invasion and metastasis dr wirsma arif harahap surgical oncologist
TRANSCRIPT
Invasion and MetastasisDr Wirsma Arif Harahap
Surgical Oncologist

• Benign tumors generally do not spread by invasion or metastasis
• Malignant tumors are capable of spreading by invasion and metastasis
Malignant versus Benign Tumors

1. Biology of tumor growth
2. Tumor angiogenesis
3. Tumor progression and heterogeneity
4. Cancer Cells and Microeviroment
5. Tumor spread
OBJECTIVE

1. Biology of tumor growth
2. Tumor angiogenesis
3. Tumor progression and heterogeneity
4. Cancer Cells and Microeviroment
5. Tumor spread
OBJECTIVE

1. Biology of tumor growth
The natural history of malignant tumors can be divided into four phase:
A. Transformation B. Growth of transformation cells C. Local invasion D. Distant metastases

Tumor growth
(a) Rate of growth
Benign: slowly years to decades
Malignant: rapidly moths to years

(b) Pattern of growth
① Expansile a. Well-demarcated and
encapsulated b. Gradually c. Surgically enucleated easely. d. The particular growth pattern
of benign tumors

Expansile Growth pattern

② Invasive
a. Progressive infiltration, invasion, and destruction of the surrounding tissue
b. Ill-defined and non-encapsuled
c. The particular growth pattern of malignant tumors
d. Be surgically enucleated difficultly

Invasive growth pattern

③ Exospheric
a. Tumors growth projecting on the surface, booty cavities, or the lumen
b. Commonly polyp, mushroom, and finger-like
c. Growth pattern of both benign and malignant tumors

Exospheric growth pattern
1. Biology of tumor growth
2. Tumor angiogenesis
3. Tumor progression and heterogeneity
4. Cancer Cells and Microeviroment
5. Tumor spread
OBJECTIVE

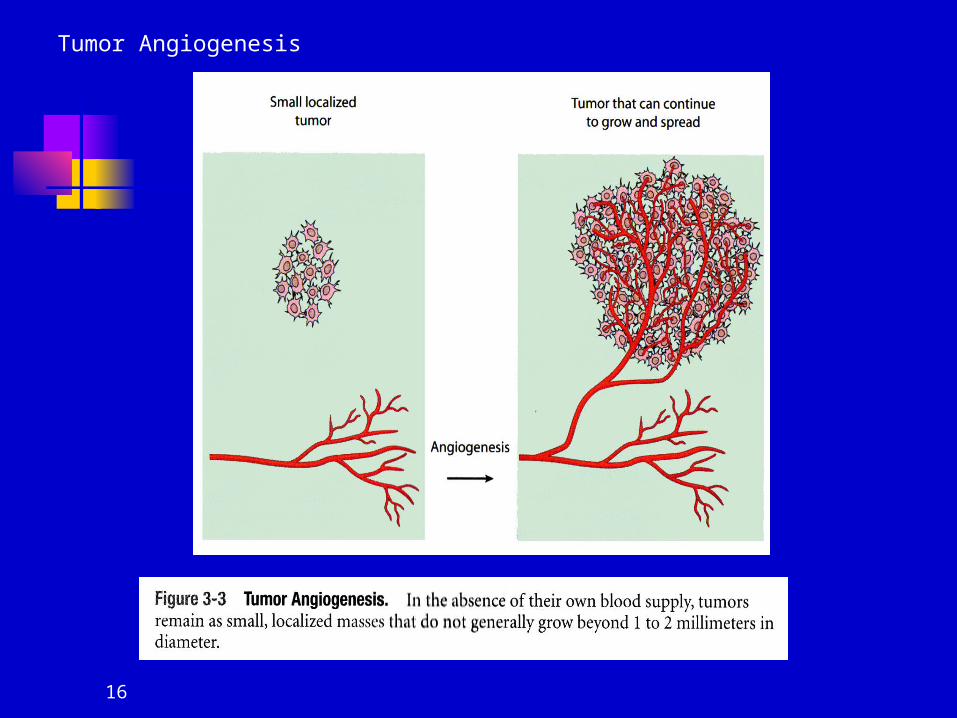
(2) Tumor angiogenesis Angiogenesis is necessary for biologic
correlate of malignancy.
Development cancer > 1mm hypoxia cell cancer release hif ( hipoxia inducing factor ) endothel release VEGF ( vascular endothelial growth fc)
VEGF angiogenesis

15
Tumor Angiogenesis
16
Tumor Angiogenesis

Angiogenesis is required for tumors to grow beyond a few millimeters in diameter
► In 1971, Judah Folkman, signal molecules for new blood vessel formation
► Tumor angiogenesis The processes of cancer cells
stimulate the development of a blood supply

18
Tumor Angiogenesis

1. Biology of tumor growth
2. Tumor angiogenesis
3. Tumor progression and heterogeneity
4. Cancer Cells and Microeviroment
5. Tumor spread
OBJECTIVE
(3) Tumor progression and heterogeneity
Despite most malignant tumors are monoclonal in origin, by the time they become clinically evident, their constituent cells are extremely heterogeneous resulting from multiple mutations that accumulate independently in different cells.
1. Biology of tumor growth
2. Tumor angiogenesis
3. Tumor progression and heterogeneity
4. Cancer Cells and Microeviroment
5. Tumor spread
OBJECTIVE
4. Cancer Cells and Microeviroment
Cancer cells cannot growth by itself It is need support by
microenviroment (stromal). Lack of supporting cancer cells
will die.
Tumor Tumor CellsCells
-Epithelial-Epithelial
-Mesenchymal-Mesenchymal
--HematopoieticHematopoietic
MicroenvironmentMicroenvironment
-Fibroblasts/-Fibroblasts/MyofibroblastsMyofibroblasts
-Endothelial CellsEndothelial Cells
-Myoepithelial CellsMyoepithelial Cells
-LeukocytesLeukocytes
-Extracellular Matrix-Extracellular Matrix
-Usually Bulk of TumorUsually Bulk of Tumor

Bi-directional Interactions Bi-directional Interactions between Cancer cells and between Cancer cells and
enviromentenviroment
Microenvironment can contribute positive or negative signals to tumor cells: signalsmay be mediated by bioactive productsor cell-cell contact
Tumor cells modify the microenvironment to produce bioactive products such as growth factors, chemokines, matrix-degrading enzymes that enhance the proliferation,survival, invasion, and metastasis of tumor cells.
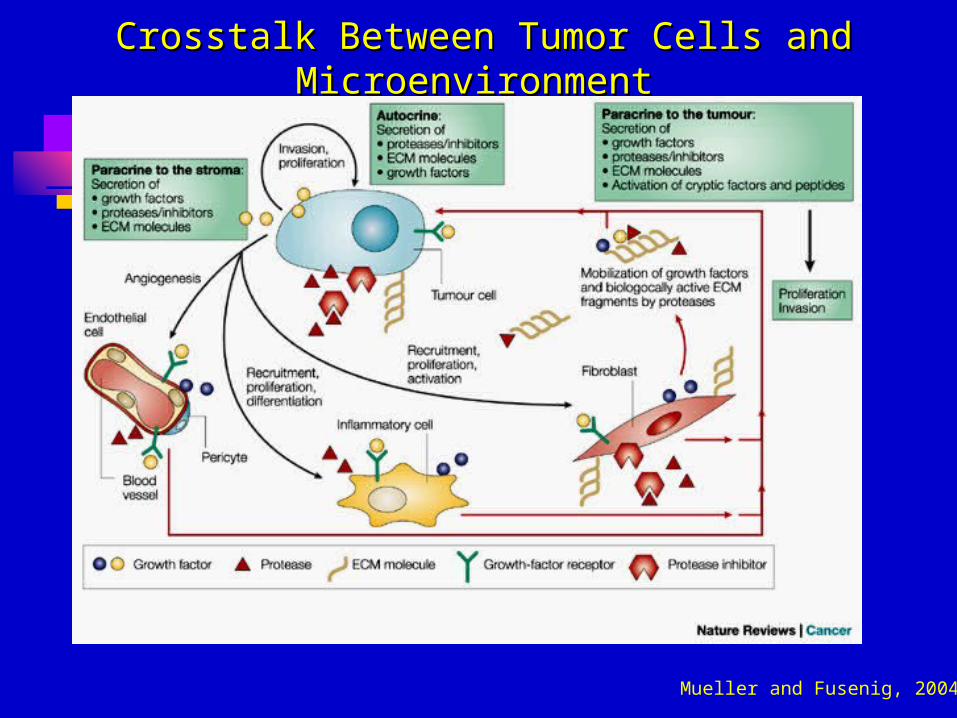
Crosstalk Between Tumor Cells and Crosstalk Between Tumor Cells and MicroenvironmentMicroenvironment
Mueller and Fusenig, 2004
1. Biology of tumor growth
2. Tumor angiogenesis
3. Tumor progression and heterogeneity
4. Cancer Cells and Microeviroment
5. Tumor spread
OBJECTIVE

5. Tumor spread
The spread is a cheracteristic of malignant tumors
(1) Local invasion(2) Metastasis

The steps and mechanism of invasion :
i. Cancerous cells attaching basement
membrane. ii. Local proteolysis iii. Locomotion
Cancers cells invade, penetrate local tissue fissure progressively.
1. Local Invasion

The three steps of invasion
Liotta, LA. Tumor invasion and metastasis-role of the extracellular matrix. Cancer Res 46: (1986)
1
Matrix attachment
2
Matrix degradation
Locomotion
3

How do cells move through tissues? Acquire invasive ability
Ability to degrade extracellular matrix (ECM)
Acquire motile ability Lose cell-cell junctions (EMT-like switch) Acquire motile capability
Directed migration to hospitable sites Chemotaxis Communication between tumor and host
cells

31
Cell motility activation By signal molecules From cancer cells or surrounding cells
Proteases production To remove cancer cell movement
barriers Plasminogen activator (plasminogen
→ plasmin) (fig. 3-9)
How do cells move through tissues?Cont..

32
Invasion and Metastasis

Matrix degradation by proteinases
Metalloproteinases (MMPs)Serine proteinases (plasmin, uPA)Cysteine proteinase (Cathepsin B,L)
Aspartyl proteinases (Cathepsin D)Threonine proteinases (not extracellular)

(2) Metastasis
Definition: metastasis connotes the development of secondary implants discontinuous with the primary tumor, possibly in remote tissue.

35
Distant Metastasis
Cancer Cells Follow The blood stream
Growth in anotherOrgan

Invasion and Metastasis

Figure 14.4 The Biology of Cancer (© Garland Science 2007) p. 591
Invasion-Metastasis Cascade Adapted from Fidler, Nat. Rev. Cancer 3: 453-458, 2003

Colon Carcinoma Metastatic to Liver
Breast Carcinoma Metastatic to Brain
Fig. 2.2b and c
Weinberg
p. 27

Organ-specific factors play a role in determining where cancer cells will metastasize
► Seed and soil hypothesis► Only a few sites provide an optimal
environment for the growth for a particular type of cancer cell
► The ability of cancer cells to grow in different locations is affected by interactions between cancer cells and molecules present in the specific organs

① Lymphatic metastasis a. This is the most common pathway
for initial dissemination of carcinoma.
b. Tumor cells gain access to an afferent lymphatic channel and carried to the regional lymph nodes.
In lymph nodes, initially tumor cell are confined to the subcapsular sinus; with the time, the architecture of the nodes may be entirely destroyed and replaced by tumor.

c. Through the efferent lymphatic channels tumor may still be carried to distanced lymph rode, and enter the bloodstream by the way of the thoracic duct finally.
d. Destruction of the capsule or infiltration to neighboring lymph nodes eventually causes these nodes to become firm, enlarged and matted together.

Metastasis via Lymphatics
Lymphatic Drainage of the Breast
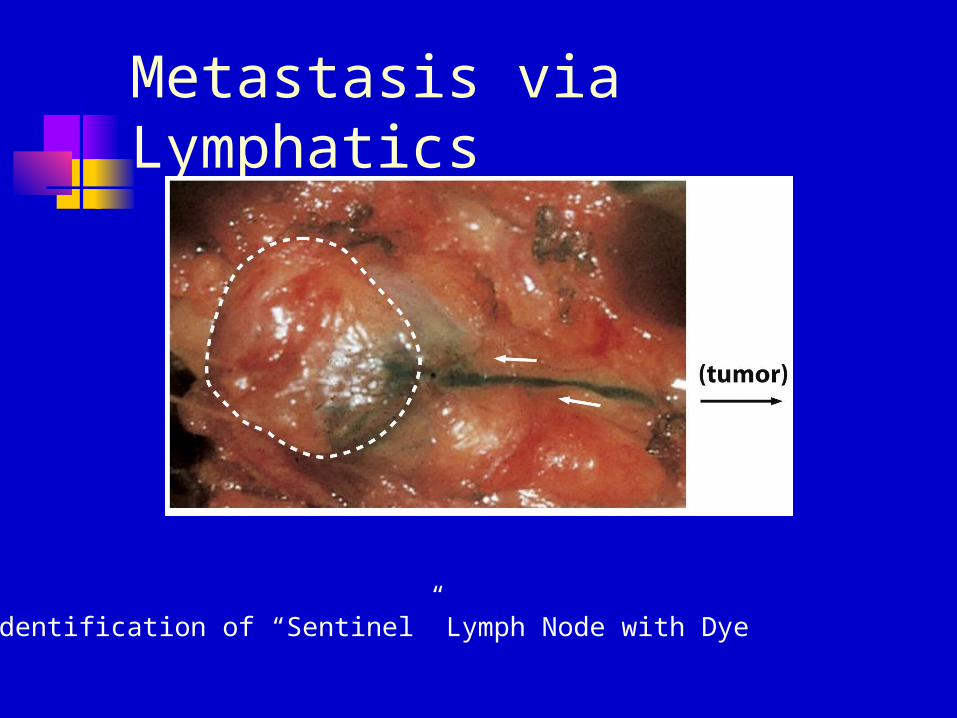
Metastasis via Lymphatics
Identification of “Sentinel” Lymph Node with Dye

Metastasis via Lymphatics
H&E Staining: Breast Ca in Lymph Node

Metastasis via Lymphatics
Keratin Staining: Breast Ca in Lymph Node
② Hematogenous metastasis
a. This pathway is typical of sarcoma but is also used by carcinoma
b. Process: tumor cells →small blood vessels→ tumor emboli→ distant parts→ adheres to the endothelium of the vessel→ invasive the wall of the vessel→ proliferate in the adjacent tissue→ establish a new metastatic tumor.
c. follow the direction of blood flow. Tumors entering the superior or inferior vena cava will be carried to the lungs tumors entering the portal system will metastasize to the liver.
d. Some cancers have preferential sites for metastases lung cancer offal metastasize to the brain, bones, and adrenal glands.
Prostate cancer frequently metastasize to the bones.
e. Morphologic features of metastasis tumors multiple, circle, scatter

③ Implantation metastasis
a. Tumor cells seed the surface of body cavities
b. Most often involved is the peritoneal cavity
c. But also may affect pleural, pericardial, subarachnoid, and joint space.

Mechanisms of invasion and metastasis
① Invasion of the extracellular metastasis
a. Loosening up of tumor cells from each other: E-adhering expression is reduced
b. Attachment to matrix components: cancer cells have many more receptors of lamina and fibronectin.
c. Degradation of extra cellular matrix:Tumor cells can secrete proteolytic enzymes
or induce host cells to elaborate proteases.

② Vascular dissemination and homing of tumor cells
a. Tumor cells may also express adhesion molecules whose ligands are expressed preferentially on the endothelial cells of target organ.
b. Some target organs may liberate chmoattractonts that tend to recruit tumor cells to the site. e. g. insulin-like growth factor Ⅰ, Ⅱ.
c. In some cases, the target tissue may be not an permissive environment. i. g. inhibitors of proteases could prevent the establishment of mend of a tumor cottony.
③ Molecular genetics of metastases
At present, no single “metastasis gene” has been found, just son conciliates
a. High expression of nm23 gene often accompanied with low metastatic potential.
b. KAI-I gene, located on 11pn-2, expressed in normal prostate but not in metastasis prostate cancer.
c. KISS gene, also located on human chromosome Ⅱ, analogous manner in human malignant melanoma.

(Quoted fromRobbins 《 PathologyBasis of disease 》 )

Figure 14.42 The Biology of Cancer (© Garland Science 2007) p. 635
Primary Tumors and Preferred Sites of Metastatic Spread

Presence of Micrometastases and Clinical Prognosis: Colon Cancer
Figure 14.50b The Biology of Cancer (© Garland Science 2007) p. 645

Factors Hindering Metastatic Spread
1. Metastasis-Suppressor Genes:e.g. - TIMP: Tissue Inhibitor of Metalloproteinases
- CAD1 gene: for E-cadherin
2. Host Responses Activated Macrophages Natural Killer Cells Cytotoxic Lymphocytes
3. Hydrodynamic Effects in Host circulation
4. Failure to Recognize and Arrest at Secondary SiteStopMets

56
Specific genes promote or suppress the ability of cancer cells to metastasize
► Matrix metalloproteinases (MMPs) inhibitors can inhibit cancer cells metastasis
► Metastasis promoting genes MMPs
► cancer cells Enhancement of metastasis promoting
genes Diminishing of metastasis suppressor genes

Routes of tumor spread• Hematogenous (bloodstream)
sarcomas, carcinomas, leukemias
• Lymphatic (lymph nodes)carcinomas
• Direct extension (surface implantation, ascites) ovarian, other carcinomas

Organ site preference for metastasis
Colon adenocarinoma LiverBreast adenocarcinoma Bone, brain, adrenalProstate adenocarcinoma BoneLung: SCLC Bone, brain, liverMelanoma - cutaneous Brain, liver, colonThyroid adenocarcinoma BoneKidney clear cell carcinoma Bone, liver, thyroidTestis carcinoma LiverBladder carcinoma BrainNeuroblastoma Liver, adrenal
Lung and liver: common sites of metastasis