is there any evidence for the validity of diagnostic ... · for accommodative and nonstrabismic...
TRANSCRIPT

J
R
If
P
a
b
RA
1h
ournal of Optometry (2014) 7, 2---21
www.journalofoptometry.org
EVIEW
s there any evidence for the validity of diagnostic criteria usedor accommodative and nonstrabismic binocular dysfunctions?
ilar Cacho-Martíneza,∗, Ángel García-Munoza, María Teresa Ruiz-Canterob
Departamento de Óptica, Farmacología y Anatomía, Universidad de Alicante, Alicante, SpainÁrea de Medicina Preventiva y Salud Pública, Universidad de Alicante, CIBERESP, Alicante, Spain
eceived 8 October 2012; accepted 21 December 2012vailable online 9 March 2013
KEYWORDSAccommodation,ocular;Diagnosis;Review literature astopic;Vision, binocular;Vision disorders
AbstractPurpose: To analyze the diagnostic criteria used in the scientific literature published in the past25 years for accommodative and nonstrabismic binocular dysfunctions and to explore if theepidemiological analysis of diagnostic validity has been used to propose which clinical criteriashould be used for diagnostic purposes.Methods: We carried out a systematic review of papers on accommodative and non-strabicbinocular disorders published from 1986 to 2012 analysing the MEDLINE, CINAHL, PsycINFO andFRANCIS databases. We admitted original articles about diagnosis of these anomalies in anypopulation. We identified 839 articles and 12 studies were included. The quality of includedarticles was assessed using the QUADAS-2 tool.Results: The review shows a wide range of clinical signs and cut-off points between authors.Only 3 studies (regarding accommodative anomalies) assessed diagnostic accuracy of clinicalsigns. Their results suggest using the accommodative amplitude and monocular accommodativefacility for diagnosing accommodative insufficiency and a high positive relative accommoda-tion for accommodative excess. The remaining 9 articles did not analyze diagnostic accuracy,assessing a diagnosis with the criteria the authors considered. We also found differencesbetween studies in the way of considering patients’ symptomatology. 3 studies of 12 analyzed,performed a validation of a symptom survey used for convergence insufficiency.Conclusions: Scientific literature reveals differences between authors according to diagnos-tic criteria for accommodative and nonstrabismic binocular dysfunctions. Diagnostic accuracystudies show that there is only certain evidence for accommodative conditions. For binocular
anomalies there is only evidence about a validated questionnaire for convergence insufficiencywith no data of diagnostic accuracy.ouncil of Optometry. Published by Elsevier España, S.L. All rights
© 2012 Spanish General C reserved.∗ Corresponding author at: Departamento de Óptica, Farmacología y Anatomía, Apartado 99, Universidad de Alicante, Alicante, Spain.E-mail address: [email protected] (P. Cacho-Martínez).
888-4296/$ – see front matter © 2012 Spanish General Council of Optometry. Published by Elsevier España, S.L. All rights reserved.ttp://dx.doi.org/10.1016/j.optom.2013.01.004

Evidence for the validity of diagnostic criteria for general binocular dysfunctions 3
PALABRAS CLAVEAcomodación, ocular;Diagnóstico;Revisión de laliteratura;Visión, binocular;Desórdenes de lavisión
¿Existe alguna evidencia en cuanto a la validez de los criterios diagnósticos utilizadospara las disfunciones acomodativas y binoculares no estrábicas?
ResumenObjetivo: Analizar los criterios diagnósticos utilizados en la literatura científica publicada enlos últimos 25 anos en relación a las disfunciones acomodativas y binoculares no estrábicas,así como explorar si se han utilizado los análisis epidemiológicos de validez diagnóstica paraproponer qué criterios clínicos deberían utilizarse a fines diagnósticos.Métodos: Llevamos a cabo una revisión sistemática de los artículos científicos sobre disfuncionesacomodativas y binoculares no estrábicas publicados desde 1986 a 2012, analizando las basesde datos de MEDLINE, CINAHL, PsycINFO y FRANCIS. Admitimos artículos originales acerca de losdiagnósticos de dichas anomalías en cualquier población. Identificamos 839 artículos e incluimos12 estudios. Se evaluó la calidad de los artículos incluidos utilizando la herramienta QUADAS-2.Resultados: La revisión mostró una amplia gama de signos clínicos y sus puntos de corte diag-nósticos entre autores. Únicamente 3 estudios (relativos a anomalías acomodativas) abordaronla exactitud diagnóstica de los signos clínicos. Sus resultados sugieren el uso de la amplitudde acomodación y la flexibilidad acomodativa binocular para el diagnóstico de la insuficien-cia acomodativa y una alta acomodación relativa positiva para el exceso de acomodación.Los 9 artículos restantes no analizaban la exactitud diagnóstica, abordando el diagnóstico conlos criterios considerados por los autores. También hallamos diferencias entre los estudios encuanto al modo de considerar la sintomatología de los pacientes. 3 estudios de los 12 analiza-dos llevaron a cabo una validación de una encuesta de sintomatología para la insuficiencia deconvergencia.Conclusiones: La literatura científica revela ciertas diferencias entre los distintos autores encuanto a los criterios diagnósticos para las disfunciones acomodativas y binoculares no estrábi-cas. Los estudios de exactitud diagnóstica muestran que existe sólo cierta evidencia relativa alas condiciones acomodativas. En cuanto a las anomalías binoculares solo existe cierta eviden-cia relativa a un cuestionario validado para la insuficiencia de convergencia, sin datos sobre laexactitud diagnóstica.© 2012 Spanish General Council of Optometry. Publicado por Elsevier España, S.L. Todos losderechos reservados.
earibc(rrgtbat
trthtve
Introduction
Accommodative and nonstrabismic binocular anomalies arevisual dysfunctions which can interfere with a subject’sperformance or impair one’s ability to function efficientlyat work. In fact, those persons who perform considerableamounts of close vision, such as reading or computer work,are more likely to develop symptoms and signs related toaccommodative or vergence dysfunctions.1 The most com-mon classification to categorize vergence disorders wasoriginally developed by Duane2 for application to strabismusand was later extended to nonstrabismic binocular visionanomalies by Tait.3 Other authors have included the need toregard vergence anomalies as syndromes of deterioration orhave proposed classifications based on graphical analysis.4
However, these categorizations have been descriptive whichdoes not necessarily imply etiology and they only considervergence mechanism in its unfused or open loop state4 but,as other authors have shown,5 these models do not estimatethe contribution of proximal factor. For this reason, severalauthors state that predictions about binocular anomaliesshould be based on measurements under fusion conditions,4
so that the classification of vergence anomalies should spec-ify binocular status with fusion present.
In this sense, Wick6 described a classification systemfor nonstrabismic binocular anomalies that represents an
aa
a
xpansion of Duane’s classification and is based on consider-tion of the distance phoria (tonic vergence) and the AC/Aatio. In this system, the possible diagnoses can be dividednto three main categories of binocular vision problemsased on the AC/A ratio. Low AC/A ratio anomalies refer toonvergence insufficiency (CI) and divergence insufficiencyDI), normal AC/A ratio are basic exophoria, basic esopho-ia and fusional vergence dysfunction (FVD) and high AC/Aatio disorders include convergence excess (CE) and diver-ence excess (DE). According to accommodative anomalies,he classification used is originally from Donders7 and haseen popularized by several authors.4,8---11 It includes thenomalies of accommodative insufficiency (AI), accommoda-ive excess (AE) and accommodative infacility (AIN).
In general, accommodative and binocular dysfunctionsend to provoke difficulties related mainly to activitiesequiring close vision. Symptoms commonly associated withhese anomalies may include blurred far or near vision,eadaches, diplopia, difficulty in reading, loss of concen-ration, and in many cases, impossibility to maintain clearision for a reasonable period of time.12---15 Results of sev-ral accommodative and binocular tests, which may be
ltered, are named as the signs used for diagnosing thesenomalies.11Although research has suggested that these dysfunctionsre commonly found in clinical practice,16---27 the scientific

4
lfagotandg�
P
lchtpsttotpmainorvt
dvotuftcrttkcswpef
iissoaa
da
my
sddatd
M
Wi2Fle
fiiceticigw
•••
•
•
•
•
••••
••
•
•
iterature provides different clinical diagnostic criteria usedor these conditions, sometimes with dissimilar diagnosesmong authors.4,28,29 A good example is observed for conver-ence insufficiency condition. Dwyer4 uses a large exophoriaf 12 � in addition to the clinical signs of reduced posi-ive fusional vergence (PFV), reduced vergence facility (VF)nd a fixation disparity curve Type III with no allusion to theear point of convergence (NPC). Other authors28 make theiagnosis of convergence insufficiency using the signs of areater exophoria at near vision rather than distance (≥4), a failure of Sheard’s criterion or a minimum normativeFV at near vision, and receded NPC.
The exact impact of these anomalies on quality ofife is not known. Several studies have found some asso-iation between vergence disorders and attention deficityperactivity disorder30,31 and there is also some indicationhat convergence insufficiency can be related to readingroblems.32 In any case, considering their symptoms, iteems obvious that clinical recognition would be impor-ant to prevent unnecessary frustration among patients. Inhat sense, vision clinicians diagnose and treat a wide rangef visual and ocular anomalies, including not only refrac-ive problems, but also accommodative and binocular visionroblems, among others. Treatment of patients with accom-odative and binocular disorders is based on interpreting
nd analyzing the results of visual examination. Accordingly,t is important that accurate information about the diag-osis is available, as the treatment prescribed will dependn the diagnosis. For this reason it is essential not only foresearchers but also for clinicians to know the diagnosticalidity of the clinical criteria often used for these condi-ions.
Diagnostic validity (or diagnostic accuracy) of clinicaliagnostic tests is usually examined by means of predictivealues, sensitivity and specificity or analyzing the receiverperator curve (ROC).33 A ROC curve shows how severe therade-off is between sensitivity and specificity and can besed to help decide where the best cut-off point should beor a particular test. It shows the accuracy of a diagnos-ic test which can be described as the area under the ROCurve. In epidemiological terms the diagnostic validity rep-esents the scientific evidence33 about the way to diagnosehese visual conditions. In relation to clinical practice, theerm ‘evidence’ is used specifically to refer to sources ofnowledge that are relevant to the practical solution for alinical problem.34 Such problems may be more general orpecific. It should be a decision on which available treatmentill provide the best outcome for a particular condition andatient. Or even they might be such as the choice of the bestxamination procedure to minimize risk of misdiagnosis orailure to detect a particular disease or condition.34
In that sense, the strongest form of clinical evidences a ‘‘systematic review’’ of a number of trials or stud-es addressing the one clinical question.35 Suitable trials ortudies are extracted from the literature by a well-designedearch strategy.34 A systematic review is then an overviewf primary studies, which is conducted according to explicitnd reproducible methodology which may contain a meta-
nalysis but not necessarily.36Therefore, the aim of this study is to analyze theiagnostic criteria used in the scientific literature forccommodative and nonstrabismic binocular dysfunctions by
•
P. Cacho-Martínez et al.
eans of a systematic review of papers published in the pastears about the diagnosis of these conditions.
Specific aims are to explore which symptoms and clinicaligns are used by different studies; to explore if an epi-emiological analysis of diagnostic validity has been used inifferent studies related to the diagnosis of these conditionsnd to evaluate if authors utilize these results to recommendhe clinical criteria to diagnose these anomalies or use otheriagnostic criteria.
ethods
e carried out an exhaustive search on content publishedn four health-science databases from 1986 to January 25,012. The search was carried out using MEDLINE, CINAHL,rancis and PsycINFO databases. We decided to study thisarge time frame in order to avoid omission of possible rel-vant information on these anomalies.
The search strategy was based on the use of terms inree language related to these visual anomalies, search-ng in all fields of the databases. The search equationncluded Boolean operators, truncated symbols and wildcardharacters which are specific signs used in information sci-nces and in databases selected. As we wanted to examinehe anomalies of accommodative excess, accommodativensufficiency, accommodative infacility, convergence insuffi-iency, convergence excess, divergence excess, divergencensufficiency, basic esophoria, basic exophoria, fusional ver-ence dysfunction and hyperphoria, the search terms usedere the following:
(Accommodative excess) OR (excess of accommodation) (Accommodative spasm) OR (spasm of accommodation) (Accommodative insufficiency) OR (insufficiency of
accommodation) (Accommodative infacility) OR (infacility of accommoda-
tion) (Accommodative disorder*) OR (accommodative anomal*)
OR (accommodative dysfunction*) (Disorder* of accommodation) OR (anomal* of accommo-
dation) OR (dysfunction* of accommodation) (Convergence insufficiency) OR (insufficiency of conver-
gence) (Convergence excess) OR (excess of convergence) (Convergence spasm) OR (spasm of convergence) (Divergence excess) OR (excess of divergence) (Divergence insufficiency) OR (insufficiency of diver-
gence) Basic e?ophoria (Vergence disorder*) OR (vergence anomal*) OR (vergence
dysfunction*) (Binocular disorder*) OR (binocular anomal*) OR (binocu-
lar dysfunction*) (Vergence infacility) OR (reduced fusional vergence) OR
(fusional vergence dysfunction*) OR (fusional vergenceanomal*) OR (fusional vergence disorder*)
Hyperdeviation* OR hypodeviation* OR hypophoria* ORhyperphoria* OR (vertical deviation*) OR vertical disor-der*) OR (vertical anomal*) OR (vertical dysfunction*) notsurgery.

inoc
traacamgg
R
Tosli
tolrtasippdr
swCtmA
rcidt
catthoabdt
ias
Evidence for the validity of diagnostic criteria for general b
The inclusion criteria were original articles whosepurpose were to study the diagnosis of accommodativeand nonstrabismic binocular dysfunctions. They could bedescriptive studies or clinical studies with sample popula-tions including all ages from children to adults. As the aim ofthis review was only related to diagnosis of these conditionsand we wanted to know if the scientific literature publishedhad analyzed the diagnostic validity of clinical criteria used,we excluded papers about the prevalence and treatment ofthese conditions. We also excluded studies not fundamen-tally concerned with the diagnosis of accommodative andnonstrabismic binocular disorders; publications related tothe performance of optometric tests but not related to diag-nosis of anomalies; expert guides or opinions; non-originalarticles and studies on strabismic binocular disorders or ocu-lar pathologies.
Using the search terms, we found 839 articles. Followingthe inclusion and exclusion criteria, we initially selected 42articles for exhaustive study and to confirm inclusion. Ofthe 797 articles we excluded 326 (40.9%) which mentionedbut were not fundamentally related to diagnosis of theseanomalies, 195 (24.5%) dealt with strabismic anomalies, 125(15.7%) were concerned with ocular pathologies, 75 (9.4%)concerning treatment and prevalence of dysfunctions and 76(9.5%) were studies about the assessment of several tests.
Of the 42 articles, 30 did not fulfill the inclusion crite-ria and were excluded from further analysis. The remainingincluded articles (n = 12) were analyzed.4,28,29,37---45
As selected studies were not related to any interventionand were not homogeneous, no meta-analysis was per-formed. Accordingly, included articles were reviewed usinga range of variables. We examined the methodological char-acteristics, showing the characteristics of the sample andexploring if studies had analyzed the diagnostic validity ofthe criteria used. We also examined and registered infor-mation regarding the clinical signs and the cut-off pointstaken into account for each anomaly. We also explored theresults of each study, compiling data about their conclu-sions, biases and limitations. Finally, to examine the qualityof included articles, we used the QUADAS-2 tool which isused to test the quality of studies about diagnostic accu-racy included in systematic reviews46 and recommended bythe Cochrane Collaboration.47 The QUADAS tool consists of4 key domains that discuss: patient selection, index test,reference standard, and flow of patients through the studyand timing of the index tests and reference standard (flowand timing). For each domain there are signaling questionswhich aid the reviewer to judge the risk of bias (high, low orunclear) and concern regarding applicability of each study.For the domain of patient selection is considered if the sam-ple is consecutive or randomized. The index test consider ifan index test result is interpreted without the knowledgeof the results of the reference standard as the potential forbias is related to the subjectivity of interpreting index testand the order of testing. The domain of reference standardis considered to know if the reference standard, its conductor its interpretation may have introduced bias. Thus the aimis to know if the reference standard is likely to correctly
classify the target condition and if the reference standardresults are interpreted without knowledge of the results ofthe index test. The last domain (flow and timing) is consid-ered if there is an appropriate interval between the indexcgtq
ular dysfunctions 5
est and reference standard, if all patients receive the sameeference standard, and if all patients are included in thenalysis. Finally, the QUADAS-2 tool includes also data ofpplicability so that the aim is to know if there are con-erns that the included patients and setting, the index test,nd the target condition defined by the reference standardatch the review question. These QUADAS-2 results are sug-
ested to be shown in a tabular presentation and with araphical display.
esults
able 1 contains the methodological characteristics of eachf the studies reviewed. It shows the characteristics of theample and study population, the type of dysfunction ana-yzed, the information about the validation of symptoms andf each study analyses the diagnostic validity of clinical signs.
Of the twelve articles reviewed, five of them are prospec-ive clinical studies which select patients and severalptometric tests are carried out.29,37,38,41,45 Two studies col-ect data retrospectively from the patients’ optometricecords42,44 and two reports make a descriptive analysis ofhe dysfunctions.4,43 On the other hand, three papers28,39,40
lso study the diagnosis, although their aim is to validate aymptom questionnaire related to these anomalies. Accord-ng to the samples, most of the articles refer to clinicalopulations,28,29,39---42,44 with two studies37,38 in which theopulation is collected from schools. Four studies28,37,38,40
eal with child populations and other six studies29,39,41,42,44,45
efer to adult populations.According to the type of dysfunctions, CI is the most
tudied condition when considering binocular anomalies,ith seven studies.4,28,37,39---41,44 There are two studies aboutE,4,41 DI,4,43 DE,4,44 basic exophoria4,44 and only one relatedo basic esophoria.4 For accommodative conditions there areore studies on AI, with six studies,4,29,37,38,41 compared withE with three reports4,41,42,45 and only one about AIN.4
Regarding the validity of diagnostic criteria, threeeports28,39,40 perform a validation of the symptoms used foronvergence insufficiency. There are also three studies29,38,41
n which several epidemiological tools are used to test theiagnostic accuracy of clinical signs used for several condi-ions.
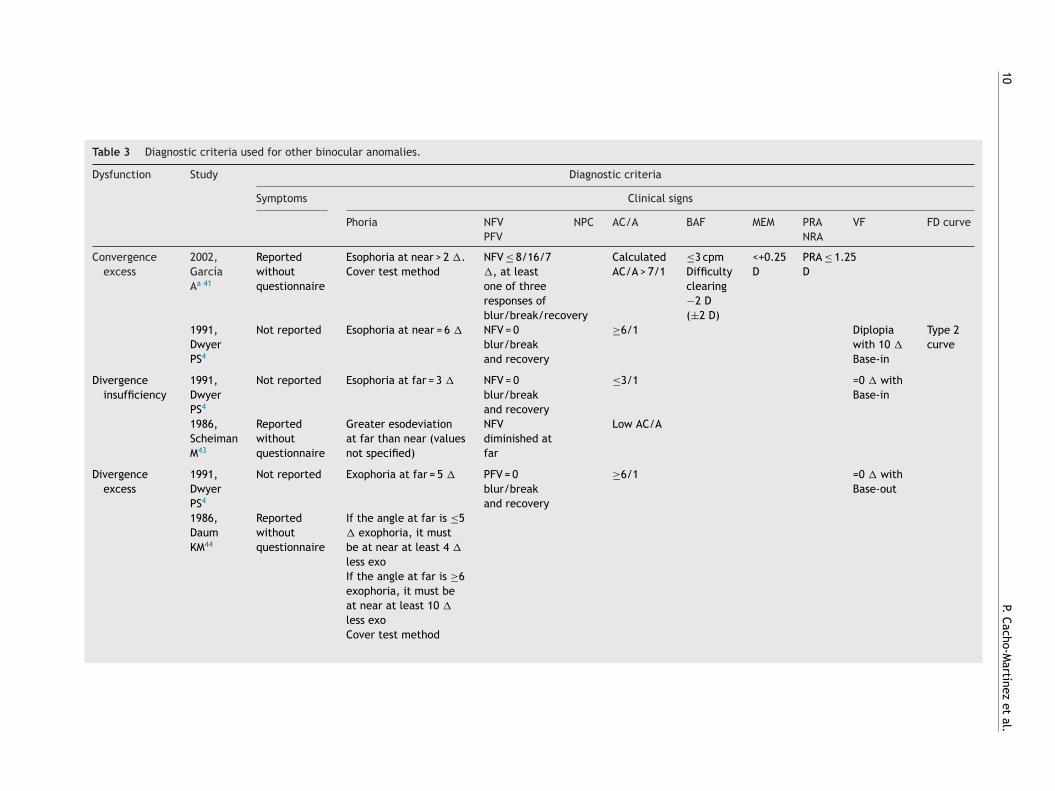
Tables 2---4 show the diagnostic criteria used foronvergence insufficiency, other binocular anomalies, andccommodative dysfunctions, respectively. They show bothhe clinical signs and the cut-off points used to diagnosehese conditions by each author. The tables also includeow the authors collected patients’ symptoms. As we canbserve the authors use more than one test to diagnose thenomalies, ranging from one to seven clinical signs for bothinocular and accommodative dysfunctions. There are alsoifferences in the cut-offs used to decide if a patient fails aest.
Table 5 shows the conclusions obtained, biases and lim-tations identified in the papers. Several studies related toccommodative dysfunctions29,38,41,42 obtain specific conclu-ions, suggesting the use of several diagnostic tests. The
onclusions obtained for binocular dysfunctions are moreeneral and less focused on suggesting the use of particularests. There is also a notable absence of validated symptomuestionnaires used to diagnose the anomalies.
6
P. Cacho-M
artínez et
al.
Table 1 Methodological characteristics of the 12 studies included.
Study Characteristics of the sample Study population Dysfunction Diagnostic validity ofsymptoms
Diagnostic validity ofclinical signs
2006, Marran LF37 299 children (46.1% male, 53.9%female)Age range not specifiedMean age: 11.5 ± 0.63 years
19 schools CIAI
2006, Sterner B38 First examination: 72 children (43male, 29 female)Age: 5.8---10 yearsMean age not specified
School AI ROC analysis usingsymptoms at near asthe gold standard
Second examination: 59 childrenafter 1.8 years (34 male, 25 female)Age: 7.8---11.8 yearsMean age not specified
Positive and negativepredictive values
2004, Rouse MW39 46 patients with CI (28% male, 72%female)Age: 19---30 yearsMean age: 24.3 ± 3.6 years
6 optometric clinics CI ROC analysis to testthe ability of CISSV-15 questionnairea
to discriminatebetween CI and NBVgroups
46 patients with normal binocularvision (23% male, 77% female)Age: 19---30 yearMean age: 24.4 ± 3.2 years
2003, Borsting EJ40 47 children with CI62.5% male, 57.5% femaleAge: 9---18 yearsMean age: 11.5 ± 2.2 years56 children with NBV (54.5% male,45.5% female)Age: 9---18 yearsMean age: 11.4 ± 2.2 years
5 optometric clinics CI Sensitivity andspecificity for theCISSb score
2002, García A41 69 patients (29 male, 40 female)Age: 13---35 yearsMean age: 20.8 ± 4.7 years
Optometric clinic AI, AE, CI, CE Sensitivity andspecificity analysis

Evidence for
the validity
of diagnostic
criteria for
general binocular
dysfunctions
7
Table 1 (Continued)
Study Characteristics of the sample Study population Dysfunction Diagnostic validity ofsymptoms
Diagnostic validity ofclinical signs
2002, Cacho P29 41 patients with diminished AA40 patients with normal AASex not specifiedAge: 13---35 yearsMean age not specified
Optometric clinic AI Sensitivity andspecificity analysis
1999, Borsting E28 14 children with CI (8 male, 5female)Age: 8---13 yearsMean age: 10.75 ± 1.8 years14 children with NBV (5 male, 9female)Age: 8---13 yearsMean age: 11.2 ± 1.75 years
Optometric clinic CI Sensitivity andspecificity analysis ofCIRSc symptom surveyand Odds ratio
1991, Dwyer PS4 Sample not used --- AI, AE, AIN, CI,CE, DI, DE,BExo, BEso
1988, Rutsein RP42 17 patients (6 male, 11 female)Age: 7---39 yearsMean age: 17.9 years
University optometricclinic
AE
1988, Chrousos GA45 10 patients (4 male, 6 female)Age: 10---19 yearsMean age not specified
Not specified AI
1986, Scheiman M43 Sample not used --- DI
1986, Daum KM44 179 patients (69 male, 110 female)Age: 2---56 yearsMean age: 19.7 years
Optometric clinic CI, BExo, DE
NBV: normal binocular vision, AI: accommodative insufficiency, AE: accommodative excess, CI: convergence insufficiency, CE: convergence excess, AIN: accommodative infacility, DI:divergence insufficiency, DE: divergence excess, BExo: basic exophoria, BEso: basic esophoria, NPC: near point of convergence, AA: accommodative amplitude, NFV/PFV: negative/positivefusional vergence, MAF/BAF monocular/binocular accommodative facility, PRA/NRA: positive/negative relative accommodation.
a CISS V-15: 15-item version of CISS, Convergence Insufficiency Symptom Survey.b CISS: 13-item of CISS, Convergence Insufficiency Symptom Survey.c CIRS symptom survey: Convergence Insufficiency and Reading Study symptom survey.

8
P. Cacho-M
artínez et
al.
Table 2 Diagnostic criteria used for convergence insufficiency.
Dysfunction Study Diagnostic criteria
Symptoms Clinical signs
Phoria PFV NPC AC/A BAF MEM PRA VF FD curveNFV NRA
Convergenceinsufficiency
2006,MarranLFa 37
CISS V-15symptomquestionnaire
Exophoria at near≥4 � greater thanat distanceVon Graefemethod
PFV failures toreach Sheard’s11criteria orfailure to haveminimumnormative PFVat near, ≤15�
for break
≥6 cmbreak
2004,RouseMW39
CISS V-15symptomquestionnairescore ≥ 21
Exophoria at near≥4 � greater thanat distanceVon Graefemethod
PFV failures toreach Sheard’s11criteria orfailure to haveminimumnormative PFVat near, ≤15�
for break
≥6 cm
2003,BorstingEJ40
CISS V-15symptomquestionnairescore ≥ 16
Exophoria at near≥4 � greater thanat distanceVon Graefemethod
PFV failures toreach Sheard’s11criteria orfailure to haveminimumnormative PFVat near, ≤15�
for break
≥6 cm
2002,García,Ab 41
Reportedwithoutquestionnaire
Exophoria at near>6 �. Cover testmethod
PFV ≤ 11/14/3�, at least oneof threeresponses ofblur/break/recovery
>10 cmbreak or>17.5recovery
CalculatedAC/A < 3/1
≤3 cpmDifficultyclearing+2 D(±2 D)
<+0.25D
NRA≤1.50D
1999,BorstingE28
CIRS symptomquestionnairescore ≥9
Exophoria at near≥4 � greater thanat distanceMethod notspecified
Failed Sheard’scriterion orminimum PFVat near,≤12/15/4 �
≥7.5 cmbreak

Evidence for
the validity
of diagnostic
criteria for
general binocular
dysfunctions
9
Table 2 (Continued)
Dysfunction Study Diagnostic criteria
Symptoms Clinical signs
Phoria PFV NPC AC/A BAF MEM PRA VF FD curveNFV NRA
1991,DwyerPS4
Not reported Exophoria atnear = 12 �
PFV = 0blur/break andrecovery
≤3/1 Diplopiawith 12 �
Base-out
Type 3curve
1986,DaumKM44
Reportedwithoutquestionnaire
If the angle at faris ≤5 � exophoria,it must be at nearat least 4 � moreexoIf the angle at faris ≥6 exophoria, itmust be at near atleast 10 � moreexoCover test method
NPC: near point of convergence, NFV/PFV: negative/positive fusional vergence, BAF: binocular accommodative facility, MEM: MEM dynamic retinoscopy, PRA/NRA: positive/negativerelative accommodation, �: prism diopters.
a Authors consider having an exophoria at near a fundamental sign and CI may be diagnosed with one, two or three clinical signs.b Authors diagnose CI considering exophoria, PFV and NPC as fundamental signs and patients must have at least two signs of the remaining four signs.
10
P. Cacho-M
artínez et
al.
Table 3 Diagnostic criteria used for other binocular anomalies.
Dysfunction Study Diagnostic criteria
Symptoms Clinical signs
Phoria NFV NPC AC/A BAF MEM PRA VF FD curvePFV NRA
Convergenceexcess
2002,GarcíaAa 41
Reportedwithoutquestionnaire
Esophoria at near > 2 �.Cover test method
NFV ≤ 8/16/7�, at leastone of threeresponses ofblur/break/recovery
CalculatedAC/A > 7/1
≤3 cpmDifficultyclearing−2 D(±2 D)
<+0.25D
PRA ≤ 1.25D
1991,DwyerPS4
Not reported Esophoria at near = 6 � NFV = 0blur/breakand recovery
≥6/1 Diplopiawith 10 �
Base-in
Type 2curve
Divergenceinsufficiency
1991,DwyerPS4
Not reported Esophoria at far = 3 � NFV = 0blur/breakand recovery
≤3/1 =0 � withBase-in
1986,ScheimanM43
Reportedwithoutquestionnaire
Greater esodeviationat far than near (valuesnot specified)
NFVdiminished atfar
Low AC/A
Divergenceexcess
1991,DwyerPS4
Not reported Exophoria at far = 5 � PFV = 0blur/breakand recovery
≥6/1 =0 � withBase-out
1986,DaumKM44
Reportedwithoutquestionnaire
If the angle at far is ≤5� exophoria, it mustbe at near at least 4 �
less exoIf the angle at far is ≥6exophoria, it must beat near at least 10 �
less exoCover test method

Evidence for
the validity
of diagnostic
criteria for
general binocular
dysfunctions
11
Table 3 (Continued)
Dysfunction Study Diagnostic criteria
Symptoms Clinical signs
Phoria NFV NPC AC/A BAF MEM PRA VF FD curvePFV NRA
Basic exophoria 1991,DwyerPS4
Not reported Uncompensatedexophoria at far andnear
=4.5/1
1986,DaumKM44
Reportedwithoutquestionnaire
If the angle at far is ≤5� exophoria, it can beat near between 0 and3 � more or less exoIf the angle at far is ≥6exophoria, it can be atnear between 0 and 9� less exo or between0 and 3 � more exoCover test method
Basic esophoria 1991,DwyerPS4
Not reported Uncompensatedesophoria at far andnear
=4.5/1
NFV/PFV: negative/positive fusional vergence, NPC: near point of convergence BAF: binocular accommodative facility, MEM: MEM dynamic retinoscopy, PRA/NRA: positive/negative relativeaccommodation, VF: vergence facility, FD: fixation disparity, �: prism diopters.
a Authors diagnose CE considering esophoria, NFV as fundamental signs and patients must have at least two signs of the remaining four signs).

12
P. Cacho-M
artínez et
al.
Table 4 Diagnostic criteria used for accommodative anomalies.
Dysfunction Study Diagnostic criteria
Symptoms Clinical signs
AA MAF BAF MEM PRA NRA Visual acuity Refractiveerror
Accommodativeinsufficiency
2006,MarranLF37
CISS V-15symptomquestionnaire
Monocular AA 2D ≤ Hofstetter’sminimum ageformula:15---0.25 × ageMonocular Push upmethod
2006,SternerB38
Reported byseveralquestions
AA < 8 D monocularand < 10 D binocularAAMonocular Push-upmethod
2002,García,Aa 41
Reportedwithoutquestionnaire
Reduced AA: atleast 2 D < minimumage appropriateamplitude ofHofstetter’s formula(15---0.25 × age)Monocular Push-upmethod
≤6 cpmDifficultyclearing−2 D(±2 D)
≤3 cpmDifficultyclearing−2 D(±2 D)
>+0.75 D ≤1.25 D
2002,CachoPb 29
Reportedwithoutquestionnaire
Reduced AA: atleast 2 D < minimumage appropriateamplitude ofHofstetter’s formula(15---0.25 × age)Monocular Push-upmethod
≤6 cpmDifficultyclearing−2 D(±2 D)
≤3 cpmDifficultyclearing−2 D(±2 D)
>+0.75 D ≤1.25 D
1991,DwyerPS4
Not reported AA 3 D < Hofstetter’sformula:15---0.25 × age
Blurred with−2 D (±2 D)
≥+1.00 D ≤1.00 D
1988,ChrousosGA45
Reportedwithoutquestionnaire
AA below thenormal for thepatients’ agesMonocular push-upmethod

Evidence for
the validity
of diagnostic
criteria for
general binocular
dysfunctions
13
Table 4 (Continued)
Dysfunction Study Diagnostic criteria
Symptoms Clinical signs
AA MAF BAF MEM PRA NRA Visual acuity Refractiveerror
Accommodativeexcess
2002,García,Ac 41
Reportedwithoutquestionnaire
≤6 cpmDifficultyclearing−2 D(±2 D)
≤3 cpmDifficultyclearing+2 D(±2 D)
<0 D Highfinding≥3.50 D
≤1.50 D Variable Variableretinoscopyandsubjectiverefraction
1991,DwyerPS4
Not reported Blurred with+2 D (±2 D)
≤−0.50 D ≤1.00 D
1988,RutseinRP42
Reportedwithoutquestionnaire
A leadmovement.Value notspecified
Varies. Maybesomewhatreduced
Varies(frequentlyemmetropia)
Accommodativeinfacility
1991,DwyerPS4
Not reported Disorder offacility(values notspecified)
AA: accommodative amplitude, MAF: monocular accommodative facility, BAF: binocular accommodative facility, MEM: MEM dynamic retinoscopy, PRA: positive relative accommodation,NRA: negative relative accommodation.
a Authors consider AA and MAF as fundamental signs and patients must have at least two signs of the rest of three signs.b Authors consider AA and MAF fundamental signs, being BAF, MEM and PRA complementary signs.c Authors consider VA, Refractive error and MAF as fundamental signs and patients must have at least two signs of the rest of three signs.

14 P. Cacho-Martínez et al.
Table 5 Conclusions, bias and limitations of the studies.
Year of publicationand author
Conclusions Bias/limitations identifiedby the authors
Bias/limitations observed in thereview
2006, Marran LF37 CI is a separate and uniqueclinical condition and can occurwithout a comorbid AI condition.However, CI by itself is not ahighly symptomatic condition.Only when the CI is comorbidwith AI, do children with CIscore higher than children withnormal binocular vision, stronglysuggesting that the high score isdriven by the AI condition.
--- ---
2006, Sterner B38 The ROC analysis illustrate thatthe AA has potentialdiscrimination ability foraccommodative insufficiency.Values of 8 D monocular or 11 Dbinocular are values which couldbe used as reference valuessince they clearly imply a highrisk of symptoms for childrenwith results below these limits.
Children below 7.5 yearswith no reportedsymptoms could have beenbiased as they tend to givethe ‘‘correct’’ reply justto please the interviewer.The population could bedescribed as an invitedpopulation. Perhapschildren with symptomswere more willing to takepart in the study implyingthat the prevalence ishigher than it would be ifa true screening wasapplied.The choice of referencesvalues of AA is somewhatarbitrary.
No validated symptomquestionnaire used.Binocular accommodativeamplitude considered.Accommodative amplitude resultsinterpreted with the knowledge ofthe results of subjective symptomsof patients.
2004, Rouse MW39 Adults with symptomatic CI havea significantly higher CISS scorethan adults with NBV.The CISS is a valid and reliableinstrument that can be usedclinically or as an outcomemeasure for research studies ofadults with CI. A CISS score ≥ 21distinguish between adults withnormal and abnormal levels ofsymptoms.
--- Clinical population. Conclusions arenot representative of generalpopulation.Questionnaire results interpretedwith the knowledge of the results ofdiagnosis.
2003, Borsting E J40 Children with CI show asignificantly higher CISSsymptom score than childrenwith normal binocular vision.The CISS is a valid and reliableinstrument to use as an outcomemeasure for children aged 9 to18 who are enrolled in clinicalresearch concerning CI. A CISSscore of ≥16 distinguishbetween children with normaland abnormal levels ofsymptoms associated with CI.
--- Clinical population. Conclusions arenot representative of generalpopulation.Questionnaire results interpretedwith the knowledge of the results ofdiagnosis.
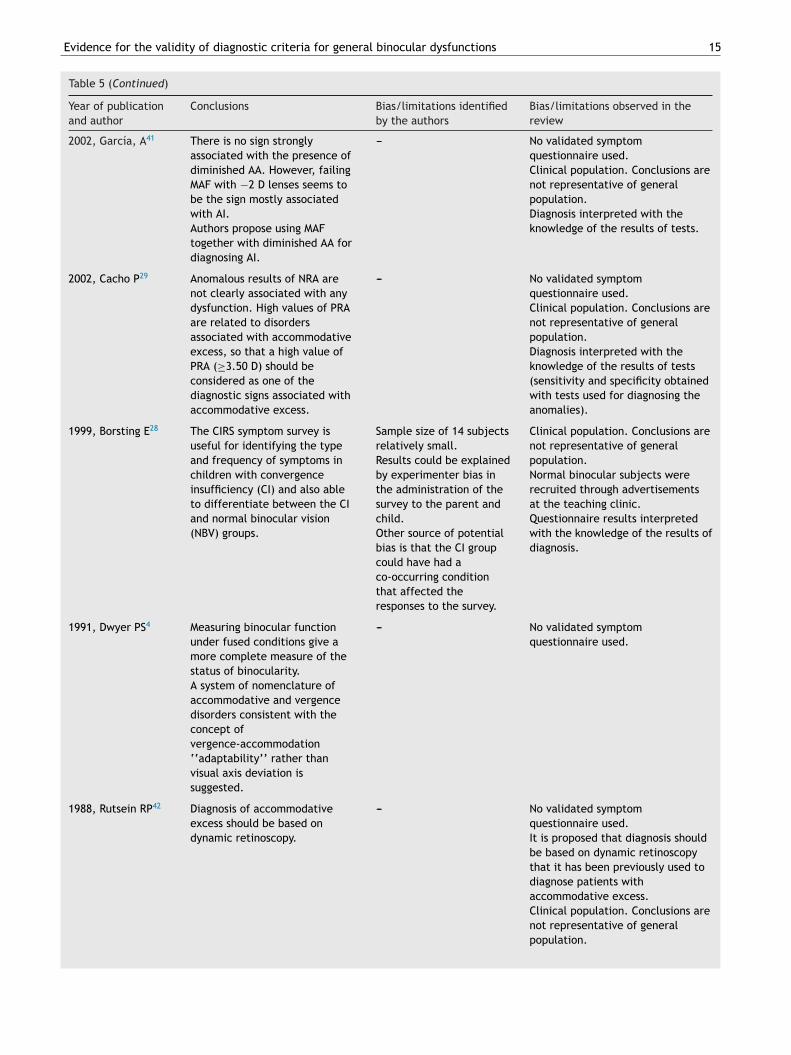
Evidence for the validity of diagnostic criteria for general binocular dysfunctions 15
Table 5 (Continued)
Year of publicationand author
Conclusions Bias/limitations identifiedby the authors
Bias/limitations observed in thereview
2002, García, A41 There is no sign stronglyassociated with the presence ofdiminished AA. However, failingMAF with −2 D lenses seems tobe the sign mostly associatedwith AI.Authors propose using MAFtogether with diminished AA fordiagnosing AI.
--- No validated symptomquestionnaire used.Clinical population. Conclusions arenot representative of generalpopulation.Diagnosis interpreted with theknowledge of the results of tests.
2002, Cacho P29 Anomalous results of NRA arenot clearly associated with anydysfunction. High values of PRAare related to disordersassociated with accommodativeexcess, so that a high value ofPRA (≥3.50 D) should beconsidered as one of thediagnostic signs associated withaccommodative excess.
--- No validated symptomquestionnaire used.Clinical population. Conclusions arenot representative of generalpopulation.Diagnosis interpreted with theknowledge of the results of tests(sensitivity and specificity obtainedwith tests used for diagnosing theanomalies).
1999, Borsting E28 The CIRS symptom survey isuseful for identifying the typeand frequency of symptoms inchildren with convergenceinsufficiency (CI) and also ableto differentiate between the CIand normal binocular vision(NBV) groups.
Sample size of 14 subjectsrelatively small.Results could be explainedby experimenter bias inthe administration of thesurvey to the parent andchild.Other source of potentialbias is that the CI groupcould have had aco-occurring conditionthat affected theresponses to the survey.
Clinical population. Conclusions arenot representative of generalpopulation.Normal binocular subjects wererecruited through advertisementsat the teaching clinic.Questionnaire results interpretedwith the knowledge of the results ofdiagnosis.
1991, Dwyer PS4 Measuring binocular functionunder fused conditions give amore complete measure of thestatus of binocularity.A system of nomenclature ofaccommodative and vergencedisorders consistent with theconcept ofvergence-accommodation‘‘adaptability’’ rather thanvisual axis deviation issuggested.
--- No validated symptomquestionnaire used.
1988, Rutsein RP42 Diagnosis of accommodativeexcess should be based ondynamic retinoscopy.
--- No validated symptomquestionnaire used.It is proposed that diagnosis shouldbe based on dynamic retinoscopythat it has been previously used todiagnose patients withaccommodative excess.Clinical population. Conclusions arenot representative of generalpopulation.

16 P. Cacho-Martínez et al.
Table 5 (Continued)
Year of publicationand author
Conclusions Bias/limitationsidentified by the authors
Bias/limitations observed inthe review
1988, Chrousos GA45 The AA of patients with AI isconsiderably below the normalfor the patients’ ages. Therange of the deficiency is from3.5 D to 8 D with an average of6 D below the minimum normalfor their respective ages.The clinical recognition of AI isimportant to preventunnecessary frustration inthese individuals.
--- No validated symptomquestionnaire used.It is not reported the value ofthe minimal accommodativeamplitude used for consideringaccommodative insufficiency.
1986, Scheiman M43 Divergence insufficiency mustbe differentiated fromdivergence paralysis as well asfrom sixth nerve palsy,convergence excess and basicesophoria, all of which canpresent with an esodeviationat distance.The differential diagnosisdepends very much upon thenature of the patient’ssymptoms.
--- No validated symptomquestionnaire used.
1986, Daum KM44 Patients with exodeviations,when divided into three classeson the basis of the relationbetween the near and distanceangles of deviation, showsignificant differences invarious clinical parameters.Patients with equalexodeviations have the largestangles of deviations overalland those with CI generallyhave smaller angles than theother groups. Differences inthe AC/A ratios are to beexpected on the basis of theclassification criteria.
The data should not beconsidered exactlyrepresentative of thegeneral populationbecause the clinic formwhich the records weredrawn is a referral clinic.
No validated symptomquestionnaire used.Clinical population.Conclusions are notrepresentative of generalpopulation.
CI: convergence insufficiency, AI: accommodative insufficiency, AA: accommodative amplitude, MAF: monocular accommodative facility,ters.
v(o2tgiildt
D
Ttbsbc
NRA/PRA: negative and positive relative accommodation, D: diop
As only 6 of 12 included studies show the diagnosticalidity, QUADAS-2 results are only presented for themTables 6 and 7). Furthermore, to better understand resultsf quality rating, the 6 studies analyzed by the QUADAS-
tool were divided into two categories: those designedo assess the accuracy of clinical signs and those investi-ating the validation of a questionnaire for convergencensufficiency. These results are also presented in a graph-cal display, showing the proportion of studies with high,
ow or unclear risk of bias. Figs. 1 and 2 show the QUADAS-2omain for articles related to clinical signs and those relatedo symptoms, respectively.nbds
iscussion
he scientific literature targeting the field addressed inhis review is extensive. The review reveals differencesetween authors according to diagnostic criteria used in thecientific literature for accommodative and nonstrabismicinocular dysfunctions. However, most of the publicationsonsist of narrative overviews describing methods, tech-
iques, symptoms, for the clinical evaluation of generalinocular anomalies. In contrast, only a few studies wereesigned for assessing the accuracy of clinical tests andymptoms. Diagnostic accuracy studies show that there is
Evidence for the validity of diagnostic criteria for general binocular dysfunctions 17
Table 6 Quality rating of the 3 included studies related to clinical signs (QUADAS −2 results).
Study Risk of bias Applicability concerns
Patientselection
Indextest
Referencestandard
Flow andtiming
Patientselection
Indextest
Referencestandard
2006, Sterner B38
2002, García A41 ?
2002, Cacho P29 ? ?
( ) low risk; ( ) high risk; (?) unclear risk.
Table 7 Quality rating of the 3 included studies related to symptoms (QUADAS −2 results).
Study Risk of bias Applicability concerns
Patientselection
Indextest
Referencestandard
Flow andtiming
Patientselection
Indextest
Referencestandard
2004, Rouse MW39
2003, Borsting EJ40
1999, Borsting E28
( ) low risk; ( ) high risk; (?) unclear risk.
Flow and timing
Reference standard
Index test
Patient selection
0%
Proportion of studies with low, high or unclearRISK of BIAS
Qua
das-
2 D
omai
n
Proportion of studies with low, high, or unclearConcerns regarding applicability
20% 40% 60% 80% 100% 0% 20%
Low High Unclear
40% 60% 80% 100%
Fig. 1 QUADAS-2 domain for articles related to clinical signs.29,38,41
Flow and timing
Reference standard
Index test
Patient selection
0% 20%
Proportion of studies with low, high or unclearRisk of BIAS
Proportion of studies with low, high, or unclearConcerns regarding applicability
Qua
das-
2 D
omai
n
40% 60% 80% 100% 0% 20%
Low High Unclear
40% 60% 80% 100%
articl
jtAj
w
Fig. 2 QUADAS-2 domain for
only certain evidence for accommodative conditions. Forbinocular anomalies there is only evidence about a validatedquestionnaire for convergence insufficiency with no data ofdiagnostic accuracy about binocular anomalies so that theevidence of diagnostic criteria for binocular dysfunctionscannot be found within papers that have been published
over the past years. In any case, we should consider thatthese arguments may only be applied within the frameworkof this study. The data supplied refers to the past 25 yearsand the articles analyzed have been published in scientificcv
r
es related to symptoms.28,39,40
ournals. Therefore, there may be data in earlier publica-ions or publications not listed within the databases we used.nyway the papers we reviewed were all in peer-reviewedournals.
According to binocular conditions, no study was found inhich the authors assessed the diagnostic validity33 of the
linical signs used. That is, no one used data of predictivealues, sensitivity and specificity or assessed the ROC curve.Although CI is one of the binocular anomalies mosteferred to,4,28,37,39---41,44 in no case the authors validate the

1
tsbbabst(apcdcarta
todsvcgoaaoac
lcTweitfae
tbastr(maaicbtmtbI
fo
oMfmcwevr±≤mtue
avWfissicoc
diadonmouTwsso
iAntatclwribi
8
ests used by comparison against an established referencetandard (gold standard). They reach their diagnoses on theasis of the criteria they consider patients should have,ut fail to specify why certain clinical signs are taken intoccount and others are not. The same is true for the otherinocular anomalies, although they are the subject of fewertudies. Thus, Marran et al.,37 adopt the classification sys-em used by the Convergence Insufficiency Treatment TrialCITT) Group20,22 for CI. It includes the signs of an exophoriat near vision greater than at far at least 4 �, insufficientositive fusional vergence (PFV), and receded near point ofonvergence (NPC). This classification system, as the authorseclare in their study,20 is based on the signs most often asso-iated with convergence insufficiency. However, there is nonalysis of the validity of these signs to confirm the accu-acy of them. The studies which deal with a validation ofhe convergence insufficiency symptom survey (CISS)28,39,40
lso use this classification of CI.Similarly, in Daum44 retrospective study the exodevia-
ions are classified into three classes without an explanationf this classification. The study of García et al.,41 follows aiagnostic criteria based upon the authors particular con-ideration. Dwyer4 study describes a diagnostic model forergence accommodation disorders taking into account theonvergence-accommodation interactions. The author sug-ests a system of nomenclature consistent with the conceptf vergence-accommodation adaptability rather than visualxis deviation. Similarly, other authors43 make a descriptivenalysis about the characteristics and differential diagnosisf DI. They define this condition by referring to the signsccording to different authors, but they do not validate thelinical signs.
As it can be observed, studies about binocular anoma-ies show that it is difficult to provide information on whaturrent criteria should be considered reliable for clinician.he reason is that none of the studies reviewed analyseshich clinical signs have the best diagnostic accuracy forach binocular dysfunction. For that reason, future stud-es related to binocular anomalies should address this issue,hat is, the diagnostic validity of different clinical signs usedor each anomaly. Knowing this evidence, clinicians couldpply diagnostic criteria being aware of their decision forach individual case.
Considering accommodative conditions, there are onlyhree of the seven studies which use diagnostic criteriaased on epidemiological analysis. For this reason only theserticles were assessed using the QUADAS-2 tool. Thus, in thetudy by Sterner et al.,38 the authors test with ROC analysishe discrimination ability of accommodative amplitude andelative accommodations for accommodative insufficiencyAI). ROC analysis illustrates that the amplitude of accom-odation (AA) is a test that has potential discrimination
bility for AI. The authors state that as they have found relationship between AA and subjective symptoms, theres reasonable evidence to use reference values of AA. Thehoice with ROC analysis is 8 D for monocular and 11 D forinocular which implies that children with results belowhese limits have a high risk of symptoms. If either 8 D
onocular or 11 D binocular are used as diagnostic criteria,o have a joint diagnosis of AI should be considered an AAelow these values together with the presence of symptoms.n any case, the authors state that the choice of these values
asAi
P. Cacho-Martínez et al.
or AA is somewhat arbitrary and should be investigated bythers.
The authors of Cacho et al.,29 analyze the conditionf AI. They determine as the most sensitive tests ofEM retinoscopy, monocular and binocular accommodative
acility (MAF, BAF) and positive and negative relative accom-odation (PRA, NRA), together with AA, for classifying this
ondition. The authors recommend the use of MAF alongith AA for their diagnosis based on sensitivity results. How-ver, the authors do not assess the ROC analysis or predictivealues to test the accuracy of these tests. Conclusions areelated to sensitivity results which consider that failing the2.00 D monocular accommodative facility (with a value3 cpm) seems to be the sign most associated with accom-odative insufficiency. The risk of bias of this study is that
he authors do not clarify the order of the tests, so that isnclear if the index test were interpreted without knowl-dge of the results of reference standard and conversely.
Similarly, García et al.,41 analyze different tests associ-ted with accommodative excess (AE). They find that highalues of PRA are related to disorders associated with AE.hile their conclusions are based on sensitivity and speci-city results, there is an important bias in this study sinceensitivity and specificity values are obtained through theame tests previously used to diagnose the anomalies. Thats, the reference standard results (the diagnosis of eachondition) were interpreted with knowledge of the resultsf the index tests (each clinical test assessed), situation thatould have introduced bias in the study.
The other four studies about accommodative anomalieso not analyze their diagnostic criteria using epidemiolog-cal analysis and thus there is no analysis of the diagnosticccuracy of diagnostic criteria used. Thus, Marran et al.,37
efine AI referring to Daum12 study as having an amplitudef accommodation at least 2 D below Hofstetter’s age-basedorms on the Donder’s monocular push-up test. Dwyer4
akes a classification for accommodative disorders based onptometric literature but without an explanation of the val-es of accommodative tests used for diagnosing anomalies.he reader of this study must make an effort to understandhich signs need to be present to affirm a particular diagno-
is. In addition, other authors as Chrousos et al.,45 report aeries of ten healthy patients with AI making only an analysisf their vision findings.
These results show that there is certain evidence accord-ng to diagnostic criteria for accommodative anomalies.lthough there are three studies29,38,41 which test the diag-ostic accuracy for clinical signs, QUADAS-2 tool results showhat there are certain shortcomings in the design, conductnd reporting of these studies. Good results are shown abouthe population and flow and timing items. Patients wereonsecutively chosen in two studies29,41 since the other ana-yzed invited population. All studies have no risk of biashen considering the item of flow and timing, as all patients
eceived the index test and reference standard, all werencluded in the analysis and there were a good time intervaletween index tests and reference standard. However, theres a high risk of bias when considering reference standard
nd index test. Thus, only one study38 interprets referencetandard without knowledge of the results of the index test.ccording to index test, none of the studies interpret thendex test without the knowledge of reference standard.

inoc
Aacbar
acamswiatrmatm
ofCo5o�
ssiemaor
ia0stlna
cp
tsptdtst
Evidence for the validity of diagnostic criteria for general b
However, these studies have good applicability when consid-ering patients who would benefit of these considerations.
With this quality analysis we should only state that thereis certain evidence to use the amplitude of accommoda-tion and monocular accommodative facility for diagnosingaccommodative insufficiency. Similarly, for accommodativeexcess there is certain evidence, although with a risk of bias,that a high positive relative accommodation should be usedas a clinical diagnostic sign.
According to the role played by patients’ symptoma-tology, the review shows that all the studies consider thepresence of symptoms essential to diagnose anomalies.However, there are differences in the way of asking aboutsymptoms as well as to calibrate their severity. Several stud-ies manage symptoms according to the authors’ criteria.Some authors simply refer to symptoms or asthenopia ingeneral.4,29,41,45 Other studies use small patient symptomquestionnaires,38 and others simply compile or present thesymptoms described by the patients.42---44 However, there arefour studies which refer to the use of a validated symp-tom questionnaire.28,37,39,40 Particularly, three of them arestudies whose purpose is to validate a questionnaire of symp-toms. Rouse et al.,39 perform a ROC analysis to test theability of CISS V-15 to discriminate between patients withconvergence insufficiency and those with normal binocularvision. Borsting et al.,40 use the sensitivity and specificityanalysis to test the CISS score, and Borsting et al.,28 use thesensitivity and specificity analysis and Odds ratio to test theCIRS score. All of these three studies28,39,40 conclude thatthe CISS is a valid and reliable instrument for evaluatingsymptoms in adults and children with CI. The appropriateepidemiological methods applied establish that there is avalidated symptom questionnaire for convergence insuffi-ciency. However, the lack of specific questionnaires for theother accommodative and binocular anomalies makes diffi-cult the task of calibrating the severity of their symptomswhich may be useful for diagnostic purposes.
QUADAS-2 results for articles in which a validation of aquestionnaire for convergence insufficiency has been stud-ied also show certain quality rating. For articles relatedto symptoms28,39,40, we can observer that there is a risk ofbias when considering index test and patient selection. Thisis because all three studies interpret the index text (thequestionnaire) with knowledge of the results of the refer-ence standard (diagnosis of convergence insufficiency) andfurthermore because in any case patients of these threestudies were consecutive or randomized. These results implythat in general there is certain concern regarding applica-bility related to patient selection. These results also suggestthat there is certain evidence according to a validatedquestionnaire for convergence insufficiency that should beused when considering patients’ symptomatology for thiscondition.
In addition to the lack of diagnostic validity, the reviewalso reveals the coincidences and differences according tothe clinical signs and the cut-off used by each author.
As we can observe, to diagnose CI all theauthors4,28,37,39---41,44 agree to consider the exophoria at
near vision. The other clinical tests most commonly usedare the PFV and the NPC. For the other binocular dysfunc-tions, the tests most frequently mentioned are the phoriameasurement, the fusional vergences for CE and DI, and theefpp
ular dysfunctions 19
C/A ratio for CE and DI. However, the other binocular testsre used less frequently. We can deduce that the authorsonsider the phoria measurement necessary to diagnose ainocular anomaly, and the tests classified as monocularnd binocular at the same time, such as BAF, MEM dynamicetinoscopy and PRA and NRA, are not so required.
Similarly, for AI, all the authors4,29,37,38,41,45 use the lowmplitude of accommodation (AA) to diagnose it. The otherlinical tests commonly used are MEM retinoscopy, BAFnd PRA.4,29,41 However, only two authors29,41 mention theonocular accommodative facility (MAF) which is an exclu-
ively accommodative test. The same occurs with AE inhich the MEM retinoscopy is the most frequently used clin-
cal sign4,41,42 but the MAF testing is not as commonly useds it should be expected for an accommodative dysfunc-ion, with only one study in which this test is used.41 Theseesults highlight the need to investigate the role of accom-odative tests made under binocular conditions to diagnose
ccommodative anomalies, as well as to establish whetherhey should be used more or less frequently than exclusivelyonocular tests.According to the cut-offs, this review also shows the lack
f uniformity in the cut-off points used to decide if a patientails a particular test. The most significant examples are forI and AI. In the case of CI there are four different cut-ff points used for exophoria at near vision, ranging from�28,37,39,40 to 16�.44 Thus, some studies use the cut-offf having a greater exophoria at near than distance of ≥4.28,37,39,40 Others consider an exophoria at near >6 �.41 One
tudy4 uses the cut-off of 12 � and the other author44 clas-ifies CI based upon the angle of deviation at far. If at fars ≤5 � of exophoria, it must be at near at least 4 � morexo. If the angle of deviation at far is ≥6 � of exophoria, itust be at near at least 10 � more exo. These differences
lso occur for NPC, considering a receded NPC with valuesf ≥6 cm,37,39,40 ≥7.5 cm28 and >10/17.5 cm for break andecovery.41
The same happens with the low AA used for diagnos-ng AI. Some authors consider that the patient must haven AA 2 D below Hofstetter’s minimum age formula 15 ---.25 × age.29,37,41 Others consider having 3 D below the Hof-tetter’s minimum age formula.4 There is one study in whichhe authors use a monocular AA < 8 D and <10 D for binocu-ar AA.38 And there are other authors who consider that it isecessary to have an AA below the normal for the patient’sge, but do not specify which value.45
Obviously, discrepancies about the clinical signs and theirut-offs may cause the same patient to be diagnosed with aarticular anomaly or not, depending on the criteria applied.
Another important issue observed in this review is relatedo the limitation of the type of population used in thetudies. Seven reports reveiwed28,29,39---42,44 examine sampleopulations obtained from optometric clinics or centers. Ashese populations are selected and not randomized theyo not represent the general population. Furthermore, onlywo studies37,38 analyze school populations, which are con-idered less biased. It should be taken into account thathe population studied at school is very similar to the gen-
ral child population. Accordingly, the conclusions reachedor each study can only be applied in the context of theseopulations and should not be extrapolated to the generalopulation.
2
C
Iaue
adtHtaslc
afitn
awndapm
C
T
R
0
onclusions
n summary, this review reveals that although the authorspply a wide range of diagnostic criteria, there is a lack ofniformity for the type and number of clinical signs used forach dysfunction as well as for the cut-off used.
There is certain evidence to use the amplitude ofccommodation and monocular accommodative facility foriagnosing accommodative insufficiency and a high posi-ive relative accommodation for accommodative excess.owever, there is a lack of studies which have evaluatedhe diagnostic accuracy of clinical signs used for binocularnomalies so that the evidence about the diagnostic clinicaligns cannot be found within papers that have been pub-ished over the last years. This implies that currently usedlinical diagnostic criteria should assess diagnostic validity.
The review also shows that there is evidence according to validated symptom questionnaire for convergence insuf-ciency with a lack of specific questionnaires to calibratehe severity of symptoms for the other accommodative andonstrabismic binocular anomalies.
Further research should be carried out on accommodativend binocular dysfunctions, with properly designed studies,ith good epidemiological analysis to validate the criteriaecessary for the accurate diagnosis of general binocularisorders. It should be necessary not only for professionals,s they will be sure of a particular diagnosis, but also foratients as they will benefit from receiving the best treat-ent option.
onflicts of interest
he authors declare not to have any conflicts of interest.
eferences
1. Cooper J, Burns C, Cotter S, Daum J, Griffin J, Scheiman M.Care of the patient with accommodative and vergence dys-function. St. Louis: American Optometric Association; 2006.
2. Duane A. A new classsification of the motor anomalies of theeye, based upon physiologic principles. Part 2. Pathology. AnnOphthalmol. 1897;6:247---260.
3. Tait EF. Accommodative convergence. Am J Ophthalmol.1951;34:1093---1107.
4. Dwyer P. Clinical criteria for vergence accommodation dysfunc-tion. Clin Exp Optom. 1991;74:112---119.
5. Wick B, London R. Analysis of binocular visual function usingtests made under binocular conditions. Am J Optom PhysiolOpt. 1987;64:227---240.
6. Wick BC. Horizontal deviation. In: Amos J, ed. Diagnosis andmanagement in vision care. Boston: Butterworth-Heinemann;1987:461---510.
7. Donders F. On the anomalies of accommodtion and refractionof the eye. London: New Syndeham Society; 1864.
8. London R. Accommodation in ocular assessment. In: BarresiB, ed. Ocular assessment: the manual of diagnosis for officepractice. Boston: Butterworth-Heinemann; 1984:123---130.
9. Cooper J. Accommodative dysfunction. In: Amos J, ed.Diagnosis and management in vision care. Boston: Butterworth-
Heinemann; 1987:431---454.10. Zellers J, Alpert T, Rouse M. A review of the literature and anormative study of accommodative facility. J Am Optom Assoc.1984;55:31---37.
P. Cacho-Martínez et al.
11. Scheiman M, Wick B. Clinical management of binocular vision.Philadelphia: Lippincott Williams & Wilkins; 2008.
12. Daum K. Accommodative dysfunction. Doc Ophthalmol.1983;55:177---198.
13. Weisz C, How to find and treat accommodative disorders.Optometry. 1983;(January):48---53.
14. Scheiman M, Mitchell G, Cotter S, et al. A randomized clinicaltrial of treatments for convergence insufficiency in children.Arch Ophthalmol. 2005;123:14---24.
15. Daum K. Convergence insufficiency. Am J Optom Physiol Opt.1984;61:16---22.
16. Hokoda S. General binocular dysfunctions in an urban optome-try clinic. J Am Optom Assoc. 1985;56:560---562.
17. Scheiman M, Gallaway M, Coulter R, et al. Prevalence of visionand ocular disease conditions in a clinical pediatric population.J Am Optom Assoc. 1996;67:193---202.
18. Porcar E, Martinez-Palomera A. Prevalence of general binoculardysfunctions in a population of university students. Optom VisSci. 1997;74:111---113.
19. Lara F, Cacho P, García A, Megías R. General binocular dis-orders: prevalence in a clinic population. Ophthalmic PhysiolOpt. 2001;21:70---74.
20. Rouse M, Hyman L, Hussein M, Solan H. Frequency of conver-gence insufficiency in optometry clinic settings. ConvergenceInsufficiency and Reading Study (CIRS) Group. Optom Vis Sci.1998;75:88---96.
21. Abdi S, Rydberg A. Asthenopia in schoolchildren, orthopticand ophthalmological findings and treatment. Doc Ophthalmol.2005;111:65---72.
22. Borsting E, Rouse M, Deland P, et al. Association of symptomsand convergence and accommodative insufficiency in school-age children. Optometry. 2003;74:25---34.
23. Rouse M, Borsting E, Hyman L, et al. Frequency of convergenceinsufficiency among fifth and sixth graders. The ConvergenceInsufficiency and Reading Study (CIRS) group. Optom Vis Sci.1999;76:643---649.
24. Dwyer P. The prevalence of vergence accommodation disordersin a school-age population. Clin Exp Optom. 1992;75:10---18.
25. Letourneau J, Duci S. Prevalence of convergence insuffi-ciency among elementary school children. Can J Optom.1988;50:194---197.
26. Pickwell L, Viggars M, Jenkins T. Convergence insufficiency ina rural population. Ophthalmic Physiol Opt. 1986;6:339---341.
27. Cacho-Martínez P, García-Munoz Á, Ruiz-Cantero MT. Do wereally know the prevalence of accomodative and nonstrabismicbinocular dysfunctions? J Optom. 2010;3:185---197.
28. Borsting E, Rouse MW, De Land PN. Prospective comparisonof convergence insufficiency and normal binocular children onCIRS symptom surveys. Convergence Insufficiency and ReadingStudy (CIRS) group. Optom Vis Sci. 1999;76:221---228.
29. Cacho P, García A, Lara F, Seguí M. Diagnostic signs of accom-modative insufficiency. Optom Vis Sci. 2002;79:614---620.
30. Granet D, Gomi C, Ventura R, Miller-Scholte A. The relation-ship between convergence insufficiency and ADHD. Strabismus.2005;13:163---168.
31. Grönlund M, Aring E, Landgren M, Hellström A. Visual functionand ocular features in children and adolescents with attentiondeficit hyperactivity disorder, with and without treatment withstimulants. Eye (Lond). 2007;21:494---502.
32. Simons H, Grisham J. Binocular anomalies and reading prob-lems. J Am Optom Assoc. 1987;58:578---587.
33. Fletcher RH, Fletcher SW. Clinical Epidemiology: The Essen-tials. Philadelphia: Lippincott Williams & Wilkins; 2007.
34. Anderton PJ. Implementation of evidence-based practice in
optometry. Clin Exp Optom. 2007;90:238---243.
inoc
Assessing methodological quality. In: Deeks J, Bossuyt P, Gat-sonis C, eds. Cochrane handbook for systematic reviews ofdiagnostic test accuracy version 100: the cochrane collabora-
Evidence for the validity of diagnostic criteria for general b
35. Canadian Task Force on Preventive Health Care. New grades forrecommendations from the Canadian Task Force on PreventiveHealth care. CMAJ. 2003;169:207---208.
36. Graham AM. Finding retrieving and evaluating journal andweb-based information for evidence-based optometry. Clin ExpOptom. 2007;90:244---249.
37. Marran L, De Land P, Nguyen A. Accommodative insufficiencyis the primary source of symptoms in children diagnosed withconvergence insufficiency. Optom Vis Sci. 2006;83:281---289.
38. Sterner B, Gellerstedt M, Sjöström A. Accommodation and therelationship to subjective symptoms with near work for youngschool children. Ophthalmic Physiol Opt. 2006;26:148---155.
39. Rouse M, Borsting E, Mitchell G, et al. Validity and reliabil-ity of the revised convergence insufficiency symptom survey inadults. Ophthalmic Physiol Opt. 2004;24:384---390.
40. Borsting E, Rouse M, Mitchell G, et al. Validity and reliabil-ity of the revised convergence insufficiency symptom survey in
children aged 9 to 18 years. Optom Vis Sci. 2003;80:832---838.41. García A, Cacho P, Lara F. Evaluating relative accommoda-tions in general binocular dysfunctions. Optom Vis Sci. 2002;79:779---787.
ular dysfunctions 21
42. Rutstein R, Daum K, Amos J. Accommodative spasm: a study of17 cases. J Am Optom Assoc. 1988;59:527---538.
43. Scheiman M, Gallaway M, Ciner E. Divergence insufficiency:characteristics diagnosis treatment. Am J Optom Physiol Opt.1986;63:425---431.
44. Daum K. Characteristics of exodeviations: I. A comparison ofthree classes. Am J Optom Physiol Opt. 1986;63:237---243.
45. Chrousos G, O’Neill J, Lueth B, Parks M. Accommodation defi-ciency in healthy young individuals. J Pediatr OphthalmolStrabismus. 1988;25:176---179.
46. Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: arevised tool for the quality assessment of diagnostic accuracystudies. Ann Intern Med. 2011;155:529---536.
47. Reitsma J, Rutjes A, Whiting P, Vlassov V, Leeflang M, Deeks J.
tion. 2009.