control practices during one’s childhood.
Lastly, due to the low number of participants, as well as an entirely female sample, it is
difficult to assert whether or not the findings of the current study are applicable to all children
who have experienced parental feeding control practices during their childhoods. With this
being said, the current study’s preliminary constructivist GT was assessed based on its ability to
answer Charmaz’ (2014) evaluation questions regarding the GT’s credibility, originality,
resonance, and usefulness. Altogether, through answering these questions, the current study’s
constructivist GT was deemed to have met Charmaz’ (2014) substantive criteria and, therefore, is
viewed as valuable. Altogether, future research should endeavour to address the previously
mentioned limitations in order to develop a model that has increased theoretical applicability.
Potential future research directions are outlined below.
Future Research
There are numerous directions for future research based on the current study’s findings
and limitations. To begin, although the current study’s participants ranged in ethnicities and
educational backgrounds, the low number of participants, as well as the wholly female sample,
was a limitation of the current study. As such, it would be important to conduct a similar study,
on a grander scale (i.e., with more research participants of all genders), to discern whether or not
89
the findings of the current study apply to all genders. Alternatively, it could also be interesting
to investigate gender differences in childhood experiences of parental feeding control practices.
Another direction for future research could include a quantitative analysis of the meaning
making, psychological, and behavioural impacts of parental feeding control practices. It would
be interesting to discern whether or not the findings of this study could be replicated through
quantitative means. For example, future research could explore the internalization of weight bias
in individuals who have experienced parental feeding control during their childhoods by utilizing
internalized weight bias measures.
Moreover, future research could endeavour to evaluate the temporal aspect of the current
study’s findings. For instance, does the meaning making process occur before the psychological
and behavioural impacts appear? In line with this idea, it would be interesting to research this
phenomenon longitudinally to establish the order of events associated with childhood
experiences of parental feeding control practices.
Finally, it would be important that future research studies attempt to identify ways to
reduce weight stigma among parents of children who are classified as overweight or obese (e.g.,
evaluating the effectiveness of empathy inducing methods related to childhood overweight and
obesity; Puhl & Latner, 2007). As was previously discussed, results from a study conducted by
Musher-Eizenman and colleagues (2007) indicate that the more parents endorse anti-fat attitudes,
the more likely they are to employ parental feeding control practices to manage their children’s
weight. As such, if weight stigma among parents is reduced, the likelihood of using parental
feeding control practices, as well as the likelihood that children will experience the negative
meaning making and psychological impacts associated with these feeding methods, also
diminishes.
90
Conclusion
The aim of the current research study was to understand the meaning making and
psychological impacts of experiencing parental feeding control practices, aimed at promoting
weight loss or preventing weight gain, during one’s childhood. This aim was achieved by
conducting a constructivist GT study in which transcribed semi-structured interviews, with
individuals who experienced parental feeding control during their childhoods, were analyzed.
This study’s preliminary constructivist GT represents the interconnection between the identified
core concepts associated with childhood experiences of parental feeding control. Specifically,
the theory proposes a meaning making process, consisting of perceiving parental motivation for
using parental feeding control practices, internalizing parental messages about weight, and
viewing self-worth as contingent on weight. The preliminary constructivist GT suggests that
individuals experience a process of meaning making which leads to the internalization of the
belief that being overweight is bad. Furthermore, the theory outlines a psychological process
which involves becoming self-conscious about their weight and size, feeling guilt about eating,
and fearing weight gain. Next, it is theorized that undergoing parental feeding control practices
during one’s childhood, as well as experiencing the meaning making and psychological impacts
of these practices, come together to encourage the use of maladaptive eating behaviours.
Furthermore, the meaning making, psychological, and behavioural impacts are theorized to have
a lasting impact on participants’ psychological well-being, which takes the form of persistent
weight preoccupation. Overall, parental feeding control practices were seen as unhelpful and
damaging. Altogether, this preliminary constructivist GT fits within, and adds to, the existing
literature. Notably, the theory draws a link between the feeding literature and the weight
stigma/weight bias literature by creating a new understanding of how individuals come to

91
internalize weight bias, as well as how individuals are impacted by the internalization of anti-fat
attitudes. Moreover, this preliminary constructivist GT offers further evidence against the use of
parental feeding control practice to promote weight loss or prevent weight gain in child
populations.
To conclude, in today’s society, parents feel an incredible amount of pressure, from a
variety of sources (e.g., media, physicians, other parents, etc.), to manage their children’s weight
(i.e., ensure that their children fall within the “medically-acceptable” and “socially desirable”
weight range; Ristovski-Slijepcevic, Chapman, & Beagan, 2010). Furthermore, as it is common
practice for adults to address their personal weight concerns through self-imposed dietary
control, it is not surprising that parents may choose to address their children’s weight struggles
by exerting control over their eating (i.e., utilizing parental feeding control practices). Given the
small amount of research on the impacts of parental feeding control practices, as well as the
resulting lack of parental knowledge on the negative consequences of these feeding methods, I
do not blame parents for choosing to address their children’s weight concerns through parental
feeding control practices. In fact, it is my belief that these feeding methods are most often
implemented by parents who have the best of intentions (i.e., they want to protect their children
from experiencing the negative consequences associated with childhood overweight and
obesity); however, despite these good intentions, parental feeding control practices have been
found to be associated with unintended negative psychological, meaning making, and
behavioural consequences. Therefore, I believe it is imperative that parents become aware of the
potential negative outcomes of parental feeding control practices so that they can make informed
decisions related to addressing their children’s weight concerns. Overall, it is my hope that
parents become informed of the unintended negative meaning making and psychological impacts

92
of parental feeding control practices through the dissemination of the current study’s research
findings, and that fewer children experience the lasting eating- and weight-related struggles
associated with experiencing these controlling feeding methods.
93
References
Adams, G. R., Hicken, M., & Salehi, M. (1988). Socialization of the physical attractiveness
stereotype: Parental expectations and verbal behaviors. International Journal of
Psychology, 23, 137-149. doi:10.1080/00207598808247757
Altman, M., & Wilfley, D. E. (2015). Evidence update on the treatment of overweight and
obesity in children and adolescents. Journal of Clinical Child & Adolescent Psychology,
44, 521-537. doi:10.1080/15374416.2014.963854
American Dietetic Association. (2006). Position of the American Dietetic Association:
Individual-, family-, school-, and community-based interventions for pediatric
overweight. Journal of the American Dietetic Association, 106, 925-945.
doi:10.1016/j.jada.2006.03.001
Andrews, T. (2012). What is social constructionism? The Grounded Theory Review, 11, 39-46.
Retrieved from http://groundedtheoryreview.com/2012/06/01/what-is-social-
constructionism/
Anzman, S. L., & Birch, L. L. (2009). Low inhibitory control and restrictive feeding practices
predict weight outcomes. The Journal of Pediatrics, 155, 651-656.
doi:10.1016/j.jpeds.2009.04.052
Ball, G. D., Garcia, A. P., Chanoine, J. P., Morrison, K. M., Legault, L., Sharma, A. M., ... &
Holt, N. L. (2012). Should I stay or should I go? Understanding families’ decisions
regarding initiating, continuing, and terminating health services for managing pediatric
obesity: The protocol for a multi-center, qualitative study. BMC Health Services
Research, 12, 486-486. doi:10.1186/1472-6963-12-486

94
Bauer, K. W., Yang, Y. W., & Austin, S. B. (2004). “How can we stay healthy when you’re
throwing all of this in front of us?” Findings from focus groups and interviews in middle
schools on environmental influences on nutrition and physical activity. Health Education
& Behavior, 31, 34-46. doi:10.1177/1090198103255372
Baumrind, D. (1991). The influence of parenting style on adolescent competence and substance
use. The Journal of Early Adolescence, 11, 56-95. doi:10.1177/0272431691111004
Bayer, J. K., Ukoumunne, O. C., Lucas, N., Wake, M., Scalzo, K., & Nicholson, J. M. (2011).
Risk factors for childhood mental health symptoms: National longitudinal study of
Australian children. Pediatrics, 128, e865-e879. doi:10.1542/peds.2011-0491
Bell, L. M., Curran, J. A., Byrne, S., Roby, H., Suriano, K., Jones, T. W., & Davis, E. A. (2011).
High incidence of obesity co-morbidities in young children: A cross-sectional study.
Journal of Paediatrics and Child Health, 47, 911-917. doi:10.1111/j.1440-
1754.2011.02102.x
Birch, L. L. (2006). Child feeding practices and the etiology of obesity. Obesity, 14, 343-344.
doi:10.1038/oby.2006.45
Birch, L. L., & Davison, K. K. (2001). Family environmental factors influencing the developing
behavioral controls of food intake and childhood overweight. Pediatric Clinics of North
America, 48, 893-907. doi:10.1016/S0031-3955(05)70347-3
Birch, L. L., & Fisher, J. A. (1995). Appetite and eating behavior in children. Pediatric Clinics of
North America, 42, 931-953. doi:10.1016/S0031-3955(16)40023-4
Birch, L. L., & Fisher, J. O. (1998). Development of eating behaviors among children and
adolescents. Pediatrics, 101, 539-549. Retrieved from
http://www.adinapearson.com/kvpaHB2WmRY5/wp-
95
content/uploads/2014/09/Development-of-eatign-behaviors-among-children-and-
adolescents.pdf
Birch, L. L., & Fisher, J. O. (2000). Mothers' child-feeding practices influence daughters' eating
and weight. The American Journal of Clinical Nutrition, 71, 1054-1061. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2530928/
Birch, L. L., Fisher, J. O., & Davison, K. K. (2003). Learning to overeat: Maternal use of
restrictive feeding practices promotes girls’ eating in the absence of hunger. The
American Journal of Clinical Nutrition, 78, 215-220. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2530927/
Birch, L. L., Fisher, J. O., Grimm-Thomas, K., Markey, C. N., Sawyer, R., & Johnson, S. L.
(2001). Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of
parental attitudes, beliefs and practices about child feeding and obesity proneness.
Appetite, 36, 201-210. doi:10.1006/appe.2001.0398
Birch, L. L., McPhee, L., Shoba, B. C., Pirok, E., & Steinberg, L. (1987). What kind of exposure
reduces children's food neophobia?: Looking vs. tasting. Appetite, 9, 171-178.
doi:10.1016/S0195-6663(87)80011-9
Birch, L. L., McPheee, L., Shoba, B. C., Steinberg, L., & Krehbiel, R. (1987). “Clean up your
plate”: Effects of child feeding practices on the conditioning of meal size. Learning and
Motivation, 18, 301-317. doi:10.1016/0023-9690(87)90017-8
Birch, L. L., & Ventura, A. K. (2009). Preventing childhood obesity: What works? International
Journal of Obesity, 33, S74-S81. doi:10.1038/ijo.2009.22
96
Boeije, H. (2002). A purposeful approach to the constant comparative method in the analysis of
qualitative interviews. Quality and Quantity, 36, 391-409.
doi:10.1023/A:1020909529486
Bornstein, M. H., & Zlotnik, D. (2009). Parenting styles and their effects. In J. Benson & M.
Haith (Eds.), Social and emotional development in infancy and early childhood (pp. 496-
509). Oxford, UK: Academic Press.
Brown, R., & Ogden, J. (2004). Children’s eating attitudes and behaviour: A study of the
modelling and control theories of parental influence. Health Education Research, 19,
261-271. doi:10.1093/her/cyg040
Brownell, K. D., Kelman, J. H., & Stunkard, A. J. (1983). Treatment of obese children with and
without their mothers: Changes in weight and blood pressure. Pediatrics, 71, 515-523.
Retrieved from http://pediatrics.aappublications.org.ezproxy.lib.ucalgary.ca/content/
pediatrics/71/4/515.full.pdf
Brownell, K. D. (2005). Weight bias: Nature, consequences and remedies. New York, NY:
Guilford Press.
Brylinsky, J. A., & Moore, J. C. (1994). The identification of body build stereotypes in young
children. Journal of Research in Personality, 28, 170-181. doi:10.1006/jrpe.1994.1014
Burke, V. (2006). Obesity in childhood and cardiovascular risk. Clinical and Experimental
Pharmacology and Physiology, 33, 831-837. doi:10.1111/j.1440-1681.2006.04449.x
Campbell, K. J., Crawford, D. A., & Ball, K. (2006). Family food environment and dietary
behaviors likely to promote fatness in 5–6 year-old children. International Journal of
Obesity, 30, 1272-1280. doi:10.1038/sj.ijo.0803266
97
Carels, R. A., Burmeister, J., Oehlhof, M. W., Hinman, N., LeRoy, M., Bannon, E., ... &
Ashrafloun, L. (2013). Internalized weight bias: Ratings of the self, normal weight, and
obese individuals and psychological maladjustment. Journal of Behavioral Medicine, 36,
86-94. doi:10.1007/s10865-012-9402-8
Carels, R. A., Wott, C. B., Young, K. M., Gumble, A., Koball, A., & Oehlhof, M. W. (2010).
Implicit, explicit, and internalized weight bias and psychosocial maladjustment among
treatment-seeking adults. Eating Behaviors, 11, 180-185.
doi:10.1016/j.eatbeh.2010.03.002
Carnell, S., Cooke, L., Cheng, R., Robbins, A., & Wardle, J. (2011). Parental feeding behaviours
and motivations. A qualitative study in mothers of UK pre-schoolers. Appetite, 57, 665-
673. doi:10.1016/j.appet.2011.08.009
Carper, J. L., Fisher, J. O., & Birch, L. L. (2000). Young girls' emerging dietary restraint and
disinhibition are related to parental control in child feeding. Appetite, 35, 121-129.
doi:10.1006/appe.2000.0343
Charmaz, K. (2006). Constructing grounded theory: A practical guide through qualitative
analysis. Thousand Oaks, CA: Sage.
Charmaz, K. (2008). Grounded theory. In J. A. Smith (Ed.), Qualitative psychology: A practical
guide to research methods, (pp. 81-110). Thousand Oaks, CA: Sage.
Charmaz, K. (2014). Constructing grounded theory (2nd
ed.). Thousand Oaks, CA: Sage.
Cooke, L. J., Chambers, L. C., Añez, E. V., & Wardle, J. (2011). Facilitating or undermining?
The effect of reward on food acceptance. A narrative review. Appetite, 57, 493-497.
doi:10.1016/j.appet.2011.06.016
98
Corbin, J., & Strauss, A. (2008). Criteria for evaluation. In J. Corbin, & A. Strauss (Eds.), Basics
of qualitative research (3rd
ed., pp. 297-312). Thousand Oaks, CA: Sage.
Costanzo, P. R., & Woody, E. Z. (1985). Domain-specific parenting styles and their impact on
the child's development of particular deviance: The example of obesity proneness.
Journal of Social and Clinical Psychology, 3, 425-445. doi:10.1521/jscp.1985.3.4.425
Crandall, C. S. (1995). Do parents discriminate against their heavyweight daughters? Personality
and Social Psychology Bulletin, 21, 724-724. doi:10.1177/0146167295217007
Crawford, P. B., Story, M., Wang, M. C., Ritchie, L. D., & Sabry, Z. I. (2001). Ethnic issues in
the epidemiology of childhood obesity. Pediatric Clinics of North America, 48, 855-878.
doi:10.1016/S0031-3955(05)70345-X
Creswell, J. W. (2007). Qualitative inquiry and research design: Choosing among five
approaches (2nd
ed.). Thousand Oaks, CA: Sage.
Cutting, T. M., Fisher, J. O., Grimm-Thomas, K., & Birch, L. L. (1999). Like mother, like
daughter: Familial patterns of overweight are mediated by mothers' dietary disinhibition.
Journal of the American Academy of Child & Adolescent Psychiatry, 38, 1323-1323.
doi:10.1097/00004583-199910000-00028
Daniels, S. R. (2006). The consequences of childhood overweight and obesity. The Future of
Children, 16, 47-67. doi:10.1353/foc.2006.0004
Darling, N., & Steinberg, L. (1993). Parenting style as context: An integrative model.
Psychological Bulletin, 113, 487-496. doi:10.1037/0033-2909.113.3.487
Davies, M. (2000). The Blackwell encyclopedia of social work. Oxford, UK: Wiley-Blackwell.

99
Davison, K. K., & Birch, L. L. (2001a). Childhood overweight: A contextual model and
recommendations for future research. Obesity Reviews, 2, 159-171. doi:10.1046/j.1467-
789x.2001.00036.x
Davison, K. K., & Birch, L. L. (2001b). Weight status, parent reaction, and self-concept in five-
year-old girls. Pediatrics, 107, 46-53. doi:10.1542/peds.107.1.46
Davison, K. K., & Birch, L. L. (2004). Predictors of fat stereotypes among 9-year-old girls and
their parents. Obesity Research, 12, 86-94. doi:10.1038/oby.2004.12
Dietz, W. H. (1998). Health consequences of obesity in youth: Childhood predictors of adult
disease. Pediatrics, 101, 518-525. Retrieved from
http://go.galegroup.com.ezproxy.lib.ucalgary.ca/ps/i.do?p=AONE&sw=w&u=ucalgary&
v=2.1&it=r&id=GALE%7CA20546878&sid=summon&asid=48e5006c6e7426a6f9adc80
01efda71c
DiSantis, K. I., Hodges, E. A., Johnson, S. L., & Fisher, J. O. (2011). The role of responsive
feeding in overweight during infancy and toddlerhood: A systematic review.
International Journal of Obesity, 35, 480-492. doi:10.1038/ijo.2011.3
Durso, L. E., & Latner, J. D. (2008). Understanding self‐directed stigma: Development of the
Weight Bias Internalization Scale. Obesity, 16, S80-S86. doi:10.1038/oby.2008.448
Eisenberg, M. E., Neumark-Sztainer, D., & Story, M. (2003). Associations of weight-based
teasing and emotional well-being among adolescents. Archives of Pediatrics &
Adolescent Medicine, 157, 733-738. doi:10.1001/archpedi.157.8.733
Epstein, L. H., Paluch, R. A., Beecher, M. D., & Roemmich, J. N. (2008). Increasing healthy
eating vs. reducing high energy-dense foods to treat pediatric obesity. Obesity, 16, 318-
326. doi:10.1038/oby.2007.61

100
Epstein, L. H., Valoski, A., Wing, R. R., & McCurley, J. (1990). Ten-year follow-up of
behavioral, family-based treatment for obese children. JAMA, 264, 2519-2523.
doi:10.1001/jama.1990.03450190051027
Faith, M. S., Scanlon, K. S., Birch, L. L., Francis, L. A., & Sherry, B. (2004). Parent-child
feeding strategies and their relationships to child eating and weight status. Obesity
Research, 12, 1711-1722. doi:10.1038/oby.2004.212
Farkas, M. S., & Grolnick, W. S. (2010). Examining the components and concomitants of
parental structure in the academic domain. Motivation and Emotion, 34, 266-279.
doi:10.1007/s11031-010-9176-7
Fernandez, J. R., Klimentidis, Y. C., Dulin-Keita, A., & Casazza, K. (2012). Genetic influences
in childhood obesity: Recent progress and recommendations for experimental designs.
International Journal of Obesity, 36, 479-484. doi:10.1038/ijo.2011.236
Fisher, J. O., & Birch, L. L. (1999). Restricting access to palatable foods affects children's
behavioral response, food selection, and intake. The American Journal of Clinical
Nutrition, 69, 1264-1272. Retrieved from http://ajcn.nutrition.org/content/69/6/1264.short
Fisher, J. O., & Birch, L. L. (2002). Eating in the absence of hunger and overweight in girls from
5 to 7 y of age. The American Journal of Clinical Nutrition, 76, 226-231. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2604807/
Flegal, K. M., Tabak, C. J., & Ogden, C. L. (2006). Overweight in children: Definitions and
interpretation. Health Education Research, 21, 755-760. doi:10.1093/her/cyl128
Francis, L. A., & Birch, L. L. (2005). Maternal influences on daughters' restrained eating
behavior. Health Psychology, 24, 548-554. doi:10.1037/0278-6133.24.6.548
101
Francis, L. A., Hofer, S. M., & Birch, L. L. (2001). Predictors of maternal child-feeding style:
Maternal and child characteristics. Appetite, 37, 231-243. doi:10.1006/appe.2001.0427
Francis, L. A., & Susman, E. J. (2009). Self-regulation and rapid weight gain in children from
age 3 to 12 years. Archives of Pediatrics & Adolescent Medicine, 163, 297-302.
doi:10.1001/archpediatrics.2008.579
Freedman, D. S., Dietz, W. H., Srinivasan, S. R., & Berenson, G. S. (1999). The relation of
overweight to cardiovascular risk factors among children and adolescents: The Bogalusa
Heart Study. Pediatrics, 103, 1175-1182. doi:10.1542/peds.103.6.1175
Gable, S., & Lutz, S. (2000). Household, parent, and child contributions to childhood obesity.
Family Relations, 49, 293-300. doi:10.1111/j.1741-3729.2000.00293.x
Ghezelije, T. N. & Emami, A. (2009). Grounded theory: Methodology and philosophical
perspective. Nurse Researcher, 17, 15-23. Retrieved from
http://nurseresearcher.rcnpublishing.co.uk
Glaser, B. G. (1992). Emergence vs. forcing: Basics of grounded theory analysis. Mill Valley,
CA: Sociological Press.
Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded theory. Chicago, IL: Aldine.
Golan, M., & Crow, S. (2004). Parents are key players in the prevention and treatment of weight-
related problems. Nutrition Reviews, 62, 39-50. Retrieved from
https://www.researchgate.net/profile/Moria_Golan/publication/8680901_Parents_Are_Ke
y_Players_in_the_Prevention_and_Treatment_of_Weight-
Related_Problems/links/00b4952a5efc770e17000000.pdf

102
Graves, T., Meyers, A. W., & Clark, L. (1988). An evaluation of parental problem-solving
training in the behavioral treatment of childhood obesity. Journal of Consulting and
Clinical Psychology, 56, 246-250. doi:10.1037/0022-006X.56.2.246
Gray, W. N., Janicke, D. M., Wistedt, K. M., & Dumont-Driscoll, M. C. (2010). Factors
associated with parental use of restrictive feeding practices to control their children's food
intake. Appetite, 55, 332-337. doi:10.1016/j.appet.2010.07.005.
Grier, S. A., Mensinger, J., Huang, S. H., Kumanyika, S. K., & Stettler, N. (2007). Fast-food
marketing and children's fast-food consumption: Exploring parents' influences in an
ethnically diverse sample. Journal of Public Policy & Marketing, 26, 221-235.
doi:10.1509/jppm.26.2.221
Grolnick, W. S., & Pomerantz, E. M. (2009). Issues and challenges in studying parental control:
Toward a new conceptualization. Child Development Perspectives, 3, 165-170.
doi:10.1111/j.1750-8606.2009.00099.x
Guerrieri, R., Nederkoorn, C., & Jansen, A. (2007). How impulsiveness and variety influence
food intake in a sample of healthy women. Appetite, 48, 119-122.
doi:10.1016/j.appet.2006.06.004
Guxens, M., Mendez, M. A., Julvez, J., Plana, E., Forns, J., Basagaña, X., ... & Sunyer, J. (2009).
Cognitive function and overweight in preschool children. American Journal of
Epidemiology, 170, 438-446. doi:10.1093/aje/kwp140
Harper, L. V., & Sanders, K. M. (1975). The effect of adults' eating on young children's
acceptance of unfamiliar foods. Journal of Experimental Child Psychology, 20, 206-214.
doi:10.1016/0022-0965(75)90098-3
103
Hayden-Wade, H. A., Stein, R. I., Ghaderi, A., Saelens, B. E., Zabinski, M. F., & Wilfley, D. E.
(2005). Prevalence, characteristics, and correlates of teasing experiences among
overweight children vs. non-overweight peers. Obesity Research, 13, 1381-1392.
doi:10.1038/oby.2005.167
Heath, H., & Cowley, S. (2004). Developing a grounded theory approach: A comparison of
Glaser and Strauss. International Journal of Nursing Studies, 41, 141-150.
doi:10.1016/S0020-7489(03)00113-5
Henwood, K. L., & Pidgeon, N. F. (2003). Grounded theory in psychological research. In P.
Camic, J. Rhodes, & L. Yardley (Eds.), Qualitative research in psychology: Expanding
perspectives in methodology and design (pp. 131-155). Washington, DC: APA
Publications.
Hetherington, M. M., Cecil, J. E., Jackson, D. M., & Schwartz, C. (2011). Feeding infants and
young children. From guidelines to practice. Appetite, 57, 791-795.
doi:10.1016/j.appet.2011.07.005
Ho, M., Garnett, S. P., Baur, L., Burrows, T., Stewart, L., Neve, M., & Collins, C. (2012).
Effectiveness of lifestyle interventions in child obesity: Systematic review with meta-
analysis. Pediatrics, 130, e1647-e1671. doi:10.1542/peds.2012-1176
Holland, J. C., Kolko, R. P., Stein, R. I., Welch, R. R., Perri, M. G., Schechtman, K. B., ... &
Wilfley, D. E. (2014). Modifications in parent feeding practices and child diet during
family‐based behavioral treatment improve child zBMI. Obesity, 22, E119-E126.
doi:10.1002/oby.20708

104
Holt, N. L., Moylan, B. A., Spence, J. C., Lenk, J. M., Sehn, Z. L., & Ball, G. D. (2008).
Treatment preferences of overweight youth and their parents in Western Canada.
Qualitative Health Research, 18, 1206-1219. doi:10.1177/1049732308321740
Hubbs-Tait, L., Kennedy, T. S., Page, M. C., Topham, G. L., & Harrist, A. W. (2008). Parental
feeding practices predict authoritative, authoritarian, and permissive parenting styles.
Journal of the American Dietetic Association, 108, 1154-1161.
doi:10.1016/j.jada.2008.04.008
Hughes, S. O., Power, T. G., Fisher, J. O., Mueller, S., & Nicklas, T. A. (2005). Revisiting a
neglected construct: Parenting styles in a child-feeding context. Appetite, 44, 83-92.
doi:10.1016/j.appet.2004.08.007
Hutchinson, S. A., & Wilson, H. S. (2001). Grounded theory: The method. In P. L. Munhall
(Ed.), Nursing research, a qualitative perspective (3rd
ed., pp. 209-244). Mississauga,
ON: Jones and Barlett.
Israel, A. C., Stolmaker, L., & Andrian, C. A. (1985). The effects of training parents in general
child management skills on a behavioral weight loss program for children. Behavior
Therapy, 16, 169-180. doi:10.1016/S0005-7894(85)80043-5
Jackson, C., Henriksen, L., & Foshee, V. A. (1998). The Authoritative Parenting Index:
Predicting health risk behaviors among children and adolescents. Health Education &
Behavior, 25, 319-337. doi:10.1177/109019819802500307
Jansen, E., Daniels, L. A., & Nicholson, J. M. (2012). The dynamics of parenting and early
feeding–constructs and controversies: A viewpoint. Early Child Development and Care,
182, 967-981. doi:10.1080/03004430.2012.678593

105
Johnson, S. L. (2000). Improving preschoolers' self-regulation of energy intake. Pediatrics, 106,
1429-1435. doi:10.1542/peds.106.6.1429
Johnson, S. L., & Birch, L. L. (1994). Parents' and children's adiposity and eating style.
Pediatrics, 94, 653-661. Retrieved from
http://pediatrics.aappublications.org.ezproxy.lib.ucalgary.ca/content/pediatrics/94/5/653.f
ull.pdf
Joyce, J. L., & Zimmer-Gembeck, M. J. (2009). Parent feeding restriction and child weight. The
mediating role of child disinhibited eating and the moderating role of the parenting
context. Appetite, 52, 726-734. doi:10.1016/j.appet.2009.03.015
Kiess, W., Reich, A., Muller, G., Meyer, K., Galler, A., Bennek, J., & Kratzsch, J. (2001).
Clinical aspects of obesity in childhood and adolescence-diagnosis, treatment and
prevention. International Journal of Obesity & Related Metabolic Disorders, 25, S75-
S79. doi:10.1038/sj.ijo.0801704
Kirschenbaum, D. S., Harris, E. S., & Tomarken, A. J. (1984). Effects of parental involvement in
behavioral weight loss therapy for preadolescents. Behavior Therapy, 15, 485-500.
doi:10.1016/S0005-7894(84)80051-9
Kraig, K. A., & Keel, P. K. (2001). Weight-based stigmatization in children. International
Journal of Obesity, 25, 1661-1666. doi:10.1038/sj.ijo.0801813
Kral, T. V., & Rauh, E. M. (2010). Eating behaviors of children in the context of their family
environment. Physiology & Behavior, 100, 567-573. doi:10.1016/j.physbeh.2010.04.031
Latner, J. D., Barile, J. P., Durso, L. E., & O'Brien, K. S. (2014). Weight and health-related
quality of life: The moderating role of weight discrimination and internalized weight bias.
Eating Behaviors, 15, 586-590. doi:10.1016/j.eatbeh.2014.08.014

106
Latner, J. D., & Stunkard, A. J. (2003). Getting worse: The stigmatization of obese children.
Obesity Research, 11, 452-456. doi:10.1038/oby.2003.61
Lindsay, A. C., Sussner, K. M., Greaney, M. L., & Peterson, K. E. (2011). Latina mothers'
beliefs and practices related to weight status, feeding, and the development of child
overweight. Public Health Nursing, 28, 107-118. doi:10.1111/j.1525-1446.2010.00906.x
Lichtman, M. (2013). Qualitative research in education: A user’s guide (3rd
ed.). Los Angeles,
CA: Sage.
Lucas, N., Maguire, B., & Nicholson, J. M. (2010). Parenting practices and behaviours.
Australian Institute of Family Studies LSAC Annual Statistical Report, 2010, 43-56.
Retrieved from http://growingupinaustralia.gov.au/pubs/asr/2010/asr2010.pdf#page=59
Ludwig, D. S., & Ebbeling, C. B. (2001). Type 2 diabetes mellitus in children: Primary care and
public health considerations. JAMA, 286, 1427-1430. doi:10.1001/jama.286.12.1427
Lytle, L. A., Varnell, S., Murray, D. M., Story, M., Perry, C., Birnbaum, A. S., et al. (2003).
Predicting adolescents' intake of fruits and vegetables. Journal of Nutrition Education
and Behavior, 35, 170-178. doi:10.1016/S1499-4046(06)60331-X
Maccoby, E., & Martin, J. (1983). Socialization in the context of the family: Parent-child
interaction. In P. H. Mussen & E. M. Hetherington (Eds.), Handbook of child psychology:
Socialization, personality, and social development (Vol. 4, pp. 1-101). New York, NY:
Wiley.
Marbell, K. N., & Grolnick, W. S. (2013). Correlates of parental control and autonomy support
in an interdependent culture: A look at Ghana. Motivation and Emotion, 37, 79-92.
doi:10.1007/s11031-012-9289-2
107
McCann, T. V., & Clark, E. (2003). Grounded theory in nursing research: Part 1 -
Methodology. Nurse Researcher, 11, 7-18. Retrieved from
http://go.galegroup.com.ezproxy.lib.ucalgary.ca/ps/i.do?id=GALE%7CA111897099&sid
=summon&v=2.1&u=ucalgary&it=r&p=AONE&sw=w&asid=641e6032514a2afe19be25
0c484f0b20
McCann, T. V., & Clark, E. (2003a). Grounded theory in nursing research: Part 2 -
Critique. Nurse Researcher, 11, 19-28. Retrieved from
http://go.galegroup.com.ezproxy.lib.ucalgary.ca/ps/i.do?id=GALE%7CA111897100&sid
=summon&v=2.1&u=ucalgary&it=r&p=AONE&sw=w&asid=74a5f02cc69752fd1a3abb
2b3389d698
Miles, M. B., Huberman, A. M., & Saldaña, J. (2014). Qualitative data analysis: A methods
sourcebook. (3rd ed.). Thousand Oaks, CA: Sage.
Mills, J., Bonner, A., & Francis, K. (2006). The development of constructivist grounded theory.
International Journal of Qualitative Methods, 5, 1-10. Retrieved from
http://ejournals.library.ualberta.ca/index.php/IJQM/index
Mischler E. G. (1979). Meaning in context: Is there any other kind? Harvard Educational
Review, 49, 1-19. Retrieved from
http://www.metapress.com.ezproxy.lib.ucalgary.ca/content/b748n4133677245p/
Monasta, L., Batty, G. D., Cattaneo, A., Lutje, V., Ronfani, L., Van Lenthe, F. J., & Brug, J.
(2010). Early-life determinants of overweight and obesity: A review of systematic
reviews. Obesity Reviews, 11, 695-708. doi:10.1111/j.1467-789X.2010.00735.x
108
Musher-Eizenman, D. R., Holub, S. C., Hauser, J. C., & Young, K. M. (2007). The relationship
between parents’ anti-fat attitudes and restrictive feeding. Obesity, 15, 2095-2102.
doi:0.1038/oby.2007.249.
Must, A., & Strauss, R. S. (1999). Risks and consequences of childhood and adolescent obesity.
International Journal of Obesity & Related Metabolic Disorders, 23, S2-S11.
doi:10.1038/sj/ijo/0800852
Nederkoorn, C., Braet, C., Van Eijs, Y., Tanghe, A., & Jansen, A. (2006). Why obese children
cannot resist food: The role of impulsivity. Eating Behaviors, 7, 315-322.
doi:10.1016/j.eatbeh.2005.11.005
Nederkoorn, C., Smulders, F. T., Havermans, R. C., Roefs, A., & Jansen, A. (2006). Impulsivity
in obese women. Appetite, 47, 253-256. doi:10.1016/j.appet.2006.05.008
Neumark-Sztainer, D., Falkner, N., Story, M., Perry, C., Hannan, P. J., & Mulert, S. (2002).
Weight-teasing among adolescents: Correlations with weight status and disordered eating
behaviors. International Journal of Obesity, 26, 123-131. doi:10.1038/sj.ijo.0801853
Neumark-Sztainer, D., Story, M., & Faibisch, L. (1998). Perceived stigmatization among
overweight African-American and Caucasian adolescent girls. Journal of Adolescent
Health, 23, 264-270.
Neumark-Sztainer, D., Story, M., & Harris, T. (1999). Beliefs and attitudes about obesity among
teachers and school health care providers working with adolescents. Journal of Nutrition
Education, 31, 3-9. doi:10.1016/S0022-3182(99)70378-X
O'Donnell, S. I., Hoerr, S. L., Mendoza, J. A., & Goh, E. T. (2008). Nutrient quality of fast food
kids meals. The American Journal of Clinical Nutrition, 88, 1388-1395. Retrieved from
http://s3.amazonaws.com/academia.edu.documents/39858638/1388.pdf?AWSAccessKey

109
Id=AKIAIWOWYYGZ2Y53UL3A&Expires=1492639393&Signature=SJq5zIA09snX3
YHmzznmyICsLAg%3D&response-content-
disposition=inline%3B%20filename%3DNutrient_quality_of_fast_food_kids_meals.pdf
Ogden, J., Reynolds, R., & Smith, A. (2006). Expanding the concept of parental control: A role
for overt and covert control in children's snacking behaviour? Appetite, 47, 100-106.
doi:10.1016/j.appet.2006.03.330
Park, M. H., Falconer, C., Viner, R. M., & Kinra, S. (2012). The impact of childhood obesity on
morbidity and mortality in adulthood: A systematic review. Obesity Reviews, 13, 985-
1000. doi:10.1111/j.1467-789X.2012.01015.x
Pearl, R. L., White, M. A., & Grilo, C. M. (2014). Overvaluation of shape and weight as a
mediator between self-esteem and weight bias internalization among patients with binge
eating disorder. Eating Behaviors, 15, 259-261. doi:10.1016/j.eatbeh.2014.03.005
Philippas, N. G., & Lo, C. W. (2004). Childhood obesity: Etiology, prevention, and treatment.
Nutrition in Clinical Care: An Official Publication of Tufts University, 8, 77-88.
Retrieved from http://dc8qa4cy3n.search.serialssolutions.com/?ctx_ver=Z39.88-
2004&ctx_enc=info%3Aofi%2Fenc%3AUTF-
8&rfr_id=info%3Asid%2Fsummon.serialssolutions.com&rft_val_fmt=info%3Aofi%2Ff
mt%3Akev%3Amtx%3Ajournal&rft.genre=article&rft.atitle=Childhood+obesity%3A+et
iology%2C+prevention%2C+and+treatment&rft.jtitle=Nutrition+in+clinical+care+%3A
+an+official+publication+of+Tufts+University&rft.au=Philippas%2C+Niki+G&rft.au=L
o%2C+Clifford+W&rft.date=2005-04-01&rft.issn=1096-6781&rft.eissn=1523-
5408&rft.volume=8&rft.issue=2&rft.spage=77&rft_id=info%3Apmid%2F16013226&rft
.externalDocID=16013226¶mdict=en-US

110
Puhl, R., & Brownell, K. D. (2001). Bias, discrimination, and obesity. Obesity, 9, 788-805.
doi:10.1038/oby.2001.108
Puhl, R. M., & Latner, J. D. (2007). Stigma, obesity, and the health of the nation's children.
Psychological Bulletin, 133, 557-580. doi:10.1037/0033-2909.133.4.557
Raitakari, O. T., Juonala, M., & Viikari, J. S. A. (2005). Obesity in childhood and vascular
changes in adulthood: Insights into the cardiovascular risk in young Finns study.
International Journal of Obesity, 29, S101-S104. doi:10.1038/sj.ijo.0803085
Raskin, J. D. (2002). Constructivism in psychology: Personal construct psychology, radical
constructivism, and social constructionism. In J. D. Raskin & S. K. Bridges (Eds.),
Studies in meaning: Exploring constructivist psychology (pp. 1-25). New York, NY: Pace
University Press.
Reedy, J., & Krebs-Smith, S. M. (2010). Dietary sources of energy, solid fats, and added sugars
among children and adolescents in the United States. Journal of the American Dietetic
Association, 110, 1477-1484. doi:10.1016/j.jada.2010.07.010
Rifas-Shiman, S. L., Sherry, B., Scanlon, K., Birch, L. L., Gillman, M. W., & Taveras, E. M.
(2011). Does maternal feeding restriction lead to childhood obesity in a prospective
cohort study? Archives of Disease in Childhood, 96, 265-269.
doi:10.1136/adc.2009.175240
Riggs, N. R., Spruijt-Metz, D., Sakuma, K. L., Chou, C. P., & Pentz, M. A. (2010). Executive
cognitive function and food intake in children. Journal of Nutrition Education and
Behavior, 42, 398-403. doi:10.1016/j.jneb.2009.11.003
111
Ristovski-Slijepcevic, S., Chapman, G. E., & Beagan, B. L. (2010). Being a ‘good mother’:
Dietary governmentality in the family food practices of three ethnocultural groups in
Canada. Health, 14, 467-483. doi:10.1177/1363459309357267
Rhee, K. (2008). Childhood overweight and the relationship between parent behaviors, parenting
style, and family functioning. The Annals of the American Academy of Political and
Social Science, 615, 12-37. doi:10.1177/0002716207308400
Rhee, K. E., Coleman, S. M., Appugliese, D. P., Kaciroti, N. A., Corwyn, R. F., Davidson, N. S.,
... & Lumeng, J. C. (2009). Maternal feeding practices become more controlling after and
not before excessive rates of weight gain. Obesity, 17, 1724-1729.
doi:10.1038/oby.2009.54
Roberts, K. C., Shields, M., de Groh, M., Aziz, A., & Gilbert, J. A. (2012). Overweight and
obesity in children and adolescents: Results from the 2009 to 2011 Canadian Health
Measures Survey. Health Reports, 23, 37-41. Retrieved from
http://s3.amazonaws.com/academia.edu.documents/44335748/Overweight_and_obesity_i
n_children_and_a20160402-18206-
7rm2uu.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1492640517
&Signature=%2FUKfV%2FSA42Ltt2xu2QbWrsNFKjk%3D&response-content-
disposition=inline%3B%20filename%3DOverweight_and_obesity_in_children_and_a.pd
f#page=39
Robinson, S., Marriott, L., Poole, J., Crozier, S., Borland, S., Lawrence, W., et al. (2007).
Dietary patterns in infancy: The importance of maternal and family influences on feeding
practice. British Journal of Nutrition, 98, 1029-1037. doi:10.1017/s0007114507750936

112
Rudman, L. A., Feinberg, J., & Fairchild, K. (2002). Minority members' implicit attitudes:
Automatic ingroup bias as a function of group status. Social Cognition, 20, 294-320.
doi:10.1521/soco.20.4.294.19908
Russell-Mayhew, S. (in press). The weight of the world in her hands. Invited chapter. In N.
Arthur & C. Collins (Eds.), Culture-Infused Counselling (3rd
ed.). Counselling Concepts.
Russell-Mayhew, S., Nutter, S., Alberga, A., Jelinski, S., Ball, G. D., Edwards, A., ... & Forhan,
M. (2016). Environmental scan of weight bias exposure in primary health care training
programs. The Canadian Journal for the Scholarship of Teaching and Learning, 7, 1-14.
doi:10.5206/cjsotl-rcacea.2016.2.5
Russell-Mayhew, S., Nutter, S., Ireland, A., Gabriele, T., Bardick, A., Crooks, J., & Peat, G.
(2015). Pilot testing a professional development model for preservice teachers in the area
of health and weight: Feasibility, utility, and efficacy. Advances in School Mental Health
Promotion, 8, 176-186. doi:10.1080/1754730X.2015.1040040
Sacher, P. M., Kolotourou, M., Chadwick, P. M., Cole, T. J., Lawson, M. S., Lucas, A., &
Singhal, A. (2010). Randomized controlled trial of the MEND program: A family‐based
community intervention for childhood obesity. Obesity, 18, S62-S68.
doi:10.1038/oby.2009.433
Satter, E. M. (1986). The feeding relationship. Journal of American Dietetic Association, 86,
352-356. Retrieved from http://www.adinapearson.com/kvpaHB2WmRY5/wp-
content/uploads/2014/09/The-feeding-relationship.pdf
Satter, E. (1990). The feeding relationship: Problems and interventions. The Journal of
Pediatrics, 117, 181-189. doi:10.1016/S0022-3476(05)80017-4
113
Savage, J. S., Fisher, J. O., & Birch, L. L. (2007). Parental influence on eating behavior:
Conception to adolescence. The Journal of Law, Medicine & Ethics, 35, 22-34.
doi:10.1111/j.1748-720X.2007.00111.x
Savoye, M., Shaw, M., Dziura, J., Tamborlane, W. V., Rose, P., Guandalini, C., ... & Caprio, S.
(2007). Effects of a weight management program on body composition and metabolic
parameters in overweight children: A randomized controlled trial. JAMA, 297, 2697-
2704. doi:10.1001/jama.297.24.2697
Schvey, N. A., & White, M. A. (2015). The internalization of weight bias is associated with
severe eating pathology among lean individuals. Eating Behaviors, 17, 1-5.
doi:10.1016/j.eatbeh.2014.11.001
Schvey, N. A., Roberto, C. A., & White, M. A. (2013). Clinical correlates of the Weight Bias
Internalization Scale in overweight adults with binge and purge behaviours. Advances in
Eating Disorders: Theory, Research and Practice, 1, 213-223.
doi:10.1080/21662630.2013.794523
Shomaker, L. B., & Furman, W. (2009). Interpersonal influences on late adolescent girls' and
boys' disordered eating. Eating Behaviors, 10, 97-106. doi:10.1016/j.eatbeh.2009.02.003
Shunk, J. A., & Birch, L. L. (2004). Girls at risk for overweight at age 5 are at risk for dietary
restraint, disinhibited overeating, weight concerns, and greater weight gain from 5 to 9
years. Journal of the American Dietetic Association, 104, 1120-1126.
doi:10.1016/j.jada.2004.04.031
Skouteris, H., McCabe, M., Swinburn, B., Newgreen, V., Sacher, P., & Chadwick, P. (2011).
Parental influence and obesity prevention in pre-schoolers: A systematic review of
interventions. Obesity Reviews, 12, 315-328. doi:10.1111/j.1467-789X.2010.00751.x

114
Sleddens, E. F. C., Gerards, S. M. P. L., Thijs, C., de Vries, N. K., & Kremers, S. P. J. (2011).
General parenting, childhood overweight and obesity-inducing behaviors: A review.
International Journal of Pediatric Obesity, 6, e12-e27.
doi:10.3109/17477166.2011.566339
Smith, M. (2011). Measures for assessing parenting in research and practice. Child and
Adolescent Mental Health, 16, 158-166. doi:10.1111/j.1475-3588.2010.00585.x
Snethen, J. A., Broome, M. E., & Cashin, S. E. (2006). Effective weight loss for overweight
children: A meta-analysis of intervention studies. Journal of Pediatric Nursing, 21, 45-
56. doi:10.1016/j.pedn.2005.06.006
Spruijt-Metz, D. (2011). Etiology, treatment, and prevention of obesity in childhood and
adolescence: A decade in review. Journal of Research on Adolescence, 21, 129-152.
doi:10.1111/j.1532-7795.2010.00719.x
Spruijt-Metz, D., Li, C., Cohen, E., Birch, L., & Goran, M. (2006). Longitudinal influence of
mother’s child-feeding practices on adiposity in children. The Journal of Pediatrics, 148,
314-320. doi:10.1016/j.jpeds.2005.10.035
Strauss A. L. & Corbin J. M. (1990). Basics of qualitative research. Newbury Park, CA: Sage
Publications.
Strauss, R. S., & Pollack, H. A. (2003). Social marginalization of overweight children. Archives
of Pediatrics & Adolescent Medicine, 157, 746-752. doi:10.1001/archpedi.157.8.746
Storch, E. A., Milsom, V. A., DeBraganza, N., Lewin, A. B., Geffken, G. R., & Silverstein, J. H.
(2007). Peer victimization, psychosocial adjustment, and physical activity in overweight
and at-risk-for-overweight youth. Journal of Pediatric Psychology, 32, 80-89.
doi:10.1093/jpepsy/jsj113

115
Thompson, M. E. (2010). Parental feeding and childhood obesity in preschool-age children:
Recent findings from the literature. Issues in Comprehensive Pediatric Nursing, 33, 205-
267. doi:10.3109/01460862.2010.530057
Tweed, A., & Charmaz, K. (2012). Grounded theory methods for mental health practitioners. In
D. Harper & A. R. Thompson (Eds.), Qualitative research methods in mental health and
Psychotherapy: A guide for students and practitioners (pp.131-146). Oxford, UK: Wiley-
Blackwell.
Ventura, A. K., & Birch, L. L. (2008). Does parenting affect children's eating and weight status?
International Journal of Behavioral Nutrition and Physical Activity, 5, 15-27.
doi:10.1186/1479-5868-5-15
Vereecken, C., Legiest, E., De Bourdeaudhuij, I., & Maes, L. (2009). Associations between
general parenting styles and specific food-related parenting practices and children's food
consumption. American Journal of Health Promotion, 23, 233-240.
doi:10.4278/ajhp.07061355
Vivier, P., & Tompkins, C. (2008). Health consequences of obesity in children and adolescents.
In E. Jelalian & R. G. Steele (Eds.), Handbook of childhood and adolescent obesity (pp.
11-24). New York, NY: Springer US.
Vos, M. B., & Welsh, J. (2010). Childhood obesity: Update on predisposing factors and
prevention strategies. Current Gastroenterology Reports, 12, 280-287.
doi:10.1007/s11894-010-0116-1
Wabitsch, M. (2000). Overweight and obesity in European children: Definition and diagnostic
procedures, risk factors and consequences for later health outcome. European Journal of
Pediatrics, 159, S8-S13. doi:10.1007/PL00014368
116
Wake, M., Nicholson, J. M., Hardy, P., & Smith, K. (2007). Preschooler obesity and parenting
styles of mothers and fathers: Australian national population study. Pediatrics, 120,
E1520-E1527. doi:10.1542/peds.2006-3707
Walker, L., & Kirby, R. (2010). Conceptual and measurement issues in early parenting practices
research: An epidemiologic perspective. Maternal and Child Health Journal, 14, 958-
970. doi:10.1007/s10995-009-0532-8
Wang, S. S., Brownell, K. D., & Wadden, T. A. (2004). The influence of the stigma of obesity on
overweight individuals. International Journal of Obesity, 28, 1333-1337.
doi:10.1038/sj.ijo.0802730
Wardle, J., Sanderson, S., Guthrie, C. A., Rapoport, L., & Plomin, R. (2002). Parental feeding
style and the inter-generational transmission of obesity risk. Obesity Research, 10, 453-
462. doi:10.1038/oby.2002.63
Webber, L., Cooke, L., Hill, C., & Wardle, J. (2010). Associations between children's appetitive
traits and maternal feeding practices. Journal of the American Dietetic Association, 110,
1718-1722. doi:10.1016/j.jada.2010.08.007
Weiss, D. L. (2013). The heavy: A mother, a daughter, a diet. New York, NY: Ballantine Books.
Weiss, R., & Caprio, S. (2005). The metabolic consequences of childhood obesity. Best Practice
& Research Clinical Endocrinology & Metabolism, 19, 405-419.
doi:10.1016/j.beem.2005.04.009
Whitaker, R. C., Wright, J. A., Pepe, M. S., Seidel, K. D., & Dietz, W. H. (1997). Predicting
obesity in young adulthood from childhood and parental obesity. New England Journal of
Medicine, 337, 869-873. doi:10.1056/NEJM199709253371301
117
Wilson, W., & Barn, H. T. (2012). Constructive grounded theory in the search for meaning on
global mindedness: A novice researcher’s guide. International Journal of Evidence Based
Coaching and Mentoring, 6, 1-14. Retrieved from
http://ijebcm.brookes.ac.uk/documents/special06-paper-01.pdf
World Health Organization. (2014). Commission on Ending Childhood Obesity: Facts and
Figures on Childhood Obesity. World Health Organization. Retrieved from
http://www.who.int/end-childhood-obesity/facts/en/
World Health Organization. (2016). Media Centre: Obesity and Overweight Fact Sheet. World
Health Organization. Retrieved from
http://www.who.int/mediacentre/factsheets/fs311/en/
Young, R. A., & Collin, A. (2004). Introduction: Constructivism and social constructionism in
the career field. Journal of Vocational Behaviour, 64, 373-388.
doi:10.1016/j.jvb.2003.12.005
Young, K. M., Northern, J. J., Lister, K. M., Drummond, J. A., & O'Brien, W. H. (2007). A
meta-analysis of family-behavioral weight-loss treatments for children. Clinical
Psychology Review, 27, 240-249. doi:10.1016/j.cpr.2006.08.003
118
Appendix A
Recruitment Poster
Werklund School of Education
Did your parents put you on a
diet as a child?
Are you between the ages of 18-29?
Participate in an interview study!
If you were put on a diet by your parents as a child, and are between the ages
of 18 and 29, you may be eligible to participate.
You will be asked to answer questions such as “What was your childhood
experience of being put on a diet by your parents?” and “How do you think
parental dietary control has affected you?”
If you are interested, please contact the researcher, Isabel Brun at
This study has been approved by the University of Calgary Conjoint Faculties Research Ethics
Board.
Isab
el Bru
n
ibru
n@
uca
lgary
.ca
Isab
el Bru
n
ibru
n@
uca
lgary
.ca
Isab
el Bru
n
ibru
n@
uca
lgary
.ca
Isab
el Bru
n
ibru
n@
uca
lgary
.ca
Isab
el Bru
n
ibru
n@
uca
lgary
.ca
Isab
el Bru
n
ibru
n@
uca
lgary
.ca
Isab
el Bru
n
ibru
n@
uca
lgary
.ca
Isab
el Bru
n
ibru
n@
uca
lgary
.ca
119
Appendix B
Recruitment Screening Questions
Thank you for your interest in my study. My primary research inquiry is to understand how
young adults describe their childhood experiences of being put on a diet by their parents.
I’d like to ask you a few questions to ensure that you fit participation criteria for my research
study on childhood experiences of parental feeding control.
1. Are you a young adult (ages 18-29)?
2. Have you ever been put on a diet by your parents during your childhood?
3. Did your parents put you on a diet the purpose of weight loss promotion or weight gain
prevention?
4. Have you ever experienced impaired memory (in ways that might get in the way of you
remembering or talking about these childhood experiences)?
5. Was the parental feeding control you experienced a consequence of a pattern of neglect
or abuse? (versus parents just trying to ‘do the right thing’)
6. Do you have any condition that causes impaired perceptions?

120
Appendix C
Consent Form
Name of Researcher, Faculty, Department, Telephone & Email:
Isabel Brun, Werklund School of Education, Counselling Psychology, (506) 999-2524, [email protected]
Supervisor:
Dr. Shelly Russell-Mayhew, Werklund School of Education, Counselling Psychology, (403) 220-8375,
Title of Project:
How do young adults describe their childhood experiences of being put on diets by their parents?
Sponsor:
None
This consent form, a copy of which has been given to you, is only part of the process of informed consent. If you
want more details about something mentioned here, or information not included here, you should feel free to ask.
Please take the time to read this carefully and to understand any accompanying information.
The University of Calgary Conjoint Faculties Research Ethics Board has approved this research study.
Purpose of the Study
To examine remembered childhood experiences of parental feeding control.
Study Rationale
In Canada, childhood obesity continues to be a serious public health concern. Research demonstrates that
children with obesity are at a greater risk for developing a variety of health issues, and are more susceptible to
weight-related bullying, stigmatization, and marginalization than their non-obese peers. Parents of children who
struggle with their weight might want to protect their children from the previously mentioned negative
consequences. One way of protecting their children might be to control their food intake (i.e., put them on a diet)
in order to try to manage their weight and size.
Parental feeding control practices are often implemented with the best of intentions. Yet, research suggests that
these practices can have a negative impact on children’s eating behaviours. Despite these concerns, minimal

121
research has been conducted to thoroughly examine how children experience these practices. In order to attend to
this gap in research, the current study will examine remembered childhood experiences of parental feeding control
by asking the following question: How do young adults describe their childhood experiences of being put on diets
by their parents?
What Will I Be Asked To Do?
Should you agree to participate, you will be asked to share your childhood experiences of being put on a diet by
your parents in an individual face-to-face interview. During the interview, we will discuss your experiences, and I
will ask you about how these practices have impacted you socially and psychologically. I will also ask you about
any further thoughts and views on this topic, and will make sure I understand your experiences well. Interview
questions will be sent to you via e-mail prior to the interview for your consideration. I will use an audio recorder
to record all interviews, and will transcribe the interviews verbatim, to ensure accuracy of data analysis.
Additionally, I will conduct the interview in a private room at the University of Calgary, or another quiet and
private place of your choosing. I will be emailing you initial results so that you can confirm or adjust the
information to ensure accuracy. Your participation in the interview portion of the study will require
approximately 60 – 90 minutes of your time, and is completely voluntary - you may withdraw from the study at
any time before or during the interview process. You may also decline to answer any of interview questions. If
you choose to withdraw, you may verbally indicate this to the researcher. Should you choose to withdraw before
the interview is complete, you will be asked if data up to that point may be retained for data analysis and your
decision will be honoured. Data cannot be withdrawn after the interview process is complete.
What Type of Personal Information Will Be Collected
Should you agree to participate, you will be asked to provide your, as well as your parent’s, demographic
information including: gender, age, level of education, household income, and ethnic background. This
information, along with the audio-recorded interview, will be kept separate from your name and will be identified
only by a pseudonym of your choosing. Only the primary researcher and her supervisor will have access to the
audio-recordings and demographic information.
Are there Risks or Benefits if I Participate?
There are no foreseeable risks, harms, or inconveniences to you as the participant. The interview questions will
ask about childhood experiences related to parental feeding control. The focus will be on the impacts of such
practices. If the interview topics cause negative thoughts or emotional distress, you are encouraged to let the
researcher know, and a counselling appointment may be set up through the University of Calgary Wellness Centre
(if you are a student), or through the Calgary Counselling Centre.
The University of Calgary Counselling Center is located in the Wellness Centre
(Room 370, MacEwan Student Centre)
Open Monday to Friday from 9:00-4:30
Ph: 403 210-9355 (210-WELL)
The Calgary Counselling Centre is located downtown Calgary
#200, 940 6th Ave, SW, Calgary
Ph: 403 265-4980
122
You may find it interesting to talk about your childhood experiences of parental feeding control practices. Your
participation in this study may also help to identify potential impacts of parental feeding control practices which
could inform parenting strategies related to weight issues. You will receive a $20.00 gift certificate upon arriving
at the interview site.
What Happens to the Information I Provide?
Participation is completely voluntary, anonymous and confidential. You are free to discontinue participation at
any time before or during the interview process. If you choose to withdraw from the study, you will be asked if
the information provided up to that point can be kept for analysis, and your decision will be honoured.
No one except the researcher and her supervisor will be allowed to hear any of the answers on the interview tape.
There are no names on the questionnaire. Group information will be summarized for any presentation or
publication of results. The demographic questionnaires, which include participant and parental demographic
information, will be kept in a locked cabinet only accessible by the researcher and her supervisor. The anonymous
data will be stored for five years on a computer disk, at which time, it will be permanently erased. The data you
provide will be used towards completion of Master’s thesis.
Signatures
Your signature on this form indicates that 1) you understand to your satisfaction the information provided to you
about your participation in this research project, and 2) you agree to participate in the research project.
In no way does this waive your legal rights nor release the investigators, sponsors, or involved institutions from
their legal and professional responsibilities. You are free to withdraw from this research project at any time before
or during the interview process. You should feel free to ask for clarification or new information throughout your
participation.
Participant’s Pseudonym: ______________________________________________________________________
Participant’s Name: (please print) ________________________________________________________
Participant’s Signature: __________________________________________ Date: ________________
Researcher’s Name: (please print) _______________________________________________________
Researcher’s Signature: ________________________________________ Date: _________________
123
Questions/Concerns
If you have any further questions or want clarification regarding this research and/or your participation,
please contact:
Ms. Isabel Brun
Werklund School of Education, Department of Counselling Psychology
(506) 999-2524, [email protected]
and Dr. Shelly Russell-Mayhew, Werklund School of Education, Department of Counselling Psychology
(403) 220-8375, [email protected]
If you have any concerns about the way you have been treated as a participant, please contact an Ethic
Resource Officer, Research Services Office, University of Calgary at (403) 210-9863; email
A copy of this consent form has been given to you to keep for your records and reference. The
investigator has kept a copy of the consent form.
Additional Community Mental Health Resources
Clinical Services Contact Information
Family physicians Yellow pages
Psychiatrists Yellow pages
Psychologists Yellow pages
Calgary Health Region
Calgary Eating Disorder Program*
May need referral from G.P.
403-955-8700
Access Mental Health 403-943-1500
Calgary Counselling Centre** 403-265-4980
Calgary Association of Self-Help 403-266-8711
Calgary Family Services 403-269-9888
Catholic Family Services 403-233-2360
Jewish Family Services 403-287-3510
Calgary Catholic Immigration Society 403-298-4111
*Consultants are available to provide information about eating disorders and treatment options.
**Provides individual, couple, family, & group counselling for individuals with an eating disorder. Offers
sliding scale fees according to family size and income.
Distress and Crisis Resources Contact Information
Emergency Services Dial 911
Distress Centre 266-1605

124
Men’s Line 266-HELP (4357)
Teen Line 264-TEEN (8336)
Calgary Mental Health Crisis and Emergency Services Mobile
Response Team
266-1605
Canadian Mental Health Association Suicide Services (available 8:30
am to 4:30 pm)
297-1744
Calgary Health Region Mental Health Line 943-1500
Organizations Contact Information
Psychologists Association of Alberta (referrals) 1-888-424-0297
Canadian Mental Health Association (Calgary Office) 297-1700
Canadian Psychological Association www.cpa.ca
National Eating Disorder Information Centre www.nedic.ca
Calgary Eating Disorder Program 943-7700
www.crha-health.ab.ca/eatingdis
Eating Disorder Education Organization (Edmonton) www.edeo.org
National Eating Disorders Association (U.S.) www.edap.org
Other eating disorder-related web sites www.anred.com
www.anad.org
http://eatingdisorders.mentalhelp.net/
125
Appendix D
Participant Demographic Information Form
Pseudonym: __________________________________________________________
Gender: ______________________________________________________________
Age: _________________________________________________________________
Highest Level of Education Attained: _____________________________________
Income Status (please check one):
□ Under $20,000 □ $100,000 to just under $150,000
□ $20,000 to just under $40,000 □ $150,000 and above
□ $40,000 to just under $60,000 □ Prefer not to answer
□ $60,000 to just under $80,000
□ $80,000 to just under $100,000
Ethnic Background (please check one or specify as “other” and explain):
□ European /European-Canadian □ French-Canadian
□ Aboriginal □ Métis
□ Asian / Asian-Canadian □ South Asian / South Asian Canadian
□ African / African Canadian □ Caribbean / Caribbean Canadian
□ Middle Eastern / Middle Eastern Canadian □ Latin American/Latin American Canadian
Other (please specify) ____________________________________________

126
Participant’s Parents’ Demographic Information
Mother’s Highest Level of Education Attained: _____________________________________
Father’s Highest Level of Education Attained: ______________________________________
Mother’s Ethnic Background (please check one or specify as “other” and explain):
□ European /European-Canadian □ French-Canadian
□ Aboriginal □ Métis
□ Asian / Asian-Canadian □ South Asian / South Asian Canadian
□ African / African Canadian □ Caribbean / Caribbean Canadian
□ Middle Eastern / Middle Eastern Canadian □ Latin American/Latin American Canadian
Other (please specify) ____________________________________________
Father’s Ethnic Background (please check one or specify as “other” and explain):
□ European /European-Canadian □ French-Canadian
□ Aboriginal □ Métis
□ Asian / Asian-Canadian □ South Asian / South Asian Canadian
□ African / African Canadian □ Caribbean / Caribbean Canadian
□ Middle Eastern / Middle Eastern Canadian □ Latin American/Latin American Canadian
Other (please specify) ____________________________________________

127
Parental Household Income (please check one)
□ Under $20,000 □ $100,000 to just under $150,000
□ $20,000 to just under $40,000 □ $150,000 and above
□ $40,000 to just under $60,000 □ Prefer not to answer
□ $60,000 to just under $80,000
□ $80,000 to just under $100,000
Who was responsible for controlling your food intake (selecting both is an option)?
Mother _______ Father _________

128
Appendix E
Interview Questions
Primary Research Question: How do young adults describe their childhood experiences of being
put on diets by their parents?
Today, I’d like to talk with you about your childhood experience of parental feeding control.
Parental feeding control can include not permitting a child to eat specific foods (e.g., junk food),
only allowing a child to eat small portions of particular foods (i.e., putting a child on a diet),
monitoring a child’s consumption of certain foods (e.g., snack foods), and/or pressuring a child
to eat particular foods (e.g., vegetables). So, putting a child on a diet in order to reduce their
weight or size would be considered parental feeding control. Today, I would like to talk with
you about your childhood experiences of these practices, as well as its effects on various aspects
of your life.
1. Start by telling me the story of the first time your parents controlled your food
intake.
What do you think lead your parents to control your food intake in this
way?
Which parent was more involved in the food control?
What was your experience with the other parent?
What is your explanation of why this parent was more involved?
How do you make sense of this? How do you explain their
decision/motivation to control your food?
2. What other experiences of this kind of controlling practices are important for me
to know about?
What was it like for you?
3. In what ways have you been impacted by being put on a diet by your parents as a
child?
4. If you could offer advice to parents who are currently raising children, what
would that be?
What would you want parents to know about your experience of being put
on a diet by your parents as a child?
5. What have you learned from this experience (three main insights)?
129
6. Other questions (if not already answered):
How did your parents control your diet?
How long did your parents control your diet?
How often did your parents control your diet?
Did your parents agree on controlling your food intake?
What other non-family members were involved in controlling your diet?
What other family members participated in dietary control?
7. What have I missed?
What else is important for me to know about your childhood experience of
being put on a diet by your parents?

130
Appendix F
Sample Memos
March 14, 2017
- Participants report that guilting a child into losing weight doesn’t work.
o *Individuals aren’t shamed into losing weight*
o Participants describe that “guilt tripping” creates disconnection within the parent-
child relationship and causes them psychological distress (e.g., intense feelings of
guilt) when they eat foods that were restricted or are perceived as “bad”.
- Internalizing dietary control
o Participants have taken on the responsibility of controlling their own eating. They
describe internalizing parental dietary restriction and control.
They often feel guilt when they act in contradiction to their parents’
dietary wishes.
They also report engaging in calorie counting, restriction, and
purging to lessen their guilt associated with eating bad or restricted
foods.
- Long-lasting impacts of parental feeding control practices
o Participants report still struggling with weight preoccupation
Feeling badly about their weight and size (e.g., self-conscious or
dissatisfied with their bodies)
Engaging in compensatory eating behaviours (e.g., going on 1200 calorie
diets to lose weight, or purging to lessen their guilt when they eat “bad”
foods or eat too much).
Related to a fear of gaining weight?
o Further related to internalized parental messages about
weight?
- Is this fear of gaining weight, that my participants have been describing, related to
internalized weight bias or internalized parental messages about weight and size?
o Through their perception of parental motivations for using parental feeding
control practices, they are receiving certain messages about weight:
Being overweight is bad
Being overweight is less-than
Being overweight is unattractive
Being overweight is unhealthy
Etc.