introduction
DESCRIPTION
Introduction. Geraldine Reilly Gilead Science. Objectives. To review TDF interaction data To review triple nucleoside data To discuss the relevance of these data to clinical practice To present the EMTRIVA dataset - PowerPoint PPT PresentationTRANSCRIPT

Introduction
Geraldine Reilly
Gilead Science

Objectives
To review TDF interaction data
To review triple nucleoside data
To discuss the relevance of these data to clinical practice
To present the EMTRIVA dataset
To discuss questions regarding Emtriva and requirements for additional data or information
To review TDF safety data

Nucleoside (cytosine) analogue
One capsule, once daily, without food restrictions
Long intracellular half-life
Significant HIV RNA reductions
Favorable safety profile
Durable efficacy and safety in treatment-naïve and treatment-experienced patients
EMTRIVA™
(emtricitabine)

Mean Steady-State Plasma Emtricitabine Concentration Following 200 mg QD Dose
0.001
0.01
0.1
1
10
0 24 48 72 96 120
Time (hrs post dose)
Pla
sma
Em
tric
itab
ine
Co
nc
(µg
/mL
)
Mean In Vitro IC90
Mean In Vitro IC50
Plasma half-life ~ 10 hours
Wang L, et al. XIV International AIDS Conference, Barcelona 2002, Poster #4546

Intracellular FTC-TP Concentration Following 200 mg QD Dose¹
0.01
0.1
1
10
0 24 48 72 96 120
Time (hrs post dose)
FTC-TP mean half-life ~ 39 hours
1Wang L, et al. XIV International AIDS Conference, Barcelona 2002, Poster #45462Moore K., et al, AIDS 1999;13:2239-50
3TC-TP mean half-life ~ 16 hours²
FT
C-5
'-T
P C
on
c in
PB
MC
(p
mo
le/1
06 cel
ls

Pharmacokinetic Considerations for Approved and Investigational Once-daily NRTIs
0
5
10
15
20
25
30
35
40
45
50
ZDV d4T ABC 3TC FTC
Serum half-life Intracellular half-life
Hou
rs
Investigational Approved Approved Approved ApprovedQD as QD or BID as QD or BID as QD as QD
24 hours
12 hours
Centers for Disease Control and Prevention. MMWR Recomm Rep. 2002;51(RR-7):1-64
TDFddI
* Piliero, et al. 43rd ICAAC, Chicago, 2003. ** Anderson, et al. AIDS 2003; 17(15):2159-2168.
Indicates range where available
* **
**

Forgiveness and Once-dailyAntiretroviral Therapy (ART)
0 24 483612
Time (hours)
QD long half-life
BID
Dru
g c
on
cen
trat
ion
Zone of potential replication
IC90
IC50
Missed Dose
Day 1 Day 2Hypothetical and not
representative of specificARV agents
QD short half-life

Emtricitabine Pharmacology
Once-daily dosing– Serum t1/2 10 hours
– Long intracellular half-life (FTC-TP); t1/2 39 hours
Can be taken without regard to food– 93% in fed or fasted state
Renally cleared– 83% cleared through the kidneys
• Dosage reduction required in renally impaired patients
Few drug interactions– Not a substrate or inhibitor of human CYP450 enzymes
– No known clinically significant drug interactions
Pregnancy Category B

3TC and ABC naiveMonotherapy 10-day dosing vs 3TC (n=81)
Study 102
3TC and ABC naiveMonotherapy 14-day dosing (n=41)
Study 101
Patient PopulationDesign
EmtricitabineMonotherapy Studies
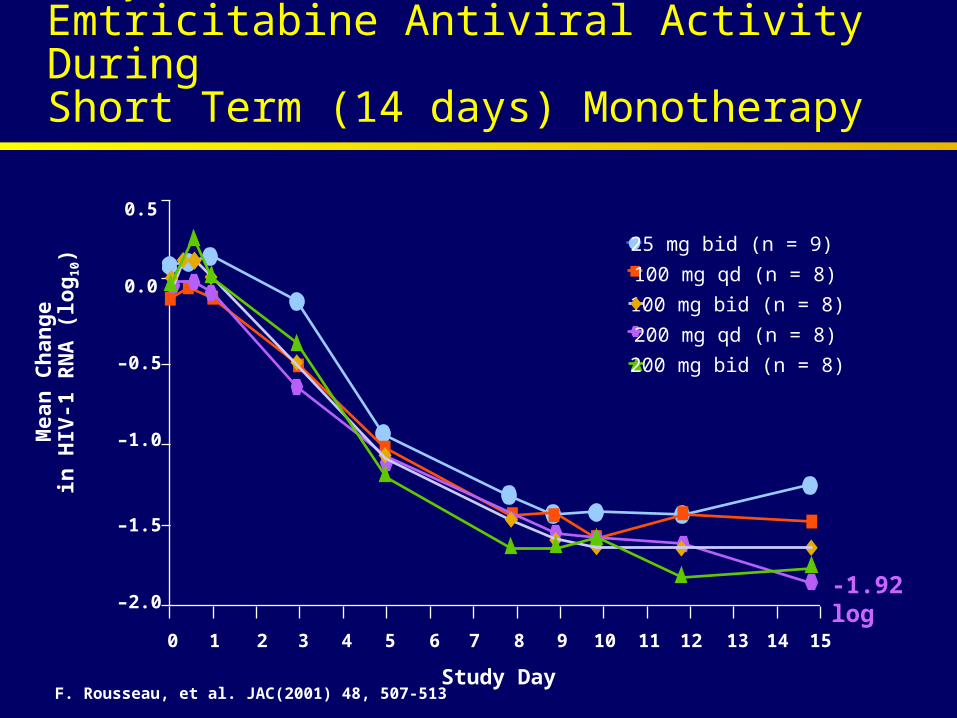
Study 101Emtricitabine Antiviral Activity During Short Term (14 days) Monotherapy
Mea
n C
han
ge
in H
IV-1
RN
A (
log
10)
25 mg bid (n = 9)
100 mg qd (n = 8)
100 mg bid (n = 8)
0.5
0.0
–0.5
–1.0
–1.5
–2.0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Study Day
200 mg qd (n = 8)
200 mg bid (n = 8)
-1.92 log
F. Rousseau, et al. JAC(2001) 48, 507-513

Study 102Emtricitabine Antiviral Activity Compared to Lamivudine150 mg BID in Short Term (10 Days) Monotherapy
0
–0.5
–1.0
–1.5
–2.0
1 2 3 4 5 6 7 8 9 10 11 12
3TC 150 mg bid (n=20)FTC 25 mg qd (n=21)FTC 100 mg qd (n=19)FTC 200 mg qd (n=21)
Study Day
Mea
n C
han
ge
i n
HI V
- 1 R
NA
(L
og
1 0)
Delehanty J. et al, 6th CROI. Chicago 1999. Abstract #16
*p<0.05 for FTC 200 mg QD compared to each of the other treatment arms
-1.7 log
-1.5 logp<0.05*

Study 102Emtricitabine Antiviral Activity Compared to Lamivudine150 mg BID in Short Term (10 Days) Monotherapy
0
–0.5
–1.0
–1.5
–2.0
1 2 3 4 5 6 7 8 9 10 11 12
3TC 150 mg bid (n=20)
FTC 200 mg qd (n=21)
Study Day
Mea
n C
han
ge
i n
HI V
- 1 R
NA
(L
og
1 0)
Delehanty J. et al, 6th CROI. Chicago 1999. Abstract #16
*p<0.05 for FTC 200 mg QD compared to each of the other treatment arms
-1.7 log
-1.5 logp<0.05*
Summary: Preclinical and PK
In vitro preclinical findings
– 10-fold greater relative substrate specificity for HIV-1 RT than 3TC
– 24-fold less relative substrate specificity for mtDNA gamma polymerase
Pharmacokinetics clearly support QD dosing
– Plasma half life of 10 hours with linear kinetics and plasma values > IC90 ~ 84 hrs
– Triphosphate intra-cellular half life ~ 39 hrs Potent antiviral activity
– 1.92 log10 reduction in plasma HIV-1 RNA after 14 days of monotherapy (FTC-101)
– Statistically greater reduction in plasma HIV-1 RNA after 10 days of monotherapy compared to 3TC (FTC-102)

HIV RNA <400 copies/ml
CD4: no restriction
3TC switch to FTC in 3TC-stable patients(n=440)
Study 303
Patient PopulationDesign
Clinical Program Overview:Efficacy and Safety Studies
HIV RNA <400 copies/ml
CD4: no restriction
PI switch to FTC/ddI/EFV (n=355)
ANRS 099(Alize)
Treatment-Naïve Studies
Switch Studies
HIV RNA >5000 copies/ml
CD4: no restriction
FTC vs d4T [+ddI/EFV] (n=571)
Study 301
HIV RNA >5000 copies/ml
CD4 >100 cells/mm³
FTC/ddI/EFV - Open Label (n=40)
ANRS 091(MONTANA)

Study 301

Study 301 Study Design
ART-naive patients
(N = 571)
randomized 1:1,
double-blind
FTC 200 mg QDddI QDEFV QDd4T placebo BID
d4T BIDddI QDEFV QDFTC placebo QD
Week 48
Week 48
Cahn P, et al. 10th CROI, Boston, 2003, Poster #606.

Study 301 Baseline Characteristics
4041HIV-1 RNA >100,000 (%)
324312Mean CD4 count (cells/mm3)
4.84.8Mean HIV-1 RNA (log10)
56%48%Caucasian
86%84%Male
3636Mean age (y)
d4T+ddI+EFV (n=285)
FTC+ddI+EFV (n=286)
Cahn P, et al. 10th CROI, Boston, 2003, Poster #606.

Study 301
Patient Disposition at Week 48
*p<0.05
FTC+ddI+EFV (n=286)
d4T+ddI+EFV (n=285)
Patients Discontinued from Study * 49 (17%) 78 (27%)
D/C due to Adverse Event* 16 (6%) 33 (12%)
Treatment Failure* 8 (3%) 22 (8%)
Other 25 (9%) 23 (8%)
LTFU 9 (3%) 12 (4%)
Request for withdrawal 5 (2%) 4 (1%)
Protocol Violation 7 (2%) 2 (<1%)
Noncompliance 2 (<1%) 3 (1%)
Cahn P, et al. 10th CROI, Boston, 2003, Poster #606.

0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48
Weeks
% P
atie
nts
wit
h H
IV-1
RN
A <
50
cop
ies/
mL
d4T+ddI+EFVFTC+ddI+EFV
BL
74%
58%
p = 0.0001
Intent to Treat (Missing = Failure)
Study 301 % Patients < 50 copies/mL
Cahn P, et al. 10th CROI, Boston, 2003, Poster #606.

0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48
Weeks
% P
atie
nts
wit
h H
IV-1
RN
A <
50
cop
ies/
mL
BL
91%
84%
d4T+ddI+EFVFTC+ddI+EFV
As Treated (Missing = Excluded)
p<0.05
Data on file. Gilead Sciences, Inc. June 2003.
Study 301 % Patients < 50 copies/mL

Study 301 Mean Change From Baseline in Absolute CD4+
0
40
80
120
160
200
BL 4 8 12 16 20 24 28 32 36 40 44 48
Weeks
Me
an
Ch
an
ge
Fro
m B
as
eli
ne
- A
bs
olu
te C
D4
+ C
ell
Co
un
t
d4T+ddI+EFVFTC+ddI+EFV
168
134
p = <0.05
Intent to Treat (Missing = Failure)
Data on file. Gilead Sciences, Inc. June 2003.

* Reported in > 3% of FTC-treated patients in Study 301 or 303 Only events that occurred in > 10% in either arm were analyzed for statistical significance.
p<0.05* *
26%21%19%13%12%13%
25%16%11%4%6%9%
DizzinessInsomniaAbnormal dreams**Neuropathy/Peripheral neuritis**Paresthesia**Depressive disorders
32%23%12%12%
23%13%8%9%
Diarrhea**Nausea**DyspepsiaVomiting
17%25%17%
14%22%12%
Abdominal PainHeadacheAsthenia
D4T+ddI+EFV(n=285)
FTC + ddI + EFV (n=286)Adverse Events
Study 301Selected* Treatment-Emergent Adverse EventsThrough 48 Weeks (All Grades, Regardless of Causality)

p<0.05* *
3%6%
6%5%
MyalgiaArthralgia
10%8%
12%14%
RhinitisIncreased cough**
33%30%Rash event
D4T+ddI+EFV(n=285)
FTC + ddI + EFV (n=286)Adverse Events
Study 301Selected* Treatment-Emergent Adverse EventsThrough 48 Weeks (All Grades, Regardless of Causality)
* Reported in > 3% of FTC-treated patients in Study 301 or 303 Only events that occurred in > 10% in either arm were analyzed for statistical significance.

<1%<1%Bilirubin (>2.5 x ULN)
6%5%ALT (>5.0 x ULN)
9%6%AST (>5.0 x ULN)
11%12%Creatinine Kinase (>4.0 x ULN)
38%34%Percentage with Grade 3 or Grade 4 laboratory abnormality
D4T+ddI+EFV(n=285)
FTC + ddI + EFV (n=286)Number of Patients Treated
* Reported in > 1% of FTC-treated patients in Study 301 or 303** Only events that occurred in > 10% in either arm were analyzed for statistical significance.
Study 301 Treatment-Emergent Grade 3/4 Laboratory Abnormalities* Through 48 Weeks

7%5%Neutrophils (<750 mm3)
6%9%Triglycerides (>750 mg/dL)
3%2%Serum Glucose (<40 or >250 mg/dL)
1%<1%Pancreatic amylase (>2.0 x ULN)
10%5%Serum amylase (>2.0 x ULN)**
2%1%Serum lipase (>2.0 x ULN)
D4T+ddI+EFV(n=285)
FTC + ddI + EFV (n=286)Number of Patients Treated
p<0.05* *
* Reported in > 1% of FTC-treated patients in Study 301 or 303 Only events that occurred in > 10% in either arm were analyzed for statistical significance.
Study 301 Treatment-Emergent Grade 3/4 Laboratory Abnormalities* Through 48 Weeks, Cont

Study 301Virology
FTC-resistant isolates have been selected in vitro – Genotypic analyses demonstrated M184V or M184I mutation
37.5 % (6/16) of isolates from FTC-treated patients with virologic failure in study 301 showed reduced susceptibility to FTC associated with the development of the M184V/I mutation

Interim Analysis: – After last enrolled patient completed 24-weeks of treatment– Median duration of follow-up was 42-weeks– Efficacy and safety data– Results presented at the 42nd ICAAC, September 2002
DSMB Recommendation:– Termination of the double-blind comparative phase of study– d4T-treatment group discontinued and all patients offered open-label
access to the FTC-treatment group
Study Completion: – After last enrolled patient completed 48-weeks of treatment – Median duration of follow-up was 60-weeks– Update of efficacy and results
Study 301DSMB Interim Analysis Review

FTC in Treatment-naïve Patients: Conclusions
FTC+ddI+EFV is a convenient, potent and well- tolerated once-daily regimen in ARV-naïve patients
– Durable efficacy reported to 3 years (MONTANA)
Once-daily FTC demonstrated superior efficacy and safety as compared to twice-daily d4T (FTC 301)

Dose and Dose Interval Adjustments of NRTIs for Patients with Renal Impairment
Drug Renal Impairment
CBV Not recommended
TZV Not recommended
AZT Dose adjust per guidelines
3TC Dose adjust per guidelines
FTC Dose interval adjust per guidelines
TDF Dose interval adjust per guidelines
d4T Dose adjust per guidelines
ddI EC Dose adjust per guidelines
ABC Unknown

Emtricitabine: Dose Interval Adjustment in Renal Impairment

ARV Pregnancy Categorization
Category B: TDF, FTC, ddI
- NFV, RTV, SQV, T-20
Category C: CBV, TRZ, 3TC, AZT, d4T, ABC, ddC
- DLV, NVP, EFV, APV, IDV, IDV/r, fos-APV/r
Category D: Hydroxyurea
FDA Pregnancy Categories – Definitions*
A: Controlled studies in women in first trimester show no risk
B: Animal studies do not indicate risk OR human studies show no risk to fetus (although animal studies may show adverse effect)
C: Animal studies show adverse effects (teratogenic or embryocidal); no controlled studies in pregnant women; weigh benefits versus risks
D: Positive evidence of human risk; benefits may outweigh risks for serious diseases where alternatives not available
X: Risk shown; risk outweighs benefit
*FDA Federal Register

Hyperpigmentation
Hyperpigmentation was rare and generally mild and non-progressive– 3% (29/814) of patients in studies 301,302,303– 28/29 Grade 1; 1/29 Grade 2– Only 2 progressed from Grade 1 to 2
Observed primarily on the palms/soles after 3 months– Median time to onset 88 days– Occurred at a higher rate in black patients (8%)
Never required FTC discontinuation
Resolved in some patients (5/29) while on treatment
Emtricitabine NDA filing June 2003

Hyperpigmentation of the Palms

Nail Discoloration Observed with AZT
Observed primarily on fingernails and toenails1-3
– Color ranges from dark brown to purple1-3
Onset: 4 months to 1 year after starting AZT1-4
Incidence:– In a study of Combivir (AZT/3TC) + ABC, the
incidence of nail discoloration was 5.7%4
– In two retrospective studies, the incidence was 42% and 39%, respectively2,3
• Of those who developed it, 67-82% were African American2,3
1 Rahav et l. Scan J Infect Dis 1992; 24:557-612 Groark et al. J Am Acad Dermatol 1989; 21:1032-3
3 Don et al. Ann Intern Med 1990; 112-145-64 GlaxoWellcome Medical Information

Emtricitabine Virology
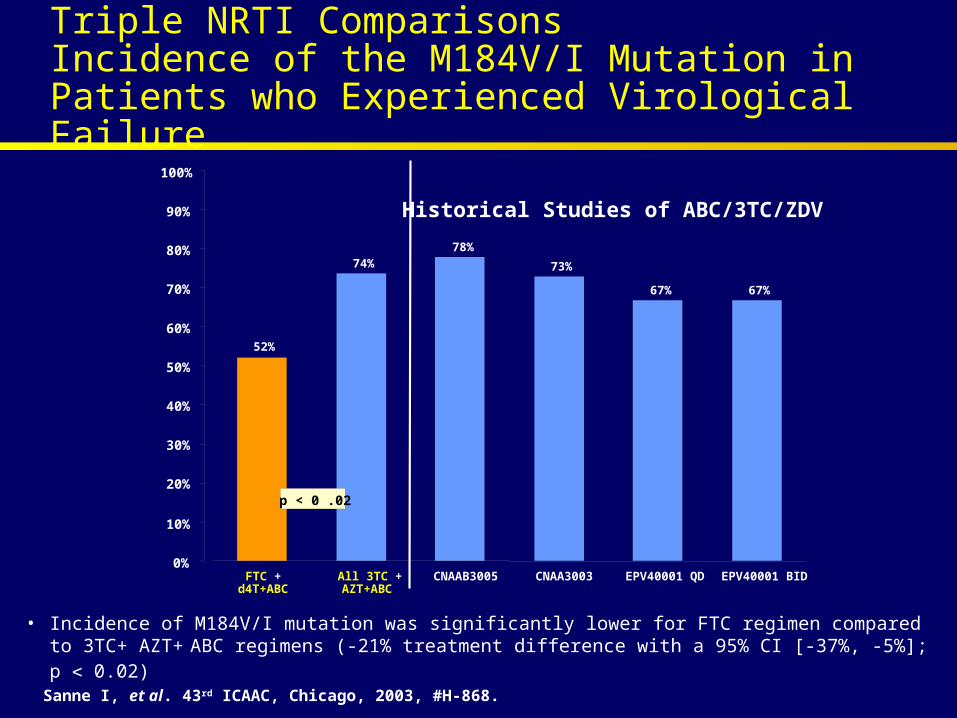
Triple NRTI ComparisonsIncidence of the M184V/I Mutation in Patients who Experienced Virological Failure
52%
74%78%
73%
67% 67%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
FTC +d4T+ABC
All 3TC +AZT+ABC
CNAAB3005 CNAA3003 EPV40001 QD EPV40001 BID
p < 0 .02
• Incidence of M184V/I mutation was significantly lower for FTC regimen compared to 3TC+ AZT+ ABC regimens (-21% treatment difference with a 95% CI [-37%, -5%]; p 0.02)
Sanne I, et al. 43rd ICAAC, Chicago, 2003, #H-868.
Historical Studies of ABC/3TC/ZDV

Future StudiesDiscussion

The Future: TDF/FTC Fixed Dose Combination Tablet
Tenofovir and Emtricitabine fixed dose combination
Study 934 in progressTDF/FTC/EFV vs COM/EFV
Bioequivalence and stability studies in progress

Other Studies
TDF + FTC backbone --– What other studies should be performed to better
characterize the clinical role of this NRTI backbone?
– Specific regimens or third agents?– Different patient populations?– Other?

Other Studies
EMTRIVA --– What other studies should be performed to better
characterize Emtriva and its place in clinical care?
– Comparative trials?– Different patient populations?– Other?

Emtriva & VireadSummary of Similar Characteristics
Durable efficacy in clinical trials– Both Emtriva and Viread have shown efficacy in both treatment-naïve
and treatment-experienced patients
Tolerability and safety
Convenience– Both one tablet dosed once-daily
Pharmacokinetics– Both have long intracellular half-lives, true once-daily dosing– Both can be taken without regard to food
Co-infection– Though not indicated for hepatitis B, both have demonstrated potency
against hepatitis B in co-infected patients
Thank you!