introduction of complementary foods and the relationship...
TRANSCRIPT

Introduction of Complementary Foods and theRelationship to Food Allergy
WHAT’S KNOWN ON THIS SUBJECT: Breast milk is protectiveagainst many conditions, but its role in allergy has not beenestablished. Infant-feeding recommendations support exclusivebreastfeeding for 26 weeks, whereas allergy preventionrecommendations advise exclusive breastfeeding for 4 to 6months with continued breastfeeding thereafter.
WHAT THIS STUDY ADDS: Evidence that continued breastfeedingwhile solids are introduced into the diet and delaying theintroduction of solids until at least 17 weeks of age are associatedwith fewer food allergies.
abstractOBJECTIVES: To address questions regarding breastfeeding, comple-mentary feeding, allergy development, and current infant-feedingrecommendations.
METHODS: This was a nested, case-control within a cohort study inwhich mothers of 41 infants diagnosed with food allergy by the age of2 years (according to double-blind, placebo-controlled food challenge)and their 82 age-matched controls kept prospective food diaries ofhow their infants were fed in the first year of life.
RESULTS: Infants who were diagnosed with food allergy by the timethey were 2 years of age were introduced to solids earlier (#16weeks of age) and were less likely to be receiving breast milk whencow’s milk protein was first introduced into their diet.
CONCLUSIONS: This study supports the current American Academy ofPediatrics’ allergy prevention recommendations and the EuropeanSociety of Pediatric Gastroenterology, Hepatology and Nutrition rec-ommendations on complementary feeding to not introduce solidsbefore 4 to 6 months of age. It also supports the American Academyof Pediatrics’ breastfeeding recommendations that breastfeedingshould continue while solids are introduced into the diet and thatbreastfeeding should continue for 1 year, or longer, as mutually de-sired by mother and infant. Pediatrics 2013;132:e1529–e1538
AUTHORS: Kate E.C. Grimshaw, PhD, RD,a Joe Maskell,MSc,b Erin M. Oliver, MSc,a Ruth C.G. Morris, DipHE RN(Child),c Keith D. Foote, MBBS, FCPCH,d E.N. Clare Mills,PhD,e Graham Roberts, DM, MRCPCH,a and Barrie M.Margetts, PhD, FFPHf
aClinical and Experimental Sciences Academic Unit and fPrimaryCare and Population Sciences Academic Unit, University ofSouthampton Faculty of Medicine, Southampton, United Kingdom;bPublic Health Sciences and Medical Statistics, University ofSouthampton, Southampton, United Kingdom; cWellcome TrustClinical Research Facility, University Hospital Southampton NHSFoundation Trust, Southampton, United Kingdom; dHampshireHospitals Foundation Trust, Winchester, United Kingdom; andeInstitute of Inflammation and Repair, Manchester AcademicHealth Science Centre, Manchester Institute of Biotechnology,The University of Manchester, Manchester, United Kingdom
KEY WORDSbreastfeeding, food allergy, infant feeding, prevention
ABBREVIATIONSDBPCFC—double-blind, placebo-controlled food challengePIFA—Prevalence of Infant Food Allergy StudyWHO—World Health Organization
Dr Grimshaw was involved in writing the original study protocol,data collection, diagnosis of food allergy, statistical analysis anddata management, and initial drafting and revision of themanuscript; Mr Maskell was involved in statistical analysis anddata management, and revision of the manuscript for importantintellectual content; Ms Oliver and Ms Morris were involved indata collection, diagnosis of food allergy, and revision of themanuscript for important intellectual content; Dr Foote wasinvolved in the initiation and set up of the study, data collection,diagnosis of food allergy, and revision of the manuscript forimportant intellectual content; Prof Mills was involved in theconception and design of the original study protocol andrevision of the manuscript for important intellectual content;Prof Roberts was involved in the initiation and set-up of thestudy, data collection, diagnosis of food allergy, statisticalanalysis and interpretation of the data, and revision of themanuscript for important intellectual content; and ProfMargetts was involved in the initiation and set-up of the study,statistical analysis and interpretation of the data, and revisionof the manuscript for important intellectual content. All authorsapproved the final manuscript as submitted.
(Continued on last page)
PEDIATRICS Volume 132, Number 6, December 2013 e1529
ARTICLE
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

Since announcement of the WorldHealth Organization (WHO) recom-mendation that all infants be exclu-sively breastfed for 26 weeks, therehas been an ongoing debate as towhether the recommendation is whollyappropriate for all infants from de-veloped countries. The debate is wellillustrated by a review by Fewtrell et al1
and the letters of response publishedin 2011.2–4
Although there is no doubt as to thenutritional and emotional benefits ofbreastfeeding, the crux of the argu-ment is the benefit of exclusivebreastfeeding to 26 weeks. One side(pro– exclusive breastfeeding to 26weeks) believe breast milk to be nu-tritionally adequate to the age of 6months, that exclusive breastfeedingis protective against a plethora of in-fant conditions,5–8 and that thesebenefits are demonstrated in de-veloped as well as underdevelopedcountries.9 This view is currently ad-vocated by the American Academy ofPediatrics, the European Society ofPediatric Gastroenterology, Hepatol-ogy and Nutrition, and the UK De-partment of Health.10–12 The other sideof the argument is that although ex-clusive breastfeeding for 26 weeks isundoubtedly the best recommenda-tion for infants in underdevelopedcountries, in developed countries,where the risk of gastrointestinalinfections are reduced and allergicconditions are increased, the benefitsof exclusive breastfeeding for thislong are not as strong. Calls for fur-ther work in this area have beenmade, with the American Academy ofPediatrics recommending that solidsbe introduced between 4 and 6 monthsof age for allergy prevention.10,13 Failureto resolve the debate undermines theauthority of current infant-feeding rec-ommendations, which can cause con-fusion in health care workers andparents alike.
To inform the debate, we examinedthe relationship between breast-feeding, complementary feeding, andallergy development in a nested,case-control study within a cohortstudy in which mothers kept pro-spective food diaries of how theirinfantswere fed in thefirst yearof life.The study design facilitated the col-lection of accurate data on the initi-ation, duration, and exclusivity ofbreastfeeding, aswell as the nature ofintroduction of solids.
METHODS
The PIFA (Prevalence of Infant Food Al-lergy) study is a prospective birth co-hort of 1140 infants recruited between2006 and 2008, and it was the UK cohortof the EuroPrevall project14 with studysize and eligibility criteria determinedby that study’s protocol.15 It receivedapproval from the research and de-velopment departments at the RoyalHampshire County Hospital, Winchesterand Southampton General Hospital,and ethical approval was granted bythe North and Mid Hampshire LocalResearch Ethics Committee and theSouthampton and South West Hamp-shire Local Research Ethics Committee(05/Q1703/34).
Infants from the PIFA study who hadbeen diagnosed as having a food al-lergy (according to a double-blind,placebo-controlled food challenge[DBPCFC]15) and their 2 age-matchedcontrols were included in a “nestedwithin a cohort, case-control study.”Controls comprised infants with birth-days closest to the index cases andwhose parents consented. They wereassessed by using the same symptom-atic questionnaire and physical exami-nation to ensure that they exhibited nosigns of food allergy.
Study Design
The PIFA study has a longitudinal pro-spective cohort design starting from
birth. Interested women met 1 of thestudy research fellows; informedconsent was recorded, and baselineinformation on socioeconomic, envi-ronmental, and family allergy historywas collected. Women were also in-vited to keep food diaries for theirinfants from birth until 1 year of age.Mothers/caregivers returned the fooddiaries to the study office monthly.Mothers were also sent a new symp-tom sheet every 2 months to facilitateidentification of symptomatic infants,with parents being asked to contactthe study team if they thought theirchild developed signs of allergic dis-ease. One of the parents was asked tocomplete the EuroPrevall telephonequestionnaire when their infantreached the age of 12 months andagain at 24 months. The symptomaticsheets and the 12- and 24-monthquestionnaires also served to identifyinfants who may have a food allergy.Prospective completion of fooddiariesand symptom sheets reduced the po-tential for experimental bias.
Food Allergy Diagnosis
Possible cases of food allergy weretriaged via telephone, and thosepatients fulfilling the EuroPrevall-widecriteria for assessment were invitedfor a symptomatic visit, at which theEuroPrevall symptomatic question-naire was completed, a physical ex-amination was performed, skin pricktesting was completed, and a bloodsample was taken.15 Any infant witha convincing clinical history of foodallergy, presence of serum-specificimmunoglobulin E to a common foodallergen ($0.35 kU/L), and/or a posi-tive skin prick test result ($3-mmwheal) was placed on an exclusion dietfor the suspected food(s). If symptomsimproved, the child attended theSouthampton Wellcome Trust ClinicalResearch Facility for a DBPCFC. The di-agnostic criterion for food allergy inthis study for all infants was a positive
e1530 GRIMSHAW et al
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

DBPCFC (which included delayed reac-tions up to 48 hours after the chal-lenge).
Dietary Intake Data
At recruitment, parents were asked torecord daily anything their child ate ordrank for the first year of life on fooddiary sheets designed for the purpose,and they were instructed on theircompletion. Diary sets (which con-sistedof 4weekly sheets)weresentoutevery 2 months, with parents beingasked to return each diary to the studyoffice once it was completed. Freepostenvelopes were provided for theirreturn.
To reduce the burden of food diarycompletion, parents were asked to re-cord what the child consumed but notthe amounts of food taken. Upon re-ceipt, diarieswere reviewed, andwherethey lacked adequate detail (eg, type ofinfant formula given), parents werecontacted by telephone so these datacould be recorded. The data from alldiaries were analyzed in the samemanner to determine the timing ofspecific events such as when infantformula or any solid/semi-solid foodwas first introduced into the diet andtheageatwhichbreastfeedingstopped.In the current article, “exclusivebreastfeeding” is defined as when aninfant receives only breast milk, water,or vitamin/mineral drops. “Introduc-tion of solid foods” refers to when theinfants first received solid/semi-solidfoods.
Statistical Analysis
A descriptive analysis of baselinecharacteristics (obtained via standardquestionnaire administered at re-cruitment15), any health and clinicalsymptoms (obtained by using a symp-tomatic questionnaire and physicalexamination), and dietary intake data(obtained via food diary analysis)for infants involved in the study was
conducted by using SPSS version 17(IBM SPSS Statistics, IBM Corporation,Armonk, NY). Continuous variableswere described in terms of means 6standard deviations or medians andranges depending on their distribution.Categorical variables were describedin terms of numbers and percentages.Descriptive statistics, x2 tests, andMann-Whitney U tests were used on allavailable dietary intake data. Kaplan-Meier survival analysis was used toestablish additional details aboutbreastfeeding duration. The studysample size had sufficient power todetect an odds ratio of $0.48 at 80%power and a significance level of .05.This equates to infants who went on todevelop a food allergy receiving solids2 weeks earlier than for the infantswho did not develop a food allergy.
Finally, analysisbyusingamultivariablelogistic model was conducted. Thisanalysis included variables that theprevious analyses had identified asbeing significantly different betweenthe study groupsandalso factorswhichare considered to be associated withallergy development.
RESULTS
Participants
Infants were from the PIFA study (N =1140) who had either been diagnosedas having a food allergy according toDBPCFC (n = 41) or were their age-matched controls (n = 82). Figure 1shows infant numbers at each stageof the main PIFA study and alsothe stages of diagnosis of the food-allergic infants. The study infants(N = 123) were born between January2006 and October 2007. Median ma-ternal age was 33 years (range: 19–43years), and median infant weight was3420 g (range: 2160–5060 g). Baselinecharacteristics for the infants whobecame food allergic and their con-trols are detailed in Table 1. The de-mographic characteristics of the mainPIFA study population (N = 1140) dif-fered from those of the communityfrom which it was recruited because ithad a large proportion of older, well-educated mothers. However, the in-fants in the 2 experimental groups ofthe current study (N = 123) did notdiffer significantly from each other forany demographic or environmental
FIGURE 1Flowchart of participants in the PIFA study.
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 e1531
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

measurement. Median age at start ofsymptoms of food allergy was 24weeks (range: 0–64 weeks). Medianage at DBPCFC was 56 weeks. The mostcommon causative food was hen’s egg(22 infants), closely followed by cow’smilk (20 infants). Twelve infants wereallergic to .1 food. Infants displayeddiffering symptoms, with some infantsdisplaying .1 symptom. The mostcommon symptom was physician-diagnosed eczema (12 infants), withvomiting being the second most com-mon (11 infants). Details of the infantdiet when symptoms started are givenin Table 2. No infant who was allergicto egg experienced symptoms beforeconsuming egg; however, 1 peanut-allergic infant experienced cutane-ous symptoms after contact with theallergen before any peanut consump-tion.
Breastfeeding
Ninety-five percent of all mothers in-cluded in the study initiated breast-feeding, with a median duration of 20weeks (range: 0–64 weeks). Medianduration for exclusive breastfeedingwas 8 weeks (range: 1–26 weeks), with
50% of mothers still exclusivelybreastfeeding at 9 weeks. There wasno statistically significant differencebetween breastfeeding initiation, du-ration, or exclusive breastfeeding du-ration between the symptomatic andcontrol infants (Table 3). Exclusivitywas lost to whey-predominant infantformula in 78% of infants, with only2 infants losing exclusivity due to adifferent type of formula (casein-predominant and extensively hydro-lyzed formula). The second mostcommon way for infants to lose theirexclusive breastfeeding status was tohave rice introduced into the diet (inthe form of “baby rice”).
Kaplan-Meier analysis indicated howthe nature of breastfeeding differedbetween the 2 study groups (Fig 2). Thisdifference was not significant (gener-alized Wilcoxon [Breslow] test, P =.335).
Concurrent Feeding With Cow’sMilk Protein and Breast Milk
There was no statistically significantdifference between groups for the agecow’s milk (in any form) was introducedinto the diet (Table 4). However, among
infants who received both cow’s milk inany formandbreastmilk (n= 27, allergygroup; n = 72, control group), the du-ration of concurrent feeding was 5.5weeks in the allergy group versus 9weeks in the control group (P = .047). Toinvestigate whether the duration ofoverlap was important, the variableswere recoded to provide a categorical“concurrent breastfeeding” variable.Again, there was a statistically signifi-cant difference between the groups forconcurrent feeding with cow’s milk inany form and breast milk (P = .015),suggesting that any concurrent feedingis beneficial. Because the timing of theoverlap may be important, a post hocanalysis was conducted to comparewhether the ages when concurrentbreastfeeding occurred differed be-tween the 2 groups, and no significantdifference was found (Mann-WhitneyU test, P = .300).
There were insufficient numbers ofinfants commencing foods other thancow’s milk while being breastfed toexplore whether this factor affectedthe development of food allergy.
Introduction of Solid Foods
The mean age of any solid introductionwas 20.3 weeks. The food with the ear-liestmedianageof introductionwasriceat 20 weeks (given predominantly as“baby rice”), with carrots introduced ata median age of 21 weeks and applesand bananas at a median age of 22weeks. The food that was most com-monly introduced before 17 weeks ofage was rice (20 infants). The othercommon foods introduced before 17
TABLE 1 Characteristics of the Mother and Infant Pairs Included in This Prospective Case-ControlStudy
Characteristic Food Allergy (n = 41) Control (n = 82) P a
Male gender 24 (58.5) 43 (52.4) .522Median birth weight, g 3480.0 (2160–4120) 3370.0 (2270–5060) .913b
Median length, cm 53.0 (48–59) 52.0 (47–61) .909b
Duration of pregnancy, wk 39.5 (36–42) 40.0 (36–42) .062b
Median maternal age, y 31.0 (19–43) 33.0 (22–42) .192b
Median paternal age, y 33.5 (21–42) 34.0 (23–49) .247b
Maternal educationDid not complete basic education 0 (0) 0 (0) .448Completed basic education 4 (9.7) 6 (7.3)Junior college/vocational training 11 (26.8) 15 (18.3)University/college 26 (63.4) 61 (74.4)
Median maternal prepregnancy BMI, kg/m2 22.9 (16.6–43.0) 22.8 (16.5–49.2) .323b
Maternal asthma 11 (26.8) 11 (13.4) .067Maternal allergy 22 (53.7) 31 (37.8) .105Maternal smoking 1 (2.4) 3 (3.7) 1.000Only child 24 (58.5) 49 (59.8) .570Urban dwelling 8 (19.5) 11 (13.4) .378Pet ownership 26 (63.4) 40 (48.8) .142
Data are presented as n (%) or median (range).a x2 test.b Mann-Whitney U test.
TABLE 2 Details of Infant Diet at Time WhenSymptoms Started
Infants Diet at Start of Symptoms No. of Infants
Infant formula and solids 15Infant formula 9Infant formula and breast milk 5Breast milk 5Breast milk, infant formula,and solids
4
Breast milk and solids 3
e1532 GRIMSHAW et al
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

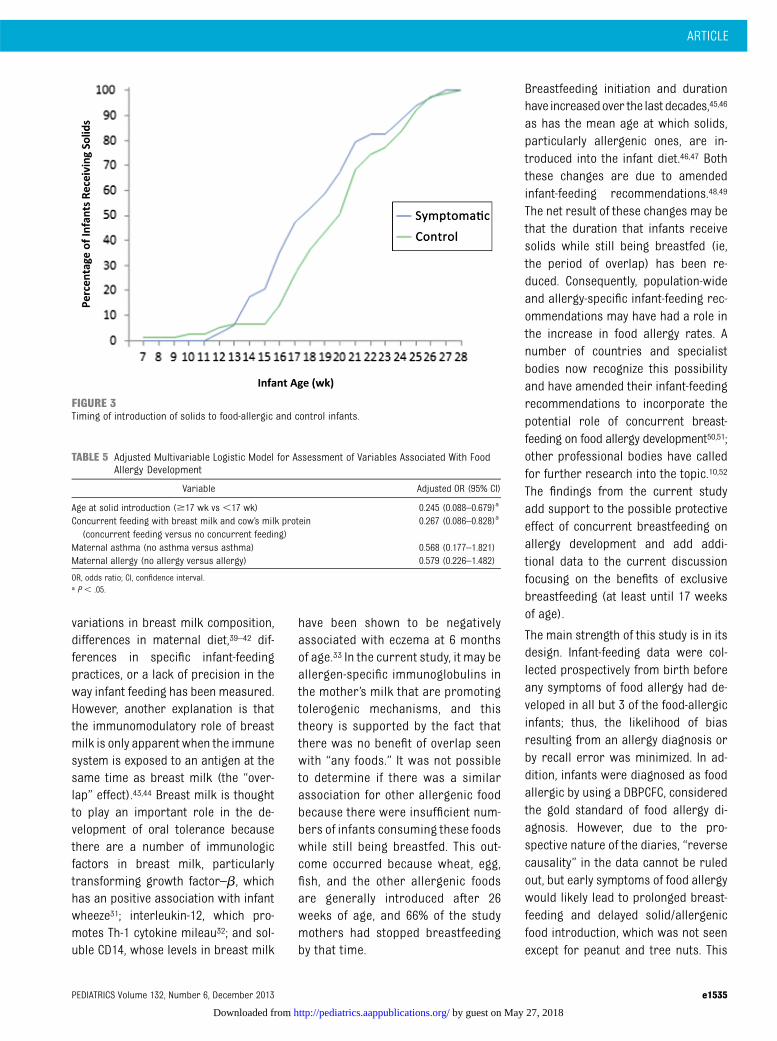
weeks of age were apples, bananas, andpears (11, 8, and 8 infants, respectively).The first cow’s milk protein taken as aningredient was most likely to be fromyogurt/fromage frais. Solids were in-troduced significantly earlier in food-allergic infants compared with controlinfants (P = .044), as was cow’s milk asan ingredient (P = .049) and peanut (P =.037) (Table 4). Control infants were in-troduced to solids first, but between 12and 16 weeks, 15% of food-allergicinfants were introduced to solids com-pared with only 9% of control infants(Fig 3). A post hoc analysis was
undertaken that stratified the timingof complementary food introductioninto 2 groups: introduction before andincluding 16 weeks of age and intro-duction at $17 weeks of age. Signifi-cantly more food-allergic infants wereintroduced to complementary foods at#16 weeks than control infants (35%vs 14%; P = .011).
Multivariable Logistic Model
The model included age at solid intro-duction, concurrent breastfeeding, andcow’s milk in any form, which werevariables that the previous analyses
had identified as being significantlydifferent between the study groups.Age at solid introduction was changedto a categorical variable because theresult of the post hoc analysis foundthat solid introduction before 17 weeksof age was strongly associated withfood allergy development. The concur-rent breastfeeding and cow’s milk vari-able was also recoded into a categoricalvariable because earlier analysisshowed any concurrent breastfeedingseemed to be beneficial. Cow’s milk asan ingredient was not included in themodel due to multicollinearity, andage at first peanut consumption wasnot included due to reverse causation.Factors considered to be associatedwith allergy development (maternalasthma, allergy, education, age, petownership, infant gender, and singlebirth) were also included in thismodel. Maternal smoking was not in-cluded in the model because theproportion of smoking mothers wasrare for all infants (3.3%) and was notsignificantly different between thegroups.
TABLE 3 Breastfeeding Characteristics for Infants With Food Allergy and Control Infants in theStudy
Characteristic Food Allergy (n = 41) Control (n = 82) P
No. (%) initiating breastfeeding 38 (92.7) 79 (96.3) .210a
Breastfeeding duration, wkMedian 21.0 24.0 .295b
Interquartile range 3.0–30.5 7.0–31.0Range 0–64 0–52
Exclusive breastfeeding duration, wkMedian 5.0 8.5 .933b
Interquartile range 2.8–16.3 4.0–15.0Range 1–26 1–24
a x2 test.b Mann-Whitney U test.
FIGURE 2Kaplan-Meier survival analysis plot showing duration of breastfeeding for symptomatic and control infants.
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 e1533
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

This analysis found that the associationbetween solid introduction beyond 17weeks of age and the concurrentbreastfeeding and cow’s milk intro-duction and allergy development re-mained once the effects of otherpotentially confounding variables werecontrolled for (odds ratio: 0.292 [95%confidence interval: 0.099–0.859]; oddsratio: 0.279 [95% confidence interval:0.080–0.971], respectively [data notshown]). However, because a modelwith 10 variables may be too many fora sample size of 123, the model wasreduced by removing the variables thathad a small effect (odds ratio between0.80 and 1.25), and the results areshown in Table 5. Results were similarif the analysis was stratified according
to maternal asthma and maternal al-lergy (data not shown).
DISCUSSION
Within this nested case-control study,we found that early introduction ofsolids was associated with the de-velopment of food allergy. Infantswith food allergy were much morelikely to have had solids introducedbetween 12 and 16 weeks than con-trol infants.
The delayed introduction of solids intothe infant diet (particularly of aller-genic foods) has in the past been ad-vocated for preventing allergy,16 but ithas led to disappointing results inclinical trials.17,18 A number of birth
cohort studies have failed to show anybenefit on allergic outcome by delayingthe introduction of solids, and 2 foundan association between the delayedintroduction of milk19 and egg20,21 andincreased incidence of eczema andatopic sensitization.19–22 However, thesestudies did not indicate an age beforewhich solids should not be introducedinto the diet to avoid allergies. Ourfindings, conversely, suggest 17 weeksis a crucial time point, with solid foodintroduction before this time ap-pearing to promote allergic diseasewhereas solid food introduction afterthat time point seems to promote tol-erance. This finding implies that themechanism, which acts post–17 weeksof age, is a nonallergen-specific tol-erogenic immunologic mechanism be-cause the food diary data showed thatthe foods introduced at this time weremainly fruit and vegetables, which arenot considered allergenic. Epigeneticor immunologic mechanisms may beimplicated because the foods that areintroduced during this time deliver thesubstrates required for the inductionof such processes.23–26 Fruits and veg-etables have been shown to modifyimmune responses in older children,19,20
with the proposed mechanism beingdue to their antioxidant action on in-flammatory processes27 and Tregcells28 or their action on the gut mi-croflora.29,30
In addition, we demonstrated a pro-tective effect on food allergy de-velopment when cow’s milk protein, inwhatever form, was given in theinfant’s diet concurrently with breastmilk. One of the perceived benefits ofbreastfeeding is the reduced risk ofallergy due to the presence of a num-ber of immunomodulatory factors inbreast milk.31–33 However, the evidencethat breastfeeding prevents allergiesis contradictory, with some reviewsshowing a benefit while others didnot.34–38 These findings may be due to
TABLE 4 Age at Introduction of Complementary Foods Given for All Infants (N = 123) and for EachStudy Group
Variable All Infants(N = 123)
Food Allergy(n = 41)
Control(n = 82)
P a
Median age at introduction of solids, wkAny solid/semi-solid food 20 18 20 .044Interquartile range 17.0–22.0 16.0–21.0 17.0–23.0Range 7–28 12–27 7–28
Duration of concurrent breastfeedingand any solid food
0 0 0 .303
Interquartile range 0.0–9.0 0.0–8.5 0.0–9.75Range 0.38 0–38 0–33
Duration of concurrent breastfeedingand cow’s milk in any form
8.0 5.5 9.0 .047
Interquartile range 2.0–20.0 0.0–15.5 3.5–21.5Range 0–51 0–51 0–45
Cow’s milk as an ingredient 25.0 22.0 26.0 .049Interquartile range 21–28.5 17.5–26.5 21.0–29.0Range 13–52 13–52 16–52
Cow’s milk in any form 4 3 5 .283Interquartile range 1.0–14.0 1.0–11.5 1.0–14.3Range 1–49 1–49 1–32
Hen’s egg protein 35 39 35 .087Interquartile range 29.5–40.0 30.0–39.0 29.0–39.0Range 17–52 20–52 17–52
Wheat 27 27 26 .573Interquartile range 25.0–29.0 24.0–30.0 25.0–29.0Range 13–52 13–52 13–50
Fish 29 29 29 .860Interquartile range 26.0–34.0 26.0–35.0 26.0–34.0Range 17–52 20–52 17–52
No. (%) of infants who had eatenpeanuts before age 52 wk
11(8.9) 5 (12.2) 6 (7.3) .055b
No. (%) of infants who had eatentree nuts before age 52 wk
9 (7.3) 3 (7.3) 6 (7.3) .309b
No. (%) of infants who had eatensesame before age 52 wk
13 (10.6) 5 (12.2) 8 (9.8) .051b
a Mann-Whitney U test comparing infants with food allergy and control infants.b x2 test.
e1534 GRIMSHAW et al
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from
variations in breast milk composition,differences in maternal diet,39–42 dif-ferences in specific infant-feedingpractices, or a lack of precision in theway infant feeding has been measured.However, another explanation is thatthe immunomodulatory role of breastmilk is only apparent when the immunesystem is exposed to an antigen at thesame time as breast milk (the “over-lap” effect).43,44 Breast milk is thoughtto play an important role in the de-velopment of oral tolerance becausethere are a number of immunologicfactors in breast milk, particularlytransforming growth factor–b, whichhas an positive association with infantwheeze31; interleukin-12, which pro-motes Th-1 cytokine mileau32; and sol-uble CD14, whose levels in breast milk
have been shown to be negativelyassociated with eczema at 6 monthsof age.33 In the current study, it may beallergen-specific immunoglobulins inthe mother’s milk that are promotingtolerogenic mechanisms, and thistheory is supported by the fact thatthere was no benefit of overlap seenwith “any foods.” It was not possibleto determine if there was a similarassociation for other allergenic foodbecause there were insufficient num-bers of infants consuming these foodswhile still being breastfed. This out-come occurred because wheat, egg,fish, and the other allergenic foodsare generally introduced after 26weeks of age, and 66% of the studymothers had stopped breastfeedingby that time.
Breastfeeding initiation and durationhave increasedover the last decades,45,46
as has the mean age at which solids,particularly allergenic ones, are in-troduced into the infant diet.46,47 Boththese changes are due to amendedinfant-feeding recommendations.48,49
The net result of these changes may bethat the duration that infants receivesolids while still being breastfed (ie,the period of overlap) has been re-duced. Consequently, population-wideand allergy-specific infant-feeding rec-ommendations may have had a role inthe increase in food allergy rates. Anumber of countries and specialistbodies now recognize this possibilityand have amended their infant-feedingrecommendations to incorporate thepotential role of concurrent breast-feeding on food allergy development50,51;other professional bodies have calledfor further research into the topic.10,52
The findings from the current studyadd support to the possible protectiveeffect of concurrent breastfeeding onallergy development and add addi-tional data to the current discussionfocusing on the benefits of exclusivebreastfeeding (at least until 17 weeksof age).
The main strength of this study is in itsdesign. Infant-feeding data were col-lected prospectively from birth beforeany symptoms of food allergy had de-veloped in all but 3 of the food-allergicinfants; thus, the likelihood of biasresulting from an allergy diagnosis orby recall error was minimized. In ad-dition, infants were diagnosed as foodallergic by using a DBPCFC, consideredthe gold standard of food allergy di-agnosis. However, due to the pro-spective nature of the diaries, “reversecausality” in the data cannot be ruledout, but early symptoms of food allergywould likely lead to prolonged breast-feeding and delayed solid/allergenicfood introduction, which was not seenexcept for peanut and tree nuts. This
FIGURE 3Timing of introduction of solids to food-allergic and control infants.
TABLE 5 Adjusted Multivariable Logistic Model for Assessment of Variables Associated With FoodAllergy Development
Variable Adjusted OR (95% CI)
Age at solid introduction ($17 wk vs ,17 wk) 0.245 (0.088–0.679)a
Concurrent feeding with breast milk and cow’s milk protein(concurrent feeding versus no concurrent feeding)
0.267 (0.086–0.828)a
Maternal asthma (no asthma versus asthma) 0.568 (0.177–1.821)Maternal allergy (no allergy versus allergy) 0.579 (0.226–1.482)
OR, odds ratio; CI, confidence interval.a P , .05.
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 e1535
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

action occurred because parents ofallergic children were happier to in-troduce these foods due to skin pricktest results, which control children didnot have. Consequently, it is appropri-ate to consider that this study’s find-ings reflect a possible causal link withfood allergy development. A weaknessof the study is that the demographiccharacteristics of the study populationdiffered from the demographic char-acteristics of the community fromwhich it was recruited. However, theinfants in the 2 experimental groupsof this study (N = 123) did not differsignificantly from each other for anydemographic or environmental mea-surement, although due to under-powering (51% for asthma and 43% formaternal allergy), the analysis may nothave been able to identify weak asso-ciations.
CONCLUSIONS
This study supports current allergyprevention recommendations that sol-ids should not be introduced before17 weeks of age10,11 and the generalfeeding recommendations that breast-feeding should continue while solids
are introduced into the diet and be-yond.13 These guidelines are in linewith the WHO recommendation forbreastfeeding to continue alongsidesolid foods until 2 years of age.53
However, it does not provide evidenceon the relationship between exclusivebreastfeeding to 26 weeks of age(compared with 17 weeks) and allergydevelopment because insufficient num-bers of women in the study were ableto exclusively breastfeed for that long.This situation is reflected in generalpopulation data which show that in2010, only 12% of UK women managedto exclusively breastfeed to 17 weeks.46
Exclusive breastfeeding rates in theUnited States seem to be higher, with46% of US women exclusively breast-feeding for 3 months,45 but this valuestill falls short of the WHO recommen-dation. One reason for the low levels ofexclusive breastfeeding may be thatthe recommendations seem to offerconflicting advice.
Although we are waiting for more re-search to be conducted to determinethe optimum duration of exclusivebreastfeeding for the best overallhealth outcome of all infants, health
professionals can provide advice that isconsistent by encouraging exclusivebreastfeeding for as long as possible,followed by continued breastfeedingalongside the introduction of comple-mentary foods tomaximize thedurationof concurrent breastfeeding and solidfood introduction.
ACKNOWLEDGMENTSWe thank all families who took part inthe PIFA study and the midwives ofWinchester and Eastleigh Health CareTrust for their support of the study andhelp in recruitment, particularly T.Kemp. We also thank all staff involvedin the daily running of the study andthe staff in the Child Health and Well-come Trust Clinical Research Facilityat Southampton General Hospital forfollowing up the participants and per-forming the clinicalwork needed to es-tablish the diagnosis of food allergy,particularly L. Gudgeon, R. King, J.Garland, E. Francis, S. Pestridge, K.Scally, E. Gatrell, L. Bellis, A. Acqua,and R. Kemp. Our thanks also go to Pro-fessor Jonathan Hourihane for hiscrucial role in initially setting up thePIFA study.
REFERENCES
1. Fewtrell M, Wilson DC, Booth I, Lucas A. Sixmonths of exclusive breast feeding: howgood is the evidence? BMJ. 2011;342:c5955
2. Renfrew MJ, McGuire W, McCormick FM.When to wean. Analysis article on breastfeeding was misleading. BMJ. 2011;342:d987
3. Wright CM. When to wean. Infection moreimportant than anaemia or allergy. BMJ.2011;342:d1000
4. Williams AF, Prentice A. Scientific AdvisoryCommittee on Nutrition replies to MaryFewtrell and colleagues. BMJ. 2011;342:d980
5. Howie PW, Forsyth JS, Ogston SA, Clark A,Florey CD. Protective effect of breast feed-ing against infection. BMJ. 1990;300(6716):11–16
6. Wilson AC, Forsyth JS, Greene SA, Irvine L,Hau C, Howie PW. Relation of infant diet to
childhood health: seven year follow up ofcohort of children in Dundee infant feedingstudy. BMJ. 1998;316(7124):21–25
7. Lucas A, Cole TJ. Breast milk and neonatalnecrotising enterocolitis. Lancet. 1990;336(8730):1519–1523
8. Raisler J, Alexander C, O’Campo P. Breast-feeding and infant illness: a dose-responserelationship? Am J Public Health. 1999;89(1):25–30
9. Kramer MS, Kakuma R. Optimal duration ofexclusive breastfeeding. Cochrane Data-base Syst Rev. 2012;(8):CD003517
10. Greer FR, Sicherer SH, Burks AW; AmericanAcademy of Pediatrics Committee on Nu-trition; American Academy of PediatricsSection on Allergy and Immunology. Effectsof early nutritional interventions on the
development of atopic disease in infantsand children: the role of maternal dietaryrestriction, breastfeeding, timing of in-troduction of complementary foods, andhydrolyzed formulas. Pediatrics. 2008;121(1):183–191
11. Agostoni C, Decsi T, Fewtrell M, et al;ESPGHAN Committee on Nutrition. Com-plementary feeding: a commentary by theESPGHAN Committee on Nutrition. JPediatr Gastroenterol Nutr. 2008;46(1):99–110
12. Department of Health. Feeding yourbaby from birth to five. Available at: http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/Publicationsandstatistics/Pub-lications/publicationspolicyandguidance/DH_107303. Accessed September 10, 2013
e1536 GRIMSHAW et al
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

13. Section on Breastfeeding. Breastfeedingand the use of human milk. Pediatrics.2012;129(3). Available at: www.pediatrics.org/cgi/content/full/129/3/e827
14. McBride D, Keil T, Grabenhenrich L, et al.The EuroPrevall birth cohort study on foodallergy: baseline characteristics of 12,000newborns and their families from nineEuropean countries. Pediatr Allergy Immu-nol. 2012;23(3):230–239
15. Keil T, McBride D, Grimshaw K, et al. Themultinational birth cohort of EuroPrevall:background, aims and methods. Allergy.2010;65(4):482–490
16. Kleinman RE. American Academy of Pe-diatrics recommendations for comple-mentary feeding. Pediatrics. 2000;106(5):1274
17. Zeiger RS, Heller S. The development andprediction of atopy in high-risk children:follow-up at age seven years in a pro-spective randomized study of combinedmaternal and infant food allergen avoid-ance. J Allergy Clin Immunol. 1995;95(6):1179–1190
18. Koplin J, Osborne N, Martin P, et al. Canearly introduction of egg prevent egg al-lergy in infants? A population based studyof an infant cohort. J Allergy Clin Immunol.2010;126:807–813
19. Snijders BE, Thijs C, van Ree R, van denBrandt PA. Age at first introduction of cowmilk products and other food products inrelation to infant atopic manifestations inthe first 2 years of life: the KOALA BirthCohort Study. Pediatrics. 2008;122(1). Avail-able at: www.pediatrics.org/cgi/content/full/122/1/e115
20. Zutavern A, Brockow I, Schaaf B, et al; LISAStudy Group. Timing of solid food in-troduction in relation to eczema, asthma,allergic rhinitis, and food and inhalantsensitization at the age of 6 years: resultsfrom the prospective birth cohort studyLISA. Pediatrics. 2008;121(1). Available at:www.pediatrics.org/cgi/content/full/121/1/e44
21. Filipiak B, Zutavern A, Koletzko S, et al; GINI-Group. Solid food introduction in relation toeczema: results from a four-year pro-spective birth cohort study. J Pediatr. 2007;151(4):352–358
22. Zutavern A, von Mutius E, Harris J, et al.The introduction of solids in relation toasthma and eczema. Arch Dis Child. 2004;89(4):303–308
23. Prescott SL, Smith P, Tang M, et al. Theimportance of early complementary feed-ing in the development of oral tolerance:concerns and controversies. Pediatr Al-lergy Immunol. 2008;19(5):375–380
24. Pali-Schöll I, Renz H, Jensen-Jarolim E. Up-date on allergies in pregnancy, lactation,and early childhood. J Allergy Clin Immu-nol. 2009;123(5):1012–1021
25. Calder PC, Albers R, Antoine JM, et al. In-flammatory disease processes and inter-actions with nutrition. Br J Nutr. 2009;101(suppl 1):S1–S45
26. Lack G. Epidemiologic risks for food allergy.J Allergy Clin Immunol. 2008;121(6):1331–1336
27. Chatzi L, Kogevinas M. Prenatal and childhoodMediterranean diet and the development ofasthma and allergies in children. PublicHealth Nutr. 2009;12(9A):1629–1634
28. Tan PH, Sagoo P, Chan C, et al. Inhibition ofNF-kappa B and oxidative pathways in hu-man dendritic cells by antioxidative vita-mins generates regulatory T cells. JImmunol. 2005;174(12):7633–7644
29. Blaut M. Relationship of prebiotics andfood to intestinal microflora. Eur J Nutr.2002;41(suppl 1):I11–I16
30. Claesson MJ, Jeffery IB, Conde S, et al. Gutmicrobiota composition correlates withdiet and health in the elderly. Nature. 2012;488(7410):178–184
31. Oddy WH, Halonen M, Martinez FD, et al.TGF-beta in human milk is associated withwheeze in infancy. J Allergy Clin Immunol.2003;112(4):723–728
32. Camporota L. Interleukin-12 and the de-velopment of atopy. Clin Exp Allergy. 2001;31(10):1481–1484
33. Jones CA, Holloway JA, Popplewell EJ, et al.Reduced soluble CD14 levels in amnioticfluid and breast milk are associated withthe subsequent development of atopy, ec-zema, or both. J Allergy Clin Immunol. 2002;109(5):858–866
34. Muraro A, Dreborg S, Halken S, et al.Dietary prevention of allergic diseasesin infants and small children. Part III:critical review of published peer-reviewedobservational and interventional studiesand final recommendations. Pediatr AllergyImmunol. 2004;15(4):291–307
35. Friedman NJ, Zeiger RS. Prevention andnatural history of food allergy. In: LeungDYM, Sampson HA, Geha RS, Szefler SJ,eds. Pediatric Allergy. Principles andPractice. St Louis, MO: Mosby; 2003:495–509
36. Gdalevich M, Mimouni D, David M, MimouniM. Breast-feeding and the onset of atopicdermatitis in childhood: a systematic reviewand meta-analysis of prospective studies. JAm Acad Dermatol. 2001;45(4):520–527
37. Gdalevich M, Mimouni D, Mimouni M.Breast-feeding and the risk of bronchialasthma in childhood: a systematic review
with meta-analysis of prospective studies. JPediatr. 2001;139(2):261–266
38. Kramer MS, Matush L, Vanilovich I, et al;Promotion of Breastfeeding InterventionTrial (PROBIT) Study Group. Effect of pro-longed and exclusive breast feeding on riskof allergy and asthma: cluster randomisedtrial. BMJ. 2007;335(7624):815
39. Patin RV, Vítolo MR, Valverde MA, CarvalhoPO, Pastore GM, Lopez FA. The influence ofsardine consumption on the omega-3 fattyacid content of mature human milk. JPediatr (Rio J). 2006;82(1):63–69
40. Furuhjelm C, Warstedt K, Larsson J, et al.Fish oil supplementation in pregnancy andlactation may decrease the risk of infantallergy. Acta Paediatr. 2009;98(9):1461–1467
41. Hoppu U, Kalliomäki M, Isolauri E. Maternaldiet rich in saturated fat during breast-feeding is associated with atopic sensiti-zation of the infant. Eur J Clin Nutr. 2000;54(9):702–705
42. Hoppu U, Rinne M, Salo-Väänänen P, LampiAM, Piironen V, Isolauri E. Vitamin C in breastmilk may reduce the risk of atopy in theinfant. Eur J Clin Nutr. 2005;59(1):123–128
43. Poole JA, Barriga K, Leung DY, et al. Timingof initial exposure to cereal grains and therisk of wheat allergy. Pediatrics. 2006;117(6):2175–2182
44. Norris JM, Barriga K, Klingensmith G, et al.Timing of initial cereal exposure in infancyand risk of islet autoimmunity. JAMA. 2003;290(13):1713–1720
45. Centers for Disease Control and Prevention.Breastfeeding report card, United States, 2012.Available at: http:// www.cdc.gov/breastfeeding/data/reportcard.htm. Accessed August 1, 2012
46. Health and Social Care Information Centre.Infant Feeding Study 2010. Available at: www.hscic.gov.uk/catalogue/PUB08694. AccessedOctober 9, 2013
47. Grummer-Strawn LM, Scanlon KS, Fein SB.Infant feeding and feeding transitions dur-ing the first year of life. Pediatrics. 2008;122(suppl 2):S36–S42
48. American Academy of Pediatrics Committeeon Nutrition. Pediatric Nutrition Handbook.6th ed. Elk Grove Village, IL AmericanAcademy of Pediatrics; 2008
49. Department of Health. Infant Feeding Rec-ommendation. London, UK: The StationeryOffice; 2004
50. Australasian Society of Clinical Immunologyand Allergy. Infant Feeding Advice 2010.Available at: www.allergy.org.au/images/stories/aer/infobulletins/2010pdf/ASCIA_Infant_Feeding_Advice_2010.pdf. AccessedOctober 9, 2013
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 e1537
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

51. Muche-Borowski C, Kopp M, Reese I, Sitter H,Werfel T, Schäfer T; German Society forAllergology and Clinical Immunology(DGAKI); Society of German Allergologists(ADA); German Society for Pediatricand Adolescent Medicine (DGKJ); German
Society of Dermatology (DDG); German So-ciety of Pediatric Allergology (GPA). Allergyprevention. J Dtsch Dermatol Ges. 2010;8(9):718–724
52. Høst A, Halken S, Muraro A, et al. Dietaryprevention of allergic diseases in infants
and small children. Pediatr Allergy Immu-nol. 2008;19(1):1–4
53. World Health Organisation (WHO). 55th WorldHealth Assembly. Infant and young child nutri-tion. Available at: www.who.int/nutrition/topics/WHA55.25_iycn_en.pdf. Accessed October 9, 2013
(Continued from first page)
www.pediatrics.org/cgi/doi/10.1542/peds.2012-3692
doi:10.1542/peds.2012-3692
Accepted for publication Sep 13, 2013
Address correspondence to Kate E.C. Grimshaw, PhD, RD, Clinical and Experimental Sciences Academic Unit, Mailpoint 803, Level F, South Academic Block,Southampton General Hospital, Tremona Rd, Southampton, SO16 6YD, UK. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr Roberts declares an association with Danone Baby Nutrition (sat on scientific advisory board 2011–2012), Dr Grimshaw declares anassociation with Nutricia Ltd (November 2011 for input into meeting regarding the “state of the art” of infant feeding and allergy development and June 2012 fora lecture given to pediatric gastroenterologists entitled “Nutritional Management of Food Allergy”), and Dr Mills declares an association with Novartis (forattending 1 board meeting in 2010 regarding the use of a double-blind, placebo-controlled food challenge as an outcome measure in a food allergy immunotherapystudy), Pepsico International (for advice on plant food allergen management in a factory environment), and DBV Technologies (for food challenge mealpreparations). The other authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by the UK Food Standards Agency (project TO7046) as part of the European Union’s EuroPrevall Project (contract FOOD-CT-2005-514000).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
e1538 GRIMSHAW et al
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

DOI: 10.1542/peds.2012-3692 originally published online November 18, 2013; 2013;132;e1529Pediatrics
E.N. Clare Mills, Graham Roberts and Barrie M. MargettsKate E.C. Grimshaw, Joe Maskell, Erin M. Oliver, Ruth C.G. Morris, Keith D. Foote,
Introduction of Complementary Foods and the Relationship to Food Allergy
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/132/6/e1529including high resolution figures, can be found at:
References
-1http://pediatrics.aappublications.org/content/132/6/e1529.full#ref-listThis article cites 43 articles, 14 of which you can access for free at:
Subspecialty Collections
munology_subhttp://classic.pediatrics.aappublications.org/cgi/collection/allergy:imAllergy/Immunologyubhttp://classic.pediatrics.aappublications.org/cgi/collection/nutrition_sNutritionrders_subhttp://classic.pediatrics.aappublications.org/cgi/collection/blood_disoBlood Disordersfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pediatrics.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
ISSN: . 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from

DOI: 10.1542/peds.2012-3692 originally published online November 18, 2013; 2013;132;e1529Pediatrics
E.N. Clare Mills, Graham Roberts and Barrie M. MargettsKate E.C. Grimshaw, Joe Maskell, Erin M. Oliver, Ruth C.G. Morris, Keith D. Foote,
Introduction of Complementary Foods and the Relationship to Food Allergy
http://pediatrics.aappublications.org/content/132/6/e1529located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: . 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 27, 2018http://pediatrics.aappublications.org/Downloaded from