introduction, natural history and pathogenesis of hiv infection dr.k.bujji babu, md. consultant hiv...
TRANSCRIPT
Introduction,Natural History
andPathogenesis of HIV infection
Dr.K.Bujji Babu, MD.
Consultant HIV Physician
Bujjibabu HIV Clinic

HIV/AIDS Historical Milestones• 1981 First Report of AIDS, USA
• 1983 Discovery of HIV
• 1984 ELISA for HIV Developed
• 1986 HIV-2 Identified, HIV & AIDS Reported in India
• 1987 First Antiretroviral-ZDV Approved
• 1989 Screening Blood Units Mandatory
• 1991 First Report of HIV-2 in India
• 1994 ZDV Reduces MTCT -ACTG 076. Protease Inhibitors Approved by
FDA
• 1996 Discovery of Chemokine Receptors• 1998 Short-term ZDV for MTCT CDC-Thai
• 1999 Nevirapine for MTCT- HIVNET 012

The Human Immunodeficiency Virus


Genome of HIV



Life Cycle of HIV
DS dna COMPLEX
Protease
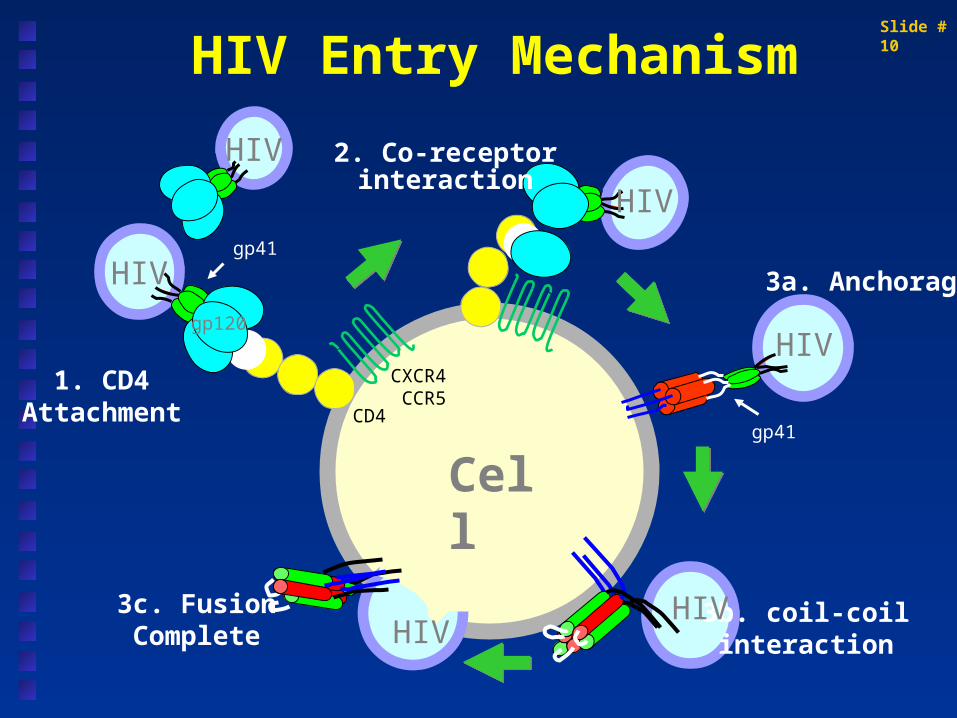
HIV Entry Mechanism
3c. FusionComplete
1. CD4Attachment
3b. coil-coilinteraction
CXCR4CCR5
HIV
HIV
gp120
3a. Anchorage
CD4
2. Co-receptorinteraction
Cell
HIV
HIV
HIV
gp41
gp41
HIV
Slide #10

HIV Fusion Inhibition by T-20
Source: www.trimeris.com

Molecular heterogeneity of HIV 1
Catagorized into 3 groups
group M ( major ) : subtypes or clades
A,B,C,D,F,G,H,J
:CRFs
AE,AG,AGI,AB
group O ( outlier ) :
group N

HIV-1 subtypes
SUBTYPE C - PREDOMINANT
India South Africa Ethiopia Botswana Tanzania
Account for a third HIV infections in world
SUBTYPE B - PREDOMINANT
America’s Europe Australia & New Zealand Japan IDUs in Thailand, China,
Myanmar
Account for about a tenth of HIV infections world over.
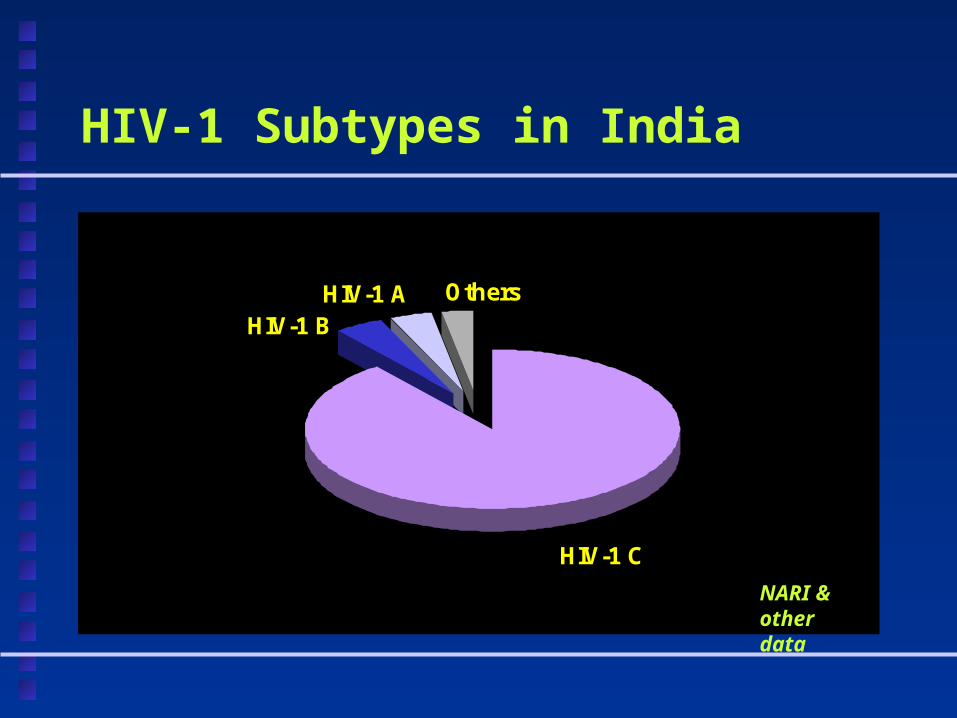
HIV-1 Subtypes in India
HIV-1 C
HIV-1 AHIV-1 B
Others
NARI & other data

Differences in HIV-1 & HIV -2
• Amino Acid Homology is between 40-60%
• Majority of Infections are HIV-1 (~89%), HIV-2 (2-4%) & remaining dual Reactivity in India
• Transmission by sex & MTCT less efficient
• Immunodeficiency develops slowly & milder
• NNRTI not active against HIV-2
• HIV-2 mainly present in West African nations, prevalence rate more than 1%; now found all over the world

Transmission of HIV
Sexual Injection drug users Blood and blood products Maternal transmission Occupational exposure

Body fluids which can transmit HIV
Blood and bloody fluids Potentially infectious: semen, vaginal
secretions, CSF, pleural, peritoneal, pericardial, amniotic fluid or tissue
CANNOT transmit: saliva, tears, sweat, non bloody urine or faeces

Per-contact risk estimate for sexual exposures with HIV+ and unprotected
Anal receptive 0.8 – 3.2% Anal insertive 0.02 – 0.2% Vaginal receptive 0.05 – 0.15% Vaginal insertive 0.03 – 0.09% Oral receptive 0.04%

Risk of transmission following accidental needle injury
Hepatitis B virus 6 – 30% Hepatitis C virus 0 – 7%(1.8%) HIV 0 – 0.3%

Typical course of HIV infected person

Entry through mucosal surface/blood
Dendritic cells/macrophages
Transport to regional lymph nodes
CD4 cells infected

Characteristics of acute HIV infection
Acute retroviral syndrome – 50-70% cases Fever,fatigue,rash,myalgia,pharyngitis, lymphadenopathy,night sweats, weight loss, candidiasis, oral ulcers etc.
High viral RNA - mean 12 million copies/ml
CD4 counts decline, CD8 counts rise
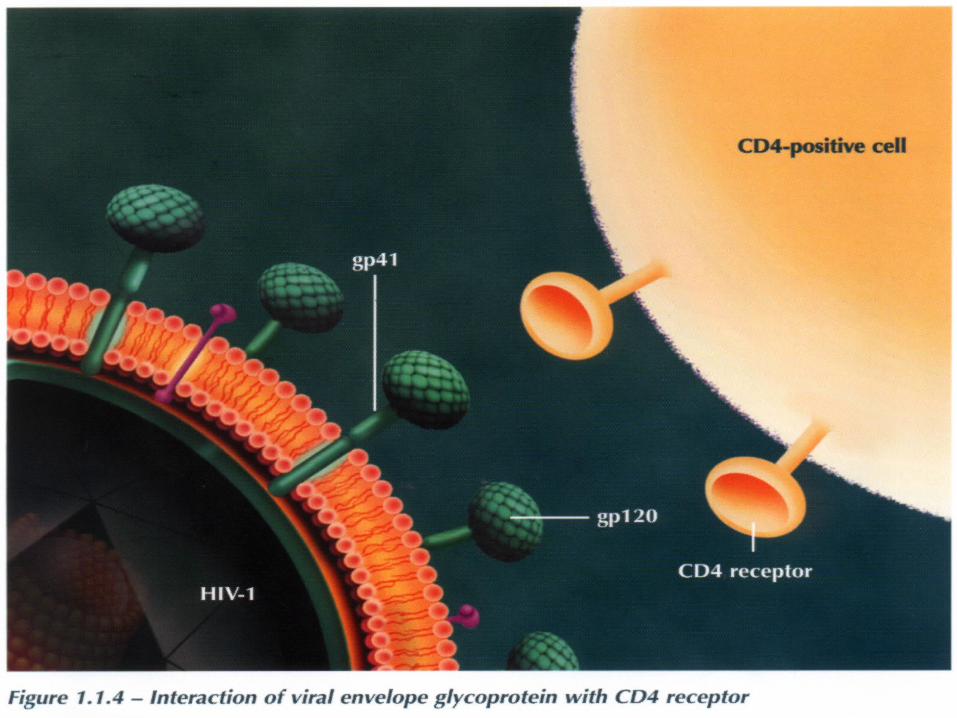
Entry of HIV into human cells
CD4+ receptor CCR5 and CXCR-4 receptors Cells affected :
- CD4+ lymphocytes, naïve and memory (latent pool)
- Macrophages/monocytes
-Tissues such as CNS, testes
Evasion of immune system control
Mutation of virus CD8+ CTLs – deletion of initially
expanded clones due to massive viral antigen exposure
CD8+ CTLs – segregation in the peripheral blood
Large pool of latently infected cells that cannot be eliminated by CD8+ CTLs

Generation of latently infected CD4+T cells
Latently infected cells
A pool of latently infected CD4+T cells present in all HIV individuals
Established early during the course of primary HIV infection
Major obstacle to goal of eradication of virus

Persistent infection
Viral latency is responsible for persistence of HIV
HIV preferentially infects memory CD4 cells whose half-life varies from 6 to 43 months
Even in patients whose viral load < 50 copies/ml for 5 years, this is detectable
Transmission still occurs
Viral dynamics
High levels of viral replication and destruction in plasma and lymph nodes
Almost 10 billion virions produced every day
In primary HIV infection viral population is relatively homogenous
Later due to rapid replication and mutation a diverse population is produced - quasispecies

Viral dynamics
Half life of circulating virion 30 min Productively infected CD4 cell – 1 day Large amount (app. 1 billion) of virus
produced and cleared form circulation each day
HIV1 replication cycle – 1.5 days

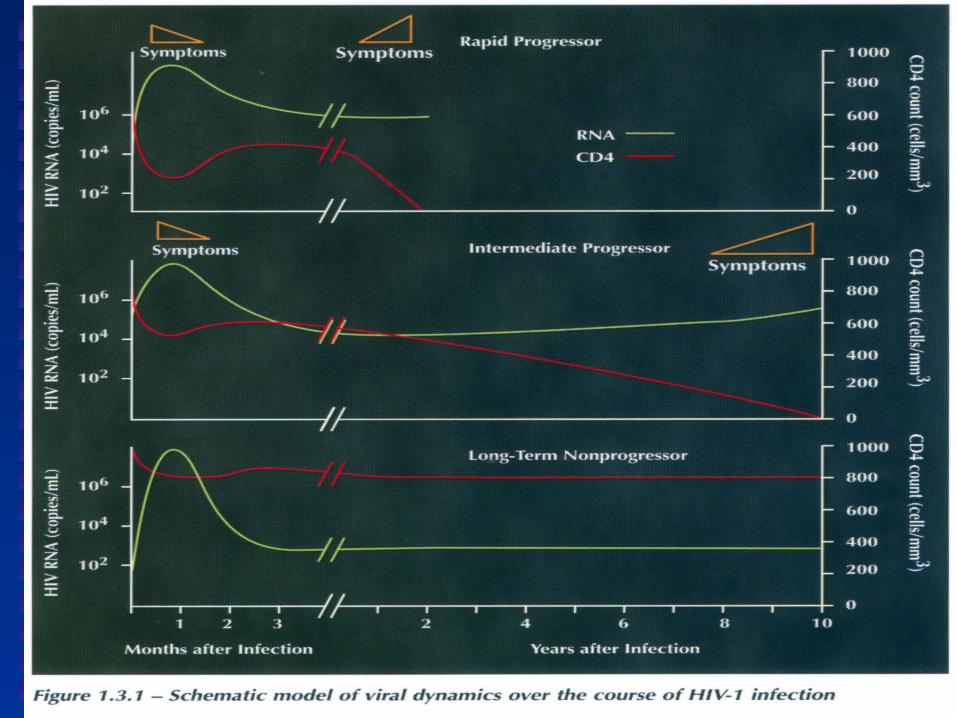
Dynamics of HIV infection in vivo

Viral ‘Set Point’
The level of viral load after seroconversion or virologic equilibrium between viral replication and immunologic containment of viral replication
Higher the set point, more rapid is disease progression
Within the first 6-12 months of infection Initiating antiretroviral therapy may alter
the set point
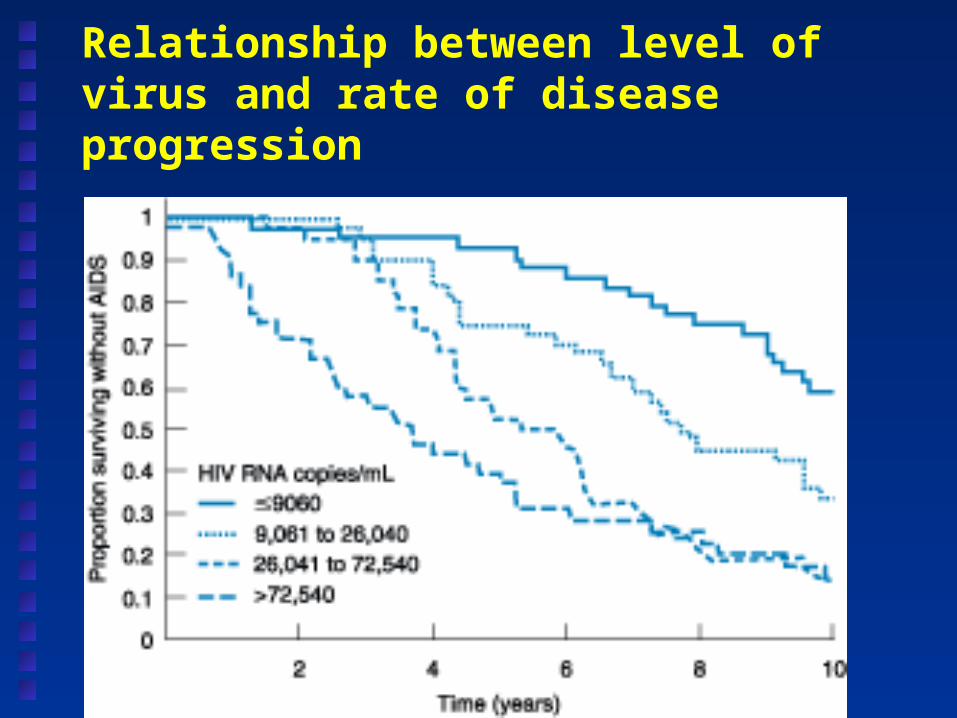
Relationship between level of virus and rate of disease progression

Long term nonprogressors
HIV infection > 10 years, CD4 cells normal range , stable over years and not received ART
They have low viral burden, low level of viremia and normal immune function
No qualitative abnormalities detected in the virus in most patients
Small subset defect in nef gene Host factors : CCR5 – 32 deletion; CCR2 641
mutation; SDF1-3 mutation; RANTES – 28G mutation; maximal HLA heterozygosity of class 1 loci

Mechanism of immunosuppression
Quantitative decrease in CD4+ cells Qualitative decrease in function:
suboptimal responses to vaccines Apoptosis CD4+ maintained for years probably due
to repletion rather than latent virus Decline by an average of 40-80 cells/year
without therapy

Immune responses to HIV
Activation of HIV clones of CD4 T cells and subsequent loss
CD8 cells rapidly increase in acute infection – kill infected cells and secrete chemokines
Gradual failure -‘viral escape’
- HIV actually kills T cells
- decreased production

Summary
Primary HIV infection Early/middle stages of disease – clinical
latency is not disease latency Advanced HIV disease – CD4 < 200
cells/ml Late-stage HIV disease – CD4 < 50
cells/ml