invasive aspergillosis ofthe airways: radiographic, ct ... · bronchopneumonia and thenodules...
TRANSCRIPT

P. Mark Logan, FFRRCSI #{149}Steven L. Primack, MD #{149}Roberta R. Miller, MDNestor L. MUller, MD, PhD
Invasive Aspergillosis ofthe Airways:Radiographic, CT, and Pathologic Findings’
383
PURPOSE: To assess the radio-graphic, computed tomographic (CT),
and pathologic findings in invasiveaspergillosis of the airways.
MATERIALS AND METHODS: Thestudy included nine consecutive pa-tients (aged 17-65 years [median, 49yearsl) with pathologically provedinvasive aspergillosis of the airways.All nine underwent chest radiogra-phy and seven underwent CT within
3 days of diagnosis.
RESULTS: The radiographic findingsinclude normal parenchyma (n = 1),unilateral consolidation (n = 1), bilat-eral consolidation (n = 5), and ill-defined nodules (n = 2). The main
findings at CT included lobar con-solidation (ti = 1), bilateral predomi-nantly peribronchial consolidation(ii = 3), ground-glass attenuation(n = 1), and centrilobular nodulesless than 5 mm in diameter (n = 2).At pathologic examination, the pen-bronchial inifitrates representedbronchopneumonia and the nodulesrepresented Aspergillus bronchiolitiswith a variable degree of peribron-chiolar organizing pneumonia andhemorrhage.
CONCLUSION: Radiographic find-ings of invasive aspergillosis of theairways consist of consolidation orill-defined nodules. At CT, the con-solidation can be seen to be penbron-chial and the nodules centrilobular.
Index terms: Aspergillosis, 60.2056 #{149}Bronchi,infection, 60.2056, 671.2056 #{149}Lung, infection,
60.2056
Radiology 1994; 193:383-388
I From the Departments of Radiology (P.M.L,S.LP., N.LM.) and Pathology (R.R.M.), Univer-sity of British Columbia and Vancouver Hospitaland Health Sciences Center, 855 W 12th Aye,Vancouver, BC, Canada, V5Z 1M9. ReceivedApril 12, 1994; revision requested May 17; revi-sion received June 20; accepted June 27. Ad-dress reprint requests to N.L.M.
0 RSNA, 1994
I NVASWE aspergillosis is a relativelycommon pulmonary complication
in the immunocompromised patient.The organisms may invade the bloodvessels of the airways (1). The angio-invasive form leads to ocdusion of
large- or medium-caliber arteries byplugs of hyphae and to developmentof infected infarcts. It is characterizedradiologically by the presence of nod-ules, masslike infiltrates, and subseg-mental and segmental consolidation(2-7). Less commonly, the organismsinvade the airways rather than thevessels. Invasive aspergillosis cen-tered on the airways accounts forl4%-34% of cases (4,8). Airway-inva-sive aspergillosis, like the angioinva-sive form, occurs in immunocompro-mised patients. The diagnosis is basedon the presence of organisms deep tothe basement membrane. Althoughairway-invasive aspergillosis is well
recognized in the pathologic and
clinical literature (9-12), it has re-
ceived little attention in the radiologicliterature.
The aim of this study was to reviewthe radiographic, computed tomo-graphic (CT), and pathologic findingsin invasive aspergillosis of the air-ways.
MATERIALS AND METHODS
All autopsies, open lung biopsies, and
transbronchial biopsies performed at ourinstitution are prosected by a single surgi-
cal pathologist (R.R.M.). This pathologistmaintains a log of all patients who are in-
munocompromised because of malig-nancy, acquired immunodeficiency syn-drome (AIDS), or immunosuppressivechemotherapy, and who undergo autopsyor lung biopsy. Patients receiving onlycorticosteroid therapy were not includedunless there was other evidence of immu-nosuppression. Records from January 1988to July 1993 were reviewed to identifycases of invasive pulmonary aspergillosis;27 were identified. Eighteen (67%) of these
cases were angioinvasive aspergillosis.Nine cases (33%) were infections involv-
ing the airways predominantly or exclu-sively, including cases of tracheobronchi-tis, bronchiolitis, bronchopneumonia, andlobar pneumonia. In all cases, there wasno evidence of a concomitant pulmonaryprocess. These nine patients form the basisfor the present report.
The nine patients included five womenand four men, ranging in age from 17 to
65 years (median, 49 years). All patients
had received immunosuppressive ther-apy. Three patients had undergone bonemarrow transplantation, three had leuke-
mia, one had undergone renal transplan-tation, one had undergone double lungtransplantation, and one had Wegenergranulomatosis. Three of the nine patientswere profoundly leukopenic (absoluteneutrophil count, < 0.5 x 109/L) at the
time of diagnosis (Table 1); two of these
patients had recently received chemo-therapy for leukemia, and one had under-gone renal transplantation. All patientswere first seen with a 1-3-week history offever. Seven patients also gave a history ofcough and dyspnea, and one complainedof chest pain. Auscultation of the lungsrevealed moderate wheeze in three pa-tients.
All nine patients underwent chest radi-ography and seven underwent chest CTwithin 3 days of histologic diagnosis. CTwas performed in seven patients to iden-tify or further delineate pulmonary abnor-
malities and to determine the optimal sitefor biopsy. All CT scans were obtainedwith thin sections (1.0-1.5-mm collima-lion) at 10-mm intervals. The images werereconstructed with a high-spatial-fre-quency algorithm (high-resolution CT).Scans were viewed at standard mediasti-nal windows (level, 35 HU; width, 450I-LU) and lung windows (window level,
-700 HU; width, 1,500 HU).The radiographs and CT scans were as-
sessed by two radiologists (P.M.L, N.L.M),and conclusions were reached by consen-sus. The pathologic specimens were pro-sected by the surgical lung pathologist.The diagnosis of invasive aspergillosis ofthe airways in these nine patients wasmade on the basis of identification of As-pergillus organisms deep to the basementmembrane of the involved airways. Thediagnosis was made at autopsy in fivecases, at open lung biopsy in two cases,and at transbronchial biopsy in two cases.

Figure 1. Patient 2. (a) Chest radiograph of a 49-year-old woman demonstrates consolidation in the right lower lobe. Transbronchial biopsy
demonstrated Aspergillus bronchitis and pneumonia. (b) CT scan (1.5-mm collimation, high-spatial-frequency algorithm) demonstrates the right
lower lobe consolidation.
384 #{149}Radiology November 1994
At our institution, autopsy examination of
the lungs necessitates complete examina-tion of both lungs.
RESULTS
Radiographic features of invasiveaspergillosis of the airways included
normal parenchyma (n = 1), unilat-eral (n = 1) (Fig 1) or bilateral (n = 5)
areas of consolidation, and bilateral
ill-defined nodules 3-5 mm in diam-eter (n = 2) (Fig 2) (Table 1).
Findings in all seven CT examina-tions were abnormal. The main find-
ings at CT included lobar consolida-
tion (n = 1) (Fig 1), bilateral predomi-nantly peribronchial consolidation(n = 3) (Fig 3), ground-glass attenua-
tion (n = 1), and centnlobular nodulesless than 5 mm in diameter (n = 2)
(Table 1). Two patients with peribron-chial consolidation also had bilateral1-5-mm-diameter centrilobular nod-ules (Fig 4) (Table 1). The patient withextensive bilateral ground-glass at-
tenuation and one of the patientswith centrilobular nodules also hadassociated bronchiectasis (Fig 2). Inthe first of these two patients, a CTscan obtained 5 weeks later demon-strated resolution of the ground-glassattenuation but progression of thebronchiectasis. The second patienthad extensive ground-glass attenua-tion and no evidence of bronchiecta-sis on a CT scan obtained 6 weeks
previously.In all cases, at pathologic examina-
Table 1Clinical and Radiologic Data for Nine Patients with Invasive Aspergillosis of the Airways
Patient No.!Sex/Age (y)
Reason forImmunosuppression
Absolute NeutrophilCount (x 109!L) Chest Radiographic Findings Predominant CT Findings
l!M/59 Renal transplant < 0.5 Normal parenchyma Bilateral 5-10-mm-diameter areas of peribron-dual consolidation, occasional halos ofground-glass attenuation
2!F!493�!M/65
LeukemiaLeukemia
Not available*<0.4
Consolidation in right lowerlobeIll-defined small nodules in right
lung and left lower lobe
Consolidation in rightlower lobeCentrilobular micronodules in right lung
and left lower lobe4!F!17 Bone marrow transplant > 4.0 Bilateral ifi-defined nodules Centrilobular micronodules, diffuse
bronchiectasis5*/M/52 Leukemia < 0.5 Bilateral nodular areas of con-
solidationBilateral 1-5-cm-diameter areas of peribron-
dual consolidation, centrilobular micronod-ules
6!F!29 Bone marrow transplant > 1.5 Patchy areas of consolidation ...
7/M!29 Bone marrow transplant > 2.0 Patchy areas of consolidation Bilateral peribronchial consolidation, centri-lobular micronodules
8!F!52 Double lung transplant > 8.0 Patchy consolidation, lowerzone predominance
Diffuse ground-glass attenuation, mild bron-chiectasis, occasional 0.5-2.0-cm-diameternodules
9!F/46 Treatment for Wegenergranulomatosis
> 8.0 Extensive bilateral consolidation ...
* Accurate neutrophil count not available owing to the presence of extensive infiltrates of acute myelogenous leukemia.t This patient had Aspergillus bronchopneumonia in the right lung and left lower lobe without any evidence of angioinvasion. In addition, he had angloinva-
sive aspergillosis with hemorrhagic infarction of the left upper lobe that corresponded to consolidation of the left upper lobe on the radiograph and CT scan.� This patient had nodular areas of attenuation with air crescent formation in the right lung. Although not pathologically proved, these areas of attenuation
were thought to represent angioinvasive aspergillosis coexisting with the pathologically proved airways-invasive disease.

‘I’
d. e.
Volume 193 #{149}Number 2 Radiology #{149}385
tion, Aspergillus organisms were seendeep to the basement membrane (Fig2e) (Table 2). In eight patients, hy-phae were found in the airway lu-mina; in patient 6, hyphae were notseen but were recovered by means ofculture. In seven patients, a neutro-phil-rich inflammatory reaction was
found in association with the de-nuded epithelial cells and hyphae. Alocalized organizing pneumoniawithout neutrophils was found in
I
Figure 2. Patient 4. (a) Chest radiograph of
17-year-old girl demonstrates bilateral ill-defined nodules (arrows) (Fig 2 continues).
patient 3, who was severely neutro-
penic. A mononuclear and poorly
formed granulomatous reaction with-out neutrophils was found in patient6, who lacked stainable hyphae in thebronchioles as mentioned. In six pa-tients, the infiltrates were grosslynodular, and the nodularity was due
to a zone of hemorrhage or organiz-
ing pneumonia surrounding the nor-mal airways (Fig 4). In the two pa-tients who underwent transbronchialbiopsy gross nodularity could not be
assessed, and in patient 9 the infil-trates were confluent without appre-
ciable nodularity. In five of six pa-
tients with either grossly nodularinfiltrates or small areas of peribron-chial consolidation the lung tissuebetween abnormal areas was essen-tially normal, and in patient 7 therewas early diffuse alveolar damage in
the background lung tissue.In seven of the nine patients, there
was no pathologic evidence of con-comitant angioinvasive aspergillosis.Patient 3 had pathologically demon-strated angioinvasive aspergillosiswith an infarct in the left upper lobe.Patient 5 had evidence of only air-way-invasive aspergillosis at open
lung biopsy of the left lower lobe.
However at CT this patient had twopulmonary nodules with halos of
ground-glass attenuation and air cres-cent formation in the right lung (Fig
4). This appearance suggests that the
patient had angioinvasive aspergillo-sis in the right lung coexisting with
pathologically proved airway-inva-
sive aspergillosis in the left lower
lobe.
Two patients had airway-invasiveaspergillosis affecting the trachea or
main-stem bronchi in addition to dis-
ease of the more peripheral airways.
No abnormality of the trachea ormain-stem bronchi was identified atCT in either case.
of the five patients with diseasediagnosed at autopsy, one died of
respiratory failure related to Aspergil-lus infection and the other four diedof other complications related to theirimmunosuppression, with the As per-
gillus infection being a contributing
factor. Follow-up CT in the four re-
maining patients was performed 6
weeks to 6 months after the initialdiagnosis and demonstrated completeclearing of the abnormalities relatedto the Aspergillus infection. One of the
Figure 2. Patient 4 (continued). (b) CT scan(1.5-mm collimation, high-spatial-frequency
algorithm) through the lower lobes showscentrilobular nodules less than 5 mm in di-
ameter (arrows) and diffuse bronchiectasis.
(c) CT scan (1.5-mm collimation, high-spatial-frequency algorithm) further demonstrates
diffuse bronchiectasis and predominantly
centrilobular micronodules (arrow). (d) Patho-
logic specimen of left lower lobe, cut in the
same plane as the CT scan, demonstrates pu-
rulent bronchitis and bronchiolitis (arrows).
(e) Microscopic section (original magnifica-tion, x20) demonstrates bronchiolitis with
Aspcrgillus species invading through bron-
chiolar wall (straight arrows). Also note pen-
bronchiolar inflammation. Adjacent bloodvessel (curved arrow) is normal.

a. b.
Figure 3. Patient 1. (a) CT scan of a 59-year-old man (1.5-mm collimation, high-spatial-fre-quency algorithm) demonstrates localized areas of consolidation in a predominantly peribron-
chial distribution (arrows). (b) Targeted CT scan (1.5-mm collimation, high-spatial-frequency
algorithm) through the left upper lobe demonstrates focal areas of consolidation in a predomi-
nantly penibronchial distribution (arrows).
h1�Figure 4. Patient 5. CT scan of a 52-year-old man (1.5-mm collima-tion, high-spatial-frequency algorithm) demonstrates diffuse cen-tnilobular nodules (white arrows) and a focal area of consolidation
in the left lower lobe (black arrow). At pathologic examination, the
nodule corresponded to bronchiolar-based abscess containing hy-phae in the center surrounded by a zone of organizing pneumonia.
The cavitating mass in the right lung with air crescent formation ispresumed to represent angioinvasive aspergillosis.
386 #{149}Radiology November 1994
two patients with coexistent angioin-vasive disease recovered and one died.
DISCUSSION
In a review of 98 cases of invasiveaspergillosis in patients with cancer,Young et al (8) found that 67 patientshad angioinvasive aspergillosis and31 had invasive aspergillosis of theairways, including bronchitis, bron-
chopneumonia, and lobar pneumoniawithout evidence of vascular inva-sion. In the series of Orr et al (4), 14%of patients were found to have eitherAspergillus bronchitis or broncho-pneumonia. Of 27 cases of invasiveaspergillosis diagnosed at our institu-tion, nine (33%) involved the airwayspredominantly or exclusively.
Both airway-invasive and angioin-vasive aspergillosis have similar clini-cal symptoms. Both occur in immuno-compromised patients. Most patientsare first seen with fever, cough, andprogressive dyspnea. Airway-invasiveaspergillosis differs from allergic bron-chopulmonary aspergillosis, whichclassically occurs as a hypersensitivityreaction, usually in patients withasthma (13). Airway-invasive aspergil-losis is diagnosed on the basis of iden-
tification of organisms deep to thebasement membrane. In allergic bron-chopulmonary aspergillosis, the or-ganisms remain within the airway
lumen. The standard therapy for in-vasive aspergillosis is intravenous ad-ministration of amphotericin B. Allour patients were treated accordingly.Aspergillus organisms caused or con-tributed to the deaths of five of ournine patients (56%); the remainingfour patients completely recoveredafter therapy. These data correspondto the reported 60% mortality rate forpatients with angioinvasive aspergil-losis (14).
The radiologic manifestations ofangioinvasive aspergillosis are wellknown and reflect the presence ofhemorrhagic infarcts. The findingsinclude nodules, masslike infiltrates,and subsegmental and segmental con-solidation (2-6). Findings in recentstudies have suggested that CT mayallow early recognition of angioinva-sive pulmonary aspergillosis by de-picting a characteristic halo ofground-glass attenuation (CT halosign) around the nodules (5,15). Thishalo has been shown at pathologicexamination to represent hemor-rhagic necrosis (6,16).
Another relatively common, albeitlate, finding in invasive pulmonaryaspergillosis is the presence of an air
crescent representing air between re-
tracted, infarcted lung and the adja-
cent lung parenchyma (17). The diag-nosis of invasive aspergillosis of the
airways necessitates that Aspergillusorganisms be identified deep to thebasement membrane of the affectedairways. This is in contradistinction to
allergic bronchopulmonary aspergil-losis, in which the proximal and sub-
segmental airways are dilated andfilled with thick mucus-containingeosinophils and fungal hyphae (13)but in which organisms are not identi-fled deep to the basement membrane.
The radiographic findings of air-way-invasive aspergillosis are non-specific, ranging from normal to
patchy areas of consolidation or bron-chopneumonia (3,8). In the majorityof cases in our series, there was a peri-bronchial or peribronchiolar distribu-tion of abnormalities at CT, rangingfrom centrilobular nodules less than0.5 cm in diameter to peribronchialareas of consolidation up to 5 cm in
diameter. At pathologic inspection,these airway-based infiltrates or nod-
ules were due to Aspergillus organ-
Volume 193 #{149}Number 2 Radiology #{149}387
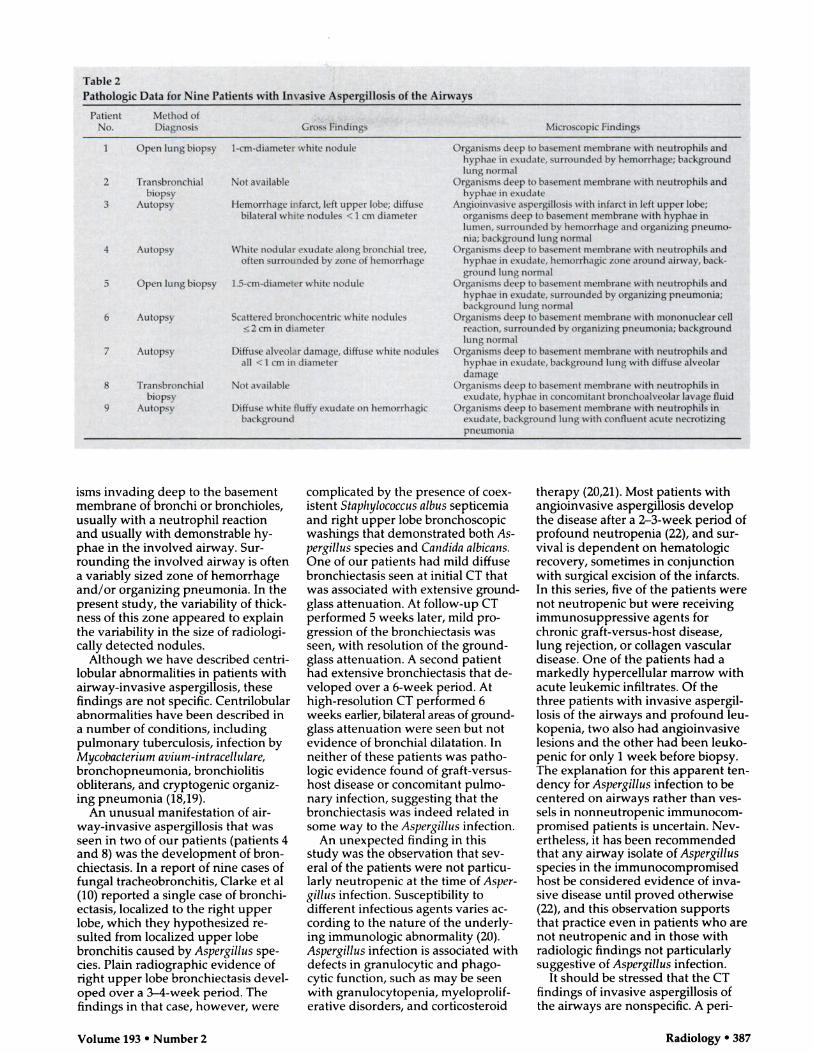
Table 2Pathologic Data for Nine Patients with Invasive Aspergillosis of the Airways
PatientNo.
Method ofDiagnosis Gross Findings Microscopic Findings
1 Open lung biopsy 1-cm-diameter white nodule Organisms deep to basement membrane with neutrophils and
hyphae in exudate, surrounded by hemorrhage; backgroundlung normal
2 Transbronchial Not available Organisms deep to basement membrane with neutrophils andbiopsy hyphae in exudate
3 Autopsy Hemorrhage infarct, left upper lobe; diffuse
bilateral white nodules < I cm diameter
Angioinvasive aspergillosis with infarct in left upper lobe;
organisms deep to basement membrane with hyphae inlumen, surrounded by hemorrhage and organizing pneumo-nia; background lung normal
4 Autopsy White nodular exudate along bronchial tree,often surrounded by zone of hemorrhage
Organisms deep to basement membrane with neutrophils andhyphae in exudate, hemorrhagic zone around airway, back-ground lung normal
5 Open lung biopsy 1.5-cm-diameter white nodule Organisms deep to basement membrane with neutrophils andhyphae in exudate, surrounded by organizing pneumonia;background lung normal
6 Autopsy Scattered bronchocentnc white nodules� 2 cm in diameter
Organisms deep to basement membrane with mononuclear cellreaction, surrounded by organizing pneumonia; backgroundlung normal
7 Autopsy Diffuse alveolar damage, diffuse white nodulesall < I cm in diameter
Organisms deep to basement membrane with neutrophils andhyphae in exudate, background lung with diffuse alveolardamage
8 Transbronchial Not available Organisms deep to basement membrane with neutrophils inbiopsy exudate, hyphae in concomitant bronchoalveolar lavage fluid
9 Autopsy Diffuse white fluffy exudate on hemorrhagicbackground
Organisms deep to basement membrane with neutrophils inexudate, background lung with confluent acute necrotizing
pneumonia
isms invading deep to the basementmembrane of bronchi or bronchioles,
usually with a neutrophil reaction
and usually with demonstrable hy-phae in the involved airway. Sur-rounding the involved airway is oftena variably sized zone of hemorrhageand/or organizing pneumonia. In thepresent study, the variability of thick-ness of this zone appeared to explainthe variability in the size of radiologi-
cally detected nodules.
Although we have described centri-
lobular abnormalities in patients withairway-invasive aspergillosis, these
findings are not specific. Centrilobularabnormalities have been described in
a number of conditions, includingpulmonary tuberculosis, infection byMycobacterium avium-intracellulare,bronchopneumonia, bronchiolitisobliterans, and cryptogenic organiz-ing pneumonia (18,19).
An unusual manifestation of air-way-invasive aspergillosis that was
seen in two of our patients (patients 4and 8) was the development of bron-chiectasis. In a report of nine cases of
fungal tracheobronchitis, Clarke et al(10) reported a single case of bronchi-ectasis, localized to the right upperlobe, which they hypothesized re-sulted from localized upper lobebronchitis caused by Aspergillus spe-
cies. Plain radiographic evidence ofright upper lobe bronchiectasis devel-
oped over a 3-4-week period. Thefindings in that case, however, were
complicated by the presence of coex-
istent Staphylococcus albus septicemia
and right upper lobe bronchoscopic
washings that demonstrated both As-pergillus species and Candida albicans.One of our patients had mild diffusebronchiectasis seen at initial CT that
was associated with extensive ground-
glass attenuation. At follow-up CT
performed 5 weeks later, mild pro-
gression of the bronchiectasis was
seen, with resolution of the ground-
glass attenuation. A second patient
had extensive bronchiectasis that de-
veloped over a 6-week period. At
high-resolution CT performed 6
weeks earlier, bilateral areas of ground-glass attenuation were seen but not
evidence of bronchial dilatation. Inneither of these patients was patho-
logic evidence found of graft-versus-host disease or concomitant pulmo-
nary infection, suggesting that the
bronchiectasis was indeed related in
some way to the Aspergillus infection.
An unexpected finding in thisstudy was the observation that sev-
eral of the patients were not particu-larly neutropenic at the time of As per-
gillus infection. Susceptibility to
different infectious agents varies ac-cording to the nature of the underly-
ing immunologic abnormality (20).
Aspergillus infection is associated withdefects in granulocytic and phago-
cytic function, such as may be seen
with granulocytopenia, myeloprolif-erative disorders, and corticosteroid
therapy (20,21). Most patients with
angioinvasive aspergillosis develop
the disease after a 2-3-week period of
profound neutropenia (22), and sur-vival is dependent on hematologic
recovery, sometimes in conjunctionwith surgical excision of the infarcts.In this series, five of the patients werenot neutropenic but were receiving
immunosuppressive agents forchronic graft-versus-host disease,lung rejection, or collagen vascular
disease. One of the patients had a
markedly hypercellular marrow with
acute leukemic infiltrates. Of the
three patients with invasive aspergil-
losis of the airways and profound leu-
kopenia, two also had angioinvasive
lesions and the other had been leuko-
penic for only 1 week before biopsy.The explanation for this apparent ten-dency for Aspergillus infection to becentered on airways rather than yes-
sels in nonneutropenic immunocom-
promised patients is uncertain. Nev-
ertheless, it has been recommendedthat any airway isolate of Aspergillusspecies in the immunocompromisedhost be considered evidence of inva-
sive disease until proved otherwise
(22), and this observation supports
that practice even in patients who are
not neutropenic and in those with
radiologic findings not particularlysuggestive of Aspergillus infection.
It should be stressed that the CTfindings of invasive aspergillosis of
the airways are nonspecific. A pen-

388 #{149}Radiology November 1994
bronchial or peribronchiolar distribu-tion of abnormalities has been de-scribed in patients with viral, fungal,
and mycobacterial infection and inpatients with bronchiolitis obliteransorganizing pneumonia (1,6). How-ever, a high degree of suspicion forinvasive disease of the airways shouldbe maintained if there is any airwayisolate of Aspergillus species in an im-munocompromised host, even in anonneutropenic patient who does nothave the characteristic radiologicfindings. Nevertheless, biopsy or cul-lure proof of the diagnosis of invasiveaspergillosis of the airways is still de-
sirable before instituting therapy. #{149}
References1. Williams DM, KrickJA, Remington JS.
Pulmonary infection in the compromisedhost. Am Rev Respir Dis 1976; 114:359-394.
2. Klein DL, Gamsu G. Thoracic manifesta-
tions of aspergillosis. AJR 1980; 134:543-552.
3. Gefter WB. The spectrum of pulmonaryaspergillus. J Thorac Imaging 1992; 7:56-74.
4. Orr DP, Myerowitz RL, Dubois PJ. Patho-radiologic correlation of invasive pulmo-nary aspergillosis in the compromised host.Cancer 1978; 41:2028-2039.
5. Kuhlman JE, Fishman EK, Burch PA, KarpJE, Zerhouni EA, Siegelman SS. CT of in-
vasive pulmonary aspergillosis. AJR 1988;150:1015-1020.
6. Brown MJ, Miller RR, Muller NL. Acutelung disease in the immunocompromisedhost: CT and pathologic findings. Radiol-ogy 1994; 190:247-254.
7. Mori M, GlavinJR, Barloon TJ, GingrichRD. Stanford W. Fungal pulmonary in-fections after bone marrow transplanta-tion: evaluation with radiography and CT.Radiology 1991; 178:721-726.
8. Young RC, Bennett JE, Vogel CL, CarbonePP, DeVita VT. Aspergillosis: the spec-trum of disease in 98 patients. Medicine1970; 49:147-173.
9. Okudaira M, SchwarzJ. Tracheobroncho-pulmonary mycoses caused by opportunis-tic fungi, with particular reference to as-pergillosis. Lab Invest 1962; 11:1053-1064.
10. Clarke A, SkeltonJ, Fraser RS. Fungal tra-
cheobronchitis: report of 9 cases and re-view of the literature. Medicine 1991; 70:1-14.
11. Tazelaar HD, Baird AM, Mill M, GrimesMM, Schulman LL, Smith CR. Broncho-
centric mycosis occurring in transplant re-cipients. Chest 1989; %:92-95.
12. Kramer MR, Denning DW, Marshall SE, etal. Ulcerative tracheobronchitis after lungtransplantation: a new form of invasiveaspergillosis. Am Rev Respir Dis 1991; 144:552-556.
13. Fraser RS, Par#{233}jAP, Fraser RG, Pare PD.Synopsis of diseases of the chest. 2nd ed.Philadelphia, Pa: Saunders, 1994; 347-351.
14. Albelda SM, Talbot GH, Gerson SL, MillerWT, Cassileth PA. Pulmonary cavitationand massive hemoptysis in invasive pal-
monary aspergillosis. Am Rev Respir Dis1985; 131:115-120.
15. KuhhnanJE, Fishman EK, Burch PA, et aLInvasive pulmonary aspergillosis in acuteleukemia: the contribution of CT to earlydiagnosis and aggressive management.
Chest 1987; 92:95-99.16. Hruban RH, Meziane MA, Zerhouni EA,
Wheeler PS, DumlerJS, Hutchins GM.Radiologic-pathologic correlation of the CThalo sign in invasive pulmonary aspergillo-sis. J Comput Assist Tomogr 1987; 11:534-536.
17. Curtis AMB, Smith GJW, Ravin CE. Aircrescent sign of invasive pulmonary asper-gillosis. Radiology 1979; 133:17-21.
18. Gruden JF, Webb WR, Warnock M. Cen-trilobular opacities in the lung on high-resolution CT: diagnostic considerationsand pathologic correlation. AJR 1994; 162:569-574.
19. Lee KS, Kuilnig P, Hartman TE, Muller NL.Cryptogenic organizing pneumonia: CTfindings in 43 patients. AIR 1994; 162:543-546.
20. FishmanjA. Diagnostic approach topneumonia in the immunocompromised
host. Semin Respir Inf 1986; 1:133-144.21. Ettinger NA, TrU1OCk liP. Pulmonary con-
siderations of organ transplantation. AmRev Respir Dis 1991; 144:213-223.
22. Moreau P, ZaharJR, Milpied N, et al. Lo-calized invasive pulmonary aspergillosis inpatients with neutropenia. Cancer 1993;72:3223-3226.