issue 16 • may/june 2009 dia4ribe - diatribe 16 - may_jun 2009... · diatribe • research and...
TRANSCRIPT
I S S U E 1 6 • M AY / J U N E 2 0 0 9
From the Editor ...............1
Quotable Quotes ............2
Logbook ...........................3James Hirsch discusses his personal effort to defend Sonia Sotomayor
Test Drive ........................5The new second-generation OmniPod PDM, UST200
Learning Curve ................7Clinical trials and the FDA demystified
Conference Pearls ...........11The 2009 ADA scientific ses-sions: JDRF CGM trial and GLP-1 and other updates in type 1 and type 2 diabetes therapies
Trial Watch ......................13Oral insulin to prevent type 1, the TINSAL-2D trial of salsalate, and CGM for people with type 2
What We’re Reading .......14The Look AHEAD trial of lifestyle intervention in type 2 diabetes
New Now Next ...............16 Team Type 1 wins Race Across America, the JDRF Children’s Congress, the Medicare Diabetes Screen-ing Project, A1c as a diag-nostic tool for diabetes, and Cycloset approval
diaTribe Dialogue ............. 18Dr. George Eisenbarth on the prevention of type 1 diabetes
in this issue
research and product news for people with diabetes
1
®
from the editor
A fter this year’s American Diabetes Association Scientific Sessions (June 5-9), I can say with confidence that the future is looking bright for diabetes. Over the last couple of years, the diaTribe
team and I have been pleased and surprised by the volume of research going on to improve the lives of people with both type 1 and type 2, and this year was absolutely no exception. The meeting was a thoroughly
impressive showcase of new developments in therapies, clinical practice, and management techniques, and there are a lot of interesting things on the horizon!
The first thing that I was so happy to see at the meeting was INCREDIBLE enthusiasm about continuous glucose monitoring (CGM). To me, it really seems that the latest new generations of CGM systems are coming into their own as a critical tool in diabetes man-agement. We owe a lot to the work of the JDRF, which presented new one-year data at ADA from its well-respected CGM study (see this issue’s Conference Pearls). If the first half of the JDRF’s CGM results helped to push this technology onto the diabetes stage, this follow-up data really puts it in the spotlight, showing that participants continued to show lower A1cs and reduced hypoglycemia with CGM use.
Meanwhile, on June 26 patients who use Sanofi-Aventis’s Lantus insulin received the alarming news that “a possible link” may exist between the insulin and a higher risk for cancer. The European Association for the Study of Diabetes, which published the report, made a call for more research but also urged patients who are using Lantus to continue taking it. We are concerned about the potential for sensational media coverage and undue fear not only among Lantus users but also among other long-acting insulin users. There may be safety risks to assess with Lantus, but if there are, the benefits should be assessed and balanced as well. It’s too early to draw any firm conclusions about Lantus (see Quotable Quotes). On a personal note, I hope the report does not herald a return to human insulins, which from my experience caused far more hypoglycemia than insulin analogs.
Finally, we’re very excited about this issue’s giveaway, which allows us to share our excitement about CGM in a more—shall we say—physical way. For this month, DexCom has given diaTribe a $500 credit for DexCom merchandise, which we will give to one lucky reader! Visit www.diatribe.us/dexcomgiveaway to enter the drawing. Like all of our giveaways, this is open to non-readers as well—help us spread the word about CGM.
Yours truly,
Kelly L. Close
To get your free subscription to diaTribe, visit www.diaTribe.us.
www.diaTribe.us
ILLU
ST
RA
TIO
N: D
AN
IEL
BE
LKIN
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
2
diaTribe staffEditor in ChiefKelly L. Close
Managing EditorsKaku ArmahBrendan Milliner
Senior Advisor James S. Hirsch Contributors Daniel BelkinEric ChangJenny LesserDana LewisLisa RotensteinTony ShengMark SorrentinoKerri Morrone SparlingJessica SwienckowskiSanjay TrehanEllen UllmanNick WilkieMark Yarchoan
diaTribeadvisory board
Dr. Richard Bergenstal, MD Jennifer Block, RN, CDEDr. Zachary Bloomgarden, MDDr. Bruce Bode, MDDr. Nancy Bohannon, MDDr. Bruce Buckingham, MDDr. Wendell Cheatham, MD Dr. Steven Edelman Dr. Satish Garg, MD Dr. Barry Ginsberg, MD, PhDJeff HalpernDr. Lutz Heinemann Debbie Hinnen, CDEDr. Irl Hirsch, MDJeff HitchcockDr. Lois Jovanovic, MDDr. David Kendall, MDDr. Aaron Kowalski, PhDDr. Harold Lebovitz, MD, PhDLinda Parks, CDEDr. William H. Polonsky, PhDMichael RobintonDr. Francesco Rubino, MDGary Scheiner, MS, CDEJane Jeffrie Seley, NP, CDEDr. Jay Skyler, MD Dr. Paul Strumph, MD Dr. William Tamborlane, MDVirginia Valentine, CDEDr. Howard Wolpert, MDGloria Yee, RN, CDEDr. Paul Zimmet, MD, PhD Dr. Bernard Zinman, MD Dr. Howard C. Zisser, MD
quotable quotesLantus and cancer“The recent reports from Europe regarding Lantus being associated with cancer does not represent anything close to a proper scientific analysis. The data was very confusing, unexplainable, not consistent and far from anything that should change the way we currently use any type of insulin. Stay focused on the most important issues with your health: blood sugar levels as close to goal as you can avoiding hypoglycemia and get your blood pressure and cholesterol levels in the correct range.”
- Steve Edelman, MD (UCSD, San Diego, CA) speaking about a recent study calling into question the safety of Lantus long-acting insulin.
Dealing with diabetes and obesity“When you are dancing with a bear, you can’t get tired and sit down. You have to wait for the bear to get tired and sit down. Obesity and diabetes are our bears of today.”
- Minnie Joycelyn Elders, MD (University of Arkansas College of Medicine, Little Rock, AR), a former US Surgeon General, discussing healthcare disparities at the AACE meeting in May, 2009.
Pointing the way with CGM“Often the most successful patients with CGM are those who view the device as a compass rather than as a GPS.”
- William H. Polonsky, PhD (Behavioral Diabetes Institute, San Diego, CA) at the 2009 American Diabetes Association (ADA) meeting, discussing the psychological aspects of continuous glucose monitoring.
fingersticks

www.diaTribe.us
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
3
logbook Sonia, the White House, and MeT1/2
By James S. Hirsch
I had never heard of Sonia Sotomayor when my brother called me and said President Obama might need our help with his next Supreme Court nominee.
My brother is Dr. Irl Hirsch, Professor of Medicine at the University of Washington in Seattle, who is one of America’s leading diabetologists. He called me in early May to tell me that he had received a call from Sonia
Sotomayor’s doctor, who had a request. It appeared that the judge, who serves on the U.S. Court of Appeals, was on the short list of nominees to replace U.S. Supreme Court Justice David Souter.
Sotomayor’s doctor told my brother that the judge has had type 1 diabetes since she was a child and that she was in excellent health. However – if she were nominated – the White House was concerned that her medical condition might be used by opponents to under-mine her confirmation. So the White House had asked him a favor: find a highly respect-ed physician who could write an op-ed defending her.
In theory, an attack against Sotomayor would go like this: a Supreme Court justice has lifetime tenure, but how much “life” would this diabetic justice actually have to give, and would she be able to handle the physical demands of working on the nation’s highest court? Even if her adversaries didn’t believe those were legitimate issues, they could use them in a quiet smear campaign against her.
Sotomayor’s doctor thought that my brother had the credentials to answer those charges. The op-ed’s purpose would not be to defend Sotomayor per se, but to explain how the improvements in diabetes care have allowed patients to live and thrive just as they would without diabetes; how the disease should not be a limiting factor in anyone’s professional aspirations; and how it should be a non-issue in the consideration for a Supreme Court nominee. The White House told Sotomayor’s doctor that it would place the op-ed in a mainstream publication.
This is where I come in.
My brother told Sotomayor’s doctor that he would be willing to write such an op-ed, but he asked if he could co-write it with me. Irl has published many articles, but mostly in medical journals, while I’ve written a book for lay readers about diabetes, “Cheating Des-tiny,” and of course I write for diaTribe. As I said, I had never even heard of Sotomayor until my brother called me with the back story, but I was happy to help out. Sotomayor’s doctor said he had no objections to a co-author, so my brother and I waited for President Obama’s decision on the nominee.
When he announced it on May 26, Irl and I quickly began preparing the op-ed and had it written in 48 hours. We described why improvements in diabetes care should make the disease moot in determining the qualifications of a well-controlled patient, and we wrote that Sotomayor’s diabetes makes her nomination a true medical milestone.
Irl and I submitted the article to Sotomayor’s doctor, who forwarded it to his contact at the White House.
Even if Sonia
Sotomayor’s adversaries
didn’t believe that
diabetes was a
legitimate issue, they
could use it in a quiet
smear campaign
against her.
www.diaTribe.us
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
4
Then a funny thing happened. There was no response from the White House. No calls, no emails, nothing. Our hard work went there and died. The powers that be apparently didn’t need an op-ed defending their nominee against attacks on her health.
Which was actually a very good thing.
For all the medical progress that my brother and I discussed, perhaps the most important sign of progress has been that Sotomayor’s diabetes has created so few stirs. It’s received considerable attention, of course, and is central to her biography – how at age 8, her di-agnosis redirected her ambitions: she had wanted to be a private eye, like her hero Nancy Drew, but her doctor told her that was no longer possible, so she pursued more academic interests, which eventually led her to the law. President Obama deftly turned her diabetes into an asset – her ability to overcome it, to manage it, is another sign of her strength of character.
Some right-wing bloggers cited the judge’s diabetes either as a liability or made coarse remarks about her health. But those comments had no traction. The New York Times and other papers published stories confirming that Sotomayor’s diabetes, as long as it is under control, should not affect her duties on the bench. No U.S. Senator is dumb enough to attack a judicial appointment for a medical condition, particularly one as prevalent as dia-betes. Republicans realized from the outset that if they were going to block Sotomayor’s path to the Supreme Court, they would have to find something more substantial than her faulty pancreas.
But does her diabetes matter in how she would perform her duties as a justice? Ironically, I think the answer is yes, but in a good way.
President Obama noted that one quality he wanted in his nominee was “empathy” – the ability to understand the plight of others. This, however, was scorned by the opposition. Conservatives pine for “strict constructionists” – judges who impassively apply the law, who segregate their own feelings so their decisions carry a platonic sheen of objectivity. In this scenario, personal experience distorts perceptions, creates biases, and taints the quest for truth. Judges should not feel your pain. They should apply the law. Empathy is bad.
But if this were indeed true, we could just create a computer program with some sort of judicial algorithm: feed it the facts of the case, apply the laws, push a few buttons, and the computer would spit out the correct decision. But we don’t do that, of course. We under-stand that judges will be guided by laws and precedents but also by their own experience and sensibilities.
In this sense, Sotomayor’s health is a fascinating question – how has her experience as a lifelong diabetic shaped her own view of the world, and how might that affect her deci-sions on the court?
We can only speculate, but I do know this: she was dealt a bad hand early in her life. So too has every other child diagnosed with type 1 diabetes. To succeed in those circumstanc-es requires a certain mindset. You cannot feel sorry for yourself. You cannot blame others. You cannot play the victim. Rather, you have to accept responsibility, be dedicated, and know that your body will hold you accountable for every decision you make.Chances are, you will not feel pity for those with petty complaints. You know the differ-ence between a real grievance and a flimsy one.
For all the medical
progress that my
brother and I discussed,
perhaps the most
important sign of
progress has been that
Sotomayor’s diabetes
has created so few
stirs.
www.diaTribe.us
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
5
Because Sotomayor is a liberal Latina who grew up amid poverty in the South Bronx, she was assumed to be a soft touch on discrimination claims. Claims by minorities, women, gays, whomever – she would take their side because she finds common ground with the underdog.
So many were surprised when Tom Goldstein, in his SCOTUSblog (SCOTUS stands for Supreme Court of the United States), found that in the 96 race-related cases she decided while on the court of appeals, she had voted to reject discrimination claims 78 times while she upheld the claims 10 times. In other words, she rarely sided with those who presented themselves as victims.
Didn’t surprise me one bit. Sotomayor’s empathy is her asset. She knows what it means to be a victim and will not find common ground with pseudo victims. She knows quite well what it means to be betrayed for reasons beyond one’s control.
Assuming she is confirmed for the Supreme Court, her triumph will be America’s tri-umph. I have no idea what kind of judge she’ll be, but if you come to her with a grievance, you better have a damn good case.
Test Drive The Second-Generation OmniPod PDMT1/2
by Kelly Close
In the Test Drive section of diaTribe issue #4, I wrote about my experience with the first generation OmniPod. I called it “one of the best products that has come along in a decade” for two main reasons. First, for me, there is less hassle with disposable pump-ing and it’s much smaller than traditional pumps. As a tubeless insulin pump, it allows an added level of discretion since the insulin reservoir is tucked away into a pod that automatically inserts the cannula sits on your body without the need for an infusion set. No one sees it. The pod wirelessly communicates to a Personal Diabetes Manager (PDM; looks a lot like a BlackBerry), which is the control center for giving insulin instructions and also doubles as a blood glucose meter, a food database, and a logbook. This brings me to the crux of this issue’s Test Drive: the new OmniPod PDM released in June 2009.
The two biggest changes to the OmniPod PDM have to do with how the device looks and downloading information from the device. I’ll start with the first.
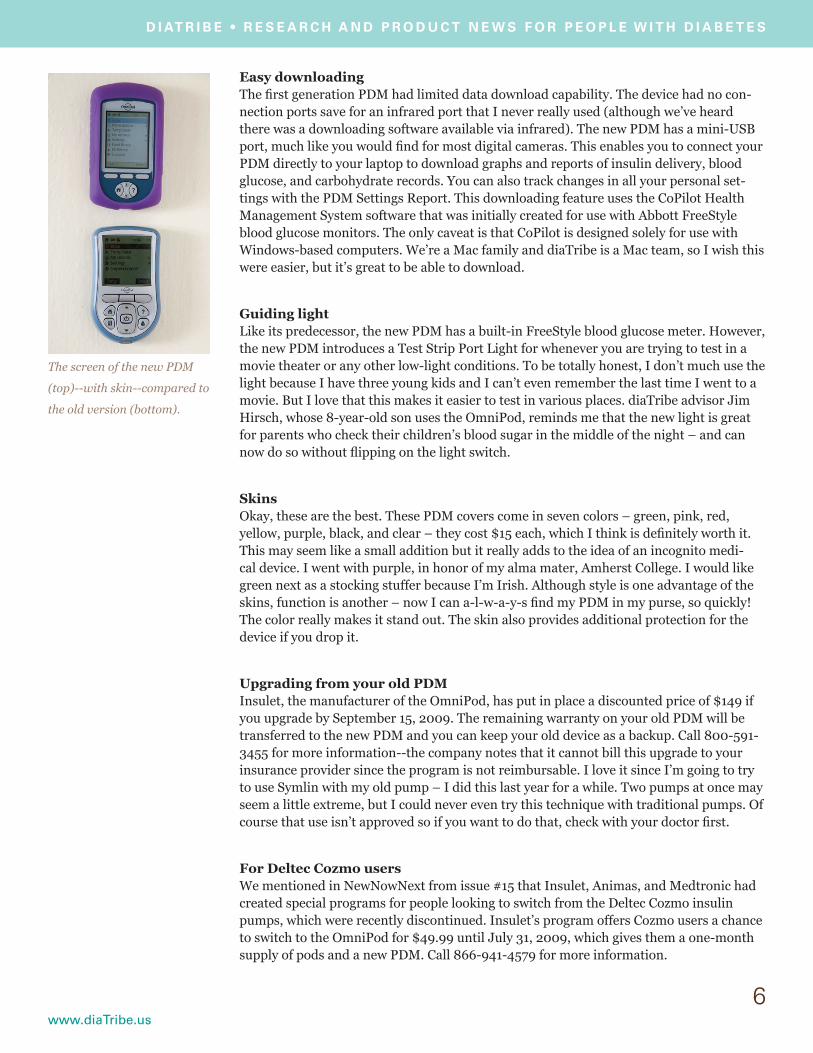
Smaller, sleeker, and more color The side-by-side pictures of the first generation PDM next to the newer one (model UST200) don’t necessarily give you the best sense of the improvements made to the de-vice. Overall, the PDM looks and feels much sleeker than the older version and the screen is considerably larger in the newer version. The new PDM is thinner and less bulbous than its predecessor, and while it isn’t that much smaller than the old version, the streamlined shape makes it feel far more compact. I was really taken by the crisp color on-screen, a marked improvement over the often difficult-to-read previous version, which had black text over a blue backlight. And, very cool, the command buttons have all been reworked to be smaller and more intuitive as a navigation tool. Overall, the new PDM is still not quite at iPhone level but it’s moving in the right direction.
5
Sotomayor’s empathy
is her asset. She knows
quite well what it
means to be betrayed
for reasons beyond
one’s control.
An edge-on view of the new
OmniPod PDM (left) next to
the old.
www.diaTribe.us
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
6
Easy downloadingThe first generation PDM had limited data download capability. The device had no con-nection ports save for an infrared port that I never really used (although we’ve heard there was a downloading software available via infrared). The new PDM has a mini-USB port, much like you would find for most digital cameras. This enables you to connect your PDM directly to your laptop to download graphs and reports of insulin delivery, blood glucose, and carbohydrate records. You can also track changes in all your personal set-tings with the PDM Settings Report. This downloading feature uses the CoPilot Health Management System software that was initially created for use with Abbott FreeStyle blood glucose monitors. The only caveat is that CoPilot is designed solely for use with Windows-based computers. We’re a Mac family and diaTribe is a Mac team, so I wish this were easier, but it’s great to be able to download.
Guiding lightLike its predecessor, the new PDM has a built-in FreeStyle blood glucose meter. However, the new PDM introduces a Test Strip Port Light for whenever you are trying to test in a movie theater or any other low-light conditions. To be totally honest, I don’t much use the light because I have three young kids and I can’t even remember the last time I went to a movie. But I love that this makes it easier to test in various places. diaTribe advisor Jim Hirsch, whose 8-year-old son uses the OmniPod, reminds me that the new light is great for parents who check their children’s blood sugar in the middle of the night – and can now do so without flipping on the light switch.
SkinsOkay, these are the best. These PDM covers come in seven colors – green, pink, red, yellow, purple, black, and clear – they cost $15 each, which I think is definitely worth it. This may seem like a small addition but it really adds to the idea of an incognito medi-cal device. I went with purple, in honor of my alma mater, Amherst College. I would like green next as a stocking stuffer because I’m Irish. Although style is one advantage of the skins, function is another – now I can a-l-w-a-y-s find my PDM in my purse, so quickly! The color really makes it stand out. The skin also provides additional protection for the device if you drop it.
Upgrading from your old PDMInsulet, the manufacturer of the OmniPod, has put in place a discounted price of $149 if you upgrade by September 15, 2009. The remaining warranty on your old PDM will be transferred to the new PDM and you can keep your old device as a backup. Call 800-591-3455 for more information--the company notes that it cannot bill this upgrade to your insurance provider since the program is not reimbursable. I love it since I’m going to try to use Symlin with my old pump – I did this last year for a while. Two pumps at once may seem a little extreme, but I could never even try this technique with traditional pumps. Of course that use isn’t approved so if you want to do that, check with your doctor first.
For Deltec Cozmo usersWe mentioned in NewNowNext from issue #15 that Insulet, Animas, and Medtronic had created special programs for people looking to switch from the Deltec Cozmo insulin pumps, which were recently discontinued. Insulet’s program offers Cozmo users a chance to switch to the OmniPod for $49.99 until July 31, 2009, which gives them a one-month supply of pods and a new PDM. Call 866-941-4579 for more information.
The screen of the new PDM
(top)--with skin--compared to
the old version (bottom).

www.diaTribe.us
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
7
Final thoughtsThe changes made to the new PDM are predominantly external and help to make me feel like my OmniPod is more of a consumer device (like a phone or camera) and less like a medical device. This is important since my insulin pump is a long-term investment and should blend in with my everyday life as much as possible. I still think that the PDM (and even the insulin pods themselves) can be made less obtrusive and the downloading and use of graphs and reports could be even simpler still. While I love that downloads can give me access to my insulin, meal, and blood glucose data, I cannot honestly say I devote 30 minutes every Sunday looking over graphs from the previous week. I can say, however, that it is going to be easier to show my endocrinologist what has been going on with my diabetes management – I look forward to using her PC to download my charts!
Some ask if it is really worth it having a tubeless pump. I can honestly say I’ve loved all my pumps (I’ve worn one for over a decade) and that I’d never be able to go back to a traditional one with tubing. I have found “no tubing” incredibly liberating. But everyone’s mileage varies – that is just me! If you’re in the market for a pump, check out disposable.
learning curve Inside Drug DevelopmentT1/2
by Brendan Milliner and Lisa Rotenstein
In diaTribe, we sometimes talk about drugs that are “not yet approved”, “at the FDA” or “in the regulatory process”. Some recent approvals of diabetes drugs in the US have stirred some controversy, and we think it’s important for our readers to understand the basics of how drugs are discovered and approved. In this issue of Learning Curve, we’ll take you through the development and regulatory process for drugs. As an example, we’ll be following a recently approved diabetes drug called Cycloset, which acts on the brain to help improve blood sugar (see this issue’s NewNowNext for more detail) – this drug, made by a company called VeroScience, actually spent TEN years at FDA before it was approved. This is a timely topic, because there are a number of drugs currently before the FDA in the US and other regulatory agencies globally – just to name a few, liraglutide, exenatide once-weekly, saxagliptin, alogliptin, and Afresa inhaled insulin are all at the FDA now, waiting for a decision.
PreclinicalMany older drugs were discovered by surprise, when somebody realized accidentally that a substance had a therapeutic effect. Today, most diabetes drug development follows a more linear track. First, researchers identify a “target” – something in the body that if acted on will have a positive effect. Next, the pharmaceutical industry works to develop a drug – usually a compound that is made by chemists, but sometimes a “biologic” that is made by living cells – that will act on this target.
Before this new drug can be evaluated in people, it must first be tested for safety and ef-fectiveness in test tubes and in animals. These non-human studies are termed preclinical studies. The kinds of cells or animals used for these trials varies depending on the type of compound used, how it will be administered (as an injection, a pill, etc.), and which part of the body it is designed to affect. Many trials of diabetes medications are done in mice, which can be genetically manipulated to show symptoms of the disease being studied and are easy to care for, and primates, which are biologically much more similar to humans.
The changes made
to the new PDM are
predominantly external
and help to make me
feel like my OmniPod
is more of a consumer
device (like a phone or
camera) and less like a
medical device.
IMA
GE
FR
OM
WW
W.S
CIE
NC
ED
AIL
Y.C
OM
www.diaTribe.us
The types of preclinical trials conducted with animals can vary quite a bit as well, but the primary goal is to establish that the drug is both effective enough to warrant human study and safe enough that human volunteers won’t be putting themselves in serious danger. Studies in animals also test to make sure the compound won’t cause cancer or mutations, or damage an embryo or fetus. By giving animals such as mice very high concentrations of a potential drug, researchers can find the limits of safety so that they don’t accidentally give a dangerous dose to a human subject.
Mouse models are also often used to simulate human diseases. As an example, in one of the animal trials during the development of Cycloset, researchers gave the drug to mice that were genetically modified to be obese, and then monitored their weight, body compo-sition, and the concentrations of sugar and other substances in their blood. The abstract of this trial is available at www.tinyurl.com/ntf6x5.
Clinical trialsClinical trials (studies in human volunteers) for a particular drug are initiated after all laboratory and animal work has been completed and the data has been presented to the regulatory bodies for assessment. Clinical trials are designed to assess the safety, efficacy, and action of a drug in human subjects. Each clinical trial phase asks a different question about the drug.
Phase 1 trialsA phase 1 trial is the first stage of testing of a drug in people. There are usually two of these trials and they generally involve small groups of healthy people without diabetes (usually 20-80 individuals). They explore what dose of a drug should be given by look-ing at the safety of different doses. Most of the work is done in a hospital or clinic while health professionals assess the drug’s tolerability and mechanism of action in patients (including the speed of action and the drug’s interactions with other substances in the body). The first studies start with a single dose of drug; subsequent studies are called multiple dose studies. Volunteers may dose for a period of hours to a couple weeks, depending on the drug. Typically a company can establish a range of doses that are per-ceived to be sufficiently safe and tolerable for further testing.
Phase 2 trialsPhase 2 trials typically have larger groups of participants (100-300 individuals), and these people usually have the disease the drug is intended to treat. They look to see how well the drug works for its specified purpose, and data are still collected about its safety. This is the first time the company sees whether the drug works as planned, but also the first time when a drug can fail based on a lack of efficacy.
This type of trial examines several potential doses of the drug within the range identified in phase 1 to determine at which dose levels the drug is efficacious. These trials are still usually held in a limited number of locations. For Cycloset, phase 2 trials determined that the best dose is around 1.6 mg per day, with a maximum of 4.8 mg per day. The studies showed that patients should take the drug in the morning and before meals for a maxi-mum effect, and that they can increase the number of tablets gradually if they don’t see an effect at first—up to the maximum of 4.8 mg.
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
8
Clinical trials are
designed to assess
the safety, efficacy,
and action of a drug in
human subjects. Each
clinical trial phase asks
a different question
about the drug.
www.diaTribe.us
9
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
Phase 3 trialsThis phase of testing is usually much larger than the other two phases—typically, several thousand patients will be enrolled. Phase 3 trials help to provide large-scale efficacy and side effect data so that researchers can understand how best to use the drug. They help to make sure that the drug works in a range of different patients, and doesn’t cause rare side effects that might have been missed in smaller trials.
Typically there are at least two phase 3 trials with similar endpoints, so that research-ers can prove that the effects and safety findings weren’t just a function of chance, and that the effects can be repeated. These trials are large, expensive, and are the last hurdle before sending the drug’s information to the FDA for approval.
Often as these studies are being conducted, additional phase 1 studies looking at drug interactions (with commonly used medications) or in special populations (those over age 65 or those with kidney disease and/or cardiovascular disease) are conducted as well for an even greater understanding of the effects of the drug across all relevant groups of potential users. For example, many people with type 2 diabetes are over 65, take several other medications for their cholesterol or blood pressure, and may have some decrease in kidney function – it is important to know how these patients will do with a new drug for diabetes.
VeroScience conducted a phase 3 trial comparing the adverse events in patients receiving Cycloset with those receiving a placebo, and continued to look at whether Cycloset effec-tively lowered blood glucose and A1c. The phase 3 trial included 3,000 people with type 2 diabetes over two years. It allowed VeroScience to be able to label its drug and report observed side effects to the FDA—nausea, fatigue, vomiting, etc. Other serious adverse effects weren’t seen with Cycloset use in this trial.
Submission and approvalUpon completion of phase 3 trials, the company must submit a New Drug Application (or NDA) to the FDA. The NDA contains information from the entire development program of the compound (preclinical and clinical), and also includes information on plans for manufacturing and marketing the drug to consumers. The company then waits for the FDA to reach a decision on whether the drug is marketable. After the FDA has accepted a filing, it sets a “PDUFA date”, which is the time by which the FDA must reach a decision. The review process may take a year or longer (as is currently the case, especially in dia-betes, although Cycloset’s ten years at the FDA was extreme), and additional studies are sometimes required to further convince the FDA of the safety or efficacy of a candidate drug.
Typically, the FDA will convene a panel of experts to advise it based on a more detailed analysis of the data (this panel is called an Advisory Committee). During a one-day meet-ing, the Committee is asked to debate specific questions put forward by the FDA and then give its final opinion by a vote. The FDA is not required to follow the recommendations of the Advisory Committee, but it usually does. See NewNowNext in diaTribe issue 15 for our coverage of the Advisory Committees for two diabetes drugs that haven’t yet been ap-proved as of press time: saxagliptin and liraglutide.
If a drug is approved by the FDA, the sponsoring company may begin to sell the drug and advertise to consumers and health care professionals. In many cases, the company may be asked to conduct additional large-scale trials of the drug once it is already on the
9
© M
IKE
BA
NN
ON
WW
W.M
OR
DA
NT
OR
AN
GE
.CO
M
Typically, the FDA
will convene a panel
of experts to advise
it based on a more
detailed analysis of the
data (this panel is called
an Advisory Committee).
www.diaTribe.us
10
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
market—these are known as post-marketing trials. Cycloset was just approved by the FDA in May 2009, and its sponsoring company VeroScience was able to begin marketing at this year’s ADA meeting. Notably, regulatory processes must take place in every single country or region in which a company wants to sell a drug.
The approval process for diabetes drugs has become more complicated since the FDA released new guidance intended to reduce the risk of cardiovascular (CV) side effects from diabetes drugs. This new guidance is in addition to the previous FDA requirements. To rule out CV effects, a drug must be given to a large number of people over a long period of time (often many years), and this type of trial can be expensive and difficult for drug companies to complete before the drug is approved and making money. There has been a great deal of controversy surrounding this issue in the diabetes community, because of fears that the new restrictions will make companies less willing to develop new diabetes drugs that could be helpful for patients. You can visit www.diatribe.us/fdaletter.pdf to see the advice given to companies by the FDA. Particularly following new data given at this year’s ADA, we think the requirement for pre-approval screening is not necessary and may delay innovative new treatments for people with diabetes.
How can I enroll in a clinical trial?Enrolling in a clinical trial is often a good way to explore new therapies and gain access to cutting-edge medications that haven’t yet been approved by the FDA. It is also often a great way to learn more about your disease. Everyone that participates in a clinical trial will go through an informed consent process, and will hear about all the known risks and benefits and everything that will be involved in their participation. They can then choose whether or not to participate. Most clinical trials are blinded and randomized, which means you won’t know whether you are on the test medication, a comparator drug, or a placebo “dummy pill.” It is important to know that you and the doctor won’t have any say in the treatment that each individual participant receives--treatment groups are random-ly assigned, and neither you nor your doctor will know. This helps with reducing bias in trials, but is important to know before you participate. At the same time, clinical trials are just that—trials—and so not all questions about these drugs have been answered.One way to get involved with a trial is to ask your doctor—many doctors are part of trials or lead trials themselves. You can also go to several websites to see if you’d qualify for any trials or some of the drugs being tested might meet your needs:
The American Diabetes Association trials website: http://www.diabetes.org/diabetes-research/clinical-trials/trials-home.jsp
Federal government trials websites:
Type 1 Diabetes:• http://clinicaltrials.gov/ct2/results?term=Type+1+Diabetes
Type 2 Diabetes : http://clinicaltrials.gov/ct2/results?term=Type+2+Diabetes •
General Clinical Trial Info: http://clinicaltrials.gov/ct2/info/understand•
How to find out about or report drug side effectsThe FDA plays an important role in monitoring the safety of drugs even after they get to market, and as a member of the public you have access to FDA safety warnings. Also, you can do your part in informing others by reporting side effects that you experience while on a medication. Both the FDA safety warnings and the reporting system can be accessed through MedWatch at http://www.fda.gov/Safety/MedWatch/default.htm.
Enrolling in a clinical
trial is often a good
way to explore new
therapies and gain
access to cutting-
edge medications
that haven’t yet been
approved by the FDA.
It is also often a great
way to learn more
about your disease.
www.diaTribe.us
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
11
conference pearls ADA 2009T1/2
The diaTribe team just got back from the 2009 ADA Scientific Sessions in New Orleans, and (in between meals of crayfish and jambalaya) we’ve seen some very exciting new developments. The conference was huge this year — about 12,000 people attended (though that fell from about 20,000 last year, probably due to the economy and the fact that everyone likes diaTribe’s hometown, San Francisco) — and was packed with presentations and research posters on every topic relating to diabetes that you could imagine. We’ve focused on several of the most important results from the patient perspective: the one-year results of the JDRF continuous glucose monitoring trial and overviews of new therapies in development for type 1 and type 2 diabetes.
The JDRF CGM trial after one yearIn our report about the 2008 EASD (European Association for the Study of Diabetes) meeting in diaTribe issue 12, we talked about the results of a trial by the Juvenile Diabe-tes Research Foundation (JDRF) trial that investigated the efficacy of continuous glucose monitoring over a period of six months. At this year’s ADA, the JDRF released new one-year results that (happily!) confirmed the benefits of CGM use.
The results of the original trial showed that CGM can help patients improve their blood sugar control. Adults with a starting A1c of ≥ 7% using CGM lowered their A1c by an aver-age of 0.5%. In children and teenagers, there was no significant difference in A1c with CGM use, although there was a trend toward an A1c decrease in children. Those subjects with starting A1cs < 7% were able to maintain a low A1c with CGM use.
The new findings presented at ADA showed that the CGM benefits for adults were sus-tained over one year, and showed for the first time that children with starting A1cs over 7% were able to reduce their A1c with CGM. Even more importantly, rates of hypoglyce-mia continued to fall with CGM use—so much so that both the adults and children in the less than 7% A1c group had NO severe hypoglycemia during the second half of the trial! The second half also confirmed an important message from the first six months of the trial: in all age groups, the people who got an A1c benefit from CGM were the ones who used it more frequently. These results show quite persuasively that CGM can be useful to help people improve their control, and should help encourage reimbursement and greater CGM use in people with diabetes of all ages. If you decide to invest in a CGM device, and you commit yourself to using it frequently and making changes based on the results, you will be able to improve your glucose control.
While the JDRF trial didn’t study people with type 2 diabetes, we’re confident that CGM can be useful in people with type 2 as well, particularly those who are taking insulin. We’ve seen increased interest in using the technology for type 2 from other diabetes experts as well—in our survey at the ADA meeting, 59% of health care providers said they would prescribe CGM to their type 2 patients if it were widely reimbursed!
Update on therapies for type 1There was LOTS of talk at the ADA about the artificial pancreas, and after hearing about it for so long, we think it’s finally getting close, thanks to all the amazing researchers! Dr. Bruce Buckingham of Stanford University gave an intriguing talk about how algorithms
ILLU
ST
RA
TIO
N: D
AN
IEL
BE
LKIN
At this year’s ADA, the
JDRF released new
one-year results that
(happily!) confirmed
the benefits of CGM
use.
www.diaTribe.us
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
can be used with insulin pumps and CGM to reduce nocturnal hypoglycemia. His artificial pancreas system uses a combination of five different algorithms to decide when hypo-glycemia is imminent, and then a computer automatically shuts off insulin delivery. In his studies, 84% of all nighttime hypoglycemic events were avoided with the algorithm. It’s a bit like Medtronic’s Low Glucose Suspend (see NewNowNext in issue 11), but more sophisticated in that it can look ahead to sense impending hypoglycemia instead of just reacting to low glucose levels. Presentations like this make us very excited about closed-loop research, which is proceeding faster than we could have imagined.
In drug-related news, we heard from Dr. Peter Gottlieb about an initial trial of Bayhill Therapeutics’ first-in-class DNA “vaccine” for type 1 diabetes, currently named BHT-3021. The drug works by making the immune system more tolerant to a person’s own insulin, preventing immune attack on beta cells and stopping the progression of type 1 diabetes. Initial results suggest that the drug is well tolerated and may help to preserve beta-cell function, but the effect may wear off over time. Bayhill recently entered into a collaboration with the drug company Genentech, which is great news, suggesting that the class might hold real promise. You can read conference pearls in diaTribe issue #15 for more information about diabetes vaccines—we’re cautiously optimistic about this ap-proach for those at high risk of type 1, and we’ll keep you up to date as more data become available.
Update on therapies for type 2Important type 2 research at this year’s ADA was plentiful, and we heard about plenty of things that people with type 2 should be aware of.
First, there were many studies about new entrants on the GLP-1 treatment front—while Amylin’s Byetta has long been the only player in this class, there are now many different therapies jockeying for a spot. The most near-term are Novo Nordisk’s liraglutide (Vic-toza), which is a GLP-1 agonist like Byetta, and Amylin’s exenatide once-weekly, a modi-fied form of Byetta that only has to be taken once per week. Liraglutide has faced some hurdles at the FDA (see NewNowNext in issue #15), but it seems to be moving forward very quickly in the EU. In terms of efficacy, liraglutide studies seem to show that the drug is more efficacious than the Byetta, but we haven’t yet seen any data comparing it to exenatide once-weekly. Drugs that reduce A1c, cause weight loss, and also are easy to take could be transformational, assuming that all the safety data hold.
The next new class of drugs to be approved by the FDA may be a type of drug called an SGLT-2 inhibitor, which works by preventing your kidneys from absorbing their normal amount of glucose and causing you to excrete excess glucose in your urine. So far, results have been fairly promising, showing that the drug reduces glucose levels and lowers weight without major side effects. We look forward to seeing more data to assess the class and learn what the experts really think.
Finally, we heard some interesting new results from a company called Xoma, which is developing a drug to treat the inflammatory processes (the bodies response to a foreign body) that underlie type 2 diabetes. The drug, called XOMA 052, inhibits an inflamma-tory chemical called IL-1beta that may be implicated in the decreased insulin secretion that occurs in advanced type 2 diabetes. Patients who were treated with a single dose of XOMA 052 saw a 1.0% A1c decrease that was sustained over a 90-day interval. Patients will eventually need to be treated again, but this drug is interesting to us because of its potential to dramatically simplify the treatment strategy for type 2 diabetes, and because it attacks the disease from a different angle than other therapies currently on the market.
12
The next new class of
drugs to be approved
for type 2 diabetes
may be something
called an SGLT-2
inhibitor, which
prevents your kidney
from absorbing normal
amounts of glucose.
www.diaTribe.us
Going forwardThe rest of this year is going to be exciting one for diabetes. Hopefully, we’ll see the intro-duction of new type 2 therapies like liraglutide and saxagliptin (Onglyza), and continued acceptance of CGM in both type 1 and type 2 populations. While we don’t see any dramat-ic changes in diabetes treatment soon, it’s this kind of continued progress that eventually makes a big difference in the lives of people with diabetes.
trial watch Oral Insulin for Prevention of Diabetes in Relatives at Risk for Type 1 Diabetes MellitusT1
ClinicalTrials.gov Identifier: NCT00419562 http://clinicaltrials.gov/ct2/show/NCT00419562
The face of type 1 diabetes has changed greatly in the last decades. We now know that type 1 diabetes is an autoimmune disorder: it results when the immune system mistaken-ly attacks the beta cells, the body’s natural source of insulin. Recent findings suggest that early administration of insulin by mouth, before the onset of the disease, may desensitize the overactive immune system to the presence of insulin – thereby preventing the devel-opment of diabetes.
This study – which received a plug in this year’s Banting Lecture, typically one of the most important talks at the ADA Scientific Sessions – examines the preventative effects of oral insulin in individuals at risk for developing type 1 diabetes. To be considered, par-ticipants must not have diabetes but be at high-risk for development – i.e., have a near relative who was diagnosed with type 1 diabetes before age 40 and started insulin therapy within one year of diagnosis. If the relative is a parent, sibling, or a child, participants must be three to 45 years old; if the relative is a niece, nephew, aunt, uncle, grandparent, cousin, or half-sibling, participants must be three to 20 years old. This study is recruiting at 36 locations worldwide (and chaired by diaTribe advisory board member Dr. Jay Skyler of the University of Miami!). To find a center near you, visit the link above and look under “Contacts and Locations.”
Targeting Inflammation Using Salsalate for Type 2 Diabetes-Stage II (TINSAL-T2D-II)T2
ClinicalTrials.gov Identifier: NCT00799643http://clinicaltrials.gov/ct2/show/NCT00799643
The mechanisms underlying type 2 diabetes are still not completely understood. While many possibilities have been proposed, mounting evidence indicates that chronic inflam-mation (a prolonged immune reaction involving the simultaneous healing and destruc-tion of cells) may play a role.
This study investigates whether a common anti-inflammatory agent, salsalate, can im-prove blood sugar control in patients with type 2 diabetes. While the trial is also examin-ing the safety of salsalate in type 2 patients, the drug has been widely used to treat arthri-tis and is in the non-steroidal anti-inflammatory drug (NSAID) class, which includes such everyday drugs as aspirin and ibuprofen.
To be considered for enrollment, subjects must be between the ages of 18 and 75 and have an A1c greater than 7.0% and less than 9.5%. They also must have been diagnosed with
13
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
www.diaTribe.us
type 2 diabetes at least eight weeks before screening. Subjects taking Avandia or Actos in the last six months or Byetta in the last three months may not apply. To enroll, contact [email protected].
Continuous Glucose Monitoring in Patients With Type 2 Diabetes (CGM)T2
ClinicalTrials.gov Identifier: NCT00529815http://clinicaltrials.gov/ct2/show/NCT00529815
It seems sometimes that diabetes devices and gadgets are mostly reserved for the type 1 population. However, a number of recent studies have suggested that reducing variability in blood glucose scores is beneficial for anyone with diabetes and can help reduce com-plications down the line – suggesting the use of continuous glucose monitoring (CGM), which provides a real-time output of blood glucose trends, may have value in this popula-tion. How excellent!
This study examines whether the additional use of CGM by subjects with type 2 diabetes improves their ability to control glucose levels as compared with standard finger sticking. Participants will use a DexCom CGM device for 12 weeks and be monitored for changes in A1c levels over a total of 52 weeks. To be considered, subjects must be between 18 and 80 years old and have an A1c between 7% and 12%. The trial is currently recruiting in the Washington, DC area – to enroll, contact [email protected] or call (202) 782-1492.
what we’re reading Look AHEAD – practical implications from an T1/2
intensive lifestyle interventionby Tony Sheng
Diet and exercise are usually the first therapies prescribed by health care practitioners for patients newly diagnosed with type 2 diabetes, but what sounds like simple and effective therapies have failed time and time again in the United States. For busy people with cluttered lives and a million things on their minds, allocating that extra hour a day to jog, those extra three hours a week to do groceries, and the extra money to pay for healthier foods—well, it’s just too much extra! Even for those who are determined to purge their bodies of junk food and defeat their sedentary lifestyles, behavioral change is hard to sustain. Some previous studies on diet and exercise interventions have demonstrated impressive improvements in weight and diabetes management but have been conducted in unrealistic settings (i.e., eating every meal at the study site). However, we’re encouraged by the results of a study called Look AHEAD (Action For Health in Diabetes), which suggest that diet and exercise can be an effective therapy for obesity and type 2 diabetes even without complicated study procedures.
The Look AHEAD trial was designed to see if and how a long-term intensive lifestyle intervention program would affect the risks of cardiovascular disease and death in obese patients with type 2 diabetes. Patients that took part in the intensive lifestyle interven-tion were given basic education about diabetes and were taught the importance of eat-ing a healthy diet and of being physically active. They were encouraged to lose 10% of their body weight, restrict their diets to around 1,500 calories a day, and to exercise 175
14
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
We’re encouraged
by the results of the
Look AHEAD study,
suggesting that diet
and exercise can be
an effective therapy
for obesity and type 2
diabetes
www.diaTribe.us
minutes per week. During the first year, participants were seen in clinic weekly with three weight-loss group meetings and one individual counseling session per month. In years two through four, a minimum of two contacts per month was expected.
Of the 5,145 patients in the massive trial, around 95% stayed on the program. Many behavioral studies have trouble retaining subjects in part because of unrealistic require-ments. Look AHEAD’s high retention rate speaks to the adoptability of the program.
More impressive were the improvements in weight, fitness, and cardiovascular risk fac-tors. Patients on the intensive intervention lost weight (8.6% of their body weight in the first year!), improved fitness, glycemic control, systolic blood pressure, and triglyceride levels. Not surprisingly, these patients also required fewer diabetes medications and insulin. Fewer medications needed means less medication purchased, which means less money spent by the patient! The study also showed that physical activity was the most significant factor in explaining the dramatic weight loss. In his talk at the ADA Scientific Sessions in New Orleans, Dr. Thomas A. Wadden of the University of Pennsylvania Medi-cal School suggested that the success of group treatments seen in the Look AHEAD study might be due to the support and competition in the group setting.
Look AHEAD presents what we already knew (that diet and exercise are important and effective diabetes and obesity therapies) and puts a practical twist on it. Many past stud-ies were controlled too tightly and created environments that could not be translated to the real world. Look AHEAD showed real improvements with at least three hours of exer-cise a week and only two or three meetings per month with a weight-loss. This trial shows that if you can educate yourself on healthy eating and exercise habits, set goals, and find a few other people to lose weight with you, you can (really!) lose weight and improve your diabetes.
Editor’s Note: As always, remember that diaTribe doesn’t give treatment advice. Al-ways consult your doctor before starting a new exercise or treatment program.
Insights from Look AHEAD:
Diabetes education is vitally important. • All participants in the intensive intervention program attended a one-hour diabetes education class that placed a special emphasis on hypoglycemia, cardiovascular disease symptoms, and foot care.
Setting high goals may help people to lose more weight. • Patients in the intensive intervention program set a goal of losing 10% of their body weight. Not everybody met this goal, but the average weight loss was over 8%! It’s the slow, incremental improvements that will add up and make a difference in the long run.
Proper diet is absolutely critical for weight loss.• It is important to control portions of food. Think of your stomach as a bathtub, and calories as water. Calo-ries you consume from food enter the tub, and any exercise you do drains the water out. If you don’t exercise enough, the tub will overflow. A constantly overflowing tub leads to obesity, type 2 diabetes, and cardiovascular problems. The diet rec-ommended for patients in the intensive intervention program was based on ADA guidelines and National Cholesterol Education programs and includes a maximum of 30% of total calories from total fat, a maximum of 10% of total calories from saturated fat, and a minimum of 15% of total calories from protein.
15
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
This trial shows that
if you can educate
yourself on healthy
eating and exercise
habits, set goals, and
find a few other people
to lose weight with
you, you can (really!)
lose weight and
improve your diabetes.
www.diaTribe.us
According to Dr. Wadden, exercise was the most important factor in • achieving weight loss in this study. Patients in the intensive intervention program were encouraged to exercise 175 minutes a week. This translates to 25 minutes a day. Start by taking walks after meals, and count any exercise that lasts longer than 10 minutes towards your goal.
There are benefits of a team approach to weight loss. • Dr. Wadden believes that the significant weight loss experienced in this trial might be due in part to the support and competition in the group meetings during the trial.
Quitting smoking improves cardiovascular health. • All individuals in the program that smoked were encouraged to stop smoking, and were provided with self-help materials and/or referrals to local programs. People with diabetes are al-ready two to three times more likely to die from cardiovascular events, and smoking just increases that risk!
NewNowNext Team Type 1 sets record, wins first place at 2009 Race Across AmericaT1
On June 26th, diabetes didn’t stop Team Type 1 from cruising to a record-setting victory in the 2009 eight-person Race Across America (RAAM, http://www.raceacros-samerica.org/). The team finished the 3,000 mile race—30% longer than the Tour de France!—from Oceanside, CA to Annapolis, MD in four days, 22 hours, and 32 minutes, all while managing their diabetes. Of the eight riders on the Team Type 1 RAAM team, six of them competed with the OmniPod, Insulet’s patch insulin pump.
The Team Type 1 RAAM team inspired the world with their record-setting victory in the 8-person division in 2007, and proves once again how people with type 1 diabetes can overcome the difficulties of diabetes to achieve incredible success. “Our team’s mission is to show people with diabetes that they can accomplish anything if they work hard to control their disease,” said Joe Eldridge, co-founder of Team Type 1. “We hope our team’s performance inspires other people to manage their diabetes so they can achieve their own goals.” Congrats to Team Type 1 for their average 23 mph speed!
JDRF Children’s Congress We recently attended the three-day JDRF Children’s Congress in Washington DC T1
(June 22-24, 2009). The goal of the 150 young delegates (ages 4-17 years, who all have type 1 diabetes) was to raise awareness about the disease and to remind legislators to consider the importance of diabetes in children. The Children’s Congress has been key in diabetes advocacy since it was founded 10 years ago.
One major highlight of the 2009 Children’s Congress arose when President Obama met with the 150 delegates on June 23rd on the White House portico. This was the first time a sitting President met with the delegates, and we thought it highlighted the new adminis-tration’s focus on healthcare. Rick Rosbach, one of the parents who attended with his son Ben (7), said it was an amazing experience and that he saw the “human face” of the President come out. President Obama was very personable with the children, he said, “even picking up one four year-old who was quite nervous” and putting him on his lap.
16
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
The victorious Team Type 1

www.diaTribe.us
The Congress ended with a Senate Hearing on, “Type 1 Diabetes Research -- Real Prog-ress and Real Hope for a Cure” at which many prominent figures spoke--Mary Tyler Moore (the JDRF International Chairman), Griffin P. Rodgers, MD (Director of the National Institute of Diabetes and Digestive and Kidney Diseases), “Sugar” Ray Leonard (an Olympic gold medal boxer), and singer-songwriter Nick Jonas. Senator Susan Col-lins (R-ME) gave a personal promise to the children in her closing remarks, saying, “I will remember you and I will do everything I can to advance the research that will lead to a cure.” Delegates met with their representatives at the end of the Congress to thank them for their support of diabetes research, asking them to vote for the renewal of the Special Diabetes Program ($150 million in funding). Happily, his main take away from the event was that “we are not alone.” To apply for the 2011 Congress, text ‘CC11’ to 56333.
Medicare Diabetes Screening Project Type 2 diabetes is finally being recognized on a national and federal level as a T2
major threat to the health of older individuals and a powerful force in driving up the costs of Medicare. Former Senate Majority Leader Tom Daschle recently met with experts on diabetes education and research along with representatives of senior-living communities to discuss the need to increase awareness of free Medicare diabetes screen-ing in the aging population. Despite the availability of free testing, reportedly less than 10% of Medicare beneficiaries are tested for diabetes each year.
The Medicare Diabetes Screening Project (MDSP), supported by Novo Nordisk, is helping to change that. A new alliance between the MDSP and the National Council on Aging is promoting the launch of a new outreach program called “Diabetes Screening: Medicare Benefits for Better Health.” The new project is designed to equip leaders of organizations, agencies, and companies that serve seniors with the tools to better educate the aging population about Medicare benefits for diabetes screening. We hope this project takes off and more seniors are able to take advantage of the free screening available.
If someone you know is over the age of 65, covered by Medicare, and has at least one diabetes risk factor (high blood pressure, high cholesterol, overweight, history of high glu-cose, history of gestational diabetes, or family history of diabetes), please encourage them to ask their health care provider for a free diabetes screening. You can find more informa-tion at http://www.screenfordiabetes.org/.
Cycloset approved by FDA In early May, a drug called Cycloset (also known as bromocriptine) was approved T2
by the FDA for use in type 2 diabetes. Cycloset, developed by VeroScience, works in the brain to simulate the action of a chemical called dopamine. It is the first drug in its class approved for the treatment of diabetes and (even more exciting for us!) the first drug approved under the FDA’s new cardiovascular guidelines.
The concept for the drug originated after scientists at VeroScience noticed that, while ani-mals become obese and insulin resistant during annual periods of hibernation or migra-tion, they automatically revert back to a non-obese non-insulin resistant state when the next season arrives with no apparent side effects. After a careful analysis of brain signals from hibernating and non-hibernating animals, VeroScience noticed a variation of dop-amine (a neurotransmitter) levels that might account for this prediabetes/non-diabetes transformation.
17
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S

www.diaTribe.us
Cycloset aims to take advantage of this brain chemistry by attempting to mimic mother nature in reversing diabetes. Cycloset is a once-daily therapy to be taken in the morning. It has been approved as a monotherapy (to be taken by itself) as well as with a sulfony-lurea or metformin. In phase 3 trials, Cycloset produced an A1c decrease of about 0.7% after 24 weeks, without any increase in serious side effects. We are impressed by its side effect profile and mechanism of action, and think it may be a good alternative treatment for some people with diabetes. You can go to www.cycloset.com for more information.
A1c as a diagnostic tool Most people with diabetes should be familiar with the term A1c—a measure of T2
the glycated hemoglobin in blood that gives an estimation of glycemic control over a period of several months. As red blood cells circulate, glucose present in the blood will stick to your red blood cells (a process called glycation). A1c testing is nothing new, but experts have begun thinking about using A1c as a way of diagnosing type 2 diabetes, something that until now could only be done with more difficult tests. The argument for using A1c is that it’s easier for patients, because it requires only a blood sample, and won’t change depending on what people eat or do in the days leading up to the test. If you already have diabetes, this isn’t going to change your management. Experts at ADA set 6.5% or above as the A1c threshold for diagnosing diabetes.
diaTribe dialogue Dr. George EisenbarthT1
For this issue, diaTribe had the opportunity to talk with Dr. George Eisenbarth, the recipient of the Banting Medal for diabetes research—the American Diabetes As-sociation’s highest honor. Dr. Eisenbarth’s research has laid the foundations for tar-geted treatment of type 1 diabetes. His Banting lecture was captivating—hundreds and hundreds of people packed the room, eagerly awaiting his words. Not very many of the medals have been given out for type 1 research in recent years, so we were pretty excited about this.
The most uplifting and promising part of his talk was that the “tipping point”—the ability to prevent type 1—is near. It all depends on a “trimolecular complex” discovered by Dr. Eisenbarth that explains the details of how a person’s immune system is respon-sible for starting down the disease path. The formation of this “trimolecular complex” involves the improper activation of the immune system’s ‘attack cells’ (T-cells). These attack cells activate pathways that destroy beta cells, the pancreatic cells that produce insulin. Ultimately, this leads to type 1 diabetes. Dr. Eisenbarth is now working on drugs that would prevent type 1 in mice and is looking to see if this all works the same way in humans.
In this interview, Dr. Eisenbarth discusses how his discoveries can move us towards preventing diabetes and what they mean for diagnosing and predicting the disease.
diaTribe: Thank you so much for being with us, Dr. Eisenbarth. We were thrilled to hear you deliver the Banting Lecture at this year’s ADA Meeting. What a thrill for people with type 1 that type 1 diabetes was the focus of the lecture. After so many years of hearing about a cure, it is wonderful to hear we really are getting much closer. Let’s hit the
18
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
www.diaTribe.us
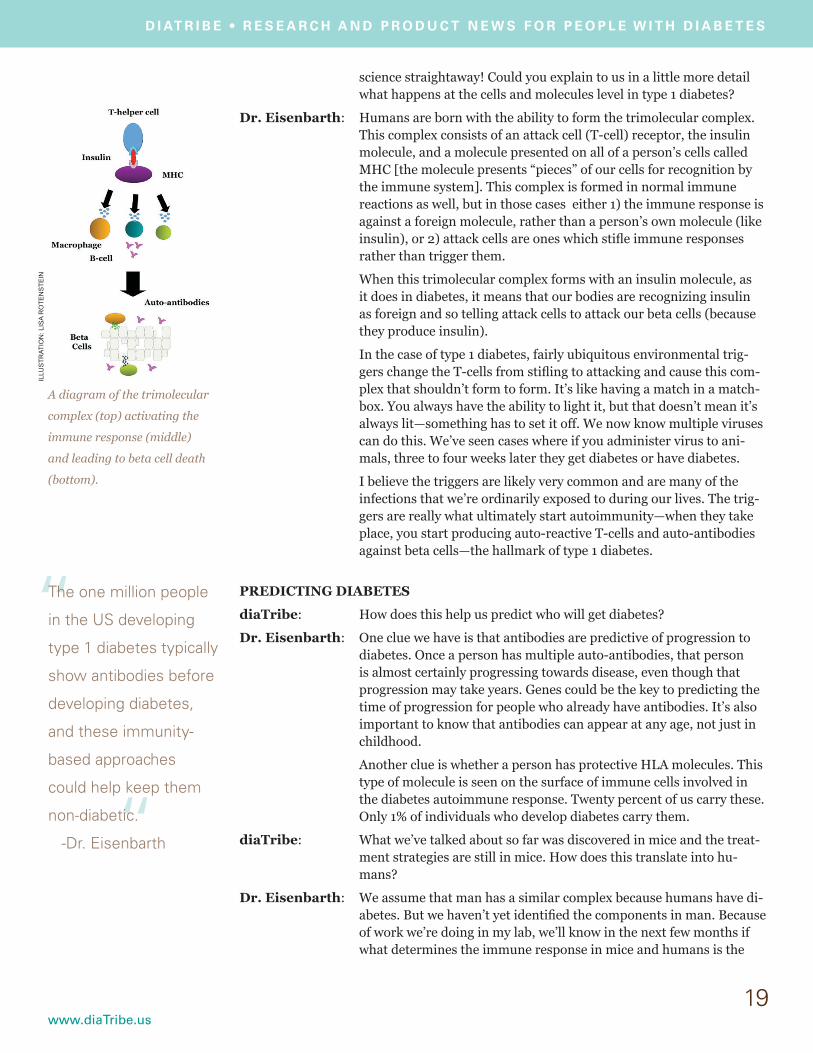
science straightaway! Could you explain to us in a little more detail what happens at the cells and molecules level in type 1 diabetes?
Dr. Eisenbarth: Humans are born with the ability to form the trimolecular complex. This complex consists of an attack cell (T-cell) receptor, the insulin molecule, and a molecule presented on all of a person’s cells called MHC [the molecule presents “pieces” of our cells for recognition by the immune system]. This complex is formed in normal immune reactions as well, but in those cases either 1) the immune response is against a foreign molecule, rather than a person’s own molecule (like insulin), or 2) attack cells are ones which stifle immune responses rather than trigger them.
When this trimolecular complex forms with an insulin molecule, as it does in diabetes, it means that our bodies are recognizing insulin as foreign and so telling attack cells to attack our beta cells (because they produce insulin).
In the case of type 1 diabetes, fairly ubiquitous environmental trig-gers change the T-cells from stifling to attacking and cause this com-plex that shouldn’t form to form. It’s like having a match in a match-box. You always have the ability to light it, but that doesn’t mean it’s always lit—something has to set it off. We now know multiple viruses can do this. We’ve seen cases where if you administer virus to ani-mals, three to four weeks later they get diabetes or have diabetes.
I believe the triggers are likely very common and are many of the infections that we’re ordinarily exposed to during our lives. The trig-gers are really what ultimately start autoimmunity—when they take place, you start producing auto-reactive T-cells and auto-antibodies against beta cells—the hallmark of type 1 diabetes.
PREDICTING DIABETES
diaTribe: How does this help us predict who will get diabetes?
Dr. Eisenbarth: One clue we have is that antibodies are predictive of progression to diabetes. Once a person has multiple auto-antibodies, that person is almost certainly progressing towards disease, even though that progression may take years. Genes could be the key to predicting the time of progression for people who already have antibodies. It’s also important to know that antibodies can appear at any age, not just in childhood.
Another clue is whether a person has protective HLA molecules. This type of molecule is seen on the surface of immune cells involved in the diabetes autoimmune response. Twenty percent of us carry these. Only 1% of individuals who develop diabetes carry them.
diaTribe: What we’ve talked about so far was discovered in mice and the treat-ment strategies are still in mice. How does this translate into hu-mans?
Dr. Eisenbarth: We assume that man has a similar complex because humans have di-abetes. But we haven’t yet identified the components in man. Because of work we’re doing in my lab, we’ll know in the next few months if what determines the immune response in mice and humans is the
19
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
“
“The one million people
in the US developing
type 1 diabetes typically
show antibodies before
developing diabetes,
and these immunity-
based approaches
could help keep them
non-diabetic.
-Dr. Eisenbarth
A diagram of the trimolecular
complex (top) activating the
immune response (middle)
and leading to beta cell death
(bottom).
ILLU
ST
RA
TIO
N: L
ISA
RO
TE
NS
TE
IN

www.diaTribe.us
same. [Once this is known, this will help with translating treatments designed for mice into humans].
PROSPECTS FOR TREATING TYPE 1 DIABETES
diaTribe: How does our new understanding of type 1 diabetes autoimmunity help us better treat the disease?
Dr. Eisenbarth: This knowledge gives us lots of new targeted options for treatment. The first approach involves blocking formation of the complex we’ve been talking about so that the autoimmune reaction never starts. We are working on creating small molecules that can do this.
“Vaccination” against the complex is another exciting choice. We are trying to generate antibodies to the complex so that the immune sys-tem knows to destroy it. We’re testing this concept in mice right now.
The one million people in the US developing type 1 diabetes typically show antibodies before developing diabetes, and so with these kinds of approaches, you could administer treatment to keep them non-diabetic [and prevent the disease].
diaTribe: What’s the outlook for people who have had diabetes for 25 or 30 years now that we have this insight?
Dr. Eisenbarth: None of the approaches I talked about would work in these patients. By this point, all of their beta cells would probably have been killed.
Nevertheless, we need to prevent the autoimmune killing for islet transplantation procedures or stem cell replacement of islets intend-ed to cure diabetes [otherwise islets or stem cells are destroyed by our bodies].
The approaches we’re talking about are all about prevention—spe-cifically about antibodies and T-cells. The antibodies are what cause diabetes’ effects. If we can prevent antibody formation or survival, we can help prevent beta-cell failure.
We thought Dr. Eisenbarth’s work and his Banting Lecture have huge implications for the field. What does it all mean? We hope that eventually, if a person presents with auto-antibodies, doctors will be able to treat them in a way that stops the progression of their diabetes and the death of their beta-cells. This will take time—time to translate mouse work to humans and time to develop new drugs. Maybe we’ll be able to identify the environmental triggers and have patients who are genetically susceptible to diabetes avoid them. And in the meantime—it makes us smarter and gives direction so we can be specific in designing therapies.
We’d also like to put in a plug for patients to get their antibodies checked if they’ve been recently diagnosed with type 1 or are first degree relatives of patients with type 1. TrialNet, at www.diabetestrialnet.org, is a wonderful resource that is conducting trials related to the prevention and early diagnosis of type 1 diabetes.
D I AT R I B E • R E S E A R C H A N D P R O D U C T N E W S F O R P E O P L E W I T H D I A B E T E S
diaTribe publishes information about diabetes products and research. This information is not a substitute for medical advice and should not be used to change treatment or therapy. diaTribe urges readers to consult with professional care providers in all matters relating to their health.
Why not subscribe for free to diaTribe? Receive the latest information from the cutting edge of diabetes research and product innovation. For more information, visit www.diaTribe.us
®
“
“The approaches we’re
talking about are all
about prevention—
specifically about
antibodies and T-cells.
The antibodies are
what cause diabetes’
effects. If we can
prevent antibody
formation or survival,
we can help prevent
beta-cell failure.
-Dr. Eisenbarth