introduction - weber state universityradpacs.weber.edu/images/s_clampitt/05-mri_prostate mri.pdf ·...
TRANSCRIPT

Amir Fuad Hussain
INTRODUCTIONProstate cancer:More common in Western vs Asian countriesHowever, high incidence is seen among Asian immigrants to Western countries within one generation – possible predisposing environmental factorsIn Malaysia, 6th most frequent cancer & accounts for 5.7% of cancers in malesIn Malaysia, among the major ethnic groups, the Chinese record the highest incidence of this cancer – possible predisposing genetic factorsA diet high in fats ‐ also associated with a higher incidence Source: Malaysian Oncological Society website URL: http://www.malaysiaoncology.org/article.php?aid=32
INTRODUCTIONProstate cancer:Symptoms‐ dysuria, haematuria, urgency+/‐ frequency of micturition, bone painDiagnosis – combination of DRE & PSA. MRI findings alone are non‐specific and may be similar to prostatitis, prostatic abscess & BPHConfirmation of diagnosis – Transrectal biopsy under ultrasound guidanceStaging – CT , MRI, Bone scanTreatment: Surgery, Hormonal treatment, radiotherapySource: Malaysian Oncological Society website URL: http://www.malaysiaoncology.org/article.php?aid=32
INTRODUCTIONImaging in Prostate cancer:CT – conventional thorax, abdomen, pelvis – to look for metastasesMRI – to assess intrapelvic diseaseBone scan – to assess distribution of bony metastases
Source: Malaysian Oncological Society website URL: http://www.malaysiaoncology.org/article.php?aid=32

PROSTATE MRIIs the most accurate non‐invasive method for staging local extent of prostate caHas become the definitive test for determining treatment options (e.g. surgery vs radiotherapy)Development of the endorectal coil has increased the accuracy of detection to 82% (compared to 66‐69% using the body coil)
Source: R Harris, A Schned, J Heaney – Staging of Prostate Cancer with Endorectal MR Imaging: Lessons from a learning curve – Radiographics 1995 Vol 15 No 4
PROSTATE MRIThe combination of conventional T2‐weighted sequences AND MR Spectroscopy has been shown to improve cancer detection, localization of cancers in the peripheral & transitional zones of the prostateCombination MR + MRS: Sensitivity 91% Specificity 95%MR alone: Sensitivity 77% Specificity 81%
Source: Choi et al– Functional MR Imaging of Prostate Cancer– Radiographics 2007 Vol 27 No 1
PROSTATE MRI – advantages of MRI over other imaging modalities
It does not use ionizing radiation.
It can obtain images in sagittal, coronal, axial, and/or oblique planes.
It provides more soft tissue contrast than other radiological techniques, and PC has low signal intensity as compared to surrounding regions of healthy tissue. This decrease in signal intensity is due to differences in structure between cancerous and normal prostate tissue.
Endorectal/pelvic phased array coil MRI has demonstrated higher accuracy than other modalities in assessing seminal vesicle invasion and extra‐capsular extension (ECE) of PC (96% and 81%r respectively)*Within the same exam, endorectal MRI can also be used to assess the possibility of PC spread to lymph nodes and bones within the pelvis and close to the prostate.
*Source: Hricak H, White S, Vigneron D, et al: Carcinoma of the prostate gland: MR imaging with pelvic phased‐array coils versus integrated endorectal— pelvic phased‐array coils. Radiology 193:703‐9, 1994
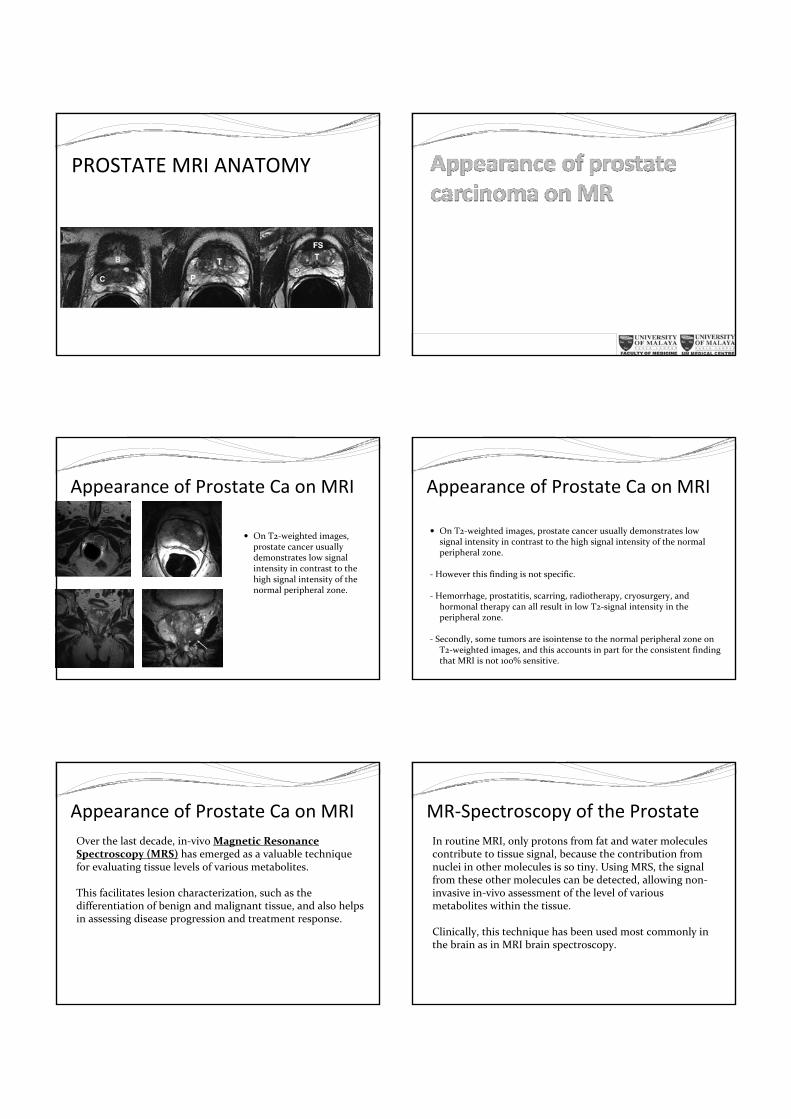
PROSTATE MRI ANATOMYOn T1‐weighted MR images, the normal prostate gland demonstrates homogeneous intermediate to‐low signal intensity. However T1‐weighted MR imaging has insufficient soft‐tissue contrast resolution for visualizing the intraprostatic anatomy or abnormality.
The zonal anatomy of the prostate gland is best depicted on high‐resolution T2‐weighted images. On T2‐weighted images, the normal peripheral zone demonstrates a high signal intensity. The signal intensities in the central and transition zones are lower than those in the peripheral zone. The anterior fibromuscular stroma has low signal intensity.
PROSTATE MRI ANATOMY
PROSTATE MRI ANATOMY
Appearance of Prostate Ca on MRI
On T2‐weighted images, prostate cancer usually demonstrates low signal intensity in contrast to the high signal intensity of the normal peripheral zone.
Appearance of Prostate Ca on MRI
On T2‐weighted images, prostate cancer usually demonstrates low signal intensity in contrast to the high signal intensity of the normal peripheral zone.
‐ However this finding is not specific.
‐ Hemorrhage, prostatitis, scarring, radiotherapy, cryosurgery, and hormonal therapy can all result in low T2‐signal intensity in the peripheral zone.
‐ Secondly, some tumors are isointense to the normal peripheral zone on T2‐weighted images, and this accounts in part for the consistent finding that MRI is not 100% sensitive.
Appearance of Prostate Ca on MRIOver the last decade, in‐vivo Magnetic Resonance Spectroscopy (MRS) has emerged as a valuable technique for evaluating tissue levels of various metabolites.
This facilitates lesion characterization, such as the differentiation of benign and malignant tissue, and also helps in assessing disease progression and treatment response.
MR‐Spectroscopy of the ProstateIn routine MRI, only protons from fat and water molecules contribute to tissue signal, because the contribution from nuclei in other molecules is so tiny. Using MRS, the signal from these other molecules can be detected, allowing non‐invasive in‐vivo assessment of the level of various metabolites within the tissue.
Clinically, this technique has been used most commonly in the brain as in MRI brain spectroscopy.
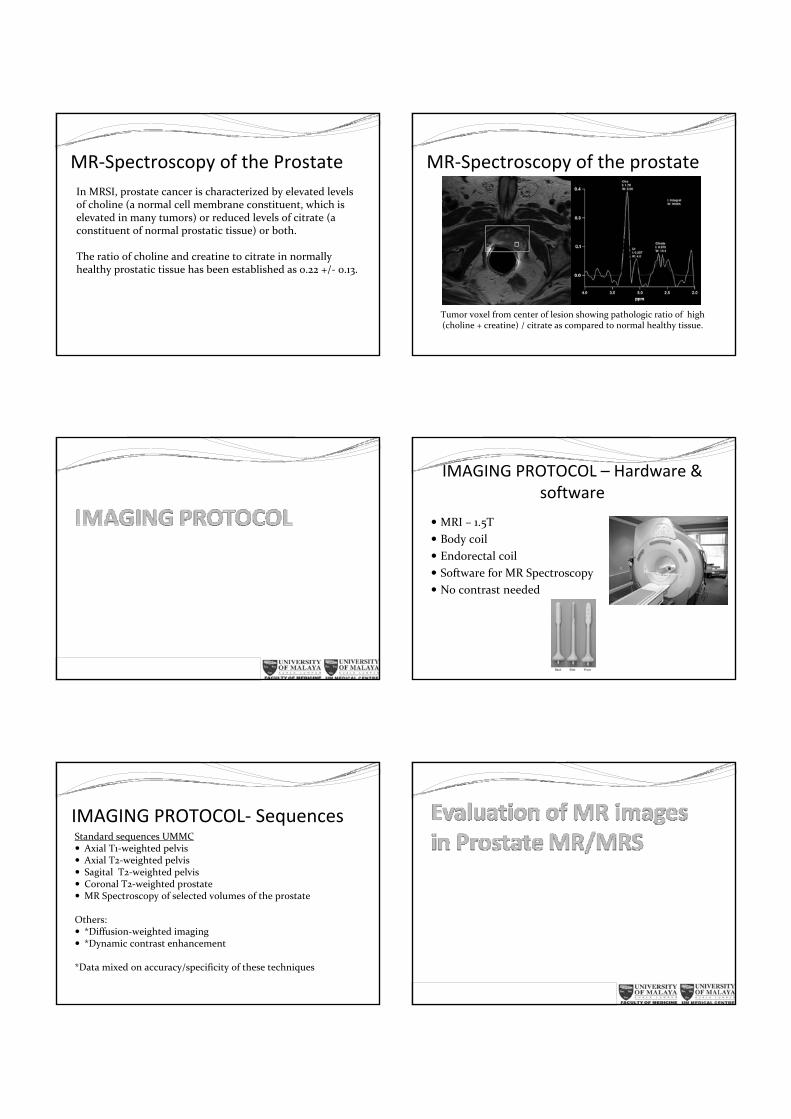
MR‐Spectroscopy of the ProstateIn MRSI, prostate cancer is characterized by elevated levels of choline (a normal cell membrane constituent, which is elevated in many tumors) or reduced levels of citrate (a constituent of normal prostatic tissue) or both.
The ratio of choline and creatine to citrate in normally healthy prostatic tissue has been established as 0.22 +/‐ 0.13.
MR‐Spectroscopy of the prostate
Tumor voxel from center of lesion showing pathologic ratio of high (choline + creatine) / citrate as compared to normal healthy tissue.
IMAGING PROTOCOL – Hardware & software
MRI – 1.5T Body coilEndorectal coilSoftware for MR SpectroscopyNo contrast needed
IMAGING PROTOCOL‐ SequencesStandard sequences UMMC
Axial T1‐weighted pelvisAxial T2‐weighted pelvisSagital T2‐weighted pelvisCoronal T2‐weighted prostateMR Spectroscopy of selected volumes of the prostate
Others:*Diffusion‐weighted imaging*Dynamic contrast enhancement
*Data mixed on accuracy/specificity of these techniques

Evaluation of MR Images in Prostate Carcinoma
Carcinoma usually from PZ – appear as hypointense lesion Extracapsular extension : irregular bulging of the prostatic outline, breach of the capsule with extracapsular spread, asymmetry of the neurovascular bundles, and loss of the rectoprostatic angle.Invasion of seminal vesicles ‐ Contiguous areas of low signal intensity extending into the seminal vesicles from the base of the prostate (Note – this also may be seen post‐radiotherapy & post‐biopsy)Invasion of bladder/rectumLymph nodes – lymph nodes >1 cm considered involved
T2‐weighted axial MRI‐
Hypointense lesion in the peripheral zone
Axial T2WI
Hypointense lesion in the right PZ, with focal bulge and loss of the rectoprostatic angle
‐ Extracapsular extension and involvement of the neurovascular bundle
Axial T2WI
Benign prostatic hypertrophy
Nodular enlargement of the transitional zoneCompression of the PZLow intensity fibrous capsule
Coronal T2WI
Benign prostatic hypertrophy
Enlarged transitional zoneNormal deliniation of zonal anatomy on T2WI
Coronal T2WI – nodular hypointense lesions in the PZ ‐Carcinoma

Coronal T2WI –
Hypointensity within the right seminal vesicle –seminal vesicle involvement
Abnormally high Ch+Cr/Ci ratio‐carcinoma
Normal – Ci peak higher than Ch_CR =
Thank you