irs fo,m ~@15
TRANSCRIPT

Employer identification number
Fo,m 8879-EO
Department of the TreasuryInternal Revenue Service
Name of exempt organization
IRS e-file Signature Authorizationfor an Exempt Organization
For calendar year 2015, or fiscal year beginning. .• 2015, and ending • 20
••..Do not send to the IRS. Keep for your records.••..Information about Form 8879-EO and its instructions is at www.irs.govlform887geo.
OMS No. 1545-'878
~@15Seneca Falls Develo mcnt Cor orationName and title of officer
26.0283628
Joell Murne .Karsten ChairType of Return and Return Information (Whole Dollars Only)
Check the box for the return for which you are using this Form 8879-EO and enter the applicable amount, if any, from the return. If youcheck the box on line 1a, 2a, 3a, 4a, or Sa, below, and the amount on that line for the return being filed with this form was blank, thenleave line 1b, 2b, 3b, 4b, or 5b, whichever is applicable, blank (do not enter -D-). But, if you entered -D- on the return, then enter .D- onthe applicable line below. Do not complete more than 1 line in Part I.
1a Form 99D check here ~ 0 b Total revenue, if any (Form 99D, Part VIII, column (A), line 12) 1b -------2a Form 99D-EZ check here ~ [2] b Total revenue, if any (Form 99D-EZ, line 9) . 2b 58,854.3a Form 112D-POL check here ~ 0 b Total tax (Form 112D-POL, line 22) . 3b4a Form 99D-PF check here ~ 0 b Tax based on investment income (Form 99D-PF, Part VI, line 5) 4b _Sa Form 8868 check here ~ 0 b Balance Due (Form 8868, Part I, line 3c or Part II, line 8c) 5b _
~ as my signatureEnter five numbers, butdo not enter all zeros
to enter my PIN
ImII Declaration and Signature Authorization of OfficerUnder penalties of perjury, I declare that I am an officer of the above organization and that I have examined a copy of theorganization's 2D15 electronic return and accompanying schedules and statements and to the best of my knowledge and belief, theyare true, correct, and compiete. I further declare that the amount in Part I above is the amount shown on the copy of theorganization's electronic return. I consent to allow my intermediate service provider, transmitter, or electronic return originator (ERO)to send the organization's return to the IRS and to receive from the IRS (a) an acknowledgement of receipt or reason for rejection ofthe transmission, (b) the reason for any delay in processing the return or refund, and (c) the date of any refund. If applicable, Iauthorize the U.S. Treasury and its designated Financial Agent to initiate an electronic funds withdrawal (direct debit) entry to thefinancial institution account indicated in the tax preparation software for payment of the organization's federal taxes owed on thisreturn, and the financial institution to debit the entry to this account. To revoke a payment, I must contact the U.S. Treasury FinanciaiAgent at 1-888-353-4537 no later than 2 business days prior to the payment (settlement) date. I aiso authorize the financial institutionsinvolved in the processing of the electronic payment of taxes to receive confidential information necessary to answer inquiries andresolve issues related to the payment. I have selected a personal identification number (PIN) as my signature for the organization'selectronic return and, if applicable, the organization's consent to electronic funds withdrawal.
Officer's PIN: check one box onlyo I authorize Bonn Dioguardi & Ray. LLP
ERO firm name
on the organization's tax year 2015 electronically filed return. If I have indicated within this return that a copy of the return isbeing filed with a state agency(ies) regulating charities as part of the IRS Fed/State program, I aiso authorize the aforementionedERO to enter my PIN on the return's disclosure consent screen.
o As an officer of the organization, I will enter my PIN as my signature on the organization's tax year 2D15 electronically filed return.If I have indicated within this return that a copy of the return is being filed with a state agency(ies) regulating charities as part ofthe IRS Fed/St r am, I will e er he return's disclosure consent screen.
Dale •.
Certification and AuthenticationERO's EFIN/PIN. Enter your six-digit electronic filing identificationnumber (EFIN) followed by your five-digit self-selected PiN.
do not enter all zeros
I certify that the above numeric entry is my PiN, which is my signature on the 2D15 eiectronically filed return for the organizationindicated above. I confirm that I am submitting this return in accordance with the requirements of Pub. 4163, Modernized e-File (MeF)Information for Authorized IRS e-file Providers for Business Returns.ERD's signature ••. Date •.
ERO Must Retain This Form - See InstructionsDo Not Submit This Form To the IRS Unless Requested To Do So
For Paperwork Reduction Act Notice, see back of form. Cat. No. 37189W Fo"" 8879-EO (2015)
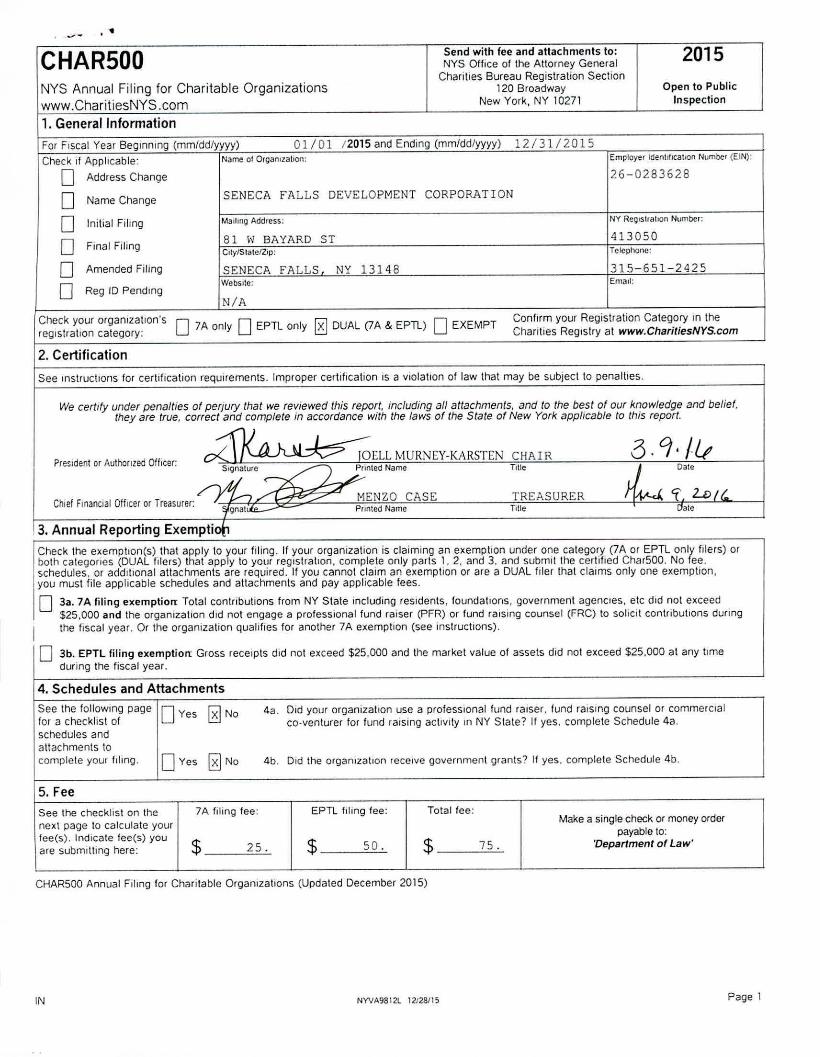
. -" ••CHAR500NYS Annual Filing for Charitable Organizationswww.ChariliesNYS.com1. General Information
Send with fee and attachments to:NYS Office of the Attorney General
Charities Bureau Registration Section120 Broadway
New York, NY 10271
2015Open to Public
Inspection
SENECA FALLS DEVELOPMENT CORPORATION
413050
26-0283628
NY ReOlSlfahon Number:
315-651-2425Email:
Employer Identilicallon Number (EIN):12131/2015
NY 13148
N/A
81 \; BAYARD 5TClly1Stalc/Z,p:
SENECA FALLSWebSIte:
Marling Address:
For FIScal Year Beginning (mmidd/yyyy) 01/01 /2015 and Ending (mm/ddlyyyy)Check If Applicable: Name01 Orgamzation:o Address Change
o Name Change
o InitIal FIling
o Final Filing
o Amended Filing
DReg ID Pending
Check your organization's D D rv1 Dreglslrat,on calegory: 7A only EPTl only ~ DUAL (lA & EPTl) EXEMPT
2. Certification
Confirm your Registration Category in theCharities Registry at www.CharitiesNYS.com
See Instructtons for certification requirements. Improper certification IS a VIolatIon of law that may be subject to penalties.
Dale
6.9,1&J Dale
~ 'f L.D/f..TREASURERTitle
MENZO CASEPflllied Name
We certify under penalties of perjury that we reviewed this report, including afJattachments, and to the best at our Knowledge and belief,they are true. correct and complete in accordance with the laws of the State of New York app/lcable to this report.
~~I.l.Presidentor AuthOrIZedOfficer:
IOELL MURNEY-KARSTEN CIIA I R_S;;lure ~~nledName Tille
. / Y'l,.--,AChief FInanCIalOfficer or Treasurer:
Qnatllle--
3. Annual Reporting Exempti~Check the exemptlon(s) that apply 10 your filing. If your organization is claiming an exemption under one calegory (7A or EPTL only filers) orboth categories (DUAL filers) that apply to your reglslralion, complete only paris 1. 2. and 3. and submit the certifIed Char500. No fee.SChedules, or addlllonal attachments are required. If you cannol claim an exemption or are a DUAL filer that claims only one exemption,you must file applicable schedules and attachments and pay applicable fees.o 3a. 7A filing exemption: Total contributions from NY State including reSidents. foundatIons, government agenCies, etc did nol exceed
$25.000 and the organization did not engage a professional fund raiser (PFR) or fund raiSIng counsel (FRC) to solicit contributions dUfingI the fiscal year. Or the organization qualifIes for another 7A e:-;emptlon (see instructions).
o 3b. EPTL filing exemption Gross receipts did not exceed $25.000 and the market value of assets did not exceed $25.000 at any timeduring the fiscal year.
4. Schedules and AttachmentsSee the follOWing pagefor a checklist ofschedules andattachments tocomplete your fIling.
DYes 0 No
DYes 0No
4a. Old your organization use a professional fund raiser. fund raiSing counselor commercialco-venturer for fund raising activity In NY Slate? It yes. complete Schedule 4a.
4b. Did the orgamzatlon receIve government grants? If yes. complete Schedule 4b.
5. FeeSee the checklist on thenext page to calculate yourfee(s). Indicate fee(s) youare submItting here:
7A filing fee:
$ 25.
EPTL filing fee:
$ 50.
Total fee:
$ 75.
Make a single check or money orderpayable to:
'Department of Law'
CHAR500 Annual Filmg for Charitable Organizations (Updated December 2015)
IN NYVA98121 12128115 Page 1

,.SENECA fALLS DEVELOP~IENT COHPORATION 413050
CHAR500Annual Filing Checklist
Simply submit the certifled CHAR500 with no fee. schedule. or additional attachments IF:. Your organization is registered as 7A only and you marked the 7A filing e,;emption in Part 3 .. Your organization is registered as EPTl only and you marked the EPTL filing exemption in Part 3.. Your organization is registered as DUAL and you marked both the 7A and EPTL filing exemption in Part 3.
Checklist of Schedules and Attachments
Check the schedules you must submit With your CHAR500 as described in Part 4:
oo
II you answered 'yes' in Part 4a, submit Schedule 4a: ProfeSSional Fund Raisers (PFR), Fund Raising Counsel (FRC), CommercialCo' Venturers (CCV)
If you answered 'yes' In Part 4b. submIt Schedule 4b: Government Grants
Check Ihe fmancial attachments you must submit WIth your CHAR500;
o IRS Form 990, 990.EZ, or 990-PF, and 990.T If applicable
o All additional IRS Form 990 Schedules, including Schedule B (Schedule of Contributors).
o Our organization was eligible tor and filed an IRS 990-N e-postcard. We have included an IRS Form 990.EZ for slate purposes only.
If you are a 7A only or DUAL filer ,submit the applicable Independent Certified PublIC Accountant's Review or Audit Report:
o ReVIew Report If you received total revenue and support greater than $250,000 and up to $500,000.
o Audit Report if you received lotal revenue and support greater than $500,000
~ No ReVIew Report or Audit Report IS required because lotal revenue and support is less Ihan $250,000
o We are a DUAL flIer and checked box 3a, no Review Report or AudIt Reporl IS required
Calculate Your Fee
For 7A and DUAL filers. calculate the 7A fee:
o $0, If you checked the 7A exemption In Part 3a
o $25, if you dId not check the 7A exemption in Part 3a
For EPTl and DUAL filers, calculate the EPTl lee:
o $0, If you checked the EPTl exemptIon in Part 3b
o $25, If the NET WORll-i is less than $50,000
81 $50, If the NET WORll-i is $50,000 or mo,e but less than $250,000
o $100, ,I the NETWORll-i IS $250,000 or more bulless than $1,000,000
o $250, If the NETWORll-i is $1,000,000 or more but less than $10,000,000
o $750, If the NET WORll-i is $10,000,000 or more but less than $50,000,000
o $1500, II the NET WORTH IS less $50,000,000 or more
Send Your FilingSend your CHAR500, all schedules and attachments. and tolal fee to:
NYS Office of the Attorney GeneralChanties Bureau Registration Section'20 BroadwayNew York, NY 10271
CHAR500 Annual Filmg for Chantable Organizations (Updated December 2015)
b my Regl.tration ClJtegory 7A, EPTl.. DUAL or EXEMPnOfgamzaholls are assll~netJ a Rcg1slrallon CategOfy uponregistfa\lon wllh tile NY Chantltes Bureau:
74. filers ale registered to soliCit conlflbulions ,n New YOfkunder Arbclc 7,A ot tile EJecutlvc law (7A')
EPTL '1lcfS are reOlstered under the Estates. Po",~rs &. Trustslaw ('EPTl) because they hold ,lS~ets andfor conduct i1Cllvlt!eslor charllable tlufDCSes In NY,
DUAL filers are rCl),stcred under wth 7A and EPTl,
EXEMPT flh~r$ have reo'stefed wllh the NY Ctld/ltoeS Bureatland mcet Condl(lons in Schedule E • Reg/s'r.,lt;mE.empf/on tor Cher/fftJltI Orgenlz.tioM. TheseoflJanlzallOn are nol reqUired to lile (fllnual flnanclal'cpOftsbtll mar do so voluntarily.
Conllrm your Registration CaleQory and learn more about NYlilW at _,ChllfHH1sNYS.com
Wher. do' tlnd my org.rltzallon's NET WORTH?NET WORTH lor lee purposes IS calculated on:, IRS Form 990 p,),t I, line 22• IRS FOfln 990 EZ Pa,1 I line 21. IRS form 990 Pf, Cillculate (he dille-renee between
Total Assets at Fall Market Value (Pari II. hne 16(C») andTolalliabililies (part II. !rne 23{b)).
IN NYVA9B12l 12'28115 Page 2
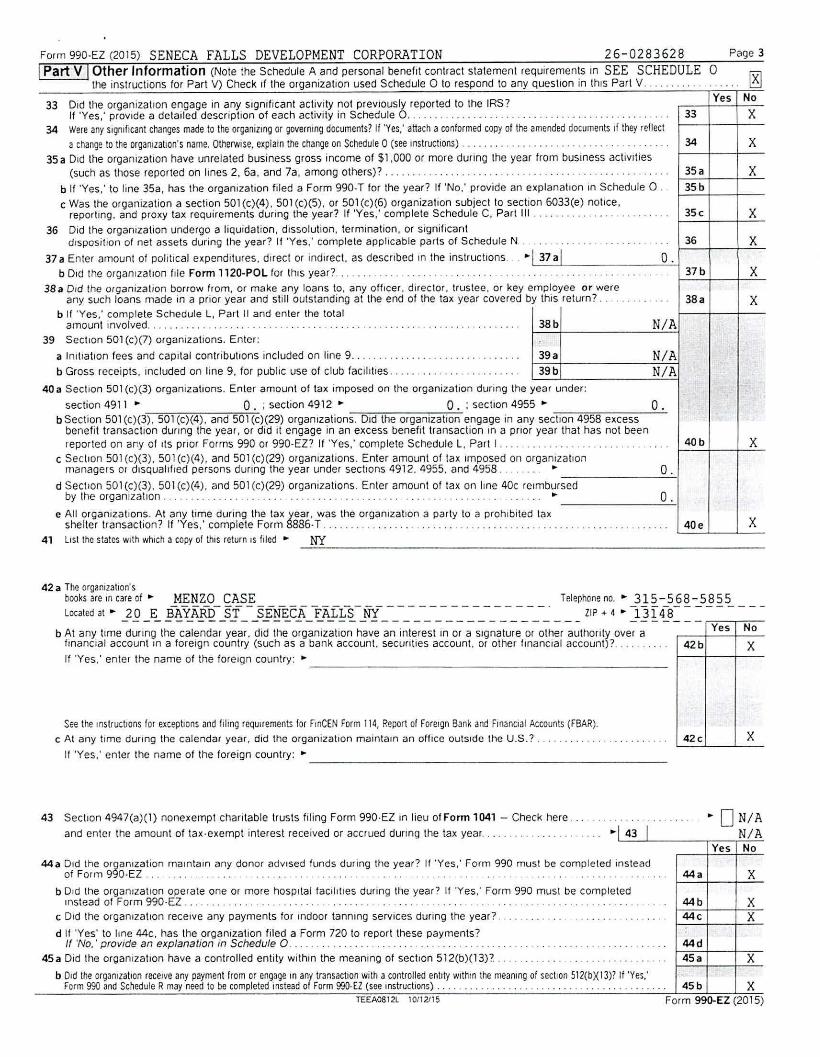
Form 990.EZ (2015) SENECA FALLS DEVELOPMENT CORPORATION 26-0283628IPart V IOther Information (Note the Schedule A and personal benefit contract statement ,eqUlrements In SEE SCHEDULE
the instructions for Pari V) Check If the organization used Schedule 0 to respond to any question in this Part V .
x
x
Page 3
0~.. ....
Yes No
X
X
X
X
X
X
X38.
37b
34
33
35a
35b
35c
40b
36
40e
o .
o.o.
N/AN/A
N/A
o.
38b
33 Old the organizallon engage in any sigmficant activity not previously reported to the IRS?11'Yes,' provide a detailed description of each activity in Schedule O. . . . .. .. .. . .. . .. .. . . . . .. . .
34 Were any Significantchanges made to the organizingor governingdocuments? If 'Yes: attacha conformed copy of the amended documents If they relleeta change to the organizatIOn's name. Otherwise, explarn the Change on Schedule 0 (see lnstructlOns) ....•........................•.......
35 a Old the organization have unrelated business gross income of $1,000 or more dUring the year trom business actIVIties(such as those reported on hnes 2. 6a, and 7a, among others)? . . . . . . . . . . . . . . . . . .. . .
b If 'Yes,' to line 35a, has the organlzallon filed a Form 990-T for the year? If 'No,' provide an explanalJon in Schedule 0 ..c Was the organization a section 501(c)(4), 501 (c)(5), or 501 (c)(6) organizalion subjeclto secllon 6033(e) notrce,reporting. and proxy tax requirements during the year? If 'Yes,' complete Schedule C. Part III .
36 Did the organization undergo a liquidation, dissolution, termination, or signiflcantdIsposition of net assets during the year? If 'Yes,' complete applicable parts of Schedule N. . ..... _. . . .. .. _...
37 a Enter amount of political expenditures, direct or indIrect, as described In the instrucllons, ..•. I 37 alb Old the organization file Form 1120~POL for thiS year? .. _. ... . . . . . . . . . . . .. . ..... ,.. . ..
38a D,d the organization borrow from, or make any loans to, any officer, dIrector, trustee, or key employee or wereany such loans made in a prior year and still outstanding at the end of the tax year covered by thiS return? .
b If 'Yes,' complete Schedule L, Part II and enter the totalamount Involved .. _. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . .
39 Section 501 (c)(7) orgaOlzatlons. Enter:
a 100tration fees and capital contributIOns included on line 9 , . . . . . . .. .. . . . 39 a
b Gross receipts, Included on line 9, for pubhc use of club faCIlities _. . . .. . . .. .. . . .. .. . 39 b
40 a Section 501 (c)(3) organizations. Enter amount of tax Imposed on the organization dUring the year under:
section 4911 •. O. ; section 4912 •. O. : section 4955 •.b Sec lion 501 (c)(3). 501 (c)(4). and 501 (c)(29) organIZations. D,d the organization engage in any section 4958 e,cessbenefit transaction durmg the year, or did It engage in an excess benefit transaction In a pnor year that has not beenreported on ar.y of ItS pnor Forms 990 or 990-EZ? If 'Yes,' complete Schedule L, Part I.. . . . . .. . .. .. . . .. . . . . ....
c Sec lion 501 (c)(3). 501 (c)(4), and SOl (c)(29) organlZalions. Enter amount of ta' unposed on organlZallonmanagers or disqualified persons dunng the year under sectlQns 4912. 4955, and 4958... ... .. •.
d Seclion SOl (c)(3). SOl (c)(4). and 501 (c)(29) organIZations. Enter amount of ta, on line 40c re,mbursedby the organization _. . . . . . . . . . .. . _ •.
e All organization:;. ~t a~y ti~e dunng the tax year, was the orgamzatlon a party to a prOhibited taxshelter transactton. If Yes, complete Form 8886-T _ _ _ _ .
41 list the stalesWithwhIcha COpy01thiS return ISfiled" NY
-- Yes No
42b X
42c XSeethe InstructJonsfor exceptionsanclfiling reQuHementsfor F'lnCENForm 114,Report01ForeignBankand FmanclalAccounts(fBAR).
c At any time dunng the calendar year, did the organization maintam an office outside the U.S.? ..
If 'Yes,' enter the name of the foreign country: •. _
b At any tlme during the calendar year. did the organization have an interest in or a signature or other authOrity over aIrnanClal account In a foreign country (such as a bank account. secuntles account, or other finanCial account)? .
If 'Yes,' enter the name of the foreign country: •. ~ _
423 Theorganization'sbook"",""",f. MENZO CASE Telephoneno.• 315-568-5855Localed,I. JQ _E_ f12tABILsf_-_s%~lcFJ~:.AJf~-_Nf_-_-_-_-_-_-_-_-_-_-_-_-_-_-_- liP + 4 • }E4:( - - - - - - --
43 Sec lion 4947(a)(1) nonexempt chantable trusts filing Form 990.EZ In lieu of Form 1041 - Check here.
and enter the amount of tax-exempt interest received or accrued dUring the tax year ..0 N/A
N/AI Yes I No
44a ~fldF:;;~ 093o~EZ~i~.n ~~~,.nt~.I~.~~~ .~~~~~ ~.d.V.I~~~.f.~~~~ .d.~r~ng.l~.e.~~ar:. l.'.'~.e.s,: :O(~.~~~~~S~ .~~ ~.om~~~t.e.~~ns~~~~ . 44. XbOld Ihe orgaOlzatlon operate one or more hospItal taclhlles dUring the year? If 'Yes,' Form 990 must be completedInstead of Form 990-EZ .. .. ..... .. .. . . .. . . ' ... .. ... . .. .. . . .. .. . .. . .. ... ' .. 44b X
C Old the organization receive any payments for IOdoor tanOlng services during the year? .. . ... . . . .. .. .. ... .. . .. . . .... 44c Xd If 'Yes' to line 44e. has the organization tiled a Form 720 to report these payments?If 'No,' provide an explanation in Schedule O ........................... _............. .. . ... . . _ .. ... . . . .... .. .. . .. 44d
453 Did the organization have a controlled entity within the meaning at secllon 512(b)(13)? .. . . . . ......... . .. ........ 45. Xb Old theorganizationreceiveany paymenllrom or engageIn any transactIonwith a controlledentity wlthrn the meanrngof section 512(bX13)?If 'Yes,' ..form 990 andScheduleRmayneedto be completedInsteadof Form99O-£l (see instructions) ..... _... ... . .. . . .. . . . .. ....... . . . . . . . . . 45b X
TEEA0812l 10112115 Form 99IJ.EZ (2015)

Form 990.EZ (2015) SENECA FALLS DEVELOPMENT CORPORATION 26-0283628 Page 4
Yes No
Check If the organizallon used Schedule 0 to respond 10 any question In this Part VI. ...... .. ... ' . . . . .. . ... nYes No
47 Old the organization engage in lobbying actIVIties or have a section SOl(h) eleclton in effect during the lax year? If 'Yes,'complete Schedule C, Part II......... .... .. .... .. ......... ,' ........... . ....... . ... ,.- .. ....... . .... . . .. . .. . . 47 X
48 Is the orgamzatlon a school as descnbed in section 170(b)(1)(A)(II)? If 'Yes.' complete Schedule E. .. . . . . . . . . ......... 48 X49a Did the organizalion make any transfers to an exempt non-chantable related organization? .... . . . .. .. . . , . , . , .. .. .. 49 • X
b If 'Yes,' was the related organIzation a section 527 organization? .................. '.' . ... . .. .. . . . . ...... , .. . .... . . 49b
46 Did the organization engage. directly or indirectly, in political campaign activIties on behalf of or in OPPosition to Icandidates for public office? If 'Yes.' complete Schedule C. Part I. ,................. 46 X
IPart VI I Section 501(cX3) organizations onlyAll section 501(c)(3) organizations must answer questions 47-49b and 52, and complete the tablesfor lines 50 and 51.
50 Complete this table for the organization's five highest compensated employees (other Ihan offICers, directors, trustees and keyemployees) who each received more than $100,000 of compensation from the organization. If there IS none, enler 'None.'
(b) Average hours(d) Heatlh benelils.
(ill) Name and title 01 oach employee pCI .•••eek de"otcd (e) Reportable compensahon contributIons to employee te) Eslrrnated amount o!
\0 POSition(Forms W.211m.MISC) benehl plans. 311ddelerred oll'er 'umpen~al,on
,0rnpenSdtlon
NONE------------------- -----
------------------------------------------------------------------------------------------------
f Total number of other employees paId over $100,000 ~ -----------51 Complete this table for the organization's live highest compensated independent contractors who each received more Ihan $100.000 ofcompensatIon from the organlzatlon. If there is none, enter 'None.'
(.)Nal11l.' c1lld bus,ness addre!>!> 01 each mdependcnt ,ontraclor (b) TYflC 01 serv,c{,' (c) Compcn .••llton
NONE - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - - - - - -- - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
d Total number of olher Independent contractors each recelvmg over $100,000 ..52 Did the organization complete Schedule A? Note: All section 501(c)(3) organizations must attach a
completed Schedule A . . . . . . . . . . . . . . . . . . . . . .
-- ~Yes
P00105271
PTIN
• 16-1460600585 381-9660
• ~Yes DNaForm 990-EZ (2015)
Check 0 IIsell. employed
Fllm's EIN
Phone no.
CHAIR
"2 -.Datep,eo.a'~ Slonalure
Ie; .-', -I -'.".L.-& RAY LLP
MICHAEL S. BOYCHUKF"m', n,m, - BONN DIOGUARDIF"m'"""". 70 LINDEN OAKS
ROCHESTER NY 14625-2804
~5'011, 4.1'
~ IQEU MlJRNEV-KARSTEN'Type or pflnt name and title
P/lnlrrype p'epare"s name
PaidPreparerUse Only
SignHere
May the IRS dISCUSSthIs return With the preparer shown above' See instructions
Un.1t:' penalhes 01 perl"r)/. I ceclar{,' 11'\;111have e.arnned IhI$leturn. mcl(jj,ng acco",pan~'NJ M:~diJes 3nd Slal(~mcnts. and 10 ttl(: best o! nlY Kt1Owled~eand behe~. ,t IStlue. COfrect. and complete. Decl 'at, of preparel 0 IS based on all ,nlornlatlon of wh,ch preparer has any knowledoe.
TEEA0812L 10/12/15

SCHEDULE A(Form 990 or 990.EZ)
Oo!p::ulmenl of th.~ Treasury11l~\."rnillRevcnu..:' Service
Public Charity Status and Public SupportComplete if the organization is a section 501(cX3} organization or a section
4947(aXl} nonexempt charitable trust.•. Attach to Form 990 or Form 990.EZ.
•. Information about Schedule A (Form 990 or 990.EZ) and its instructions isat www.irs.gov/form9g0.
2015Open to Public
Inspection
R A church, convenllon of churches. or association of churches descnbed In section 170(bX1XAXi).
HA schoOl descnbed In section 170(bX1XAXii}. (Attach Schedule E (Form 990 or 990.EZ).)
UA hospital or a cooperative hospital service organization described In section 170(bX1XAXiii),
U.A. medical research organization operated In conJunctton WIttl a hospital described In section 170(bX1XA}(iii) Enter ltle t1cspltal''5.
name, City, and slate:
DAn organrzatlon operated for ihc-benefit of a college o~ ~n~cr;ty a-wned or ope;aied- by a go~ern-;-nenta[unit descr~ed -;n- sccti~n - - - .170(bX1XAXiv). (Complele Pa'i 11.)o A federal. state, or local government or governmental Unit descrIbed In section 17O(bX1XAXv).
~ An organIzatIon that normally receIves a substanllal part of ItS support flam a govelnmental unrt or tram the general publ!c descllbedHI section 170(bX1XAXvi). (Complete Part II.)D A community trust described In section 170(bX1XAXvi}. (Complete Pari II.)
DAn organlzallon that normally receives; (1) more than 33.113% of its support from contnbutlons. membership fces, and gross receiptsfrom actlVlttes relaled to Its exempt functrons - subject to certain exceptions. and (2) no more tt1an 33.1/3% of Its support frorn grossInvestment income and unrelated bUSiness taxable Income (less section 511 tax) from busrnesses acqlured by the organIzation afterJune 30. 1975. See section S09(aX2}. (Complete Part Ill.)
BAn organJzatron organized and operated exclUSively to test for publiC safety. See section 509(aX4).
An organlzailon orgaOlzed and operated exclUSIVely for the benefll of. to perform the functrons of. or to carry Out ttle purposes of oneor more publtcly SUPpOI ted organizations deSCribed III section S09(aXl) or section 509(aX2). See section 509(aX3}. Check llle DOx InIlfles 11a ltlrougtl 11d that deSCribes the type of supporting orgaOlzatlon and complete lines 11e. 11f, and 11g.o Type I. A supporting orgonlzalJon operated, superVised, Of controlled by lIs supported OIganizatlon(s). typrcally by giving the supportedorgamzatlon(s) the power to regularly apPolnl or elect a majority of the dlrectOls 01 truslees of the supporting organlzatlon. You mustcomplete Part IV, Sections A and B.o Type II. A SUPPoltmg OIganizatlon supervised 01' contlolled In connection wlltlltS slIPported organ1zatlon(s), by havmg control ormanagement of the supportmg organIzation vested In the same persons tflat control or manage the supported organlzatlon(s). Youmust complete Part IV, Sections A and C,o Type III functionally integrated. A supporting organization operated In connection WIth. and functIonally Hllegraled Wlttl. Its supportedorganlzatlon(s} (see instructions). You must complete Part IV, Sections A, D, and E.D Type III non.functionally integrated. A supporting OJganizatlon operated In connectJon With ItS supporled organlzation(s) lhat IS nolfunctionally Integlaled. The organlzallon generally must satisfy a distribution reqUirement and an allentlveness requHement (seemslrucllons). You must complete Part IV, Sections A and 0, and Part V.DCheck thiS box Jf IIle olganrzahon received a wnt\(Hl determination from lhe IRS that IllS a Type I. Type II. Type III functionallyIntegrated, or Type 111non.functlonally Integrated supporting organrzatlon
I Enler ttle number of suppo/ted organizations .... .. 1 _
9 PrOVIde the following information ~bout the supported Ofganllallon(s).
1
234
5
67
8
9
1011
a
b
c
d
e
(il Naone III ~hl!~'OIICO (ii) Elr .•(Iii) Trpe Cl O'l}.,n'i<l!lon (iv) I!, Iho: (v) Amount 01 n,onc!il.fy (vi) A"~Ju"l ol Clhe'
o"I",,,;o;ltIO" (tlcs(roIICd0" hnts 1S (..r"an,l,lhollliSteel f",=~,:ll (s~e"~:.;.1.;liC~,!.:' s,,::C'! (~('e,r,~:•.Atu;"~\above «..:c Instrllct'ons» ,n yow \)Overnml}
uOI;umellt?
Ves No
(A)
(8)
(e)
(D) I(E)
TotalBAA For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990.EZ. Schedule A (Form 990 or 990.El) lOl5
Tn.:,\Q.tOlL 10/12115
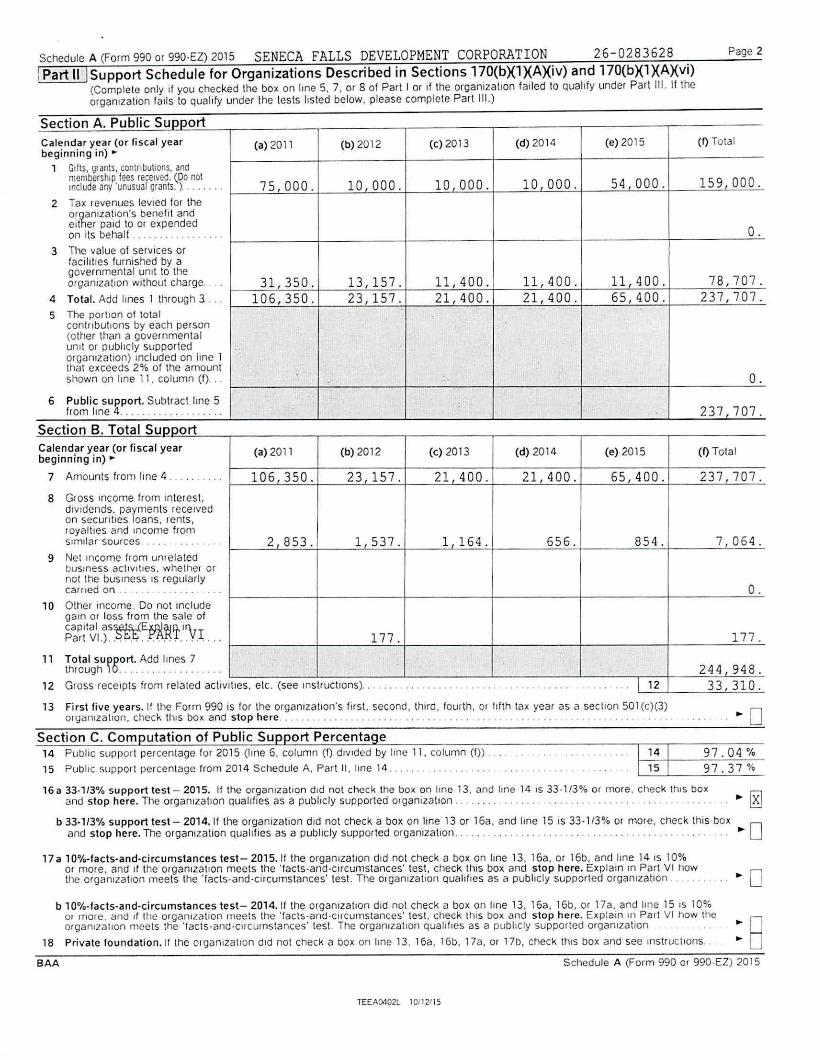
Schedule A (Form 990 or 990-EZ) 2015 SENECA FALLS DEVELOPMENT CORPORATION 26-0283628IPart ulSupport Schedule for Organizations Described in Sections 170(bX1XAXiv) and 170(bX1XAXvi)
(Complete only If you checked lhe box on Irne 5. 7. or 8 of Part J or If the organization failed to Qualify under Part 111.If theorganIzation falls to qualify under the lests listed below, please complete Part Ill.)
Page 2
rh~~~gS~~g~.~..~~.d.~'~12 Gross receipts from r
,,
Section B. Total SupCalendar year (or fiscal yebeginning in) ~
7 Amounts from line 4
8 Gross lflcomc from IndiVidends, paymentson seCUrities loans. IloyaltIes and IncomeSImilar sources ...
9 Net Income flom unrebUSiness aC\IVJ!lcs, Wnol the bus mess IS recar/led on .
10 Other income. Do notgain or IOS5 from thecapital as~EflX1!Part Vl.}.. ..... ..
Section A. Public SupportCalendar year (or fiscal year (a) 2011 (b) 2012 (c) 2013 (d) 2014 (e) 2015 (Q Totalbeginning in) ~
1 Gdt~, grants. contllbutlOns, andmembership fees received. (,00 not 75 000. 10 000. 10 000. 10 000. 54 000. 159 000.Include Jny 'unusual Qranls. )........
2 Tax revenues levied for theor~anizatlon's benefit andcll er paId to or expended O.on Jls behalf. .. .. ... " .. . ....
3 Tl1e value 01 services orfacilIties furnished by agovernmental unIt 10 theOIganizatJon without charge . . . 31,350. 13,157. 11,400. 11,400. 11,400. 78,707.
4 Total. Add Imes J through 3 ... 106,350. 23,157. 21,400. 21,400. 65,400. 237,707.5 The portlon of total
cantil buttons by each person(ottler than a governmentalumt or publicly sUPPorlcd '.'organlzatron) Included on Iinc 1that exceeds 2% of the amountshown on line 11, column (1)... .. O .
6 Public support. Sublract Imc 5 :from Iinc 4 ................. .. 237,707 .
nortar (a) 2011 (b) 2012 (c) 2013 (d) 2014 (e) 2015 (Q Total
....... . .. 106 350. 23 157. 21.400. 21,400. 65,400 . 237,707.terest.receIvedents.from. ..... 2 853. 1 537. 1 164. 656. 854 . 7,064.latedhelhCl orgularJy.. .. .. . O .Includesale of
~.''\rI... 177 . 177 .es 7..... . 244 948 .
elated activlttes, cle. (see IllslructlOns). .. ... ' .. .. ...... . - ... .. .. .. ... .... ... I 12 33,310 .
1415
13 First five years. If the Form 990 is for the organlzatlon's firSt. second, lhlrd. fourth, or hlth tax year as a secllon 501 (c)(3)organlzallon. check thiS box and stop here, ..
Section C. Computation of Public Support Percentage14 Public SUPPOlt percentage for 2015 (line 6. column (I) dlV1ded by hnc 11, colLlmn (I» ...
15 PublIC SlJpport percentage from 2014 Schedule A. Part II, line 14 .97.04 %97.37 %
16a 33.113% support test- 2015. If the organization did not check the box on line 13. and hne 14 IS 33."3% or more. check thiS box rv1and stop here. The organization quahfles as a publicly supported organization. .. . .. .. . ..............................••. ~
b 33.113% support test - 2014.11 the organrzatJon dId not check a box on hne 13 or 16a. and line 15 is 33- 1f3% or more, check this box -- 0and stop here. The organization QualifIes as a pUblicly supported organization............ ..,............. ••.
17a 10%,.facts.and-circumstances test- 2015.11 the organJzatlon did not check a box on Ime 13. 16a. or 16b. and line 14 IS 10%or more, and II the organizatIon meets the 'Iacts.and-circumstances'test. check thiS box and stop here. ExplaIn In Part VI tlQWtile organrzatlon meets the 'Iacts.and,cllcumslances' test. The olganlzatlon qualifies as a pubhcly supported orgamzatlon ..........•. 0
b 10%-facts.and-circumstances test- 2014, If the organlzallon dId nol check a box on hne 13. 16a, 16b. or 17a. and line 15 IS 10%01 /flore. and If 1I1(~orgaOiLation meels Ihe 'lacls.and.cilcumstances' test, check thl5 box and stop here. Explain III Palt VI how the •. norganlza\lon meets the 'tacts.and,clrcurnstances' lest. The organizatIon qualifIes as a publicly supported organIzatIon . .
18 Private foundation. II the olganlzatlon dId not check a bOX on hne 13. 163, 1Gb, 178.01 17b, cheCk thIS box and sec Instructions •. 0BAA Schedule A (Form 990 0' 990.EZ) 2015
TEEA0402l 10f121l 5
OMS No. 1545-0047
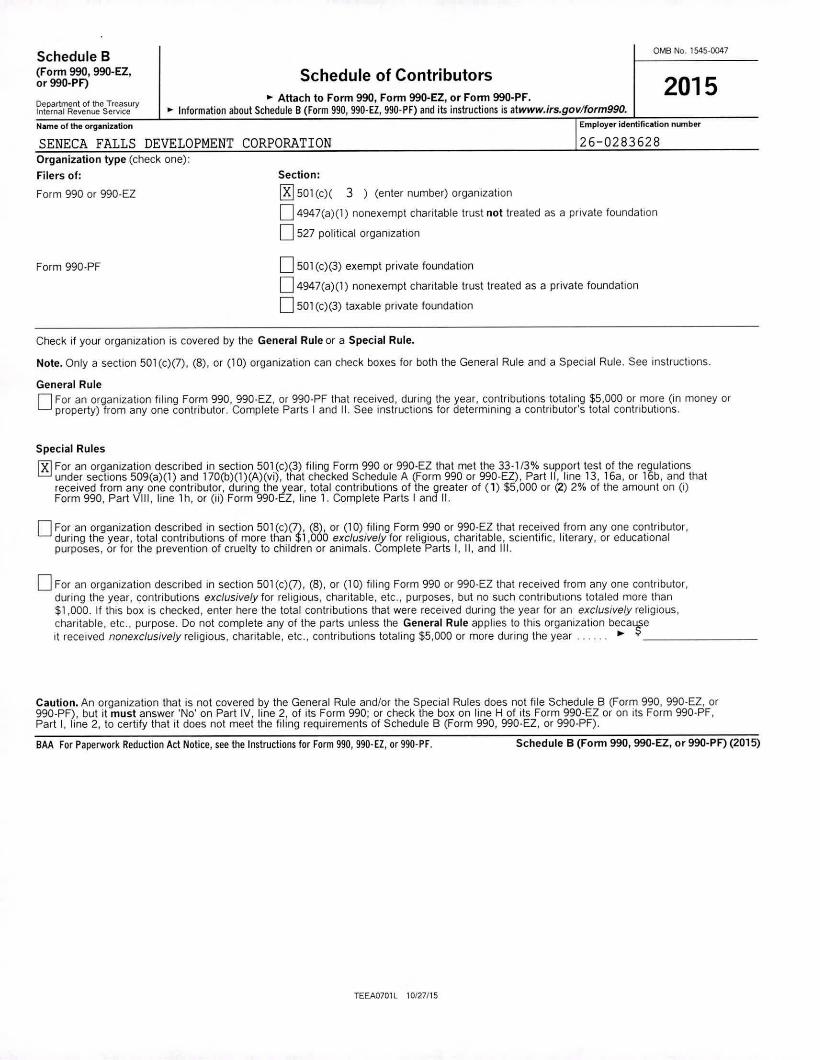
2015Schedule of Contributors~ Attach to Form 990, Fonn 990-EZ, or Fonn 990-PF.
~ Information about Schedule B (Form 990, 990-El, 990.PF) and its instructions is atwww.irs.gov/form990.Employer identification nU'nberName 01 the organization
Department of the TreasuryInlernal Revenue Service
Schedule B(Fonn 990, 990-EZ,or 990-PF)
26-0283628
Section:
00501 (c)( 3 ) (enter number) organizallon
o 4947(a)(1) nonexempt charitable trust not treated as a private foundation
0527 political organization
SENECA FALLS DEVELOPMENT CORPORATIONOrganization type (check one):
Filers of:
Form 990 or 990-EZ
Form 990-PF 0501 (c)(3) exempt private foundation
o 4947(a)(1) nonexempt charitable trust treated as a private foundation
D 501 (c)(3) taxable private foundation
Check if your organization is covered by the General Rule or a Special Rule.
Note. Only a section 501 (c)(7), (8), or (10) organization can check boxes for both the General Rule and a Special Rule. See instructions.
General Ruleo For an organization filing Form 990, 990-£Z, or 990-PF that received, during the year, contributions totaling $5,000 or more (in money orproperty) from anyone contributor. Complete Parts I and II. See instructions for determining a contributor's total contnbutlons.
Special Rules
~ For an organization described in section 501 (c)(3) filing Form 990 or 990.£Z that met the 33- 1/3% support test of the regulationsunder sections 509(a)(I) and 170(b)(I)(A)(vi), that checked Schedule A (Form 990 or 990-EZ), Part II, line 13, 16a, or 16b, and thatreceived from anyone contributor, during the year, total contributions of the greater of (1) $5,000 or (2) 2% of the amount on (i)Form 990, Part VIII, line lh. or (Ii) Form 990-EZ, line 1. Complete Parts I and II.
o For an organization described in section 501 (c)(7), (8), or (10) filing Form 990 or 990-E2 that received .from anyone contributor,during the year, total contnbutions of more than $1,000 exclusively for religious, charitable, sCIentific, lIterary, or educationalpurposes, or for the prevention of cruelty to children or animals. Complete Parts I, II, and Ill.
o For an organization described in section 501 (c)(7), (8), or (10) filing Form 990 or 990.EZ that received from anyone contributor,during the year, contributions exclusively for religious, charitable, etc., purposes, but no such contributions totaled more than$1,000. If this box is checked, enter here the total contributions that were received during the year for an exclusively religious,charitable. etc., purpose. Do not complete any of the parts unless the General Rule applies to this organization beca~eIt received nonexclusively religious, chantable, etc., contributions totaling $5,000 or more during the year.. . . ..•. _
Caution. An organization that is not covered by the General Rule and/or the Special Rules does not file Schedule B (Form 990, 990-£Z, or990-PF), but it must answer 'No' on Part IV, line 2, of its Form 990; or check the box on line H of its Form 990-£2 or on its Form 990-PF,Part I, line 2, to certify that it does not meet the filing requirements of Schedule B (Form 990, 990-£Z, or 990-PF).
BAA For Paperwork Reduction Act Notice, see the Instructions for Form 990, 990-El, or 990-PF. Schedule B (Fonn 990, 990-EZ, or 99O.PF) (2015)
TEEA0701L 10f27115

Employer identification number
26-0.283628Schedule B (Form 990, 990.EZ, or 990.PF) (2015)Name of organization
SENECA FALLS DEVELOPMENT CORPORATIONI Part I I Contributors (see instructions). Use duplicate copies of Part I if addltlOnal space is needed.
Page 1 of 1 of Pari I
(a) (b) (c) (d)Number Name, address, and ZIP + 4 Total Type of contribution
contributions
1 TOWN OF SENECA FALLS Person ~~------------------------------------- Payroll 081 W. BAYARD ST $______ S.1LQ..OQ.:. Noncash 0~-------------------------------------SENECA FALLS, NY 13148 (Complete Part II for~------------------------------------- noncash contributions.)
(a) (b) (c) (d)Number Name, address, and ZIP + 4 Total Type of contribution
contributions
Person 0--- ~------------------------------------- Payroll 0
~------------------------------------- $ Noncash 0-----------(Complete Part II for~------------------------------------- noncash contributions.)
(a) (b) (c) (d)Number Name, address, and ZIP + 4 Total Type of contribution
contributions
Person 0--- r------------------------------------- Payroll 0-------------------------------------- $ Noncash 0-----------
(Compiete Part 11for-------------------------------------- noncash contributions.)
(a) (b) (c) (d)Number Name, address. and ZIP + 4 Total Type of contribution
contributions
Person 0--- -------------------------------------- Payroll 0-------------------------------------- $ Noncash 0-----------
(Complete Part II for-------------------------------------- noncash contnbutions.)
(a) (b) (c) (d)Number Name, address, and ZIP + 4 Total Type of contribution
contributions
Person 0--- -------------------------------------- Payroll 0-------------------------------------- $ Noncash 0-----------
(Complete Part II tor-------------------------------------- noncash contrlbuttons.)
(a) (b) (c) (d)Number Name, address, and ZIP + 4 Total Type of contribution
contributions
Person 0--- -------------------------------------- Payroll 0-------------------------------------- $ Noncash 0-----------
(Complete Part II for-------------------------------------- noncash contributions.)
BAA TEEA0702L 10/12115 Schedule B (Fonn 990, 990-EZ, or 990.PF) (2015)

SENECA FALLS DEVELOPMENT CORPORATION
SCHEDULE 0(Form 990 or 99Q-EZ)
Departmenl of the TreasuryInternal Revenue Service
Name of the orOanizaliOn
Supplemental Information to Form 990 or 990-EZComplete to provide information for responses to specific questions on
Form 990 or 990-EZ or to provide any additional information.~ Attach to Form 990 or 99Q-EZ.
• Information about Schedule 0 (Form 990 or 990.EZ) and its instructions isat www.irs.govlform990.
OMS No. 1545.0047
2015Open to PublicInspection
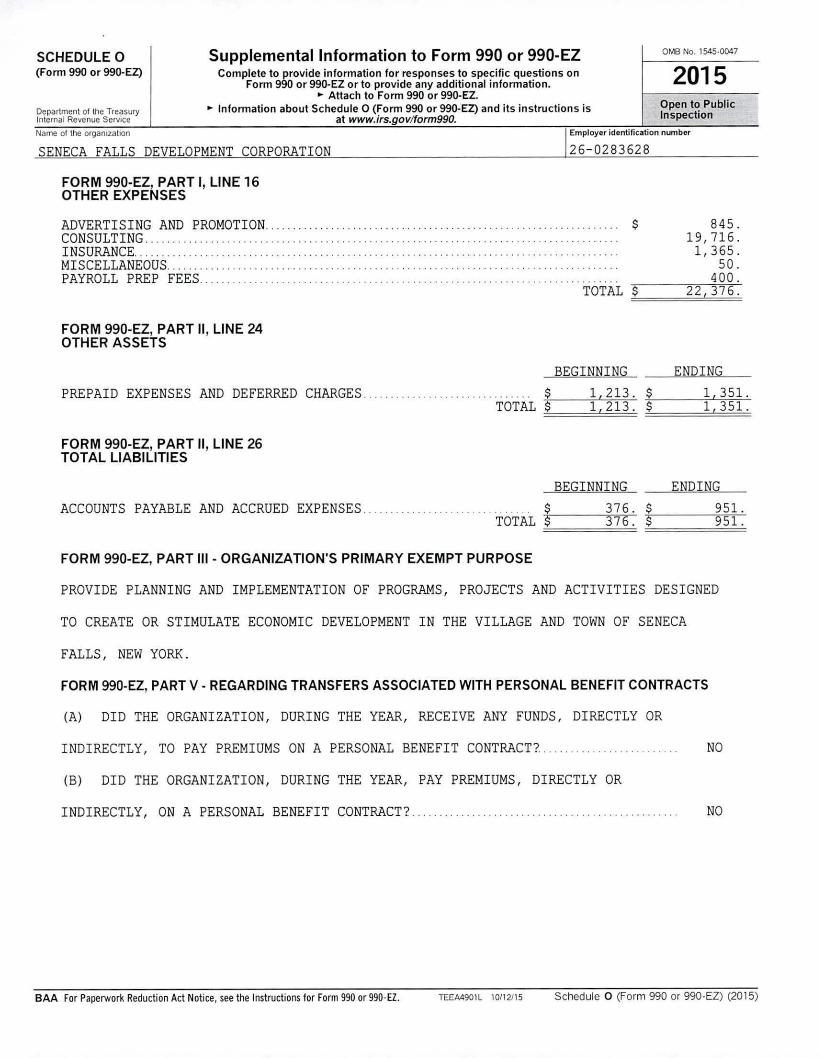
FORM 990-EZ, PART I, LINE 16OTHER EXPENSES
ADVERTISING AND PROMOTION ....CONSULTING .INSURANCE..... . .MISCELLANEOUS .PAYROLL PREP FEES .
FORM 990-EZ, PART II, LINE 24OTHER ASSETS
PREPAID EXPENSES AND DEFERRED CHARGES . TOTAL
FORM 990-EZ, PART II, LINE 26TOTAL LIABILITIES
ACCOUNTS PAYABLE AND ACCRUED EXPENSES............................TOTAL
FORM 990-EZ, PART III - ORGANIZATION'S PRIMARY EXEMPT PURPOSE
$
TOTAL $
BEGINNING$ 1,213. $$ 1,213. $
BEGINNING$ 376. $$ 376. $
845.19,716.1,365.
50.400.
22,376.
ENDING1,351.1,351.
ENDING951.951.
PROVIDE PLANNING AND IMPLEMENTATION OF PROGRAMS, PROJECTS AND ACTIVITIES DESIGNEDTO CREATE OR STIMULATE ECONOMIC DEVELOPMENT IN THE VILLAGE AND TOWN OF SENECAFALLS, NEW YORK.FORM 990-EZ, PART V - REGARDING TRANSFERS ASSOCIATED WITH PERSONAL BENEFIT CONTRACTS
(A) DID THE ORGANIZATION, DURING THE YEAR, RECEIVE ANY FUNDS, DIRECTLY ORINDIRECTLY, TO PAY PREMIUMS ON A PERSONAL BENEFIT CONTRACT? ....(B) DID THE ORGANIZATION, DURING THE YEAR, PAY PREMIUMS, DIRECTLY ORINDIRECTLY, ON A PERSONAL BENEFIT CONTRACT? .....
NO
NO
BAA For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ. TEEA4901 L 10/12115 Schedule 0 (Form 990 or 990.EZ) (2015)
SENECA FALLS DEVELOPMENT CORPORATION
SCHEDULE 0(Form 990 or 990-EZ)
Department of the TreasuryInternal Revenue Service
Name 01 the organlza\lon
Supplemental Information to Form 990 or 990-EZComplete to provide information for responses to specific questions on
Form 990 or 990-EZ or to provide any additional information .• Attach to Form 990 or 990-EZ.
•. Information about Schedule 0 (Form 990 or 990-EZ) and its instructions isat www.irs.govlform990.
OMS No. 1545.0047
2015Open to PublicInspection ••
FORM 990-EZ, PART I, LINE 16OTHER EXPENSES
ADVERTISING AND PROMOTION.CONSULTING. .. ..INSURANCE .MISCELLANEOUS .PAYROLL PREP FEES .
FORM 990-EZ, PART II, LINE 24OTHER ASSETS
............... $ 845.19,716.
. ......... 1,365.50.
. ... , .... 400.TOTAL $ 22,376.
PREPAID EXPENSES AND DEFERRED CHARGES. TOTAL
FORM 990-EZ, PART II, LINE 26TOTAL LIABILITIES
BEGINNING$ 1,213. $$ 1,213. $
ENDING1,351.1,351.
ACCOUNTS PAYABLE AND ACCRUED EXPENSES . ....TOTAL
BEGINNING$ 376. $$ 376. $
ENDING951.951.
FORM 990-EZ, PART 111- ORGANIZATION'S PRIMARY EXEMPT PURPOSE
PROVIDE PLANNING AND IMPLEMENTATION OF PROGRAMS, PROJECTS AND ACTIVITIES DESIGNEDTO CREATE OR STIMULATE ECONOMIC DEVELOPMENT IN THE VILLAGE AND TOWN OF SENECAFALLS, NEW YORK.FORM 990-EZ, PART V • REGARDING TRANSFERS ASSOCIATED WITH PERSONAL BENEFIT CONTRACTS
(A) DID THE ORGANIZATION, DURING THE YEAR, RECEIVE ANY FUNDS, DIRECTLY ORINDIRECTLY, TO PAY PREMIUMS ON A PERSONAL BENEFIT CONTRACT?.....(B) DID THE ORGANIZATION, DURING THE YEAR, PAY PREMIUMS, DIRECTLY ORINDIRECTLY, ON A PERSONAL BENEFIT CONTRACT?.
NO
NO
BAA For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990.EZ. TEEA4901L 10/12115 Schedule 0 (Form 990 or 990.EZ) (2015)

Schedule 0 (Form 990 or 990.EZ) 2015Name of the organization
SENECA FALLS DEVELOPMENT CORPORATIONFORM 990.EZ, PART 111-ORGANIZATION'S PRIMARY EXEMPT PURPOSE
Employer fdentifiClition nUllbe-r
26-0283628
Page 2
BAA
PROVIDE PLANNING AND IMPLEMENTATION OF PROGRAMS, PROJECTS AND ACTIVITIES DESIGNEDTO CREATE OR STIMULATE ECONOMIC DEVELOPMENT IN THE VILLAGE AND TOWN OF SENECAFALLS, NEW YORK.
Schedule 0 (Form 990 or 990.EZ) (2015)TEEA4902l 10112115